Embed Size (px)
Citation preview

A
IsioMtiaaCifP
K
I
pmaabt
dc
PT
1h
Available online at www.sciencedirect.com
European Journal of Integrative Medicine 5 (2013) 296–307
Review article
Mind–body therapies for functional bowel disorders—A review of recentclinical trials�
Oliver Grundmann a,b,∗, Saunjoo L. Yoon b
a College of Pharmacy, Department of Medicinal Chemistry, University of Florida, FL 32610, USAb College of Nursing, Department of Adult and Elderly, University of Florida, FL 32610, USA
Received 23 October 2012; received in revised form 28 March 2013; accepted 30 March 2013
bstract
ntroduction: Functional bowel disorders (FBDs) significantly affect a person’s daily life; however, because their diagnosis is mostly based onymptom presentation, time to diagnosis is long. This delay in diagnosis remains true even when other methods, such as biochemical parameters,mmunogenic and inflammatory markers, are used to differentiate the type of disorder. As treatment approaches are mainly symptom-based andften result in suboptimal outcomes, mind–body therapies may offer benefits either used alone or in combination with pharmacological treatments.ethodology: Thus, the purposes of this article are to: (1) describe the scientific knowledge based on currently available clinical trials of mind–body
herapies for FBDs, (2) examine potential benefits of using such therapies and, (3) provide recommendations regarding their clinical applicationn the treatment of FBDs. The literature search covered the last decade from June 2002 to June 2012 and resulted in a total of 19 original researchrticles that met the inclusion criteria. The four common mind–body therapies, which include yoga, hypnotherapy, cognitive behavioral therapy,nd biofeedback, were examined in this article.onclusion: The heterogeneity of clinical study designs as well as the wide disparity in defining primary outcome variables often limits the compar-
son of studies on the same mind–body therapy. Overall findings of these studies were promising, but not conclusive, and further recommendationsor the research direction of mind–body therapies are proposed.ublished by Elsevier GmbH.
eywords: CAM; Functional bowel disorders; Hypnotherapy; Mind–body therapies; Yoga
rt6fts
ntroduction
Functional bowel disorders (FBDs) represent a significantortion of gastrointestinal disorders with a high prevalence esti-ated in the range of 15–35% of adults [1,2]. The classification
nd diagnosis of FBDs is based on symptom representation
nd has been classified by the Rome foundation into irritableowel syndrome (IBS), functional bloating, functional constipa-ion, functional diarrhea, and unclassified FBDs [1]. The mostAbbreviations: FBD, functional bowel disorder; IBS, irritable bowel syn-rome; 5-HT, serotonin; CAM, complementary and alternative medicine; CBT,ognitive behavioral therapy; GI, gastrointestinal.� Editor’s Choice.∗ Corresponding author at: Department of Medicinal Chemistry, College ofharmacy, University of Florida, P.O. Box 100485, Gainesville, FL 32610, USA.el.: +1 352 246 4994; fax: +1 352 392 9455.
E-mail address: [email protected] (O. Grundmann).
s
ooiFstitId
876-3820/$ – see front matter. Published by Elsevier GmbH.ttp://dx.doi.org/10.1016/j.eujim.2013.03.007
ecent Rome III criteria define FBDs as a subgroup of func-ional gastrointestinal disorders with onset of symptoms at least
months prior to diagnosis and other diagnostic criteria activeor 3 months [3]. In spite of differential diagnosis and classifica-ion, treatment for FBDs is primarily based on patient-specificymptoms because of their unclear pathophysiology as well asignificant overlap in symptoms among the different types.
While previous classifications were based on the presencef symptoms, the new classification indicates that pathophysi-logical parameters such as morphological, biochemical, andmmunogenic changes can be evaluated for the diagnosis ofBDs [4]. For instance, there is significant indication thaterotonin transmission and receptors, which are located inhe intestinal tract and central nervous system, as well as
mmunogenic responses, inflammatory markers, and preexis-ing conditions, contribute to the development of IBS [5–7].n addition, the development of functional constipation andiarrhea—hallmarks of IBS—may result from an imbalance of
rnal o
cdihU
psaoan5dfartIatw
nm“btcgas[spof
rtnaa(uaoorptlh[tta
atuafar(pt
M
eCIt(TtUaemb
lJC“b“srasF(rsv
R
Y
pttvt
O. Grundmann, S.L. Yoon / European Jou
holinergic and serotonergic nerve transmission and receptorysfunction in the enteric system [8]. Although more researchs needed, new ways of identifying and classifying symptomsave led to more frequent and accurate diagnoses of IBS in theS [9].More frequent diagnoses, however, do not correlate to better
harmacological treatment approaches, which have demon-trated limited success due to the pain sensitivity that oftenccompanies other symptoms. For example, laxatives and theff-label use of a serotonin 5-HT4 receptor agonist, tegaserod,re predominantly used for constipation [10] while opioid ago-ists such as loperamide and diphenoxylate and a serotonin-HT3 antagonist (i.e., alosetron), may be used for managingiarrhea [5]. The reduction of bloating and gas formation—otherrequent symptoms of FBDs—can be achieved with surfactantsnd changes in lifestyle and diet restrictions [9]. Smooth muscleelaxants, tricyclic antidepressants, and selective serotonin reup-ake inhibitors can also be used for general symptom relief [5].n sum, despite the many pharmacological approaches that arevailable and because of the variety of often conflicting symp-oms, there is no silver bullet to alleviate conditions associatedith FBDs.Because pathophysiological as well as psychosocial compo-
ents affect symptom severity of FBDs [1], one of the solutionsay be the use of mind–body therapies, which are defined as
focusing on the interactions among the brain, mind, body, andehavior, with the intent to use the mind to affect physical func-ioning and promote health” [11]. Under this definition, yoga, Taihi, meditation, hypnotherapy, deep-breathing exercises, pro-ressive relaxation, and acupuncture, are mind–body therapiess they serve to raise awareness of body sensations and engage inelf-regulation of body processes in order to alleviate symptoms12,13]. One study pointed out that women with FBDs haveignificantly lower expectations of success and benefits fromsychological interventions such as cognitive behavioral therapyr yoga than from taking oral medications although psychosocialactors predominantly determined improvement [14].
Although historically these therapies have not been popular,ecent years have shown an increase in interest and use: indeed,he 2007 National Health Interview Survey results showed thatearly 4 out of 10 US adults use some form of complementarynd alternative medicine (CAM) with a rise in mind–body ther-pies, specifically deep-breathing exercises (12.7%), meditation9.4%), and yoga (6.1%) [15]. Despite the rise in general pop-larity, CAM was only used by 1.2% of US adults for stomachnd gastrointestinal disorders [15], indicating that there is anpportunity for CAM to play an increased role in the treatmentf FBDs, particularly if patients are as receptive to using it asecent surveys have shown. When Harris and Roberts asked 256atients with IBS about the acceptability of certain treatments,hey found that tablets were most acceptable (84%) followed byife-style changes (82%), yoga (77%), stomach cream (68%),omeopathy (65%), heat pad (64%) and hypnotherapy (64%)
16]. Another study revealed that 50% of IBS patients are turningo CAM because of low satisfaction levels with conventionalreatment, and that hypnotherapy and cognitive behavior ther-py (CBT) were the most clinically effective, CAM treatmentm
Ie
f Integrative Medicine 5 (2013) 296–307 297
pproaches [17]. However, because these approaches have limi-ations that mind body therapies lack (e.g. hypnotherapy dependspon the “hypnotizability” of a patient, while CBT depends uponvailability and patient preference) the latter represents a power-ul treatment for patients with FBDs. Thus, the purposes of thisrticle are to: (1) describe the scientific knowledge based on cur-ently available clinical trials of mind–body therapies for FBDs,2) examine potential benefits of using such therapies, and (3)rovide recommendations regarding their clinical application inhe treatment of FBDs.
ethodology
Complementary and alternative medicine (CAM) can be cat-gorized into five areas according to the National Center foromplementary and Alternative Medicine (NCCAM), National
nstitute of Health (NIH). These are (1) Alternative Medical Sys-ems, (2) Biological Based Therapies, (3) Mind/Body Therapies,4) Manipulative and Body Based Therapies, and (5) Energyherapies. This article will review current research regarding
he most commonly used mind–body therapies for FBDs in theS, which are yoga, hypnotherapy, cognitive behavioral therapy,
nd biofeedback [18]. Acupuncture and massage therapy werexcluded because the former is categorized as an “alternativeedical system” and the latter within “manipulative and body
ased therapies”.Inclusion criteria of the literature search were (1) English
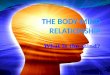
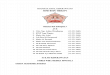
anguage only, (2) articles published between June 2002 andune 2012, (3) Medline, PsycINFO, EBSCO, Alt-Health Watch,INAHL, and PubMed databases, and (4) the search termsmind–body therapies”, “yoga”, “hypnotherapy”, “cognitiveehavioral therapy”, or “biofeedback”, in combination withfunctional bowel disorders”, “irritable bowel syndrome”, “con-tipation”, “functional abdominal pain”, or “diarrhea”. Thisesulted in retrieval of a total of 518 references. Of those, reviewrticles, protocols, case reports, duplicated publications, andtudies with less than 20 patients were excluded for review.inally, 19 original research articles met the review criteriaFig. 1). The 19 original research articles for review includedandomized and non-randomized as well as non-blinded andingle-blinded studies because the nature of mind–body inter-entions often do not allow for blinding (Table 1).
esults
oga
Yoga is a mind–body therapy with roots in ancient Indianhilosophy that combines physical postures (asanas), breathingechniques (pranayama), and relaxation or meditation in ordero balance the mind and body [19]. It has shown benefits for aariety of acute and chronic disorders [20–23] and because ofhis, is presently being used by 10% of IBS patients for symptom
anagement [18].Although clinical studies involving yoga and patients with
BS are few, there is some evidence to suggest a positive influ-nce of yoga on both pain and anxiety. For example, one study

298
O.
Grundm
ann, S.L
. Yoon
/ E
uropean Journal
of Integrative
Medicine
5 (2013)
296–307
Table 1Clinical studies involving mind–body therapies for the treatment of functional bowel disorders.
Reference Publication year Country Sample characteristicsand size (N)
Study design # of sessions (duration) Outcome
YogaTaneja et al. [24] 2004 Canada IBS-D, IBS
determined by RomeII criteria (N = 22)
Randomized,non-double blinded,non-placebocontrolled
8 sessions (2 months) Significant reductions in bowelsymptom, state anxiety, and autonomicsymptom scores comparable or greaterthan standard therapy
Kuttner et al. [25] 2006 Netherlands All IBS forms, IBSdetermined by Rome Icriteria (N = 28)
Randomized,non-double blinded,non-placebocontrolled
1 yoga session followed by 4 weeks ofhome sessions, wait-list control receivedsame protocol after 1 month wait (2months)
Significant reduction in GI symptomsand emotion-focused pain coping in bothgroups after yoga intervention,non-significant reductions in painintensity and anxiety scores
Brands et al. [26] 2011 United States All IBS forms andfunctional abdominalpain determined byRome III criteria(N = 20)
Non-randomized,non-double blinded,non-placebocontrolled
10 yoga sessions over 12 weeks in twogroups of children (ages 8–11 and12–18) with 3 month follow-up period
Results of the pilot study indicatesignificant decreases in pain intensityscores for children in both age groupscompared to baseline
HypnotherapyGonsalkorale et al. [33] 2004 United States All IBS forms, IBS
determined by Rome Icriteria (N = 78)
Non-randomized,non-double blinded,non-placebocontrolled
12 sessions (12 weeks) Significant improvements in HAD scoresand IBS symptoms compared to baseline
Palsson et al. [34] 2002 United Kingdom All IBS forms, IBSdetermined by Rome Icriteria (N = 42)
Randomized,non-double-blinded,non-placebo-controlled
7 sessions with post-evaluation (7– 28weeks)
Significant reduction in IBS symptoms inboth pain-specific and non-pain-specifichypnotherapy groups, reductions inanxiety and depression scores forpain-specific hypnotherapy
Vlieger et al. [36,44] 2007 United Kingdom Pediatric patients withfunctional abdominalpain or IBS, IBSdetermined by RomeII criteria (N = 53)
Randomized,non-double-blinded,non-placebocontrolled
6 sessions over 3 months with follow-up(12 weeks with 1 year follow-up)
Significant improvement in IBSsymptom scores, abdominal pain anddistension, and anxiety compared tostandard medical therapy, at 5 yearfollow-up pain intensity and frequencyscores remained significantly lower inboth the supportive therapy andhypnotherapy groups
Lea et al. [37] 2003 United Kingdom All IBS forms, IBSdetermined by Rome Icriteria (N = 40)
Non-randomized,non-double-blinded,non-placebocontrolled
12 sessions over 3 months with follow-up(12 weeks with 2 week follow-up)
Moderate improvement in rectalsensitivity, significant improvement inanxiety and depression symptomscompared to baseline
Gonsalkorale et al. [42] 2003 United Kingdom All IBS forms, nodocumentation of IBSdiagnosis (N = 204)
Non-randomized,non-double-blinded,non-placebocontrolled
12 sessions over 3 months (12 weekswith 6 year follow-up)
Significant improvement in IBSsymptom scores, abdominal pain anddistension, and HAD compared topre-treatment in responders
Roberts et al. [43] 2006 United Kingdom All IBS forms, nodocumentation of IBSdiagnosis (N = 81)
Randomized,non-double-blinded,placebo-controlled
5 sessions over 5 weeks with 12 monthfollow-up
Significant improvement in overallsymptom scores, pain, and diarrheascores compared to placebo after 3months, but results were not maintainedafter 12 months with no differencebetween groups

O.
Grundm
ann, S.L
. Yoon
/ E
uropean Journal
of Integrative
Medicine
5 (2013)
296–307
299Table 1 (Continued)
Reference Publication year Country Sample characteristicsand size (N)
Study design # of sessions (duration) Outcome
Lindfors et al. [47] 2012 Sweden All IBS forms, IBSdetermined by RomeII criteria in twoseparate studies(N = 90 for study 1,N = 48 for study 2)
Randomized,non-double-blinded,placebo-controlled
12 session over 3 months ofhypnotherapy in private practices orindividual therapy for the control group(study 1) or in a hospital (study 2) with await-list as control group
Significant and maintainedimprovements in overall symptom scoresin study 1 patients compared withplacebo group, smaller andnon-maintained improvements insymptom scores for patients in study 2compared to baseline and control group
Flik et al. [49] 2011 Netherlands All IBS forms, IBSdetermined by RomeIII criteria (N = 354)
Randomized,non-double-blinded,placebo-controlled
6 sessions over 12 weeks of individualhypnotherapy, group hypnotherapy, oreducational supportive therapy (placebo)
Study results expected by end of 2013.
Cognitive behavioral therapy (CBT)Tkachuk et al. [61] 2003 Canada All IBS forms, IBS
determined by Rome Icriteria (N = 28)
Randomized,non-double-blinded,non-placebo-controlled
10 CBT sessions or symptom monitoringwith telephone contact over 9 weeks with3 month follow-up
Significant improvements in cognitivescale for functional bowel disorders,assertiveness questionnaire, and shortform 36 health survey – physical healthcomponent scale
Drossman et al. [55],Weinland et al. [56]
2003, 2010 United States FBDs (IBS, functionalabdominal pain,painful constipation,and unspecified FBD),no documentation ofFBD diagnosis(N = 431)
Randomized,non-double-blinded,placebo-controlled
12 CBT, anti-depressant, or educationalsessions over 3 months (12 weeks with 1year follow-up)
Significant improvements in satisfaction,global well-being, and responder rate ofCBT group vs. education group at 1 yearfollow-up, CBT as effective asantidepressant in reducing IBSsymptoms
Kennedy et al. [58] 2006 United Kingdom All IBS forms, nodocumentation of IBSdiagnosis (N = 149)
Randomized,non-double-blinded,non-placebo-controlled
6 CBT sessions over 6 weeks in additionto mebeverine hydrochloride fortreatment of IBS symptoms inintervention group, only mebeverinetreatment in control group with 12 monthfollow-up
Significant reduction in symptom scoresand increase in quality of life measuresin patients receiving CBT compared tomebeverine alone although effects ofCBT were not lasting beyond 6 monthsduring follow-up
Mahvi-Shirazi et al. [60] 2008 Iran All IBS forms, IBSdetermined by RomeII criteria (N = 50)
Randomized,non-double-blinded,non-placebo-controlled
8 CBT sessions over 2 months Significant improvements in IBSsymptoms (Rome-II questionnaire) andpsychological symptoms (SCL-90-R)
Jones et al. [57] 2011 Australia All IBS forms, IBSdetermined by Rome Icriteria (N = 105)
Randomized,non-double-blinded,non-placebo-controlled
8 CBT or relaxation sessions over 2months (8 weeks with 1 year follow-up)
Significant improvements in mood(HAD scale) and IBS symptoms (BSSS)after CBT comparable to relaxationtherapy and standard medical care
BiofeedbackDing et al. 2011 China Functional
constipationdetermined by RomeIII criteria (N = 21)
Non-randomized,non-double-blinded,non-placebo-controlled
10 1-h biofeedback sessions, initiallyevery other day followed by 2–3 timesper week for 8 weeks, manometry andanal electrode were used to measuresphincter contractions, patients wereasked to keep sphincter constrictionswithin certain range through relaxationand constriction of the pelvic floormuscles
Significant improvements in severalpsychological questionnaires (self-ratinganxiety scale, self-rating depressionscale), several variables on the 36-itemshort-form health survey for quality oflife, and the Bristol stool scale. Nochanges in autonomic function asevaluated by high and low frequencyheart rate bands.

300 O. Grundmann, S.L. Yoon / European Journal of Integrative Medicine 5 (2013) 296–307
e sele
epdeitapitlpppyyitatsdtyfsdaawtwid
slp
aotwsdpptsode
yytsa
H
iit
Fig. 1. Flow chart illustrating th
valuated the effect of mixed Surya Nadi pranayama yogaostures and select breathing techniques in 22 patients withiarrhea-predominant IBS and found that yoga was at least asffective as loperamide in reducing both anxiety and motil-ty scores in IBS patients [24]. The subjects were split intowo groups: one group received the standard pharmacologicalnti-diarrhea treatment with loperamide while another groupracticed yoga twice a day for two months. Evaluation of anx-ety and motility scores before, 1 month, and 2 months intohe intervention showed that yoga was at least as effective asoperamide in reducing both anxiety and motility scores in IBSatients (p < 0.01 for bowel symptom scores in conventional and
< 0.001 in yoga group after 2 months compared to baseline; < 0.02 for state anxiety scores in conventional and p < 0.004 inoga group after 2 months compared to baseline). Furthermore,ogic intervention resulted in significantly better improvementn autonomic symptom score (p < 0.05 for yoga group comparedo conventional group after 2 months of intervention), which isn indicator of reduced parasympathetic tone while normalizinghe sympathetic activity to provide balance in motility. Anothertudy evaluated the effect of yoga on 25 IBS patients who wereiagnosed by Rome I criteria and aged 11–18 [25]. After an ini-ial screening, they were given an instructional and introduced tooga self-practice at home. Once they had engaged in practiceor one month, they were interviewed again using a 10-pointcale pain score, pain coping questionnaire, and the Children’sepression inventory form. The authors found that there was
significant difference in functional disability, child manifestnxiety, and emotion-focused avoidance between the yoga andaitlist group at a significance level of p < 0.1. In addition, gas-
rointestinal symptoms and anxiety-related avoidance behavior
ere significantly reduced after 1 month, further supporting thedea that yoga can benefit patients with IBS [25]. However,ue to the small sample size and the use of only descriptive
oewh
ction criteria for clinical trials.
tatistics, the study results remain questionable, especially inight of the higher p-value of 0.1 instead of the widely accepted
< 0.05 with a potential for a type II error.A similar pilot study evaluated yoga in two adolescent groups,
ged 8–11 and 12–18 years, who were diagnosed with either IBSr functional abdominal pain according to Rome III criteria inhe Netherlands [26]. After 10 Hatha yoga sessions lasting 1.5 hith suggestive and general relaxation elements, the pain inten-
ity and frequency scores for both patient groups significantlyecreased compared to baseline (p = 0.031 and p = 0.004 forain frequency in 8–11 and 12–18 year old group respectively,
= 0.015 for pain intensity in 8–11 year old group). In particular,he pain frequency score in the younger patient group remainedignificantly lowered at a 3 month follow-up (p = 0.04). Becausef the significant results, the authors plan to conduct a similarlyesigned study with a larger patient population to provide furthervidence for the benefits of yoga in treating FBDs.
Although there are only a few studies that indicate a benefit ofoga in the treatment of FBDs, the evidence to date suggests thatoga may alleviate pain and anxiety in a diverse patient popula-ion. However, the current trials are limited by their small sampleize, which indicates that further studies with larger sample sizesre necessary to support the findings.
ypnotherapy
Hypnosis or hypnotherapy, is one of the oldest practices fornduction and maintenance of a sedative or anesthetic state, ands associated with relaxation, elevated mood, reduced pain sensi-ivity as well as a lower heart and respiration rate [27]. Similar to
ther mind–body therapies, hypnosis induces a state of height-ned internal awareness of and control over bodily processesithout losing control or consciousness [28]. The effects ofypnosis are evident in certain brain regions, particularly the
rnal o
fan
tr[F[
onHfts
aIidsabptstisotcsggepDphhttswpiwprbssmsi
s1itm
hpiacwss
sgcpcab
psIwoapatptao[cscifirtcfltttfirb
O. Grundmann, S.L. Yoon / European Jou
rontolimbic attention system, which is associated with beingble to shift focus from unpleasant stimuli to pleasurable oreutral emotions [29].
Because hypnosis has primarily been used to initiate a seda-ive and anesthetic state, it has demonstrated effectiveness ineducing both acute pain during surgery as well as chronic pain30–32]. Furthermore, hypnosis has been shown to help improveBD symptoms as effectively as pharmacological treatments27,33–38].
The application of hypnosis specifically for the treatmentf IBS has been introduced and utilized as gut-directed hyp-otherapy by Peter Whorwell and colleagues at the Universityospital of South Manchester in the 1980s [39]. This approach
ocuses specifically on a framework that provides patients withhe necessary hypnotic skills to control gut function and reduceymptoms.
In fact, in one study, gut-focused hypnotherapy relieved painnd increased quality of life after 12 hypnotherapy sessions in 78BS patients who did not respond to conventional pharmacolog-cal treatments [33]. The overall extracolonic symptom scoreecreased by 70.7 points (p < 0.01), the overall IBS symptomcore decreased by 159.7 points (p < 0.001), and the over-ll quality of life score increased by 75.4 points (p < 0.001)etween pre- and post-hypnotherapy intervention. Nearly allarameters of the cognitive scale improved with the excep-ion of the self-nurturance and perfectionism scores. Anothertudy found similar results for 42 IBS patients who werereated with 12 weeks of hypnotherapy, in which significantmprovements in rectal pain, sensitivity, anxiety, depression, andomatic symptoms were observed [34,37]. This study consistedf two sub-studies that used different evaluation techniqueso test the different hypotheses. In the first sub-study, whichonsisted of 18 patients, seven 45-min individual hypnosis ses-ions were administered to two groups of 9 participants: oneroup received pain-specific verbal suggestions while the otherroup did not. Rectal muscle tone and pain threshold werevaluated in conjunction with a daily diary of GI symptoms,ain frequency and severity, and administration of the Beckepression inventory. The second sub-study consisted of 24atients that were randomized into an immediate and delayedypnosis treatment groups. The immediate group received sevenypnosis sessions with pain-specific verbal suggestions overhe course of 12 weeks after a 2 week baseline observa-ion period while the delayed waiting-list group received theame hypnotherapy treatment after 4 months. Both groupsere interviewed 4 months and 8 months after enrollment. Allatients in the first sub-study were evaluated with the phys-cal symptoms inventory and an autonomic functioning test,hich involved measurement of skin conductance, skin tem-erature, and muscle tension via electromyography (EMG). Theesults showed an immediate effect on abdominal pain (p < 0.001etween baseline and posttreatment), bloating (p = 0.002), andtool consistency (p = 0.003) with pain-specific and non-pain-
pecific hypnotherapy; however, there was no change in bowelovements per day (p = 0.733). Significant improvements inomatization (p = 0.0001 pre-treatment vs. post-treatment), anx-ety (p = 0.008), and depression (p = 0.03) were observed in the
o
st
f Integrative Medicine 5 (2013) 296–307 301
econd study. The effect of hypnotherapy lasted for at least0 months after study admission with significant (p < 0.05)mprovements in abdominal pain, bloating, and stool consis-ency. These findings indicate that hypnosis is a promising
ind–body therapy for patients of FBDs.Similarly, a review by Gholamrezaei and colleagues of 13
ypnotherapy, clinical studies showed that hypnotherapy was aromising way to alleviate symptoms of IBS, but methodologicnadequacies hampered its efficacy [40]. The authors provided
list of recommendations that might improve the quality oflinical trials which included—among other suggestions—aell-defined study population, a large sample size to allow for
mall effect sizes, and the use of validated instruments to mea-ure changes in a reliable manner.
Another review of hypnosis by Whorwell, which related thepecific type of hypnotherapy to the outcome [41], found thatut-directed or symptom-directed hypnotherapy can alleviateolonic and non-colonic ailments related to IBS and improveatient quality of life. Whorwell concluded that hypnotherapyan influence psychological and gastrointestinal responses byltering the central processing of noxious stimuli and can thuse used in the treatment of many disorders.
However, because these studies were limited by small sam-le sizes, it is important to examine studies with larger sampleizes to establish validity. In a clinical study that included 204BS patients, the long-term effects of hypnotherapy after a 12eek hypnotherapy intervention were evaluated over the coursef 6 years [42] and revealed significantly improved pain severitynd frequency, bloating, and overall quality of life, especially inatients who continued to practice self-administered hypnother-py. In addition, a 2007 Cochrane database review regardinghe use of hypnotherapy for IBS, which included a total of 147atients in four studies between 1998 and 2006, demonstratedhat, in comparison to conventional pharmacological therapylone, 5–12 hypnotherapy sessions significantly reduced theverall symptom and abdominal pain scores after 3 months38]. Although the authors of the review [38] found significanthanges in frequency of bowel movements, abdominal pain, andtool consistency, they were not able to determine an overallonfidence interval for the improvements due to heterogene-ty of the study outcome measures and evaluation tools. Thesendings are supported by a study of 81 IBS patients that wereandomized to receive 5 gut-directed hypnotherapy sessions overhe course of 5 weeks in addition to standard care or standardare alone; results indicated significantly lower symptom scoresor pain (p = 0.02), diarrhea (p = 0.046), and overall quality ofife (p = 0.008) after 3 months [43]. The study notes though,hat these differences could not be maintained in comparisono the control group after 12 months, thus indicating a limit tohe chronic effects of hypnotherapy after intervention. Thesendings suggest that the results seen in smaller studies can beeplicated on a larger scale, further establishing that hypnosis cane an effective complementary treatment for chronic sufferers
f FBDs.Because children with IBS may suffer from higher socialtigma, they could require special consideration in regardso symptom alleviation. One study investigated the use of

3 rnal o
gdIrmrp6t27aoiffdransfmic
eusd3aalsdataiAah
IIthm1wIh(toa
atTah
rte1pttsb(santdi(nii
fatetabcpllccbcrlowfi
iNpt
02 O. Grundmann, S.L. Yoon / European Jou
ut-directed hypnotherapy in 53 children ages 8–18 who wereiagnosed with either functional abdominal pain (N = 31) orBS (N = 22) according to Rome II criteria [36]. Patients wereandomized to receive either 6 hypnotherapy sessions over 3onths or conventional treatment with supportive therapy. (The
esults were not separated into an IBS and functional abdominalain group, which is a limitation of the study.) However, at 3,, and 12 months following the intervention, more children inhe hypnotherapy group showed either an improvement (26%,2%, and 11%, respectively) or were in clinical remission (59%,1%, and 85%, respectively) compared to the supportive ther-py group. Both groups also showed a significant improvementf pain intensity and frequency scores after 1 year follow-ng the intervention (p < 0.001 for hypnotherapy and p = 0.002or supportive therapy group). The authors conducted a 5-yearollow-up study with the original group of patients [36] toetermine pain intensity and frequency [44]. Both parametersemained significantly lower after 5 years in the hypnotherapynd the supportive therapy arm of the initial study, but the hyp-otherapy group presented significantly lower scores than theupportive therapy group for both pain intensity (p = 0.003) andrequency (p = 0.002). Thus, although the primary study hadostly positive outcomes, it provided few insights into specific
mprovements and was also limited by the inclusion of multipleonditions in a small sample size.
The role of gut-directed hypnotherapy for IBS has also beenvaluated in a patient population of 75 IBS patients diagnosedsing Rome II criteria with evaluation of quality of life and IBSymptom questionnaires pre- and post-intervention [45]. Gut-irected hypnotherapy was administered over the course of a
month period in 5–7 sessions. The predominant symptoms ofbdominal pain and distension decreased significantly (p < 0.05)fter hypnotherapy as did almost all health-related quality ofife measures (emotional (p < 0.05), mental health (p < 0.05),leep (p < 0.05), energy (p < 0.05), physical health (p < 0.05),iet (p < 0.001), social (p < 0.05) and physical role (p < 0.001)s well as anxiety scores (p < 0.05)). However, the limitation ofhe study was the absence of a control group and the fact thatt least some of the improvements may have been linked to thendividual attention patients received from the nurse therapist.s a result, the author advocates for an appropriately trained
nd educated GI nurse specialist to be involved in gut-directedypnotherapy for IBS patients.
Although gut-directed hypnotherapy is beneficial for manyBS patients, it appears to be of particular benefit to refractoryBS patients if they respond to the treatment. In a retrospec-ive study, Lindfors et al. evaluated 208 patients who receivedypnotherapy between 2000 and 2006 using a subjective assess-ent questionnaire for IBS symptoms [46]. Of the 208 patients,
03 were classified as responders that improved significantlyith hypnotherapy with 73% still using hypnotherapy for their
BS symptoms during the 5-year follow-up. Overall, 100% ofypnotherapy responders compared to 74% of non-responders
p < 0.001) considered gut-directed hypnotherapy a worthwhilereatment. The use of hypnotherapy may serve both the purposef complementing the traditional pharmacological approachess well as providing patients who do not get adequate relief orpTtt
f Integrative Medicine 5 (2013) 296–307
re refractory to current conventional treatment an alternativereatment for long-term relief of IBS symptoms and severity.he relief experienced with the continued use of hypnother-py appears to be sustained over years following the initialypnotherapy intervention.
Because IBS symptoms can alter with the environment,esearchers evaluated the influence of setting on hypnotherapeu-ic effectiveness. In this study, hypnotherapy sessions occurredither in the private practice of a clinical psychologist (study) or a hospital setting (study 2) [47]. For both studies, 138atients with refractory IBS were either randomly assignedo receive hypnotherapy sessions over 12 weeks or assignedo a waiting list in study 2 and receive supportive therapy intudy 1 as control treatments. At a follow-up of 3 months,oth hypnotherapy groups showed significant improvementsp < 0.05) in symptom scores for IBS (total GI symptoms, sen-ory symptoms, and bowel habits) compared to the baselinend respective control groups, but after 1 year, only the hyp-otherapy group assigned to private practice sessions was ableo maintain reduced pain (p < 0.01), bloating (p < 0.01), andiarrhea (p < 0.05), improved quality of life (emotional function-ng (p < 0.01), mental health (p < 0.05), sleep (p < 0.05), energyp < 0.01), and social role (p < 0.05)). The other 3 groups showedo significant improvement compared to baseline, which mayndicate that the hypnotherapy environment can significantlynfluence clinical outcomes.
Similarly, because symptoms of IBS appear to be linked toood ingestion, researchers investigated the effect of hypnother-py in post-prandial IBS patients refractory to conventionalherapy [48]. A total of 28 patients were assigned to receiveither 1-h hypnotherapy sessions over 12 weeks or supportiveherapy for the same time period. Colonic distension was evalu-ted at baseline and after 3 months using a barostat measurementefore and after a 1-h duodenal lipid infusion. The results indi-ated that hypnotherapy reduced symptoms, with higher balloonressure compared to supportive therapy, which significantlyowered gas (p < 0.01), discomfort (p < 0.01), and pain (p < 0.01)evels 1 h after lipid infusion. Due to these findings, the authorsoncluded that hypnotherapy affects both motor and sensoryomponents in the GI tract. This study, however, was limitedy a small sample size as well as a failure to include chole-ystokinin measurements that impact significantly gastrocolonicesponse. In addition, although this study was well-designed, itacks questionnaires that are commonly used when evaluatingverall improvement and personal perception of the patients,hich would further support the physiological findings. There-
ore, the study cannot be directly compared to other studies thatncorporate these tools.
Based on the small sample size of previous studies involv-ng IBS patients and hypnotherapy, a research group in theetherlands is currently conducting a study including 354atients with IBS diagnosis [49]. Patients are randomly assignedo either individual or group hypnotherapy sessions and com-
ared to educational sessions that served as the placebo group.he aim of the study is to provide further support for theherapeutic application of hypnotherapy in reducing IBS symp-oms as well as become one of the few studies that compares

rnal o
ir2
ttgaserqiw
C
tblptacibt
ct4asppa1rsdpCpcbwCwmswehasf
twadr[aalcdtstI
iaciwtsqioaamtcIc
miwwto[ep(s(pestm
s
O. Grundmann, S.L. Yoon / European Jou
ndividual to group settings in a hypnotherapy intervention;esults of the study are expected to be published at the end of013.
Overall, hypnotherapy in the treatment of FBDs has showno be effective in a number of small clinical studies comparedo either wait-list or conventional pharmacological treatmentroups. It appears to be important to maintain regular hypnother-py as an intervention to retain the effectiveness in reducing theymptoms of FBDs. However, inadequate study designs and het-rogeneity in regards to the outcome measures warrant furtheresearch in order to solidify the current findings. In addition, fre-uency and durations of hypnotherapy interventions should benvestigated further for generalizability and maximum benefitsith minimum frequency.
ognitive behavioral therapy
Patients with chronic conditions often have a negative atti-ude that limits their ability to heal. However, this attitude cane altered with cognitive behavioral therapy (CBT), which chal-enges negative thoughts and causes patients to focus on a moreositive outlook. A review of meta-analyses has shown CBTo be effective in a number of chronic conditions [50] suchs depressive disorders [51], obesity [52], insomnia [53], andhronic pain [54], but improvement with these conditions is notmmediate; indeed, CBT requires at least 8–10 weekly sessionsefore improvement of symptoms is observed because it takesime for patients to adjust their perspective.
In addition to these chronic conditions, present researchurrently demonstrates the effectiveness of CBT in easing symp-oms of FBDs. For example, in one large study that examined31 female patients suffering from FBDs, CBT was at leasts effective as the antidepressant, desipramine in reducingymptoms [55]. Participants who were diagnosed with IBS,ainful functional constipation, chronic functional abdominalain, or unspecified FBD according to Rome I criteria werellocated to one of four treatment arms: 135 patients received2 CBT sessions over the course of 3 months, 66 patientseceived 12 modified-attentional control sessions during theame time period, 135 patients were randomized to receiveesipramine (final dose 150 mg/day), and 66 patients receivedlacebo for 3 months. The composite score when comparingBT with modified-attentional control and desipramine withlacebo resulted in a significant improvement for CBT overontrol (p < 0.0001) while desipramine was not significantlyetter than placebo (p = 0.16). However, patient satisfactionas significantly higher for the desipramine (p = 0.011) andBT (p = 0.0004) groups. In addition, the CBT group presentedith significantly (p = 0.04) improved global well-being after 3onths compared to the control. The responder rate was also
ignificantly higher in the CBT group vs. control (p < 0.0001)hile desipramine responder rate was not significantly differ-
nt from placebo. Interestingly, neither CBT nor desipramine
ad a significant effect on IBS quality of life and the McGillverage daily pain scores. A further analysis of the outcomeuggests that satisfaction with treatment depends on cognitiveactors such as confidence in treatment, perceived control overscIa
f Integrative Medicine 5 (2013) 296–307 303
he illness, and reduction in negative cognition of the symptoms,hich may be better obtained with CBT than medication ther-
py alone [56]. In another, clinical study, 105 IBS patients wereiagnosed using Rome I criteria, and used either CBT (N = 34),elaxation therapy (N = 36), or standard medical care (N = 35)57]. Results showed that CBT was able to affect mood (mainlynxiety and depression) and change bowel symptoms as muchs relaxation and standard clinical care. However, this study wasimited because the CBT group received both standard clinicalare and relaxation therapy; thus, researchers were unable toistinguish which variable determined the outcome. Althoughhese findings are supportive of the use of CBT to ease FBDymptoms, more research is needed that investigates the poten-ial mediator role that CBT plays between mood changes andBS symptoms.
Another study investigated the complementary use of CBTn patients with IBS receiving mebeverine hydrochloride as anntispasmodic treatment [58]. Only patients that were not wellontrolled after 4 weeks of mebeverine treatment were random-zed to receive either complementary CBT (N = 72) or continueith only mebeverine (N = 77). Patients receiving CBT in addi-
ion to mebeverine showed significant improvements in overallymptom severity scores (95% CI −109 to −32) and increaseduality of life (95% CI −35.4 to −7.9) at 3 months after thentervention. However, the benefits of CBT appeared to wanever time and did not reduce the overall social costs, following
one-year follow-up period. This may point to the necessity of long-term supportive treatment with CBT in addition to com-only used medication for IBS. The secondary analysis [58] of
he original study [57] indicated that behavioral and cognitiveomponents were important in the treatment of IBS and thatBS-related cognition and behaviors were actually mediators ofhange for IBS patients who received CBT [59].
When CBT as a complementary therapy is compared toedication treatment alone, it is evident that CBT not only
mproves IBS-related symptoms, but also mental health andell-being. For example, in one study, 50 IBS patients whoere diagnosed according to Rome II criteria were assigned
o receive medication treatment alone or 8 CBT sessionsver the course of 2 months as a complementary therapy60]. Results indicated significant reduction of all param-ters in the CBT group following the intervention. Thesearameters included Rome-II score (p = 0.001), somatizationp = 0.0001), obsessive-compulsiveness (p = 0.0001), interper-onal sensitivity (p = 0.0001), depression (p = 0.002), anxietyp = 0.0001), hostility (p = 0.0001), phobic anxiety (p = 0.0001),aranoid ideation (p = 0.003), psychoticism (p = 0.001), and gen-ral symptom index (p = 0.0001) that were evaluated usingtandardized questionnaires. Although the results were posi-ive, this study was limited because it lacked a placebo for the
edication group alone.Researchers primarily investigate CBT using individual ses-
ions, but recent studies have examined CBT in a group therapy
etting. A study conducted in Canada investigated the use ofognitive behavioral group therapy in 28 patients diagnosed withBS according to Rome I criteria over the course of 9 weeks with3 month follow-up [61]. Patients were randomized to receive

3 rnal o
ewot((caicNp
mConiCdmspcce
iitst
B
oopieiTccrism
gapdtgO
opaotastws
iwsisppbsbfrans
iabmicsrsf
bhtat
C
hMeutn
04 O. Grundmann, S.L. Yoon / European Jou
ither a CBT intervention as a group or symptom monitoringith weekly telephone contact. Significant improvements werebserved for the CBT group therapy arm over the course ofhe study for the cognitive scale for functional bowel disordersp = 0.002 vs. control group), on the assertiveness questionnairep = 0.035), and the short form 36 health survey physical healthomponent scale (p = 0.036). This study had a small sample sizend the control group was offered CBT after completion of thenitial 9 week treatment, which may have influenced the per-eption of initial treatment effects at the 3 month follow-up.onetheless, the results indicate that group-directed CBT mayrovide similar relief and benefits in treating IBS.
Taylor et al. incorporated a range of complementaryind–body therapies while investigating the benefits of groupBT, educational, and hypnotherapy sessions in 158 participantsver the course of 4 months [62]. Participants had been diag-osed with IBS according to Rome II criteria and were dividednto small groups of 4–7 patients who received a combination ofBT, IBS education, and gut-directed hypnotherapy. The pooledata for all 23 groups showed marked and significant improve-ents for psychological and general well-being, gastrointestinal
ymptom rating, and prevention of enjoyment of life scales (all < 0.001 post- vs. pre-intervention). Although this study suc-essfully addressed a holistic approach to IBS treatment, theonclusions that can be drawn are limited because the effects ofach therapy are difficult to distinguish.
The current research on the effectiveness of CBT in FBDss promising, but due to small sample sizes and heterogeneityn study protocols, including dosages and duration of interven-ion, further research with larger sample sizes and standardizedtudy protocols are warranted to establish CBT as an effectivereatment for patients with FBDs.
iofeedback
Biofeedback training, which allows patients to gain controlver certain physiological functions, also assists them in rec-gnizing the often subconscious dysfunction through a simplehysiological measurement (e.g. temperature, blood pressure,ntestinal distension) and visualization. Biofeedback can thenmploy both motor skill and sensory discrimination training tomprove the patient’s awareness and allow for adaptations [63].he use of biofeedback has long been employed in a number ofonditions including substance abuse, hypertension, headaches,hronic pain, constipation, and anxiety disorders [64]. Withespect to general, functional gastrointestinal disorders, train-ng specific muscle groups and recognition of symptoms canubstantially aid patients, but the voluntary control of smoothuscles and secretory responses remains very limited [63].Biofeedback has been evaluated in a number of functional
astrointestinal disorders such as fecal incontinence, functionalnorectal pain, irritable bowel syndrome, and functional dys-epsia. One study, which included 19 patients with functional
isorders, provided participants with an 8-week treatment pro-ocol of biofeedback training and compared them to a controlroup of 40 patients who received conventional therapy [65].f the 59 patients, 24 had been diagnosed with IBS while thetslo
f Integrative Medicine 5 (2013) 296–307
thers had been diagnosed with fibromyalgia, functional cardiacain, myofacial pain, or panic and anxiety disorders with som-tization. The study mainly focused on the feasibility and costf the biofeedback treatment rather than evaluation of symp-om reductions, which were noted as significant (p < 0.05) forll conditions in the 11 symptom questionnaire. Results of thistudy, however, did not indicate any specific variables and fac-ors that would benefit IBS patients. Also, the overall evaluationas brief and not well explained, thus limiting replication of the
tudy as well as applicability to other FBDs.Another study evaluated the effect of biofeedback train-
ng in 21 patients with functional constipation [66]. Patientsere evaluated before treatment and again after 10 biofeedback
essions as well as home training. Patients reported signif-cant improvements in several clinical parameters, such aspontaneous frequency of bowel movement (p < 0.01 post- vs.re-intervention), straining effort (p < 0.01), sensation of incom-lete evacuation (p < 0.01), stool consistency (p < 0.01), andloating (p < 0.01). In addition, both anxiety and depressioncores also improved significantly (p < 0.01) following biofeed-ack intervention. Changes in quality of life showed significanceor some factors but not others, especially physical and socialole functioning, and mental health. The authors did not findn indication for an influence of biofeedback on autonomouservous system function, which may be attributed to the smallample size in the study.
Biofeedback has also been evaluated for symptom reliefn patients with IBS with limited results. Small studies using
variety of physiological measures including bowel sounds,alloon probes, or general electromyogram and temperatureeasures as indicators for stress responses had varied, unpromis-
ng results. There are some indications that certain generalognitive approaches supported by biofeedback may improveymptoms of bloating and GI distress in IBS patients, but moreesearch is needed to substantiate this report. Table 1 includes aummary of the clinical studies involving mind–body therapiesor the treatment of functional bowel disorders.
The currently available research for biofeedback is limitedy small sample sizes, mostly uncontrolled study protocols, andeterogeneity in the use of various biofeedback approaches. Fur-her research with rigorous trial designs are needed to provide
higher level of evidence for the benefits of biofeedback in thereatment of FBDs.
onclusions
Functional bowel disorders remain a challenge for both theealthcare providers and patients in diagnosis and treatment.any pharmacological approaches are unspecific to the dis-
ase and often result in suboptimal outcomes that leave patientsnsatisfied with treatment. The use of mind–body therapies forhe alleviation of symptoms has been evolving with a growingumber of trials establishing a body of evidence of their effec-
iveness. However, many studies remain challenged by smallample sizes, incomplete explanation of the study protocol, orack of rigor of the study designs that do not utilize control groupsr include baseline characteristics. At present, the strongest
rnal o
smaoastpmmsptcpivv
dhwbotcaIbc
irmtnta[aapii
iBhaaOChhp
t
ttcmr
astdapbioos
F
s
C
A
w
R
O. Grundmann, S.L. Yoon / European Jou
cientific support exists for the use of hypnotherapy in the treat-ent of IBS and potentially other FBDs associated with pain
nd gastrointestinal discomfort. Although research findings forther mind–body therapies are limited and not conclusive, theselternative treatment approaches are not associated with anyignificant side effects, unlike many available pharmacologicalreatments. Thus, whenever a patient has an FBD and standardharmacological care alone proves to be unsatisfactory thenind–body therapies should be considered as a viable comple-ent to standard pharmacological therapies. When comparing
tudies using hypnotherapy, CBT, and brief psychodynamicsychotherapy, Blanchard reached the conclusion that thesereatments are effective in reducing IBS symptoms without indi-ating superiority for one treatment over another [67]. He alsooints out that a lack of uniform success in reasonable sized trialsndicates that further research on a larger scale and comparingarious mind–body treatment options is necessary to establishalidity.
In line with the rise in popularity of CAM, the United King-om National Institute for Health and Clinical Excellence (NHS)as released guidelines on the diagnosis and treatment of IBS inhich cognitive behavioral therapy, hypnotherapy, and biofeed-ack are addressed [68]. While the NHS guidelines suggest anverall improvement of symptoms and symptom management,he guidelines highlight the need for larger and well-designedlinical studies. One of the findings was that cognitive behavioralnd hypnotherapy were generally more effective in refractoryBS patients. However, the NHS guidelines are not clear aboutiofeedback and relaxation techniques, largely due to insuffi-ient research data regarding their effectiveness.
Of importance to the use of mind–body therapies to the med-cal community is their cost-to-benefit or cost-to-effectivenessatio which may help to establish such complementary treat-ent approaches further. In this area, even less data is available
o date. Van Tilburg and colleagues evaluated the cost effective-ess of mind–body therapies in the treatment of FBDs and foundhat there is a significant cost-benefit to using mind–body ther-pies and other CAM as complements to conventional therapy18]. The authors also concluded that most patients are gener-lly satisfied with conventional care, and are only seeking outdditional treatment options. Thus, future studies should com-are the cost-benefit ratio and effectiveness of CAM therapiesn the treatment of FBDs, thus allowing patients to make a morenformed decision.
Another factor that may limit the use of mind–body therapiesn the treatment of FBDs is access to well-qualified therapists.oth funding limitations (e.g. CAM therapy not covered byealth insurance, unaffordable for low-income households) and
lack of regulation and adequate training of therapists may limitccess and use of mind–body therapies in many populations.verall though, there has been a steady increase in the use ofAM therapies especially among rural populations that oftenave restricted access to standard treatment providers or do not
ave healthcare coverage to provide for expensive medicine andhysician costs [69].Overall, although it is inconclusive to determine the effec-iveness and usefulness of using mind–body therapies for FBDs,
f Integrative Medicine 5 (2013) 296–307 305
he majority of published studies indicate positive outcomes ofhese therapies [14]. Patients who have not responded well toonventional therapies are best suited to benefit from the use ofind–body therapies, but CAM treatment can provide additional
elief to patients treated with conventional medicines.Thus, recommendations for future research related to this
rea include, but are not limited to: (1) study with larger sampleizes and rigorous trial design, (2) examining the mechanisms ofhese interventions to alleviate symptoms, (3) investigating theosages and durations of the intervention for short-term effectsnd retaining long-term effects, and (4) standardizing the studyrotocols based on a type of mind–body therapy, which woulde beneficial for replication of a study and generalizing the find-ngs. Finally, a combination of certain mind–body therapies withther types of complementary therapies may be beneficial as partf an integrative and holistic approach to manage the diverseymptoms of FBDs.
inancial support
The authors did not receive any financial support for thistudy.
onflict of interest disclosure
The authors declare that no conflicts of interest exist.
cknowledgement
We would like to thank Debra McDonald for her editorialork in completing this manuscript.
eferences
[1] Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, SpillerRC. Functional bowel disorders. Gastroenterology 2006;130(5):1480–91.
[2] Gunnarsson J, Simren M. Efficient diagnosis of suspected functionalbowel disorders. Nature Clinical Practice: Gastroenterology & Hepatology2008;5(9):498–507, http://dx.doi.org/10.1038/ncpgasthep1203.
[3] Drossman DA. The functional gastrointestinal disorders andthe Rome III process. Gastroenterology 2006;130(5):1377–90,http://dx.doi.org/10.1053/j.gastro.2006.03.008.
[4] Wilder-Smith CH. The balancing act: endogenous modulation ofpain in functional gastrointestinal disorders. Gut 2011;60(11):1589–99,http://dx.doi.org/10.1136/gutjnl-2011-300253.
[5] Grundmann O, Yoon SL, Moshiree B. Current developments for the diag-nosis and treatment of irritable bowel syndrome. Current PharmaceuticalDesign 2010;16(33):3638–45.
[6] Ohman L, Simren M. Pathogenesis of IBS: role of inflammation, immu-nity and neuroimmune interactions. Nature Reviews Gastroenterology &Hepatology 2010;7(3):163–73, http://dx.doi.org/10.1038/nrgastro.2010.4.
[7] Rodriguez-Fandino O, Hernandez-Ruiz J, Schmulson M. Fromcytokines to toll-like receptors and beyond – current knowledgeand future research needs in irritable bowel syndrome. Jour-nal of Neurogastroenterology and Motility 2010;16(4):363–73,http://dx.doi.org/10.5056/jnm.2010.16.4.363.
[8] Tanaka Y, Kanazawa M, Fukudo S, Drossman DA. Biopsychosocial model
of irritable bowel syndrome. Journal of Neurogastroenterology and Motility2011;17(2):131–9, http://dx.doi.org/10.5056/jnm.2011.17.2.131.[9] Grundmann O, Yoon SL. Irritable bowel syndrome: epidemiology,diagnosis and treatment: an update for health-care practitioners.

3 rnal o
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
06 O. Grundmann, S.L. Yoon / European Jou
Journal of Gastroenterology and Hepatology 2010;25(4):691–9,http://dx.doi.org/10.1111/j.1440-1746.2009.06120.x.
10] Rivkin A. Tegaserod maleate in the treatment of irritable bowel syndrome:a clinical review. Clinical Therapeutics 2003;25(7):1952–74.
11] Medicine NCfCaA. In: Health NIo, editor. What is complementary andalternative medicine? 2011.
12] Mehling WE, Wrubel J, Daubenmier JJ, Price CJ, Kerr CE, Silow T, et al.Body awareness: a phenomenological inquiry into the common groundof mind–body therapies. Philosophy, Ethics, and Humanities in Medicine2011;6(6), http://dx.doi.org/10.1186/1747-5341-6-6, 1747-5341-6-6 [pii].
13] Eriksson EM, Moller IE, Soderberg RH, Eriksson HT, Kurlberg GK.Body awareness therapy: a new strategy for relief of symptoms inirritable bowel syndrome patients. World Journal of Gastroenterology:WJG 2007;13(23):3206–14.
14] Drossman D, Morris CB, Hu Y, Toner BB, Diamant N, WhiteheadWE, et al. Characterization of health related quality of life (HRQOL)for patients with functional bowel disorder (FBD) and its response totreatment. American Journal of Gastroenterology 2007;102(7):1442–53,http://dx.doi.org/10.1111/j.1572-0241.2007.01283.x.
15] Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicineuse among adults and children: United States, 2007. National Health Statis-tics Reports 2008;(12):1–23.
16] Harris LR, Roberts L. Treatment for irritable bowel syndrome: patients’attitudes and acceptability. BMC Complementary and Alternative Medicine2008;8(65).
17] Shen YH, Nahas R. Complementary and alternative medicine fortreatment of irritable bowel syndrome. Canadian Family Physician2009;55(2):143–8.
18] van Tilburg MA, Palsson OS, Levy RL, Feld AD, Turner MJ, Dross-man DA, et al. Complementary and alternative medicine use and costin functional bowel disorders: a six month prospective study in alarge HMO. BMC Complementary and Alternative Medicine 2008;8(46),http://dx.doi.org/10.1186/1472-6882-8-46, 1472-6882-8-46 [pii].
19] Field T. Yoga clinical research review. Complementary Therapies in Clini-cal Practice 2011;17(1):1–8, http://dx.doi.org/10.1016/j.ctcp.2010.09.007.
20] Uebelacker LA, Tremont G, Epstein-Lubow G, Gaudiano BA, Gillette T,Kalibatseva Z, et al. Open trial of Vinyasa yoga for persistently depressedindividuals: evidence of feasibility and acceptability. Behavior Modifica-tion 2010;34(3):247–64, http://dx.doi.org/10.1177/0145445510368845.
21] John PJ, Sharma N, Sharma CM, Kankane A. Effectivenessof yoga therapy in the treatment of migraine without aura:a randomized controlled trial. Headache 2007;47(5):654–61,http://dx.doi.org/10.1111/j.1526-4610.2007.00789.x.
22] Cade WT, Reeds DN, Mondy KE, Overton ET, Grassino J, Tucker S, et al.Yoga lifestyle intervention reduces blood pressure in HIV-infected adultswith cardiovascular disease risk factors. HIV Medicine 2010;11(6):379–88,http://dx.doi.org/10.1111/j.1468-1293.2009.00801.x.
23] Saper RB, Sherman KJ, Cullum-Dugan D, Davis RB, Phillips RS, Culpep-per L. Yoga for chronic low back pain in a predominantly minoritypopulation: a pilot randomized controlled trial. Alternative Therapies inHealth and Medicine 2009;15(6):18–27.
24] Taneja I, Deepak KK, Poojary G, Acharya IN, Pandey RM, SharmaMP. Yogic versus conventional treatment in diarrhea-predominant irritablebowel syndrome: a randomized control study. Applied Psychophysiologyand Biofeedback 2004;29(1):19–33.
25] Kuttner L, Chambers CT, Hardial J, Israel DM, Jacobson K, Evans K. Arandomized trial of yoga for adolescents with irritable bowel syndrome.Pain Research and Management 2006;11(4):217–23.
26] Brands MM, Purperhart H, Deckers-Kocken JM. A pilot study of yogatreatment in children with functional abdominal pain and irritable bowelsyndrome. Complementary Therapies in Medicine 2011;19(3):109–14,http://dx.doi.org/10.1016/j.ctim.2011.05.004.
27] Cuellar NG. Hypnosis for pain management in theolder adult. Pain Management Nursing 2005;6(3):105–11,
http://dx.doi.org/10.1016/j.pmn.2005.05.004. S1524-9042(05)00034-2[pii].28] Hrezo RJ. Hypnosis: an alternative in pain management for nurse practi-tioners. Nurse Practitioner Forum 1998;9(4):217–26.
[
f Integrative Medicine 5 (2013) 296–307
29] Rainville P, Hofbauer RK, Paus T, Duncan GH, Bushnell MC, Price DD.Cerebral mechanisms of hypnotic induction and suggestion. Journal ofCognitive Neuroscience 1999;11(1):110–25.
30] Abrahamsen R, Baad-Hansen L, Zachariae R, Svensson P. Effect ofhypnosis on pain and blink reflexes in patients with painful temporo-mandibular disorders. The Clinical Journal of Pain 2011;27(4):344–51,http://dx.doi.org/10.1097/AJP.0b013e3181ffbfcb.
31] Jensen MP, Ehde DM, Gertz KJ, Stoelb BL, Dillworth TM, Hirsh AT,et al. Effects of self-hypnosis training and cognitive restructuring on dailypain intensity and catastrophizing in individuals with multiple sclerosis andchronic pain. International Journal of Clinical and Experimental Hypnosis2011;59(1):45–63, http://dx.doi.org/10.1080/00207144.2011.522892.
32] Mackey EF. Effects of hypnosis as an adjunct to intravenous sedationfor third molar extraction: a randomized, blind, controlled study. Interna-tional Journal of Clinical and Experimental Hypnosis 2010;58(1):21–38,http://dx.doi.org/10.1080/00207140903310782.
33] Gonsalkorale WM, Toner BB, Whorwell PJ. Cognitive changein patients undergoing hypnotherapy for irritable bowel syn-drome. Journal of Psychosomatic Research 2004;56(3):271–8,http://dx.doi.org/10.1016/s0022-3999(03)00076-x.
34] Palsson OS, Turner MJ, Johnson DA, Burnett CK, Whitehead WE. Hyp-nosis treatment for severe irritable bowel syndrome: investigation ofmechanism and effects on symptoms. Digestive Diseases and Sciences2002;47(11):2605–14.
35] Whorwell PJ. Effective management of irritable bowelsyndrome—the Manchester Model. International Journalof Clinical and Experimental Hypnosis 2006;54(1):21–6,http://dx.doi.org/10.1080/00207140500323006.
36] Vlieger AM, Menko-Frankenhuis C, Wolfkamp SC, Tromp E, Ben-ninga MA. Hypnotherapy for children with functional abdominal pain orirritable bowel syndrome: a randomized controlled trial. Gastroenterology2007;133(5):1430–6, http://dx.doi.org/10.1053/j.gastro.2007.08.072.
37] Lea R, Houghton LA, Calvert EL, Larder S, Gonsalkorale WM, WhelanV, et al. Gut-focused hypnotherapy normalizes disordered rectal sensitivityin patients with irritable bowel syndrome. Alimentary Pharmacology andTherapeutics 2003;17(5):635–42.
38] Webb AN, Kukuruzovic RH, Catto-Smith AG, Sawyer SM. Hyp-notherapy for treatment of irritable bowel syndrome. CochraneDatabase of Systematic Reviews (Online) 2007;(4):CD005110,http://dx.doi.org/10.1002/14651858.CD005110.pub2.
39] Gonsalkorale WM. Gut-directed hypnotherapy: the Manchesterapproach for treatment of irritable bowel syndrome. InternationalJournal of Clinical and Experimental Hypnosis 2006;54(1):27–50,http://dx.doi.org/10.1080/00207140500323030.
40] Gholamrezaei A, Ardestani SK, Emami MH. Where does hypnotherapystand in the management of irritable bowel syndrome? A systematic review.Journal of Alternative and Complementary Medicine (New York, NY)2006;12(6):517–27, http://dx.doi.org/10.1089/acm.2006.12.517.
41] Whorwell PJ. Hypnotherapy for irritable bowel syndrome: the responseof colonic and noncolonic symptoms. Journal of Psychosomatic Research2008;64(6):621–3, http://dx.doi.org/10.1016/j.jpsychores.2008.02.022.
42] Gonsalkorale WM, Miller V, Afzal A, Whorwell PJ. Long term benefits ofhypnotherapy for irritable bowel syndrome. Gut 2003;52(11):1623–9.
43] Roberts L, Wilson S, Singh S, Roalfe A, Greenfield S. Gut-directedhypnotherapy for irritable bowel syndrome: piloting a primary care-based randomised controlled trial. The British Journal of GeneralPractice: The Journal of the Royal College of General Practitioners2006;56(523):115–21.
44] Vlieger AM, Rutten JM, Govers AM, Frankenhuis C, Benninga MA.Long-term follow-up of gut-directed hypnotherapy vs. standard carein children with functional abdominal pain or irritable bowel syn-drome. American Journal of Gastroenterology 2012;107(4):627–31,http://dx.doi.org/10.1038/ajg.2011.487.
45] Smith GD. Effect of nurse-led gut-directed hypnotherapy upon health-
related quality of life in patients with irritable bowel syndrome.Gastrointestinal Nursing 2005;15:678–84.46] Lindfors P, Unge P, Nyhlin H, Ljotsson B, Bjornsson ES, AbrahamssonH, et al. Long-term effects of hypnotherapy in patients with refractory

rnal o
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
O. Grundmann, S.L. Yoon / European Jou
irritable bowel syndrome. Scandinavian Journal of Gastroenterology2012;47(4):414–20, http://dx.doi.org/10.3109/00365521.2012.658858.
47] Lindfors P, Unge P, Arvidsson P, Nyhlin H, Bjornsson E, Abra-hamsson H, et al. Effects of gut-directed hypnotherapy on IBSin different clinical settings-results from two randomized, controlledtrials. American Journal of Gastroenterology 2012;107(2):276–85,http://dx.doi.org/10.1038/ajg.2011.340.
48] Simren M, Ringstrom G, Bjornsson ES, Abrahamsson H. Treatment withhypnotherapy reduces the sensory and motor component of the gastro-colonic response in irritable bowel syndrome. Psychosomatic Medicine2004;66(2):233–8.
49] Flik CE, van Rood YR, Laan W, Smout AJ, Weusten BL, Whor-well PJ, et al. A randomised controlled trial on hypnotherapyfor irritable bowel syndrome: design and methodological chal-lenges (the IMAGINE study). BMC Gastroenterology 2011;11(137),http://dx.doi.org/10.1186/1471-230x-11-137.
50] Butler AC, Chapman JE, Forman EM, Beck AT. The empir-ical status of cognitive-behavioral therapy: a review ofmeta-analyses. Clinical Psychology Review 2006;26(1):17–31,http://dx.doi.org/10.1016/j.cpr.2005.07.003.
51] Thase ME, Dube S, Bowler K, Howland RH, Myers JE, Fried-man E, et al. Hypothalamic-pituitary-adrenocortical activity andresponse to cognitive behavior therapy in unmedicated, hospitalizeddepressed patients. The American Journal of Psychiatry 1996;153(7):886–91.
52] Tsiros MD, Sinn N, Brennan L, Coates AM, Walkley JW, Petkov J, et al.Cognitive behavioral therapy improves diet and body composition in over-weight and obese adolescents. American Journal of Clinical Nutrition2008;87(5):1134–40.
53] Vitiello MV, Rybarczyk B, Von Korff M, Stepanski EJ. Cognitive behav-ioral therapy for insomnia improves sleep and decreases pain in olderadults with co-morbid insomnia and osteoarthritis. Journal of Clinical SleepMedicine: JCSM: Official Publication of the American Academy of SleepMedicine 2009;5(4):355–62.
54] Turner JA, Holtzman S, Mancl L. Mediators, moderators, and predictors oftherapeutic change in cognitive-behavioral therapy for chronic pain. Pain2007;127(3):276–86, http://dx.doi.org/10.1016/j.pain.2006.09.005.
55] Drossman DA, Toner BB, Whitehead WE, Diamant NE, Dalton CB, Dun-can S, et al. Cognitive-behavioral therapy versus education and desipramineversus placebo for moderate to severe functional bowel disorders. Gastroen-terology 2003;125(1):19–31.
56] Weinland SR, Morris CB, Dalton C, Hu Y, Whitehead WE, Toner BB, et al.Cognitive factors affect treatment response to medical and psychologicaltreatments in functional bowel disorders. American Journal of Gastroen-terology 2010;105(6):1397–406, http://dx.doi.org/10.1038/ajg.2009.748.
[
f Integrative Medicine 5 (2013) 296–307 307
57] Jones M, Koloski N, Boyce P, Talley NJ. Pathways connectingcognitive behavioral therapy and change in bowel symptomsof IBS. Journal of Psychosomatic Research 2011;70(3):278–85,http://dx.doi.org/10.1016/j.jpsychores.2010.10.004. S0022-3999(10)00389-2 [pii].
58] Kennedy TM, Chalder T, McCrone P, Darnley S, Knapp M, Jones RH,et al. Cognitive behavioural therapy in addition to antispasmodic therapyfor irritable bowel syndrome in primary care: randomised controlled trial.Health Technology Assessment 2006;10(19), iii–iv, ix–x, 1–67.
59] Reme SE, Stahl D, Kennedy T, Jones R, Darnley S, Chalder T.Mediators of change in cognitive behaviour therapy and mebever-ine for irritable bowel syndrome. Psychological Medicine 2011:1–11,http://dx.doi.org/10.1017/s0033291711000328.
60] Mahvi-Shirazi M, Fathi-Ashtiani A, Rasoolzade-Tabatabaei S-K, AminiM. Irritable bowel syndrome treatment: cognitive behavioral therapy versusmedical treatment. Archives of Medical Science 2008;8(1):123–9.
61] Tkachuk GA, Graff LA, Martin GL, Bernstein CN. Randomized controlledtrial of cognitive-behavioral group therapy for irritable bowel syndromein a medical setting. Journal of Clinical Psychology in Medical Settings2003;10(1):57–69.
62] Taylor EE, Read NW, Hills HM. Combined group cognitive-behaviourtherapy and hypnotherapy in the management of the irritable bowel syn-drome: the feasibility of clinical provision. Behavioural and CognitivePsychotherapy 2004;32:99–106.
63] Chiarioni G, Whitehead WE. The role of biofeedback in the treatmentof gastrointestinal disorders. Nature Clinical Practice: Gastroenterology &Hepatology 2008;5(7):371–82, http://dx.doi.org/10.1038/ncpgasthep1150.
64] Yucha CB, Montgomery D. Evidence-based practice in biofeedback andneurofeedback. Faculty Publications; 2008.
65] Ryan M, Gevirtz R. Biofeedback-based psychophysiological treatment in aprimary care setting: an initial feasibility study. Applied Psychophysiologyand Biofeedback 2004;29(2):79–93.
66] Ding M, Lin Z, Lin L, Zhang H, Wang M. The effect of biofeedbacktraining on patients with functional constipation. Gastroenterology Nursing2012;35(2):85–92.
67] Blanchard EB. A critical review of cognitive, behavioral, and cognitive-behavioral therapies for irritable bowel syndrome. Journal of CognitivePsychotherapy 2005;19(2):101–23.
68] Excellence NIfHaC, editor. Irritable bowel syndrome in adults: diagnosisand management of irritable bowel syndrome in primary care. NationalInstitute for Health and Clinical Excellence; 2008.
69] Su D, Li L. Trends in the use of complementary and alter-native medicine in the United States: 2002–2007. Journal ofHealth Care for the Poor and Underserved 2011;22(1):296–310,http://dx.doi.org/10.1353/hpu.2011.0002.