Embed Size (px)
Citation preview

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
Report on a QI Project Eligible for Part IV MOC
Michigan Caries Prevention Program Instructions Determine eligibility. Before starting to complete this report, go to the UMHS MOC website [ocpd.med.umich.edu], click on “Part IV Credit Designation,” and review sections 1 and 2. Complete and submit a “QI Project Preliminary Worksheet for Part IV Eligibility.” Staff from the UMHS Part IV MOC Program will review the worksheet with you to explain any adjustments needed to be eligible. (The approved Worksheet provides an outline to complete this report.) Completing the report. The report documents completion of each phase of the QI project. Final confirmation of Part IV MOC for a project occurs when the full report is submitted and approved. An option for preliminary review (recommended) is to complete a description of activities through the intervention phase and submit the partially completed report. (Complete at least items 1-16 and 27a-b.) Staff from the UMHS Part IV MOC Program will provide a preliminary review, checking that the information is sufficiently clear, but not overly detailed. This simplifies completion and review of descriptions of remaining activities. Questions are in bold font and answers should be in regular font (generally immediately below the questions). To check boxes electronically, either put an “X” in front of a box or copy and paste “ ” over the blank box. For further information and to submit completed applications, contact either:
Grant Greenberg, MD, UMHS Part IV Program Lead, 763-232-6222, [email protected] R. Van Harrison, PhD, UMHS Part IV Program Co-Lead, 734-763-1425, [email protected] Ellen Patrick, UMHS Part IV Program Administrator, 734-936-9771, [email protected]
Report Outline
Section Items
A. Introduction 1-6. Current date, title, time frame, project leader, specialties/subspecialties involved, funding
B. Plan 7-10. General goal, patient population, IOM quality dimensions addressed, experimental design
11-12. Baseline measures of performance, specific performance objectives 13. Data review and identifying underlying (root) causes
C. Do 14-16. Intervention(s), who is involved, initiated when
D. Check 17-18. Post-intervention performance measurement, data collection, performance level
E. Adjust – Replan 19. Review, continuing/new underlying causes,
F. Redo 20-21. Second intervention
G. Recheck 22-23. Post-adjustment performance measurement, data collection, performance level
H. Readjust plan 24. Review, continuing/new underlying causes to address
I. Future plans 25-28. Subsequent PDCA cycles, standardize processes, “spread” to other areas
J. Physician involvement 29-31. Physician’s role, requirements, reports, reflections, participation, number
K. Sharing results 32. Plans for report, presentation, publication
L. Project Organization 33. Part of larger initiative, organizational structure, resources, oversight, Part IV opportunity

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
QI Project Report for Part IV MOC Eligibility A. Introduction 1. Date (this version of the report): March 8, 2016 2. Title of QI project: Michigan Caries Prevention Program 3. Time frame
a. Date physicians begin participating (may be in design phase): July 1, 2015, for the first group. b. End date: Each group of participants is engaged for approximately 7 months, with the first group finishing in January 2016. A new group starts each month with the last of the 15 groups starting in September 2016 and finishing March 31, 2017 - see Appendix A for timeline of participation waves.
4. Key individuals
a. QI project leader [also responsible for attesting to the participation of physicians in the project]
Name: Carley Kirk, MS, RDH Title: Physician Engagement Lead Organizational unit: Altarum Institute Phone number: 734-302-4727 Email address: [email protected] Mailing address: 3520 Green Court, Suite 300, Ann Arbor, MI. 48105
a. Clinical leader to whom the project leader reports regarding the project [responsible for
overseeing/”sponsoring” the project within the specific clinical setting] Name: Stephanie Goodson, MD, FAAP Title: Assistant Professor of Pediatrics Organizational unit: University of Michigan Phone number: 810-227-9510 Email address: [email protected] Mailing address: 8001 Challis Rd. Brighton, MI. 48116
5. Approximately how many physicians were involved in this project categorized by specialty
and/or subspecialty? In the first wave, July 2015, 7 pediatricians and 1 physician assistant participated.
6. Will the funding and resources for the project come only from internal UMHS sources?
Yes, only internal UMHS sources No, funding and/or resources will come in part from sources outside UMHS,
which are: Center for Medicare and Medicaid Innovation Health Care Innovation Award The Multi-Specialty Part IV MOC Program requires that projects engage in change efforts over time, including at least three cycles of data collection with feedback to physicians and review of project results. Some projects may have only three cycles while others, particularly those involving rapid cycle improvement, may have several more cycles. The items below are intended to provide some flexibility in describing project methods. If the items do not allow you to reasonably describe the methods of your specific project, please contact the UMHS Part IV MOC Program office. B. Plan 7. General goal
University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
a. Problem/need. What is the “gap” in quality that resulted in the development of this project? Children at risk for early childhood caries often do not receive preventive oral health services during well-child visits. Preventive oral health services beginning at the 6 month well-child visit is supported by the American Academy of Pediatrics (AAP) Section on Oral Health policy and the Bright Futures periodicity schedule. These services include oral health screenings, fluoride varnish applications, and recommending seeing/facilitating referral to a dentist for the child to be seen at 12 months of age or at the time of first tooth emergence, whichever occurs first. However, primary care physicians are not prepared to provide oral health screenings and fluoride varnish applications and are not aware of the need to recommend seeing a dentist in this time frame. Primary care physicians generally lack the education and training to provide these services. Most physicians are not aware they can bill most insurers for oral screening and varnish application. To bill Medicaid for providing these services a special “Smiles for Life” certification is required. As of May 2015, only 3.4% of primary care physicians in Michigan were Smiles for Life certified to provide preventive oral health services to patients ages 0-3 years. A very low percentage of children participating in Medicaid/MIChild receive these services or dental recommendations/referrals.
b. Physician’s role. What is the physician’s role related to this problem? Physicians provide preventive care during “well child” exams. Children often will see their physician up to eight times before they see a dentist. Physicians are able to make a significant impact on preventing dental caries among their patients. There is an important opportunity to provide preventive oral health services is during the well-child visit exam.
c. Project goal. What general outcome regarding the problem should result from this
project? (Specific aims/targets are addressed in #12b.) Increase of oral health screenings, increase of fluoride varnish applications, and increase recommendations for/referrals to a dental home*, resulting in an improvement in children’s oral health.
The Michigan Caries Prevention Program was created to transform the system of children’s oral health care in Michigan through providing the necessary education, technical assistance, and resources to primary care providers and clinical staff to increase the number of children receiving preventive oral health services during well-child visits and increase recommendations for/referrals to a dental home. * The American Academy of Pediatrics and the American Academy of Pediatric Dentistry define a
“dental home” as the “ongoing relationship between the dentist and the patient, inclusive of all aspects of oral health care delivered in a comprehensive, continuously accessible, coordinated, and family-centered way.”
8. Patient population. What patient population does this project address. All children ages 0-3
years who receive preventive care in the participating primary care practices in Michigan. 9. Which Institute of Medicine Quality Dimensions are addressed? [Check all that apply.] Effectiveness Equity Safety Efficiency Patient-Centeredness Timeliness 10. What is the experimental design for the project?
Pre-post comparisons (baseline period plus two or more follow-up measurement periods) Pre-post comparisons with control group Other: _____________________________
11. Baseline measures of performance:
a. What measures of quality are used? Six aspects of care are measured. Within each practice 15 charts are randomly pulled for patients seen for a 9-month visit and 15 practice charts are pulled for patients seen for a 12-
University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
month visit. (If fewer than 15 patients are seen, all that are seen are selected.) For each of the two sets of charts, three aspects of care are measured: oral health screening performed, fluoride varnish applied, and a recommendation for/referral to a dental home is made. The percentage of each group of patients receiving each type care was calculated as follows. Oral health screening – calculated separately for 9-month visits and 12-month visits Denominator: Number of patient charts pulled Numerator: Number of patients with oral health screening performed Fluoride varnish – calculated separately for 9-month visits and 12-month visits Denominator: Excluding patients without teeth, the remaining number of patient charts pulled Numerator: Number of these patients with fluoride varnish applied Recommendation for/referral to a dental home – calculated separately for 9-month visits and 12-
month visits Denominator: Excluding patients with a known dental home, remaining number of charts pulled Numerator: Number of these patients with recommendation for/referred to a dental home.
b. Are the measures nationally endorsed? If not, why were they chosen?
Fluoride varnish- based on the Dental Quality Alliance (DQA) and National Quality Forum (NQF) measure: Topical Fluoride for Children at Elevated Caries Risk, Dental Services. This measure focuses on children with elevated risk; before the United States Preventive Services Task Force (USPSTF) released their new guidelines recommending fluoride varnish for all children regardless of risk. This measure also is specific to the dental setting, but because of the nature of our intervention, we have adopted it to apply to the medical setting as well. Oral health screening- based on the DQA/NQF Measure: Oral Evaluation, Dental Services. This measure is specific to the dental setting, but because of the nature of our intervention, we have adopted it to apply to the medical setting as well. Recommendation for/referral to a dental home- This is not based on any measure, this is based on the American Academy of Pediatrics (AAP) and American Academy of Pediatric Dentistry (AAPD) guidelines recommending the establishment of a dental home by the 1st birthday.
d. What is the source of data for the measure (e.g., medical records, billings, patient
surveys)? Patient charts (i.e., patient medical record).
e. What methods were used to collect the data (e.g., abstraction, data analyst)?
Chart review by pulling a random sample of patient charts and abstracting relevant data. f. For what time period was the sample collected for baseline data?
The sample for baseline was collected from June 2015. 12. Specific performance objectives
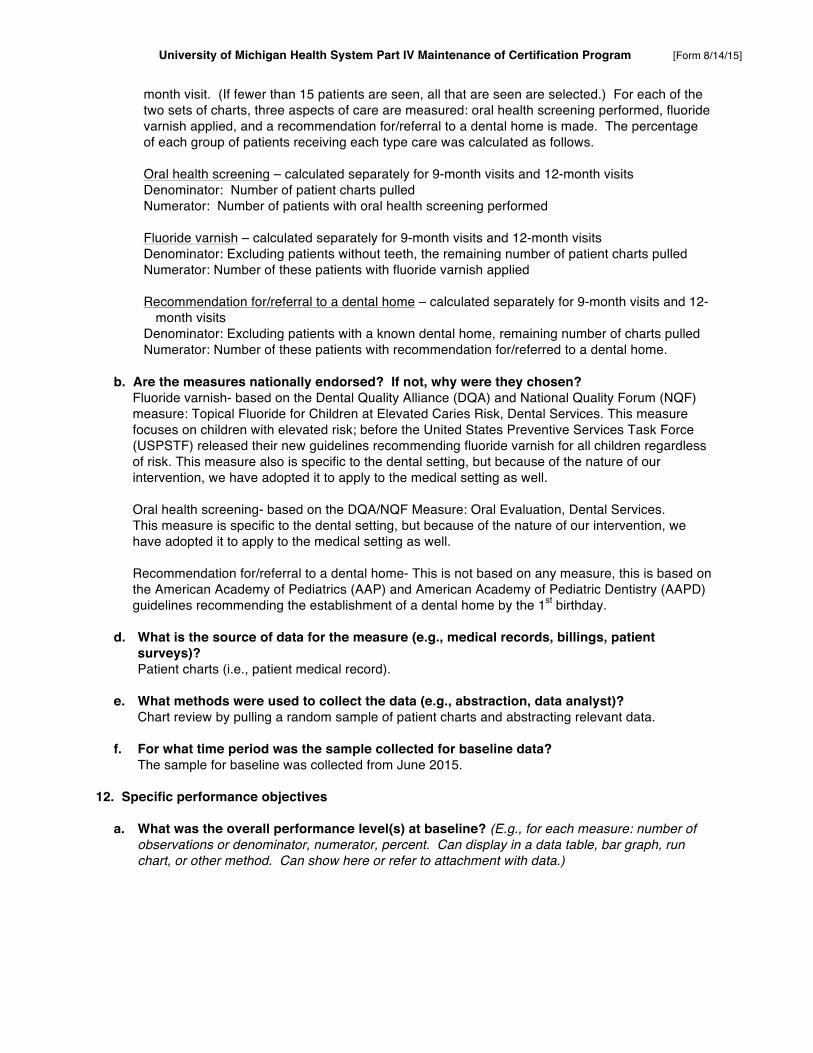
a. What was the overall performance level(s) at baseline? (E.g., for each measure: number of observations or denominator, numerator, percent. Can display in a data table, bar graph, run chart, or other method. Can show here or refer to attachment with data.)
University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
Mean Across Five Practices for Percent of Patients with Service Performed
Service Baseline 6/1-6/30/15
Goal
Oral health screening 9-month visit 16% 75% 12-month visit 0% 75%
Fluoride varnish
9-month visit 0% 50% 12-month visit 0% 50%
Recommend/refer to
dental home
9-month visit 0% 50% 12-month visit 9% 50%
N = 5 practices. (Individual practice means are based on samples of up to 15 cases) Please see Appendix B for performance percentages and sample sizes within individual practices.
b. Specific aim: What was the target for performance on the measure(s) and the timeframe for
achieving the target? Recommended goals:
75% of patients receive oral health screenings 50% of eligible patients receive fluoride varnish applications 50% of eligible patients receive dental home recommendations/referrals.
The timeframe to achieve these goals is by the end of the second improvement cycle, 7 months from the cohort’s initiation of participation in the project.
c. How were the performance targets determined, e.g., regional or national benchmarks?
No national performance targets exist. Project leaders set goals based on likely practical performance rates given priorities for clinical prevention and time limitations during any one well-child visit and the possibility of providing the services at a subsequent well-child visit.
13. Data review and identifying underlying (root) causes.
a. Who was involved in reviewing the baseline data, identifying underlying (root) causes of the problem(s), and considering possible interventions (“countermeasures”) to address the causes? Briefly describe: • Who was involved? Participating physicians, nurse practitioners, physician assistants, and
clinical support staff.
• How? (e.g., in a meeting of clinic staff) Meetings will occurred during clinical staff meetings.
• When? Before the end of month 1 of the group’s participation, i.e. by the end of July 2015 for the first group.
b. What were the primary underlying/root causes for the problem(s) that the project can
address? (Causes may be aspects of people, processes, information infrastructure, equipment, environment, etc. List each primary cause separately.) The general causes identified are: Clinical personnel

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
Do not have the education and training to perform the procedures Office set-up and workflow Resources needed to perform the procedures are not stocked No routine processes to coordinate office staff in delivering the care Financial incentive Without training and certification, the procedures cannot be billed
C. Do 14. Intervention(s). Describe the interventions implemented as part of the project.
Education/training. Central program personnel will train physicians, nurse clinicians, and physician assistants to: • Perform oral screening and apply fluoride varnish. • Utilize a clinical decision support tool to incorporate recommendation/referral to dental homes
into routine care provision. • Understand AAP policy and the Bright Futures periodicity schedule related to providing
preventive oral health services during well-child visits. • Make operational changes in the process of well-child care that facilitate the provision and
documentation of appropriate care. • Collect and report individual practice data.
Office set-up and workflow. Trained clinicians will work with their office staff to make operational changes in the local process of well-child care that facilitate the provision and documentation of appropriate care. Please see Appendix C for an example of practice workflow and associated roles within the clinic.
Financial incentives. Physicians and nurse practitioners who have been trained and have set up appropriate office procedures can bill most insurers for preventive oral health services and will become certified to bill Medicaid for these services.
15. Who was involved in carrying out the intervention(s) and what were their roles? In order to
carry out the intervention, participating physicians, nurse practitioners, physician assistants, and clinical support staff were involved. Central program personnel provided training and advice to local clinics. A local oral health champion, a member of the clinical staff, is identified. This role is often filled by a physician or lead clinical staff member. The oral health champion helps arrange for training, ensures staff are implementing the new changes, and maintains enthusiasm among the care team around oral health. The champion ensures that fluoride varnish is ordered as needed, and follows up with the technical assistance staff regarding any questions or issues that come up throughout implementation. Physicians and nurse practitioners participate in training and subsequently obtain certification to provide preventive oral health services to patients during the appropriate well-child visits. Physicians conduct the oral health screening and oral health counseling during the evaluation portion of the visit. Physicians recommend/refer patients to dental homes as needed. Trained clinical support staff, including physician assistants, can be delegated the preventive oral health services task of applying fluoride varnish.

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
All clinic personnel participate in determining the local practice workflow to deliver and document services.
16. When was the intervention initiated? (For multiple interventions, initiation date for each.)
Before the end of month 1 of the group’s participation, i.e. by the end of July 2015 for the first group. D. Check 17. Post-intervention performance measurement. Did this data collection follow the same
procedures as the initial collection of data described in #11: population, measure(s), and data source(s)?
Yes No – If no, describe how this data collection 18. Performance following the intervention.
a. The collection of the sample of performance data following the intervention occurred for the time period: During 9/1-30/15 (month 3 of the cycle).
b. What was post-intervention performance level? (E.g., for each measure: number of
observations or denominator, numerator, percent. Can display in a data table, bar graph, run chart, or other method. Can show here or refer to attachment with data.)
Mean Across Five Practices for Percent of Patients with Service Performed
Service Baseline
6/1-6/30/15 Post-Intervention
9/1-9/30/15 Goal
Oral health screening 9-month visit 16% 59% 75% 12-month visit 0% 57% 75%
Fluoride varnish
9-month visit 0% 16% 50% 12-month visit 0% 21% 50%
Recommend/refer to
dental home
9-month visit 0% 0% 50% 12-month visit 9% 20% 50%
N = 5 practices. (Individual practice means are based on samples of up to 15 cases) Please see Appendix B for performance percentages and sample sizes within individual practices.
c. Did the intervention produce the expected improvement toward meeting the project’s
specific aim (item 12.b)? While some improvement occurred in 5 of the 6 measures, considerable improvement is needed to reach goals.
E. Adjust – Replan 19. Review of post-intervention data and identifying continuing/new underlying causes.

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
a. Who was involved in reviewing the post-intervention data, identifying underlying (root)
causes of the continuing/new problem(s), and considering possible adjustments to interventions (“countermeasures”) to address the causes? Briefly describe: • Who was involved? Participating physicians, nurse practitioners, physician assistants, and
clinical support staff.
• How? (e.g., in a meeting of clinic staff) Meetings occurred during clinical staff meetings.
• When? Before the end of month 4 of the group’s participation, i.e. during October 2015 for the first group.
b. What were the primary underlying/root causes for the continuing/new problem(s) that the
project can address? (Causes may be aspects of people, processes, information infrastructure, equipment, environment, etc. List each primary cause separately.)
Clinical personnel. Are less aware of the importance of dental recommendations/referrals at the 9-month visit than the
12-month visit. Children at 9 months with a tooth are to be recommended/referred for an initial dental visit. Even if the child does not have a tooth at 9 months, the recommendation/referral at 9 months is important for parents to have advance time to schedule a recommended initial dental visit by the time the child is 12 months of age.
New staff hires brought on after the initial training lack education related to the appropriate services. Enthusiasm of some clinical staff reduces over time. Office workflow. Documentation of new services is difficult, especially documentation of dental recommendations/
referrals. Financial incentive. Adding new billing codes to certain EHR systems is time consuming.
F. Redo 20. Second intervention. What additional interventions/changes were implemented?
Education/training of clinical personnel. Central program personnel performed an on-site technical assistance meeting with the oral health champion to continue education and sharing of additional resources related to: • Adjusting operational changes to better facilitate documentation of appropriate care, specifically
recommendations/referrals to a dental home. • Importance of dental home recommendations/referrals during the 9-month visit. • Continuing clinical staff enthusiasm by emphasizing the ease of providing services. Utilizing the
follow-up conversations to ensure services continue to be provided, and clinical staff have access to onboarding resources for new staff.
• Inputting billing codes into the EHR system earlier in the process. Office set-up and workflow. The oral health champion will work with their clinical staff to incorporate education, resources, and online certification with newly hired staff to support the continued provision of services. The oral health champion will work with the trained providers to document appropriate care and adjust local workflows as needed. Financial incentive. The oral health champion will work with their clinic’s billing support staff to ensure billing codes are inputted correctly to avoid a delay in delivery of care.

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
21. The second intervention was initiated when? (For multiple interventions, initiation date for each.)
Before the end of month 4 of the group’s participation, i.e. by the end of October 2015 for the first group.
G. Recheck 22. Post-second intervention performance measurement. Did this data collection follow the
same procedures as the initial collection of data described in #11: population, measure(s), and data source(s)?
Yes No – If no, describe how this data collection
23. Performance following the second intervention.
a. The collection of the sample of performance data following the intervention(s) occurred for the time period: During 11/1-12/31/15 (months 5 and 6 of the cycle).
b. What was the performance level? (E.g., for each measure: number of observations or
denominator, numerator, percent. Can display in a data table, bar graph, run chart, or other method. Can show here or refer to attachment with data.)
Mean Across Five Practices for Percent of Patients with Service Performed
Service Baseline
6/1-6/30/15 Post-Intervention
9/1-9/30/15 Post-
Adjustment 11/1–12/31/15
Goal
Oral health screening 9-month visit 16% 59% 88% 75% 12-month visit 0% 57% 90% 75%
Fluoride varnish
9-month visit 0% 16% 37% 50% 12-month visit 0% 21% 48% 50%
Recommend/ refer to
dental home
9-month visit 0% 0% 80% 50% 12-month visit 9% 20% 83% 50%
N = 5 practices. (Individual practice means are based on samples of up to 15 cases) Please see Appendix B for performance percentages and sample sizes within individual practices.
c. Did the second intervention produce the expected improvement toward meeting the project’s specific aim (item 12.b)? Improvement occurred in 6 of the 6 measures. There is opportunity for further improvement with 2 of the 6 measures.
H. Readjust

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
24. Review of post-second intervention data and identifying continuing/new underlying causes.
a. Who was involved in reviewing the data, identifying underlying (root) causes of the continuing/new problem(s), and considering additional possible adjustments to interventions (“countermeasures”) to address the causes? Briefly describe: • Who was involved? Participating physicians, nurse practitioners, physician assistants, and
clinical support staff.
• How? (e.g., in a meeting of clinic staff) Meetings occurred during clinical staff meetings.
• When? Before the end of month 7 of the group’s participation, i.e. during January 2016 for the first group.
b. What were the primary underlying/root causes for the continuing/new problem(s) that the
project can address? (Causes may be aspects of people, processes, information infrastructure, equipment, environment, etc. List each primary cause separately.)
Clinical personnel. Feel less comfortable providing the fluoride varnish service to the 9 and 12 month olds due to the
lack of patient cooperation, and fear of getting bit. Unsure of ability to provide fluoride varnish to an uncooperative child. Enthusiasm of some clinical staff reduces over time. Office workflow. Documentation of dental recommendations/referrals is difficult when the task is not specifically
assigned to the correct clinical staff member. If no additional cycles of adjustment are to be documented for the project for Part IV credit, go to item
#25. If a few additional cycles of adjustments, data collection, and review are to be documented as part of the
project to be documented, document items #20 – #24 for each subsequent cycle. Copy the set of items #20 – #24 and paste them following the last item #24 and provide the information. When the project to be documented for Part IV credit has no additional adjustment cycles, go to item #25.
If several more cycles are included in the project for Part IV credit, contact the UM Part IV MOC Program to determine how the project can be documented most practically.
I. Future Plans 25. How many subsequent PDCA cycles are to occur, but will not be documented as part of the
“project” for which Part IV credit is designated? No formal additional PDCA cycles are planned for this wave of participants. Overall performance rates met the goals for 4 out of the 6 measures. Project leaders will remain an available resource until the end of the grant period (August 2017).
26. How will the project sustain processes to maintain improvements?
Improvements that have now become part of the clinical workflow should remain self-sustaining over time. Peer-to-peer oral health champion networks are available as a resource, and a best practices webinar on the application of fluoride varnish for very young children is under development. This webinar will be made available to all current and previous participants to increase their ability and their confidence in their ability to provide fluoride varnish to 9 and 12 month olds.
27. Do other parts of the organization(s) face a similar problem? If so, how will the project be
conducted so that improvement processes can be communicated to others for “spread” across applicable areas?

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
Project leaders have been able to identify consistent barrier trends to implementing preventive oral health services during the 9 and 12 month well-child visits among subsequent waves of participants. The local changes that were made by this first wave of participants have been an integral part of rapid cycle process improvement to assist the central program personnel in their education, training, and technical assistance efforts for future waves of participants.
28. What lessons (positive or negative) were learned through the improvement effort that can be used to prevent future failures and mishaps or reinforce a positive result?? • Include clinical support staff. Including all clinical support staff in the training significantly helps
with obtaining staff buy-in during the early stage of implementing preventive oral health services. • Importance of oral health champion. The oral health champion plays an important role as they
often are the ones who are able to assist in making local operational changes that are a best fit for their clinic, and are easily able to identify key clinical support staff to ensure that sustainment of the changes is achieved.
• Demonstrate safe fluoride varnish application. A hands-on demonstration of fluoride varnish application that includes safe provider hand positioning would help alleviate fears of biting.
J. Provider Involvement
Note: To receive Part IV MOC a provider must both: a. Be actively involved in the QI effort, including at a minimum:
• Work with care team members to plan and implement interventions • Interpret performance data to assess the impact of the interventions • Make appropriate course corrections in the improvement project
b. Be active in the project for the minimum duration required by the project 29. Provider’s role. What were the minimum requirements for providers to be actively involved in
this QI effort? (What were providers to do to meet each of the basic requirements listed below? If this project had additional requirements for participation, also list those requirements and what physicians had to do to meet them.) a. Interpreting baseline data, considering underlying causes, and planning intervention. (As
appropriate, use or modify the following response.) Providers had to participate as described in item #13a.
b. Implementing intervention. (As appropriate, use or modify the following response.) Providers had to participate as described in items #14, #15, and #16.
c. Interpreting post-intervention data, considering underlying causes, and planning changes. (As appropriate, use or modify the following response.) Providers had to participate as described in item #19a.
d. Implementing further intervention/adjustments. (As appropriate, use or modify the following response.) Providers had to participate as described in items #20 and #21.
e. Interpreting post-adjustment data, considering underlying causes, and planning changes. (As appropriate, use or modify the following response.) Providers had to participate as described in item #24a.
30. How were reflections of individual providers about the project utilized to improve the overall
project? During the project providers participated in clinical staff meetings about the project and shared their reflections and suggestions for improvements with the local Oral Health Champion and other staff. Beyond the local clinic, participant reflections of the project have been utilized to develop a best practices webinar that will focus on the application of fluoride varnish for uncooperative young children, safe provider positioning, and a peer-to-peer forum to share lessons learned.

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
31. How did the project ensure meaningful participation by providers who subsequently request
credit for MOC participation? All providers seeking MOC credit participated in the initial and follow-up chart reviews, were actively engaged in the discussion during data review meetings, and helped to determine operational steps to improve performance. Onsite technical assistance occurred regularly throughout the project, and the local Oral Health Champion provided oversight to ensure providers participated as expected.
K. Sharing Results 32. Are you planning to present this QI project and its results in a:
Yes No Formal report to clinical leaders? Yes No Presentation (verbal or poster) at a regional or national meeting? Yes No Manuscript for publication?
L. Project Organizational Role and Structure 33. UMHS QI/Part IV MOC oversight – this project occurs within:
University of Michigan Health System • Overseen by what UMHS Unit/Group?
• Is the activity part of a larger UMHS institutional or departmental initiative?
No Yes – the initiative is:
Veterans Administration Ann Arbor Healthcare System • Overseen by what AAVA Unit/Group?
• Is the activity part of a larger AAVA institutional or departmental initiative?
No Yes – the initiative is:
An organization affiliated with UMHS to improve clinical care • The organization is: Altarum Institute
• The type of affiliation with UMHS is:
Accountable Care Organization type (specify which):
BCBSM funded, UMHS lead state-wide Collaborative Quality Initiative (specify which):
Other (specify): Project-specific agreement between UMHS and Altarum Institute for joint sponsorship of activities of the Michigan Caries Prevention Program funded by a Center for Medicare and Medicaid Innovation Health Care Innovation Award

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
Appendix A. Timeline for Waves of Groups Participating Fifteen groups participate, each group starting a month after the previous group starts. A group participates in two cycles of data-guided improvement over seven months. The first group starts July 1, 2015 and the last group finishes March 31, 2017.

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
Appendix B. Performance by Practice for Percent of Patients with Service Performed
Service Baseline
6/1-6/30/15 Post-Intervention
9/1-9/30/15 Post-Adjustment 11/1–12/31/15
Goal
Medical Practice A Oral health screening
9-month visit 0%* 17% (n=6) 40% (n=10) 75% 12-month visit 0%* 33% (n=6) 50% (n=6) 75%
Fluoride varnish 9-month visit 0%* 17% (n=6) 40% (n=10) 50% 12-month visit 0%* 50% (n=6) 50% (n=6) 50%
Recommend/refer to dental home
9-month visit 0%* 0% (n=6) 0% (n=10) 50% 12-month visit 0%* 0% (n=6) 17% (n=6) 50%
Medical Practice B Oral health screening
9-month visit 80% (n=15) 80% (n=15) 100% (n=13) 75% 12-month visit 0% (n=15) 53% (n=15) 100% (n=15) 75%
Fluoride varnish 9-month visit 0% (n=15) 40% (n=15) 77% (n=13) 50% 12-month visit 0% (n=15) 33% (n=15) 93% (n=15) 50%
Recommend/refer to dental home
9-month visit 0% (n=15) 0% (n=15) 100% (n=13) 50% 12-month visit 47% (n=15) 0% (n=15) 100% (n=15) 50%
Medical Practice C Oral health screening
9-month visit 0%* 0% (n=5) 100% (n=11) 75% 12-month visit 0%* 0% (n=5) 100% (n=11) 75%
Fluoride varnish 9-month visit 0%* 0% (n=5) 36% (n=11) 50% 12-month visit 0%* 20% (n=5) 45% (n=11) 50%
Recommend/refer to dental home
9-month visit 0%* 0% (n=5) 100% (n=11) 50% 12-month visit 0%* 0% (n=5) 100% (n=11) 50%
Medical Practice D Oral health screening
9-month visit 0%* 100% (n=6) 100% (n=3) 75% 12-month visit 0%* 100% (n=4) 100% (n=3) 75%

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
Fluoride varnish 9-month visit 0%* 0% (n=6) 33% (n=3) 50% 12-month visit 0%* 0% (n=4) 33% (n=3) 50%
Recommend/refer to dental home
9-month visit 0%* 0% (n=6) 100% (n=3) 50% 12-month visit 0%* 100% (n=4) 100% (n=3) 50%
Medical Practice E Oral health screening
9-month visit 0%* 100% (n=4) 100% (n=12) 75% 12-month visit 0%* 100% (n=1) 100% (n=6) 75%
Fluoride varnish 9-month visit 0%* 25% (n=4) 0% (n=12) 50% 12-month visit 0%* 0% (n=1) 17% (n=6) 50%
Recommend/refer to dental home
9-month visit 0%* 0% (n=4) 100% (n=12) 50% 12-month visit 0%* 0% (n=1) 100% (n=6) 50%
Mean percent for all practices (N = 5 practices) Oral health screening
9-month visit 16% 59% 88% 75% 12-month visit 0% 57% 90% 75%
Fluoride varnish 9-month visit 0% 16% 37% 50% 12-month visit 0% 21% 48% 50%
Recommend/refer to dental home
9-month visit 0% 0% 80% 50% 12-month visit 9% 20% 83% 50%
% = percent of patients that received the service n = number of eligible patient charts pulled * = the clinic did not previously provide the service, so no charts were pulled and the clinic mean
at baseline is 0%

University of Michigan Health System Part IV Maintenance of Certification Program [Form 8/14/15]
Appendix C. Model for Workflow to Provide Caries Prevention Services