Embed Size (px)
Citation preview

8/14/2019 Microvascular Retractor a New Concept of.34
http://slidepdf.com/reader/full/microvascular-retractor-a-new-concept-of34 1/4
NEW INSTRUMENTATION
MICROVASCULAR RETRACTOR: A NEW CONCEPT
OF RETRACTING AND REPOSITIONING CEREBRAL
BLOOD VESSELS
A. Samy Youssef, M.D.,Ph.D.
Department of Neurosurgery,University of South Florida,
Tampa, Florida
Harry R. van Loveren, M.D.
Department of Neurosurgery,University of South Florida,Tampa, Florida
Reprint requests:A. Samy Youssef, M.D., Ph.D.,Department of Neurosurgery,
University of South Florida,Harbourside Medical Tower Suite 730,
4 Columbia Drive,Tampa, FL 33606.Email: [email protected].
Received, December 3, 2003.
Accepted, January 14, 2005.
OBJECTIVE: In this technical note, we report our results with a newly designedretractor blade that can be directly applied for the retraction and repositioning of cerebral blood vessels and delicate neural structures.
METHODS: This new malleable retractor with a semicircular tip was designed to fit in theflexible arms of a self-retaining retractor system. After prototype evaluation and optimiza-tion in laboratory studies, we used the new retractor in 15 patients during surgicalprocedures that included retraction of the internal carotid artery during aneurysm clipping,expansion of the surgical window, and transposition of cranial nerves.
RESULTS: No intraoperative injuries occurred to neurovascular structures. The retrac-tor blade remained stable on pulsating vessels during the procedure and largelypreserved the vessel diameter.
CONCLUSION: The new retractor incorporates the existing advantages offered by flexibleself-retaining retractor blades with those features that adapt to blood vessel retraction.Rather than concentrating force at one point as typical retractors do, the semicircular tipdistributes the retraction force over multiple points along its circumference.
KEY WORDS: Internal carotid artery, Microvascular, Retractor
Neurosurgery 57[ONS Suppl 1]:ONS-199–ONS-202, 2005 DOI: 10.1227/01.NEU.0000164457.86335.A3
Akey to successful neurosurgery is adequate exposure,of which a basic element is retraction. Every surgicalretraction instrument offers benefits with limitations.
Even ordinary retraction of brain tissue, which has been the
focus of extensive studies, results in injury to the brain if
overused. Since the introduction of the concept of neurovas-cular retraction, its evolution has involved continuous refine-
ments to reach an optimum design for a retractor system.
Different situations during microsurgical procedures neces-sitate retraction on neurovascular structures. In one of the best
examples, vascular retraction that is applied to the supracli-
noid internal carotid artery (ICA) during anterior cranial fossa
surgery aids in the visualization and dissection of ICA aneu-rysms (e.g., posterior communicating artery or anterior cho-
roidal aneurysms). Such retraction expands the opticocarotidor carotid-oculomotor window during resection of parasellar
lesions and expands the opticocarotid corridor (or mostly the
carotid-oculomotor corridor) to basilar artery aneurysms.However, brain retraction systems have been inappropri-
ately applied to cerebral blood vessels in terms of location of
retraction and their application in two-dimensional space. Ef-fective retraction requires positioning in three-dimensional
space. Additional limitations exist for the currently available
instruments for vascular retraction that include handheld re-tractors or mechanical self-retaining retractors with straightmicroretractor blades. Handheld retraction is usually per-formed by suction tips or microdissectors. The limitation
posed by gross muscle activity during handheld retraction isdisproportionate to the fine and precise movements involvedin microdissection or clipping of an aneurysm. Muscle fatigue
increases when the surgeon’s hand remains longer in a certainposition. Additionally, the existing straight microretractorsconcentrate the force of retraction through the retractor blade
to one point at the tip; this force might cause undue injurious
force to the vessel wall and narrowing of the vessel lumen. Ina report presented by Matsuyama et al. (2), direct retraction of
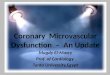
the ICA with a spatula caused its injury, especially in geriatricpatients with severe atherosclerotic changes. Distortion in-flicted by retraction on the vessel demonstrated in a computer-simulated model reported by Koyoma et al. (1) provided
further documentation about the harmful effects of retraction(Fig. 1, A and B).
Although self-retaining retractors should provide maximaldiscrete retraction and optimum tissue sparing, current instru-
NEUROSURGERY VOLUME 57 | OPERATIVE NEUROSURGERY 1 | JULY 2005 | ONS-199

8/14/2019 Microvascular Retractor a New Concept of.34
http://slidepdf.com/reader/full/microvascular-retractor-a-new-concept-of34 2/4
ment designs cannot achieve these requirements. In this tech-nical note, we describe a new microvascular retractor to over-come these previously mentioned limitations that wasdesigned and tested in collaboration with Schaerer MayfieldUSA, Inc. (formerly Ohio Medical Instrument Co.), Cincinnati,OH. We report on the effectiveness of this new microvascularretractor, which was developed in the cadaveric laboratoryand subsequently tested in the operating room.
PATIENTS AND METHODS
Technical Description
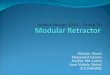
We designed a new retractor blade, from which a prototypewas developed (Fig. 2) by Schaerer Mayfield USA, Inc., to fit inthe flexible arms of the Budde halo self-retaining retractorsystem (Schaerer Mayfield USA, Inc.) The new retractor hasthe following properties: 1) it is malleable; 2) it comes in twodifferent lengths (9.14 and 11.2 cm) that can be adjusted ac-cording to depth of exposure; 3) it has a semicircular tip withrounded edges to disperse retraction pressure broadly acrossthe blood vessel wall. The 3-mm wide tip has three differentdiameters (3, 5, and 7 mm) based on anatomic studies per-formed by Saeki and Rhoton (3) , who reported that the ICA
diameter averages 4.3 mm(range, 2.5–7.0 mm) abovethe posterior communicat-ing artery.
Laboratory Testing
After prototype evaluation,we used this new retractor blade in the microsurgical lab-oratory to determine its effec-tiveness in the retraction of silicon-injected cadavericcere- bral blood vessels, especiallythe supraclinoid ICA. Optimi-zation focused on establishingthe design for the length, tipdimensions and configura-tion, ease of retractor applica-tion and removal, safety to blood vessel walls, and stabil-ity during procedures.
Clinical Experience
We documented the feasi- bility of this new retractor inclinical applications in 15 pa-tients who underwent surgi-cal treatment for 12 upper basilar artery aneurysms, 1pericallosal artery aneu-rysm, 1 foramen magnum
meningioma, and 1 petro-clival meningioma.During surgery of basilar
aneurysms, retraction on the
supraclinoidal ICA allowedthe expansion of the carotid-oculomotor or the opticocarotid
window in the transsylvian exposure of the aneurysms. In no
other situation is vessel repositioning more critical than in ex-pansion of the carotid-oculomotor window for clipping upper
basilar artery aneurysms. In the interhemispheric exposure of the
pericallosal aneurysm, retraction of the callosomarginal artery better exposed the aneurysm for clipping. In the foramen mag-
num meningioma exposed via a transcondylar approach, we
used the new retractor to mobilize and reposition the vertebralartery. Retraction of cranial nerves was possible with the new
device; for example, mobilization of the trigeminal nerve facili-
tated resection of a petroclival meningioma through a presig-moid approach.
In all 15 cases, we observed no intraoperative injuries to neuro-
vascular structures. The retractor blade remained stable on pulsat-ing vessels throughout the procedure, and the vessel diameter was
largely preserved. We detected no postoperative ischemia or infarc-
tions associated with the territories of retracted vessels.
FIGURE 1. A computer-generatedrepresentation showing the displacedartery and a retractor. A, original di-rection of the retractor is downward.The tip ofthe retractor is moved tothe
point that shows the minimum dis-tance (closed circle). The open cir-cle is the center of displacement. B,surface contours of the arterial modelafter displacement and morphologicalchanges.Thecenter of displacement isdetermined (open circle). The dis-tance between the point and each
polygon is calculated, and two pointsshowing the minimum and maxi-
mum distances (dmin and dmax)are determined (from, Koyama T,Okudera H, Kobayashi S: Computer-
generatedsurgical simulationof mor- phological changes in microstruc-tures: Concepts of “virtualretractor”—Technical note. J Neuro-
surg 90:780–785, 1999 [1]).
FIGURE 2. Photographs showing thenew microvascular retractor blades with asemicircular tip. A, blades come in threedifferent diameters (3, 5, and 7 mm). B,close-up view of the semicircular tip show-ing the 3-mm width (courtesy of the De-
partment of Neurosurgery, University of South Florida, Tampa, FL).
YOUSSEF AND VAN LOVEREN
ONS-200 | VOLUME 57 | OPERATIVE NEUROSURGERY 1 | JULY 2005 www.neurosurgery-online.com

8/14/2019 Microvascular Retractor a New Concept of.34
http://slidepdf.com/reader/full/microvascular-retractor-a-new-concept-of34 3/4
DISCUSSION
In this article, we report our results with a new retractor blade design for the direct retraction and repositioning of cerebral blood vessels, delicate neural structures (e.g., cranialnerves), or both. We believe the conformal design of thisretractor blade may reduce some of the risks associated withself-retaining brain retractors, such as impairment to regionalcerebral circulation, direct injury to atherosclerotic vessels,and thromboembolic complications that are caused by directretraction of cerebral blood vessels.
The proposed design incorporates the existing advantages of-
fered by flexible self-retaining retractor blades with those specificfeatures that adapt to blood vessel retraction. The shape of thenew microvascular retractor is adjustable, and the appropriatelength is selected according to the depth of the operative field.When compared with a typical retractor blade that concentratesforce at one point, the semicircular tip distributes the force of retraction over multiple points along its circumference. Thissemicircular tip may decrease the force applied to the vessel walland preserve the vessel lumen (Fig. 3B). This tip may anchor thevessel and permit its manipulation during retraction in the ver-tical and horizontal planes.
In our laboratory and clinical studies with this new retrac-tor, we achieved a wider working space with steady and saferetraction (Fig. 3, A and B). We used this retractor blade for thefollowing purposes. First, retraction of the ICA during micro-vascular procedures (e.g., aneurysm clipping) allowed thesurgeon use of both hands for dissection and clipping. Typi-cally, a surgeon must use one hand for dissection and clippingand the other hand for retraction. Second, expansion of theopticocarotid or carotid-oculomotor window was achievedduring tumor resection or clipping of basilar aneurysms.Third, transposition of cranial nerves was safely performedduring microsurgical procedures. After prototype develop-ment and testing, we have used the new microvascular retrac-
tor blade in the laboratory and operating room without tech-nical difficulty or surgical complications.
CONCLUSIONS
Direct vascular retraction is valuable in microneurosurgery
to achieve optimum exposure. With distribution of the retrac-tion force along the circumference of its semicircular blunt tip,the design of this new retractor blade avoided the risk of directinjury to vessel walls or regional cerebral ischemia. We suc-cessfully used this blade during surgery without anycomplications.
REFERENCES
1. Koyama T, Okudera H, Kobayashi S: Computer-generated surgical simula-
tion of morphological changes in microstructures: Concepts of “virtual re-
tractor”—Technical note. J Neurosurg 90:780–785, 1999.
2. Matsuyama T, Shimomura T, Okumura Y, Sakaki T: Mobilization of the
internal carotid artery for basilar artery aneurysm surgery. J Neurosurg
86:294–296, 1997.3. Saeki N, Rhoton AL Jr: Microsurgical anatomy of the upper basilar artery and
the posterior circle of Willis. J Neurosurg 46:563–578, 1977.
Acknowledgments
We gratefully acknowledge Siviero Aggazzi, M.D., Skull Base Fellow, who
assisted with the operative images. We thank Mary Kemper for editorial assis-
tance and Martha Cooper and Tonya Hines, medical illustrators, for their
valuable contribution to this article.
COMMENTS
In this report, the authors describe an innovative retractor that can beused to mobilize cerebral vessels during microsurgical procedures.
We commend Dr. van Loveren for his ongoing technical contributionsto the fields of cerebrovascular and cranial base surgery. Although theconcept of the need of vessel repositioning in certain situations is validand the design of the presented retractor is novel, we discouragereliance on self-retaining retractors. Based on the experience of thesenior commentator (MGY), wide splitting of the sylvian fissure andthe arachnoidal layers of the basal cisterns without the use of self-retaining brain retractors facilitates ample exposure and multipletrajectories. Using the latter technique, the internal carotid artery, forexample, can be mobilized intermittently medially or laterally usingthe side of a blunt tip microsuction while the surgeon maintains theability to use a microbipolar or microscissor with the other hand forfurther dissection or exposure.
M. Gazi Yasargil
Little Rock, ArkansasSaleem I. Abdulrauf
St. Louis, Missouri
Safe retraction of vascular (and neural) structures is a real technicalproblem during deep-seated microsurgical operations. To the best
of my knowledge, no special instrument has been created for that useup to this time. I agree that the retractor presented by the authors has
been designed according to logical bases and adheres to accurateergonomic principles. Good adjuncts to this preparatory work would
be flow measurements on the retracted arteries in clinical cases andhistological studies in animal experiments for nerves. In my practice,
FIGURE 3. Intraoperative microscopic photographs showing the supraclinoidICA and the upper basilar artery (BA) after dissection of arachnoid and incisionof the distal dural ring (A) and after placement of the microvascular retractorblade on the ICA between the posterior communicating artery (PCOM) andanterior choroidal artery (AChoA) (B). Note the increased exposure of the BAand PCOM added by lateral repositioning of the ICA while preserving the vesselcaliber. MCA, middle cerebral artery; ON, optic nerve; P1 and P2, posteriorcerebral artery proximal and distal to PCOM, respectively (courtesy of theDepartment of Neurosurgery, University of South Florida, Tampa, FL).
MICROVASCULAR RETRACTOR
NEUROSURGERY VOLUME 57 | OPERATIVE NEUROSURGERY 1 | JULY 2005 | ONS-201

8/14/2019 Microvascular Retractor a New Concept of.34
http://slidepdf.com/reader/full/microvascular-retractor-a-new-concept-of34 4/4
I like to use handheld, ball-tip, microsuckers (200005 Sindou Ball-point suction Kit, Lolbinger LP, Dallas, TX) for displacing and holdingapart vascular structures and, more rarely, cranial nerves. I prefer toperform retractions in a “mobile” way; this allows me to intermit-tently reduce tension on the retracted structures. However, the au-thors’ microretractor could be useful when a long-duration retractor is
required, especially if the surgeon’s second hand needs be used forpurposes other than holding retracting vessels (or nerves). The instru-ment designed by Youssef and van Loveren seems to be well adaptedto retraction of delicate vascular structures; nevertheless, I have someconcerns about its current use. Because it is semicircular to allow good“anchorage” of the vessel, I would fear a risk of stretching or eventearing-avulsing the retracted structure if abrupt involuntary dis-placement occurs during surgical maneuvers. This would be verysimilar with what may happen when using a too-closed semicircularhook for manipulating vessels or nerves. Placing a supplementaryinstrument in addition to spatula sucker, etc. into the operative fieldwould add to the overcrowding of the often narrow corridor to thedeep surgical target. Paradoxically, its purpose of making surgeryeasier could incline surgeons to perform long-steady retractions thatmight lead to impairment of vascular and above all neural structures.
Despite these concerns, I think that such a microretractor will be auseful complement in microsurgical kits.
Marc P. Sindou
Lyon, France
Youssef and van Loveren describe the design of a new retractor and itseffectiveness in the operatingroom.As we all know, all retractors can
certainly pose significant risk in the operating room. The authors took theinitiative to effectively develop a microvascular retractor in a cadaveric
laboratory before subjecting it to subsequent tests in the clinical arena.This new retractor was used in 15 cases, 12 of which involved upper
basilar artery aneurysms. One involved pericallosal artery aneurysm, one
foramen magnum meningioma, and one petroclival meningioma. Theauthors reported no intraoperative injury to neurovascular structures, nopostoperative ischemia, and certainly no infarction associated with terri-
tories of the retracted vessel. The advantage of this newly designedretractor blade rests in the round semicircular tip that distributes retrac-tion pressure broadly across the blood vessel wall. Other reported ad-vantages include availability of variable lengths, adjustability of theretractor’s shape, and its use with the Budde halo self-retaining retractor
system (OMI, Inc., Cincinnati, OH).
Peyman R. Tabrizi
Robert F. Spetzler
Phoenix, Arizona
The retractor described by Youssef and van Loveren seems to be agenial idea to render the vascular retraction softer and less dan-
gerous when it is necessary. For example, it could be important inmoving the vertebral artery during surgical removal of foramen me-
ningiomas or other pathology involving that area approached throughthe dorsolateral approach. In these cases, I already use the Budde haloself-retaining retractor system, applying it on the vessel using a microarm that terminates with a rounded edge. This, however, is notmalleable and often slides on the artery more than desired. I look
forward to this microvascular retractor appearing on the market, andI congratulate the authors for the brilliant idea.
Albino Bricolo
Verona, Italy
In-training Liaison
The Congress of Neurological Surgeons exists for the purpose of promoting public welfare through the advancement of neurosur- gery by a commitment to excellence in education and by a dedi-cation to research and scientific knowledge.
—Mission Statement, Congress of Neurological Surgeons
Inherent in this commitment is a critical charge to serve the needs of the in-trainingindividual. Considering the importance of this vital group within the neurosurgicalcommunity, the Journal has established a position within its board structure termedIn-training Liaison. The individual holding this position will act as a spokespersonespecially addressing the needs and concerns of individuals in in-training positionsglobally, as they relate to journal content and perspective.
The current individual holding this position is:
William J. Mack, M.D.
Issues attendant to in-training matters should be conveyed to Dr. William J. Mack atthe Department of Neurological Surgery, Columbia College of Physicians and Sur-geons, Neurological Institute of New York, 710 W. 168th Street, Box 64, New York, NY10032; email: [email protected].
YOUSSEF AND VAN LOVEREN
ONS-202 | VOLUME 57 | OPERATIVE NEUROSURGERY 1 | JULY 2005 www.neurosurgery-online.com