Embed Size (px)
Citation preview
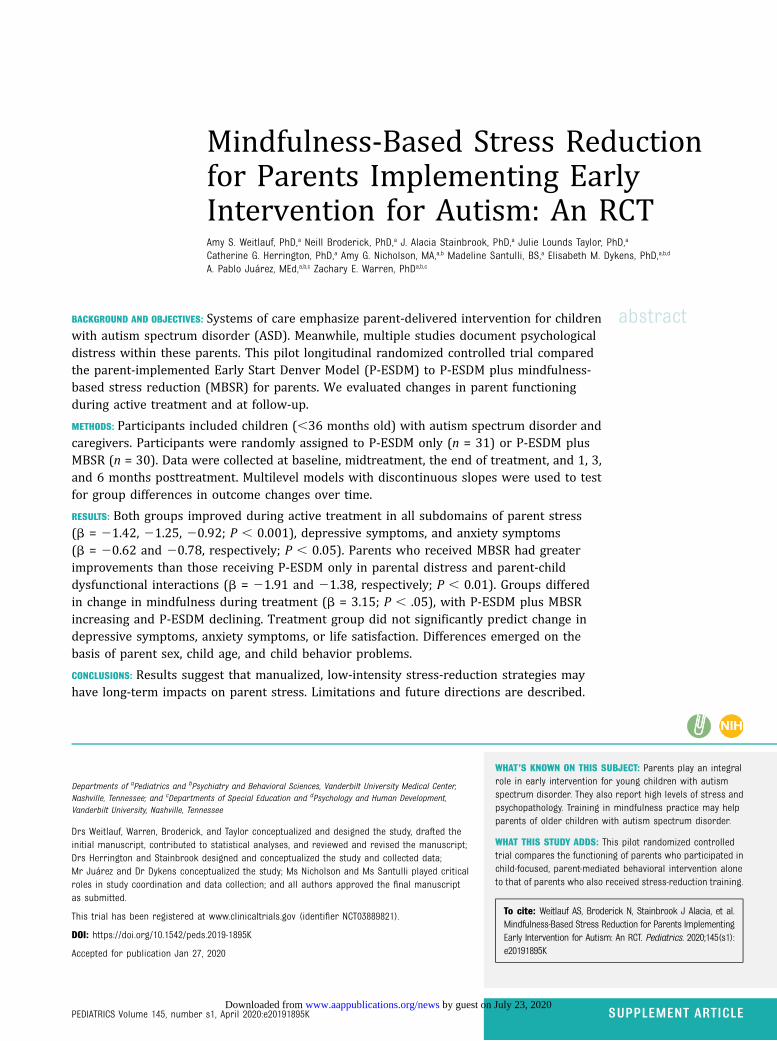
Mindfulness-Based Stress Reductionfor Parents Implementing EarlyIntervention for Autism: An RCTAmy S. Weitlauf, PhD,a Neill Broderick, PhD,a J. Alacia Stainbrook, PhD,a Julie Lounds Taylor, PhD,a
Catherine G. Herrington, PhD,a Amy G. Nicholson, MA,a,b Madeline Santulli, BS,a Elisabeth M. Dykens, PhD,a,b,d
A. Pablo Juárez, MEd,a,b,c Zachary E. Warren, PhDa,b,c
abstractBACKGROUND AND OBJECTIVES: Systems of care emphasize parent-delivered intervention for childrenwith autism spectrum disorder (ASD). Meanwhile, multiple studies document psychologicaldistress within these parents. This pilot longitudinal randomized controlled trial comparedthe parent-implemented Early Start Denver Model (P-ESDM) to P-ESDM plus mindfulness-based stress reduction (MBSR) for parents. We evaluated changes in parent functioningduring active treatment and at follow-up.
METHODS: Participants included children (,36 months old) with autism spectrum disorder andcaregivers. Participants were randomly assigned to P-ESDM only (n = 31) or P-ESDM plusMBSR (n = 30). Data were collected at baseline, midtreatment, the end of treatment, and 1, 3,and 6 months posttreatment. Multilevel models with discontinuous slopes were used to testfor group differences in outcome changes over time.
RESULTS: Both groups improved during active treatment in all subdomains of parent stress(b = 21.42, 21.25, 20.92; P , 0.001), depressive symptoms, and anxiety symptoms(b = 20.62 and 20.78, respectively; P , 0.05). Parents who received MBSR had greaterimprovements than those receiving P-ESDM only in parental distress and parent-childdysfunctional interactions (b = 21.91 and 21.38, respectively; P , 0.01). Groups differedin change in mindfulness during treatment (b = 3.15; P , .05), with P-ESDM plus MBSRincreasing and P-ESDM declining. Treatment group did not significantly predict change indepressive symptoms, anxiety symptoms, or life satisfaction. Differences emerged on thebasis of parent sex, child age, and child behavior problems.
CONCLUSIONS: Results suggest that manualized, low-intensity stress-reduction strategies mayhave long-term impacts on parent stress. Limitations and future directions are described.
WHAT’S KNOWN ON THIS SUBJECT: Parents play an integralrole in early intervention for young children with autismspectrum disorder. They also report high levels of stress andpsychopathology. Training in mindfulness practice may helpparents of older children with autism spectrum disorder.
WHAT THIS STUDY ADDS: This pilot randomized controlledtrial compares the functioning of parents who participated inchild-focused, parent-mediated behavioral intervention aloneto that of parents who also received stress-reduction training.
To cite: Weitlauf AS, Broderick N, Stainbrook J Alacia, et al.Mindfulness-Based Stress Reduction for Parents ImplementingEarly Intervention for Autism: An RCT. Pediatrics. 2020;145(s1):e20191895K
Departments of aPediatrics and bPsychiatry and Behavioral Sciences, Vanderbilt University Medical Center,Nashville, Tennessee; and cDepartments of Special Education and dPsychology and Human Development,Vanderbilt University, Nashville, Tennessee
Drs Weitlauf, Warren, Broderick, and Taylor conceptualized and designed the study, drafted theinitial manuscript, contributed to statistical analyses, and reviewed and revised the manuscript;Drs Herrington and Stainbrook designed and conceptualized the study and collected data;Mr Juárez and Dr Dykens conceptualized the study; Ms Nicholson and Ms Santulli played criticalroles in study coordination and data collection; and all authors approved the final manuscriptas submitted.
This trial has been registered at www.clinicaltrials.gov (identifier NCT03889821).
DOI: https://doi.org/10.1542/peds.2019-1895K
Accepted for publication Jan 27, 2020
PEDIATRICS Volume 145, number s1, April 2020:e20191895K SUPPLEMENT ARTICLE by guest on July 23, 2020www.aappublications.org/newsDownloaded from

Symptoms of autism spectrumdisorder (ASD) may become evidentby age 18 months.1–3 Emergingevidence suggests that earlybehavioral intervention improvesoutcomes,4,5 with some interventionmodels including parents in criticalroles.5 Parent-delivered earlyintervention may promote skillgeneralization and allow systems ofcare to spread therapist time and costacross more children. In parallel,however, multiple studies havedocumented high levels ofpsychological stress and distresswithin the parents of children withASD,6–12 more so than in parents ofchildren with other diagnoses.13–16
Although this distress may negativelyimpact families during a critical timeof diagnostic understanding andservice initiation, little has been doneto deliberately study and supportparents as part of early interventiondelivery.
Parent involvement in interventionmay generalize strategy use acrosssettings.17,18 Incorporating parentsinto treatment is a core component ofmany state early interventionsystems19; as applied to autism, thisframework offers opportunities foraddressing not only child but alsobroader family functioning. However,rigorous studies of parent-mediatedinterventions for young childrenhave yielded mixed results.5,17,20–27
Although undoubtedly influencedby variability within the autismphenotype, parent and familycharacteristics may affect how suchtraining programs are perceived andimplemented.28–30 Parent stress andcoping strategies may be influencedby factors such as parent or child sex,child age, and child problembehaviors.28,29,31–41 Some of theserelations may be reciprocal, withparenting stress changing asa function of, but then also directlyimpacting, child functioning overtime.16,28,29,31,32,42–44 These chroniceffects may therefore impact parent-training paradigms, which emphasize
increased parental responsivity andactive provision of learningopportunities.22,23,45,46
Increasingly, studies haveinvestigated ways to directly supportparents of children withdevelopmental disabilities.47 Onepromising avenue is mindfulness-based stress reduction (MBSR).48
Several studies have documented thatMBSR may reduce stress, improvesleep and health, and increaselife satisfaction for parents ofindividuals with developmentaldisabilities.9,14,49–51 Parents trainedin MBSR report more positivitytoward their children, less negativityregarding their children’s impact onthe family, lower reactivity, and morefrequent use of positive reappraisalstrategies.9,51–53 Parents who practiceself-compassion report lower levelsof depression and parenting stress,44
with 2 studies finding sustainedeffects of mindfulness practiceon parent psychological distressand emotional and behavioraloutcomes.50,53 Although promising,these works primarily deliveredMBSR in isolation to parents ofolder children. One previous studycombined mindfulness-basedtraining for adolescents with ASDwith parallel parent training, withimprovements seen in parental stressand child behavior problems.53
Little is known about how thecombination of MBSR and low levelsof early parent-mediated behavioralintervention impacts the functioningof parents of young children with newASD diagnoses. This work attemptedto address parent stress and distressby providing parents with skills-focused stress-reduction strategiesduring the postdiagnostic period. Theprimary aim of this pilot randomizedcontrolled trial was to compare theeffectiveness of a parent-mediatedbehavioral intervention, the parent-implemented Early Start DenverModel (P-ESDM), to that interventionplus MBSR in enhancing parentfunctioning. We hypothesized that
both groups would improve in parentfunctioning over time and thatcompared with the P-ESDM–onlygroup, parents in P-ESDM plus MBSRwould show greater reductions instress, depression, and anxiety as wellas increased self-reported lifesatisfaction and mindfulness. Asecond aim was to examine whethertreatment response differed on thebasis of 5 covariates: child age attreatment initiation, child sex, parentsex, child autism severity, andbehavior problems.
METHODS
Participants
Participating parents were recruitedfrom a diagnostic clinic from 2015 to2017. Eligibility criteria includedhaving a child (,36 months of age atconsent) with a gold standard ASDdiagnosis and parental Englishfluency. Exclusion criteria includedsevere child sensorimotorimpairment. All procedures wereapproved by the medical centerinstitutional review board.
We used a random-number generatorwith a planned maximum enrollmentof 70 participants. Allowing ∼10%attrition, this provides 80% power todetect an effect size of 0.71 for 1primary outcome or an effect size of0.91 if a multiple-comparisoncorrection was applied for 7coprimary outcomes. We placed halfof the generated numbers into eachgroup. Blinded staff obtained consentthen accessed a unique computer fileto determine group assignment.
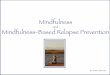
Of 103 eligible families, 63 consentedto participate (Fig 1). Twoparticipants did not have data thatcould be included in analyses: 1(P-ESDM only) provided inaccuratedata and a second (P-ESDM plusMBSR) withdrew without providingany parental data. This yielded a finalsample of 61 families included inanalyses (Tables 1 and 2). Of these 61families, 7 withdrew before
82 WEITLAUF et al by guest on July 23, 2020www.aappublications.org/newsDownloaded from
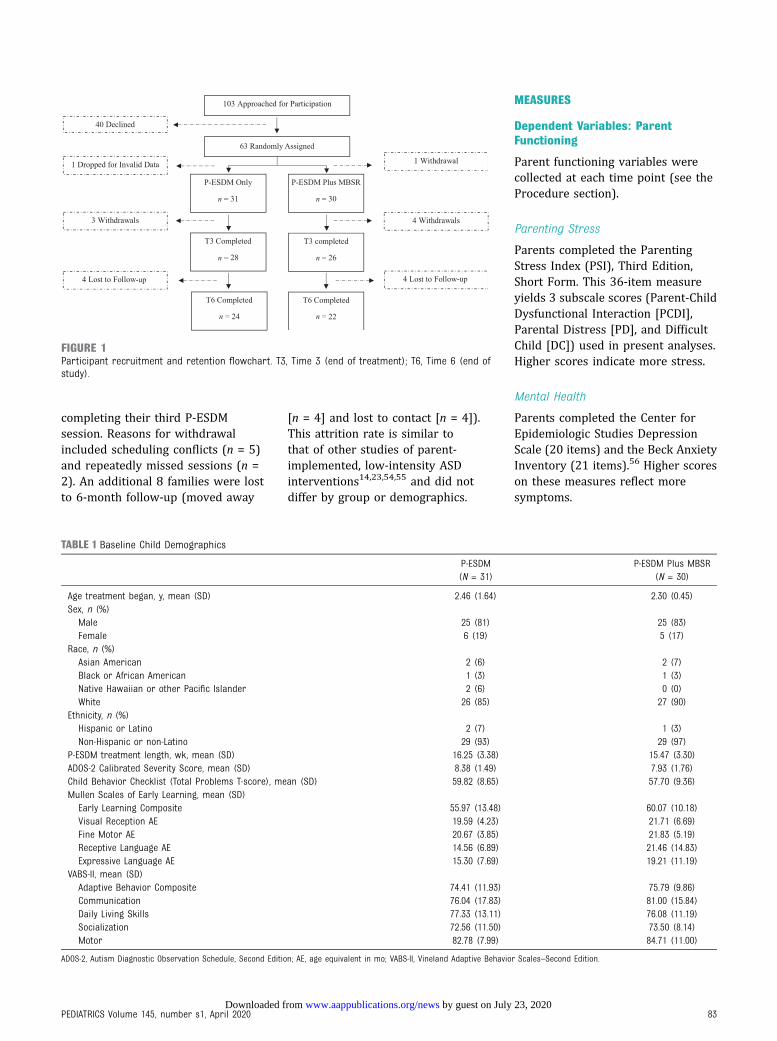
completing their third P-ESDMsession. Reasons for withdrawalincluded scheduling conflicts (n = 5)and repeatedly missed sessions (n =2). An additional 8 families were lostto 6-month follow-up (moved away
[n = 4] and lost to contact [n = 4]).This attrition rate is similar tothat of other studies of parent-implemented, low-intensity ASDinterventions14,23,54,55 and did notdiffer by group or demographics.
MEASURES
Dependent Variables: ParentFunctioning
Parent functioning variables werecollected at each time point (see theProcedure section).
Parenting Stress
Parents completed the ParentingStress Index (PSI), Third Edition,Short Form. This 36-item measureyields 3 subscale scores (Parent-ChildDysfunctional Interaction [PCDI],Parental Distress [PD], and DifficultChild [DC]) used in present analyses.Higher scores indicate more stress.
Mental Health
Parents completed the Center forEpidemiologic Studies DepressionScale (20 items) and the Beck AnxietyInventory (21 items).56 Higher scoreson these measures reflect moresymptoms.
FIGURE 1Participant recruitment and retention flowchart. T3, Time 3 (end of treatment); T6, Time 6 (end ofstudy).
TABLE 1 Baseline Child Demographics
P-ESDM(N = 31)
P-ESDM Plus MBSR(N = 30)
Age treatment began, y, mean (SD) 2.46 (1.64) 2.30 (0.45)Sex, n (%)Male 25 (81) 25 (83)Female 6 (19) 5 (17)
Race, n (%)Asian American 2 (6) 2 (7)Black or African American 1 (3) 1 (3)Native Hawaiian or other Pacific Islander 2 (6) 0 (0)White 26 (85) 27 (90)
Ethnicity, n (%)Hispanic or Latino 2 (7) 1 (3)Non-Hispanic or non-Latino 29 (93) 29 (97)
P-ESDM treatment length, wk, mean (SD) 16.25 (3.38) 15.47 (3.30)ADOS-2 Calibrated Severity Score, mean (SD) 8.38 (1.49) 7.93 (1.76)Child Behavior Checklist (Total Problems T-score), mean (SD) 59.82 (8.65) 57.70 (9.36)Mullen Scales of Early Learning, mean (SD)Early Learning Composite 55.97 (13.48) 60.07 (10.18)Visual Reception AE 19.59 (4.23) 21.71 (6.69)Fine Motor AE 20.67 (3.85) 21.83 (5.19)Receptive Language AE 14.56 (6.89) 21.46 (14.83)Expressive Language AE 15.30 (7.69) 19.21 (11.19)
VABS-II, mean (SD)Adaptive Behavior Composite 74.41 (11.93) 75.79 (9.86)Communication 76.04 (17.83) 81.00 (15.84)Daily Living Skills 77.33 (13.11) 76.08 (11.19)Socialization 72.56 (11.50) 73.50 (8.14)Motor 82.78 (7.99) 84.71 (11.00)
ADOS-2, Autism Diagnostic Observation Schedule, Second Edition; AE, age equivalent in mo; VABS-II, Vineland Adaptive Behavior Scales–Second Edition.
PEDIATRICS Volume 145, number s1, April 2020 83 by guest on July 23, 2020www.aappublications.org/newsDownloaded from
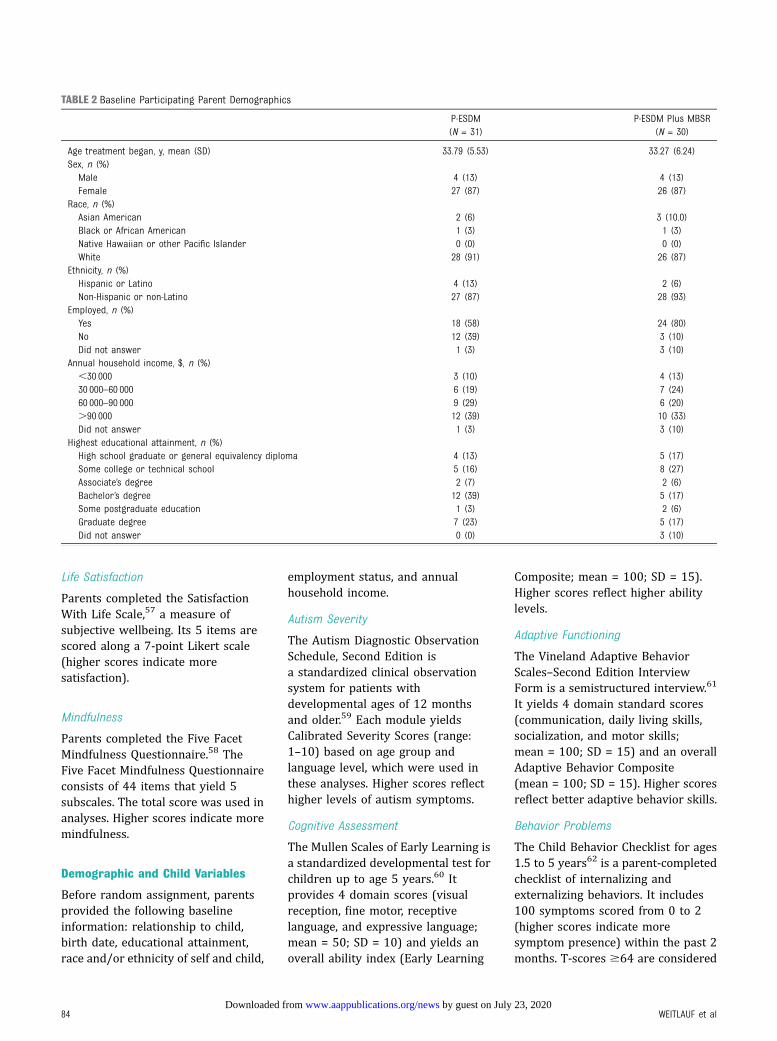
Life Satisfaction
Parents completed the SatisfactionWith Life Scale,57 a measure ofsubjective wellbeing. Its 5 items arescored along a 7-point Likert scale(higher scores indicate moresatisfaction).
Mindfulness
Parents completed the Five FacetMindfulness Questionnaire.58 TheFive Facet Mindfulness Questionnaireconsists of 44 items that yield 5subscales. The total score was used inanalyses. Higher scores indicate moremindfulness.
Demographic and Child Variables
Before random assignment, parentsprovided the following baselineinformation: relationship to child,birth date, educational attainment,race and/or ethnicity of self and child,
employment status, and annualhousehold income.
Autism Severity
The Autism Diagnostic ObservationSchedule, Second Edition isa standardized clinical observationsystem for patients withdevelopmental ages of 12 monthsand older.59 Each module yieldsCalibrated Severity Scores (range:1–10) based on age group andlanguage level, which were used inthese analyses. Higher scores reflecthigher levels of autism symptoms.
Cognitive Assessment
The Mullen Scales of Early Learning isa standardized developmental test forchildren up to age 5 years.60 Itprovides 4 domain scores (visualreception, fine motor, receptivelanguage, and expressive language;mean = 50; SD = 10) and yields anoverall ability index (Early Learning
Composite; mean = 100; SD = 15).Higher scores reflect higher abilitylevels.
Adaptive Functioning
The Vineland Adaptive BehaviorScales–Second Edition InterviewForm is a semistructured interview.61
It yields 4 domain standard scores(communication, daily living skills,socialization, and motor skills;mean = 100; SD = 15) and an overallAdaptive Behavior Composite(mean = 100; SD = 15). Higher scoresreflect better adaptive behavior skills.
Behavior Problems
The Child Behavior Checklist for ages1.5 to 5 years62 is a parent-completedchecklist of internalizing andexternalizing behaviors. It includes100 symptoms scored from 0 to 2(higher scores indicate moresymptom presence) within the past 2months. T-scores $64 are considered
TABLE 2 Baseline Participating Parent Demographics
P-ESDM(N = 31)
P-ESDM Plus MBSR(N = 30)
Age treatment began, y, mean (SD) 33.79 (5.53) 33.27 (6.24)Sex, n (%)Male 4 (13) 4 (13)Female 27 (87) 26 (87)
Race, n (%)Asian American 2 (6) 3 (10.0)Black or African American 1 (3) 1 (3)Native Hawaiian or other Pacific Islander 0 (0) 0 (0)White 28 (91) 26 (87)
Ethnicity, n (%)Hispanic or Latino 4 (13) 2 (6)Non-Hispanic or non-Latino 27 (87) 28 (93)
Employed, n (%)Yes 18 (58) 24 (80)No 12 (39) 3 (10)Did not answer 1 (3) 3 (10)
Annual household income, $, n (%),30 000 3 (10) 4 (13)30 000–60 000 6 (19) 7 (24)60 000–90 000 9 (29) 6 (20).90 000 12 (39) 10 (33)Did not answer 1 (3) 3 (10)
Highest educational attainment, n (%)High school graduate or general equivalency diploma 4 (13) 5 (17)Some college or technical school 5 (16) 8 (27)Associate’s degree 2 (7) 2 (6)Bachelor’s degree 12 (39) 5 (17)Some postgraduate education 1 (3) 2 (6)Graduate degree 7 (23) 5 (17)Did not answer 0 (0) 3 (10)
84 WEITLAUF et al by guest on July 23, 2020www.aappublications.org/newsDownloaded from
clinically significant for broadbandscales. Because of the high correlationbetween internalizing andexternalizing subscales in this work(r = 0.61; P , .001), we used theT-score of the Total Problems scale.
Procedure
After random assignment, familieswere scheduled for their first P-ESDMsession and, when applicable, pairedwith an MBSR therapist. MBSRsessions began after the secondP-ESDM session. Data were collectedat 6 time points: baseline (beforetreatment), midtreatment (6 weeks),end of treatment (12 weeks), and 1, 3,and 6 months posttreatment.
Intervention: P-ESDM
P-ESDM consisted of 12 consecutive,weekly, clinic-based sessions that were∼1 hour long. P-ESDM began anaverage of 1.35 months after diagnosis(SD = 1.45). Because of variable familyschedules, it took an average of15.87 weeks (SD = 3.33) to complete12 sessions. Six P-ESDM therapists(separate from MBSR therapists andblinded to group assignment) werelicensed, board-certified behavioranalysts who were trained in fidelityby ESDM-certified trainers. Thismanualized intervention has a detailedparent-training curriculum anda specific coaching interventionmethod.5 Therapists introduce skillsthrough descriptions, modeling, andcoaching with embedded emphasis onskill generalizability. Fidelity wasmonitored by using the Early StartDenver Model Fidelity Checklist.Therapists covered 94% of intendedcontent across sessions with nosignificant differences seen betweengroups (P . .10).
Intervention: P-ESDM Plus MBSR
Parents who were randomly assignedto P-ESDM plus MBSR attended 6additional 1-hour individual sessions.Child care was provided to maximizeattendance. The 4 MBSR therapistswere clinicians with at least a master’sdegree and expertise in behavioral
intervention and ASD supervised bya licensed clinical psychologist withformal MBSR training. Fidelity wasmonitored by therapist-completedcontent checklists.
The MBSR protocol was based on thework of Dykens et al14 and modifiedfor individual administration forparents of young children with ASD. Itwas introduced as a skills-focusedstress-reduction program rather thanindividual therapy. The clinic-basedsessions covered topics such as anintroduction to mindfulness formanaging stress, awareness of thepresent moment, and cultivatinggratitude. Weekly handouts offeredwritten and pictorial practice cues forthe home. Suggested homeworkexercises included formal practice(eg, guided meditation) as well asactivities that are easily incorporatedinto daily routines (eg, breathawareness). Weekly homework logstracked strategy use.
Data Analysis
Multilevel models with discontinuousslopes, using Hierarchical LinearModeling software,63 were used totest for group differences in outcomechanges over time. This allowed forinclusion of all participants with atleast 1 time point of data. Wemodeled discontinuous rates ofindividual change with 2 timeepochs64: (1) linear slope from thefirst to the third time point (baseline,6 weeks into treatment, andimmediately posttreatment),representing change during activetreatment, and (2) change in linearslope from immediatelyposttreatment through the 6-monthfollow-up (immediatelyposttreatment and 1, 3, and 6 monthsposttreatment), reflecting changeposttreatment. We estimatedmultilevel models for each outcomethat included the between-subjectsvariable of treatment group, withgroups centered on 0 (P-ESDM =20.5; P-ESDM plus MBSR = 0.5).Overall slope estimates in these
models reflect change across theentire sample. Including treatmentgroup allowed us to determine if anyof the slope estimates (sloperepresenting change during activetreatment and change in slope duringposttreatment) significantly differedby treatment group. Additionalbetween-persons covariates includedchild age at treatment initiation, sexof the child, sex of the parent, baselineautism severity, and child behaviorproblems. Because this is pilot work,no corrections for multiplecomparisons were made. Allcovariates were grand mean centered.
RESULTS
Sample Characteristics
No adverse events were reported.Baseline demographic and diagnosticinformation about children andparticipating parents are reported(Tables 1 and 2).
Aim 1: Treatment Effects on ParentOutcomes
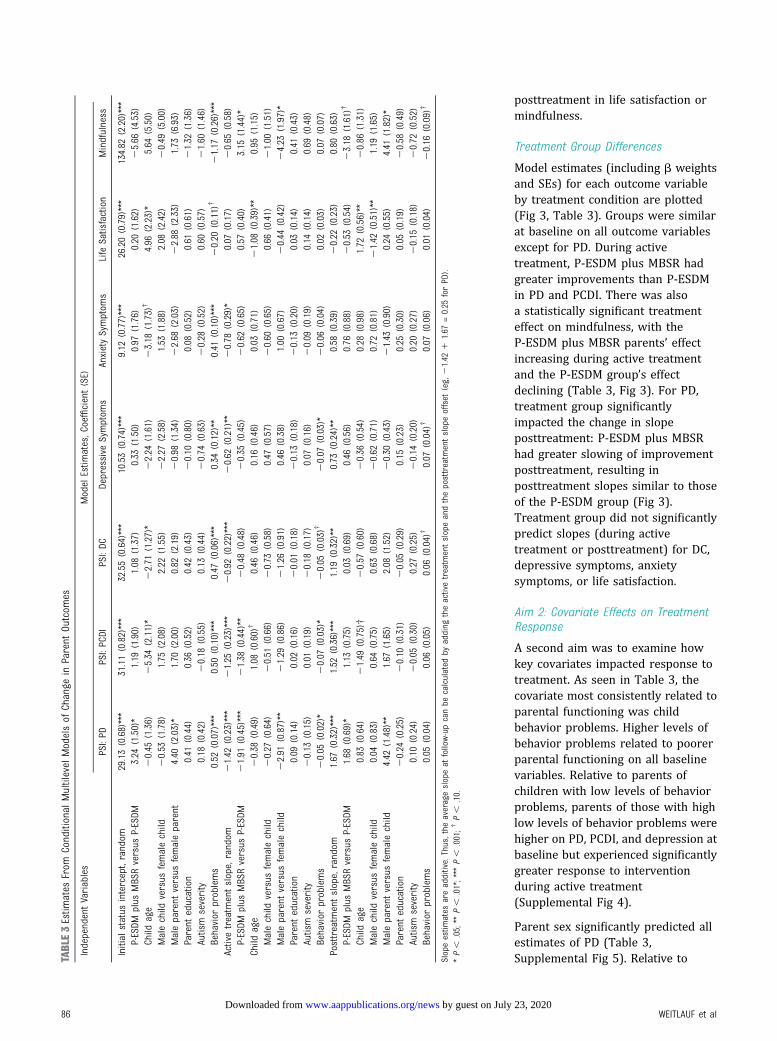
Estimates from the longitudinal modelsconditioned on treatment group andcovariates for each of the outcomevariables are presented (Table 3).
Overall Change
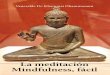
Model estimates (including b weightsand SEs) for overall change across thesample for each outcome variable areplotted (Fig 2, Table 3). Across thesample, there was statisticallysignificant average improvementduring active treatment in allsubdomains of parenting stress (PD,PCDI, and DC), depression symptoms,and anxiety symptoms. For theparenting stress subscales anddepression symptoms, symptomsworsened slightly duringposttreatment data collection (Fig 2).Change in posttreatment slope foranxiety was not statisticallysignificant, indicating thatimprovement continued. There wereno statistically significant averagechanges during active treatment or
PEDIATRICS Volume 145, number s1, April 2020 85 by guest on July 23, 2020www.aappublications.org/newsDownloaded from
posttreatment in life satisfaction ormindfulness.
Treatment Group Differences
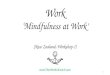
Model estimates (including b weightsand SEs) for each outcome variableby treatment condition are plotted(Fig 3, Table 3). Groups were similarat baseline on all outcome variablesexcept for PD. During activetreatment, P-ESDM plus MBSR hadgreater improvements than P-ESDMin PD and PCDI. There was alsoa statistically significant treatmenteffect on mindfulness, with theP-ESDM plus MBSR parents’ effectincreasing during active treatmentand the P-ESDM group’s effectdeclining (Table 3, Fig 3). For PD,treatment group significantlyimpacted the change in slopeposttreatment: P-ESDM plus MBSRhad greater slowing of improvementposttreatment, resulting inposttreatment slopes similar to thoseof the P-ESDM group (Fig 3).Treatment group did not significantlypredict slopes (during activetreatment or posttreatment) for DC,depressive symptoms, anxietysymptoms, or life satisfaction.
Aim 2: Covariate Effects on TreatmentResponse
A second aim was to examine howkey covariates impacted response totreatment. As seen in Table 3, thecovariate most consistently related toparental functioning was childbehavior problems. Higher levels ofbehavior problems related to poorerparental functioning on all baselinevariables. Relative to parents ofchildren with low levels of behaviorproblems, parents of those with highlow levels of behavior problems werehigher on PD, PCDI, and depression atbaseline but experienced significantlygreater response to interventionduring active treatment(Supplemental Fig 4).
Parent sex significantly predicted allestimates of PD (Table 3,Supplemental Fig 5). Relative toTA
BLE3Estim
ates
From
Conditional
Multilevel
Modelsof
Change
inParent
Outcom
es
IndependentVariables
ModelEstim
ates,C
oefficient(SE)
PSI:PD
PSI:PCDI
PSI:DC
Depressive
Symptom
sAnxietySymptom
sLife
Satisfaction
Mindfulness
Initial
status
intercept,random
29.13(0.68)***
31.11(0.82)***
32.55(0.64)***
10.53(0.74)***
9.12
(0.77)***
26.20(0.79)***
134.82
(2.20)***
P-ESDM
plus
MBSRversus
P-ESDM
3.24
(1.50)*
1.19
(1.90)
1.08
(1.37)
0.33
(1.50)
0.97
(1.76)
0.20
(1.62)
25.66
(4.53)
Child
age
20.45
(1.36)
25.34
(2.11)*
22.71
(1.27)*
22.24
(1.61)
23.18
(1.73)
†4.96
(2.23)*
5.64
(5.50)
Malechild
versus
femalechild
20.53
(1.78)
1.75
(2.08)
2.22
(1.55)
22.27
(2.58)
1.53
(1.88)
2.08
(2.42)
20.49
(5.00)
Maleparent
versus
femaleparent
4.40
(2.03)*
1.70
(2.00)
0.82
(2.19)
20.98
(1.34)
22.68
(2.03)
22.88
(2.33)
1.73
(6.93)
Parent
education
0.41
(0.44)
0.36
(0.52)
0.42
(0.43)
20.10
(0.80)
0.08
(0.52)
0.61
(0.61)
21.32
(1.36)
Autism
severity
0.18
(0.42)
20.18
(0.55)
0.13
(0.44)
20.74
(0.63)
20.28
(0.52)
0.60
(0.57)
21.60
(1.46)
Behavior
problems
0.52
(0.07)***
0.50
(0.10)***
0.47
(0.06)***
0.34
(0.12)**
0.41
(0.10)***
20.20
(0.11)
†21.17
(0.26)***
Activetreatm
entslope,random
21.42
(0.23)***
21.25
(0.23)***
20.92
(0.22)***
20.62
(0.21)**
20.78
(0.29)*
0.07
(0.17)
20.65
(0.58)
P-ESDM
plus
MBSRversus
P-ESDM
21.91
(0.45)***
21.38
(0.44)**
20.48
(0.48)
20.35
(0.45)
20.62
(0.65)
0.57
(0.40)
3.15
(1.44)*
Child
age
20.38
(0.49)
1.08
(0.60)
†0.46
(0.46)
0.16
(0.46)
0.03
(0.71)
21.08
(0.39)**
0.95
(1.15)
Malechild
versus
femalechild
20.27
(0.64)
20.51
(0.66)
20.73
(0.58)
0.47
(0.57)
20.60
(0.65)
0.66
(0.41)
21.00
(1.51)
Maleparent
versus
femalechild
22.91
(0.87)**
21.29
(0.86)
21.26
(0.91)
0.46
(0.38)
1.00
(0.67)
20.44
(0.42)
24.23
(1.97)*
Parent
education
0.09
(0.14)
0.02
(0.16)
20.01
(0.18)
20.13
(0.18)
20.13
(0.20)
0.03
(0.14)
0.41
(0.43)
Autism
severity
20.13
(0.15)
0.01
(0.19)
20.18
(0.17)
0.07
(0.16)
20.09
(0.19)
0.14
(0.14)
0.69
(0.48)
Behavior
problems
20.05
(0.02)*
20.07
(0.03)*
20.05
(0.03)
†20.07
(0.03)*
20.06
(0.04)
0.02
(0.03)
0.07
(0.07)
Posttreatm
entslope,random
1.67
(0.32)***
1.52
(0.36)***
1.19
(0.32)**
0.73
(0.24)**
0.58
(0.39)
20.22
(0.23)
0.80
(0.63)
P-ESDM
plus
MBSRversus
P-ESDM
1.68
(0.69)*
1.13
(0.75)
0.03
(0.69)
0.46
(0.56)
0.76
(0.88)
20.53
(0.54)
23.18
(1.61)
†
Child
age
0.83
(0.64)
21.49
(0.75)†
20.57
(0.60)
20.36
(0.54)
0.28
(0.98)
1.72
(0.56)**
20.86
(1.31)
Malechild
versus
femalechild
0.04
(0.83)
0.64
(0.75)
0.63
(0.68)
20.62
(0.71)
0.72
(0.81)
21.42
(0.51)**
1.19
(1.65)
Maleparent
versus
femalechild
4.42
(1.48)**
1.67
(1.65)
2.08
(1.52)
20.30
(0.43)
21.43
(0.90)
0.24
(0.55)
4.41
(1.82)*
Parent
education
20.24
(0.25)
20.10
(0.31)
20.05
(0.29)
0.15
(0.23)
0.25
(0.30)
0.05
(0.19)
20.58
(0.49)
Autism
severity
0.10
(0.24)
20.05
(0.30)
0.27
(0.25)
20.14
(0.20)
0.20
(0.27)
20.15
(0.18)
20.72
(0.52)
Behavior
problems
0.05
(0.04)
0.06
(0.05)
0.06
(0.04)
†0.07
(0.04)
†0.07
(0.06)
0.01
(0.04)
20.16
(0.09)
†
Slopeestim
ates
areadditive.Thus,the
averageslopeat
follow-upcanbe
calculated
byadding
theactivetreatm
entslopeandtheposttreatm
entslopeoffset
(eg,21.42
11.67
=0.25
forPD).
*P,
.05;**
P,
.01*;***
P,
.001;†
P,
.10.
86 WEITLAUF et al by guest on July 23, 2020www.aappublications.org/newsDownloaded from

mothers, fathers started out withhigher PD scores at baseline, improvedmore rapidly during active treatment,but then had greater slowing ofimprovement during posttreatmentwith scores that began rising duringthis time (whereas mothers stayedmore constant during posttreatment).Parent sex also predicted slopes formindfulness. Only mothers in theP-ESDM plus MBSR group increased inmindfulness during active treatment.Fathers declined in mindfulnessregardless of treatment group,although that decline was lesspronounced if they were in P-ESDMplus MBSR. Change was attenuated inall groups during posttreatment.
Child age predicted initial lifesatisfaction, change in slope duringactive treatment, and change in slopeposttreatment. Parents of youngerchildren at baseline had lifesatisfaction scores that improvedduring treatment but then declinedposttreatment. Parents of olderchildren showed the opposite pattern,
with scores that declined duringtreatment but improvedposttreatment (Supplemental Fig 5).
Other covariates had minimal or noimpact on treatment response. The sexof the child predicted posttreatmentresponse for life satisfaction but notresponse during active treatment.Child autism severity did not relate toinitial status or slopes for any parentaloutcome variables.
Follow-up Analyses
In addition to our primary analyses,we ran multilevel models to examinewhether the point estimates of parentfunctioning at the end of activetreatment (3 months) and the end offollow-up (9 months) differed bygroup. To do this, we reran themultilevel models for each outcomethat included treatment group andcovariates but changed the interceptfrom baseline to the 3-month follow-up and from baseline to the 9-monthfollow-up. Estimates representing thedifference between groups at each of
these time points are presented(Table 4). At the end of activetreatment, P-ESDM plus MBSR hadmarginally lower scores on PD andPCDI. These marginally significantdifferences persisted through the endof follow-up for PCDI. Note that noneof the group differences in pointestimates reached statisticalsignificance at P , .05.
DISCUSSION
This study provided MBSR to theparents of newly diagnosed youngchildren with ASD undergoing low-intensity, parent-mediated earlybehavioral intervention. Thiscombination treatment approachaddressed the well-established riskfor increased parenting stress andpsychopathology while also teachingparents foundational skills forinteracting with their children.
Relative to parents who receivedP-ESDM only, parents who receivedP-ESDM plus MBSR showed
FIGURE 2Model score plots showing average change across the sample during active treatment and follow-up. A, parental distress. B, parent-child dysfunctionalinteractions. C, difficult child. D, depression. E, anxiety. F, life satisfaction. G, mindfulness.
PEDIATRICS Volume 145, number s1, April 2020 87 by guest on July 23, 2020www.aappublications.org/newsDownloaded from
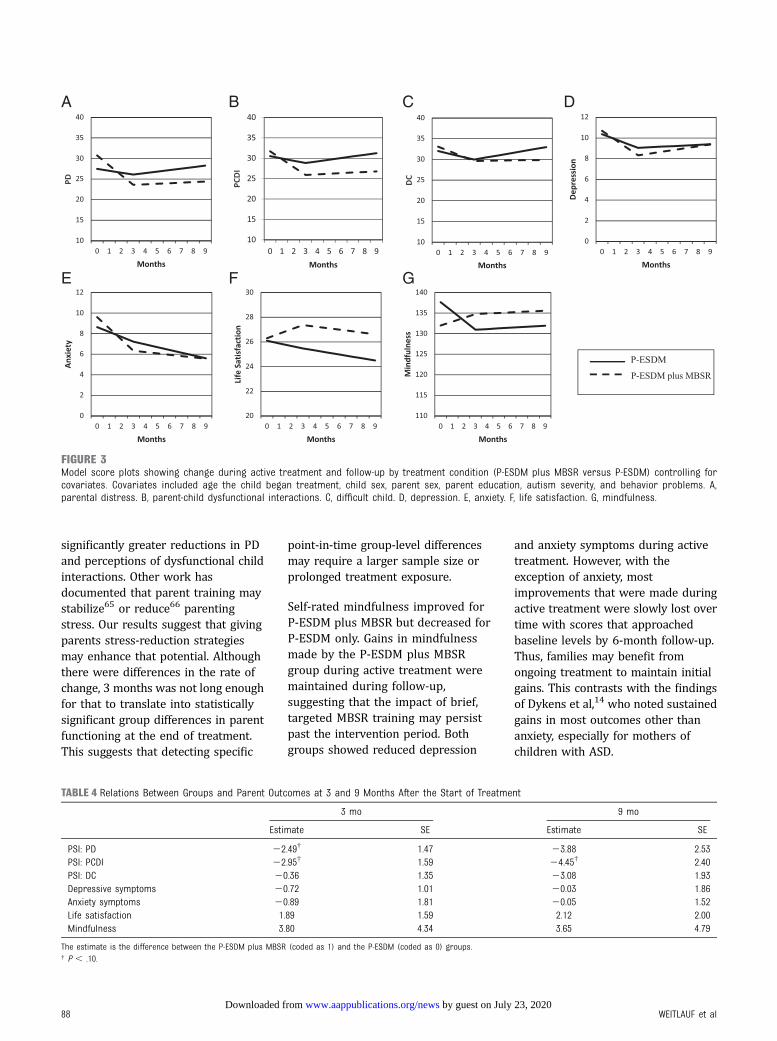
significantly greater reductions in PDand perceptions of dysfunctional childinteractions. Other work hasdocumented that parent training maystabilize65 or reduce66 parentingstress. Our results suggest that givingparents stress-reduction strategiesmay enhance that potential. Althoughthere were differences in the rate ofchange, 3 months was not long enoughfor that to translate into statisticallysignificant group differences in parentfunctioning at the end of treatment.This suggests that detecting specific
point-in-time group-level differencesmay require a larger sample size orprolonged treatment exposure.
Self-rated mindfulness improved forP-ESDM plus MBSR but decreased forP-ESDM only. Gains in mindfulnessmade by the P-ESDM plus MBSRgroup during active treatment weremaintained during follow-up,suggesting that the impact of brief,targeted MBSR training may persistpast the intervention period. Bothgroups showed reduced depression
and anxiety symptoms during activetreatment. However, with theexception of anxiety, mostimprovements that were made duringactive treatment were slowly lost overtime with scores that approachedbaseline levels by 6-month follow-up.Thus, families may benefit fromongoing treatment to maintain initialgains. This contrasts with the findingsof Dykens et al,14 who noted sustainedgains in most outcomes other thananxiety, especially for mothers ofchildren with ASD.
FIGURE 3Model score plots showing change during active treatment and follow-up by treatment condition (P-ESDM plus MBSR versus P-ESDM) controlling forcovariates. Covariates included age the child began treatment, child sex, parent sex, parent education, autism severity, and behavior problems. A,parental distress. B, parent-child dysfunctional interactions. C, difficult child. D, depression. E, anxiety. F, life satisfaction. G, mindfulness.
TABLE 4 Relations Between Groups and Parent Outcomes at 3 and 9 Months After the Start of Treatment
3 mo 9 mo
Estimate SE Estimate SE
PSI: PD 22.49† 1.47 23.88 2.53PSI: PCDI 22.95† 1.59 24.45† 2.40PSI: DC 20.36 1.35 23.08 1.93Depressive symptoms 20.72 1.01 20.03 1.86Anxiety symptoms 20.89 1.81 20.05 1.52Life satisfaction 1.89 1.59 2.12 2.00Mindfulness 3.80 4.34 3.65 4.79
The estimate is the difference between the P-ESDM plus MBSR (coded as 1) and the P-ESDM (coded as 0) groups.† P , .10.
88 WEITLAUF et al by guest on July 23, 2020www.aappublications.org/newsDownloaded from

Covariates emerged as significantpredictors of some outcome variables.Fathers improved more during activetreatment but had greater slowing ofimprovement during follow-up.Fathers may warrant specificattention within the literature as anunderstudied group with potentiallydifferent pathways of stress andcoping.39–41,67–69 Parents whoinitiated treatment at a younger agereported higher levels of stress anddistress at baseline, improved quicklyduring treatment, but had slowedprogress during follow-up relative toslightly older children. Of note,children within our study were on thecusp of transitioning from Part C toPart B services within theDepartment of Education. The impactof changes in concurrent interventionuse on parent outcomes will beexamined in future publications.
Baseline child behavior problemswere related to higher baseline levelsof parenting stress and depression aswell as more rapid improvements inthese outcomes during intervention.It is unclear to what degree this maybe a function of all 3 variables beingself-reported or the phenomenon ofregression to the mean. The relationbetween child behavior problems andparenting stress in ASD is wellestablished70–73 but complex, withrecent work suggesting an iterative,interactive process.37 Future workshould consider how all of thesevariables may interact over timegiven the potential bidirectionalnature of these relationships.37
This initial diagnostic period foryoung children represents a criticalpoint worthy of attention. Higherlevels of parent stress may impacta family’s ability to obtain andimplement intervention.28,46,65 Thisperiod also represents an opportunityfor increased understanding andrelationship building betweenparents and young children, whosecore social and communicationsymptoms may be especiallychallenging for parents to interpret.
Importantly, however, baselineautism severity did not significantlyimpact initial scores on parentingoutcomes nor change in outcomesover time. Rather, it was parent-reported levels of behavioralchallenges that were significantlyrelated to parental stress anddepression.
Although this work was longitudinal,its follow-up time frame wasrelatively brief. Our sample size wasunderpowered to conduct subgroupanalyses and test mechanisms oftreatment response. Severalparticipants were lost to attrition,which was similar across groups andsplit between families that were lostto contact and families that movedaway. This suggests that adding anextra weekly MBSR visit was not toogreat a scheduling burden relative toP-ESDM only. Parents were allowed toreschedule missed sessions, whichadded variability to treatment length.Additionally, analyses included allparticipants who provided valid dataregardless of level of participation;this provided a more conservativeestimate of treatment effects.Although we collected information onfidelity of clinician P-ESDMimplementation, fidelity of parentimplementation was not tracked,preventing us from drawingconclusions about the impact ofMBSR on parents’ treatmentimplementation. Most participantsself-identified as white women,limiting generalizability of results toother groups, and information onparenting self-efficacy was notcollected. Most participating familieshad limited access to high-intensitytreatments, and it is unclear howMBSR would pair with otherintervention models. Also, althoughrandom assignment of children toa no-treatment group would beunethical, without an untreatedgroup, questions remain about whichlongitudinal effects are because oftreatment versus maturation oranother time-related correlate.
Finally, by nature of the study design,the P-ESDM plus MBSR groupreceived more intervention sessionsthan the P-ESDM group. Thus, it isunclear whether additional parentfunctioning gains made by theP-ESDM plus MBSR group are due togreater attention or the MBSRprogram itself. Future work shouldinclude attention-matched groups tofurther evaluate standaloneintervention impact. Examiningmindfulness as a mediator oftreatment on parenting stress willalso be important when determiningwhether MBSR is the mechanism ofaction, as will investigating theimpact of child response tointervention on parent outcomes.
This study suggests that high-quality,low-intensity early intervention wasassociated with improvements in PDand parenting stress. Adding MBSRresulted in additional improvementsin parenting stress. At no point didparents in P-ESDM plus MBSR showmore symptoms of stress than parentsin P-ESDM only, suggesting that theadditional requirements on parents’time did not seem to be harmfulwithin this time-limited interventionstudy. Findings may have implicationsfor systems that partner with parentsto care for young children as well aspractitioners who work directly withparents independent of childintervention. Future analyses willexplore whether particular profiles ofchildren and families are moreamenable to this combination.
ABBREVIATIONS
ASD: autism spectrum disorderDC: Difficult ChildMBSR: mindfulness-based stress
reductionPCDI: Parent-Child Dysfunctional
InteractionPD: Parental DistressPSI: Parenting Stress IndexP-ESDM: parent-implemented
Early Start Denver Model
PEDIATRICS Volume 145, number s1, April 2020 89 by guest on July 23, 2020www.aappublications.org/newsDownloaded from

Address correspondence to Amy S. Weitlauf, PhD, Vanderbilt Kennedy Center, 230 Appleton Place, Private Mailbox 74, Nashville TN 37203. E-mail: amy.s.weitlauf@
vumc.org
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2020 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Supported by the Health Resources and Services Administration and Maternal and Child Health Bureau (R40MC27706) with core support from the Eunice
Kennedy Shriver National Institute of Child Health and Human Development (U54 HD08321). Funded by the National Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Landa R. Early communicationdevelopment and intervention forchildren with autism. Ment Retard DevDisabil Res Rev. 2007;13(1):16–25
2. Franchini M, Hamodat T, Armstrong VL,et al. Infants at risk for autismspectrum disorder: frequency, quality,and variety of joint attention behaviors.J Abnorm Child Psychol. 2019;47(5):907–920
3. Sacrey LR, Zwaigenbaum L, Bryson S,et al. Parent and clinician agreementregarding early behavioral signs in 12-and 18-month-old infants at-risk ofautism spectrum disorder. Autism Res.2018;11(3):539–547
4. Dawson G, Jones EJ, Merkle K, et al.Early behavioral intervention isassociated with normalized brainactivity in young children with autism.J Am Acad Child Adolesc Psychiatry.2012;51(11):1150–1159
5. Rogers SJ, Estes A, Lord C, et al. Effectsof a brief Early Start Denver Model(ESDM)-based parent intervention ontoddlers at risk for autism spectrumdisorders: a randomized controlledtrial. J Am Acad Child AdolescPsychiatry. 2012;51(10):1052–1065
6. Estes A, Munson J, Dawson G, Koehler E,Zhou XH, Abbott R. Parenting stress andpsychological functioning amongmothers of preschool children withautism and developmental delay.Autism. 2009;13(4):375–387
7. Estes A, Olson E, Sullivan K, et al.Parenting-related stress andpsychological distress in mothers oftoddlers with autism spectrumdisorders. Brain Dev. 2013;35(2):133–138
8. Ferna�ndez-Alcántara M, García-Caro MP,Pérez-Marfil MN, Hueso-Montoro C,Laynez-Rubio C, Cruz-Quintana F.Feelings of loss and grief in parents ofchildren diagnosed with autismspectrum disorder (ASD). Res DevDisabil. 2016;55:312–321
9. Jones L, Hastings RP, Totsika V, Keane L,Rhule N. Child behavior problems andparental well-being in families ofchildren with autism: the mediatingrole of mindfulness and acceptance. AmJ Intellect Dev Disabil. 2014;119(2):171–185
10. Tomeny TS. Parenting stress as anindirect pathway to mental healthconcerns among mothers of childrenwith autism spectrum disorder. Autism.2017;21(7):907–911
11. Weitlauf AS, Vehorn AC, Taylor JL,Warren ZE. Relationship satisfaction,parenting stress, and depression inmothers of children with autism.Autism. 2014;18(2):194–198
12. Carter AS, Martínez-Pedraza FL, Gray SA.Stability and individual change indepressive symptoms among mothersraising young children with ASD:maternal and child correlates. J ClinPsychol. 2009;65(12):1270–1280
13. Hamlyn-Wright S, Draghi-Lorenz R, EllisJ. Locus of control fails to mediatebetween stress and anxiety anddepression in parents of children witha developmental disorder. Autism. 2007;11(6):489–501
14. Dykens EM, Fisher MH, Taylor JL,Lambert W, Miodrag N. Reducingdistress in mothers of children withautism and other disabilities:a randomized trial. Pediatrics. 2014;
134(2). Available at: www.pediatrics.org/cgi/content/full/134/2/e454
15. Valicenti-McDermott M, Lawson K,Hottinger K, et al. Parental stress infamilies of children with autism andother developmental disabilities. J ChildNeurol. 2015;30(13):1728–1735
16. Picardi A, Gigantesco A, Tarolla E, et al.Parental burden and its correlates infamilies of children with autismspectrum disorder: a multicentre studywith two comparison groups. Clin PractEpidemiol Ment Health. 2018;14:143–176
17. Carter AS, Messinger DS, Stone WL,Celimli S, Nahmias AS, Yoder P. Arandomized controlled trial of Hanen’s‘More Than Words’ in toddlers withearly autism symptoms. J Child PsycholPsychiatry. 2011;52(7):741–752
18. Strauss K, Mancini F, Fava L; SPC Group.Parent inclusion in early intensivebehavior interventions for youngchildren with ASD: a synthesis of meta-analyses from 2009 to 2011. Res DevDisabil. 2013;34(9):2967–2985
19. Wainer AL, Hepburn S, McMahon GriffithE. Remembering parents in parent-mediated early intervention: anapproach to examining impact onparents and families. Autism. 2017;21(1):5–17
20. Green J, Charman T, Pickles A, et al;BASIS Team. Parent-mediatedintervention versus no intervention forinfants at high risk of autism:a parallel, single-blind, randomisedtrial. Lancet Psychiatry. 2015;2(2):133–140
21. Schreibman L, Dawson G, Stahmer AC,et al. Naturalistic developmentalbehavioral interventions: empiricallyvalidated treatments for autism
90 WEITLAUF et al by guest on July 23, 2020www.aappublications.org/newsDownloaded from

spectrum disorder. J Autism DevDisord. 2015;45(8):2411–2428
22. Kasari C, Gulsrud AC, Wong C, Kwon S,Locke J. Randomized controlledcaregiver mediated joint engagementintervention for toddlers with autism.J Autism Dev Disord. 2010;40(9):1045–1056
23. Kasari C, Lawton K, Shih W, et al.Caregiver-mediated intervention forlow-resourced preschoolers withautism: an RCT. Pediatrics. 2014;134(1).Available at: www.pediatrics.org/cgi/content/full/134/1/e72
24. Wetherby AM, Guthrie W, Woods J, et al.Parent-implemented social interventionfor toddlers with autism: an RCT.Pediatrics. 2014;134(6):1084–1093
25. Nevill RE, Lecavalier L, Stratis EA. Meta-analysis of parent-mediatedinterventions for young children withautism spectrum disorder. Autism.2018;22(2):84–98
26. Tarver J, Palmer M, Webb S, et al. Childand parent outcomes following parentinterventions for child emotional andbehavioral problems in autismspectrum disorders: a systematicreview and meta-analysis. Autism. 2019;23(7):1630–1644
27. Rogers SJ, Estes A, Lord C, et al. Amultisite randomized controlled two-phase trial of the Early Start DenverModel compared to treatment as usual.J Am Acad Child Adolesc Psychiatry.2019;58(9):853–865
28. Karp EA, Dudovitz R, Nelson BB, et al.Family characteristics and children’sreceipt of autism services in low-resourced families. Pediatrics. 2018;141(suppl 4):S280–S286
29. Carr T, Shih W, Lawton K, Lord C, King B,Kasari C. The relationship betweentreatment attendance, adherence, andoutcome in a caregiver-mediatedintervention for low-resourced familiesof young children with autismspectrum disorder. Autism. 2016;20(6):643–652
30. Strauss K, Vicari S, Valeri G, D’Elia L,Arima S, Fava L. Parent inclusion inEarly Intensive Behavioral Intervention:the influence of parental stress, parenttreatment fidelity and parent-mediatedgeneralization of behavior targets on
child outcomes. Res Dev Disabil. 2012;33(2):688–703
31. Hartley SL, Papp LM, Bolt D. Spillover ofmarital interactions and parentingstress in families of children withautism spectrum disorder. J Clin ChildAdolesc Psychol. 2018;47(sup1):S88–S99
32. Croen LA, Shankute N, Davignon M,Massolo ML, Yoshida C. Demographicand clinical characteristics associatedwith engagement in behavioral healthtreatment among children with autismspectrum disorders. J Autism DevDisord. 2017;47(11):3347–3357
33. Seymour M, Giallo R, Wood CE. Thepsychological and physical health offathers of children with AutismSpectrum Disorder compared tofathers of children with long-termdisabilities and fathers of childrenwithout disabilities. Res Dev Disabil.2017;69:8–17
34. Moody EJ, Reyes N, Ledbetter C, et al.Screening for autism with the SRS andSCQ: variations across demographic,developmental and behavioral factorsin preschool children. J Autism DevDisord. 2017;47(11):3550–3561
35. Neuhaus E, Beauchaine TP, Bernier RA,Webb SJ. Child and familycharacteristics moderate agreementbetween caregiver and clinician reportof autism symptoms. Autism Res. 2018;11(3):476–487
36. McStay RL, Dissanayake C, Scheeren A,Koot HM, Begeer S. Parenting stressand autism: the role of age, autismseverity, quality of life and problembehaviour of children and adolescentswith autism. Autism. 2014;18(5):502–510
37. Rodriguez G, Hartley SL, Bolt D.Transactional relations betweenparenting stress and child autismsymptoms and behavior problems.J Autism Dev Disord. 2019;49(5):1887–1898
38. Falk NH, Norris K, Quinn MG. The factorspredicting stress, anxiety anddepression in the parents of childrenwith autism. J Autism Dev Disord. 2014;44(12):3185–3203
39. Dardas LA, Ahmad MM. Predictors ofquality of life for fathers and mothersof children with autistic disorder. ResDev Disabil. 2014;35(6):1326–1333
40. Foody C, James JE, Leader G. Parentingstress, salivary biomarkers, andambulatory blood pressure:a comparison between mothers andfathers of children with autismspectrum disorders. J Autism DevDisord. 2015;45(4):1084–1095
41. McStay RL, Trembath D, Dissanayake C.Stress and family quality of life inparents of children with autismspectrum disorder: parent gender andthe double ABCX model. J Autism DevDisord. 2014;44(12):3101–3118
42. Bessette Gorlin J, McAlpine CP, GarwickA, Wieling E. Severe childhood autism:the family lived experience. J PediatrNurs. 2016;31(6):580–597
43. Hsiao YJ, Higgins K, Pierce T, WhitbyPJS, Tandy RD. Parental stress, familyquality of life, and family-teacherpartnerships: families of children withautism spectrum disorder. Res DevDisabil. 2017;70:152–162
44. Neff KD, Faso DJ. Self-compassion andwell-being in parents of children withautism. Mindfulness. 2015;6:938–947
45. Davlantis KS, Estes A, Dawson G, RogersSJ. A novel method for measuringlearning opportunities provided byparents to young children with autismspectrum disorder. Autism. 2019;23(6):1563–1574
46. Watson LR, Crais ER, Baranek GT, et al.Parent-mediated intervention for one-year-olds screened as at-risk for autismspectrum disorder: a randomizedcontrolled trial. J Autism Dev Disord.2017;47(11):3520–3540
47. Catalano D, Holloway L, Mpofu E. Mentalhealth interventions for parent carersof children with autistic spectrumdisorder: practice guidelines froma Critical Interpretive Synthesis (CIS)systematic review. Int J Environ ResPublic Health. 2018;15(2):E341
48. Kabat-Zinn J. An outpatient program inbehavioral medicine for chronic painpatients based on the practice ofmindfulness meditation: theoreticalconsiderations and preliminary results.Gen Hosp Psychiatry. 1982;4(1):33–47
49. Da Paz NS, Wallander JL. Interventionsthat target improvements in mentalhealth for parents of children withautism spectrum disorders: a narrativereview. Clin Psychol Rev. 2017;51:1–14
PEDIATRICS Volume 145, number s1, April 2020 91 by guest on July 23, 2020www.aappublications.org/newsDownloaded from
50. Lunsky Y, P Hastings R, Weiss JA, MPalucka A, Hutton S, White K.Comparative effects of mindfulness andsupport and information groupinterventions for parents of adults withautism spectrum disorder and otherdevelopmental disabilities. J Autism DevDisord. 2017;47(6):1769–1779
51. Neece CL. Mindfulness-based stressreduction for parents of young childrenwith developmental delays: implicationsfor parental mental health and childbehavior problems. J Appl Res IntellectDisabil. 2014;27(2):174–186
52. Rayan A, Ahmad M. Effectiveness ofmindfulness-based interventions onquality of life and positive reappraisalcoping among parents of children withautism spectrum disorder. Res DevDisabil. 2016;55:185–196
53. Ridderinkhof A, de Bruin EI, Blom R,Bögels SM. Mindfulness-based programfor children with autism spectrumdisorder and their parents: direct andlong-term improvements. Mindfulness(N Y). 2018;9(3):773–791
54. Rogers SJ, Estes A, Vismara L, et al.Enhancing low-intensity coaching inparent implemented Early Start DenverModel intervention for early autism:a randomized comparison treatmenttrial. J Autism Dev Disord. 2019;49(2):632–646
55. Kasari C, Gulsrud A, Paparella T,Hellemann G, Berry K. Randomizedcomparative efficacy study of parent-mediated interventions for toddlerswith autism. J Consult Clin Psychol.2015;83(3):554–563
56. Beck AT, Epstein N, Brown G, Steer RA.An inventory for measuring clinicalanxiety: psychometric properties.J Consult Clin Psychol. 1988;56(6):893–897
57. Diener E, Emmons RA, Larsen RJ, GriffinS. The satisfaction with life scale. J PersAssess. 1985;49(1):71–75
58. Baer RA, Smith GT, Hopkins J,Krietemeyer J, Toney L. Using self-report assessment methods to explorefacets of mindfulness. Assessment.2006;13(1):27–45
59. Lord C, Risi S, Lambrecht L, et al. Theautism diagnostic observationschedule-generic: a standard measureof social and communication deficitsassociated with the spectrum ofautism. J Autism Dev Disord. 2000;30(3):205–223
60. Mullen EL. Mullen Scales of EarlyLearning. Circle Pines, MN: AmericanGuidance Service; 1995
61. Sparrow SS, Cicchetti DV. Diagnosticuses of the Vineland Adaptive BehaviorScales. J Pediatr Psychol. 1985;10(2):215–225
62. Achenbach TM. Achenbach ChildBehavior Checklist. Burlington, VT:ASEBA; 2001
63. Raudenbush SW, Bryk AS. HierarchicalLinear Models: Applications and DataAnalysis Methods. vol. Vol 1. ThousandOaks, CA: Sage Publications; 2002
64. Singer JD, Willett JB. AppliedLongitudinal Data Analysis: ModelingChange and Event Occurrence. NewYork, NY: Oxford University Press; 2003
65. Estes A, Vismara L, Mercado C, et al. Theimpact of parent-delivered interventionon parents of very young children withautism. J Autism Dev Disord. 2014;44(2):353–365
66. Iadarola S, Levato L, Harrison B, et al.Teaching parents behavioral strategiesfor autism spectrum disorder (ASD):effects on stress, strain, andcompetence. J Autism Dev Disord. 2018;48(4):1031–1040
67. Jones L, Totsika V, Hastings RP, PetalasMA. Gender differences when parentingchildren with autism spectrumdisorders: a multilevel modelingapproach. J Autism Dev Disord. 2013;43(9):2090–2098
68. Langley E, Totsika V, Hastings RP.Parental relationship satisfaction infamilies of children with autismspectrum disorder (ASD): a multilevelanalysis. Autism Res. 2017;10(7):1259–1268
69. Hastings RP, Kovshoff H, Ward NJ, degliEspinosa F, Brown T, Remington B.Systems analysis of stress and positiveperceptions in mothers and fathers ofpre-school children with autism.J Autism Dev Disord. 2005;35(5):635–644
70. Shattuck PT, Seltzer MM, Greenberg JS,et al. Change in autism symptoms andmaladaptive behaviors in adolescentsand adults with an autism spectrumdisorder. J Autism Dev Disord. 2007;37(9):1735–1747
71. Lounds J, Seltzer MM, Greenberg JS,Shattuck PT. Transition and change inadolescents and young adults withautism: longitudinal effects on maternalwell-being. Am J Ment Retard. 2007;112(6):401–417
72. Argumedes M, Lanovaz MJ, Larivée S.Brief report: impact of challengingbehavior on parenting stress inmothers and fathers of children withautism spectrum disorders. J AutismDev Disord. 2018;48(7):2585–2589
73. Lecavalier L, Leone S, Wiltz J. The impactof behaviour problems on caregiverstress in young people with autismspectrum disorders. J Intellect DisabilRes. 2006;50(pt 3):172–183
92 WEITLAUF et al by guest on July 23, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2019-1895K2020;145;S81Pediatrics
A. Pablo Juárez and Zachary E. WarrenDykens,Catherine G. Herrington, Amy G. Nicholson, Madeline Santulli, Elisabeth M.
Amy S. Weitlauf, Neill Broderick, J. Alacia Stainbrook, Julie Lounds Taylor,Intervention for Autism: An RCT
Mindfulness-Based Stress Reduction for Parents Implementing Early
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/145/Supplement_1/S81including high resolution figures, can be found at:
References
BIBLhttp://pediatrics.aappublications.org/content/145/Supplement_1/S81#This article cites 67 articles, 2 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 23, 2020www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2019-1895K2020;145;S81Pediatrics
A. Pablo Juárez and Zachary E. WarrenDykens,Catherine G. Herrington, Amy G. Nicholson, Madeline Santulli, Elisabeth M.
Amy S. Weitlauf, Neill Broderick, J. Alacia Stainbrook, Julie Lounds Taylor,Intervention for Autism: An RCT
Mindfulness-Based Stress Reduction for Parents Implementing Early
http://pediatrics.aappublications.org/content/145/Supplement_1/S81located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2020has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on July 23, 2020www.aappublications.org/newsDownloaded from