Embed Size (px)
Citation preview

Migraine With Vasospasm andDelayed Intracerebral HemorrhageAndrew J. Cole, MD, Michel Aub\l=e'\,MD
\s=b\Three women with well-documentedmigraine associated with intracerebralhemorrhage are described. In each case,migraine headaches began during adult-hood. Unusually severe and protractedheadache heralded the onset of fixed neu-
rological deficits associated with lobar in-tracerebral hemorrhage. Striking carotidartery tenderness was characteristic. Ex-cept for a history of migraine, no cause forintracerebral hemorrhage could be estab-lished. In each case arteriography showedextensive spasm of the appropriate ex-tracranial or intracranial artery. Surgicalpathology following evacuation of twohematomata demonstrated signs of ves-sel wall necrosis associated with subacuteinflammatory changes. Vasospasm asso-ciated with severe migraine attacks mayresult in ischemia of intracranial vesselwalls, leading to necrosis and subsequentvessel rupture when perfusion pressure isrestored.(Arch Neurol. 1990;47:53-56)
Charcot, in 1881, suggested that anyof the transient neural dysfunc¬
tions of migraine could becomepermanent.1 Since then, migraine hasbeen associated with residual neuro¬logical deficits in a large number ofcases, and the concept of compli¬cated migraine has become widelyaccepted.26 Retinal, cortical, and
brain-stem lesions have each been de¬scribed. In the majority, neurologicaldysfunction is attributed to ischemiestroke, presumably secondary to vas¬cular spasm. Intracerebral hemor¬rhage in migrainous patients has onlyrarely been reported,7 and has some¬times been associatedwith preexistingarteriovenous malformations.8·9 Thisarticle describes a group of patients,all of whom are female, affected withmigraine who presented with lobar in¬tracerebral hemorrhage either duringor immediately following typical mi¬graine attacks. All patients were in¬vestigated in detail; no evidence of un¬derlying vascular malformation or tu¬mor was discovered. Radiologie studiessuggested that early and severe vaso¬
spasm of either the intracranial or ex¬tracranial vessels was important inthe development of hemorrhage.
REPORT OF CASESCase 1.—A 61-year-old woman had a
4-year history of migraine headaches pre¬ceded by an aura of left-sided paresthesias.She presented to the emergency depart¬ment complaining of severe bitemporalheadache, similar to previous attacks. Aneurological consultant found the patientto be normotensive, and the examinationresults to be entirely normal. A lumbarpuncture was performed and the results re¬vealed normal cerebrospinal fluid. She wasdischarged on analgesics and propranolol.Two days later she returned complaining
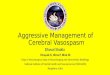
of severe headache, and, on this occasion,had a mild left hemiparesis with a leftBabinski's sign. Blood pressure was againnormal. Computed tomographic scans ofthe brain, with and without contrast infu¬sion, were normal (Fig 1, left), and she was
discharged on prednisone therapy in an ef¬fort to abort a severe migraine attack.Twenty-four hours later her headache
worsened. The following morning she was
difficult to arouse, and was again brought tothe emergency department. She was hyper-tesive, bradycardic, and stuporous, but, af¬ter stimulation, was able to follow simplecommands. She had a dense left hemiplegiaassociated with a left-sided homonymoushemianopia and right gaze preference.Brain computed tomographic scanningdemonstrated a right frontoparietal intra¬cerebral hemorrhage (Fig 1, center). A ca¬rotid arteriogram showed narrowing of theMl segment of the right middle cerebralartery (Fig 1, right). There was mass effectrelated to the hematoma, but no evidence ofarteriovenous malformation, aneurysm, ortumor. A right frontoparietal craniotomywas performed with evacuation of the hem¬atoma. Pathologic examination of the sur¬
gical material showed areas of cerebralnecrosis surrounding partially necroticruptured small arteries without evidence ofvascular malformation, tumor, or amyloidangiopathy. She made a slow recovery andwas discharged with a persistent neurolog¬ical deficit.Case 2.—A 45-year-old woman suffered
from common migraine headaches associ¬ated with photophobia and nausea for sev¬eral years. She took no medications andused no illicit drugs. One day prior toadmission she had an attack similar to herusual headaches, but somewhat more se¬vere. Twenty-four hours later, she suddenlydeveloped a left hemiparesis, associatedwith left hemihypesthesia. On admission,her blood pressure and heart rate werenormal. She was alert and cooperative.There was striking tenderness over theright carotid artery, but the pulse was nor¬mal and there were no bruits. She had adense left hemiplegia.Brain computed tomographic scanning
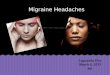
showed a homogeneous, well-defined, roundhyperdensity in the right frontoparietalregion consistent with an intracerebral he¬matoma (Fig 2, left). A right-sided internalcarotid arteriogram demonstrated an avas-cular mass in the right frontal lobe. Therewas beadlike narrowing of the extracranial
Accepted for publication April 24,1989.From the Montreal (Canada) Neurological Hos-
pital and Institute. Dr Cole is now with theDepartments ofNeurology and Neuroscience, TheJohns Hopkins University School of Medicine,Baltimore, Md.Reprint requests to Department of Neuro-
science, The Johns Hopkins University School ofMedicine, 725 N Wolfe St, Baltimore, MD 21205(Dr Cole).
Downloaded From: http://jamanetwork.com/ by a Harvard University User on 12/29/2016

Fig 1.—Case 1. Left, Normal brain computed tomographic scan with intravenous contrast infusion 2 days prior to intrace¬rebral hemorrhage. Center, Brain computed tomographic scan without contrast at time of admission showing large right-sidedfrontoparietal hematoma. Right, Right-sided internal carotid arteriogram showing focal spasm of initial segment of right middlecerebral artery.
portion of the right internal carotid artery(Fig 2, right), which was unchanged on twoseparate injections.Two days later, because of the suspicion
of underlying tumor, a right-sided frontalcraniotomy with evacuation of the hem¬atoma was performed. There was no patho¬logic evidence of tumor or of underlyingvascular abnormality. A subacute inflam¬matory infiltrate composed mainly of mac¬rophages was seen in the neuropil (Fig 3).There was some thickening of vessel wallswith increased cellularity and a mild lym-phocytic perivascular infiltrate.Case 3.—A 46-year-old woman with a 20-
year history of common migraine developeda right frontal throbbing headache associ¬ated with nausea and photophobia, whichwas similar to her usual attacks, but in¬creased progressively over several days.She was treated with analgesics that pro¬vided partial relief. Four days later, aftercontinued headache, she noted left face andarm weakness and numbness, and came tothe emergency department. Blood pressureand heart rate were normal. Carotid pulseswere full, but there was tenderness over theright carotid artery. She had right-gazepreference associated with a left hemipare¬sis involving the face and arm more thanthe leg and a left Babinski's sign. Computedtomographic scan showed a right-sidedfrontoparietal hematoma (Fig 4, left). Aselective digital right-sided carotid arterio¬gram demonstrated severe narrowing ofthe extracranial portion of the internal ca¬rotid artery (Fig 4, center). There was noevidence of arteriovenous malformation.Over the next 24 hours, severe right-sidedheadache persisted and was associated withtenderness over the scalp on the right side.She was discharged with residual left-sidedweakness, and continued to make a slow re¬covery. Three months later she underwenta repeated right-sided carotid arteriogramthat showed resolution of the narrowing
Fig 2.—Case 2. Left, Brain computed tomographic scan without contrast, showing large left-sidedfrontoparietal intracerebral hemorrhage. Right, Left internal carotid arteriogram showing spasm ofextracranial portion of internal carotid artery. Intracranial vessels are displaced by large avascu-lar mass.
that had been present on the first study (Fig4, right).
COMMENT
These patients all manifested a rel¬atively stereotyped pattern of head¬ache associated with intracerebralhemorrhage (Table). Two had commonmigraine and one suffered from classicmigraine. Suddenly, following typicalattacks, each suffered major lobar in¬tracerebral bleeding.A relationship between preexisting
migraine and intracerebral hemor-
rhage in each of these patients can
only be inferred. Intracerebral hemor¬rhage is most commonly associatedwith hypertension, aneurysmal bleed¬ing, rupture of macroscopic or crypticvascular malformations, tumor necro¬sis, primary vasculopathy, or, in popu¬lations at risk, amphetamine or co¬caine abuse. None of these conditionswas demonstrated by either the clin¬ical, artériographie, or pathologicstudies.The finding of tenderness over the
appropriate carotid artery was strik-
Downloaded From: http://jamanetwork.com/ by a Harvard University User on 12/29/2016

ing in two of the patients, and sug¬gested that carotid vessel pathologicfindings were important in the devel¬opment of intracerebral hemorrhage.Carotidynia has been associated withcarotid artery dissection, carotid ar¬
tery occlusion, carotid artery aneu¬
rysm, giant cell arteritis, and mi¬graine.10" None of our patients had avessel biopsy performed to rule outgiant cell arteritis, but normal sedi¬mentation rates argued against thisdiagnosis. There was no evidence ofocclusion or aneurysm in any of thesecases. Spontaneous carotid artery dis¬section, a diagnosis that might be sug-
gested by the artériographie findingsin case 3, remains a possibility in thatcase, but has typically been associatedwith ischemie stroke.12Brain computed tomographic scan¬
ning was highly suggestive of sponta¬neous hemorrhage in two patients, andin one case (case 2) suggested the pos¬sibility of underlying tumor. The im¬ages were not consistent with the di¬agnosis of hemorrhagic infarction inthat the hematomata were dense, wellcircumscribed, and did not show thepatchy hyperdensity usually associ¬ated with that condition. In one case(case 1), a computed tomographic scan,
Fig 3.—Case 2. Brain specimen from area adjacent to intracerebral hemorrhage showing suba¬cute inflammatory infiltrate. Arrows point to macrophages. Note perivascular lymphocytic infiltra¬tion (hematoxylin-eosin, X115).
Fig 4.—Case 3. Left, Brain computed tomographic scan without contrast showing right-sided frontoparietal intracerebralhemorrhage. Center, Digital angiogram showing extensive narrowing of extracranial portion of right internal carotid artery.Right, Right common carotid arteriogram 3 months later, showing resolution of spasm.
performed 2 days before the hemor¬rhage occurred, was entirely normal.There was no evidence of ischemia orof vascular malformation.All patients underwent artério¬
graphie studies of appropriate vessels.In each case there was evidence of sig¬nificant spasm of a major vessel sup¬plying the area in which hemorrhageoccurred. In the two patients with ca¬
rotidynia, spasm was apparent in theextracranial portion of the internalcarotid artery. In those patients thepossibility of catheter-induced spasmseemed unlikely in view of both itspersistence on repeated injections andthe existence of carotidynia prior tothe arteriogram. In the third patient,spasm was seen in the proximal seg¬ment of the middle cerebral artery.Subarachnoid hemorrhage, cerebral
trauma, central nervous system infec¬tion, drug abuse, toxemia, fibromuscu-lar dysplasia, carotid artery dissec¬tion, and cerebral vasculitis have allbeen associated with the radiographieappearance of spasm of the cerebralarteries. In the present cases, only thelatter three possibilities could be rea¬
sonably entertained.One patient (case 3) in whom the di¬
agnoses of fibromuscular dysplasia orcarotid artery dissection were consid¬ered underwent follow-up study 3months after intracerebral hemor¬rhage. At that time, spasm had com¬
pletely resolved, and the vascular ap¬pearance was normal. Follow-up an¬
giographie studies in fibromusculardysplasia have demonstrated eitherstable or progressive pathologic find¬ings, but resolution of that process hasnot been described1317 Carotid arterynarrowing due to dissection may dis-
Downloaded From: http://jamanetwork.com/ by a Harvard University User on 12/29/2016

Summary of Clinical Features
Characteristic
Cases
Age, y/sex 61/F 45/F 46/F
Type of migraine Classic Common CommonDuration ofheadache priorto intracerebralhemorrhage
24 h 4 d
Carotidynia Not noted ++++
Angiographiefindings
Spasm of middlecerebral artery
Spasm of internalcarotid artery
Spasm of internalcarotid artery
Pathologic findings Vessel wall necrosis Subacuteperivascularinflammation
Not available
appear over time, thus the diagnosisremains possible in the present case,although spontaneous hemorrhage re¬
sulting from dissection, as opposed tohemorrhagic infarction, has not previ¬ously been reported (to our knowl¬edge).12None of these patients had clinical
or serologie evidence of systemic vas-culitis. Recently, several reports havedescribed a condition known as acutebenign cerebral vasculitis character¬ized by the occurrence of transient fo¬cal neurological deficits, often associ¬ated with severe headache and mildabnormalities of the cerebrospinalfluid.1822 Angiography in those patientsdisclosed narrowing of multiple in-
tracranial and extracranial cerebralarteries, which largely improved whenrepeated examinations were doneweeks or months later. Serdaru et al22have described a patient in whom a bi¬opsy of the narrowing portion of a
temporal artery, as documented byangiography, was performed. Based onthe absence of inflammation, those au¬thors suggested that "benign cerebralvasculitis" may represent a vasospas-tic phenomenon related to an underly¬ing migrainous diathesis. Two suchpatients presented with intracerebralhemorrhage. While not described indetail in their article,18 those patientsresemble ours in their outline, and it islikely that the condition we have de-
scribed represents one extreme of thespectrum of "benign" cerebral vaso¬
spasm.A migrainous cause for the arterio-
graphically demonstrated spasm ofvessels, either extracranial or intra¬cranial, in each of the patients can onlybe suspected because of the similarityof each patient's prodromal symptomsto those associated with her typicalattacks. It is possible that intracere¬bral hemorrhage was the result oftemporary ischemia of vessel wallsfollowed by sudden reperfusion withsubsequent rupture of ischemie ves¬sels. An analogous process, as recentlysuggested by Caplan,23 may explain in¬tracerebral hemorrhage associatedwith toxemia,24 and has been suggestedto explain intracerebral hemorrhageassociated with sympathomimeticdrug abuse,25 trigeminal nerve stimu¬lation with resultant abrupt hyper¬tension,26 cold exposure,27 and carotidendarterectomy with subsequentreperfusion.28We wish to thank Dr D. Melancon for interpre¬
tation of neuroradiological studies, Dr Y. Ro-bitaille for interpretation of pathologic material,Drs A. Hakim and G. Francis for caring for twoof the patients, Drs A. Olivier and R. Leblanc forneurosurgical consultations, Dr F. Andermannfor reviewing the manuscript, and Dr L. Caplanfor helpful discussions and advice.
References
1. F\l=e'\r\l=e'\C. Contribution \l=a`\l'\l=e'\tudede la migraineophtalmique. Rev Med Paris. 1881;1:625-649.
2. Conner RC. Complicated migraine: a study ofpermanent neurological and visual defects causedby migraine. Lancet. 1962;2:1072-1075.
3. Wolff HG. Headache and Other Head Pain.2nd ed. New York, NY: Oxford University Press;1963:467-475.
4. Bradshaw P, Parsons M. Hemiplegic mi-graine: a clinical study. Q J Med. 1965;34:65-85.
5. Pearce JMS, Foster JB. An investigation ofcomplicated migraine. Neurology. 1965;15:333\x=req-\340.
6. Bartleson JD. Transient and persistent neu-rological manifestations of migraine. Stroke.1984;15:383-386.
7. Dunning HS. Intracranial and extracranialvascular accidents in migraine. Arch Neurol Psy-chiatry. 1942;48:396-406.
8. Lees F. The migrainous symptoms of cere-bral angiomata. J Neurol Neurosurg Psychiatry.1962;25:45-50.9. Troost BT, Mark LE, Maroon JC. Resolution
of classic migraine after removal of an occipitallobe AVM. Ann Neurol. 1979;5:199-201.
10. Raskin NH, Prusiner S. Carotidynia. Neu-rology. 1977;27:43-46.11. Chambers BR, Donnan GA, Riddell RJ,
Bladin PF. Carotidynia: aetiology, diagnosis andtreatment. Clin Exp Neurol. 1981;17:113-123.
12. Mokri B, Sundt TM Jr, Houser OW, Piep-gras DG. Spontaneous dissection of the cervicalinternal carotid artery. Ann Neurol. 1986;19:126\x=req-\138.
13. Galligioni F, Iraci G, Marin G. Fibromus-cular hyperplasia of the extracranial internal ca-rotid artery. J Neurosurg. 1971;34:647-651.
14. Osborn AG, Anderson RE. Angiographicspectrum of cervical and intracranial fibromus-cular dysplasia. Stroke. 1977;8:617-626.
15. So EL, Toole JF, Dalal P, Moody DM. Ceph-alic fibromuscular dysplasia in 32 patients. ArchNeurol. 1981;38:619-622.
16. Sandok BA. Fibromuscular dysplasia of theinternal carotid artery. Neurol Clin North Am.1983;1:17-26.
17. Yamamoto I, Kageyama N, Usui K, et al.Fibromuscular dysplasia of the internal carotidartery: unusual angiographic changes with pro-gression of clinical symptoms. Acta NeurochirWein. 1979;50:293-298.18. Rousseaux P, Scherpereel B, Bernard MH,
Guyot JF. Angiopathie c\l=e'\r\l=e'\braleaigu\l=e"\b\l=e'\nigne.Presse Med. 1983;12:2163-2168.
19. Michel D, Vial C, Antoine JC, et al. Angio-pathie c\l=e'\r\l=e'\bralaigu\l=e"\b\l=e'\nigne:quatre cas. Rev
Neurol Paris. 1985;141:786-792.20. Tabbaa MA, Snyder BD. Vasospasm versus
vasculitis in cases with 'isolated benign cerebralvasculitis.' Ann Neurol. 1987;21:109.
21. Snyder BD, McClelland RR. Isolated benigncerebral vasculitis. Arch Neurol. 1978;35:612-614.22. Serdaru M, Chiras J, Cujas M, Lhermitte F.
Isolated benign cerebral vasculitis or migrainousvasospasm? J Neurol Neurosurg Psychiatry.1984;47:73-76.23. Caplan L. Intracerebral hemorrhage revis-
ited. Neurology. 1988;38:624-627.24. Will AD, Lewis KL, Hinshaw DB, et al. Ce-
rebral vasoconstriction in toxemia. Neurology.1987;37:1555-1557.25. Harrington H, Heller A, Dawson D, et al.
Intracerebral hemorrhage and oral amphet\x=req-\amines. Arch Neurol. 1983;40:503-507.26. Barbas N, Caplan L, Baquis G, et al. Dental
chair intracerebral hemorrhage. Neurology.1987;37:511-512.27. Caplan LR, Neely S, Gorelick PB. Cold\x=req-\
related intracerebral hemorrhage. Arch Neurol.1984;41:227.28. CaplanL, Skillman J, Ojemann R, Fields W.
Intracerebral hemorrhage following carotid end\x=req-\arterectomy: a hypertensive complication. Stroke.1978;9:457-460.
Downloaded From: http://jamanetwork.com/ by a Harvard University User on 12/29/2016
























![Coronary Vasospasm [electronic resource]: signs, symptoms, risk](https://img.pdfslide.us/doc/110x75/6203841bda24ad121e4a5297/coronary-vasospasm-electronic-resource-signs-symptoms-risk.jpg)

