Embed Size (px)
Citation preview

Microlife: GPFrom your local Clinical Microbiology Team
O c t o b e r 2 0 1 2
In this edition we provide
an update on how to
diagnose Pertussis and
a d v i c e o n M R S A
decolonisation treatment in
the community.
We hope you find this
newsletter useful. Please
send any comments to:
Savita.gossain@heartofengland
.nhs.uk
WelcomePertussis on the increase
Laboratory Opening
Hours:
Mon - Fri: 7am - 7pm
Sat, Sun & Bank
Holidays: 8am - 4pm
Clinical enquiries:
Heartlands Hospital:
Microbiology Consultant
0121 424 3244
Good Hope Hospital:
Microbiology Consultant
07917 648323
Heartlands Hospital:
Virology enquiries:
Switchboard, bleep 2821
Out of Office Hours:
Switchboard
0121 424 2000
Whooping cough (pertussis) is a
notifiable, highly contagious,
acute bacterial infection of the respiratory
tract caused by Bordetella pertussis.1
It affects people of all ages and can
result in substantial morbidity and
mortality.
In the first 33 weeks of 2012 there have
been 5,657 cases, an eight-fold increase
from this time last year with eight reported
deaths. These deaths have all been in
young unimmunised infants.2
The highest numbers of confirmed cases
continue to be reported in the South East
and South West Regions but activity is
high across all parts of the country.
Why are rates increasing?
Several factors may account for the
apparent rise in pertussis cases, including
increased awareness, new diagnostic
methods and reduced potency of the
acellular pertussis vaccine compared to
the earlier whole cell vaccine. Previous
infection or vaccination does not
confer lifelong immunity to pertussis.
Infections with whooping cough in
vaccinated or previously infected patients
are likely to be milder.
How infectious is pertussis?
Up to 90% of non-immune household
contacts are likely to develop the disease.
It is spread by close contact with an
infected person. Patients are infectious up
to four days before the cough develops,
and for about 21 days following the onset
of symptoms.
What are the symptoms of pertussis?
Incubation period typically 7 - 10 days.
Patients initially develop a common
cold-like illness.
Outbursts of coughing (paroxysms)
within one to two weeks.
An inspiratory whoop.
Coughing bouts may be followed by
vomiting or apnoeic episodes.
Sufferers may produce thick, sticky,
clear sputum, that is often very difficult
to expectorate. This gradually worsens
and lasts over a period of 2-6 weeks.
Suspect pertussis in anyone with a
chronic paroxysmal cough, a ‘whoop’
is not always present.
Who is most at risk?
The highest incidence has been
observed in infants under 3 months.
These infants are too young to be
protected by immunisation, are at greater
risk of developing the disease and are
also at much greater risk of developing
complications, hospitalisation and death.
The DH recently introduced a temporary
programme to vaccinate pregnant women
against pertussis to protect their infants.3
Laboratory results:
For all results enquiries,
contact: 0121 424 3256 How to diagnose pertussis
For diagnostic purposes, the disease is divided into early (<2 weeks from start of symptoms) and late (>2 weeks).
Infants (if not requiring hospitalization) send culture swab (see overleaf)
Children over 12 months and
adults:
Early disease send culture swab (see overleaf)
Late disease send sample for serology (red toptube) NB: serology result only valid if not
vaccinated in the previous year

MRSA and Decolonisation
It is routine at the Heart of England NHSFoundation Trust to take a nose swab for MRSA
(Methicillin Resistant Staphylococcus aureus) fromall patients admitted to our hospitals
If the patient is positive they are treated with anantiseptic body wash and nasal cream(decolonisation treatment) whilst in hospital.
In some cases screening results may not beavailable until after the patient is discharged andtherefore your patient will not have had anytreatment. In these cases, we inform the patient andGP by automatic letter of a positive result so theneed for treatment can be assessed.
Most patients will not require any decolonisationtreatment and can be reassured that MRSA that wasdetected will go naturally. However, patients withlong standing illnesses, catheters, wounds and ivlines are at higher risk of developing an infection andwe would recommend they are prescribeddecolonisation treatment.
On completion of the 5 day course of de-colonisation, repeat swabbing is not usually required,unless clinically indicated.
There is an information leaflet advising patients onhow to use decolonisation treatment, and followingfeedback from GPs, these will, in future, be sent with
the letter to the practice.If you have any queries, comments or require
further advice please contact a member of theInfection Prevention and Control Team (0121 4241137) or Duty Microbiologist (see page 1).
MRSA Decolonisation treatment
Five days of anti-septic body wash Chlorhexi-dine Gluconate 4% Solution OD and a nasalcream Bactroban Nasal Ointment(Mupirocin 2% Nasal Ointment) TDS usedas follows:
The body wash should be used as a liquidsoap and applied directly on to the skin (notdiluted).
The patient should preferably shower or bathe daily and wash their hair twice in the5 day period with Chlorhexidine.
A small amount of the nasal cream shouldbe applied to the inner surface of each nos-tril TDS for the 5 day period.
N.B. For patients allergic to Chlorhexidine,Octenisan Wash Lotion can be used as analternative in same way as above.
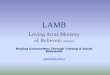
How to take a pernasal swab
A pernasal swab must be takencorrectly to ensure an accuratediagnosis of pertussis can bemade. Swabs can be orderedfrom Pathology Stores in theusual way.
1. Remove cap from media tube
by twisting.
2. Gently insert the fine, flexible
pernasal (turquoise top) swab
along the floor of the nasal cavity
until it touches the posterior naso-
pharynx & rotate 2-3 times before
withdrawing. If obstruction is en-
countered, withdraw and re-insert
through other nostril.
3. Insert the swab into the me-
dia tube.
4. Ensure the swab is labelledaccurately along with the com-
pleted request form. Send to lab ASAP.
Notification of pertussis
In all patients that you suspect
have whooping cough notify your
regional HPU immediately on
0844 225 3560.
DO NOT wait for a laboratory
diagnosis and confirmation.
How to treat pertussis
For suspected, epidemiologi-cally linked or confirmed cases,recommended antibiotic regimensaccording to the age of the patientare available on the HPA website(Ref.1).
Erythromycin, clarythromycin,azithromycin and co-trimoxazoleare all recommended but differ according to the age of the pa-tient.
Antibiotics should be adminis-tered as soon as possible after onset of illness in order to eradi-cate the organism and limit ongo-ing transmission.
Pertussis increase ctd...
References
1.HPAGuidelines.http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1287142671506; 2. Health Protection Agency. Pertussis
notifications and deaths. http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1317133571994; 3. https://www.cas.dh.gov.uk/
ViewandAcknowledgment/ViewAlert.aspx?AlertID=101844
Sagittal section of the nasal airway,reproduced from Medical Microbiology Testing in Primary Care, MansonPublishing.