Embed Size (px)
Citation preview
American Journal of Medical Genetics 25251-255 (1986)
Midtrimester Sonographic Diagnosis of Mandibulof acial Dysostosis
James P. Crane and Heidi A. Beaver
Washington University School of Medicine, Genetics Division, Department of Obstetrics and Gynecology, St. Louis, Missouri
Two fetuses at risk for mandibulofacial dysostosis (MFD) were monitored sono- graphically during the midtrimester of pregnancy. Normal facial and auricular structure were identified in one fetus, and a healthy infant was subsequently delivered. Severe microtia and micrognathia were apparent in the second fetus and a diagnosis of MFD was made and confirmed at delivery. These observations indicate that midtrimester sonographic diagnosis of severe MFD is possible.
Key words: mandibulofacial dysostosis, prenatal diagnosis, ultrasound
INTRODUCTION
Mandibulofacial dysostosis (MFD or Treacher Collins syndrome) is an autoso- mal dominant disorder characterized by malformations of the eyes, ears, maxilla, and mandible. Manifestations include downward obliquity of the palpebral fissures, lower eyelid coloboma, malar hypoplasia, and micrognathia with secondary malocclusion. The external ear is frequently hypoplastic or absent. Auricular tags, conductive hearing loss, and defects of the middle and inner ear may also be observed.
Midtrimester sonographic findings and prenatal diagnosis of MFD in two “at- risk” pregnancies are reported.
CLINICAL REPORT
Sonographic studies were conducted using an ADR 4000 SLC real-time scanner with 3.5mHz linear and 3.0mHz medium-focus sector transducers.
Received for publication August 20, 1985; revision received December 20, 1985.
Address reprint requests to James P. Crane, M.D., Genetics Division Department of Obstetrics and Gynecology, Jewish Hospital at Washington University, 216 S. Kingshighway, St. Louis, MO 63110.
0 1986 Alan R. Liss, Inc.
252 Crane and Beaver
Fig. 1. Father of affected infant in Case 1.
Case 1
S.H. and her husband were referred for genetic evaluation during her first pregnancy because her husband had facial anomalies and congenital hearing loss. Mr. H. was a 26-year-old self-employed handyman. Physical examination showed MFD with right anotia, left microtia with stenosis of the auditory canal, malar hypoplasia, marked antimongoloid obliquity of the palpebral fissures, and severe micrognathia (Fig. 1). The family history was consistent with autosomal domimant inheritance with variable expressivity .
Mr. and Mrs. H. were counseled that they had a 50% risk for MFD and told that prenatal diagnosis of this disorder had not been previously reported. The possi- bility of antenatal diagnosis using high-resolution sonography to detect severe micro- gnathia and microtia was discussed. The prospective parents requested that this be attempted.
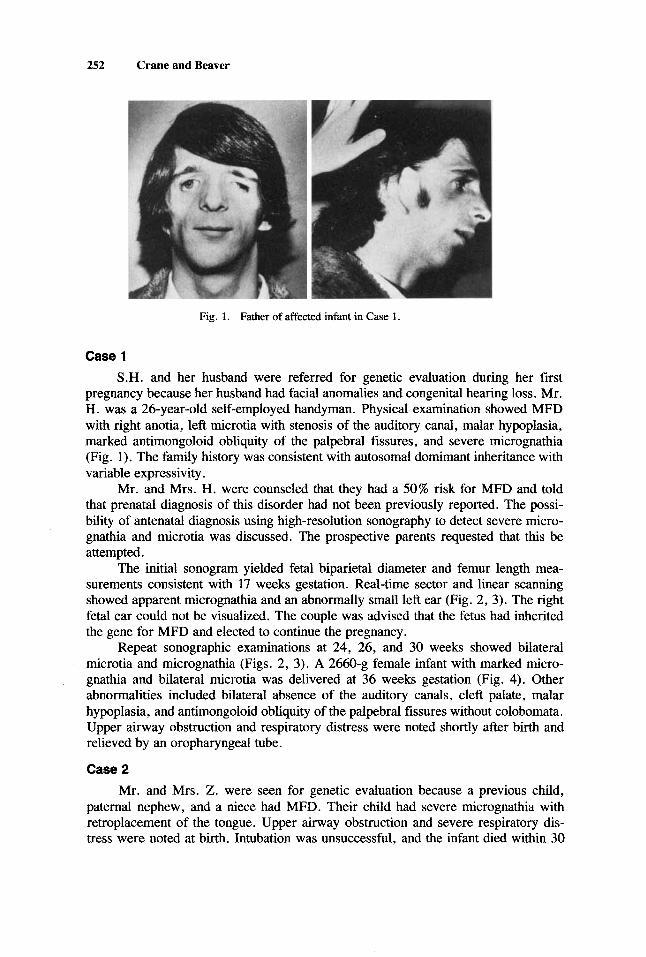
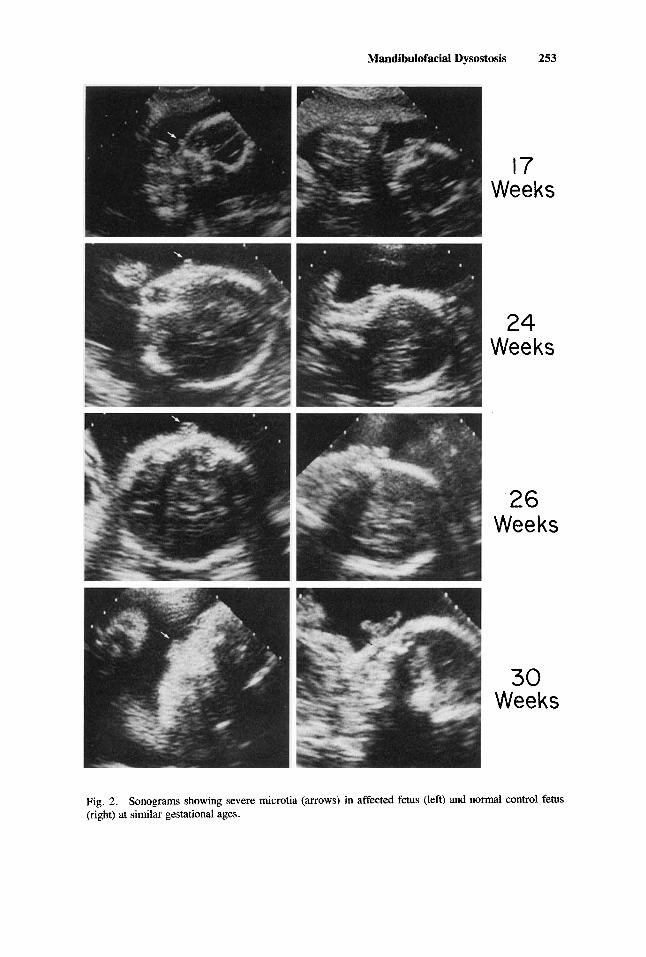
The initial sonogram yielded fetal biparietal diameter and femur length mea- surements consistent with 17 weeks gestation. Real-time sector and linear scanning showed apparent micrognathia and an abnormally small left ear (Fig. 2, 3). The right fetal ear could not be visualized. The couple was advised that the fetus had inherited the gene for MFD and elected to continue the pregnancy.
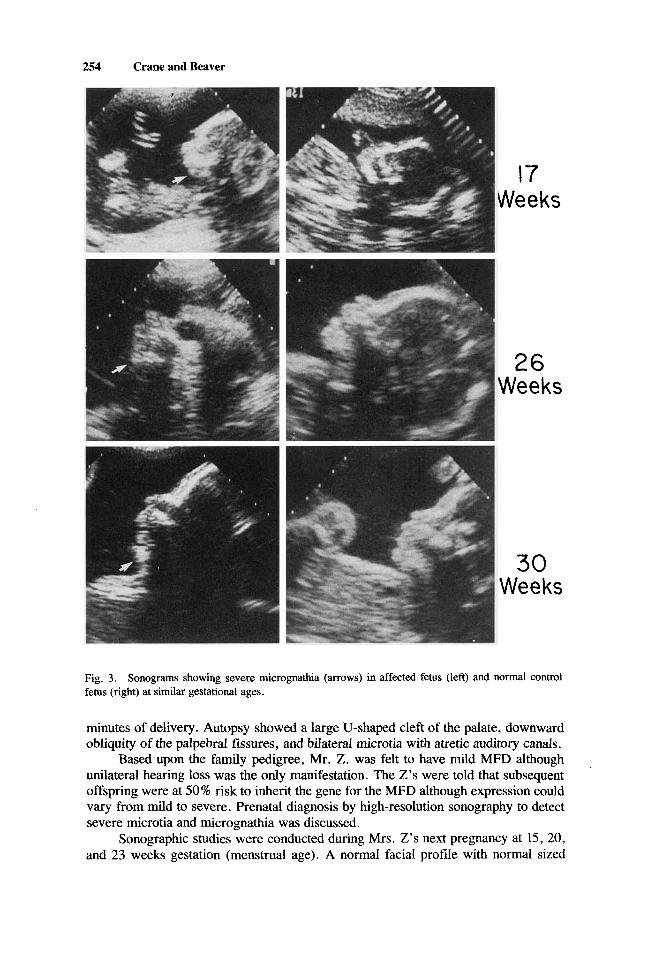
Repeat sonographic examinations at 24, 26, and 30 weeks showed bilateral microtia and micrognathia (Figs. 2, 3). A 2660-g female infant with marked micro- gnathia and bilateral microtia was delivered at 36 weeks gestation (Fig. 4). Other abnormalities included bilateral absence of the auditory canals, cleft palate, malar hypoplasia, and antimongoloid obliquity of the palpebral fissures without colobomata. Upper airway obstruction and respiratory distress were noted shortly after birth and relieved by an oropharyngeal tube.
Case 2 Mr. and Mrs. Z . were seen for genetic evaluation because a previous child,
paternal nephew, and a niece had MFD. Their child had severe micrognathia with retroplacement of the tongue. Upper airway obstruction and severe respiratory dis- tress were noted at birth. Intubation was unsuccessful, and the infant died within 30
Mandibulofacial Dysostosis 253
1-7 Weeks
24 Weeks
26 Weeks
30 Weeks
Fig. 2. (right) at similar gestational ages.
Sonograms showing severe microtia (arrows) in affected fetus (left) and normal control fetus
254 Crane and Beaver
17 Weeks
26 Weeks
30 Weeks
Fig. 3. Sonograms showing severe micrognathia (arrows) in affected fetus (left) and normal control fetus (right) at similar gestational ages.
minutes of delivery. Autopsy showed a large U-shaped cleft of the palate, downward obliquity of the palpebral fissures, and bilateral microtia with atretic auditory canals.
Based upon the family pedigree, Mr. Z. was felt to have mild MFD although unilateral hearing loss was the only manifestation. The Z’s were told that subsequent offspring were at 50% risk to inherit the gene for the MFD although expression could vary from mild to severe. Prenatal diagnosis by high-resolution sonography to detect severe microtia and micrognathia was discussed.
Sonographic studies were conducted during Mrs. Z’s next pregnancy at 15, 20, and 23 weeks gestation (menstrual age). A normal facial profde with normal sized
Mandibulofacial Dysostosis 255
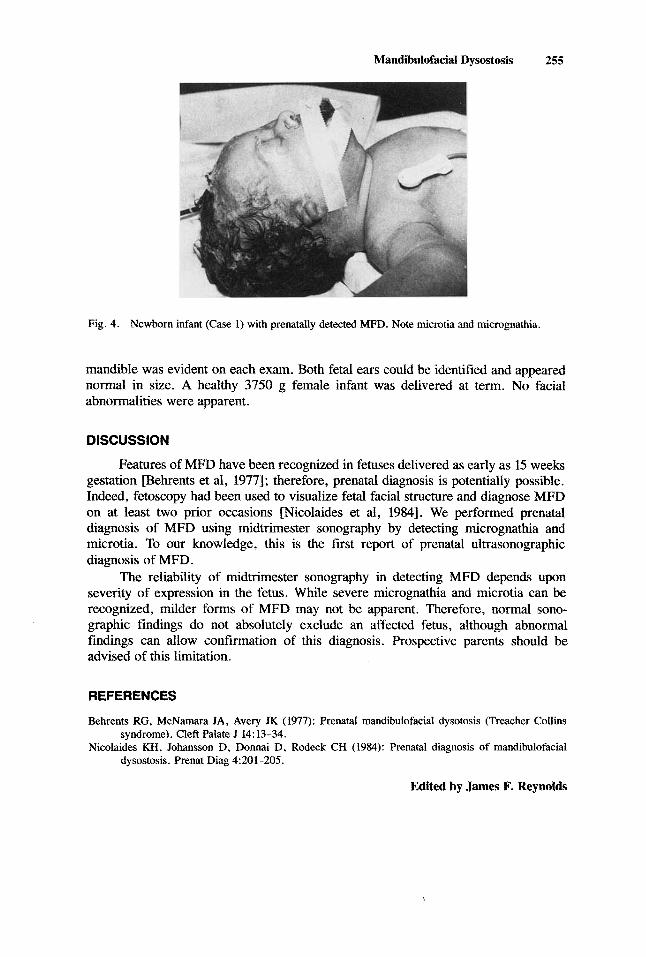
Fig. 4. Newborn infant (Case 1) with prenatally detected MFD. Note microtia and micrognathia.
mandible was evident on each exam. Both fetal ears could be identified and appeared normal in size. A healthy 3750 g female infant was delivered at term. No facial abnormalities were apparent.
DISCUSSION
Features of MFD have been recognized in fetuses delivered as early as 15 weeks gestation Pehrents et al, 19771; therefore? prenatal diagnosis is potentially possible. Indeed, fetoscopy had been used to visualize fetal facial structure and diagnose MFD on at least two prior occasions [Nicolaides et al, 19841. We performed prenatal diagnosis of MFD using midtrimester sonography by detecting micrognathia and microtia. To our knowledge? this is the first report of prenatal ultrasonographic diagnosis of MFD.
The reliability of midtrimester sonography in detecting MFD depends upon severity of expression in the fetus. While severe micrognathia and microtia can be recognized, milder forms of MFD may not be apparent. Therefore, normal sono- graphic findings do not absolutely exclude an affected fetus, although abnormal findings can allow confirmation of this diagnosis. Prospective parents should be advised of this limitation.
REFERENCES
Behrents RG, McNamara JA, Avery JK (1977): Prenatal mandibulofacial dysotosis (Treacher Collins
Nicolaides KH, Johansson D, Donnai D, Rodeck CH (1984): Prenatal diagnosis of mandibulofacial syndrome). Cleft Palate J 14:13-34.
dysostosis. Prenat Diag 4:201-205.
Edited by James F. Reynolds















![[2015.114] Sonographic Imaging of Scrotal Emergencies Including](https://img.pdfslide.us/doc/110x75/58831cd31a28abaf198ba6de/2015114-sonographic-imaging-of-scrotal-emergencies-including-.jpg)











