Embed Size (px)
Citation preview

American Journal of Medical Genetics 47:969-976 (1993)
Mild Brachmann-de Lange Syndrome. Phenotypic and Developmental Characteristics of Mildly Affected Individuals
John B. Moeschler and John M. Graham, Jr. Clinical Genetics and Child Development Center (J.B.M., J.M.G.), Dartmouth Medical School, Lebanon, New Hampshire; and Division of Clinical Genetics and Dysmorphology (J.M.G.), Ahmanson Department of Pediatrics, Steven Spielberg Pediatric Research Center, Medical Genetics Birth Defects Center, Cedars-Sinai Medical Center, UCLA School of Medicine, Los Angeles, California
~ ~ ~~~~
Since 1981, we have identified 3 patients with mild Brachmann-de Lange syndrome (BDLS) who have had subtle but definite manifesta- tions of the syndrome and mild effects on growth and development.
J.G. (B.D. 12/9/72) was first examined at 20 months. He had rather typical craniofacial findings and hirsutism, limitation of full su- pination of his arms, and brachyclinodactyly of the 5th fingers. I& was estimated at 65.
K.H. (B.D. 10/10/83) was first examined by us at age 9 months and was diagnosed as having “mild” BDLS. At age 5, K.H. has demonstrated relatively normal cognitive development (low average-average I& of 74) with specific learn- ing problems: weakness of visual-motor skills, delayed expressive language development, and articulation difficulties. At age 7, he was attending a regular 1st grade classroom, with some special education assistance.
M.E.(B.D. 4/19/78) was diagnosed at age 10 years as having “mild” BDLS. His physical changes were more subtle than those of the 2 patients above. At age 10, M.E. was in the reg- ular 4th grade classroom receiving special ed- ucation support. His I& was in the borderline- low-average range. He had strengths in rote verbal skills, with weaknesses in reading and writing.
These 3 patients demonstrate mild BDLS in which characteristic manifestations of the syndrome, particularly craniofacial anoma- lies, are present and recognizable, but quite subtle, thus making the clinical diagnosis dif- ficult. In addition, the milder physical phe-
Received for publication November 6, 1991; revision received March 5, 1993.
Address reprint requests to John B. Moeschler, M.D., Clinical Genetics and Child Development Center, Dartmouth Medical School, Lebanon, NH 03756.
0 1993 Wiley-Liss, Inc.
notype is associated with milder cognitive and behavioral consequences. When compar- ing patients with mild BDLS to those in our practice (4 others) with typical changes, we find that birth weight, absence of major anomalies, and subtlety of craniofacial abnor- malities are predictive of mildly affected pa- tients. 0 1993 Wiley-Lisa, Inc.
KEY WORDS Brachmann-de Lange syn- drome, normal intelligence, mild phenotype
INTRODUCTION Brachmann-de Lange syndrome (BDLS) in severe
form is typically easily recognized by the experienced examiner. The characteristic face, small size, and (when present) limb anomalies enable one to make the diag- nosis in the newborn or young infant. The cause of the syndrome is unknown, but monogenic (autosomal domi- nant) cause has been suggested [Robinson et al., 19851. No confirmatory cytogenetic biochemical or molecular genetic marker exists.
We report on 3 patients with mild BDLS: all have only mild developmental delays or cognitive disability; one of the three (Patient 3) has physical changes mild enough for the diagnosis to have gone unrecognized for 10V2 years.
CLINICAL REPORTS Patient 1
J.G. (BD 12/9/72) was first seen by us at age 13 years (Figs. 1-3). At that time, he had short stature (height age of 8 years a t age 13 years); synophrys, bilateral lid ptosis, long eyelashes, short triangular nose with ante- verted nares, long philtrum, smooth upper lip with notching of the middle of the vermilion border; small and posteriorly augulated ears; apparent hypertelorism (inner canthal distance 3.5 cm, 90th centile; interpupil- lary distance 6.0 cm, 90th centile; outer canthal dis-

970 Moeschler and Graham
Fig. 1. Patient 1 at age 13 years.
tance 9.0 cm, 50-75th centile). He had generalized hir- sutism. Normal public hair was present and testes measured 1 x 2 cm each. There was limited supination of the forearms and brachyclinodactyly of the 5th fingers bilaterally, each with a single flexion crease. He also had single transverse palmar flexion creases.
J.G. had been diagnosed at this institution at age 20 months. At that time he exhibited delays in growth and development. Diagnosis was based on the typical face, minor anomalies of hands and feet, and mild develop- mental delays. (Interestingly the diagnosis was con- firmed in 1975 by Dr. David W. Smith. Dr. Smith had been visiting the University of Virginia where the fam- ily was being seen by Dr. Robert Blizzard for a second opinion because they did not believe the diagnosis was BDLS.) When assessed using the Bayley Scales of Infant Development at age 22 months, J.G. was functioning at the 18 month level (Developmental Index of 76).
Now at 18 years, J.G. is attending high school taking
Fig. 2. Patient 1. Note digital anomalies and limited supination of hands.
prevocational activities. He continues to have expres- sive language and communication difficulties. Last I& measure was 66 with demonstrated weaknesses in ex- pressive language.
Patient 2 K.H. (BD 10/10/83) was referred at age 9 months for
failure to thrive, developmental delay, and to rule out Miller-Dieker syndrome. At birth he was noted to have single palmar creases, a sacral skin tag, short 5th fingers, cortical thumbs, and lid ptosis. Diagnostic eval- uation at the time included a normal CT scan and nor- mal chromosomes.
K.H. was born to a 27-year-old gravida 2 para 1 woman after a normal pregnancy. Birth weight was 2.75 kg (5%) and length was 50.5 cm (50%). Birth head cir- cumference was not recorded. Infancy was characterized

Mild Brachmann-de Lange Syndrome 971
tively weak with an age equivalent of 3 years 6 months. Language assessment (using Test for Auditory Compre- hension of Language-Revised) demonstrated low-aver- age receptive language skills (age equivalent of 4 years 4 months). One word receptive language skills esti- mated by the Peabody Picture Vocabulary Test were equivalent to 5 year 10 months. Expressive language skills (using the Pattern Elicitation Syntax Test) were more delayed than receptive abilities. In addition, he had articulation problems. Hearing was normal. At age 6 year 9 months, he was attending the regular first grade classroom at a neighborhood school.
The diagnosis of BDLS was first made at 9 months (Figs. 4-6) on the basis of microcephaly, small stature, marked hypertonia, low frontal hairline, synophrys, “bushy” eyelashes, lid ptosis (left greater than right), short triangular-appearing nose with anteverted nares, long philtrum, and mild “breaking” of upper lip with notching of middle of the vermilion border of the upper lip. A 5 x 2 mm pilonidal skin tag was present. All fingers were tapered. There was a congenital contrac- ture the left 5th finger at the PIP joint and shortness of the 1st and 5th metacarpals. Both 5th fingers exhibited a single flexion crease and there were single transverse
Fig. 3. Patient 1. Hirsutism of back.
by delays in growth and development. Although height and weight were normal at birth, by 6V2 months of age, growth was greater than 2 S.D. below the mean for height, weight and head circumference. He experienced feeding problems characterized by refusing to nurse or use a bottle and frequent vomiting. He began cup drinking and thickened foods by 6 months. By age one year, he was taking a soy-based formula thickened with cereal, but vomiting continued. Motor develop- ment was delayed at age 6% months when he was noted to have marked increase in muscle tone and retention of primitive reflexes. However, he pulled to stand at 11 months, crawled at 12 months, sat independently at 15 months, and walked independently a t 24 months. A t 15 months, he said “mama” and “dada” specifically.
At 4 years 8 months of age, K.H.’s mental age (on the McCarthy Scales of Children’s Abilities) was 3 years 6 months. At age 5 years 7 months, I& as measured by the Stanford-Binet was estimated at 74. At 6 years 7 months, K.H. had I.&. measured in the borderline range (I.&. 66; Mental Age 4 years 9 months) using the Stan- ford-Binet. This measured somewhat below the Leiter International Scales (a “nonverbal” measure of intel- ligence) Of 759 presumably because Of the language prob- lems he was exhibiting. Visual-motor skills were rela-
Fig. 4. Patient 2 at age 9 months (top) and at 27 months (bottom). Note that the facial changes are more typical at the older age.

972 Moeschler and Graham
Fig. 5. Patient 2 at age 40 months (top) and 6 years 9 months (bottom). In bottom right, note hirsutism of face.
palmar flexion creases bilaterally. He was hirsute, but because of blond coloring it was not easily apparent. Mild kyphoscoliosis (7 degrees) was noted at 18 months.
Radiographs of hand and wrist showed advanced bone age, between 15 and 18 months at age 9 months. All metacarpals appeared short with marked shortness of the first. The middle phalanx of the fifth digit was small and triangular. Upper GI series demonstrated gastro- esophageal reflux and mild colonic malrotation.
As K.H. aged, his manifestations continued to suggest BDLS (Figs. 4, 5).
Patient 3 M.E. (B.D. 4/19/78) presented at age 10V2 years for
assistance with school and behavior problems. He had been diagnosed as having Williams syndrome at about age 4 years.
He was the product of a unremarkable pregnancy born to parents 31 (father) and 28 years old. He was born at 37 weeks gestation with birth weight of 3.6 kg (50th centile); length of 47 cm (5th centile) and OFC of 34 cm (50th centile). There were minor newborn problems of transient hypoglycemia and periumbilical cellulitis that resolved without consequence. His parents first
became concerned during his infancy because of irri- tability, difficulty with feeding, and low muscle tone.
M.E. was described as a very difficult baby who nursed every 2-3 hours because of vomiting virtually every feeding until 7 months of age. He had low muscle tone and was extremely irritable. His parents reported that he “never appeared to recognize family members” during infancy. His parents first became concerned about developmental delays at age 6-8 months. They reported the following developmental events: rolling, 6 months; sit when placed, 12 months; cruising, 15 months; walking 18 months; first words, 15 months; phrases, 17 months; sentences, 36 months; toilet trained, 4 years, 8 months. Early intervention and spe- cial education services were started at age 2 years.
M.E. underwent a number of psychological assess- ments as summarized in Table I. His testing at ages 4-9 and 5-10 years probably overestimated his I& because of his apparent rote language skills (Table 11). Tests of language abilities showed that M.E. had relative strength in verbal comprehension and expression, when com- pared to general cognitive abilities (see Table 11).
These results suggested that language understanding was within a low average range and that cognitive skills, as measured on intelligence tests, are more delayed with rote language use a relative strength. M.E.’s language skills were attributed to the interventions that started at an early age.
At 7 years 10 months, tests of achievement derived from the Woodcock-Johnson Battery were done on M.E. Reading and written language were well below age ex- pectancies and comprised of alphabet knowledge; math skills consisted of counting in quantities of 5 or less; his general knowledge was similar to that of a 5-year-old.
His physical findings (Figs. 7-9) at age 10-112 years 6 months were consistent with mild BDLS. His height was 124.5 cm (< 5th centile; mean for age 7-6 years); weight 26 kg (10-25th centile); OFC 52.2 cm (50th cen- tile). He had blond hair that extended onto his forehead. His blonde coloring made his synophrys difficult to see. There was thinning and “beaking” of the upper lip, with mild notching of the vermilion border present. He had mild auricular anomalies and low-set ears. Strabismus was present. His hands were small with hypothenar hypoplasia, mild syndactyly of digits 2-3. Left total hand length was 13.3 cm; right 13.6 cm (both < 3rd centile); middle finger length; right 5.5 cm (< 3rd cen- tile) and left 5.2 cm (< 3rd centile). He had general body hirsutism, particularly notable on his back, that was
TABLE I. Intelligence Testing (M.E.) CA MA
Test (yrs) (yrs) FSIQ VIQ PIQ Binet 4-9 4-2 “low normal” WIPPSI 5-10 3-6 to4-6 73 81 70 WISC-R 7-10 64 67 65 WISC-R 8-10 63 66 65 FSIQ = Full Scale IQ. VIQ = Verbal IQ. PIQ = Performance IQ.

Mild Brachmann-de Lange Syndrome 973
Fig. 6. Patient 2. Bottom right: note pilonidal skin tag. Hands at age 9 months (bottom left) and 6 years 9 months (top right and left). Note the hypothenar hypoplasia and 1st metacarpal and 5th digital anomalies.
difficult to see because of the blonde coloring. Also noted were small areolae.
Karyotype, T4 and TSH, and urine MPS screen were all normal or negative. Lateral and AP of spine were normal. Hand and wrist roentgenograms demonstrated normal morphology with small phalanges as indicated on pattern analysis.
DISCUSSION In addition to its recognizable phenotype, BDLS is
generally characterized by severe disabilities [Hawley et al., 1985; Ptacek et al., 1963; Preus and Rex, 19831. Beck [19761 estimated that as many as 10% of patients with BDLS may have normal to near-normal intel- ligence. In our review of the literature (Table III), it appears that there are a number of reports of mild BDLS. We agree with Opitz [19851 that the milder pa- tients are underrepresented in more reviews of the con- dition and, as a result, the literature is biased toward the more severe end of the spectrum. These 3 patients are reported to add the delineation of the phenotype and
TABLE II. Laneuaee Testing (M.E.) Test Age I& Receptive Expressive
8-10 years 63
TACLR 84
OWPVT 86 (receptive)
(expressive)
to discuss the developmental characteristics of patients with mild BDLS.
All 3 of our patients had IQs that were nearly normal (Patient 1, 65; 2, 66; 3, 65). K.H. and M.E. attend the typical classroom with age appropriate peers. Now, at 18 years, J.G. attends high school, attending largely voca- tional training classes. Although J.G. uses speech, he continues to have communication problems that have hampered his ability to find work and to perform in school.
All 3 had feeding problems in infancy that occurred coincidentally with deceleration of growth. Conse- quently, all had been evaluated for “failure to thrive.” Delays in motor development were evident by age one year, but all were ambulating independently by age 2 years. Language delays were noted in the 2nd year. All were enrolled during this age range in an early inter- vention program and, subsequently, into a preschool special education program. By elementary school, all were attending the regular classroom setting with ap- propriate special education supports. None had serious medical problems; none had seizures. Hearing and vi- sion were normal in all. None had significant behavioral disturbances that complicated the educational oppor- tunities. One had attention deficit requiring stimulant medication.
In comparing the cognitive profile ofthe 3 patients, we find all had low-average to borderline I.&. estimates in preschool years, which upon reevaluation during early school age, settled into the borderline range. Patients 1 and 2 had, in addition, significant relative difficulties

974 Moeschler and Graham
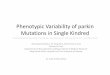
Fig. 7. Patient 3 at age 10% years. Note (top) facial hirsutism, apparent hypertelorism, long philtrum with “notching” of vermilion border of midline of upper lip and “beaking” of upper lip, and (bottom) synophrys and strabismus.
with expressive language and visual-motor abilities. Although Patient 3 had relatively strong communica- tion skills, his examiners attributed those skills to inter- vention, noting relative weakness in verbal processing abilities on I& testing.
In an effort to identify features that might better predict eventual developmental abilities, the following were reviewed: age at diagnosis; birth weight, height and OFC; presence of major limb malformations; devel- opmental milestones (age at ambulation and use of phrases).
The age a t diagnosis is affected by both patient vari- ables (e.g. presence or absence of limb anomalies; the presence of typical facial changes) and examiner vari- ables (e.g., experience). Presumably, later diagnosis would suggest subtlety of findings. In our 3 patients, the timing of diagnosis did not appear to relate to severity of disability. Patient 1 was recognized at 20 months (1975), Patient 2 at 9 months, and Patient 3 at 12.5 years.
All 3 patients had normal birth weight and length. In Patient 1, the diagnosis was made at age 20 months on the basis of the facial changes and mild hand and foot anomalies. In Patient 2, the diagnosis was made a t 9 months, although the infant was suspected shortly after birth as having Miller-Dieker syndrome. Patient 3 was not suspected to have BDLS until early adolescence,
due to the subtle nature of his physical anomalies (he had been previously diagnosed as Williams syndrome during the preschool years). In all cases, the diagnosis was made on the basis of physical findings in conjunc- tion with delays in growth and development.
In comparing our 3 mild patients with our 5 “typical” patients (Table 111)) we find that, in all BDLS patients with severe disabilities, significant growth retardation at birth was present, together with more obvious facial anomalies and, in one patient, major limb defects. None were ambulatory or could speak at 2 years.
In comparing our cases with those in the literature with normal or near normal intelligence, we find that none had major limb anomalies. None with normal in- telligence had significant intrauterine growth retarda- tion, i.e. birth weight less than 2.25 kg. Comparison of facial anomalies among those with normal or near nor- mal intelligence in the literature was not possible.
As the children with BDLS enter the elementary school years, it is important to be aware of the cognitive profile that appears to be associated with mild BDLS. We noted relative weakness in receptive and expressive language and visual-motor abilities.
None of our patients had seizures. Barr et al. [1971] found among 19 patients that all with seizures or epilep- tiform changes on EEG had associated severe mental retardation. None of our mild patients or those milder patients in the literature had seizures. Barr et al, [19711 also found a correlation with total ridge count (TRC) and intelligence: every patient with I& 5 36 had a TRC 5 75 and birth weight I 2,200 g. Unfortunately, none of our patients or others in the literature have been examined for this.
No patient with mild BDLS had major limb anoma- lies; all had minor anomalies (e.g., brachyclinodactyly of the fifth fingers). Birth weight was not a reliable predic- tor of milder developmental disabilities; some with nor- mal intelligence had birth weights < 2nd centile. How- ever, 6 of 9 patients in the literature with mild BDLS had birth weights in the normal range (i.e., above the 2nd centile). Microcephaly does not always predict se- vere disabilities. Our patient 1 had congenital micro- cephaly; case 2 had microcephaly in early childhood.
These cases remind us that some patients (perhaps as many as 10%) with BDLS will have normal to near normal intelligence. Those factors that appear to predict a better developmental outcome include normal growth parameters at birth, absence of major limb anomalies, absence of seizures, more subtle facial changes (as re- flected in some cases in older age at time of diagnosis), ambulation by 2 years, and the presence of expressive language (albeit delayed) by 2 years. The presence of major limb anomalies predicts more severe disabilities.
ACKNOWLEDGMENTS This work was supported in part by a grant from the
U.S. Department of Education, Bureau of Special Edu- cation and Rehabilatative Services (HCEEP grant #H024F800017), the New Hampshire Department of Health and Human Services, Bureau of Special Medical Services, SHARE’S Cedar-Sinai Disability Center, and the Charles H. Hood, I11 Foundation of Boston, MA. The authors acknowledge the support of Sally Trachier and

TAB
LE 1
11.
Com
pari
son
of M
ild W
ith n
pic
al B
DLS
See
n by
Aut
hors
and
Lit
erat
ure
Rep
orts
of M
ild B
DL
S
Thi
s re
port
I.Q
.
Bir
th
wei
ght
(cen
tile
)
Bir
th
leng
th
(cen
tile
)
Maj
or
Bir
th O
FC
hand
A
ge a
t use
of
phra
ses
Age
at
wal
king
(c
enti
le)
anom
alie
s (m
onth
s)
(mon
ths)
O
ther
Pa
tien
t 1
65
Pati
ent
2 Pa
tient
3
66
64
“Typ
ical
” B
DLS
at
Dar
tmou
th
J.B
. <
50
M.M
B
.F.
R.H
.
< 3
0 <
30
< 3
0
Lit
erat
ure
“mild
” B
DLS
M
acIn
tire
and
“m
ild m
enta
l E
isen
I19
651
reta
rdat
ion
1196
91
Pash
ayan
et a
l.
75
Bec
k [1
9741
77
Bec
k f1
9761
94
(c
ase
1)
L198
21
Gad
oth
et a
l.
78
Rob
inso
n et
al.
“70-
80”
1198
51
Mos
her
et a
l. “m
ild-m
oder
- I1
9851
at
e M
R
Gre
enbe
rg a
nd
- 70
R
obin
son
[198
91
5th
5th
50th
< 2
nd
< 2
nd
< 2
nd
< 2
nd
< 2
nd
i 2n
d
?
50th
10th
< 2
nd
< 2
nd
5th
5th
50th
10
th
< 2
nd
< 2
nd
< 2
nd
< 2
nd
? ? ? ? ? ? ? ?
< 5
th
min
or o
nly
20
? m
inor
onl
y 24
25
th
min
or o
nly
24
< 2
nd
min
or o
nly
none
at 3
yea
rs 6
m
onth
s no
t re
cord
ed
min
or o
nly
none
at
7 ye
ars
< 2
nd
yes
none
at
3 ye
ars
< 2
nd
min
or o
nly
none
at
5 ye
ars
? m
inor
onl
y 36
? m
inor
onl
y 36
? TR
C =
66
?
? m
inor
onl
y ?
< 2
nd
min
or o
nly
20 w
ords
at
19
mon
ths
? m
inor
onl
y ?
? m
inor
onl
y 60
? m
inor
onl
y ?
21
24
18
none
at
3 ye
ars
6
none
at
7 ye
ars
none
at
3 ye
ars
none
at
5 ye
ars
mon
ths
9 *? 9
14
> 19
?
Dia
gnos
is c
onfi
rmed
by
D.W
. Sm
ith
in
1975
som
e si
gn l
angu
age
Hea
ring
-im
pair
ed
(60-
80 d
B)
OFC
c
2nd
cent
ile
at
“mar
kedl
y im
pair
ed
two
affe
cted
off
spri
ng
norm
al O
FC a
t 9
year
s;
Mic
roce
phal
y pe
r-
sist
ed-<
2nd
cen
- til
e at
4 y
ears
Tw
o af
fect
ed o
ff-
spri
ng
norm
al o
ffsp
ring
diag
iiosi
s m
ade
at 2
8
7 ye
ars
spee
ch”
mon
ths

976 Moeschler and Graham
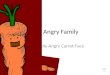
Fig. 8. Patient 3. Note the brachycephaly, hirsutism, and ear anomalies.
Ella Duhaime for assistance with manuscript prepar- ation.
REFERENCES Barr AN, Grabow JD, Matthews CG, Grosse FR, Mot1 ML, Opitz JM
(1971): Neurologic and psychometric findings in Brachmann- de Lange syndrome. Neuropaediatrie 3:46-66.
Beck B (1974): Familial occurrence of Cornelia de Lange’s syndrome. Acta Paediatr Scand 63:225-231.
Beck B (1976): Epidemiology of Cornelia de Lange’s syndrome. Acta Paediatr Scand 63531-231.
Gadoth N, Lerman M, Garty B-Z, Shmuelewitz 0 (1982): Normal intel- ligence in the Cornelia de Lange syndrome. Johns Hopkins Med J 150:70-72.
Greenberg F, Robinson L K (1989) Mild Brachmann-de Lange syn- drome: Changes ofphenotype with age. Am J Med Genet 32:90-92.
Hawley P P, Jackson L G, Kurnit D M (1985): Sixty-four patients with Brachmann-de Lange syndrome; A survey. Am J Med Genet 20: 453-459.
Mclntire MS and Eisen J D (1965): The Cornelia de Lange syndrome. A case report with mild mental retardation. Am J Ment Defic 70:438-442.
Mosher G, Schulte RL, Buehler BA, Sanger WG (1985): Pregnancy in a woman with the Brachmann-de Lange syndrome. Am J Med Genet 22:103-107.
Opitz JM (1985): Editorial Comment: The Brachmann-de Lange syn- drome. Am J Med Genet 22:89-102.
Pashayan H, Whelan D, Guttman S, Fraser FC (1969): Variability of the de Lange syndrome: Report of 3 cases and genetic analysis of 54 families. J Pediatrics 752353-858.
Reus M, Rex AP (1983): Definition and diagnosis of the Brachmann-de Lange syndrome. Am J Med Genet 16:301-312.
Ptacek W, Opitz JM, Smith DW, Gerritsen T, Waisman HA (1963): The Cornelia de Lange syndrome. J Pediatr 63:lOOO-1020.
Robinson LK, Wolfsberg E, Jones KL (1985): Brachmann-de Lange syndrome: Evidence for autosomal dominant inheritance. Am J Med Genet 22:89-102.
Fig, 9. Patient 3 hands, all a t age 10V2 years. Note mild 2-3 cutane- ous s syndactyly, hypothenar hypoplasia (top), normal hand and wrist hone morphology (by X-ray) with shortness of all digits.