Embed Size (px)
Citation preview
MIMICAL ECTROPION OR ENTROPION OF EYELIDS. MONO- AND BILATERAIA.
By S. Holth') , Oslo. (Illustrations selected from kino-films by Dr. E'mil Enroth,
Helsingfors).
In the last December number of this journal (Vol. 14 - 1936, p. 340). I published a case of ,Mirnical ectropion of up- per lids<< - a remembrance from my school days; I have never seen anything similar since then.
One of the editors, Dr. Emil Enroth in Helsingfors, has two friends presenting such an unusual innervation of the facial muscles, which is not a disease. Therefore it never oc- casions medical consultation and is hardly reported in periodi- cals; to my knowledge this sharp facial'innervation is not mentioned in the physiological handbooks.
The two friends are brothers and the eldest of a family of five who can all easily move their ears; but only the eldest two can produce rnirnical changes in the position of their eye- lids. Nothing similar is known in the parents, though, per- haps, very slightly in the mother's family.
Dr. Enroth had the excellent idea to have films taken of his two friends' performances with their eyelids; he sent me the two films and invited me - with the consent of the two brothers - to project the films before colleagues and to publish them together with the anamnestic data.
Doctor T. W., aged 47 years now, as a 12 or 13 year old boy used with his fingers to strain the skin of his temples and after large gaping, to turn his upper eyelids outward. By as-
*) Received 26th July, 1937.
371
siduous training he succeeded in performing this trick without finger-straining of the temporal skin; the unilateral eversion was most difficult to perform but finally he also succeeded i n this. He has kept in >>good forma by psycho-therapeutic use of the tricks in his practice: as otiatric surgeon he trun- quiZZizes his little patients with his eyelid performances, and often continues for a while, to the children’s delight.
Doctor T. W. himself has three children, but Done of them have learnt those tricks from their father.
Mr. S. W., aged 46 years now, is an engineer; as a 12 to 13 year old boy he observed - under futile attempts at imitating his elder brother - that his lower eyelids mould be rolled in- ward; he could never learn eversion of the upper lids.
Mr. S. 3W. like his brother has richly developed facial muscles; he has two children 12 and 13 years old, but they have in vain tried, to acquire the >art< of their father or uncle.
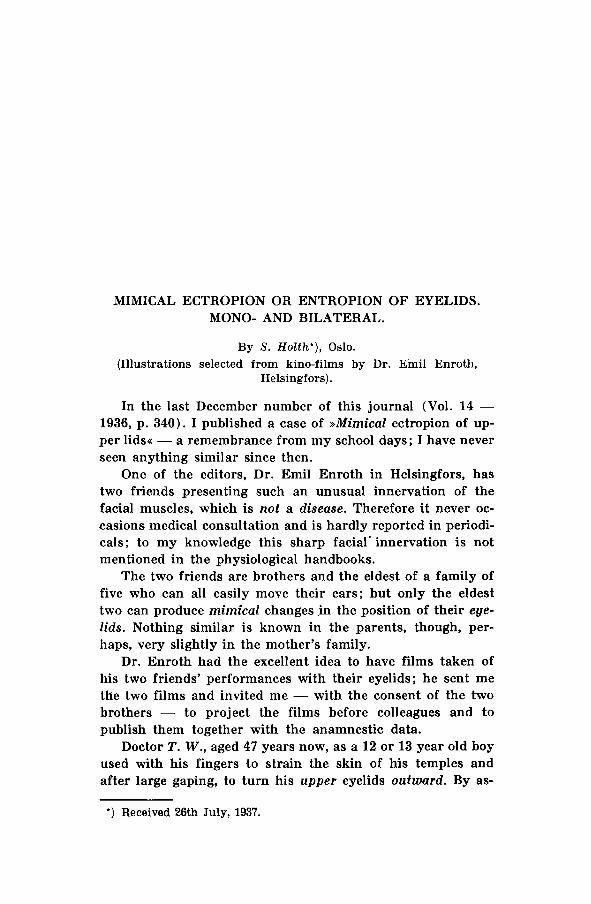
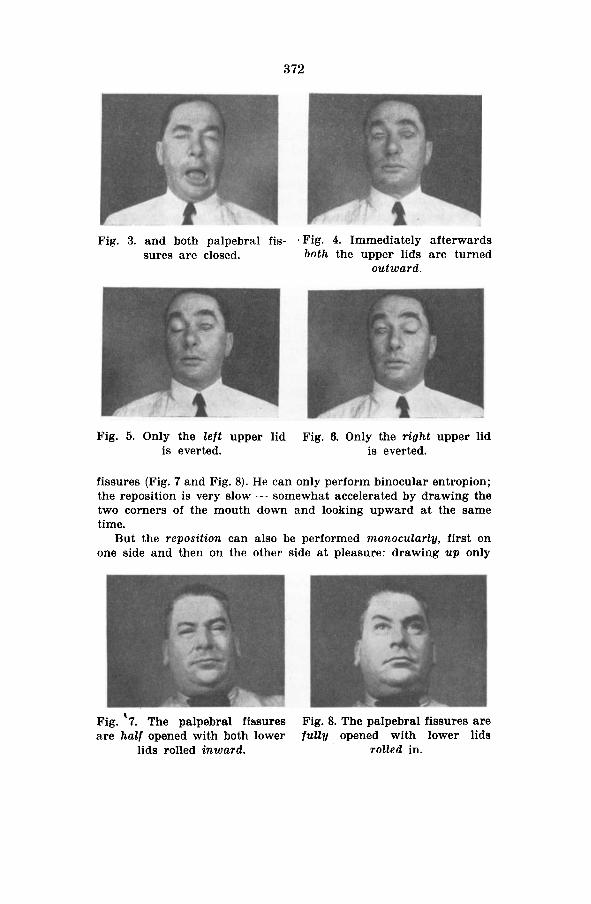
T. W. always closes both his palpebral fissures (Fig. 3) im- mediately before the binocular ectropinon (Fig. 4) - mostly after large gaping (Fig. 2); the following monucular eversions (Fig. 5.and 6) are effected under moderate mouth-mimics. - He can also per- form all the tricks without opening his mouth; but this is more .difficult and sometimes unsuccessful.
He rapidly restores the normal position of his everted lids by a simple wink, whilst his mouth is closed.
S. W. likewise begins by closing both his palpebral fissures as in Fig. 3, but he never gapes. The rolling in of the lower lids is photographically less impressive than ectropion of the upper lids. The beginning inversion cannot be seen either in reality or on the film, because the upper lids cover the iower ones - the inversion is only seen completed after half or full opening of the palpebral
Fig. 1. No mimics. Fig. 2. The mouth is opened
372
Fig. 3. and both palpebral fis- 'Fig. 4. Immediately afterwards sures are closed. both the upper lids are turned
out ward.
Fig. 5. Only the l e f t upper lid Fig. 6. Only the right upper lid is everted. is everted.
fissures (Fig. 7 and Fig. 8). He can only perform binocular entropion; the reposition is very slow - somewhat accelerated by drawing the two corners of the mouth down and looking upward at the same time.
But the reposition can also be performed monocularly, first on one side and then on the other side at pleasure: drawing up only
Fig. '7. The palpebral fissures Fig. 8. The palpebral fissures are are half opened with both lower fully opened with lower lids
lids rolled inward. rolled in.
373
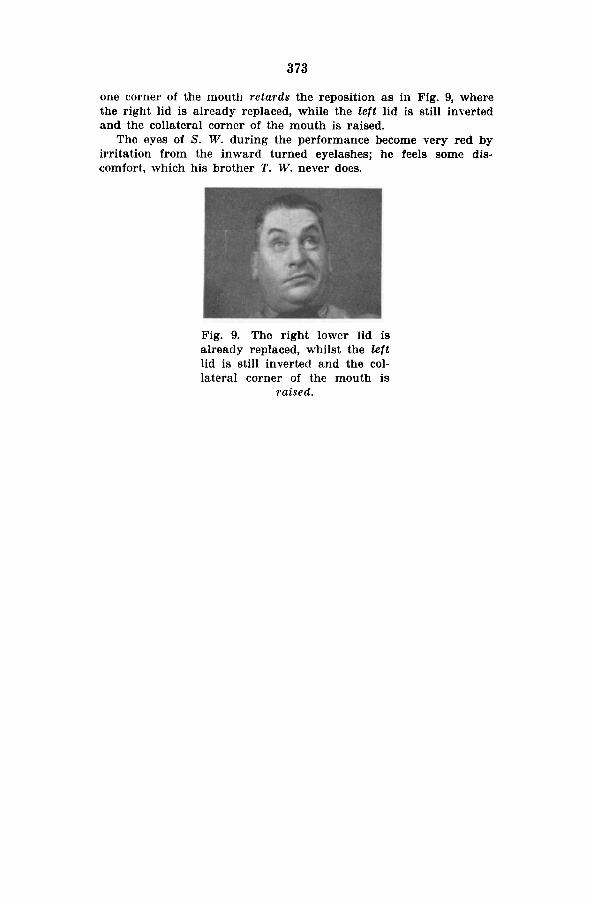
one corner of the mouth retards the reposition as in Fig. 9, where the right lid is already replaced, while the left lid is still inyerted and the collateral corner of the mouth is raised.
The eyes of S. W. during the performance become very red by irritation from the inward turned eyelashes; he feels some dis- comfort, which his brother T. W. never does.
Fig. 9. The right lower lid is already replaced, whilst the left lid is still inverted and the col- lateral corner of the mouth is
raised.












![University of Groningen Paralytic ectropion treatment with ...€¦ · of ectropion. For this purpose, a new photograph-based scoring method [the Ectropion Severity Score (ESS)] was](https://img.pdfslide.us/doc/110x75/6105e5898f8d757652610080/university-of-groningen-paralytic-ectropion-treatment-with-of-ectropion-for.jpg)