-
7/28/2019 Millers Anesthesia - Sixth Edition_ANESTHESIA
APPARATUS_18
1/6
Use of this content is subject to the Terms and Conditions of
the MD Consult web site.
Miller: Miller's Anesthesia, 6th ed., Copyright 2005
Elsevier
ANESTHESIA APPARATUS
Early Delivery Systems
For the first public demonstration of ether anesthesia, Morton
used a specially constructed glassbottle with an attached
mouthpiece (see Chapter 9 ). In England, John Snow developed a new
type ofether inhaler and took up the practice of ether anesthesia
as a full-time endeavor. His apparatusprovided valves to prevent
rebreathing, and although he experimented with methods for
carbondioxide absorption, he did not develop it into a clinically
useful technique. John Snow was aware ofthe difficulties associated
with the simple mouthpiece that was used with a noseclip by Wells
andMorton. In his book on ether published in 1847, [355] he states
the following:
For some of the adult patients, after they lost their
consciousness, made such strong
instinctive efforts to breathe by the nostrils, that the air was
forced through thelachrymal ducts, and occasionally they held the
breath altogether for a short time, andwere getting purple in the
face, when the nostrils had to be liberated, for a short time,
toallow respiration of the external air, and thus a delay was
occasioned.
With the introduction of chloroform, several inhalers were
developed to administer the agent.Ferdinand Junker[356] (18281901)
devised a simple inhaler, consisting of a bottle to hold
liquidchloroform, an inflow tube into which the anesthetist could
squeeze air with a hand pump, and anoutflow tube directed into the
mask. The Junker inhaler underwent several modifications to
improveits safety but was rarely used in the United States. Joseph
T. Clover[357][358] (18251882), the
prominent English anesthetist after John Snow, devised several
devices for the administration ofnitrous oxide, ether, and
chloroform. The Clover bag held more than 16 L of air, with
chloroformvapor at approximately 4%. Smaller concentrations could
be given by adjusting a valve on thefacemask that allowed dilution
of the chloroform with air. A clever solution to avoid the problem
ofhigh concentrations of chloroform was presented by Augustus
Vernon Harcourt (18341919) in1912. This apparatus was one of the
several "draw-over" systems that brought the inspired air over
avaporizer heated by a small candle. The chloroform double-necked
flask held the liquid chloroformand two beads that rose to the top
or sank to the bottom, depending on the temperature of the
liquid.Several draw-over chloroform delivery systems are described
in Dudley Buxton's 1914 textbook.[359]The problem with these early
delivery systems for longer procedures was the potential for
hypoxiaand partial rebreathing of expired carbon dioxide.
Other types of anesthesia machines were developed to provide
anesthesia with the insufflationmethod, whereby a small catheter
was placed with its tip near the carina to deliver air and ether
orchloroform. These were continuous-flow machines that did not rely
on respiratory movements foroxygenation and were based on the work
of Samuel Meltzer (18511920) and John Auer (18751948) demonstrating
its safe use in animals.[360] It was one solution to the problem of
pneumothoraxand respiratory decompensation during thoracic surgery.
C. A. Elsberg's (18711948) continuous-flow machine was described in
1911 and went through several modifications.[361] The
popularShipway model was used by Francis E. Shipway (18751968) to
provide anesthesia to King GeorgeV of England for rib resection and
drainage of empyema, a feat for which Shipway was knighted. In
retrospect, it is clear that these continuous flow machines were
not capable of eliminating carbondioxide in all cases,[362] and
anesthesia machines eventually were developed that allowed
to-and-frorespiration through one large-bore endotracheal tube.
Copyright 2005 Elsevier Inc. All rights reserved.
www.mdconsult.com
-
7/28/2019 Millers Anesthesia - Sixth Edition_ANESTHESIA
APPARATUS_18
2/6
Bookmark URL: /das/book/view/44273446-2/1255/33.html/top
-
7/28/2019 Millers Anesthesia - Sixth Edition_ANESTHESIA
APPARATUS_18
3/6
Use of this content is subject to the Terms and Conditions of
the MD Consult web site.
Miller: Miller's Anesthesia, 6th ed., Copyright 2005
Elsevier
Compressed Gases and Reducing Valves
Of major importance in the design of the modern anesthesia
machine was the compression of gasesin metal
34
cylinders. Oxygen and nitrous oxide were available under
compression as early as 1885 through themanufacturers S. S. White
of Philadelphia and Messrs. Coxeter of London. This allowed
thedevelopment of compact machines capable of prolonged anesthetic
delivery without the cumbersomefeature of low-pressure reservoirs.
Frederick Hewitt's first anesthetic gas machine designed forgiving
oxygen and nitrous oxide mixtures had two nitrous oxide cylinders
and one oxygen cylinder
and were fed into a large breathing bag through a double
cylinder yoke.[139]
Oxygen concentrationscould be adjusted at the stopcock near the
mask. His preferred oxygen concentrations were 5% to8%. With the
addition of oxygen, he attempted to "dispense with cyanosis, jerky
and irregularbreathing, deep stertor and clonic movements of the
extremities."
The invention of the reducing valve is accredited to Jay Albion
Heidbrink (18571957), ananesthesiologist from Minneapolis who
observed that the opening from high-pressure cylinders oftenfroze
closed as the gases were released. He described a valve that
reduced the high tank pressures toworking pressures and
incorporated this device into his Heidbrink Anesthetizer. In
Germany,Heinrich Drager (18471917) and his son Bernhard Drager
(18701928) developed reducing valvesto control an even, accurate
flow of carbon dioxide gas drawn from beer cylinders, and these
valves
were later used in the early anesthesia machines. Further
refinements to the early machines wereadded by James T.
Gwathmey[363] and H. Edmund G. Boyle[364] (18751941) chiefly
through theaddition of bubble-through heated water baths for
estimation of gas flows. The Boyle machinepassed various amounts of
oxygen through ether with a "water-sight" meter. This
flowmeterestimated the flow through the vaporizer from how many of
the holes were generating bubbles.Heidbrink further improved the
flowmeter by using an inverted float in a tube of varying taper
withcalibrations marked on the side. Rotating floats, also called
rotameters, have slanted grooves cut intothe rim, causing them to
rotate, and they are more accurate than the ball or nonrotating
floats.Rotameters were introduced in 1908 by Karl Kuppers and first
used in anesthesia in 1910.[365]
Bookmark URL: /das/book/view/44273446-2/1255/34.html/top
Copyright 2005 Elsevier Inc. All rights reserved.
www.mdconsult.com
-
7/28/2019 Millers Anesthesia - Sixth Edition_ANESTHESIA
APPARATUS_18
4/6
Use of this content is subject to the Terms and Conditions of
the MD Consult web site.
Miller: Miller's Anesthesia, 6th ed., Copyright 2005
Elsevier
Carbon Dioxide Absorption
Anesthesiologists from the first half of the 20th century were
not privileged to visit just one hospitalduring a day's work.
Visits to several institutions might take place in a single day,
with thepractitioners bringing their own delivery systems and drugs
with them as they traveled.Understandably, there was a priority for
portability and elimination of waste, because
theseanesthesiologists paid for the agents themselves. One
development that conserved gases and vaporswas the use of systems
that absorbed expired carbon dioxide and allowed rebreathing of
expiredgases.
Several ineffectual attempts were made to introduce carbon
dioxide absorption methods in the 19thcentury. John Snow and Alfred
Coleman (18281902) were motivated to conserve anesthetic gasesthat
escaped into the atmosphere through nonrebreathing valves. Coleman
devised a system of
absorbing carbon dioxide by passing the expired gases over
slaked quick lime.[366][367] The recoveredgases were then used for
subsequent anesthetics ( Fig. 1-15 ). Franz Kuhn (18661929)
describedsoda lime absorption of exhaled carbon dioxide in 1905,
but the report did not attract attention.[368]
Dennis Jackson demonstrated the use of soda lime absorption to
maintain stable levels of anesthesiafor several hours in animals
with minimal ether consumption.[369] The animals were given
additionaloxygen to meet metabolic needs, but the anesthetic gases
were rebreathed, resulting in economy andimproved maintenance of
body temperature and airway humidity. In 1923, Ralph Waters
(18841979) (see Fig. 1-18B ), working then as an anesthesia
practitioner in Sioux City, Iowa, contactedJackson and devised a
soda lime canister for clinical use.[370] The canister was attached
to a breathing
hose close to the face, and although it was cumbersome to use,
the device was widely distributed.The in-line soda lime canister
launched the academic career of Waters, who later became one of
themost prominent figures in anesthesiology during the first half
of the 20th century. In 1930, Brian C.Sword[371] altered the Waters
canister by attaching it to the chassis of a movable cart with two
hosesdirected to the airway, one for inspired gases and one for
exhaled gases.
Bookmark URL: /das/book/view/44273446-2/1255/35.html/top
Copyright 2005 Elsevier Inc. All rights reserved.
www.mdconsult.com
-
7/28/2019 Millers Anesthesia - Sixth Edition_ANESTHESIA
APPARATUS_18
5/6
Use of this content is subject to the Terms and Conditions of
the MD Consult web site.
Miller: Miller's Anesthesia, 6th ed., Copyright 2005
Elsevier
Controlled Vaporizers
With the introduction of more potent volatile anesthetics such
as halothane it became important tocontrol the concentration of
inspired vapor carefully. To solve this problem, Lucien
Morris[372]invented the copper kettle to vaporize liquid
anesthetics. Its advantage rested on the
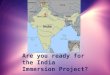
Figure 1-15 Alfred Coleman's economizing device. The anesthetic
gases entered the lower bag and passed into the upperbag through a
one-way valve. Gases were inhaled and exhaled through the tube (h),
passing over a lime container (1, 2)held in frame (k) that
eliminated carbon dioxide; (c) is gas inlet. The conserved gas in
the upper bag was used during alater anesthetic administration.
(From Coleman A: Mr. Coleman's economizing apparatus for
re-inhaling the gas. Br JDent Sci 12:443, 1869.)
35
fact that as the agent was vaporized, there was little change in
the temperature of the anestheticliquid. The copper kettle could be
used with any agent provided that the practitioner was cognizantof
the vapor pressure of the agent and the flow rates of the inspired
gases. Without the addition ofdiluent gases such as nitrous oxide
or oxygen, the copper kettle could deliver lethal concentrations
ofvapor. The vaporizers in common use today use bimetallic strips
that bend as the temperature drops,permitting more fresh gas to
enter the vaporizing chamber. Vaporizers have been designed for all
theagents in use today, including halothane, enflurane, isoflurane,
desflurane, and sevoflurane. Themodern anesthesia machines are also
equipped with scavenging systems designed to minimizeescape of
anesthetic vapors and nitrous oxide into the operating room.
Although controversial, somestudies have shown that daily exposure
to anesthetic vapors in low concentrations can havedeleterious side
effects. [373]
Copyright 2005 Elsevier Inc. All rights reserved.
www.mdconsult.com
-
7/28/2019 Millers Anesthesia - Sixth Edition_ANESTHESIA
APPARATUS_18
6/6
Use of this content is subject to the Terms and Conditions of
the MD Consult web site.
Miller: Miller's Anesthesia, 6th ed., Copyright 2005
Elsevier
Ventilators in the Intensive Care Unit
The earliest ventilator, the Fell-O'Dwyer apparatus, was
described in 1892.[374] It was used as early as1896 to provide
respiratory support in cases of opium poisoning. Rudolph Matas, a
surgeon in NewOrleans who contributed significantly to the early
development of regional anesthesia in the UnitedStates, was one of
the first to use the Fell-O'Dwyer ventilator during thoracic
surgery.[375] During thepolio epidemic, thousands of afflicted
patients were kept alive with the Drinker respirator,[376]
oftenreferred to as the iron lung, a negative-pressure device that
surrounded the patient and provided forair movement in and out of
the lungs. A Swedish ventilator called the Spiropulsator was
introducedin 1934 and modified in 1947 by E. Trier Moerch.[377]
This ventilator used a piston pump to deliver afixed volume of gas.
Ventilators today are usually an integral part of the anesthesia
machine anddirect compressed air into a rigid container containing
a bellows that inflates the lungs. Bjrn Ibsen[378] (1915-), a
Danish anesthesiologist, initiated the concept of intensive care
units in the early 1950s
to care for polio patients and guided the transition from iron
lungs to modern ventilators. Intensivecare units have since become
an integral part of the modern hospital, with anesthesiologists
activelyinvolved in their daily operation.
Bookmark URL: /das/book/view/44273446-2/1255/37.html/top
Copyright 2005 Elsevier Inc. All rights reserved.
www.mdconsult.com