Embed Size (px)
Citation preview

ContentsNATIONAL PRIORITIES-------------------------------------------------------------------------------------------------3CANCER SERVICES------------------------------------------------------------------------------------------------------3CARDIAC SERVICES---------------------------------------------------------------------------------------------------------8ELECTIVES SERVICES------------------------------------------------------------------------------------------------------12MENTAL HEALTH AND ADDICTIONS-------------------------------------------------------------------------------------15RHEUMATIC FEVER--------------------------------------------------------------------------------------------------------17STROKE SERVICES---------------------------------------------------------------------------------------------------------18
VULNERABLE SERVICES----------------------------------------------------------------------------------------------20MIDLAND MATERNITY ACTION GROUP---------------------------------------------------------------------------------20HEALTH OF OLDER PEOPLE ACTION GROUP----------------------------------------------------------------------------22RADIOLOGY NETWORK---------------------------------------------------------------------------------------------------23RENAL ACTION GROUP---------------------------------------------------------------------------------------------------26
REGIONAL ACTIVITIES------------------------------------------------------------------------------------------------29CHILD HEALTH ACTION GROUP------------------------------------------------------------------------------------------29MIDLAND REGIONAL EMERGENCY DEPARTMENTS---------------------------------------------------------------------30MIDLAND REGIONAL TRAUMA SYSTEM---------------------------------------------------------------------------------32SMOKEFREE NETWORK---------------------------------------------------------------------------------------------------33
KEY ENABLERS---------------------------------------------------------------------------------------------------------37MAORI HEALTH…………………………………………………………………………………………………………………………43WORKFORCE DEVELOPMENT PLAN--------------------------------------------------------------------------------------54INFORMATION SERVICES-------------------------------------------------------------------------------------------------58
2013/14 MEASURES - NATIONAL PRIORITY SERVICES------------------------------------------------------42CANCER NETWORK – 2013/14-----------------------------------------------------------------------------------------42CARDIAC NETWORK ------------------------------------------------------------------------------------------------------44ELECTIVE SERVICES--------------------------------------------------------------------------------------------------------48STROKE NETWORK--------------------------------------------------------------------------------------------------------50CHILD HEALTH ACTION GROUP------------------------------------------------------------------------------------------51RHEUMATIC FEVER--------------------------------------------------------------------------------------------------------52
2013/14 MEASURES – VULNERABLE SERVICES---------------------------------------------------------------59MATERNITY ACTION GROUP---------------------------------------------------------------------------------------------59RENAL ACTION GROUP---------------------------------------------------------------------------------------------------60HEALTH OF THE OLDER PERSON ACTION GROUP----------------------------------------------------------------------71RADIOLOGY NETWORK---------------------------------------------------------------------------------------------------71
2013/14 MEASURES - REGIONAL ACTIVITIES------------------------------------------------------------------76SMOKEFREE NETWORK---------------------------------------------------------------------------------------------------76MIDLAND REGIONAL TRAUMA SYSTEM---------------------------------------------------------------------------------76REGIONAL EMERGENCY DEPARTMENTS---------------------------------------------------------------------------------77
2013-14 Regional Services Plan – Midland Region DHBs 1
Quarter 4 Progress Report

2013-14 Regional Services Plan – Midland Region DHBs 2

An important note for the reader: The colour assessments are an indication of progress against agreed actions in the 2013/14 Regional Services Plan to strengthen and improve health services. Therefore conclusions about the quality, safety and effectiveness of health services provided by Midland cannot be made from assessments made in this report.Overall Status G Report Date: 18 July 2014
General Commentary:
The format uses an exception reporting basis to provide an explanation when an action that was agreed to be achieved in the quarter is not on track. Data and measures that relate to each area are provided in the back of the report (refer to the Table of Contents for easy access).
Regional networks and action groups are the fora that the DHBs in the Midland region use to lead service development initiatives A major focus of Q3 has been the development of the 2014/15 Regional Services Plan ensuring that there is a high level of engagement for the plan at all levels and line
of sight with other DHB planning documents. This has presented capacity challenges for regional groups and Project Managers. In addition, a Project Manager vacancy has required cross cover by the regional Analyst and this has meant that the ability to provide the extent of data for the Q3 report has been constrained. The Q4 report will provide an up to date report.
Risks identified in the Q2 progress report are being progressed, with the majority becoming part of the draft 2014/15 RSP.
AREAS OF FOCUS National Priorities
Gove
rnan
ce
Qua
lity
& S
afet
y
Serv
ice
Deliv
ery
Rese
arch
&
Enab
lers
/ S
uppo
rt
Ove
rall
Asse
ssm
ent Vulnerable Services
Gove
rnan
ce
Qua
lity
& S
afet
y
Serv
ice
Deliv
ery
Rese
arch
&
Enab
lers
/ S
uppo
rt
Ove
rall
Asse
ssm
ent Regional Priorities
Gove
rnan
ce
Qua
lity
& S
afet
y
Serv
ice
Deliv
ery
Rese
arch
&
Enab
lers
/ S
uppo
rt
Ove
rall
Asse
ssm
ent
Cardiac Services G G G G R G Maternity Services G G C R G Child Health G G G R G
Elective Services G C G G G G Health of Older People G G G A G Emergency Departments G G G C G G
Mental Health & Addictions G G G G G G Radiology Services G A G G A G Smokefree G G A G C G
Stroke Services G G G G A G Renal Services G A G G R G Trauma System G R G
Workforce A
Information Systems G
Cancer
Faster Cancer Treatment Implementation Plan A Tairawhiti Cancer Service Transition Plan C NZ Lung Cancer G
Cancer MDM development G Hei Pa Harakeke Action Plan 2012-14 G NZ Breast Cancer C
Cancer Care Coordination C Midland Bowel Cancer / Colonoscopy A Midland Lung Cancer G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 3

Midland Radiation Oncology G Midland Medical Oncology C Midland Palliative Care G
Midlands HRC Research C
Electives: Key contract milestones, timeframe and overarching key performance indicators (KPI)
G 1 The completion of a regional pathway for an orthopaedic procedure with documentation of a patient taking this pathway by 30 September 2013
G 2 The completion of a regional pathway for a plastics procedure with documentation of a patient taking this pathway by 31 December 2013
G 3 The completion of a regional pathway for an Ophthalmology procedure with documentation of a patient taking this pathway by 31 December 2013
G KPI 1 To demonstrate a reduction in waiting times across project services; 80 percent of patients are meeting the four month targets (ESPI 2 and 5) for the Midland region by 30 June 2014
G KPI 2 To identify total availability of resource (theatre capacity, bed capacity, staffing resource and outpatient capacity) across the Midland region relating to project areas and demonstrate an improving trend in the utilisation of that available resource by 30 June 2014
G KPI 3 To demonstrate a declining trend in hospital led cancelations by utilising regional availability and planning models by 30 June 2014 (compared to baseline information for 2011/12)
G KPI 4 To increase the number of patients that have followed a new pathway as a result of this project
NATIONAL PRIORITIES
Cancer Services Midland Cancer Network: Clinical Director, Dr Humphrey Pullon; Manager, Jan Smith
Key highlights – Qtr. 4
Medical Oncology - Midland Medical Oncology service change work between Bay of Plenty and Waikato has been completed. Bay of Plenty will have an increase of 0.5fte SMO effective 14/7/14, which will mean all BOP FSA and follow-ups will be managed at BOP. However due to Waikato SMO resignation the service change will be effective 1/4/14.
Radiation Oncology - BOP/Waikato radiation oncology transition project – start date confirmed 1/10/14. Scope of service defined with PUC volumes agreed, and progress continues on tumour specific pathways and service linkages. KKC recruiting staff. Sub-group formed to agree individual patient transition plan between 1/7/14 and 1/10/14.
Tairawhiti Adult Cancer Model of Service has been updated, finalised and sent to relevant TDH and Waikato DHB staff. Faster Cancer Treatment - Waikato FCT database under development but progress delayed due to slow access to resources required. Manual data
collection from cancer nurse tracker has recently been incorporated into database. Q3 reporting still planned to be done from new database but timeframes very tight. Midland Cancer Network analysts are now responsible for regional FCT database management and reporting on behalf of Bay of Plenty, Lakes and Waikato DHBs. Following data consolidation, treatment data related to Tairawhiti patients is forwarded to Tairawhiti cancer nurse tracker just prior to Q2 reporting date. Midland Q2 FCT data returned from Ministry of Health, analysed and report circulated to Midland Cancer Network Executive Group and key stakeholders. There are still significant gaps in data reported. Lakes DHB investigating why there were so few indicator 1 and 2 records reported. Midland members of the national FCT EAG contributed to updated FCT data definitions: face to face meeting in January, and further meetings via VC and teleconference. Final version released 7 March and circulated to stakeholders. Effective for reporting 1 July but DHBs encouraged to implement earlier as those reported with first treatment in July will need to be reported according to the new definitions. 62 day indicator to become health target sometime in 2014-15.
Ministry of Health FCT one-off RFP – The Network facilitated a regional response to Ministry of Health RFP for one off funding to support implementation of the national tumour standards and/or working towards achievement of the 62 day wait time with service improvements initiatives. Midland RFP initiatives submitted were valued at $1,065,409. Ministry of Health response to RFP due mid-April.
Regional Tumour Standard Review – Midland lung cancer self-assessments and review of data in progress. Regional Lung Cancer Working Group to review
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 4

findings in May and finalise regional report completed June 2014. National Lung Cancer work programme – Draft concept paper for Ministry of Health endorsed by Working Group on Early Detection of Lung Cancer, plan to
seek feedback from regional cancer networks. Terms of reference and work plan endorsed. Midland Cancer Network undertook review of draft national lung cancer dataset against national standards and monitoring criteria. Developing questions to test the pilot lung cancer dataset. Drafted MDM prioritisation criteria. Agreed process to undertake review and update of the National Lung Cancer Standards (2011) due for completion in 2015.
Midland MDM - Improved VC connectivity following BOPDHB video conferencing services moving from proof of concept into production and with implementation of Dimension Data managed services in the regional space. Significant improvement with connectivity to MDM endpoints on Gen-i and with Lakes MDM. Myeloma MDM now regularly scheduled. Lakes Breast MDM: Waikato medical and radiation oncologists plus a surgeon now videoconference into this MDM and are able to view PACS and pathology. Tairawhiti MDM endpoint: work underway with Gen-i and TDH IS to upgrade this endpoint to two 55” monitors. Current codec currently only supports one 27” monitor and is not able to support two monitors. Information regarding video conferencing for MDMs supplied to KKC. MDMs regularly video conferenced include Chest Conference, GI Oncology and Lakes Breast.
Midland Lung Cancer - Lung cancer database: Updating the lung cancer database using the Chest conference proforma. The data that loads up into the database from the Chest conference proforma just populates 50% of the fields in the database, the remaining 60% needs to be updated manually by CNS.
Midland colonoscopy - Midland COOs have prioritised Waikato will lead implementation of ProVation (endoscopy reporting system) with regional platform in 2014/15.
Midland Cancer Network provided contribution to the National Office of the Cancer Society of NZ in the development of their recently published Haepapatanga ki te Māori - responsiveness to Māori plan.
Risks / major challenges for noting
Faster Cancer Treatment - Continued delay in the development of the Waikato FCT database – current reporting relies on use of ad hoc scripts and data is incomplete. Waikato FCT database development now to commence in January 2014. Waikato FCT reporting is affecting Midland DHBs reporting as Waikato is the key regional DHB of service.
Midland FCT data quality, by itself, is not yet sufficient to reliably inform service improvements. Regional tumour standard reviews - Challenge to organise DHB work groups including clinicians to review lung tumour standards and access to meaningful
data to support review. Midland Kia Ora E Te Iwi (KOETI) programmes - securing sustainable funding. Commenced implementation of variation to the Waikato DHB chronic disease
whānau ora contracts. Contractual agreement to deliver 3 community cancer education forums within a 12 month period per provider. Currently these contracts are only within Waikato. Equity Manager to meet with Midland DHB P&F to discuss further contract variations.
Midland Radiation Oncology Service - Kathleen Kilgour Cancer (Bay of Plenty DHB) has indicated that there is a delayed start date, now 1 October 2014; this has the potential impact on the region radiation oncology capacity and timeliness of access. Balancing the demand for services combined with resource constraints is difficult. Project work group meets fortnightly to work through requirements.
Midland lung cancer - Waikato is closely monitoring access and timeliness to thoracic surgery for lung cancer cases. Midland medical oncology SMO workforce is vulnerable with a recent Waikato medical oncologist resignation. Issue with service change when shift in
patient flow between DHBs but revenue doesn’t match demand costs for providers creating tensions. Midland palliative care service planning progress delayed – due to Midland Cancer Network needing to prioritise workload and undertake PIR of Waikato
palliative care specialist palliative care new model of service. Midland gynae-onc – Auckland DHB and Waikato DHB initial discussion about potential service change in patient flow to follow the national advice submitted
to Ministry of Health. There are numerous issues to be worked through. Midland Cancer Network increasing workload with no additional funding to baseline contract since 2007. MCN Executive has prioritised areas of importance
for the region.
What we said we would do in Quarter 4.
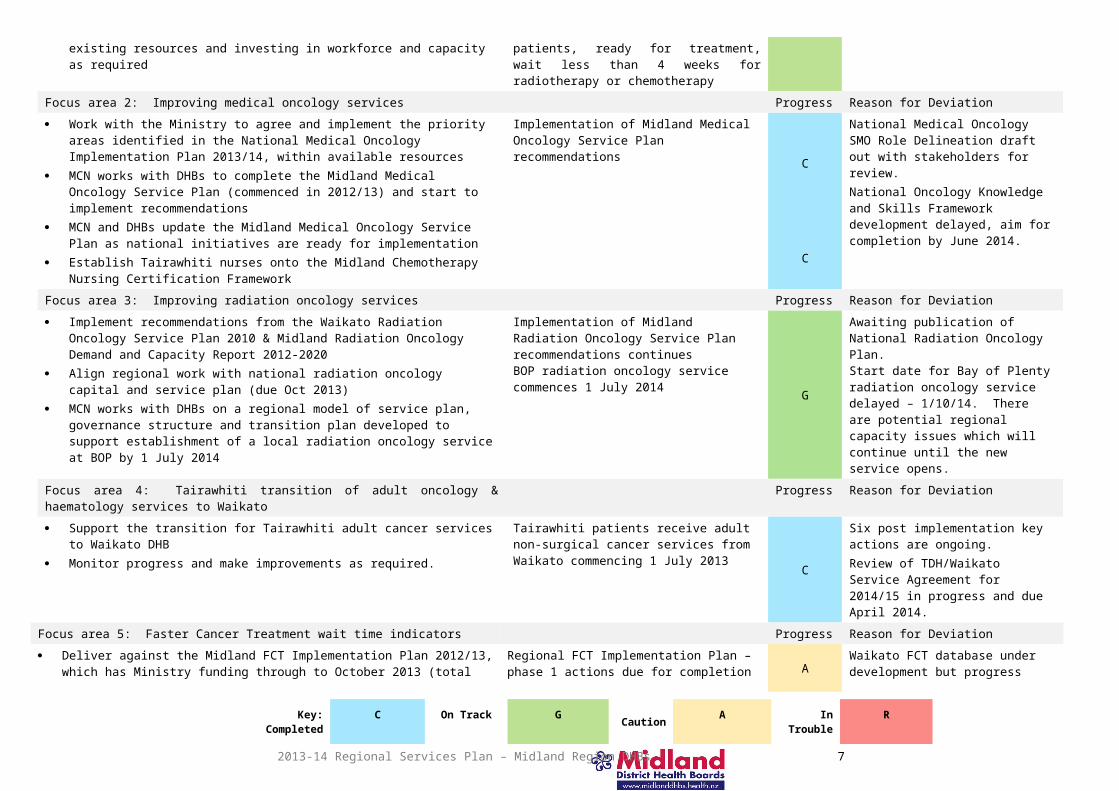
Focus area 1: Shorter waits for cancer treatment Measured by Progress Reason for Deviation Sustain performance against the radiotherapy and chemotherapy wait time
targets by more efficient use of existing resources and investing in workforce and capacity as required
DHB cancer centres report cancer treatment target monthly: All patients, ready for treatment, wait less than 4 weeks for
G Refer to Cancer Centre DHB reports
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 5

radiotherapy or chemotherapyFocus area 2: Improving medical oncology services Progress Reason for Deviation Work with the Ministry to agree and implement the priority areas identified in the
National Medical Oncology Implementation Plan 2013/14, within available resources
MCN works with DHBs to complete the Midland Medical Oncology Service Plan (commenced in 2012/13) and start to implement recommendations
MCN and DHBs update the Midland Medical Oncology Service Plan as national initiatives are ready for implementation
Establish Tairawhiti nurses onto the Midland Chemotherapy Nursing Certification Framework
Implementation of Midland Medical Oncology Service Plan recommendations
C
C
National Medical Oncology SMO Role Delineation draft out with stakeholders for review.National Oncology Knowledge and Skills Framework development delayed, aim for completion by June 2014.
Focus area 3: Improving radiation oncology services Progress Reason for Deviation Implement recommendations from the Waikato Radiation Oncology Service Plan
2010 & Midland Radiation Oncology Demand and Capacity Report 2012-2020 Align regional work with national radiation oncology capital and service plan (due
Oct 2013) MCN works with DHBs on a regional model of service plan, governance structure
and transition plan developed to support establishment of a local radiation oncology service at BOP by 1 July 2014
Implementation of Midland Radiation Oncology Service Plan recommendations continues BOP radiation oncology service commences 1 July 2014
G
Awaiting publication of National Radiation Oncology Plan.Start date for Bay of Plenty radiation oncology service delayed – 1/10/14. There are potential regional capacity issues which will continue until the new service opens.
Focus area 4: Tairawhiti transition of adult oncology & haematology services to Waikato
Progress Reason for Deviation
Support the transition for Tairawhiti adult cancer services to Waikato DHB Monitor progress and make improvements as required.
Tairawhiti patients receive adult non-surgical cancer services from Waikato commencing 1 July 2013 C
Six post implementation key actions are ongoing.Review of TDH/Waikato Service Agreement for 2014/15 in progress and due April 2014.
Focus area 5: Faster Cancer Treatment wait time indicators Progress Reason for Deviation Deliver against the Midland FCT Implementation Plan 2012/13, which has
Ministry funding through to October 2013 (total MoH funding $360k over 2012-13 & 2013/14).
Establishment of baseline data and reporting mechanisms for Faster Cancer Treatment indicators with Midland DHBs
Identify and implement actions to improve faster cancer treatment data collection systems to support service improvements along the cancer patient pathway
Focus on the front end of the process in primary care identification of high suspicion of cancer, diagnosis / decision to treat and first treatment
Support FCT trackers to map data collection points and transition to multidisciplinary team by December 2013
Midland Faster Cancer Treatment Implementation Plan is revised, updated and monitored
FCT data collection service improvements are identified, prioritised, implemented and monitored.
Begin implementing regional clinical data repositories for cancer. Scope paper to
Regional FCT Implementation Plan – phase 1 actions due for completion by end December 2013 % of patients (by DHB and ethnicity)
referred urgently with a high suspicion of cancer who receives their first cancer treatment (or other management) within 62 days
% of patients (by DHB and ethnicity) referred urgently with a high suspicion of cancer who have their first specialist assessment within 14 days
% of patients (by DHB and ethnicity) with a confirmed diagnosis of cancer who receive their first cancer treatment (or other management) within 31 days of decision-to-treat.
A Waikato FCT database under development but progress delayed due to slow access to resources required. Baseline data still in development. DHB FCT database development still in progress. Data quality and improvements still work in progress.Ministry of Health released changes and updated FCT data definitions and business rules for implementation from 1/7/14.Reporting to be monthly rather than quarterly from 1/7/14.
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 6
inform stakeholders what is the purpose, requirements and implications. Focus area 6: Faster Cancer Treatment – implement national tumour standards Measured by Progress Reason for DeviationBegin to implement the national tumour stream standards of service provision Lung developed 2011-12
Continue regional early detection for lung cancer programme within available resources
Bowel, breast, gynae, head and neck, malignant haematology, melanoma, sarcoma and upper GI developed 2012-13
Support new national tumour standard development as required. MCN work with DHBs to audit one of the tumour standards per annum. Midland breast cancer stock take of services and audit against national breast
cancer standards is completed and regional work plan by 30 June 2014 DHBs begin implementing the national tumour standards of service provision –
annual priorities identified and actions planned to address gaps Develop Midland gynae-oncology model of service and plan, informed by
national standards and national plan Support national five yearly review and update of three national standards - to be
phased from 2015/16 Implement priorities identified in the national Prostate Cancer Quality
Improvement Plan (note regional implications are unknown at this point in time). Continue supporting the Midlands Prostate Cancer Study.
Midland lung cancer improvement plan recommendations continue to be implemented and monitored
An audit of one of the tumour standards of service provision is completed by June each year
Findings from the audit are incorporated into an improvement plan is developed for tumour stream as required
Incorporate research findings into next year’s planning
G
G
Challenge to organise large number of DHB stakeholders review lung tumour standards preliminary findings. Data not complete.
Provided regional feedback to the National Gynae oncology working group who provided advice to the Ministry of Health on the number of cancer centre hubs.
Midlands Metastatic Prostate Cancer Research presentation to Midland Hei pa Harakeke work group and Ministry of Health Cancer Team.
Focus area 7: Faster Cancer Treatment – cancer nurse coordination Progress Reason for Deviation DHBs support implementation and development of DHB cancer nurse CNS
coordinator roles including participation in the national evaluation process Enable and support cancer nurse coordinators attendance at national and regional
training and mentoring forums Promote implementation of 2013 updated Midland psycho-oncology tool
Monitor and contribute to the national evaluation of the implementation of the 2012/13 Midland DHB nurse care coordination roles
Midland psycho-oncology tool implementation continues
C
Completed and on-going, refer to DHB reports.BOP DHB cancer coordinator –recruitment to recent vacancies in progress.
Focus area 8: Faster Cancer Treatment – improving multidisciplinary meetings Progress Reason for Deviation MCN support implementation of the Midland MDM work plan deliverables that
work towards compliance with the National MDM guidance and improve the functionality and coverage of multidisciplinary meetings (MDMs) across the region
Midland MDM Action Plan is reviewed and updated, recommendations implemented with DHB quarterly reporting on progress.
MCN reports the percentage of lung and bowel cancer patients reviewed at MDM by DHB and by ethnicity (reported six monthly to Cancer Programme Steering Group)
DHBs report PP24 - progress delivering improved cancer multidisciplinary meetings based on the actions agreed in the 2012/13 annual plans and additional actions using the funding for MDMs including variance in expenditure to allocated DHB MDMs funds Target: Funding MDMs for all main cancer tumour types and increasing the number of cases discussed
G
G
Six monthly report provided to MCN Executive.Monthly reporting continues with regional overview.
Focus area 9: Improving wait times for diagnostics – endoscopy and colonoscopy Progress Reason for Deviation
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 7

Support the implementation of the national Endoscopy Quality Improvement (EQI) programmeBOP DHB is the lead for the operational base for the national EQI team and programme
DHBs work with national EQI team to implement Global Rating Scale Lakes DHB continue with GRS and share learnings with region. Improve access and waiting times for diagnostic services – colonoscopy Establishment of baseline colonoscopy data 2013/14. MCN and DHBs will
review colonoscopy systems and processes related to reporting wait time indicators, develop an improvement plan as required with the aim to achieve the wait time targets
The national referral criteria for direct access to outpatient colonoscopy implemented within Midland DHBs
National EQI leads implement Global Rating Scale (GRS) into Midland DHBs by 30 June 2014 (tbc)
DHBs responsible for reporting the following DV2 indicators:
Diagnostic Colonoscopy: 50% of people accepted for an urgent
diagnostic colonoscopy receive their procedure within two weeks (14 days)
50% of people accepted for a diagnostic colonoscopy received their procedure within six week (42 days)
Surveillance colonoscopy 50% of people accepted for a surveillance
colonoscopy receive their procedure within twelve weeks (84 days) of the planned date.
A
Refer to DHBs progress reporting on colonoscopy wait time.Refer to Waikato and Bay of Plenty DHBs reporting and progress against colonoscopy wait times and planned service improvement initiatives.
Focus area 10: Improved palliative care services Progress Reason for Deviation MCN facilitate development of Midland Palliative Care Service Plan utilising
national Resource and Capability Framework Support standardisation of agreed clinical/service documents within Midland e.g.
clinical guidelines, Hospice access criteria, referral guidelines Continue to facilitate implementation of Liverpool Care Pathway - completed Continue to develop Midland palliative care education framework with a particular
focus on improving primary palliative care capability As required, support national process to develop specialist palliative care service
specifications and support DHB implementation as they come available Support regional ACP as required (Midland RTH link). MCN facilitate completion of Waikato Palliative Service Plan Complete implementation of change to model of service for adult specialist
palliative care in Waikato (conclude implementation project and hand back to business as usual) - completed
Support development of information/literature for Waikato palliative care services BOP & Lakes continue to implement palliative care service plans Support Tairawhiti palliative care model of service change and incorporate into
regional initiatives.
Midland Palliative Care Service Plan developed and implementation commenced
Midland standard documents produced Report annually providers’ progress with
implementation of the LCP Waikato Palliative Care Service Plan
completed and implementation commenced
Service improvement initiatives and implementation continues with the regional and local DHB palliative care service plans.
G
C
G
C
G
Delayed due to reprioritisation of workload. Also undertaking post implementation review of Waikato new specialist palliative care model of service. Regional Palliative Care Working Group scheduled for May.
Focus area 11: Reduce the impact & inequalities of cancer on Midland Māori Progress Reason for Deviation Continue regional Kaitiaki reference group for Midlands Prostate Cancer Study
research - completed Midland builds capacity and capability to
run local Māori health provider E te Iwi programme.
C KOETI programmes within Midland continue. Finding funding from within the sector delays progress.
Continue to facilitate Midland MHP in the E Te Iwi programme Continue to support Midland breast screening initiatives to increase Māori
participation.
G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 8

Focus area 12: National lung cancer work programme Progress Reason for Deviation Midland Cancer Network will lead and facilitate the National Cancer Lung Cancer
Working Group and work programme Two national meetings per annum G National Lung Cancer Contract
Agreement signed 19/11/13
Focus area 13: System integration & service collaboration Progress Reason for Deviation MCN supports the network collaborative work groups to progress their individual
work plans MCN continues to engage with and support clinical leaders across the cancer
programme areas to lead and contribute to identified projects.
MCN reports quarterly on work group collaboration progress
Clinical engagement evident across regional projects
G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 9

What we did in Quarter 4, in addition to what we said we would do. The reason/s for undertaking this activity Qtr 3 – The Network facilitated a regional response to Ministry of Health RFP for one off funding to
support implementation of the national tumour standards and/or working towards achievement of the 62 day wait time with service improvements initiatives. Midland RFP initiatives submitted were valued at $1,065,409. Ministry of Health response to RFP due mid-April.
One off funding to support working towards implementation of national tumour standards and/or service improvements that support achievement of the 62 wait time indicator.
Qtr 3 – Auckland DHB approached Waikato and Midland Cancer Network initial regarding gynae oncology patient flow service change
Service change impacting on patient pathways and regions revenue flow.
Cardiac Services Midland Cardiac Clinical Network Chair: Dr Gerry Devlin, Clinical Unit Leader Cardiology, Waikato Hospital
Key highlights Philippa Edwards was appointed as Project Manager for the network. Steady progress with Map of Medicine and Bay Navigator groups to ensure local pathway development aligns with regional work programmes and service delivery The draft patient information brochure will go for approval at the next Cardiac Network meeting on 30th July Primary Risk Factor management (S7). MOH results show none of the Midland DHBs is meeting the national target of 90%. However, all 5 Midland DHBs have improved
in this quarter. The national average having moved up 5% from the last quarter to 78.2% and the Midland region lifted to 80.9%, 2nd place and remaining above the national average. Work continues.
ACS targets - The region has met the 3 day acute angiogram target of > 70% with notably delivery of services to Lakes increasing from 53% to 83%. Work continues on how to balance ACS flow across the region and achieve the target for each DHB.
The target of >95% of patients presenting with Acute Coronary Syndrome who undergo coronary angiography having completion of ANZACS QI ACS and Cath/PCI registry data collection within 30 days has climbed from 85% to 88.4%, and 95% is achieved within 60days.
SIR reports available to Mar 2014 show the Midland Region achieves the Cardiac Surgery target, leading the regions at 6.95 per 10,000. However, Angiograms and angioplasty are below target and the 2014/15 plans are being prepared to address this through a data informed production planning approach that will identify opportunities for improved demand-capacity matching
The 4 Regional Cardiac Network project managers met with the National Clinical lead Gerry Devlin to align their 14/15 work programs with the national direction and to share successful initiatives across the regions.
Midland region is the only region with a working definition of High Risk Chest pain. On advice from the Maori health teams at Lakes and Waikato DHBs, Midland have formally requested to trial the Mauriora “Foundation Course in Cultural Competency –
Online” as a tool to raise the level of cultural competency, across a wide range of cardiac health professionals across the Midland region.Risks / major challenges
ANZACS-QI 95% data completion compliance is uneven across the region (see target 1.2). This is improving slowly. While the other 4 DHBs have managed to effectively resource this Waikato has their Clinical Research Centre completing this work and so far are unable to achieve the target. Work continues with key stakeholders to work through mitigation strategies to improve these results
The development of a Midland Regional Cardiac Services Plan has not begun and has been carried forward to the 14.15 work programme. Previous versions in Word have been located as a base document.
Cardiac Surgery: After a significant effort by the surgical unit Midland are on track to achieve a target of 700 patients this year. Target 3.3: Data completion in Dendrite was not met as WDHB have not installed the Dendrite data base. Cardiac surgergy waitlist now under control. Workforce. An appointment of a Midland Workforce Analyst has been made and a meeting set up for July to initiate data collection and methodology discussions to
identify future workforce demand.
What we said we would do in Quarter 4.
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 10

Governance Deliverable Timeframe Progress Reason for Deviation/Comment
G1 Regular meetings and workshops to continue to develop the MCCN
Liaise and inform other key project groups such as the National Cardiac Network and other Regional networks (as appropriate)
Progress the agreed network priorities as outlined in the Regional RSP work programme, including linking with the Midlands Rheumatic Fever work programme
Clinical leadership across the continuum of care contributing to service delivery, (not limited to the national targets) whilst ensuring sustainability and longevity of the group
Bi-monthly meetings or workshops (either face to face, or videoconferencing and/or teleconferencing in conjunction with web conference technology)
G
Quality and Safety Deliverable Timeframe Progress Reason for Deviation/Comment
Q1 ACS Including National and regional targets
1. To continue to develop, implement and review regional strategies to ensure prompt local risk stratification of suspected ACS patients and the transfer of high risk patients to the tertiary centre for angiography and revascularisation
2. Completion of ACS Project report on key milestones and gains for distribution to MCCN
Review and audit: Q2 2013
Midland ACS Project Completion Q3 2014
C
C
3. National reporting continues (via ANZACS-QI), using established measures (ACS Target 1.1).
4. ANZACS-QI: completion compliance is maintained across the region (see target 1.2 )
5. ANZACS-QI: completion compliance is maintained across the region (see target 1.3)
Quarterly reporting G
See Risks/Major challenges section for comment
G
A
Q2 ACS Clinical Pathway development The Midland Clinical forum continue review and refine the Midland Region ACS pathway from primary to tertiary care for management of patients with suspected ACS
Q3 Annually
G
Service Delivery Deliverable Timeframe Progress Reason for Deviation/Comment
S1 Service delivery planning 1. Any impacts are minuted and reviewed by the MCCN group
2. Action plan to be implemented if required3. Ensure service delivery is tailored to the needs of
the high risk population groups (such as: Maori)
Review and discuss at each MCCN meeting
G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 11

S2 Review 2006 plan. Benchmark against current and proposed future state. Develop plan and included initiatives into 14/15 regional work plan update and implement changes to the Cardiac Services Plan for the Midland Region
Review Q3 2014 Implement started Q4 2015
G
S3 Revascularisation.National targets for elective and acute revascularisation are met
1. National targets for elective and acute revascularisation are met. (as per measure 2.2)
2. Quality initiatives and work programme (in collaboration with regional DHB’s) are developed to address any regional inconsistency regional and inequity of access and outcomes
3. National agreed scoring tools are used to support prioritisation and decision making
4. Compliance is reviewed quarterly by the MCCN and any corrective action plans implemented to address issues
Captured and report regional monthly via the MCCN
Develop work programme: Q2 2013
G
G
G
G
S4 Cardiac SurgeryEnsure equity in access to and delivery of cardiac surgery targets met
Ensure equity in access to and delivery of cardiac surgery target met:1. as per measure 3.12. as per measure 3.23. as per measure 3.3
Quarterly reporting
A
See Risk/Major Challenges section for comment
S5 Cardiac care is integrated across the continuum (Primary/Secondary Care) –
Pathway Development
1. Align with current local pathway development initiatives (eg: Map of Medicine)
2. Prioritise further pathway development.3. Two regionally agreed cardiac clinical pathways
developed and implemented
6 regional pathways to be developed (with Primary and Secondary input) Q4 2016 G
S6 Cardiac care is integrated across the continuum (Primary/Secondary Care)
4. Review current state, including national and local initiatives and align with regional strategy for developing a work programme.
5. Ensure planning of work programmes will include Maori Health, Primary and Secondary Care and Public Health stakeholders
Review and prioritise Q4 2014
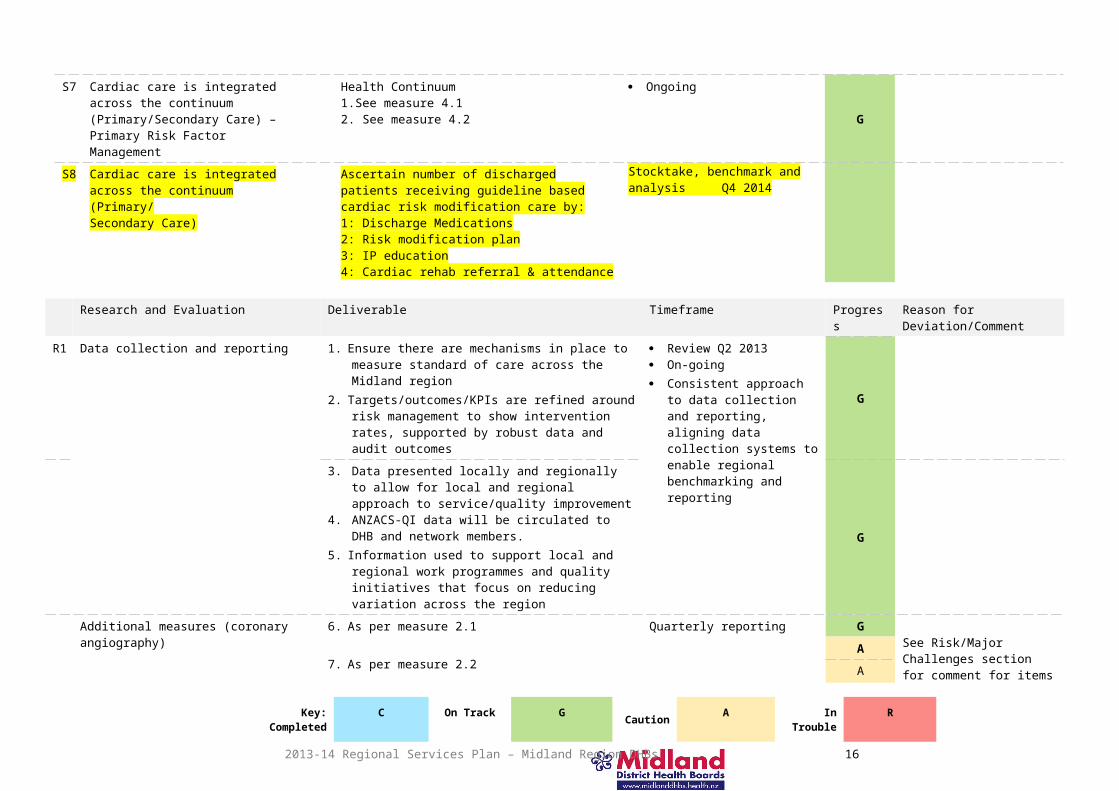
S7 Cardiac care is integrated across the continuum (Primary/Secondary Care) – Primary Risk Factor Management
Health Continuum1.See measure 4.12. See measure 4.2
OngoingG
S8 Cardiac care is integrated across the continuum (Primary/Secondary Care)
Ascertain number of discharged patients receiving guideline based cardiac risk modification care by:1: Discharge Medications2: Risk modification plan3: IP education4: Cardiac rehab referral & attendance
Stocktake, benchmark and analysis Q4 2014
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 12

Research and Evaluation Deliverable Timeframe Progress Reason for Deviation/Comment
R1 Data collection and reporting 1. Ensure there are mechanisms in place to measure standard of care across the Midland region
2. Targets/outcomes/KPIs are refined around risk management to show intervention rates, supported by robust data and audit outcomes
Review Q2 2013 On-going Consistent approach to data
collection and reporting, aligning data collection systems to enable regional benchmarking and reporting
G
3. Data presented locally and regionally to allow for local and regional approach to service/quality improvement
4. ANZACS-QI data will be circulated to DHB and network members.
5. Information used to support local and regional work programmes and quality initiatives that focus on reducing variation across the region
G
Additional measures (coronary angiography)
6. As per measure 2.1
7. As per measure 2.2
8. As per measure 2.3
Quarterly reporting GSee Risk/Major Challenges section for comment for items 7 (2.1) and 8 (2.2)
A
A
Enablers/Support Deliverable Timeframe Progress Reason for Deviation/Comment
E1 Workforce and Training.
All programme initiatives to be led by the MRTN Leadership group, in conjunction with the MCCN and the MRWFD team
Head count to service current population vs workforce to deliver the key objectives
Areas of shortage are identified Trends in cardiac workforce numbers, distribution and
forecasting are analysed by regional workforce (benchmarked against demand)
Q2 2013
Q2 2013
Q4 2014
R
See Risk section for comment
E2 Utility of existing workforce model critiqued against workforce forecasting
Options for innovative nursing and technical models explored including: Nurse Practitioner, GP/Practice Nurse, Physiologists, MRTs
Q4 2014
R
See Risk/Major Challenges section for comment
E3 Robust understanding of workforce issues and identification of workforce needs for the future including training programmes
Q2 2013 R
See Risk section for comment
E4 Supporting integration and linkages with DHB Māori Health Plans
Develop an e-learning cultural competency programme (with a cardiac care focus) which will be designed to be utilised in primary and secondary health care arenas
June 2014
R
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 13

E5 Capital Stocktake of current and future capital intentions for each DHB.
Gain regional agreement on all major capital projects Work cooperatively in alignment with the regional
procurement strategy.
Stocktake Q2 2013 Review Q4 2014 Ongoing C
E6 Information Technology (I.T)All local programme initiatives are in conjunction with the MRIS Leadership group and liaison and integration with the Regional Information Services (IS) team
Regional e-referral (secondary to tertiary)
Development, agreement and uptake of a shared regional cardiac pathway repository (eg: Midland Navigator or similar)
Development Q2 2013 Roll out Q4 2014 Ongoing Q4 2016
GOutside scope of MCCN:Part of Midland MOM project
E7 Stocktake and prioritise referral requirements Agreement of shared e-referral cardiac (with
supported clinical pathways and access criteria) across primary, secondary, and tertiary services.
Development of e-referral template.
Stocktake Q2 2013 Agreement and
Development
Q4 2014
G
Out of scope of MCCN: Awaiting a regional I.T patient management system solution
E8 I.T(shared e-learning portal)
Consolidation and prioritisation of education activities in association with primary care, public health agencies and MRWFD/MRTN across the region with regard to cardiac education packages
Work programme developed (in conjunction with all key stakeholders) breaking work into projects based on priority
Stock take, review and prioritise
Timeline dependent on development and agreement by the Midland region HR groups
Work done in alignment with the MRWFD and MRTN
G
Out of scope of MCCN:Part of Midland e-learning strategy
E9 I.T (Shared regional electronic clinical workstation)
The MCCN is to ensure involvement in the development and roll out of an agreed regional electronic clinical workstation and data repository
Timeline dependent on all Midland region DHBs affordability and implementation of the Regional ISP
GOut of scope of MCCN:Part of Midland IS solution
What we did in Quarter 4, in addition to what we said we would do. The reason/s for undertaking this activity Priority for MCCN was the review and development of the 2014/15 Cardiac Work programme Part of 14/15 Regional Service Planning
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 14

Electives Services Clinical Chair: Dr Martin Thomas, Chief Medical Officer, Lakes DHBKey highlights
1. Additional patient transfers continue around the region towards ESPI compliance with regular discussions occurring at the regional action group.2. Regional card access being trailed to reduce barriers for clinicians to work between multiple campuses.3. Cataract pathway continues to show positive results - summary of benefits attained was collected at the beginning of this year (trial ended on the 31/12/13). Details showed
large benefits some of which have likely come from work towards ESPI compliance. To make sure results are realistic and replicable data will continue to be collected until mid-year and then will be re-analysed.
4. Ophthalmology group has decided to trial a new group structure. Paper attached on group structural learning’s – overall current progress is positive.5. Auckland DHB avastin process around Nurses providing avastin treatment continues with other workforce approaches also being reviewed by the ophthalmology group.6. Patient satisfaction surveys have been collected with 256 analysable surveys received.
a. Overall results have been very positive; areas requested for improvement by patients included: Clearer information and understanding of the pre and post-surgical process – currently being worked on through the Map of Medicine pathways additional
focus will be now included in this process around discharge information as requested by patients Better connections between hospital and community care – currently being worked on through the Map of Medicine pathways.
7. A regional Chronic Pain service and how clinicians can move between DHBs is currently under discussion due to the effect on the service when a clinician goes on holiday or leaves.
8. Management of Opioid use for non-cancer pain under discussion between Mental Health and the regional Chronic Pain group draft guidelines to be established by June.9. Focus of five additional pathways for chronic pain CRIPS, Headaches, abdominal pain, lower back pain and endometriosis by the end of July.10. ACC attended the regional Chronic Pain group meeting to provide an update on national approaches from an ACC perspective and discuss ways to provide additional
education material to ACC staff to reduce workload on clinicians and inappropriate referrals. Access to Map of Medicine to be discussed.11. Regional Education program for chronic pain currently being discussed which is being based off the Taranaki pain education program as directed by the regional Chronic
Pain network.12. Referral Guidelines to Starship hospital for Chronic Pain patients currently being finalised for patients that meet the criteria. Meeting to be arranged for June with regional
Paediatric chair and Starship.13. Alternative processes and the possibility of a trial of new pathways for funding Chronic Pain patients (for an education program) to be reviewed over the next few months with
further discussions planned for June. 14. National meeting for all regional electives groups shared learning’s happening on 28th of March at the Ministry of Health – a range of learning’s and documents are being
circulated and meeting will become a quarterly event.15. First regional clinicians who are willing to move between DHBs have been discussed with regional HR. Additional progress planned for this year – regional access cards will
also aid in allowing smooth movement of these staff between campuses. Updates regularly provided to the Action Group chair.
Risks / major challenges
1. Tokoroa patients continue to be seen by Lakes for Orthopedics – a slight delay in expected volumes to date has occurred due to a delay in recruitment2. Production planning models have been more complicated than initially planned. They have been segmented into three sections and additional input has been provided by
DHBs to aid in progressing these models – regional models for most aspects have been trailed with success and will be presented to staff recommended by the action group on the 2/5/14.
3. The governance and action groups have provided additional feedback on Vascular with a meeting occurring in June.4. Orthopaedics clinical attendance reduced they will be trialling the Ophthalmology clinical workstream structure to attempt to rectify this (noted by the group that there is a lot
of work happening in the Orthopaedic space with MoH ERAS and other national work) following work programs will take into account other national work around this
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 15
specialty.
What we said we would do in Quarter 4.Governance Deliverable Timeframe Progres
sReason for Deviation
G1 To lead elective services activity on behalf of Midland DHBs
To provide clinical governance, accountability and decision making for elective services
Increased access, and equity of access, and reduced waiting times for elective services
Regional pathways developed with consistent systems and processes
The elective services group will meet at least quarterly throughout the project
The clinical working groups will meet at least monthly or bi-monthly depending on the work schedule
G
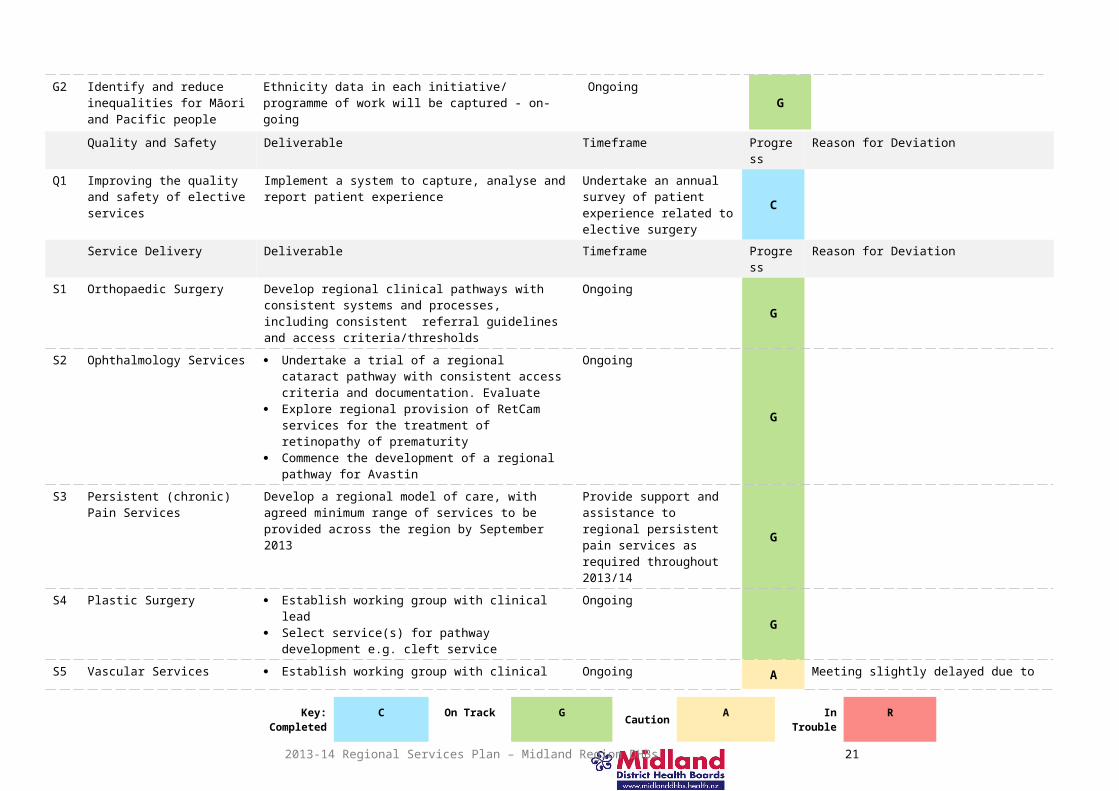
G2 Identify and reduce inequalities for Māori and Pacific people
Ethnicity data in each initiative/ programme of work will be captured - on-going
OngoingG
Quality and Safety Deliverable Timeframe Progress Reason for DeviationQ1 Improving the quality and
safety of elective services Implement a system to capture, analyse and report patient experience
Undertake an annual survey of patient experience related to elective surgery
C
Service Delivery Deliverable Timeframe Progress Reason for DeviationS1 Orthopaedic Surgery Develop regional clinical pathways with consistent
systems and processes, including consistent referral guidelines and access criteria/thresholds
Ongoing G
S2 Ophthalmology Services Undertake a trial of a regional cataract pathway with consistent access criteria and documentation. Evaluate
Explore regional provision of RetCam services for the treatment of retinopathy of prematurity
Commence the development of a regional pathway for Avastin
Ongoing
G
S3 Persistent (chronic) Pain Services
Develop a regional model of care, with agreed minimum range of services to be provided across the region by September 2013
Provide support and assistance to regional persistent pain services as required throughout 2013/14
G
S4 Plastic Surgery Establish working group with clinical lead Select service(s) for pathway development e.g. cleft
service
OngoingG
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 16

S5 Vascular Services Establish working group with clinical lead by July 2013
Consider the development of a regional vascular services with single managed/monitored waiting list
Ongoing
AMeeting slightly delayed due to leave. Meeting is now set for June.
S6 Bariatric Surgery Develop and implement a regional plan for bariatric services by November 2013
July 2013 and ongoing C
Research and Evaluation Deliverable Timeframe Progress Reason for DeviationR1 Evaluate service changes that
have resulted from the elective services project
Evaluate the regional cataract pathway On-goingG
Enablers/support Deliverable Timeframe Progress Reason for DeviationE1 Information Systems Regional production plan available on shared web-
based siteJuly 2013 and on-going
AShared visibility of production across regional DHBs is not available in current IS systems.
E2 Workforce planning and forecasting for future service requirements
A system in place for capturing up-to-date specialist capacity for each DHB and the region as a whole
Regional planning to capture workforce constraints and shortages, with the view of sharing resources where practicable
July 2013 and on-going
G
E3 Data definitions Data definitions agreed July 2013 and on-going G Added to separate from possible IS delay. On-track work on-going as data issues arise
E4 Regional production plan Visibility of production across the region July 2013 and on-going
G
Added to separate from possible IS delay. All DHBs have visibility of production within their own DHB and ability to discuss production is available around the region. However, direct IS visibility is not currently possible regionally.
What we did in Quarter 4, in addition to what we said we would do. The reason/s for undertaking this activity Regional Card access Clinicians had trouble at times moving between campuses as part of regional work as DHB cards
did not allow access to multiple DHB sites (E.G Waikato and Lakes hospitals). We have worked with regional security and found that cards can be programmed to remove this issue a document will be circulated outlining the possible process before the end of April.
Avastin Pricing Discussions continue around Avastin are being explored working with the Ministry of Health, Regional Ophthalmology clinical network with oversight of the Action group chair. The change is looking at possible changes to regulations regarding the distribution of pre-loaded syringes which would improve regional equity and provide savings.
Regular discussions around out of scope resource movements Following the discussions around Scopes and Orthopedics the regional Action Group now regularly discusses pressure areas for all DHB specialties and how resource may be able to be
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 17

moved to help. This is a quick discussion at the beginning of these meetings and has been seen as a valuable use of time as everyone is already together.
ACC involvement with Chronic Pain ACC is currently doing a large review. As part of this we have begun to work together in the area of Chronic Pain pathways using the Map of Medicine Pathways. It is seen that this will make the Map of Medicine pathways more clinically relevant and save clinicians time going between ACC information and hospital information. This will also aid ACC in making sure forms and documents reflect the clinical realities. This work is closely overseen by the Action Group chair and has the possibility of improving ACC funding by having it better follow best practice care.
Mental Health and Addictions Chair: Professor Graham Mellsop, Midland MH&A Clinical GovernanceKey highlights Midland Maori MH&A 2 day Summit held in the quarter. 120 people from across the region attended Day 1 and 98 attended Day 2. Evaluation report to be
completed. Two additional Clinical Networks established and sponsored by Clinical Governance. The Inpatient Care Network and the Duly Authorised Officers Network held
meetings in the quarter. Both were well attended. The establishment of the MH&A Clinical Workstation project commenced in the quarter. A Clinical Steering Group established involving all 5 Midland DHBs,
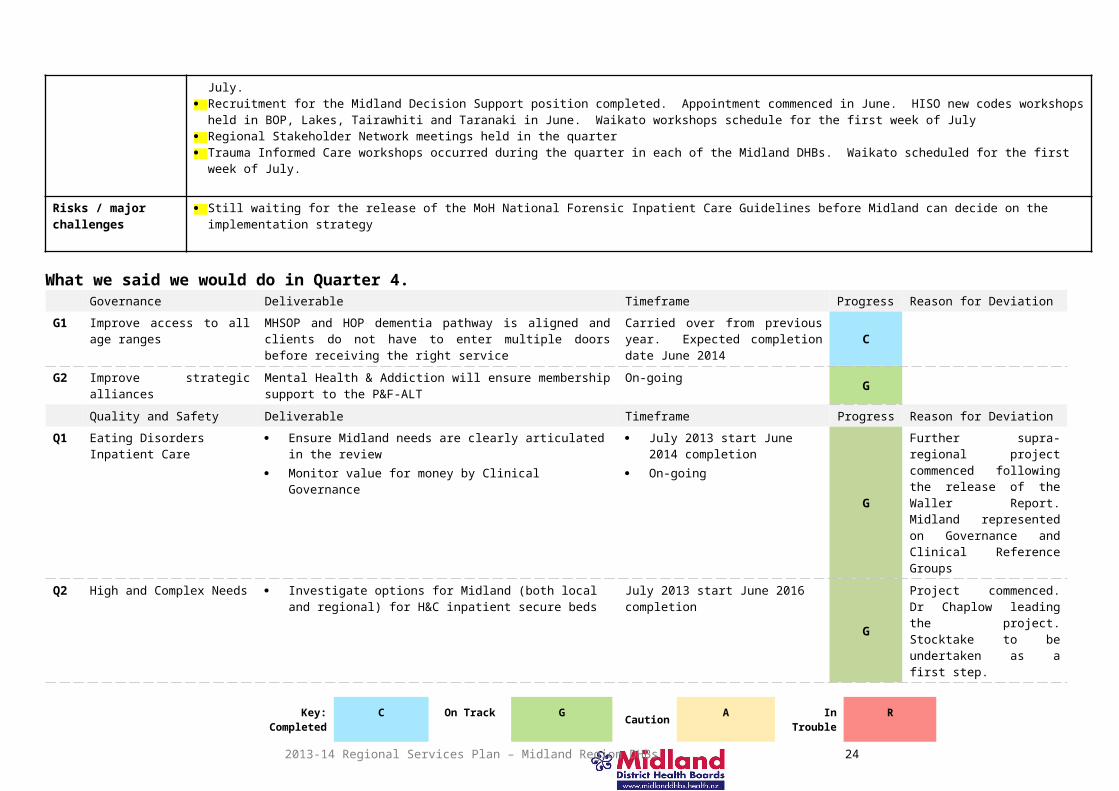
HealthShare, Ministry of Health and Canterbury DHB. First meeting schedule in July. Recruitment for the Midland Decision Support position completed. Appointment commenced in June. HISO new codes workshops held in BOP, Lakes, Tairawhiti
and Taranaki in June. Waikato workshops schedule for the first week of July Regional Stakeholder Network meetings held in the quarter Trauma Informed Care workshops occurred during the quarter in each of the Midland DHBs. Waikato scheduled for the first week of July.
Risks / major challenges
Still waiting for the release of the MoH National Forensic Inpatient Care Guidelines before Midland can decide on the implementation strategy
What we said we would do in Quarter 4.Governance Deliverable Timeframe Progress Reason for Deviation
G1 Improve access to all age ranges
MHSOP and HOP dementia pathway is aligned and clients do not have to enter multiple doors before receiving the right service
Carried over from previous year. Expected completion date June 2014 C
G2 Improve strategic alliances Mental Health & Addiction will ensure membership support to the P&F-ALT
On-going G
Quality and Safety Deliverable Timeframe Progress Reason for DeviationQ1 Eating Disorders Inpatient
Care Ensure Midland needs are clearly articulated in the review Monitor value for money by Clinical Governance
July 2013 start June 2014 completion
On-goingG
Further supra-regional project commenced following the release of the Waller Report. Midland represented on Governance and Clinical Reference Groups
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 18

Q2 High and Complex Needs Investigate options for Midland (both local and regional) for H&C inpatient secure beds
July 2013 start June 2016 completion G
Project commenced. Dr Chaplow leading the project. Stocktake to be undertaken as a first step.
Q3 Forensic Inpatient Care Align to and ensure participation in the national forensic network for inpatient beds
Recommendations are prioritised and implemented
July 2013 start June 2014 completion
July 2013 start June 2016 completion
A
Still awaiting the development of the National Guidelines. Timeframes will be amended for the 14/15 RSP Workplan
Service Delivery Deliverable Timeframe Progress Reason for DeviationS1 Youth Forensic
Implementation MoH funding is utilised as prioritised by the MoH Implement Youth Forensic Pathway recommendations Implement Youth Forensic Model of Care
July 2013 start June 2016 completedC
S2 Perinatal / Maternal Mental Health & Addiction (MoH)
Develop project scope and key stakeholders Undertake project stock take with agreed model of care
July 2013 start, June 2015 completedPhase One: Focus on the secondary service continuum
C
Phase Two: Include primary, well child and whānau ora providers
G
Phase II Final Draft report completed and to be circulated to stakeholder group for final consultation. One off Perinatal workforce funding secured, implementation plan to be developed.
Research and Evaluation Deliverable Timeframe Progress Reason for Deviation
R1 MH&A regional data management
Support continues to be provided to the NGO sector and expanded to include larger NGOs
NGOs are re-mapped to include new codes Clinical Governance identifies the Midland position Develop a process to undertake the benchmarking
July 2013 start June 2016 completed
G
HISO workshops for NGOs rolled out this quarter.
Clinical Workstation project commenced. Steering Group established. Objective identified in 14/15 RSP Workplan.
Enablers / Support Deliverable Timeframe Progress Reason for Deviation
E1 Regional Workforce Development(Midland)
A clear regional picture is obtained re the Midland workforce demands
Workforce priorities are established annually Workforce initiatives are aligned to national drivers
July 2013 start June 2016 complete C Midland MH&A Workforce Stocktake completed. All 5 DHBs completed. 70% of Midland NGOs completed. Date to be collated by Te
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 19

Pou.
E2 Mental Health and addiction strategic development (Midland)
Specialty groups provide strategic directions for the service and feed into national direction and drivers
July 2013 – June 2014C
What we did in Quarter 4, in addition to what we said we would do. The reason/s for undertaking this activity
10 Scholarships offered across Midland to attend the 2 day Supervision workshop held in Rotorua
To increase the pool of clinical Supervisors available in each of the Midland DHBs
Administrative support provided to national Nga Hau e Wha Consumer Advisory group to the MoH. Meeting held in November.
Contracted to provide administrative support by the MoH
Rheumatic Fever Interim Chair: Andrew Campbell-Stokes (HealthShare)Key highlight A teleconference was held in February which was well attended. From discussion it became clear that there were lots of potential areas to work together regionally, but
no consensus on what. A decision was made to shape a challenging Agenda and meet as a region after the Ministry had attended an international meeting, so that international best practice can be shared. A date has yet to be set, likely to be late May or early June. A focus of the meeting will be on eradicating RF in Maori children
Risks / major challenges
None identified
What we said we would do in Quarter 4 (NB: some actions are on-going with a deliverable date of 30 June 2014).Governance Deliverable Timeframe Progress Reason for Deviation
G1 A Regional advisory group will be developed
The group made up of DHB Champions will meet at least twice a year Six-monthly A
Quality and Safety Deliverable Timeframe Progress Reason for DeviationQ1 Regional collaboration Process agreed for ensuring:
Active follow up Appropriate referral to services Sharing of data held on registers
June 2014A
Quality and Safety Deliverable Timeframe Progress Reason for DeviationS1 Focus on clinical integration of rheumatic
fever services Clear Rheumatic fever care pathways are agreed Links to appropriate regional networks are established:
o Cardiac, Public, Maternity, Child Health, Oral Health
June 2014A
S2 Improve hand hygiene in schools Agreed hand-washing facilities and education standards/protocols are in place in facilities across the region
June 2014 A
Research and Evaluation Deliverable Timeframe Progress Reason for DeviationR1 Link in to national initiatives to support
service developmentNational initiatives are integrated in to local/regional service development activities e.g. housing and education
June 2014 A
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 20
Enablers/support Deliverable Timeframe Progress Reason for DeviationE1 Workforce development Education programmes in place in all DHBs.
Education programmes implemented where new technologies or protocols are developed e.g. rapid testing
June 2014A
Stroke Services Clinical Chair: Dr Peter Wright, Neurologist, Waikato DHBKey highlightsTo review
The TIA, thrombolysis and stroke care pathways have been designated a clinical lead to develop for use across the region. All DHBs now have local editors for Map of Medicine to assist with this work.Lakes DHB will commence a thrombolysis service from 1 June 2014.There are strong links with the national leadership groups. National discussion that the Midland Network is contributing to includes on-going work on coding and data collection for audit purposes.A national calendar of stroke education is updated three monthly and shared across the region’s clinicians.The education resources and focus of community based education stock take has been completed by the Stroke Foundation. This will be available for consideration by the Midland network in the near future. Significant work occurring around Maori health key worker education, specifically; looking at the Cancer Society education/resources for Maori health organisations and considering if this could be picked up as a model by the stroke foundation. An education tool for indigenous peoples has been sourced from Australia and is being considered by Maori health representatives from the Network and Stroke Foundation.The Network is working with ambulance services to understand borderzones and ‘health provider of definitive care’ for stroke patients. This information has been shared with the national leadership group and national ambulance services. A rehabilitation stock take has been completed and work now needs to be undertaken to identify gaps for improvement and future work programme. An allied staff stroke group has been formed and the first teleconference will occur 3.04.14. Initial work will be focussed on identifying how the 2014/2015 rehabilitation indicators can/will be collected. The group will also focus on key pieces of work that need to be undertaken to bridge gaps identified in the national rehabilitation stock take.The audit schedule now includes ethnicity data and some initial results are starting to be reviewed and discussed. This is on-going in terms of ensuring ethnicity data are available and correct.The audit schedule is progressing and improving over time. However data collection and input is an on-going issue, in particular coding for stroke patients who have been thrombolysed. It would be useful if at a national level patients who have had an ischaemic stroke with thrombolysis could be identified. A potential solution would be to add a ‘t’ to the I63 and I64 codes to decrease the manual collection of data. Additional audits will be added for the next quarter and include: the number of unspecified stroke code I64, as this identifies practice change needed in documentation and coding, the number of non-Maori/non Pacific under/over 65s will also be added.BOPDHB, Waikato DHB, TDHB and TDH have a stroke/thrombolysis register currently in use. Lakes DHB is developing a register and this will commence when they start thrombolysis.
Risks / major challenges
Consideration of a telestroke service is on hold until further consideration given to options in June 2014. Given that Lakes DHB does not start their thrombolysis service until 1 June 2014, this timeframe may need to be extended. This is related to the lack of maturity of thrombolysis services in some DHBs in the region currently. These services needed to be started or embedded for longer before a long term solution can be identified.
What we said we would do in Quarter 4.Governance Deliverable Timeframe Progress Reason for Deviation
G1 Local delivery of stroke services to All DHB stroke protocols and services are in line with the Stroke July 2013 and on- G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 21

meet the Stroke Guidelines (2010) Guidelines Develop pathways for acute stroke thrombolysis in TDHB and
Lakes DHB
going
G2 Regional and local implementation of national stroke work plans
Recommendations from the national work groups are incorporated into regional and local plans including:
Thrombolysis Rehabilitation TIA
July 2013 and on-going
G
Quality and Safety Initiative Deliverable TimeframeQ1 Primary prevention Education Plan
and Education Package for community based health care providers
Mapping of current education provision and gap analysis Strategy and Plan developed and available for the
primary/community sector
July 2013-June 2014
A
As per comment under key highlights, we are now working with the Stroke Foundation to develop these resources for national use – this has the potential to extend timeframes but longer term will be more useful for the sector.
Q2 Comprehensive Health Professional education programme
Lead stroke nurse forum established Online learning resources shared across stroke clinicians Case reviews occur at all Stroke Network meetings Annual regional stroke study day delivered Learning opportunities shared between Midland DHBs Māori health key worker education resources are developed
July 2013 and on-going
G
Service Delivery Deliverable TimeframeS1 Thrombolysis service in
geographically remote areas of the Midlands region
A regional approach is agreed and in place, identifying feasible service coverage.
January 2014 – June 2014 G
S2 Discharge planning and post stroke care
Undertake a stock take of community and rehabilitation services supporting patients post-discharge
Investigate options for supported discharge planning and post stroke care
July 2013 and on-going G
S3 Maori Health Access to acute stroke services is monitored for the Maori population
Measures collected including audits are broken down to include ethnicity where possible
July 2013 and on-going G
Research and Evaluation Deliverable TimeframeR1 Key audits and outcome measures
are monitored by the Stroke Network
Quarterly review of results Six monthly review of data
July 2013 and on-going G
Enablers/support Deliverable Timeframe
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 22

E1 Telestroke pilot A stock take of infrastructure is undertaken A stroke care pathway is developed to support a telestroke
service A business case to support a pilot for telestroke is developed
and signed off
July 2013 – June 2014
A
Please see risks/major challenges on previous page
What we did in Quarter 4, in addition to what we said we would do. The reason/s for undertaking this activity Under 65s stroke funding Concern by the Network that this group of stroke patients are not having their
rehabilitation needs met in some areas and the impact this has on the clinical and social outcomes for these patients
2014/2015 plan first draft finalised A regional and MoH requirement
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 23
VULNERABLE SERVICES
Midland Maternity Action Group Clinical Chair: Corli Roodt, Clinical Midwife Director, Waikato DHB
Key highlightsto review
Midland Region Midwifery Emergency Refresher Course 2014-2017 developed, including Midland attendance certificate, by the Midland maternity educators as a collaborative initiative, and approved by the Midwifery Council of New Zealand. Tairawhiti has delivered this regional training package and received positive feedback from attendees. A media release to celebrate this achievement is currently being drafted. The delivery of education will be consistent across the region, with the added benefit of maternity educators able to deliver training in other districts when required at short notice.
210 safe sleep devices purchased in support of the Midland Safe Sleep Programme and the Midland Safe Infant Sleeping (birth to 1 year) Policy Positive feedback received from the Director, Change for Our Children “During 2013, Midland was the only region where numbers of infant deaths continued to fall. This
is encouraging given that Midland has a high proportion of Maori births (43%) compared to Northern (23.4%), Central (32.8%) and Southern (18.9%) regions. Infant mortality is now similar across all regions.” A media release was released on this achievement.
Baby resuscitation mannequins purchased for each of the Midland DHBs in support of neonatal resuscitation education Formal communication by MMAG to the NZ Breastfeeding Association to advocate a review of some sections of the BFHI accreditation standards, with a positive
outcome achieved with suggested changes adopted. Maternity data is supplied to DHBs to benchmark Co-operation between MMAG members to support the DHB MQSP Annual Reports.
Risks / major challenges
Workforce deliverables are a key challenge. This is dependent on the successful recruitment to the Midland workforce advisor role, which is outside the control of MMAG.
Sustainable funding for safe sleep devices to support safe sleep practice, and reducing SUDI rates. MMAG will not be funding further safe sleep devices in the 2014/15 year but will support maternity services as they look to find sustainable alternative funding streams to support safe sleep in Midland communities.
What we said we would do in Quarter 4.Quality and Safety Deliverable Timeframe Progress Reason for Deviation
Q3 Achieve regional quality and safety efficiencies through collaboration and sharing
Evaluate achievement against maternity standards Two areas of improvement are identified from clinical indicator data and
regional solution developed Three procedures / pathways identified, developed and added to shared
database to improve consistency of practice across Midland
June 2014
C
Q4 Strengthen consistency of practices through shared educational activities
Regional education plan is developed and activities are prioritised annually
June 2014
C
Q5 Reduce the smoking and SUDI rates
Midland DHB regional Safe Infant Sleeping (Birth to 1 Year) P policy developed and in place across all Midland DHB facilities
June 2014 C
All providers of maternity services are trained in promoting safe sleeping June 2014 G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 24

messages
Service Delivery Deliverable Timeframe Progress Reason for Deviation
S3 Support framework for young vulnerable women who are pregnant
Work collaboratively with primary providers, including Maori health providers, and PHOs to identify the issues and support systems
Commence the development with relevant stakeholders and primary providers to develop a regional programme that will wrap support around young vulnerable women who are pregnant, including smoking cessation, substance abuse
June 2014
G
Enablers/support Deliverable Timeframe Progress Reason for Deviation
E1 Workforce intelligence Head count to service current population vs workforce needed for future birthing trends is identified
December 2013 R Regional workforce resource required
Areas of shortage are identified December 2013 R Regional workforce resource required
E2 Workforce utilisation Utility of existing workforce model critiqued against workforce forecasting December 2013 R Regional workforce resource requiredE3 Workforce planning and
forecasting for medical staff
Quantification of percentage of consultant time spent in obstetrics to ascertain level of obstetric workforce need
December 2013 R Regional workforce resource required
Quantification benchmarked across other three regions by RDOTs December 2013 R Regional workforce resource requiredE5 Progress connected
health concepts to improve access to clinical maternity information
Work with regional IS to develop implementation plan Participate in MCIS system development at the national level, working with
the clinical reference group and CleverMed Implementation plan commenced in early adopter site (Tairawhiti)
June 2014
R
What we did in Quarter 4, in addition to what we said we would do. The reason/s for undertaking this activity Draft 2014/15 MMAG work programme developed A MoH requirement
Regional website content developed and uploaded (including shared educational calendar for the region, highlighting of Midland agreement to work together for midwives looking to return to practice in the region, consumer focused information covering pregnancy, finding a midwife, breastfeeding, safe sleep, smoking cessation, mental health and linkages to each of the DHB maternity web pages)
A need identified by MMAG
Meeting between Chair, Project Manager, RSP Programme Manager and Director of Midland Regional Training Network has been set to discuss workforce initiatives for 2014/15
A need to identify initiatives early as regional workforce position currently being advertised
Collation of Midland maternity workforce issues and key challenges completed. This will inform workforce strategic discussions on regional initiatives for 2014/15
Collation of feedback on the use of the safe sleep sticker alert system which supports the
A need to identify initiatives early as regional workforce position currently being advertisedA need to continuously review and improve the quality of resources
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 25
implementation of the regional safe infant sleeping policy Support for the provision of CTG monitors is being considered. DHBs are trialing units (where
required), a collation of user feedback has been reviewed, and a stock-take of current CTG monitors in each of the Midland hospital maternity units is almost complete.
A need identified by MMAG, particularly for women with high BMI; and the ability to secure favorable pricing through an existing contract price by one of the Midland DHBs
Health of Older People Action Group Clinical Chair: Dr Phil Wood, Waikato DHBKey highlights Two dementia pathways have been completed and, subject to regional agreement, will be published on Map of Medicine on 17 April 2014. The pathways are Dementia
Assessment and Dementia Management. These pathways are intended to promote early diagnosis of dementia and assist with the assessment and management of dementia in primary care.A regional contract to facilitate primary care dementia education for the pathways has being negotiated with the Ministry of Health. The purpose of the contract is to improve dementia awareness and responsiveness, and provide education resources for primary care in the Midland region. The contract will run for three years.Commenced using interRAI assessment data to benchmark and compare levels of complexity for older people in the Midland region. The interRAI clinical data will identify ‘at risk’ older people and provide a range of information to support the ongoing work of the groupA work plan has been developed for the 2014/15 financial yearPhil Wood has taken over from Lorraine Taylor as chair of the health of older people action group. Lorraine chaired the group for two years from early 2012 to 2014
Risks / major challenges
None identified
What we said we would do in Quarter 4.Quality / Safety Deliverable Timeframe Progress Reason for Deviation
Q1 Principles of care for HOP services
Review existing documents and develop a set of principles of care with sign off and support from the Midland DHBs
July 2013 – December 2014
G
Service Delivery Deliverable Timeframe Progress Reason for Deviation
S1 Wrap around services are available for Older People across the sector
Define and specify HOP wrap around services Stock take of ‘wrap around’ services and benchmark against a dashboard of defined
‘essential’ wrap around services Investigate and utilise InterRAI data to inform service delivery – explore InterRAI
information being collected and develop a system to identify at risk Older People across the sector
Stock take of discharge planning processes is undertaken for acute services A best practice integrated discharge planning model is investigated and agreed by
the HOP action group
July 2013 – June 2014
G
S2 Dementia service development HOP action group to provide feedback on the National Dementia Framework during consultation phase
Undertake stock take of dementia services available across the region (full spectrum) Provide regional oversight, support and shared resources for the implementation of
July 2013 and on-going G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 26

the national dementia framework
S3 Delirium service development Undertake stock take of delirium services available across the region Work with national coders to ensure delirium coding is more accurate A pathway for the prevention and management of delirium is developed and
approved for use across the Midland DHBs including a case finding tool Delirium education and training resources are developed for use by clinicians Benchmark the % utilisation of a screening and measurement tool for risk of delirium
for those 75+ Benchmark % of intervention plans in place for delirium cases
July 2013 and on-going
A
Research and Evaluation Deliverable Timeframe Progress Reason for DeviationR1 Key audits and outcome
measures are monitored by the HOP action group. It is anticipated that actions within the work plan will see a decrease in readmission rates to acute services and admission rates to aged residential care services
Benchmark the % of patients 75+ who have an unplanned readmission to acute services
Benchmark the % of admissions to ARC within one month of discharge from acute services
July 2013 and on-going
G
Enablers/Support Deliverable Timeframe Progress Reason for DeviationE1 Workforce and training for the
Health of Older Persons’ sector Stock take of workforce activity across the region including any other workforce plans
for the HOP sector (regional and national) Stocktake of HOP workforce across the Midlands region Identification of key priorities for workforce development
July 2012 and on-going
A
To be commenced in quarter four
E2 Workforce and training for the Health of Older Persons’ sector
Undertake a stock take of ACP utilisation in the Midland region and establish a baseline of relevant clinicians and clinical settings for ACP training
Support DHBs to establish a clinical champion for ACP Promote the utilisation of ACP across the Midland region with health professionals,
patients and the broader community
July 2013 and on-going
G
What we did in Quarter 4, in addition to what we said we would do. The reason/s for undertaking this activity None
Radiology Advisory Group (MRAG) Clinical Lead: Andrew Klava, lakes DHB; Chair: Jill Wright, Manager, BOPDHBKey highlights Philippa Edwards was appointed at project manager for the group
MOH released the Service Improvement modules in May and all 5 Midland DHBs have decided to participate in the opportunity to receive funding to enable SI initiatives to be progressed
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 27
MRAG began developing the Midland Region Primary Access Criteria for CT and US and General X-ray prior to the work commencing nationally. It was decided to complete this work rather than wait as the two potentially inform each other at a national level and evolved somewhat aligned. This work was completed in May and the document is currently with the regional Radiology HODs, COOs and GM’s Planning and Funding with implementation proposed for July 2014. The development of regionally agreed criteria has involved a high level of work, engagement and collaboration regionally over 12 months. MRAG consider the adoption of the Regional Criteria will allow for a staged process towards the National Criteria, as they open access up in some areas but not in as many areas as the National Criteria. Therefore it will provide an opportunity to monitor the impact on demand and budgeting requirements at the P and F level prior to the implementation of the National Criteria.
MRAG has set itself up as an Advisory Group for pathways and other networks. In Q4 four networks have consulted with MRAG and clinical agreement sought. The HOP Action Group, Dementia sub group attended an MRAG meeting to finalise discussions on primary access to CT scans within their Dementia Pathway. The Stroke Network is working with MRAG on the Acute Stroke Thrombolysis pathway to achieve timely CT access, the Renal Network has reached agreement on access to US in the Renal Pathway and the Vascular Group attended a meeting to clarify work being undertaken regionally and to identify any impacts on radiology services. MRAG find this to be a significant improvement in communications by service with them and a successful repositioning that has the potential to ensure the development of workable pathways.
IP and ED referrals- 90% of accepted referrals to have their procedures are completed within 24 hours and 98% of accepted referrals have their procedure completed within 48 hours. All 5 DHBs are meeting this target
Community/GP and OP referrals – 70% of reports should be dispatched within 48 hours of procedure performed. WDHB OP and GP reporting times have decreased. Diagnostic Services for Primary Referred: 65% of accepted referrals for scans receive their scan within 6 weeks (42 days) for CR, for CT except for Lakes. However
the worst performing area is US where only BOP meets the KPI.
Risks / major challenges(all areas flagged with ‘Caution’ or ‘In trouble’)
National Indicators (CT and MRI) CT Scanning – Only Lakes and Tairawhiti achieve the target and Lakes joins Waikato, BOP and Taranaki in failing to deliver CT to Community referrers within 6 weeks. MRI Scanning – Only Waikato has major difficulty meeting this target. BOP is currently negotiating a new contract with additional volumes for MRI.Primary Referred Indicators: Diagnostic Services for Primary Referred: For Ultrasound. 65% of accepted referrals for scans receive their scan within 6 weeks (42 days). Only BOPDHB is currently
able to meet this target. The remaining 4 DHBs achieve only 50%. Ultrasound has a critical workforce shortage that may take some years to resolve due to the length of training involved and the increasing numbers moving to work in private practices upon qualifying
Diagnostic Services for Primary Referred: For CT. 85% of accepted referrals for scans receive their scan within 6 weeks (42 days). Only TDH is meeting this targetWorkforce. HealthShare have appointed to the Workforce Analyst position. There are Sonographer workforce issues for most DHB’s. This has created issues with service delivery timeframes. Data collected since March 2013 shows an
unchanged acceptance level of referrals however unmet demand is not currently captured. Information Technology Regionally Waikato, BOP and Tairawhiti share a PACS archive and Taranaki and Lakes send images as required to this archive for patients who transfer hospitals The WDHB CWS implementation will return to being a regional implementation throughout the 2014/15 year. This is hoped to support internal and external e-referrals MoM and Bay Navigator pathway development has impacts on radiology as they work to manage priorities within all clinical services
What we said we would do in Quarter 4.Governance Deliverable Timeframe Progress Reason for Deviation
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 28

G1 Regular meetings and workshops to continue to develop the MRRN
Liaise and inform other key project groups such as the Cancer MDM Group, Midland Primary Referred EAG, the MRRG and other regional networks (as appropriate)
Clinical leadership across the continuum of care contributing to service delivery, sustainability and longevity of the group
Monthly or bi-monthly meetings/ workshops (either face to face, or videoconferencing and/or teleconferencing in conjunction with web conferencing technology)
G
Quality and Safety Deliverable Timeframe Progress Reason for DeviationQ1 Improving Radiology outcomes As per MoH National indicators Improving Waiting Times for
Diagnostic Services for Community and Outpatient Referrals: National indicator 1: CTNational indicator 2: MRI
Review monthly Indicators set until Q4 2015
ASee comment Risks/Challenges section above
Q2 Improving Radiology outcomes As per regional KPIs(2) as noted in measures section:Regional KPI 1: Inpatient and ED Referrals (a) and (b)Regional KPI 2: Community and Outpatient Referrals
Review findings monthly Review: Q4 2014 G
Q3 Improving Radiology outcomes Implement Primary referred indicators (as noted in the measures section)Primary Referred Indicator: 1 a Primary Referred Indicator: 1 b
Primary Referred indicator : 2
Reviewing findings monthly Review:Q4 2014
G
See comment Risks/Challenges section above
A
A
Q4 Improving Radiology outcomes Standardisation of RVUs across the Midland Region Regional Standardisation Q2, 2013 C
Regular comparison and monitoring of data between Midland DHBs Q4 2014 ???Q5 Improving Radiology outcomes Shared information to identify process and efficiencies that can be
adopted and implemented Ongoing G
On-going focus on improving wait times within Radiology Improving waiting times On-going Review: Q4 2014
???
Service Delivery Deliverable Timeframe Progress Reason for DeviationS1S2
Access criteria to primary referred radiology
Agreement to use a regional primary referred access criteria, developed in conjunction with the MRRN and aligned with national criteria when available
Q2 – StocktakeQ4 - Deliverable G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 29

S3 Clinical Pathways Creating linkages with key stakeholder groups on how radiology services can help to inform clinical pathway development within the region
On-goingG
S4 Service delivery planning Any impacts are minuted and reviewed by the MRRN groupAction planned to be implemented if required
Review and discuss at each MRRN meeting G
Research and Evaluation Deliverable Timeframe Progress Reason for DeviationR1 Regional access benchmarking Analysis on activity data, affordability, and demographics. MRRN to
make recommendations as appropriateMonthly and annually G
Enablers/ Support Deliverable Timeframe Progress Reason for Deviation
E1 Workforce and Training:All programme initiatives (E1 – E5)to be in conjunction with the MRTN Leadership group and the MRWFD team
Head count of service current population vs. workforce to deliver the key objectives
Areas of shortage are identified Trends in radiology workforce numbers, distribution and
forecasting are analysed by regional workforce
Q2 2013
Q2 2013 Q4 2014
A
See comment Risks/Challenges above
E2 Utility of existing workforce model critiqued against workforce forecasting
Explore innovations for retaining radiology staff in the Midland region (eg: post vocational training including sonographers)
Q2 2013 Q4 2014
A
See comment Risks/Challenges above
E3 Explore innovations for retaining radiology staff in the Midland region (eg: post vocational training including sonographers)
Strategic plan for sustainable radiology service provision inclusive of Radiologists and Sonographers
Work with appropriate organisations boards to plan for placements in identified areas
OngoingQ4 2014
G
E4 Improving relationships and developing staff as well as completing service improvement projects
Multiple projects defined by local DHB aligning with regional initiatives
G
E5 Capital Work cooperatively as per regional procurement strategy to align capital plans and tender timetables
Continual review of timetable
Quarterly until end of 2016G
E6E7E8E9
Information technology:All programme initiatives to be in conjunction with the MRIS Leadership group. All IT initiatives in this section (E6 – E9) are dependent on deliverables being achieved as documented in the 13/14 Regional ISSP
MRRN to provide input into the development of a web based portal (Midland Navigator or similar) for use by primary and secondary health providers
Work with the Regional IS to develop an implementation plan for a shared electronic workspace
All Midland DHBs to have monitoring in place to ensure radiology
Development: Q2 - Q4 2014
Roll Out: Q4 2014 Ongoing: Q4 2016
A See comment Risks/Challenges above
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 30

reports are signed off within appropriate time frames. Roll out across the region
What we did in Quarter 4, in addition to what we said we would do. The reason/s for undertaking this activity Involvement in the MOH lead Radiology Service Improvement Project MOH request
Renal Action Group Clinical Chair: Dr Peter Sizeland, Renal Physician, Waikato DHB and Jo-Anne Deane, Manager, Waikato DHBKey highlights The Midland Regional Renal Plan 2014-2018 is nearing completion. The final stage will be updating data in the report with the latest census and health delivery data
in June Steering group has been set up to investigate a mobile home/campervan, kitted out to support dialysis patients. Contact has been made with a patient advocate to write article highlighting work that the Regional Renal team and the proposed purchase of a Home Dialysis ‘fitted
out” campervan. Set of regional KPIs have been agreed on and will be included in the 2014-2018 Regional Renal Services Plan (see list under “Renal Action Group Measure” at the
end of this report) Decision has been made by the group not to include a formal work programme for 2014/15 therefore removing them from the 2014/15 Regional Services Plan.
Risks / major challenges
Tertiary E-referral: this cannot progress until the Clinical Workstation Implementation at Waikato is complete and the orders functionality employed for the Renal Service. There is no timeline within IS for this currently Dependent on 3rd party vendor and clinical review (both Primary and Tertiary). Aligning the Map of Medicine has now been included in scope of work. Work is underway on the renal pathway
Tele-medicine: On hold as waiting for Regional protocols to be developed instead. There are issues with non-standardised and conflicting technology at each site. HealthShare has trialled a solution with implementation planned for Q4.
Workforce: HealthShare is currently recruiting to a vacant Workforce Analyst position. All workforce-related initiatives are dependent on this position being filled IT: MRRAG still suffers from the lack of a Renal data base and the Nurse Specialists work with excel spreadsheets as a substitute
What we said we would do in Quarter 4.Governance Deliverable Timeframe Progress Reason for Deviation
G1 Regular meetings and workshops to continue to develop the MRAG
Clinical leadership across the continuum of care contributing to service delivery whilst ensuring sustainability and longevity of the group
Quarterly meetings or workshops G
Liaise and inform other key project groups such as the National Renal Board and other Regional Networks
Progress the agreed network priorities as outlined in the regional RSP programme G
Quality and Safety Deliverable Timeframe Progress Reason for Deviation
Q1 Models of care In conjunction with primary and BPAC develop a standardised CKD referral process including access criteria and clinical pathway
Develop Q1 2013 A See comment Risks/Challenges
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 31

Roll out across region to primary Roll out Q4 2013
Q2 Models of care Implement education programme for GPs Programme formulated: Q4 2012 C
Service Delivery Deliverable Timeframe Progress Reason for Deviation
S1 Regional renal plan Implement work plan Plan formulated Q4 2013 G
Prioritise initiatives: Q2 2013 G
Complete outcome: Q4 2014 G
S2 Telemedicine Develop protocols for telemedicine across the region Develop protocols Q4 2012 G
Trial site (TDH) Trial: Q1 2013 A See comment Risks/Challenges
S3 Clinician education Design an education plan Q4 2012 C
S4 Service delivery planning Any impacts are minuted and reviewed by the MRAG group Review at each MRAG meeting G
Action plan to be implemented if required Review at each MRAG meeting G
Research and Evaluation Deliverable Timeframe Progress Reason for Deviation
R1 Data collection and reporting Ensure there are mechanisms in place to ensure the ability to measure standard of care across the Midland region.
Review Q2 2013 G
Targets/outcomes/KPIs are refined around risk management to show intervention rates, supported by robust data and audit outcomes
On-goingG
Data presented locally and regionally to allow for local and regional approach to service/quality improvement where appropriate
On-goingG
Enablers/Support Deliverable Timeframe Progress Reason for Deviation
E1 All programme initiatives to be in conjunction with the MRTN leadership group and the MRWFD team
Head count to service current population vs. workforce to deliver the key objectives
Q2 2013 R See comment Risks/Challenges
E2 Areas of shortage are identified Q2 2013 R See comment Risks/Challenges
E3 Workforce and Training Robust understanding of workforce issues and identification of workforce needs for the future
Trends in renal workforce numbers, distribution and forecasting are analysed by regional workforce (benchmarked against demand)
Q2 2013
Q4 2014
R
R
See comment Risks/Challenges
E5 Supporting integration and linkages Develop and roll out a programme in conjunction with Māori Plan Developed: Q2 2013 A See comment
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 32

with DHB Māori Health PlansIncreasing live donor rates in Maori and Pacific populations
Health which will be designed to be utilised in primary and secondary health care arenas
Roll out: Q4 2014 Risks/Challenges
E6 IT/ IS. All programme initiatives to be in conjunction with the MRIS leadership group. All IT initiatives are dependent on deliverables being achieved as documented in the 13/14 Regional ISSP
The MRAG is to ensure involvement in the development and roll out of an agreed regional electronic clinical workstation and data repository.
Timeline dependent on DHB affordability and implementation of the Regional ISSP A
See comment Risks/Challenges
What we did in Quarter 4, in addition to what we said we would do. The reason/s for undertaking this activity A steering group has been set up to investigate a mobile home/campervan, kitted out to support dialysis
patientsTo Improve patient access and the experience of patients on dialysis
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 33
REGIONAL ACTIVITIES
Child Health Action Group Chair: Dr David Graham, Paediatrician, Waikato DHBKey highlights A comprehensive quarterly data report is now being produced for the group – this is on-going however as data are reviewed and refined. The group continues to work
on ensuring the data are accurate and meaningful across the region. Three pieces of separate work have been identified to assist with this: Coding optimisation for secondary care/inpatient coding Consider an outpatient coding system utilised consistently across the DHBs Understand what coding occurs in the primary sector, in particular general practice
Data have been reviewed on paediatric admission rates. A stock take of regional capacity continues to be developed.A comprehensive stock take is underway on child and youth initiatives across the region, this includes national initiatives. This work is being undertaken to inform a collaborative child health project commencing in July 2014.A website solution has been finalised – introductory content has been sent through for uploading onto webpage.
The group continues to work on Map of Medicine pathways. These have now been designated a clinical lead and some additional pathways have been identified and prioritised: Asthma Bronchiolitis Gastroenteritis Community acquired pneumonia Eczema Enuresis croup
Management of constipation Skin sepsis Cellulitis UTIs Mental Health Issues – ADHD Management of cleft palate
Risks / major challenges
Workforce – We have completed a stock take of medical staff in the DHBs and nursing child health roles. Work is underway to understand what allied health roles are available for child health in the DHBs. There is currently no workforce resource within HealthShare therefore the workforce trend analysis will not be undertaken within the 2013/2014 planning timeframe. The workforce resource is actively being recruited currently.
What we said we would do in Quarter 4.Governance Deliverable Timeframe Progres
sReason for Deviation
G1
Set up governance, terms of reference, project management, secretariat, communications plan and reporting framework
Four meetings, TOR and communication plan, reporting to Planning & Funding Alliance Leadership Team
Q1 2013
G
The group has was only established in mid-August 2013 and we are still working on finalising the terms of reference – this should be done by February 2014 once the 2014/2015 first draft is finalised.
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 34
Quality and Safety Deliverable TimeframeQ1
Review of paediatric admission rates – Demand Side
Comparison of admission rates across the region and against benchmarks in NZ and overseas
Qtr 1 and 2 2013/14 G
Q2
Review of paediatric admission rates - Supply Side
Stock take of regional capacity and linkages to equity of access across the region
Qtr 3 and 4 2013/14
Research and Evaluation Deliverable Timeframe Progress Reason for DeviationR1 Stock take of current child and youth
initiatives across the regionReport and engagement process to ensure the action group is apprised of all future research activity
Qtr 3 and 4 2013/14 G
R2 Establish a focus on research based development for child and youth services
Qtr 1 and 2 2014/15
Enablers/support Deliverable TimeframeE1 Workforce Head count to service current population vs
workforce needed for future birthing trends is identified
Identify shortages
Identify supply issues and work towards regional solutions
Trend analysis of workforce numbers, distribution and forecasting are analysed by regional workforce group
Qtr 2 2013/14
Qtr 2 2013/14
Qtr 3 2013/14
Qtr 4 2013/14
G Please see risks/major challenges section above
R
R
R
E2 IS - Set up Nexus collaborative site Nexus site used by action group May to July 2013 CE3 IS – Web Communications strategy implemented Qtr 1 2013/14 CE4 IS - VC Functional VC facilities Ongoing C
What we did in Quarter 4, in addition to what we said we would do. The reason/s for undertaking this activity 2014/2015 plan first draft finalised A regional and MoH requirement
Map of Medicine Coding subgroup formed
See commentary under highlights aboveSee commentary under highlights above
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 35
Midland Regional Emergency Departments (REDs) Chair: Dr Matthew Valentine, Bay of Plenty DHB
Key highlights Midland REDs stocktake, including project tracking tool, available on Nexus for members to update 2014 NZ Emergency Care Conference planning progressing, with conference flyer released Midland ED Clinical Nurse Specialist sub group formed, with regional meeting held to progress the training and development of the role in the region Sharing of DHB ED guidelines across Midland utilising NEXUS as a shared web based repository Pre-hospital representative (St John’s) now included in REDs membership Workforce/activity survey of Midland ED clinicians – terminology definitions being refined to enable standardised benchmarking of collected data
Risks / major challenges
What we said we would do in Quarter 4.Governance Deliverable Timeframe Progress Reason for Deviation
G1 Ensure the governance structure of the Midland Regional Emergency Departments (MREDs) is functional and sustainable
Confirm MREDs Terms of Reference Develop an ongoing sustainable communication plan to inform stakeholders
and staff of MREDs progress and activities Regular MREDs meetings scheduled for key DHB emergency staff to
engage Include MREDs on the online website so that research and documentation
can be shared regionally in a secure web based environment
On-going
G
In draft for review
Quality & Safety Deliverable Timeframe Progress Reason for Deviation
Q1 ED 6 hour target Share strategies and solutions within EDs in the region for addressing the six hour target.
Identify and support departments where maximal ED changes have been made.
On-going
G
Q2 Lead an annual national emergency medicine conference
Oct 2013 conference already in planning. 2nd year of clinical director pre-meeting. 1st year of clinical nurse manager pre-meeting
On-goingC
Q4 Awareness of emergency medicine quality projects underway in region.
Stocktake of current projects. Development of tool for tracking projects
On-going C
Service Delivery Deliverable Timeframe Progress Reason for Deviation
S1 Identify strategies to address acute Identify barriers to meeting peak demand periods. On-going G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 36

demand
S2 Develop strategies to address primary-secondary integration
Monitor progress and results with primary-secondary after hours integration in Thames.
On-going C
S3 Develop ED Clinical Nurse Specialist role
Submit proposal to regional COOs. Identify clinical champion to spearhead.
On-going G
S4 Develop a working group with Midland Regional Trauma System to consider trauma care and referral patterns in rural communities
Formalise current relationship. Identify priorities from list in description
On-going
G
Research and Evaluation Deliverable Timeframe
R1 Support a community of learning within MREDs
Utilise a web based forum as a learning tool to support research, evaluation and innovation within emergency care
November 2013
C
Enablers/support Deliverable Timeframe
E1 IS support for MREDs clinical network development
Enhanced communication between MREDs and IS staff Awareness of IS technologies available to support emergency care services
and patients
OngoingG
What we did in Quarter 4, in addition to what we said we would do. The reason/s for undertaking this activity Map of Medicine presentation to REDs to raise awareness of clinical pathways in
development across the region and logins issued to REDs members Procedural sedation in remote/rural Emergency Department setting – REDs applying to
the Midland Regional Training Network to transfer the training from Pulse to Moodle
Improved connectedness of ED clinicians with pathway development, particularly where there is an ED section of the pathway.Need identified to support remote/rural workforce in Midland.
Midland Regional Trauma System Chair: Dr Grant Christey, MRTS Director, Waikato DHB
Key highlights Regional Guidelines and Clinical Transfer Matrices Regional trauma incidence studies (paediatrics, occupational, elderly, spinal injury, TBI, rural trauma, alcohol) Midland Trauma Research Centre development Regional data validation studies (Faculty Research Development Fund (FRDF), University of Auckland) Data access and research policies BBC (Better Business Case) development for pro rata has commenced (Treasury template)
Risks / major Registry and TQUAL development stalled
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 37
challenges Workforce deficits Funding (FTE) stability DHB support
What we said we would do in Quarter 4.
Governance Deliverable Timeframe Progress Reason for Deviation
G1 Ensure the governance structure of the Midland Regional Trauma System (MRTS) is functional and sustainable
Confirm MRTS Terms of Reference Develop an on-going sustainable communication plan to inform
stakeholders and staff of MRTS progress and activities Regular MRTS meetings scheduled for key DHB trauma staff to engage Include MRTS on the NEXUS website so that research and documentation
can be shared regionally in a secure web based environment
On-going
G
Quality & Safety Deliverable Timeframe Progress Reason for Deviation
Q1 MRTS Registry implementation Continue entry of regional trauma data into the Registry MRTS securing support for data entry from the Midland DHBs, enabling a
focusing of resource on timely data entry. This will assist in the timely identification of Q1 initiatives and research through trauma registry data.
Complete new registry fixes, testing, data merge and data backfill Identify ways to reduce dependence of FTE on data handling Consider alternative funding streams and resources to support the more
efficient entry of data into the Registry Develop data audit programme based on registry function Apply for funding and resources to support data handling
October 2014
G
Q2 Develop a Trauma Quality Improvement Programme (TQIP)
Commence identifying quality initiatives using the 2013 Verification Report to support prioritisation
Develop a prioritisation of the quality initiatives identified to improve trauma patient care
Allocate tasks to a draft timeline that rationalises multiple priorities for incorporation into MRTS work plan
Develop a draft MRTS strategic plan and investigate funding via DHB support
June 2014
G
Q3 Develop a Trauma Quality Improvement Programme (TQIP)
Create a comprehensive data dictionary Identify data usage guidelines
June 2014 G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 38

Develop templates that support data usage guidelines
Q4 Risk register development Development of a regional Trauma System Risk Register Individual Midland DHBs to provide their templates for consideration by
MRTS in the development of a regional Trauma System Risk Register Link regional Trauma System Risk Register to TQUIP
March 2014
G
Service Delivery Deliverable Timeframe Progress Reason for Deviation
S1 Develop MRTS Guidelines Develop agreed trauma service guidelines across the Midland region in line with international best practice, and consistent the national direction for a range of clinical areas
Identify priority areas for regional guideline development, including the development of acceptance referral matrices
Draft MRTS Guidelines developed, documented and circulated for 1st review and agreement
June 2014
G
S2 Develop a Midland Immediate Medical Response Service (MIMRS)
Develop a definition of the service provided by a MIMRS, and operational manual
Review NZ Medical Assistance Team (NZMAT) and Australian Medical Assistance Team (AUSMAT) to ensure compatibility
Develop and enact a recruitment strategy for MIMRS
G
Research and Evaluation Deliverable Timeframe
R2 Midland MRTS Conference Put together a trauma conference proposal for early 2015 for consideration January 2015 C
R3 Midland Trauma Research Unit Identify partner organisations and specific personnel (Universities, trauma care provider agencies, national and international collaborative groups, researchers, etc)
Identify priority projects and research topics Establish processes for data handling, fund management, ethics approval,
grant application processes
December 2014
G
Enablers/ Support Deliverable Timeframe Progress Reason for Deviation
E1 Develop competency of a trauma specialist workforce
Consider orientation and training requirements for staff specialising in and/or providing trauma care
June 2014R
E2 IS support for MRTS clinical network development
Enhanced communication between MRTS and IS staff Awareness of IS technologies available to support trauma services and
patients
On-going
R
Waikato DHB IS support for MRTS is unavailable due to Waikato DHB IT system upgrades
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 39
E3 MRTS structure Identify future structure and funding requirements June 2014 G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 40

Smokefree Network Gary Thompson, HealthShare Key highlights Two programme areas are delayed but remain achievable in the 13/14 year
Midland Maori Health Excellence Wananga is planned for 29-30 May 2014. The Wananga will focus on Breast screening, Cervical Screening, Smokefree and SUDI. Considerable effort has gone into pulling the Smokefree component of the Wananga together and supporting the organising committee with logistics
The Midland Smokefree programme has been given permission to engage with secondary schools of the Midland region who will attend the National Secondary Schools Kapa Haka competitions in Tairawhiti in July 28 – 1 August 2014.
The initiative will encourage and incentivise groups to compose an item depicting the harms and effects of tobacco on Maori youth and for Maori in general. The item will be performed on the national stage to a national audience. District Smokefree leaders will support the schools and composers with information and data and visually document the journey to develop and present the item. Positive progress is being made in the Maternity sector to support pregnant mothers who to quit. Great collaboration of stakeholders and engagement of regional
maternity leaders and LMC’s.
Risks / major challenges
Pacific Leadership Key issue has been the availability of Pacific Smokefree leaders to meet. Barriers included small no of providers, providers engaged in a wide range of Health and
Wellbeing initiatives and limited workforce. Mitigation: A number of Pacific leaders have indicated their ability to meet in Q2. This could be an initial meeting to agree a course of action to bring a larger group
together.Midland Smokefee Programme VisibilityThe ability to communicate effectively with key Smokefree stakeholders is heavily reduced by the lack of access to a Midland Smokefree web-site. Numerous positive examples of Smokefree activity is occurring across the region which need to be shared not only to the region but would assist with the national effort. Mitigation: - Web-site required urgentlyProgramme Support RSP reports for 12/13 highlighted the need to better coordinate resource and effort to engagement and relationship building aspects of the programme. The
rationales for this is to ensure that external organisation to Health are supported to complete the development of policies, implementation planning, evaluations, monitoring and reporting.
Where successful this work is strongly supported by local coalition groups. Waikato CC, Auckland CC and Waikato University are good examples. As more organisations are engaged through the programme the same level of support is required. Rural centres are at particular risk of not having the support to
back up the engagement. Public / Population Health have a role in engaging external organisationsMitigation: Review Public Health contracts to better align with Midland Smokefree programme objectives.
What we said we would do in Quarter 4.Governance Deliverable Timeframe Progress Reason for Deviation
Midland Smokefree Leadership Group
The Midland Smokefree Leadership Group (MSLG) is established to lead and sustain the Midland Smokefree programme to 2025
o Strong regional Smokefree DHB and sector collaborationo Maori Caucus and the Pacific Forum participate and contribute to
MSLG
Q1- MSLG confirms regional priorities Q1-Maori Caucus meets to confirm Maori
priorities Q3-Regional influence and alignment of DHB
activity Q4-MSLG reviews actions against priorities
G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 41
MSLG continues to challenge DHB’s and Iwi Board members by reporting progress and risks to achieving the Smokefree 2025 vision
o DHB’s model a high standard of Smokefree leadership and behaviour
o HR policies reflect the gold standard of Smokefree policyo 30% of DHB contracts include a gold standard Smokefree policy
measureo Improved management of patient and visitor Smoking behaviour
Q3-4 Midland Smokefree 2025 programme presentations to 2 Midland DHB CPHAC committees
The Midland Smokefree programme convenes a monthly Midland Smokefree Leaders teleconference.
Maori Caucus priorities confirmed and integrated into regional planning Key issues on teleconferences include Regional Services Planning and
DHB Annual Plans and alignment of regional priorities, sharing local activities and developing and implementing regional actions
Tobacco Free and Smokefree features strongly in the planning drafts for 2014-15
G
Midland DHB Tobacco Control Steering Group(TCSG)
TCSG and District Smokefree stakeholders meet quarterly to review and modify Smokefree action
o Alignment of DHB and Primary Care Smokefree actiono Population Health, Secondary and Primary Care align Smokefree
action toward the Midland Smokefree 2025 vision o NGO and Cessation provider contribute to District Smokefree
action planning
Q1-2 Midland Smokefree 2025 programme participation in 2 Midland DHB TCSG
Q3-4 Midland Smokefree 2025 programme participation in 2 Midland DHB TCSG
G
The Midland Smokefree programme continues to participate in District TCSG.
Teleconferences provide a positive overview of activities both local and regional
Quality and Safety Deliverable Timeframe Progress Reason for Deviation
Regional Audit Regional audit of Smokefree Tobacco Free policies within DHB service providers and contractors
o Smokefree policy audit report by provider / contractoro Audit reports prompt improvementso 90% of regional service providers and contractor Smokefree
policy is audited over 3 year
Q1-Schedule 13/14 audits against 3 Year Audit programme
Q1-4 30% of providers and contractors have their Smokefree Policy audited
G
Q4 results will better indicate progress in this activity
Service Delivery Deliverable Timeframe Progress Reason for Deviation
Maori leadership Create a regional Maori leadership forum to lead the development of Maori Smokefree initiatives
Work with National Maori Tobacco Control Leadership Group to engage the National
Q1 – Maori Caucus inaugural meeting agrees Maori priorities
Q1-2 Establish links with the National G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 42

Kohanga Reo Trust to develop Auahi Kore, Tupeka Kore Kawenata (policy) for Kohanga Reo organisations
Work with National Maori Tobacco Control Leadership Group to engage MoE to develop Tupeka Kore policy for Maori Education establishments
Develop and seek funding for a Maori Smokefree engagement initiative
Maori Tobacco Control Leadership Group NMTCLG
Q3-4 With NMTCLG establish links with MOE, National Te Kohanga Reo Trust
Q3-4 Pilot a Smokefree programme with Kohanga Reo
Q1- Develop a Maori Smokefree Tobacco Free intervention and promote for funding. (Tu Kotahi Tatou)
Maori Caucus guidance has been integrated into Regional Service Planning National Maori Tobacco Control Leadership Service Launched as Te Ara Ha Ora in
November 2013. Midland Smokefree Programme Director is a member of the Advisory Panel of Te Ara
Ha Ora Strategic Planning is almost complete which will drive National Maori Leadership
activity Government Agency engagements are underway through Te Ara Ha Ora Whakawatea Te Ha – Marae focused intervention has been developed and submitted
for the MoH Innovations Funding The Tupeka Kore Tu Mauri Ora National Secondary Schools Kapa Haka Composition
competition aims to incentivise secondary schools participating in the National Kapa Haka event in July-August to compose an item about the harm and effects of tobacco for Maori.
15 Colleges and Whare Kura from the Midland Region will be invited to submit an item for Judging
A panel of Kapa Haka experts will determine a winner. The winner will receive a Trophy and educational products for the School.
The Midland Smokefree programme brokered the development of a Tupeka Kore Policy to be introduced at Te Whare Wananga o Awanuiarangi. The policy will be launched on May 30 to coincide with World Smokefree Day.
The Policy is Tupeka Kore or Tobacco Free rather than Smokefree. No Tobacco products will be allowed on to the any facilities or campuses of the Wananga.
More importantly the Policy is tikanga based which is likely to resonate stronger among staff and students.
G
G
Pacific Leadership Establish a Midland Pacific Smokefree Leadership forum Target and re-prioritise funding for tobacco initiatives across contracting and
programme development processes
Q1-Pacific Leadership Group meets and agrees Pacific Smokefree priorities
A
Progress in Q2 has been positive. Meetings have occurred with service providers in the Waikato and BOP where the majority of the regions Pacific population live.
Several opportunities to share the direction and objectives of the Smokefree programme with a Pacific audience have been taken during Q3. There is a desire to formalised a Pacific Forum
Stephanie Erik the CE for ASH has been helpful in linking local networks with the
Q3-4 Develop and promote a Fono engagement initiative
Q4-Test the feasibility of piloting a Fono engagement initiative
A
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 43

programme
Service to Maori and Pacific women
Maternity Continue to improve the availability and reach of cessation and support services to
Maori and Pacific women particularly, pregnant and young mothers Progress toward achieving the maternity target Enhanced District and Regional collaboration of Primary and Secondary care
maternity and cessation services improves outcomes for pregnant Maori and Pacific women
Maternity nurses and Lead Maternity Carers are trained quit card providers
Q1-2 In collaboration with key stakeholders develop a referral pathway for Maori and Pacific women particularly, pregnant and young mothers
G
Waikato DHB has developed a Maternity Leadership programme to improve engagement with pregnant mothers who are smokers.
It has strong stakeholder participation including LMC It has developed a training package for practitioners who engage with pregnant
smokers to improve the ABC and more importantly the referral to cessation services including AKP
The model is being shared with regional Maternity leaders to enable duplication of learning across the region
Taranaki and Tairawhiti have a similar model and use Smoke Change training to support local stakeholders
Q3-4 Pilot and test the pathway at a service level
Q4 Report progress to DHB’s and MSLG G
G
Integrated Addictions programme
Continue to pilot an integrated addictions programme that seeks to empower whanau affected by issues relating to smoking, gambling, drugs and alcohol
Q1-2 Confirm clinical and stakeholder membership to a project steering group
Q2 Pilot developed and initiated at 2 sites across the region
A
This project is delayed slightly due to the increased activities in other regional priorities
Stakeholders are confirmed and the project plan is agreed Implementation is delayed to Q4
Q4 Report to MSLGA
Build on sector relationships
Tertiary Education providers, Territorial and Local Authorities, Business sector and Central Government Agencies support the Midland Smokefree 2025 vision
Q1-2 2 District Councils agree to develop Smokefree policy advice for Mayor and Council consideration each year
Q1-4 2 District Councils adopt a Smokefree policy each year
Q1-4 Continue to build relationship within the Tertiary Education sector to promote the development of gold standard Smokefree policies
Q1-4 Establish links with NMTCLG to advance engagement with Ministry departments
G
Sector relationship programme is on track Several BOP/Lakes Councils are undergoing a review of their SF policies
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 44

The Midland programme is focusing on integrating a 2025 strategy that sets out a phased approach to being fully Smokefree by 2025
The approach encourages Council to look past Smokefree open spaces to identify the things they can do and schedule actions to achieve them
The Midland Smokefree programme endgame framework is being promoted as guidance
G
Research/Evaluation Deliverable Timeframe Progress Reason for Deviation
Stock take Baseline Stocktake of Smokefree intervention areas to monitor progress toward 2025 go
Q1-4 Initiate the development of baseline data for Smokefree target areas by district (know your numbers
G
Several levels of district and regional data have been collected. DHB’s are matching local information with National Census information to confirm the regional tobacco use picture
G
Enablers/support Deliverable Timeframe Progress Reason for Deviation
Whānau level Smokefreeengagement
Tu Kotahi Tatou (Innovation Fund Proposal) describes a model of Smokefree engagement with Maori and Pacific at the whanau level
Q1-4 Promote Tu Kotahi Tatou for funding G
The Midland Smokefree programme has supported the development of a second application to the MoH Tobacco Control Innovations Fund
It is a marae base initiative with a Maori community development organisation that represents 12 Marae within the Tainui Cluster
Successful applicants will be notified in April 2014 On track
G
Key EnablersQ2 Maori Health report for reference:
Māori Health Midland Region General Managers for Māori Health, Chair: Ditre TamateaKey highlights Regional Governance and Decision Making
The Midland Iwi Relationship Board (MIRB) continues to participate in planning processes at a regional level and supports as appropriate regional activities which align to work undertaken by the Midland GMs Māori and Māori Health Plan targets and actions. Te Tumu Whakarae the Midlands Māori GMs, have secured two representatives (GM Māori Waikato, GM Māori Health Planning and Funding Bay of Plenty) on the Planning and Funding Alliance Leadership Team (P&F ALT). Both representatives continue to ensure that Māori Health is a priority within the regional space. Further Māori expertise/membership has been secured on the Child Health SLAT and Older Persons SLAT which report to the P&F ALT. Further Māori expertise has been secured on a range of other regional forums (Midland Cancer Network, Hei Pa Harakeke, Renal, Stroke, Cardiac, Midland Regional Training Network, Midland Mental Health Forum, Midland Smokefree Forum). The Midland Iwi Relationship Board continues to receive regular reports on the implementation of Regional Service Plan initiatives that relate to Māori Health including the Midland Māori Health Dashboard report.
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 45

At the December 2013 there was continued endorsement of the value of the Midland Māori Health Plan dashboard report with clear targets and actions which enable the Iwi members to monitor progress achieved against the plans including identifying key areas for focus and improvement such as Māori DNAs, ASH, CVD, Breast and Cervical Screening.There was support for a regional approach to the Māori Health Excellence Seminars to identify and support best practice and continuous quality improvement across the region. There was agreement to move to a shared iwi chair leadership role to foster greater ownership and accountability for their work programme.
Quality AssuranceThe target for one regional cultural audit and action plan to be completed per annum will been attained by quarter4 of 2014. A draft regional He Ritenga audit programme will be submitted to the Midland Māori GMs to approve in January 2014. The target for the standardisation for the Māori Health template within Midland has been achieved with the Midland GMs Māori adopting a standard template for all Māori Health Plans. An alignment exists between Māori Health Plans and annual plans across Midlands further the Ministry has moved to ensure that there is uniformity between the targets which must be attained for Māori, relative to non-Māori. This has ensured that performance will be measured at an equitable level across the full range of health indicators that are a priority for Māori. A national Māori Health Plan monitoring framework and indicator report piloted by Midland and endorsed by the national Tumu Whakarae and CEO groups for adoption. However, reports against the Midland DHBs performance against Māori Health Plan indicators are also still being generated to align to our internal midland reporting processes and to enable a Midland focus. Te Tumu Whakarae has invited the Lead Planner for the Regional Services Plan to its Midland Planning day in February to ensure that there is a strengthening of the alignment between Māori Health Plans and the Regional Services Plan for the 2014-2015 period.
Building Regional IT CapabilityThe reporting of service access rates is being done as part of the regional data reporting. It is expected that a regional clinical workstation and data repository will improve the quality and access to this information.
The integration of cultural assessment tools is not at this stage being delivered at a regional IT work stream level. There is work required to embed the use of cultural assessment tools in the triage, care planning and discharge planning processes. This needs to be driven by the businesses at a DHB level rather than regional IT. It is expected that as the triage, care planning and discharge planning processes move from paper to electronic, that established business rules and processes will be incorporated into the electronic process, inclusive of cultural assessment tools.The Midland region has made good progress with regards to information sharing between primary and secondary care. Electronic referrals from primary to secondary are available to all PHOs in the Midland region and there is increasing uptake of this service. Much of the region currently sends electronic discharge summaries from secondary / tertiary to primary care. The current Waikato Clinical Work Station (CWS) replacement project, which is phase 1 of the regional CWS project will enable a larger implementation of electronic discharge summaries. These activities are inclusive of Māori providers and PHOs.
Cancer ServicesThe National priority cancer areas/services identified – lung cancer, bowel cancer, breast-screening, radiation oncology service, medical oncology services as a priority. These areas align to health priority areas for Māori in the area of cancer. The prioritisation of such areas of work is based on mortality and morbidity data and vulnerability of service. Health inequalities across all these areas of cancer are well known and identified. Work on addressing health inequalities however continues to be on-going and will be medium and long term in nature. Some key developments include:
- Regional priority service changes identified – Tairawhiti adult cancer services and palliative care, Midlands Prostate Cancer Study (HRC) gynae-oncology model of service, standardise guidelines/pathways.
- Development of national tumour stream priorities (x10).- Development stage of capturing FCT wait time indicators.
Some specific work that seeks to reduce health inequalities for Māori include:- Breast-screening access for Midland Māori women on-going.- Improving palliative care health literacy and support for Māori and whanau - Supporting Tairawhiti Māori cancer patients with the transition of adult cancer services to Waikato effective 1/7/13.
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 46

- Eight Kia ora E Te Iwi cancer literacy programmes targeting Māori completed for first 6 months.- Waikato DHB P&F have included cancer component into four MHP whanau ora contracts effective 31/12/13. Planning for another 3 contracts to be agreed by June
2014.- Palliative care research hui/symposium held at lakes to share Midland palliative care and health literacy research initiatives on 16/10/13. Over 120 participants from
across NZ attended.- Midlands Prostate Cancer Study- with final draft report submitted to HRC in late November 2013. The GP Report is currently being printed and will be out to clinics
early 2014. The Equity Report is in first draft. This is an additional document that Midland felt was an important contribution to highlight inequities in the pathway of care for Māori men, aim to have this available March/April 2014.
- Following last year’s regional workshop, meeting with Auckland DHB, Lakes, BOP TDH DHB gynae meetings, a draft discussion paper on Midland gynae-oncology model of service sent out to stakeholders.
- Midland Map of Medicine lung cancer pathways agreed for suspected, non-small cell and specialist assessment.- Midland drug protocols agreed for region.
The Hei Pa Harakeke Māori Advisory Group Forum continues to provide regional support in the area of cancer as a partnership group to the Midland Cancer Network. Some particular successes with Hei Pa Harakeke include: Hei Pa Harakeke establishes a kaitiaki reference group to Prostate Cancer research initiative. The completion of a sub-regional Cough, Cough Campaign around the early detection of lunch cancer in Māori (Waikato / Lakes). The successful regional development of a Safe Sleep model and accompanying policy for Midland (Waikato led). This included a regional series of wananga, which trained over 60 staff across Midlands on safe sleep messages (Pepi-Pod initiative target high needs whanau). Promotion of Māori interests in the Faster Cancer Programme and the ongoing roll-out of E Te Iwi Cancer Literacy training in conjunction with Māori communities and Māori Providers (Waikato led). Further work will be undertaken to improve performance against cervical and breastscreening rates for Māori through the completion of Health Excellence Wananga, which will be completed by the 30th June 2014. Māori breast and cancer rates remain a significant priority for Midland further noting Midland is the poorest performing DHB region for both these indicators. The January 2014 planning day will focus on elevating this as a priority within the RSP and agreeing resourcing and focus for cancer in the first instance be on those priorities within our Māori Health Plan’s.
Elective ServicesThe region routinely reports clinical activity by DHB of domicile, ethnicity and rurality to identify inequalities in access and outcomes.The first focus has been on improving access to elective services and providing equitable access for DHBs across the region (through standardising intervention rates and scoring tools and streamlining pathways). This will provide a benefit for DHBs with a higher proportion of Maori populations. Inequalities for Māori have been identified and the work to respond to this is still to be done. Some standardisation of tools Any response is recognised to be complex and will take time for results to be measurable.
Stroke ServicesThe Midland Stroke Network has a focus on providing high quality stroke services within the hospital setting, supporting national work on strengthening the primary prevention message and encouraging Māori to access TIA and Stroke Services. One of the key developments of the workstream has been the development of a Bilingual Fast Flyer resource (Tairawhiti lead) - after consultation with local Tairawhiti Māori Health Providers a draft bilingual Fast Flyer was produced to assist Māori Health Workers and population. This was then sent out to all Midland Māori Health Mangers for comment as to relevance and tribal appropriateness. The draft was then formalised as a Midland Stroke Network communication tool.
Another key achievement has been a Māori Health Keyworker Development Resource – after consultation with Tairawhiti Māori Health Providers it was discovered that many local Māori Health Keyworkers use the NZ Stroke Foundation website to locate Stroke communication aids. On the basis of RSP Aims to “reduce duplication of effort” and “identify efficiencies” an approach was made to NZ Stroke Foundation to jointly achieve this RSP Initiative. Joint collaboration has identified an appropriate resource used in Aboriginal communities. Permission to adapt this resource for Māori Health keyworker use is currently being sought. The Aboriginal resource was also taken by a Tuhoe Kaumatua to Tuhoe communities to consider its purpose, relevance and appropriateness. C) Process within each Midland DHB (that has a resource) to ensure Māori Health Team involved in acute Stroke awareness for Māori Stroke Patients – each Midland DHB approached and asked to provide their process of how Māori Health Team become involved in acute Stroke awareness for Māori Stroke Patients.
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 47

WorkforceTe Tumu Whakarae the Midlands GM Māori have secured representation on the Midland Training Network (Waikato GM Māori and Lakes GM Māori). Kia ora Hauora the Midland Māori Health Workforce initiative (Lakes Lead) continues to meet all its deliverables. Key milestones achieved in this quarter were:
Appointment of Kia ora Hauora staff: Fallyn Flavell (Kia ora Hauora Co-ordinator) and Terere Aoake (Liaison Assistant). Fallyn and Terere will be based at Lakes DHB Māori Corporate Services with Māori Health.
Confirmed Kia ora Hauora contract with the Ministry of Health to 2016. Secondary Schools Roadshows occurred during November and December 2013. Over 500 Māori students (years 9 and 10) engaged in the programme. Ten
schools were visited from Tairawhiti, Bay of Plenty, Lakes and Waikato. The roadshow introduced the Kia ora Hauora programme and encouraged students to take science related subjects at secondary school.
Supported Tairawhiti to enable an internship programme in the different regions on Midland. Working on partnership programmes with Auckland University to work alongside the Whakapiki Ake programme and Massey University with Te Rau Puawai
programme. Terere and Fallyn will be visiting DHBs, Tertiary and Polytechnics across the region in the next few months.
Two regional workforce development training initiatives have been initiated for the non-regulated Māori Health workforce that includes E Te Iwi Training around cancer literacy and Safe Sleep as a focus on smokefree and reduction of SUDI. Further Health Excellence Wanaga will be held in health priority areas for Māori by the 30th June 2014. These wananga will target best practise around lifting performance against indicators which are health priorities identified in all Māori Health Plan’s (smoking, SUDI, ASH and Breast and Cervical cancer). Te Tumu Whakarae has placed bicultural education training in the E-learning strategy for the Midland region. Further, the Midland region has undertaken a pilot of an on-line cultural competency training package, which will target boards of governance for DHBs and have also provided governance training for iwi relationship boards across the Midland region. Midland Iwi governance training and evaluation undertaken and completed in December 2013.
Health of Older PeopleA range of measures have been agreed for Health of Older people that will be reported quarterly. These measures will be reported for older Māori and older non-Māori comparatively. Inequities in admission rates and readmission rates, between older Māori and older non-Māori data is available, but work is occurring with DHBs to further improve data quality.The process for deciding which Māori older people issues to prioritise, and which indicators will be used to measure progress is to be determined through quarterly reporting measure of older people. Progress toward achieving targets in prioritised Māori older people areas remains work in progress. A review of Home Based Support Services is occurring within Midland. Te Tumu Whakarae has secured expertise on the Older Persons SLAT. The key focus of this forum has been looking at the home based support review and how this is going to better meet the needs of Māori. Te Tumu Whakarae and their representation on the forum and the P&F ALT is seeking to ensure that a kaupapa Māori approach to home support services is retained within the Midland region. Further, communication to key stakeholder groups inclusive of Iwi Relationship Boards (IRBs) has also been identified as a priority in the development of any new model around home based support services across Midland. Another key focus of the forum is to increase awareness amongst Māori whanau communities and providers around dementia and those support services that exist to assist whanau. An initiative to look at increased awareness amongst Māori and Pacific whanau, communities, health and social service providers around dementia and input into the designing of dementia services across the region is on track with the pathway development underway, which includes Māori and Pacific communities.
Maternity Action GroupEthnicity data is being captured across all Midland Maternity Action group (MMAG) projects and work programmes, specifically this targets breastfeeding, SUDI and smoking. Ethnicity data is captured and reported across all MMAG projects and work programmes. – MMAG data is provided quarterly and where possible, is defined by ethnicity. The region routinely reports clinical activity by DHB of domicile, ethnicity and rurality to identify inequalities in access and outcomes; however, currently the Ministry of Health does not report the National Maternity Standard Measures by ethnicity. This makes it impossible to determine whether these standards are being met for Maori and whether inequalities exist across any of these areas.
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 48

HEAT application to MMAG workWhile all MMAG initiatives align to HEAT to ensure initiatives do seek to support a reducing inequalities approach, the forum has sought advice from Te Tumu Whakarae as to whether HEAT should be replaced by a Whanau Ora tool. MMAG in conjunction with Te Tumu Whakarae has successfully led the regional development of a Safe Sleep model and accompanying policy for Midland (Waikato led). This included a regional series of wananga, which trained over 60 staff across Midlands on safe sleep messages (Pepi-Pod initiative target high needs whanau). To date over 271 Pepi-Pods have been distributed to high needs whanau across Midland, this indicates that by quarter 4 report the target of 300 Pepi-Pods being distributed to high needs whanau will be well exceeded. Progress at a regional level is monitored through a National database that provides an ethnic breakdown on recipients.
In regards to timeliness and outcomes from health services between pregnant Māori women and pregnant non-Māori women. This measure is captured from data obtained from first trimester registration with an LMC. Latest figures suggest that in the Midland region, 40-60 % of Maori mothers register in the first trimester compared with 50-80% of European, with Lakes and Tairawhiti having the lowest rates in all ethnicities.
In regards to the process for deciding which Māori maternity issues to prioritise, and which indicators will be used to measure progress. Inequalities for Maori in maternity have been identified and key focus areas have been prioritised. Priority areas include SUDI, breastfeeding, smoking in pregnancy, access to pregnancy and parenting programmes (P+P), teenage pregnancy and clinical indicators. Response is recognised to be complex and will take time for results to be measurable. MMAG has identified that the births per ethnicity is changing in that the population of mothers of birthing age for Maori is increasing and for non-Maori birth rates are decreasing. MMAG concludes that service design and staffing need to shift in line with this change in demand. Approaches to this will be considered in the 2014/15 year.Progress toward achieving targets in prioritised Māori maternity areas is trending upwards. Breastfeeding, smoking and SUDI rates for Maori are improving in the Midland region. Investment in the Regional Safe Sleep Programme which integrates safe sleep, smokefree and breastfeeding messages has contributed to this shift.
Report on improving Māori attendance at pregnancy and parenting classesReport on the performance of existing Pregnancy and Parenting (P+P) Education programmes in reaching Māori women. MMAG is awaiting the consumer research report to be released by the New Zealand Institute of Rural Health (NZIRH) which is specifically looking at the rural consumer experience of pregnancy and parenting classes in the Midland region. The MoH have yet to release the Service Specifications for Pregnancy & Parenting contracts. Plan established to improve Māori participation in Pregnancy and Parenting Education programmes is established. MMAG is awaiting release of the NZIRH report to devise a plan to address access issues for Maori and other vulnerable groups. Māori targeted P+P programmes are established across the Midland region. Waikato DHB piloted the Hapu Wananga programme – a kuapapa Maori programme that targeted pregnant teens. The evaluation of this programme has been submitted to MMAG to support their planning once they have received the NZIRH report. Many other districts within Midlands also have in place kaupapa Maori P+P programmes.
Report on activity to improve Māori breastfeeding rates Explore the development of technological solutions and resources to improve Māori access to breastfeeding information and support. MMAG’s Breastfeeding/BFHI sub group is developing web content to be loaded onto the regional website under Midland Maternity which will provide breastfeeding information and support to consumers. The founder of Mama Aroha Talkcards is currently developing breastfeeding education and support applications for mobile phones and tablets in which Midlands intend to adopt as part of the Regional Safe Sleep Programme.
Renal Action GroupIn early 2013, the Waikato DHB submitted a proposal on behalf of the Midland regional renal services to the Ministry of Health Live Kidney Donor RFP. Unfortunately the Midland region was not successful in securing any funding. However, the relevant Midland DHBs felt this was an important matter to be considered and as a result, the Midland Regional Renal group have looked at ways in which this work could be carried out within existing resources. As a result the following plan actions and plan have been developed and carried out of the pass 12months.
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 49

Hui/Wananga with Maori renal patients and their whanau took place in November to identify areas of need, better understanding of renal services and the support available to both the patients and their whanau. This work involves working closely with the Midland Renal Transplant Coordinator and Te Puna Oranga-Kaitiaki. Permission from the patients and their whanau has been obtained from this wananga to utilise the information obtained and discussed with members of the Renal Transplant & Improvements in Live Organ Donation project Counties Manukau DHB. The overview directly from the Maori patients and their whanau will provide some direct insight into what is needed to support them on their renal journey. A meeting has been scheduled to meet with the coordinator for the renal transplant & improvement in live organ donation project and the health literacy project manager in early 2014. This will inform future training and development opportunities around increasing the Maori and PI donorship within the Midland region.
SmokefreeThe Midland Smokefree Māori caucus now provides cultural and equity focused guidance and advice to the Midland Smokefree Programme. Tupeka Kore, Tu Mauri Ora (tobacco free-how we want to live) is the vision for the caucus. Regional Smokefree priority areas are Māori, Pacific, Māori pregnant and young mothers, kohanga reo, kura and rangatahi. Māori quits:
- Initial analysis of annual hospitalised Māori smoker discharge data (4 of 5 DHB’s) shows 10,700 Māori smokers are discharged each year. A regional project will investigate and recommended improvements to the pathway of discharged smokers from DHB to cessation service providers.
Māori and pregnant mothers- Waikato DHB has established an inter-sectorial maternity leadership group focused on improving smokefree outcomes for young Māori pregnant mothers.
Integration of this model is being developed with other DHB’s.
Kohanga Reo - Projects to engage Kohanga Reo organisations into Tupeka Kore are underway in Taranaki and BOP. Waikato DHB continues to lead the integration and
implementation of the Tupeka Kore approach. Tupeka Kore has been integrated into various DHB settings. Regional services such as the Midland Cancer Network have gone Tupeka Kore or entirely tobacco free through the placing of a kawenata or covenant on their office premises. It is expected that the Midland breastscreening service will also go Tupeka Kore by 30th June 2014. The Tupeka Kore kawenata evidences a uniquely Māori approach to supporting a Smokefree Aotearoa by 2025.
Kura- Bernard Fergusson kura kaupapa and Brightstars bilingual education centres in the Waikato became the first Tupeka Kore education centres in the country
through the placing of kawenata over the last period. - Regional project briefs have been developed for each of the Midland smokefree programme priority areas. Midland DHB Smokefree groups initiate project briefs
as resource and staffs is available. Tupeka Kore Brand
- Shane Bradbrook, the former CEO of Te Reo Marama currently owns the copy right to Tupeka Kore. However, members of the Māori Caucus were given approval by Mr Bradbrook to use Tupeka Kore as long as the integrity and ethos of the brand is maintained. Regional services such as the Midland Cancer Network have gone Tupeka Kore and the Midland Breast Screening Service also has identified that will also go Tupeka Kore over the coming period.
Risks / major challenges
What we said we would do in Quarter 2 (NB: some actions are on-going with a deliverable date of 30 June 2014).
Priority Area Outcome Reported Progress Reason for Deviation
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 50

Regional Governance & Decision Making
- Report on Midland Iwi Relationship Board (MIRB) participating in planning process at a regional level, and supporting Midland GMs Māori , Māori Health Plans, projects, initiatives and developments.
G
- Report that Midland Planning and Funding Alliance Leadership Team (P&F ALT) have representation from Te Tumu Whakarae, the Midland Māori Health GMs forum. G
- Report that Māori expertise / membership has been secured on the Child Health SLAT and Older Persons SLAT which reports to the P&F ALT. G
- Report to confirm that progress in regards to the implementation of the RSP projects and initiatives are being forwarded to the Midland Iwi Relationship Board (MIRB) for their information (Quarter 2 and Quarter 4 reports).
G
- Report on Māori expertise secured on any regional clinical governance structures, which are established. G
Priority Area Outcome Reported Progress Reason for Deviation
Quality Assurance
- Report on one regional He Ritenga Cultural audit and action plan being completed per annum- Report on the standardisation of Māori Health Plan planning template within Midland- Report on Primary care/ PHO deliverables in AP and MHP across Midland being standardised
in planning, action and deliverables will relate to:
G
Cervical indicator and Breast Screening (link to RSP Cancer) G
Smoking cessation indicator Primary Care (link to RSP Cancer and RSP Smoke Free) G
Immunisation indictor (Link RSP Child Health/ Maternity Action Group) G
CVD indicator (link to RSP Cardiology and Stroke) G
Influenza indicator for 65yrs+ (link to RSP Older Persons) G
- Report against Midland DHB’s performance against Māori Health Plan national indicators are completed
G
Please refer to Maori Health Indicators Report attached.
MHP Indicator Narrative Report Dec 2013 - Google Drive.pdf
Building Regional IT Capability
- Regional clinical services information technology (IT) work-stream can: Report regional service access rates, interventions, outcomes and readmissions by
ethnicity (Māori comparative to non-Māori ) A
The reporting of service access rates is being done as part of the regional data reporting. It does not fit specifically within the regional clinical information technology work-stream. It is expected that a regional clinical workstation and data repository will improve the quality and access to this information.
Report that cultural assessment tools have been integrated into processes electronically into triage, care plan and discharge planning processes.
A The integration of cultural assessment tools is not at this stage being delivered at a regional IT work stream level. There is work required to embed the use of cultural assessment tools in the triage, care planning and
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 51

discharge planning processes. This needs to be driven by the businesses at a DHB level rather than regional IT. It is expected that as the triage, care planning and discharge planning processes move from paper to electronic, that established business rules and processes will be incorporated into the electronic process, inclusive of cultural assessment tools.
Report IT interface with Māori providers and PHO’s to ensure information sharing and seamless patient transition between primary and secondary / tertiary based services.
G
The Midland region has made good progress with regards to information sharing between primary and secondary care. Electronic referrals from primary to secondary are available to all PHOs in the Midland region and there is increasing uptake of this service. Much of the regional currently sends electronic discharge summaries from secondary / tertiary to primary care. The current Waikato CWS replacement project, which is phase 1 of the regional CWS project will enable a larger implementation of electronic discharge summaries. These activities are inclusive of Māori providers and PHOs.
Priority Area Outcome Reported Progress Reason for Deviation
Cancer Services
For all cancers grouped and for the following cancers separately; lung, breast, prostate and gynaecology ensure for all initiatives that the following is considered:- Report on inequities in cancer incidence and mortality between Māori and non-Māori.
G
- Report on inequities in access to, timeliness and quality of, and outcomes from cancer services between Māori and non-Māori. G
- Report on a process for deciding which Māori cancer control issues to prioritise, and which indicators will be used to measure progress. G
- Report on progress toward achieving targets in prioritised Māori cancer control areas. G
- Report on Hei Pa Harakeke Māori Advisory Group work as a forum. Specifically: Kaitiaki reference guidance and support given to prostate cancer research initiative Sub-regional cough cough campaign around early detection of lung cancer in Māori Health Excellence wānanga around best practice to improve regional breast screening
rates held Report on sub-regional Pepi-Pod initiative and smoke free messages to high needs
whānau (refer to RSP Maternity Action Group) Participate in faster cancer programme to ensure interests of Māori are upheld. E te Iwi cancer health literacy initiative with Māori communities/ NGO’s? cancer society
G
Elective Services
For elective services as part of action group reporting include measures/commentary on:- Inequities in access to and timeliness to elective services between Māori and non-Māori. G
The region routinely reports clinical activity by DHB of domicile, ethnicity and rurality to identify inequalities in access and outcomes.
- Process for deciding which Māori elective services issues to prioritise, and which indicators G The first focus has been on improving access to elective
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 52

will be used to measure progress. services and providing equitable access for DHBs across the region. Inequalities for Māori have been identified and the work to respond to this is still to be done. Any response is recognised to be complex and will take time for results to be measurable.
- Progress toward achieving targets in prioritised Māori elective services areas.A
Stroke Services
For stroke services as part of action group reporting include measures/commentary on:- Inequities in stroke incidence and mortality between Māori and non-Māori. Use surrogate
indicators if required.- Inequities in timeliness and outcomes from, stroke services between Māori and non-Māori.
GThe region routinely reports clinical activity by DHB of domicile, ethnicity and rurality to identify inequalities in access and outcomes.
- Process for deciding which Māori stroke issues to prioritise, and which indicators will be used to measure progress.
- Progress toward achieving targets in prioritised Māori stroke areas.A
Inequalities for Māori have been identified and the work to respond to this is still to be done. Any response is recognised to be complex and will take time for results to be measurable.
Initiatives are based upon data analysis around system inequalities for Māori pertaining to need, rates of access, equity of intervention and health outcomes relative to the rest of the population
- Report on Māori health key worker education resources development- Report on a FAST information Flyer being developed for the Māori health workers and
the Māori population across the region- Report on a process being developed within each DHB ( that has such a resource)
across the Midland region to ensure that the Māori health team is involved in acute stroke admissions for Māori stroke patients
G
Priority Area Outcome Reported Progress Reason for Deviation
Workforce - Report that Te Tumu Whakarae Midland Māori GM’s have Māori representation on the Midland Regional Training Network (MRTN). G
- Report against Kia ora Hauora Midland Māori health workforce development initiative completed. Specifically key deliverables in the report will detail: A minimum of 20 Midland KOH partner secondary schools engaged in the
programme 25 Midland Māori supported into first year of health related tertiary study Complete individual career plans with at least 40 Midland Māori students Provision of NCEA workshops and resources Co-ordination of student placement days, conferences, exposure activity and
engagement with tertiary providers Liaison and funding of Māori tertiary student support groups at key Midland
educational facilities
G
- Report against two regional workforce development training sessions being completed for non-regulated Māori health workforce in two health priority areas associated with RSP
G
- Report against regional E- Learning training utilised to provide training for staff around G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 53

correct ethnicity data collection and cultural competence training
- Report against Māori leadership programme instigated at a regional level to promote and foster Māori leadership in Health. G
- Report on progress of project that ensures a co-ordinated approach across the Midland region clinical networks to health literacy around cardiovascular services and heart disease. The focus is on raising public awareness and education with an emphasis on Māori.
G
- Report annually on the Māori health workforce across all five Midland DHB’s by professional group relative to non-Māori G
Note: All DHBs report against their Māori Health Workforce profile annually. This report is an annual report which will be completed by quarter four 2014.
Health of Older People
For health of older peoples services as part of action group reporting include measures/ commentary on:- Inequities between the health of older Māori and older non-Māori. Use surrogate
indicators if required.
G
The region routinely reports clinical activity by DHB of domicile, ethnicity and rurality to identify inequalities in access and outcomes.
- Inequities in admission rates and readmission rates, between older Māori and older non-Māori. G
- Process for deciding which Māori older people issues to prioritise, and which indicators will be used to measure progress. A Inequalities for Māori have been identified and the work to
respond to this is still to be done. Any response is recognised to be complex and will take time for results to be measurable.- Progress toward achieving targets in prioritised Māori older people areas. A
- Home Support review and how this is going to better meet the needs of Māori Development of resources as discussed, agreed and designed as part of the
working group. Increased awareness amongst Māori and Pacific whānau, communities, health
and social service providers around Dementia Stronger presence of Māori and Pacific health and social service providers in the
design of dementia services across the region.
A
Home based support review is progressing, however timeframes have been extended. Te Tumu Whakarae Midlands is working with the GMs Planning and Funding Midland to ensure that the interests of Maori are upheld through the review process. Some work has occurred to ensure engagement with Maori providers and Pacific providers to increase Maori/Pacific community awareness of dementia.
Maternity Action Group
For maternity services as part of action group reporting include measures/commentary on:- Maternity clinical indicators for pregnant Māori women and pregnant non-Māori women. Use
surrogate indicators if required.- Timeliness and outcomes from health services between pregnant Māori women and pregnant
non-Māori women. - Process for deciding which Māori maternity issues to prioritise, and which indicators will be
used to measure progress.- Progress toward achieving targets in prioritised Māori maternity areas.
G
Report against cultural responsiveness of all MMAG related activities All MMAG plans are reviewed against HEAT. Ethnicity data is captured and reported across all MMAG projects and work
G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 54

programmes.
Report on Reducing Māori smoking and SUDI rates A regional Safe Sleep Policy is established. The policy aligns to tikanga best practice
guidelines. Report on progress toward the 90% smoking target relating to pregnant Māori women
in LMC/obstetric care. 300 Pepi Pods are distributed to high-need whānau across the Midland region.
G
Report on improving Māori attendance at pregnancy and parenting classes Report on the performance of existing Pregnancy and Parenting (P+P) Education
programmes in reaching Māori women. Plan established to improve Māori participation in Pregnancy and Parenting Education
programmes is established. Māori targeted P+P programmes are established across the Midland region.
G
Report on activity to improve Māori breastfeeding rates Explore the development of technological solutions and resources to improve Māori
access to breastfeeding information and support.G
Renal Action Group
For renal services as part of action group reporting, include measures / commentary on:- Renal inequities between Māori non-Māori. Use surrogate indicators if required.- Inequities in access to and timeliness of renal health services between Māori and non-Māori.
GThe region routinely reports clinical activity by DHB of domicile, ethnicity and rurality to identify inequalities in access and outcomes
- Process for deciding which Māori renal issues to prioritise, and which indicators will be used to measure progress.
- Progress toward achieving targets in prioritised Māori renal areas. A
Inequalities for Māori have been identified and the work to respond to this is still to be done. Any response is recognised to be complex and will take time for results to be measurable.
Activity:- Report on work with Midland Regional Renal Clinicians to initiate a working group around
development of a plan to increase live donor rates in Māori and Pacific populations.-(linked to Midland regional renal work programme 2013/2014)
Outcome: Plan developed for increasing donor ship amongst Māori and Pacific
G
Smokefree Report on activities at a regional level to create a smoke free Aotearoa by 2025 (Refer to RSP Smoke Free section). Report against the Midland Smokefree programme specifically will detail:
Evidence that the Midland Smokefree Māori Caucus contributes to Midland Smokefree planning and decision making
C
Evidence that Tupeka Kore is integrated into various settings within DHB’s G
Māori Smokefree Tobacco Free interventions are initiated with Te Kohanga Reo, Kura Kaupapa and Whare Kura, and tertiary education G
Stock-take of district Kohanga Reo provides baseline to measure engagement, uptake and commitment to Smokefree 2025 G
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 55

Evidence of engagements with Hapū and Iwi leaders identifies opportunities to formulate and initiate Smokefree action G
Completion of funding proposal to engage Māori at a whānau level to go smoke free G
Evidence of engagement with National Māori Tobacco Leadership Group to support regional Smokefree initiatives G
ABC to Māori and Pacific pregnant and young mothers is improved by creating collaborative opportunities to enhance service solutions G
Initiate engagement with Alternative Education providers to integrate ABC into their programmes. And encourage participation in the Midland Smokefree 2025 vision
A
To date there has been no opportunity to engage with alternative education providers to integrate ABC into their programmes or to encourage the vision of a Smokefree Aotearoa by 2025. However, it is expected that engagement will occur and that this target will be attained by the end of the Q4 reporting period.
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 56

Workforce Development Plan Michael Bland, Regional Director of Training, HealthShare Key highlights A workforce advisor position description has been agreed by the Regional General Managers Human Resources group over the course of Quarter III. The position
has been advertised and interviews have been conducted. The interview panel comprised of a GM-HR representative (Taranaki) and Clinical Network Chair (Maternity), chaired by the RDoT on behalf of HealthShare Limited. The RDoT is now in negotiation with a preferred candidate with the expectation the role will be filled by the end of May 2014. No progress has been made in Cardiac, Child Health, Maternity, Radiology, and Renal workforce actions due to the unfilled vacancy. The newly appointed Workforce Advisor role will actively address outstanding workforce analytics required by the clinical networks through the course of Qtr IV and Qtr I 2014-15 (For Noting)The Midland Regional Training Network’s (MRTN) in order to better execute the ability to meet operational outcomes and better serve the Midland DHB’s in their work has been reconfigured with a more senior representative from key leaders within the region. Included are leads in Human Resources, Rural Hospital Medicine and Clinical Leadership from a large primary Healthcare Organisation. The specific work streams or multi-disciplinary work streams for implementation have been reformatted with a stronger emphasis on ‘governance leadership’ and broader clinical leadership within the operationalization of the work streams.Managed Virtual Learning Environment (MVLE) is a key portfolio within the training network. This work continues to work to scheduled developing the infrastructure and a series of regional and universal modules. 9 regional learning modules over the course of the year, as diverse as ‘Fire Training’ to ‘Intravenous Medicines Management’. The first two modules (Hand Hygiene and Code of Conduct for Nurses) is now regionally available and accessible. A recent examination of our usage illustrated 10,000 users across the Midland region, with over 6,500 new users since we moved e-learning into the regional space.The Midland Regional Course Request form has now been adopted throughout the region. An initiative to consider multi-disciplinary learning incorporating nursing and Allied Health Professionals (AHP) continues to develop. This concept has been presented to the national Allied, Scientific and Technical Conference recently. A business case paper is being developed to consider the funding streams support clinical release time and course fees. Rehabilitation and long term conditions are the immediate focus for this work. These papers will have close synergies to the clinical networks within the Regional Services Plan..PGY I & II training across the regional space is progressing slowly, the focus of this years (2014) is preparation around the new curriculum developed by New Zealand Medical Council, due for implementation in November 2014. The newly formed MRTN governance group is committing to see synergies between the PGY I & II programmes and primary care careers (including rural hospitals). E-portfolios and Career Planning are progressing to a common regional platform, particularly within the Nursing portfolio and being led out of Bay of Plenty DHB with oversight from the RDoT. The first cohort to be supported with a regional E-portfolio is the 170 METP students undertaking their first year of practice in the region.
Risks / major challenges
What we said we would do in Quarter 3 (NB: some actions are on-going with a deliverable date of 30 June 2014).Name Deliverable Timefram
e Progress Reason for Deviation
Growing the health workforce through strengthening recruitment, retention and repatriation WF1 Retention and
recruitment strategies for rural and workforces in vulnerable services
Establish another ‘warm welcome here’ site in each DHB in order to recruit, orient and socialise new health professionals to rural areas and to facilitate collegiality within the sector. This activity will be done by: 2. Develop Tairawhiti DHB as a new regional pilot site and identify other priority rural communities as part of the work in WF5
Q4 ongoing
G
WF2 Kia Ora Hauora Midland Region Programme –
Allocate DHB resource to assist Kia Ora Hauora coordinator to implement careers events in each Midland DHB in 2013/14 based on the patient journey through the
Q1-Q4 G
This work is being led by Tairawhiti DHB and progressing according to plan
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 57

promotion of Māori health as a career programme
emergency department into the hospital, and back to the community Support careers events for the three year funded programme Explore how the region may leverage off the Kia Ora Hauora health careers
website and student tracking system for student events
Shaping the future workforce through transformative changeWF3 New & emerging workforce 1. Regulated workforces
Identify regulated workforce needs from work done by HSL clinical networks. Develop and implement workplans
Q3 G
2. Non-regulated workforces. Explore options for care assistant training into primary care MRTN to Review Physician assistant pilot and evaluation in conjunction with HWNZ. Consider as a means to strengthen the workforce, including primary care
Q3 Q4 G
WF4 Ageing workforce strategies Flexible work arrangements Review the spectrum of alternative work arrangements and identify legislative or organisational barriers to implementation Develop options paper, pilot and assess feasibility Embed the Work Ability Index tool which allows the organisation to predict early retirement and put support in place for staff to reduce the likelihood
Q3
Q4 Q4
G
Strengthening health workforce intelligenceWF5 Workforce Intelligence
and modellingHead count of service current population vs. workforce to deliver the key objectives [Maternity, Renal, Radiology, Child Health, Cardiac] Areas of shortage are identified [Maternity, Renal, Radiology, Child Health, Cardiac]
Q2
Q2 A
A headcount of the current service population (within provider arm services) has been completed. Critical analysis against future workforce requirements needs to be undertaken
Develop workforce demographic information and forecasting model which is based on service needs and takes account of workforce profile [This activity is an umbrella for the rest of the work in WF5 and workforce modelling work in WF6] Identify rural midwives’ issues and work towards regional solutions [Maternity, Child Health] Trends in radiology workforce numbers, distribution and forecasting are analysed by regional workforce [Maternity, Renal, Radiology, Child Health, Cardiac]
Q4
Q3
Q4
A
Expected to be addressed urgently on the appointment of the workforce adviser role
Strengthening health workforce planningWF6 Future workforce
planning for Renal Maternity, Radiology and Cardiac services
Utility of existing workforce model critiqued against workforce forecasting [Q2 – Renal, Radiology; Q4 – Maternity, Cardiac] Develop a robust understanding of Cardiac SMO workforce issues and identify future workforce needs including training programmes Explore options for innovative workforce models
Q2 & Q4
Q2
Q4
A
A headcount of the current service population (within provider arm services) has been completed. Critical analysis against future workforce requirements needs to be undertaken
Workforce planning and Quantification of percentage of consultant time spent in obstetrics to Q2 A
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 58

forecasting for Maternity medical staff
ascertain level of obstetric workforce need Quantification benchmarked across other three regions by RDOTsStrategic plan for sustainable obstetric physician service provision inclusive of obstetric anaesthetists, SMOs, RMO training, and placements is developed
Q2 Q4
Benchmarking exercise not completed as no comparable datasets across the other three regions
Workforce planning and training for Health of Older Persons’ services
Stock take of workforce activity across the region including any other workforce plans for the HOP sector (regional and national)
Stock take of HOP workforce across the Midlands region Identification of key priorities for workforce development
Q1 ongoing
Q1 ongoing
AA headcount of the current service population (within provider arm services) has been completed. Critical analysis against future workforce requirements needs to be undertaken
Workforce planning for Elective services
A system in place for capturing up-to-date specialist capacity for each DHB and the region as a whole Regional planning to capture workforce constraints and shortages, with the view of sharing resources where practicable
Q1 ongoing A
This work is ongoing
Workforce planning for Mental Health services
Undertake a regional workforce stocktake and needs analysis Implement and support recommendations Establish workforce priorities annually Identify opportunities to build Midlands’ capacity in Trauma Informed Care Trauma informed Care workshops are delivered across Midland
Q1 start 2016 Complete A
Workforce planning for Trauma services
Determine orientation and training requirements for staff specialising in and/or providing trauma care
Q4 A
Building and expanding the capability of the health workforceMRTN 1
PGY I & II Training & Education Programmes
Undertake a stock take current education and training programmes aligned with PGY I & II clinical training programmes Identify possible synergies across Midland Develop a plan for core module development in 2014/15
Q1-Q2
Q3Q4
C
Completed, all regional programmes are now (through RDoT) working towards implementing the new curriculum developed by new Zealand Medical Council
MRTN 2
GPEP/Rural Hospital Training and Education Programmes
Undertake demography study to examine workforce and distribution of GP trainees
Q2-Q3 C
A business case has been developed with GM-HR to canvass all GP’s within the Midland Region and awaiting approval from GM-HR group.
MRTN 3
Clinical Placement Coordination
Review resource requirements for the adequate support of the local district coordination role including supervision and mentoring
Q4 C
MRTN 4
Career Planning Establish central web access for sharing career planning information and resources Implement regional status reporting mechanism. Support Midland DHBs to ensure 100% of trainees in receipt of HWNZ funding have career plans. .
Q3 Q4 & ongoing
G
This work is being developed alongside the nursing e-portfolio work stream for nursing. The medical workforce career plans will operate in the regional space once the structure has been determined by Medical Council New Zealand. Until such time those career plans remain part of individual DHB’s business
MRTN 5
Skills and Simulation Representation in national SSC processes. Establish regional information on: Current use of simulation based education
Q1 Q3
A State Services Commission has yet to establish a national working group.A new skills and simulation work stream has been
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 59

Future needs of simulation based education Current resources
established and is expected to complete a Qtr IV regional information base around equipment, facility and resources
MRTN 6
E-Learning Develop a sustainable business case to maintain and continue e-learning developments within the DHB. Build a quality assurance framework for all e-learning products.
Q1-Q2
Q2-3
G
This work is scheduled to be developed over Qtr 1 & II of 2014-15. The sustainable business case will be developed over the course of the next ten months to be presented to DHB in time for financial planning for the year 16/17.A quality assurance framework has been developed and being critiqued by the Learning and Development leads across the region with the project leaders for MVLE in HSL.
MRTN 7
Alignment of training funding to 70/20/10
Identify and report where DHBs need to maintain HO FTE to meet service needs where positions are funded via HWNZ and where budget to be redistributed. Develop service and funding plans as required for approval
Q3Q4 C
This activity has been superseded by the Medical pipeline work being undertaken by the MOH
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 60

Information Services Director, Regional Service Delivery: Darren Douglass Overall Status: Green
Key ‘output’ highlights
Regional Lead Architect recruitment completed successfully Regional IS Change process implemented and now applied to all regional IS services Orion agreement established with HealthShare for Waikato DHB licenses and support and maintenance services Waikato DHB Clinical Portal project has created the regional Clinical Workstation solution, running on regional infrastructure Regional Videoconference service implemented
Key ‘process’ highlights
Regional eSPACE programme team recruitment process commenced and preferred candidates identified Waikato DHB implementation of regional Clinical Workstation is in an advanced stage of configuration Regional Orion agreement in advanced stage of negotiation Lakes DHB Clinical Workstation business case review completed as part of the approval process. Tairawhiti DHB Clinical Workstation indicative business case in draft form Regional ePharmacy project implementation progressing well Midland Regional Platform and Midland Connected Health being transitioned to operational service management with Waikato DHB Regional videoconferencing service being transitioned to operational service management with Bay of Plenty DHB Midland DHBs projects to achieve Microsoft compliance all on track for completion
Progress and any major delays
Milestones FPSC: Delivery in line with national programme – Achieved. Midland continues to engage with the national programme led by CFOs. Specific engagement related to
ePharmacy procurement being led by Lakes DHB CFO. Microsoft COE: Continue XP migration – Achieved. Projects being delivered from individual DHBs. All Midland DHBs have active programmes aiming to achieve
compliance by April 2014. DHB CIOs reporting direct to DIA. CWS/CDR: Commence programme – Achieved. Programme governance in place, regional CWS/CDR solutions built on regional infrastructure and first DHB deployment at
Waikato DHB in progress. eMR: TDHB rollout continues – Achieved. eMR and ePA both live and rollout continues. ePA: TDHB rollout continues – Achieved. eMR and ePA both live and rollout continues. ePharmacy: Dependant on project rebaselining; Hospital pharmacy system testing complete. Pharmacy rebaselining milestone is for the first round of testing completed -
Achieved. All other milestones relate to regional clinical network work programmes and are reported in the relevant programme.
Risks / major challenges
The IS Portfolio is fully committed within DHB affordability constraints. There is no flexibility or contingency within the IS Portfolio and any additions or increases can only be accommodated by disinvesting elsewhere. This may impact on the ability to deliver RSP milestones where DHBs need to prioritise funding on investments on unaligned projects (whether they be national, regional or local). Mitigation: Transparency and visibility of RSP alignment and formal regional prioritisation structures. Action required: For noting.
Establishment of appropriate regional IS governance, IS delivery and ongoing service management capability is a pre-requisite for successful delivery of regional IS projects. Current structures and policies/ processes are still maturing and may have an impact on project delivery. Mitigation: Continued focus on establishing required structures and capability. Action required: For noting.
Business case approval timeframes have multiple steps creating time delays between accepting an initiative into the IS Portfolio and proceeding to implement. This has the potential to cause delays. Mitigation: Implement structures that support regional approvals where possible; incorporate approval timeframes into planning; early signalling of upcoming business cases. Action required: For noting
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 61

Key Projects
Hospital ePharmacy G Clinical Workstation A Taranaki Medication Management G
Regional Platform G
2013/14 MEASURES - NATIONAL PRIORITY SERVICESData reports are published to each network quarterly containing their measures updates and a wide range of demographic and service delivery data to inform the groups direction. Some of these charts and graphs are included in this section where up to date quarterly data was available at the time of publications. The data reports are available on request from HSL analyst [email protected]
Cancer Network – 2013/14Target Shorter waits for cancer treatment – refer to DHB reports
DHB cancer centres report cancer treatment target monthly: All patients, ready for treatment, wait less than 4 weeks for radiotherapy or chemotherapy
Indicator Faster Cancer Treatment (FCT) wait times1 % of patients (by DHB and ethnicity) referred urgently with a high suspicion of cancer who receives their first cancer treatment (or other management) within 62 days
2 % of patients (by DHB and ethnicity) referred urgently with a high suspicion of cancer who have their first specialist assessment within 14 days
3 % of patients (by DHB and ethnicity) with a confirmed diagnosis of cancer who receive their first cancer treatment (or other management) within 31 days of decision-to-treat
Indicator Improving colonoscopy wait times1 Diagnostic Colonoscopy: 50% of people accepted for an urgent diagnostic colonoscopy receive their procedure within two weeks (14 days)
2 Diagnostic Colonoscopy: 50% of people accepted for a diagnostic colonoscopy received their procedure within six week (42 days)
3 Surveillance colonoscopy: 50% of people accepted for a surveillance colonoscopy receive their procedure within twelve weeks (84 days) of the planned date
Indicator Multidisciplinary meetings (MDMs) – refer to DHB reportsPP24 DHB progress delivering improved cancer MDM using the funding for MDMs including variance in expenditure to allocated DHB MDM funds
Midland FCT wait time indicators
Bay of Plenty Lakes Tairawhiti Waikato MCN# % # % # % # % # %
Indicator 1 - % of patients referred urgently with high suspicion of cancer who receive their first cancer treatment (or other mgmt.) within 62 days
Q3 2012/13 23 58% 1 100% 9 56% 0 0% 33 58%
Q4 2012/13 18 62% 4 80% 14 67% 4 25% 40 56%
Q1 2013/14 26 68% 3 50% 11 46% 9 60% 49 59%
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 62

Bay of Plenty Lakes Tairawhiti Waikato MCN# % # % # % # % # %
Indicator 2 - % of patients referred urgently with high suspicion of cancer who have their FSA within 14 days
Q3 2012/13 25 64% 1 100% 4 27% 0 0% 31 56%
Q4 2012/13 16 55% 4 80% 7 41% 9 56% 36 54%
Q1 2013/14 18 47 5 83% 10 59% 9 60% 42 55%
Indicator 3 - % of patients referred urgently with high suspicion of cancer who have their FSA within 31 days
Q3 2012/13 194 74% 116 77% 14 74% 244 72% 568 74%
Q4 2012/13 203 83.5% 90 85% 32 94% 203 69% 258 78%
Q1 2013/14 210 82% 71 80% 35 95% 239 78% 555 81%
Notes:o Caution required for interpretation of above data – FCT data capture is still in development stage and data is incomplete.o Midland DHBs had 3,883 cancer registrations for 2010. Refer to MCN Executive FCT reporting detail analysis
Midland improving colonoscopy wait times indicators
July - September 2013 Urgent Colonoscopy Non-Urgent Colonoscopy Surveillance Colonoscopy
Patient waiting at the end of the month and exited during the quarter
Patient waiting at the end of the month and exited during the quarter
Patient waiting at the end of the month and exited during the quarter
DHB Waiting & scoped within
14 days
Total waiting and scoped
% within 14 days Waiting & scoped within 28
days
Total waiting and scoped
% within 28 days Waiting & scoped within 84
days
Total waiting and scoped
% within 84 days
BOP 66 123 54% 618 1713 36% 297 1177 25%
Lakes 35 61 57% 276 442 62% 107 199 56%
TDH 13 36 36% 181 245 74% 25 33 76%
Waikato 115 290 40% 789 2967 27% 158 291 54%
Midland Total 229 510 45% 1864 5367 35% 587 1700 35%
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 63

October 2013 YTD Urgent Colonoscopy Non-Urgent Colonoscopy Surveillance Colonoscopy
Patient waiting at the end of the month and exited during the quarter
Patient waiting at the end of the month and exited during the quarter
Patient waiting at the end of the month and exited during the quarter
DHB Waiting & scoped within
14 days
Total waiting and scoped
% within 14 days Waiting & scoped within
28 days
Total waiting and scoped
% within 28 days Waiting & scoped within
84 days
Total waiting and scoped
% within 84 days
BOP 17 48 35% 223 691 32% 92 567 16%
Lakes 21 27 78% 80 130 62% 29 75 39%
TDH 2 6 33% 50 97 52% 5 7 71%
Waikato 41 115 36% 289 793 36% 50 94 53%
Midland Total 81 196 41% 642 1711 38% 176 743 24%
Note: Quarter one is complete and Quarter two there is only October data available (November and December data available 11 February 2014). MoH electives team say that we are to use October data as ytd and report against this so the enclosed second table is October only.
Cardiac Network Nationally Established and Regional Reported Targets – 2012/13:Target 1. Acute Coronary Syndrome (ACS)
1.1 >70% of high risk Acute Coronary Syndrome patients accepted for coronary angiography receive it within 3 days of admission (Day of admission=Day 0)By Facility:
By Midland region: (Picture is already updated for Q4 report)
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 64

1.2 >95% of patients presenting with Acute Coronary Syndrome who undergo coronary
angiography have completion of ANZACS QI ACS and Cath/PCI registry data collection within 30daysBy Facility:
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 65

Target 2. Additional Measures2.1 For coronary angiography - 85% of accepted referrals for elective coronary angiograms will receive their procedure within 3 months (90 days) and no patient will wait longer than five
months-Data will be updated for Q4
2.2 For percutaneous revascularisation a target of 12 per 10,000 of population will be achieved
0
5
10
15
20
25N
elso
n M
arlb
orou
gh
Sou
ther
n
Wai
tem
ata
Can
terb
ury
Cap
ital a
nd C
oast
Hut
t Val
ley
Cou
ntie
s M
anuk
au
Sou
th C
ante
rbur
y
Auc
klan
d
Haw
kes
Bay
Wha
ngan
ui
Nor
thla
nd
Wai
kato
Wes
t Coa
st
Taira
whi
ti
Wai
rara
pa
Mid
Cen
tral
Bay
of P
lent
y
Lake
s
Tara
naki
Nor
th
Mid
land
Cen
tral
Cen
tral S
ub-r
egio
n
Cen
tral i
ncl N
MH
Sou
th e
xcl N
MH
Sou
th
Dis
char
ges
per 1
0,00
0 Po
pula
tion
DHB of Domicile
Standardised Discharge Rate per 10,000 National Discharge Rate per 10,000 Raw Discharge Rate per 10,000 2012/13 National Target Discharge Rate per 10,000
Year Ended 31 Dec 2013
Angioplasty Intervention Rates - All Admission Types
2.3 For coronary angiography services, a target of at least 33.9 per 10,000 of population will be achieved
0
5
10
15
20
25
30
35
40
45
50
Wai
tem
ata
Tara
naki
Sou
ther
n
Can
terb
ury
Haw
kes
Bay
Nel
son
Mar
lbor
ough
Auc
klan
d
Wai
kato
Wha
ngan
ui
Mid
Cen
tral
Nor
thla
nd
Taira
whi
ti
Hut
t Val
ley
Cou
ntie
s M
anuk
au
Sou
th C
ante
rbur
y
Bay
of P
lent
y
Lake
s
Cap
ital a
nd C
oast
Wes
t Coa
st
Wai
rara
pa
Nor
th
Mid
land
Cen
tral
Cen
tral S
ub-r
egio
n
Cen
tral i
ncl N
MH
Sou
th e
xcl N
MH
Sou
th
Dis
char
ges
per 1
0,00
0 Po
pula
tion
DHB of Domicile
Standardised Discharge Rate per 10,000 National Discharge Rate per 10,000 Raw Discharge Rate per 10,000 2012/13 National Target Discharge Rate per 10,000
Year Ended 31 Dec 2013
Angiography Intervention Rates - All Admission Types
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 66

3.1 For cardiac surgery a minimum target intervention rate of 6.5 per 10,000 of population will be achieved.
0
1
2
3
4
5
6
7
8
9
10
Wai
kato
Tara
naki
Wai
tem
ata
Wha
ngan
ui
Sou
ther
n
Nor
thla
nd
Bay
of P
lent
y
Lake
s
Taira
whi
ti
Auc
klan
d
Can
terb
ury
Cou
ntie
s M
anuk
au
Wai
rara
pa
Hut
t Val
ley
Sou
th C
ante
rbur
y
Wes
t Coa
st
Haw
kes
Bay
Nel
son
Mar
lbor
ough
Mid
Cen
tral
Cap
ital a
nd C
oast
Nor
th
Mid
land
Cen
tral
Cen
tral S
ub-r
egio
n
Cen
tral i
ncl N
MH
Sou
th e
xcl N
MH
Sou
th
Dis
char
ges
per 1
0,00
0 Po
pula
tion
DHB of Domicile
Standardised Discharge Rate per 10,000 National Discharge Rate per 10,000 Raw Discharge Rate per 10,000 2012/13 National Target Discharge Rate per 10,000
Year Ended 31 Dec 2013
Cardiac Surgery Intervention Rates for Patients Aged 15 Years and Over - All Admission Types
3.2 The waiting list for cardiac surgery will remain between 5 and 7.5% of annual cardiac throughput, and not exceed 10% of annual throughput (Waiting list target - managed via Elective services reporting)-Data will be updated for Q4
3.3 95% data completion into National Cardiac surgery database within 30 days post discharge.-No Purchase of Dendrite by Midland DHBs to date.
4.1 90% of eligible population have a CVD risk assessment within the last 5 years
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 67

4.2 Identify number of high risk patients that are receiving treatment within the midland region for:
1: Aspirin therapy, 2: Statins therapy, 3: BNP assay in assessment of suspected Heart Failure
Elective Services
1. Electives Health Target – Minimum Discharges The Midland region will deliver 31,623 elective services discharges to meet each DHB’s electives health target. The table below displays the 2013/14 health target, and shows the comparison to the 2012/13 year, including the increase required
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 68

Table 1: Electives Health Target - Minimum Discharges
DHB 2012/13 Health Target2013/14
Health Target Increase RequiredBay of Plenty 8,357 8,443 86Lakes 3,607 3,659 52Tairawhiti 2,026 2,026 0Taranaki 4,156 4,264 108Waikato 13,009 13,231 222Midland Total 31,155 31,623 468
2. Joint, Cataract and Cardiac RequirementsThe following three tables display the minimum required number of procedures to meet joint, cataract and cardiac intervention rates. Rates are standardised for age, gender, ethnicity and social deprivation. Note: These are minimum requirements
Table 2: Targeted Funding Increases – Electives Investment - JointsJoints - Rate of 21 per 10,000
DHB Total required 2013/14 Minimum to be funded under EIBay of Plenty 576 223Lakes 232 117Tairawhiti 111 39Taranaki 285 116Waikato 850 427Midland Total 2054 922
Table 3: Targeted Funding Increases – Electives Investment - CataractsCataract - Rate of 27 per 10,000
DHB Total required 2013/14 Minimum to be funded under EIBay of Plenty 740 244Lakes 289 77Tairawhiti 143 15Taranaki 361 9Waikato 1075 196Midland Total 2608 541
Table 4: Targeted Funding Increases – Electives Investment - CardiacCardiac - Rate of 6.5 per 10,000
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 69

DHB Total required 2013/14 Minimum to be funded under EIBay of Plenty 170 80Lakes 72 25Tairawhiti 35 8Taranaki 84 26Waikato 257 52Midland Total 618 191
3. Bariatric Surgery ProceduresThe National Health Board has outlined the following expectations related to bariatric surgery procedures. Firstly, that a regional plan will be developed and implemented to ensure equity in access to, and delivery of, bariatric surgery. The second expectation is that at least the following volumes of bariatric surgery procedures will be completed for each DHB population.
Table 5: Bariatric Volumes
DHB Base Additional TotalBay of Plenty 1 6 7Lakes 1 3 4Tairawhiti 0 2 2Taranaki 1 3 4Waikato 12 9 21Midland Total 15 23 38
4. Reduced Waiting TimesThe Midland region will reduce waiting times in accordance with Elective Services Patient-flow Indicators (ESPIs) as follows
Table 6: ESPI TargetsReduce waiting times TargetESPI 2: No patient waiting longer than five months for their first specialist assessment, then four months by December 2014 100% compliance
ESPI 5: Patients given a commitment to treatment to receive treatment within five months, then four months by December 2014 100% compliance
5. Develop a Midland region approach to elective services
Develop and implement a regional approach for elective services1. To develop and agree business rules for moving patients between DHBs, such as;
1.1 Referral process, including communication with referrers and patients 1.2 Clinical prioritisation - access thresholds and scoring tools1.3 Pre and post-operative care management including complications management1.4 Diagnostics1.5 Transport1.6 Supply of equipment 1.7 Post discharge nursing and support services1.8 Funding model(s)
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 70

2. To develop a regional elective services production plan to facilitate regional elective services coordination and planning. This will allow the Midland region to develop a regional elective services production plan based on relevant information from each DHB, such as;
DHB Elective health targets DHB production plans Standardised intervention rates DHB elective services contracts and funding Capacity and sub-specialty of surgeon, and theatre capacity (theatre sessions,) Referrals Wait times
2. Implement/agree consistent scoring tools and thresholds 3. Develop a regional model showing volumes for the various procedures groups 4. Develop reporting mechanisms and dashboards to report progress to each DHB that details
Number of referrals for each procedure group; year-to-date and compared to plan Numbers of surgery by procedure group completed compared to plan Number of people coming on to waiting list, number exiting, and waiting times Other reporting as agreed
Stroke Network The Network continues to work on key audits – there are still are a number of issues with data collection and we continue to make small changes to ensure information reviewed is accurate. The graphs below provide the thrombolysis rates and stroke unit utilisation rates for the Midland DHBs in the first quarter. Lakes DHB is currently not offering a thrombolysis service and TDH had six stroke presentations who were not thrombolysed because: two patients woke with stroke symptoms, two presented at greater than four hours from onset of symptoms to ED and two patients presented to ED with stroke symptoms longer than 24 hours.
80 percent of stroke patients are admitted to a stroke unit or organised stroke service with demonstrated stroke pathway
0%
20%
40%
60%
80%
100%
120%
Q3 2012/2013 Q4 2012/2013 Q1 2013/2014 Q2 2013/2014
Stroke Audit 1: % of all Stroke Pts. being cared for in a Stroke Unit
Target
Waikato
Tauranga
Taranaki
Rotorua
Gisborne
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 71

6% of potentially eligible stroke patients are thrombolysed
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
16.00%
18.00%
20.00%
Q3 2012/2013 Q4 2012/2013 Q1 2013/2014 Q2 2013/2014
Stroke Audit 2: % of Acute Ischaemic Stroke Patients Thrombolysed, Midland Region by presenting Facility
Waikato
Tauranga
Taranaki
Rotorua
Gisborne
space
Target
Child Health Action Group Increased immunisation rates Data will be updated for Q4
Reduced rates of rheumatic fever Data will be updated for Q4
Lower rates of SUDI Data will be updated for Q4
Greater co-ordination of resources across the region
Improved ASH Rates
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 72

Rheumatic Fever 2013/14 Target rheumatic fever number and rate reductions 10% below national average
Area Number Rate
Midland region 32 3.8
New Zealand 168 3.7
2013/14 Measures – Vulnerable services
Maternity Action Group Increasing number of women registering with an LMC by 12 weeks by 2016
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 73
Progress towards 90% of pregnant women who identify as smokers at the time of confirmation of pregnancy in general practice or booking with a lead maternity carer are offered advice and support to quit.
Renal Action Group
Agreed regional KPIs to be included in the 2014-2018 Regional Renal Services Plan:
RSP Measures: 1: > 85% of transplant patients completing work up within 4 months. This being
time from first meeting the transplant co-ordinator and requesting the recipient evaluation to being referred to ARTG for assessment for listing for transplantation
2: ≥70% all prevalent dialysis patients to be home based3: Average length of stay, per patient, per annum (per DHB of domicile) where the primary admission diagnosis is renal failure (N17-N19)4: ≥70% all non-late presentation patients start dialysis with long term access reflecting the patient’s modality choice
Regional Scorecard Measures:1: The number of late presentation patients for RRT to < 20% of the total number of patients who commence RRT measured each quarter.2: ≤15% on long term HD have HD through central line3: PD peritonitis rate >1:36 patients months4: new PD catheter function rate at 30/7 > 90%5: >20% of all dialysis patients are listed for kidney transplant6: >15% of all dialysis are actively listed for kidney transplant7: <5% DNA rate per DHB for renal OPD clinics8: Increased standardisation of regional renal nursing practices
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 74

Health of the Older Person Action Group Reducing readmission rates for 75+ within 28 days into acute services*
Reduce new admissions to ARC for 75+ within a month of discharge from acute services - Source of data has not yet been identified
Reduce ASH Rates
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 75

*Acute services in this document refers to services within secondary/tertiary hospital settings. Access is through any referral pathway e.g. elective surgery, ED, outpatients etc.
Radiology Network - All measures outlined apply to the Bay of Plenty DHB, Lakes DHB, Tairawhiti DHB, Taranaki DHB, and Waikato DHB1: National Indicators MoH National Radiology Indicators
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 76

CT MOH Target: Improving Waiting Times for Diagnostic Services for Community and Outpatient Referrals: CT
Comments: Tairawhiti and Lakes are having no problem Taranaki (Blue) has improved significantly. BOP has reduced delivery below the target in the past quarter Waikato has the most improvement to do to move from 65% to 85%
85% of accepted referrals for scans receive their scan within 6 weeks (42 days).
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
CT Midlands KPI - 85% of accepted referrals for Community and Outpatient scans to receive their scan within 6 weeks (42 days)
TARGET
Waikato
BOP
Taranaki
Lakes
Tairawhiti
Improving Waiting Times for Diagnostic Services for Community and Outpatient Referrals: MRI
Comments: All 5 DHBs performance was reduced in February with no obvious explanation Tairawhiti, Lakes, BOP and Taranaki generally achieve the target but all
experience variability Waikato has significant improvement t do for move from 40% to 74%
75% of accepted referrals for scans receive their scan within 6 weeks (42 days).
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
MRI - Midlands KPI - 75% of accepted referrals for Community and Out Patient referred scans receive their scan within 6 weeks
(42 days)
TARGET
Waikato
BOP
Taranaki
Lakes
Tairawhiti
2: Regional KPI’s Midland Region Radiology KPI’sDiagnostic Services for Inpatient and Emergency Department Referrals: All modalities 90% of accepted referrals to have their procedures completed within 24 hours
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 77
(CR, CT, MRI, Ultrasound, Fluoroscopy, interventional and Mammography imaging (excluding breast screening))
Comments: Midland DHBs have no problem completing IP and ED procedures within 24hrs of
referral, across all modalities
40%
50%
60%
70%
80%
90%
100%
110%
% IP
/ED
Proc
edur
es C
ompl
eted
<24
hrs
Regional KPI Radiology IP/ED Wait Times for 2012-2013Percentage of Procedures Completed within 24 hours of Referral - Target is 90%
Target
Waikato
BOP
Taranaki
Lakes
Tairawhiti
Diagnostic Services for Community and Outpatient Referrals: All modalities (CR, CT, MRI, Ultrasound, Fluoroscopy, interventional and Mammography imaging (excluding breast screening).
Comments: 4 Midland DHBs have no problem completing reports for OP and GP referrals
within 48 hrs of the examination being performed for 70% of patients Waikato DHB only achieves this for 55% of patients
70% of reports should be dispatched within 48 hours of procedure performed.
0%
20%
40%
60%
80%
100%
120%
% D
ispat
ched
with
in 4
8 hr
s of E
xam
inati
on
Perf
orm
ed
Radiology OP and GP Report Dispatch Times for 2012-2013Percentage of Reports Dispatched within 48 hours of examination performed - Target is 70%
Target
Waikato
BOP
Taranaki
Lakes
Tairawhiti
3:Primary Referred Indicator Primary Referred IndicatorsDiagnostic Services for Primary Referred: For CR and Ultrasound 65% of accepted referrals for scans receive their scan within 6 weeks (42 days).
Diagnostic Services for Primary Referred: For CT 85% of accepted referrals for scans receive their scan within 6 weeks (42 days).
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 78

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
SLAT CR - Midlands KPI - 65% of accepted referrals for Community referred plain films receive their Xray within 6 weeks
(42 days)
TARGET
Waikato
BOP
Taranaki
Lakes
Tairawhiti
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
SLAT CT - Midlands KPI - 85% of accepted referrals for Community referred CT scans receive their scan within 6 weeks (42 days)
TARGET
Waikato
BOP
Taranaki
Lakes
Tairawhiti
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
SLAT US - Midlands KPI - 65% of accepted referrals for Community referred US scans receive their scan within 6 weeks
(42 days)
TARGET
Waikato
BOP
Taranaki
Lakes
Tairawhiti
2013/14 Measures - Regional Activities
Smokefree Network
Outcome MeasureQ3-Results
BOP DHB Lakes DHB Tairawhiti DHB Taranaki DHB Waikato DHBTarget Target Target Target Target
2013/14Q3
2014/15 2013/14Q3
2014/15 2013/14Q3
2014/15 2013/14Q3
2014/15 2013/14Q3
2014/2015
Providing Smokers with Smoking Cessation advice and support - Hospitalised Total
99% 95% 93% 95% 91% 95% 95% 95% 93% 95%
90 percent of patients seen by a health practitioner in primary care are offered brief advice and support to quit smoking
82% 90% 54% 90% 47% 90% 63% 90% 51% 90%
90 percent of pregnant women who identify as smokers at the time of confirmation of pregnancy in general practice or booking with Lead Maternity Carer are offered advice and support to quit
90% 90% 90% 90% 90% 90% 90% 90% 90% 90%
Midland Regional Trauma System Regional Measures:
1) MRTS Trauma Guidelines agreed for use by Midland DHBs2) MRTS registry data input up-to-date within 12 weeks of data collection3) MRTS TQIP programme delivering regular quality reports to stakeholders4) Stakeholder communication plan operational5) Regional educational programme operational6) MIMRS is functional and sustainable7) Midland Trauma Research Unit functional and producing information for peer review
8) Mortality of severely injured (Injury Severity Score >15) is less than 10% in all Midland Hospitals
9) MRTS adequately staffed, funded, and in an optimal and sustainable state at the end of 2015National
Measures:1) Trauma registry and TQIP processes are functional and compatible with national
trauma systems and initiatives
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 79

2) National health agencies are regularly informed on the status and progress of MRTS.
Regional Emergency Departments 1) ED guidelines agreed for use by Midland DHBs and adopted across multiple DHBs2) Stakeholder communication plan operational3) Use of regional educational programmes
Key: Completed C On Track G Caution A In Trouble R
2013-14 Regional Services Plan – Midland Region DHBs 80





























