Embed Size (px)
Citation preview

Acta Astronautica 56 (2005) 839–850
www.elsevier.com/locate/actaastro
Microbiological status of cosmonauts during orbital spaceflights onSalyut and Mir orbital stations
V.K. Ilyin ∗
RF SRC Institute for Biomedical Problems RAS, 76a Khoroshevskoye Shosse, Moscow 123007, Russian Federation
Available online 29 March 2005
Abstract
The main feature of the human–microorganism eco-system forming in the environment of manned space vehicles is theperiodic accumulation of the potential for pathogenicity. This process is characterized by the activation of opportunisticpathogens, representatives of which grow in large number within the system, settle in various niches, and demonstrateexpansion, intruding into microbiocenoses of open biotopes of humans who, until contamination, have been clean of thesemicroorganisms. Clones (similar to hospital strains) arising out of these populations exhibit the ability to spread “epidemically”within isolated teams.© 2005 Elsevier Ltd. All rights reserved.
1. Introduction
The 21st century was marked by the penetration ofhumans into secluded areas both on Earth and in thenear-Earth space, as a result of intensive interaction ofbiosphere laws with the human mind. The explorationand utilization of both deep water environments andouter space require the immediate involvement of hu-mans who have to face increasingly heavy emotionaland physical stresses while in these environments.In addition, occupations associated with increasedneuroemotional strain also tended to increase in num-ber. These can be exemplified by the introductionand operation of new vintages, developmental testing
∗ Corresponding author. Tel.: +7 095 1950025;fax: +7 095 1952253.E-mail address:[email protected].
0094-5765/$ - see front matter © 2005 Elsevier Ltd. All rights reserved.doi:10.1016/j.actaastro.2005.01.009
of different items, etc. Progressive urbanization andunfavorable environments are felt keenly by the humanorganism, which responds by changing the homeo-static parameters; in turn, these changes cause strain tothe systems controlling adaptation that steadily mod-ify metabolic and physiological processes. Changes inmetabolism due to extended exposure to extreme fac-tors occur in the systems controlling adaptation thatare specifically sensitive to a given external agent.
As the duration of space missions continues tolengthen, the problem of protecting crews aboardlong-operating stations from infections becomes ofparamount importance. We can anticipate a high in-tensity of development of nosocomial strains on theInternational Space Station, where full or partial ro-tation of crews coming from different spots of theworld will be a frequent event. On the other hand,

840 V.K. Ilyin / Acta Astronautica 56 (2005) 839–850
there are indications of definite inhibition of coloniza-tion resistance in spacecrews on mission. This dictatesthe necessity to search for effective ways to strengthenthe colonization resistance in spacecrews. Analysis ofthe data on the probiotic correction of human mi-croflora in an artificial climate constitutes a part of thiswork [1].
Safety from infection in space flight is one of themajor issues of the spacecrew medical support pro-gram. After many years of research, investigators inthis discipline demonstrated the activation of humanopportunistic pathogens during stays in pressurizedmodules designed for different purposes. Many au-thors point to the high probability of infectious dis-eases in the specific environment of space vehicles. Itwas emphasized that crew automicroflora can be anagent of infection. The distinguishing feature of thesemicroorganisms is the ability to provoke infectiousdiseases under certain conditions, particularly againstdegraded immunologic reactivity and the unique mi-crobiological community establishing in pressurizedhabitats. In these cases, the main etiologic agents ofinfectious diseases are human microflora and, possi-bly, cross-infection when an agent is imparted froma carrier to a susceptible organism. Two types ofinfection sources can be considered—anthropogenicand non-anthropogenic. As for the first type ofinfections, these are predominantly obligate andopportunistic pathogens carried by humans in aclosed environment.
Investigations of human microflora before and afterspace flight were first attempted by Alekseeva[1]. Ex-perimental data of this author suggested certain shiftsin the composition of oral, fauces, and cutaneous mi-croflora of the Vostok crews. The possibility of ad-verse shifts in spacecrew microflora was verified innumerous model studies with isolation of human vol-unteers in closed environments. Of much interest weredata from the 18-day mission aboard the space vehicleSoyuz-9 in 1970. Results of the investigations showedthat, after landing, the most profound changes leadingto dysbacteriosis had occurred to the nasal and cuta-neous microflora.
The review devoted to results of the US Apolloprogram[2] stated shifts in composition of cutaneousmicroflora toward prevalence of gram-positive cocci(Staphylococci and Streptococci), partial suppressionof anaerobic microbes, and temporary colonization of
the upper respiratory tracts by exogenous microorgan-isms, largely Staphylococci, due to, perhaps, micro-bial interchange.
Based on the literature, a list of microorganismsthat may trigger infectious diseases of a cosmonaut’srespiratory tract and integument can be defined. Tobegin with, these will be pathogenic Staphylococci,Streptococci, and representatives of the Enterobacteri-aceae family;Clostridium, Pseudomonas aeruginosaand fungi will enter the list, too.
During life on a space station, the composition ofthe normal microflora of cosmonauts alters signif-icantly; this results in deterioration of their body’sresistance to infectious agents. Thus, in the one-yearexperiment with medical/engineering human subjectsthe intestinal bifidobacteria and lactobacilli werefound to sharply decrease and then disappear, enzymeand antagonistic activities were reduced, colibacillusstrains were exchanged, and some organisms exhibitedincreased toxicity. Microbiological findings of ground-based simulations were supported by results of inves-tigations in real space flights. For instance, accordingto Taylor [2], examination of the Apollo and Skylabcrews evidenced loss in anaerobic and gain in aer-obic microorganisms of various types. Of particularvalue are data concerning isolation of opportunisticpathogenics likeStaphylococcus aureus, Klebsiellaphneumoniae, P. aeruginosa, and Enterobacteriaceaefrom cosmonauts. The importance of these investi-gations has been confirmed by recent data indicatingthat these are the microbes that give rise to a numberof infectious diseases. In view of the above, spe-cial emphasis should be placed on the principles ofchemotherapy of spacecrews afflicted with infection,and the sensitivity of bacterial cultures to antibi-otics. The sensitivity to antibiotics of opportunisticpathogens isolated from crew members in 7- and96-day space flights was noted to have changed.
In a 7-day space flight, one cosmonaut was foundto haveS. aureuswith significantly strengthened re-sistance to antibiotics (penicillin G, ampicillin, olean-domycin, lincomycin). Minimal retaining concentra-tions of the drugs grew from 10 to 100 times duringthe flight but returned to baseline values after. In a 96-day space flight, selection of tetracycline and ampi-cillin resistant Staphylococci in one of the crew mem-bers was thought to be most probably associated withadministration of ampicillin by a crew member and

V.K. Ilyin / Acta Astronautica 56 (2005) 839–850 841
transmission of the ampicillin-resistant strain to an-other. Colibacilli displayed similar changes in antibi-otic sensitivity.
Changes in antibiotic sensitivity were attributed tomodification of microbial cell ultrastructure of the typeobserved in Proteum, specifically.
However, investigators considered R-plasmid trans-mission to be the most probable cause for changes inantibiotic sensitivity in cosmonauts, the more so asfeatures of medicinal resistance were easily transmit-ted to recipient strains in the laboratory.
During long-time stays of humans in a space cabinor in isolation and confinement, the microflora of crewmembers is to a degree influenced by ecological fac-tors, since these conditions instigate formation of eco-systems comprising biogenous and abiogenous com-ponents. Within these systems, humans are the centralcomponent.
Results obtained during many years of operatingorbital stations Salyut 6 and 7 indicate that microbio-cenoses of mucous membranes in the nose, mouth, andthroat develop in space. As a rule, there are signs ofthe activation of opportunistic pathogens representedby Staphylococci and gram-negative bacteria. As forStaphylococci, these signs included growth in sizeand the emergence of new residences of pathogenicStaphylococci as a result of colonization by exogenouscultures brought in by other crew members or visitingcrews. In several cases out of heterogeneous popula-tions ofS. aureusvegetating in open biotopes of cos-monauts, strains of a certain biotope would separate,distinguished by the ability to spread “epidemically”in isolated groups of people as attested to by tran-sient carriage by new hosts. Considering that strainsof S. aureusproduced toxins and, consequently, initi-ated immunologic shifts in the recipient organism, thistransient carriage can be qualified as a non-manifestedform of Staphylococcal infection. Clinical symptomsthat had been developed in several cases could beprovoked by some other non-specific damaging orasthenizing factor. In addition, a characteristic shiftin human microbiocenoses during space flight wasthe contamination of mucous membranes in the nose,mouth, and throat, and, though not so frequently, in-tegument, by gram-negative bacteria that was aliento them, (e.g.,Proteus, Klebsiella, Enterobacter, Cit-robacter, andEscherichia coli, all notorious for beingagents of nosocomial infection).
Parallel to these shifts in spacecrew microflora, theinterior and equipment of the space stations turnedinto specific sites of accumulation and proliferationof microbes, beginning with gram-negative bacte-ria and molds referred to the so-called pathogenicsaprophytes.
2. Materials and methods
2.1. Collection of microbial samples from crewmembers and laboratory procedures
2.1.1. Mouth and throat, nose, axilla, groin, scapula,urine, feces
Swabs with sampled microbes were immersed andstirred into 2 ml of physiological solution; a series ofstandard 10-fold dilutions was prepared and inoculatedon the following compact nutrient media:
• 5% Hottinger blood agar (total aerobic bacteriacount in biotope),
• mannitol-salt agar (aerobically and anaerobicallycultivated Staphylococci),
• Endo agar and hectoene agar (gram-negative bac-teria),
• McConkey agar (enterococci),• Sabouraud agar (yeast and yeast-like fungi),• MRS agar (anaerobically cultivated lactobacilli).
2.1.2. InoculationMouth: Four successive dilutions by adding 0.5 ml
of original suspension or washout to 4.5 ml of phys-iological solution. Preparation of further dilutions byway of adding 0.5 ml of preceding dilution to 4.5 mlof sterile physiological solution. Distribution of 0.1 mlof original suspension of the mouth sample and twosubsequent dilutions across mannitol-salt, McConkeyand hectoene agars, Endo, Sabouraud, and MRS me-dia. Distribution of 0.1 ml of dilutions 3 and 4 across5% Hottinger blood agar.Nose: Two successive dilutions as described above.
Microbial inoculation of original suspension and twodilutions on 5% blood agar, mannitol-salt and hectoeneagars, and Endo and Sabouraud media.Groin: Two successive dilutions as described above.
Microbial inoculation of original suspension andtwo dilutions on 5% blood agar, mannitol-salt and

842 V.K. Ilyin / Acta Astronautica 56 (2005) 839–850
hectoene agars, Endo and Sabouraud media. Seeincubation procedure in section Armpit.Axilla: Axilla microbial samples will be treated as
described in sectionGroin.Scapula: Scapula microbial samples will be treated
as described in sectionGroin.Hand: Hand microbial samples will be treated as
described in sectionGroin.Ear: Ear microbial samples will be treated as
described in sectionGroin.Feces: Nine successive dilutions by way of adding
0.5 ml of original suspension or washout to 4.5 ml ofphysiological solution or phosphate buffer. The fol-lowing nutrient and selective diagnostics media wereused for the drop method of inoculation:
• Anaerobes: Blaurock (bifidobacteria), Wilson-Blair(Clostridium), MRS (lactobacteria), neomicine-containing medium (bacteroids).
• Aerobes: MSA (Staphylococci), Kalina’s (ente-rococci), Endo and McConkey (enterobacteria),modified Simmons with citrate, malonate and in-osite (opportunistic pathogenic enterobacteria),Sabouraud (yeast-like fungi and yeast), Proteusselective medium, 5% Hottinger blood agar (totalaerobes).
2.1.3. Incubation protocol
• 24- and 48-h incubation of inoculums on 5% Hot-tinger blood agar.
• 48-h incubation of inoculums on Endo medium,mannitol-salt, hectoene and McConkey agars, mod-ified Simons with citrate, malonate and inosite, Pro-teus selective medium.
• 48- and 72-h incubation of inoculums on Sabouraudagar.
• 72-h incubation on Blaurock (bifidobacteria),Wilson-Bler (Clostridium), MRS (lactobacteria),neomicine-containing medium (bacteroids).
On completion of incubation in thermostat, newlyformed colonies of microorganisms were countedand pure cultures for subsequent identification wererecovered. Identification of gram-positive and gram-negative microorganisms (aerobes and facultativeanaerobes) was performed in consultation withBergey’s Manual.
2.1.4. The determination of disbacteriosisThe 1st degree dysbacteriosis (D1)—shifts in the
aerobic part of intestinal microflora—increase or re-duction in theEscherichiapopulation; lacto- and bi-fidoflora unaltered.
D2—slight loss in bifidoflora and appearance ofopportunistic pathogenic enterobacteria.
D3—slight reduction in the amount of bifidobacte-ria and lactoflora, and sharp change in the populationof the enterobacterial family.
D4—no bifidoflora. Material depopulation oflactoflora; activation of opportunistic pathogens (Pro-teus, Clostridium, yeast-like,Staphylococcus aureus,Esherichiawith changed enzyme activity).
2.1.5. Evaluation of antibiotic sensitivity of isolatesGram-positive cocci and rods(Antibiotics and an-
timicrobial agents): tetracycline, doxicycline, ampi-cillin, carbenicilline, oxycillin, neomycin sulfate,gentamycin, streptomycin, erythromycin, linkomycin,oleandomycin, ristomycin, rifampicin.Gram-negative rods(antibiotics and antimicrobial
agents): tetracycline, doxicycline, ampicillin, carbeni-cilline, oxycillin, neomycin sulfate, gentamycin, strep-tomycin, erythromycin, chloromycetin, polymyxin,furazolidone, nalidixic acid, 5-HOK, cephalo-sporins.Methods of antibiotic susceptibility testing:
• Agar diffusion (disks)• Minimal retaining concentrations:
(i) with fixated concentrations,(ii) method of gradient plates (for cases of super-
high (above 500�g/ml) sensitivity to antibi-otics (Navashin, and Fomina, 1982)).
2.1.6. Genetic analysisPlasmid transfer by bacterial conjugation: fresh
agarinic cultures with wild plasmids isolated fromtest-subjects and carrying determinants of resistanceto a broad range of antibiotics belonging to differ-ent groups of chemicals (ampicillin, carbenicilline,kanamycin, chloramphenicol, tetracycline) and freshagarinic culture ofE. coli strain C-600 displayingsensitivity to all antibiotics with the exception ofnalidixic acid were incubated for 24 h at 37◦C. Afterincubation, conjugation mixtures were prepared of

V.K. Ilyin / Acta Astronautica 56 (2005) 839–850 843
1 ml of donor culture with 1× 109 CFU/1 m and 1 mlof recipient culture at the same concentration.
Following the introduction of 3 ml of Hottingerbroth, the mixture was exposed to the pre-incubationconditions for 24 h. After incubation, mixtures wereinoculated in Petri dishes containing Endo mediumwith two antibacterial agents to select transconju-gates: one of the antibiotics ineffective with respectto the donor strain and nalidixic acid at the concen-tration of 100�g/ml. Colonies of transconjugates inincubated dishes were counted “pro-recipient”.
3. Results
3.1. Special and quantitative characteristics ofcosmonauts’ microflora
The data reveal that in the period prior to launch theamount of potential pathogens increases in human cov-ering tissues and mucous envelope biocenoses. Thesemicrobes form high contamination levels (Table1).
The data reveal no high priorities of pathogensin the biotopes. However, the share of conventionalpathogens increases in every tested biotope, as com-pared to the pre-flight period (Table2).
3.1.1. Intestinal microfloraBased on the data concerning intestinal microflora
in 20 cosmonauts before and after missions aboardspace vehicles Salyut/Soyuz and Mir up to 96 daysin duration, there were systematic dysbiotic shifts ofvarious degrees in each of the crew members who hadmade either short- or long-term missions.
These shifts were of identical type and trend; be-sides, main groups of opportunistic pathogens con-tributing to the progress of bacteriosis were estab-lished. Growth of their population took place againstreduction in lactobacilli, bifidoflora or disbalance be-tween bifodobacteria and colibacilli, i.e., absence ofbifidoflora prevalence natural for eubiosis.
For instance, microbiocenosis in cosmonautson the first day after landing was characterizedby changes in the number of opportunisticallypathogenic enterobacteria, Clostridium, and lacto-bacilli (p0.01, p0.05, p0.05, respectively). Whereasthe first two groups showed an increase, lactobacillitended to decrease. Documented were microecologi-
Table 1General characteristics of microbial contamination (%)
Microbial species Before flight After flight
60 day 7–5 day 0–5 day 14 day
Ratio of conventionalpathogens to totalspecies
27 48.5 35.4 27.9
Ratio of conventionalpathogens forminghigh contaminationlevel to total speciesnumber
14,4 23.7 19.7 9.3
Rate of conventionalpathogens forminghigh contaminationlevel to total num-ber of conventionalpathogens
53.3 48.9 55.8 38.4
Table 2Share of conventional pathogens in tested biotopes (% of totalisolated species)
Biotopes Before flight After flight
60 day 7–5 day 0–5 day 14 day
Throat 29.4 30.0 18.1 28.6Nose 25.0 41.1 23.0 20.0Axilla 10.0 38.4 27.2 40.0Scapula 33.3 33.3 38.4 11.1Hand 28.5 31.2 33.3 25.0Ear 33.3 33.3 30.0 18.1All biotopes 27.5 43.0 28.8 26.6
cal shifts like alterations in population of one of thegroups, or several.
In this group the increase in persons with expresseddisbacteriosis was revealed. Before flight, 73.3% oftested cosmonauts had 1st stage disbacteriosis (lessexpressed) and only 13.3% had a 2nd stage disbac-teriosis. After the flight all the stages of disbacterio-sis were found in tested crewmembers: D1—36.8%,D2—36.8%, D3—26.3%. No individuals with nor-mal microbiocenosis were identified in the post-flightperiod.
Extension of space missions led to development (D1in 30-day missions) and aggravation of dysbacteriosis(D2 and D4 in consequence of 63- and 96-day mis-sions, respectively), so too stabilization of the shifts

844 V.K. Ilyin / Acta Astronautica 56 (2005) 839–850
with features characteristic of the period of rehabili-tation.
Post-flight study revealed deficiency in bifido- andlactoflora and increased isolation of conventionalpathogens—E.coli, Enterobacteria, and Clostridia.Decrease in lactibacilli in the pre-flight period sug-gested a high risk of serious disbacteriosis.Citrobac-ter sp.,Enterobactersp., andKlebsiellasp. are mostfrequent isolates in the group with disbiotic shifts.
3.1.2. Microflora of periodontiumIn consequence of long-term orbiting cosmonauts
significantly changed, both quantitatively and qual-itatively, the contents of oral microbiocenosis wereevidenced by appearance of a number of parodontiumpathogens, specificallyActinomyces naeslundii, Pre-votella melaninogenicaand Fusobacterium nuclea-tum, and massive invasion of bacterial species whichare able to keep inflammation going. These changeswere particularly great on the first day after landingbut gradually disappeared by day 14 of return. Theseprocesses took place on the background of specialand quantitative shifts in environmental microflora,colonization of space vehicles by aerobic bacteriaand fungi (Victorov et al., 1991). These could ploughthe soil for diseases of microbial etiology, namelypathologies of and other microbiotopes in the mouth.During space flight, cosmonauts actively use personalhygienic items and means preventing various distur-bances that can develop under the influence of micro-gravity and other adverse factors. That is why effectsof the spaceflight factors alone cannot be comprehen-sively evaluated by the physiological parameters withparticipation of the human. Typically, this is doneby evaluating the main systems of animals, primatesspecifically, whose physiology is similar to humans.We fulfilled an all-round investigation with primateswho had made a 14-day space flight. Analysis ofparodontium microflora revealed the disappearanceof or reduction in the number of representatives ofnormal microbiocenosis in the mouth and emergenceof pathogenic bacteria, i.e., processes like those thathappen in cosmonauts.
Results of in-space investigations are factual proofof the data from experimental simulation of one ofthe spaceflight factors—head-down bed rest. Inca-pable, for technical reasons, to track the dynamics of
parodontium microflora and immunity in space flight,and limited to pre- and post-flight investigations, wediscovered immediately after landing a picture re-sembling what we saw after bed rest, i.e., qualitativereduction in commensal flora with a background ofbroad expansion of opportunistic and obligate agentsof inflammatory diseases of parodontium. Theseobservations are in full agreement with results ofmicrobiological analysis of other biotopes obtainedby Russian investigators and interpreted by them as“accumulation of the pathogenicity potential withinthe human–microorganism system during space flight(Victorov et al., 1991).
The literature provides facts inferring vulnerabilityof microflora and local immunity to stresses. Thus,observations were made of a reduction in commensalmicroflora of the mammalian intestine due to stress,and incidences of the sensitization of humans underspaceflight, hyperbaric, and bedrest conditions, to abroad variety of antigens including those that had notbeen present in the environment. On this ground, theseobservations were qualified as a manifestation of non-specific body reaction to extreme effects of specifi-cally changed environment (possibly, stress-inducingby character) (Lizko et al., 1987; Meshkov, 1997).
Results of our investigations allow conclusionsabout some general trends in the reaction of the paro-dontium to the extreme factors under study. They areexpressed by a suppression of commensal microfloraby opportunistic and obligate agents of parodontitisand an increase in immunoglobulins in oral fluid.Follow-up studies of functional clinical and hygienicparameters elicited their quite significant discretenessand individuality which gave no way to establishingtrends in the parameters under control. Therefore,we consider it well for determination of risks ofdiseases of periodontium under these conditions topay attention first to the quantitative growth (appear-ance) of pathogenic microorganisms and high titre ofimmunoglobulins in oral fluid.
In our opinion, these characteristics should alsobe used as a basis in the selection of candidates forcosmonauts and divers, employees for caisson opera-tions, test-subjects for simulation experiments and thelike, as part of the identification of groups at risk ofperiodontium inflammation. For instance, our resultsshowed that the great majority of subjects was char-acterized by normal biocenosis and local immunity of

V.K. Ilyin / Acta Astronautica 56 (2005) 839–850 845
Table 3Dynamics ofS. aureuscontamination of the high respiratory tract(quantity of biotopes which containS. aureus)
Testing period Contamination level (Lg CFU per swab)
0 1–3 �4
Preflight 6 3 0Inflight 0 6 3Recovery 5 0 4
Table 4Dynamics of Enterobacteriaceae contamination of high respiratorytract (quantity of biotopes which contained enterobacteria)
Testing period Contamination level (Lg CFU per swab)
0 1–3 �4
Preflight 7 3 0Inflight 0 1 3Recovery 4 5 0
the periodontium before hyperbaric experiment, spaceflight or experimental bed rest. All shifts in micro-biocenosis and local immunity of periodontium devel-oped in these specific environments. In view of thiscircumstance, we may suggest that stays in extremeconditions will aggravate disturbances identified in the“baseline” period. Therefore, risk of periodontium in-flammation in this category of human subjects willbe much higher than in subjects with a normal stateof periodontium microflora and local immunity in thebaseline period.
We believe that this identification of groups of risk isnot a criterion for selecting out as professionally unfit.It only dictates the necessity to search for and perfectcountermeasures against periodontium inflammationin humans in extreme environments.
3.1.3. Peculiarities of microflora in inflight periodThe microflora data of cosmonauts, participants of
long-term spaceflights, are presented in theTables 3–5.Data reveal a serious shift in microecological
balance between conventional pathogens and com-mensals of the high respiratory tract. The amount ofbiotopes containing conventional pathogens increasedin the inflight period, while the amount of biotopescontaining lactobacilli decreased to non-registeredvalues.
Table 5Dynamics ofLactobacillusspp. contamination of high respiratorytract (quantity of biotopes which contained lactobacilli)
Testing period Contamination level (Lg CFU per swab)
0 1–3 �4
Preflight 3 7 0Inflight 9 1 0Recovery 2 8 0
Table 6Multiple resistance ofE.coli strains isolated from cosmonauts
Number of resistance determinants Preflight Postflight
0 30 641 9 22 30 123 8 04 2 05 1 06 and more 0 0Total cultures tested 80 80
This circumstance suggests the possibility of the de-velopment of opportunistic infection onboard orbitalstations. These infections may develop during a de-crease in the first colonization barrier—commensalmicroflora. This indicates the necessity to create meansand measures for the correction of microflora contentwith the aid of ecologically compatible means thatstrengthen this barrier.
These measures can prevent infections on cover-ing tissues caused by infectious agents of variousorigins—both exogenous and opportunistic.
3.1.4. Peculiarities of antibiotic susceptibility ofspacecrew members microflora
We have summarized data of antibiotic sensitivity of1740 isolates of different conventional pathogens, iso-lated from cosmonauts during spaceflights of differentdurations. The mostly typical results of antibiotic sus-ceptibility during long-term spaceflight without visit-ing crews are given inTables 6and 7. The data aregiven for intestinalE. coli. As it comes from the givendata, during long-term autonomous flight, the antibi-otic sensitivity of crew microflora had a tendency tobe restored. Studying this phenomenon, we have hadno opportunity to receive and to analyze data in the in-flight period so far. Therefore, we used ground-based

846 V.K. Ilyin / Acta Astronautica 56 (2005) 839–850
Table 7Multiple resistance ofE.coli strains isolated from 4 volunteers inconfined habitat
Number of resistance Days of experimentdeterminants
0 7–10 20–22 30–32
0 40,5 52,0 24,3 43,71 20,0 18,7 40,1 14,22 18,7 19,4 17,0 19,73 6,8 14,0 12,2 19,74 4,3 7,0 3,2 5,75 1,7 3,0 2,1 2,36 2,4 1,4 0,5 0,57 and more 0,4 3,0 0,3 5,4
experiments in confined habitats to learn the dynam-ics of antibiotic susceptibility modifications (Tables 6and7).
As shown in the tables, the number of resistantstrains increased in 7–10 days of isolation. Furtheron, up to the 20–30th day, the decrease in antibioticresistant strains in the majority of populations tookplace. Underlying processes are the results of sub-sequent R-plasmid segregation and their spontaneouselimination in the absence of a selecting factor (an-tibiotic assumption). Lack of a marker of antibioticresistance is connected with the elimination of genecoding this sign and it is natural after a long period ofnon-consumption of antibiotics. In this case, daughtercells get a non-completed number of resistance de-terminants. The new clones, having been liberated orsemi-liberated from resistant plasmids, start to dividewith higher velocity than clones, containing full plas-mids. As a result, plasmid-free clones start to prevailin the population.
We also observed recovery of antibiotic sensitivityin the course of several missions. Post-flight, partic-ipants in 150- and 211-day missions carried strainsresistant to three antibiotics in numbers from half asmany to two and four times fewer. No strain was iden-tified with the ability to resist 4 antibiotics after land-ing. Recovery of antibiotic sensitivity on completionof space flight was conditioned by segregation andspontaneous elimination of R-plasmids deposited inmicrobial cells.
At the same time, spreading of the markers of an-tibiotic resistance from one strain to another on the
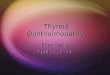
R-plasmid level was observed in a series of inves-tigations. It should be underlined that evidence ofthe appearance of a nosocomial-like strain in a con-fined habitat is strictly dependent upon the intensityof “flow” of external microbiota into the confinedhabitat during a particular isolation period (visitingcrews, admitting hardware, mail, payload, etc., seeFig. 1). The number of isolated individuals is also im-portant: more isolated individuals—more genotypes toexchange—more determinants to accumulate in onestrain—more reasons for nosocomial-like strain for-mation. As is seen from the tables, the share of thesestrains is not large in all microbiota (0.3%). However,in the case of introduction of a selective agent (re-sistance to antibiotic), the amount increases to 96%.One of the most convincing arguments for the acqui-sition of resistance determinants by plasmids is ob-tained by a strain resistance features to those antibi-otics to which it had earlier been susceptible. Commonpersistence of polyresistance pathogen and susceptiblecommensals leads to the acquisition of resistant andpathogenic genes with plasmids by the latter and thus“malignization” of a commensal. This commensal canserve as a “depot” of R-plasmids for other commensalsand pathogens. We observed acquisition of polyresis-tance genes and associated pathogenic genes (codingexonuclease activity) byS. aureusafter coexistence inone biotope withS. aureus. In this process, the maingroup that stayed in a chamber the longest period grewhighly susceptible to imported microbiota, includingmicroorganisms belonging to microflora of the mem-bers of visiting subjects.
The data presented show that within 7–10 daysof chamber isolation, indices of antibiotic resistancego up. This occurs in the period of what is calledthe acute adaptation of humans to chamber isola-tion. However, according to N.A. Polikarpov, thisis also a period of “peak” cross-contamination andgrowth of the pathogenicity potential within thehuman–microorganisms system. In consequence ofspreading of microorganisms, microbiocenoses ac-quire new determinants of resistance communicatedto plasmids by transitory strains. This is the cause ofthe strengthening of medicinal resistance of microor-ganisms during acute adaptation.
It can be concluded that quantitative growth of op-portunistic pathogens in various biotopes and commu-nication of deposited plasmids of antibiotic resistance

V.K. Ilyin / Acta Astronautica 56 (2005) 839–850 847
Volunteers Basic group members # Visiting group members
Days
A B C 1 D E F
Baseline
16
26
2 G H I 61
67
74 3 J K L
89
Recovery
CmMo Tc
SmKm
Sm AmKm Tc
Sm AmKm Tc
Sm AmKm Tc
Sm AmKm Tc
Sm AmKm Tc
Sm AmKm Tc
Am Cb Km Mo
Am Cb Km Mo
Sm KmCm AmCb Cf Mo Tc
Sm KmCm AmCb Cf Mo Tc
Sm KmCm AmCb Cf Mo Tc
Sm KmCm AmCb Cf Mo Tc
Sm KmCm AmCb Cf Mo Tc
Sm KmCm AmCb Cf Mo Tc
Sm KmCm AmCb Cf Mo Tc
Sm KmCm AmCb Cf Mo Tc
Sm KmCm AmCb Cf Mo Tc
Am Cb Km Mo
Fig. 1. Spreading of poly-resistant strains among isolated basic and visiting crews in ground-based 90-day experiment.
equally point to the need to develop a system for theirstabilization.
3.2. Lactobacterin as a means to stabilizemicrobiocenosis of various human biotopes
The method of microbial interference, eubiotics inparticular, could, in our opinion, be a universal andmighty approach to correcting microbial cenosis in a
large variety of biotopes. From two points of view,consideration of the potentiality of eubiotics in the pre-vention of deterioration of the colonization resistanceof spacecrews fully agrees with the methodology weuse to approach problems of infectious safety:
• eubiotics prepared from strains representing com-mensal saprophytic microflora are an ecologicaltherapeutic means complementary for humanorganism;

848 V.K. Ilyin / Acta Astronautica 56 (2005) 839–850
Table 8Intestinal microflora of volunteers who consumed lactobacterin
Disbacteriosis Before Aftergrade consumption consumption
0 0 251 25 392 33 383 27 144 31 0Total volunteers 116 116
• eubiotics do not have selective action on oppor-tunistic pathogens.
Below we present results of the clinical investigationsthat we performed in 1990–1992 using the well-knowneubiotics lactobacterin fabricated in the form of pelletscontaining primarily sp.Lactobacillus casei.
Lactobacilli are known to play an active role in set-ting a barrier of resistance to colonization in the oralcavity as in the intestine. With this in view, we specifi-cally focused on the problem of possible correction ofdivers’ microflora with the help of lactobacterin andto this end studied not only the effect of peroral lac-tobacterin on the quantitative and special compositionof intestinal microflora of human subjects, but alsothe quantitative and special composition of microfloraof open biotopes anatomically interfacing the intes-tine and the organs of hearing (mucous membrane ofthe oral cavity, throat, and node). In addition, we alsotested the effects of lactobacterin on sensitivity to an-tibiotics of human automicroflora.
The effects of peroral lactobacterin on the specialcomposition of intestinal microflora were determinedin 116 essentially healthy humans who consumedcommercial lactobacterin pellets for the sake of pro-phylaxis. Each subject took 4–6 pellets a day over aperiod of 14 days. No other anti-microbial or anti-inflammatory therapy was administered in the period.
Microflora of the intestine and mucous membranesof the nose and throat was investigated before the pre-ventive course, immediately, and 4 months after itscompletion.
Data concerning special changes in intestinal mi-croflora are given inTable 8.
The data point to a significant reduction in the num-ber of subjects with serious forms of dysbacteriosis.
Table 9Special changes of intestinal microflora of volunteers who con-sumed lactobacterin (% of totally isolated strains)
Microbial groups Before Afterconsumption consumption
Klebsiella Enterobacter, Serratia 56,7 26,5Proteus, Providencia 53,5 0,5Citrobacter, Escherichia 52,1 21,5
Table 10Quantitative changes of enterobacteria in nose and throat of vol-unteers who consumed lactobacterin (% cases)
Biotope Nose Throat
Type of Decrease Elimination Decrease Eliminationmodification
4,8 23,8 2,1 45,6
Most of them had intestinal microflora normalized fol-lowing lactobacterin therapy.
Results of investigations showed that preventive lac-tobacterin did decrease quantities of the species thatconstitute a real danger as opportunistic pathogensincludingKlebsiella, Enterobacteriaceae, andProteus(Table9).
Among this group there were 64 subjects whoturned out to be stable carriers ofKlebsiella pneumo-niae, Klebsiella ozenae, E. coli, and representativesof Enterobacteriaceae spp. in the throat; 44 subjectswere carriers of gram-negative bacilli on the nasalmucous membrane.
After the course of lactobacterin, 29 out of 64 carri-ers of gram-negative microorganisms in the throat didnot have them any more and 13 carriers had reducedtheir quantities 10–100 times as compared with theinitial level of 1× 103–1× 104 CFU on a swab.
Out of 44 carriers of enterobacteria who weregiven the lactobacterin course, 10 did not have gram-negative microflora in the nose at all and two had itreduced by 10 times as compared with the initial levelof 1 × 102–1× 103 CFU on a swab (Table10).
No significant shifts happened to microflora in thenose and throat in 27 out of 82 participants in theexperimental group.
The investigation made 4 months later found gram-negative recontamination of mucous membranes of thenose and fauces in only 4 subjects.

V.K. Ilyin / Acta Astronautica 56 (2005) 839–850 849
Table 11Microflora antibiotic susceptibility in the throat of volunteers whoconsumed lactobacterin
Number of resistance Before Aftermarkers consumption consumption
0 4.7 12.81–2 41.8 39.83–5 42.5 39.06 and more 11.0 8.4Total isolates 1325 1648
Microbiological investigations of the nose andfauces in the control group did not reveal positivedynamics in the period of observation.
We also delved into changes in the antibiotic sensi-tivity of the strains of opportunistic pathogens recov-ered from the intestine and upper respiratory tract ofthese subjects who took a long course of lactobacterin.
The character of shifts in the indices of antibioticpolyresistance of microorganisms recovered from thesubjects before and after this therapy can be learnedfrom the data inTable 11.
From the table it follows that the quantity of antibi-otic sensitive microorganisms grew threefold in thisperiod. At the same time, polyresistant strains less-ened, particularly those resistant to 6 and more antibi-otics. The latter decreased their number in approxi-mately half of time and a half.
Thus, we should state that eubiotic therapy usinglactobacterin results in a meaningful quantitative re-duction of microorganisms with markers of polyresis-tance to antibiotics and partial recovery of antibioticsensitivity.
As a matter of fact, this effect of lactobacterin can beexplained from the position of microecology. There arepublications (Tallmeister et al., 1977) demonstratingthe ability of lactobacilli metabolites in vitro to inhibittransfer of plasmids of antibiotics resistance.
Our own data given below also support this suppo-sition. In this case we can make a guess about the in-hibition of the conjugative R-plasmid transfer by lac-tobacterin lactobacilli and the consequent prevalenceof plasmid segregation and spontaneous eliminationover co-integration.
From the data in the tables it follows that frequencyof the conjugative transfer in the presence of living
Table 12Lactobacilli antagonism
Test - strain Growth inhibition zone (mm)around lactobacilli colonies
Shigella flexneri 34± 5E. coli C-600 25± 2P. aeruginosaPA-103 2.0E. coli J 5-3 25± 4S. typhimurium 31± 6S. aureus209 21± 4
lactobacilli cells is 1.5–3 times lower in comparisonto that in the control.
This circumstance allows supposition concerningthe ability of living rehydrated cells of lactobacilli toinhibit R-plasmid transfer. This ability could be veryproductive as one of the side effects of lactobacterinprophylaxis of humans exposed to elevated pressure,since the inhibition of conjugative transfer in a hy-perbaric environment could stimulate the formation ofstrains with hospital markers, specifically strains witha large number of determinants of antibiotics resis-tance.
Hence, on this experimental basis we can draw theconclusion that microbial interference, lactobacterintherapy in particular, is able to stabilize the microeco-logical balance in a variety of biotopes. We think thatelimination of enterobacteria from the mucous mem-brane of the nose and fauces is not a result of singularnormalization of special composition of microorgan-isms in the intestine, their main natural residence. Wealso recognize the immunity-modulating properties oflactobacilli and the ability of living lactobacilli cellsto produce bacteriocins (lactocines), which, spread-ing all over the organism via biological fluids, influ-ence the composition of microflora in many humanbiotopes. An advanced study was made to shed lighton the antagonistic properties of lactobacterin lacto-bacilli in which we used the method of delayed an-tagonism. Data of this study can be seen inTable 12.Judging by these data, lactobacilli of commercial drylactobacterin demonstrate antagonistic activity rela-tive to essentially all test strains of catalogued agentsof infection. Lactobacilli are very active relative tosuch agents of infectious diseases asEsherichia coliwith modified biochemical activity (without lactosefermentation) andSalmonella typhimurium, less active

850 V.K. Ilyin / Acta Astronautica 56 (2005) 839–850
relative toS. aureusandE. coli without changes inbiochemical activity (lactose fermentation) and leastactive relative toP. aeruginosa.
Thus, microbial interference by the course of eubi-otic lactobacterin was favorable to stabilization of thebodily lactobacilli, i.e., saprophytes, reinforcing nat-ural barriers of the colonization resistance, blockingcritical buildup of opportunistic pathogens and exoge-nous infection, translocation of pathogenic microflorainto other biotopes of the human body and, therefore,development of endogenous infection. In our view,this effect is achieved through a biotope glut with vi-able lactobacilli cells, so through, possibly, antagonis-tic performance (excretion of bacteriocines, etc.).
Consumption of lactobacterin by spacecrews onlong-term missions could, at large, resolve the prob-lems of strengthening of colonization resistance bystabilizing human automicroflora and preventing en-dogenous infection.
To effectively counteract external otitis, one ofthe nosologies that may arise during space flight,lactobacterin therapy should be combined with lo-cal administration of an ecologically complementarynon-selecting substance like trypsin and lysozymeimmobilized on dialdehydecellulose. Testing of thesesubstances was performed in 1992 in the ORL clinicof the Moscow Sechenov’s Medical Academy.
4. Conclusions
1. A quantitative growth of opportunistic pathogensand a quantitative decrease in the population of pro-tective microorganisms were observed in cosmonautsduring spaceflight.
2. The antibiotic sensitivity of cosmonauts’ mi-croflora increases during spaceflight due to the
segregation and spontaneous elimination of R-plasmids. Meanwhile, some of the conventionalpathogenic strains are capable of the accumulation ofantibiotic resistance determinants.
3. Consumption of lactobacterin and bifidum-bacterin is favorable to stabilization of intestinalmicrobiocenoses, and consumption of lactobacterinstimulates recovery of human microflora sensitivityto antibiotics.
4. There are disorders in the immune activity ofspacecrew members in spaceflights (increased sensi-tivity to allergens, decrease in normal killer activity,etc.).
5. Trypsin immobilized on dialdehyde cellulose isan effective means for prevention and treatment ofexternal otitis of varying etiology.
References
[1] O.G. Alekseeva, State of some kind of natural immunityand autoflora of cosmonauts during preflight preparationsand in postflight period of spaceships, Vostok 1–4. Problemikosmicheskoi biologii, M. Nauka. 4 (1965) 230–303 (inRussian).
[2] G. Taylor, Recovery of medical important microorganisms fromApollo astronauts, Aerospace Medicine 45 (8) (1974) 824–882.
Further reading
[3] I.N. Kornyushenkova, Human microflora statement inspaceflights, and ecological means of its correction,Proceedings of the 31st Scientific Assembly of COSPAR,Birmingham, UK, 1996, Book of Abstracts, p. 369.