Embed Size (px)
Citation preview
Folic acid supplementation and fortification in Nova Scotia
Michiel Van den HofDalhousie UniversityHalifax, Nova Scotia
History of Folate History of Folate ResearchResearch
1976-1991 - Numerous small studies suggesting benefit of folic acid supplementation
1991- “Landmark” paper on benefit of folic acid supplementation to reduce the
recurrence of NTDs*
* MRC Vitamin Study Research Group: Lancet 1991
History of Folate History of Folate ResearchResearch
1992 -Research shows that folic acid supplementation reduces open NTDs in low-risk women*
*Czeizel AE, Dudas I: N Engl J Med 1992
History of Folate History of Folate ResearchResearch
1991 - 1994
- Canadian recommendations about folic acid supplementation issued:
- Health Canada
- SOGC
- Canadian Task Force on the Periodic Health Examination
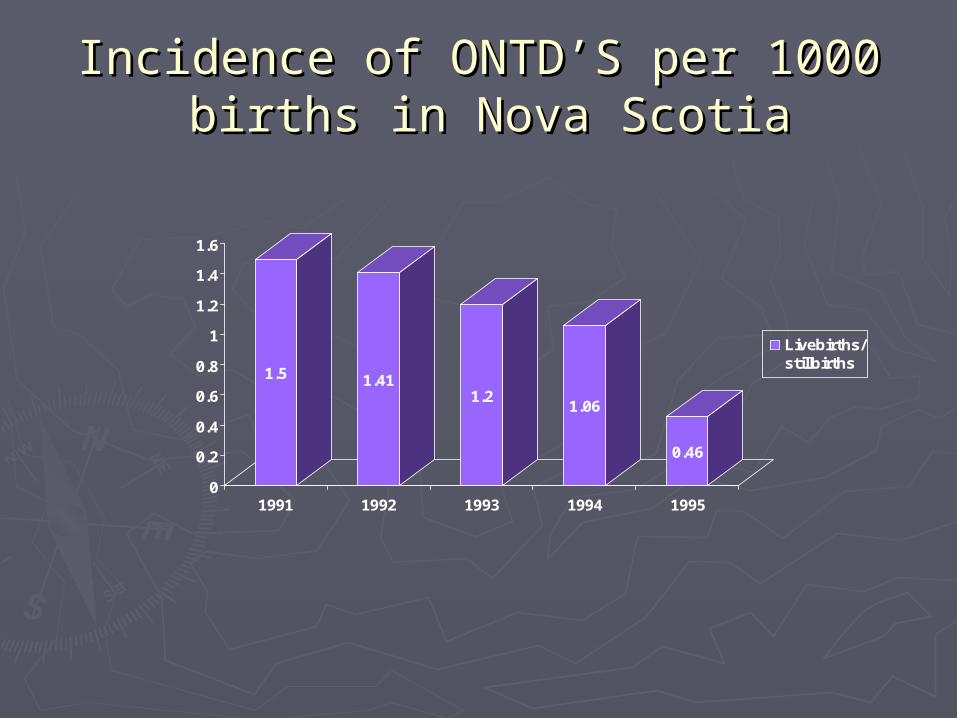
Incidence of ONTD’S per 1000 Incidence of ONTD’S per 1000 births in Nova Scotiabirths in Nova Scotia
1.5 1.411.2
1.06
0.46
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1991 1992 1993 1994 1995
Livebirths/stillbirths
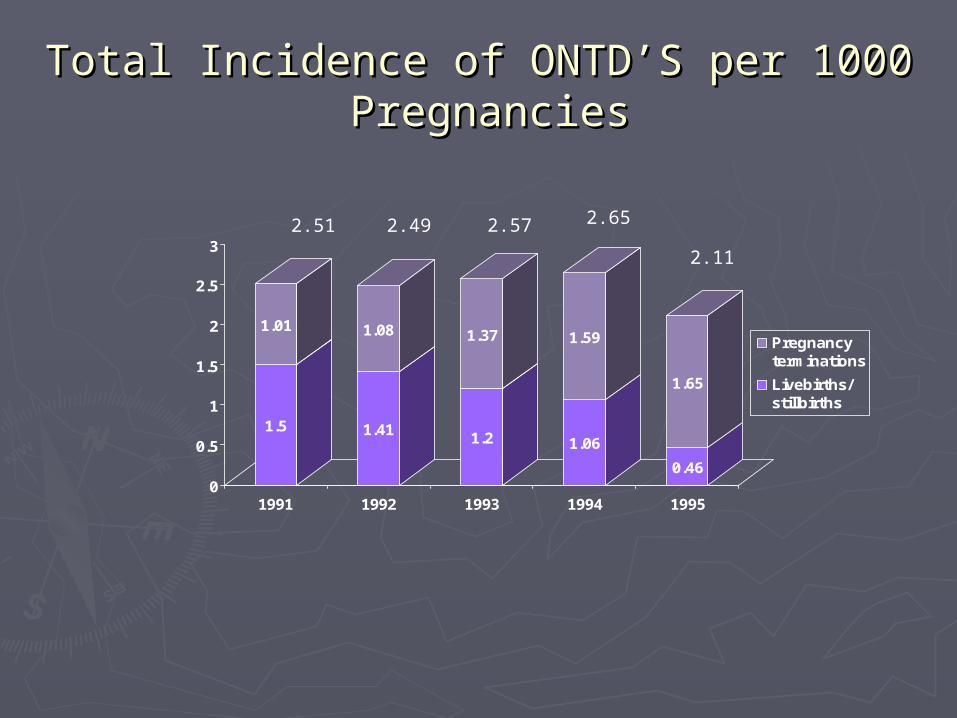
Total Incidence of ONTD’S per 1000 Total Incidence of ONTD’S per 1000 PregnanciesPregnancies
1.5
1.01
1.41
1.08
1.2
1.37
1.06
1.59
0.46
1.65
0
0.5
1
1.5
2
2.5
3
1991 1992 1993 1994 1995
Pregnancyterminations
Livebirths/stillbirths
2.51 2.49 2.57 2.65
2.11
History of Folate History of Folate ResearchResearch
1993 - 1999
- < 45% of pregnant women taking folic acid before conception
History of Folate History of Folate ResearchResearch
March 1996
- US-FDA orders all enriched grain products to be fortified (.14/100gm) starting January 1, 1998
History of Folate History of Folate ResearchResearch
November 1, 1998
- Health Canada endorses similar fortification
Questions?Questions?
Did recommendations for folic acid supplementation work?
Did the “small” amount of fortification work?
Folic Acid Folic Acid Supplementation/FortificationSupplementation/Fortification
Methods:
Nova Scotia Perinatal Database
plus
Nova Scotia Fetal Anomaly Database
combined have information on all births and birth defects that occur in this province.
Folic Acid Folic Acid Supplementation/FortificationSupplementation/Fortification
Open neural tube defects:
- spina bifida
- anencephaly
- other
Folic Acid Folic Acid Supplementation/FortificationSupplementation/Fortification
Pre-supplementation 1991-1994
Post-supplementation
but pre-fortification 1994-1997
Pre-fortification 1991-1997
Post-fortification 1998-2000
Folic Acid Folic Acid Supplementation/FortificatSupplementation/Fortificat
ionion
Risks for Folic Acid Fortification:
Delay diagnosis of vitamin B12 deficiency which may result in neurologic effects.
Folic Acid Folic Acid Supplementation/FortificatioSupplementation/Fortificatio
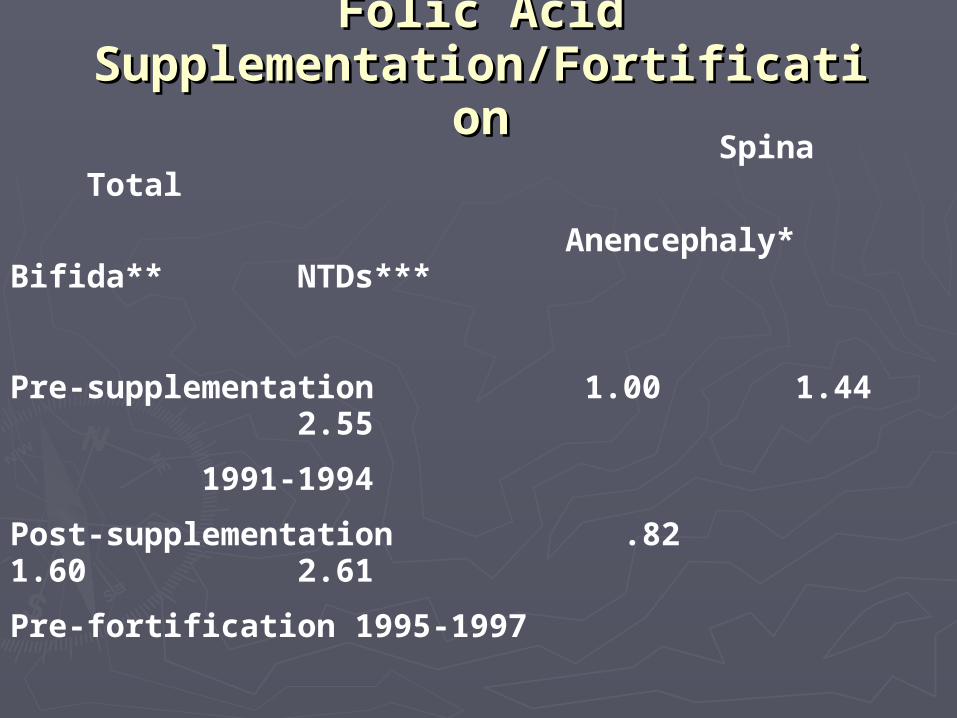
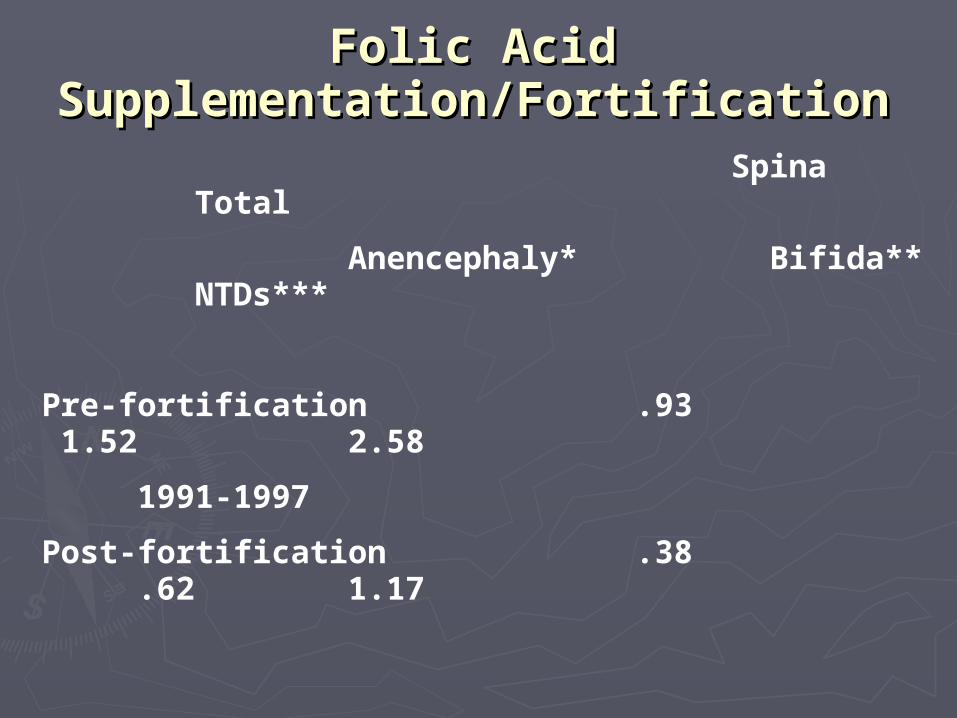
nn Spina Total
Anencephaly* Bifida** NTDs***
Pre-supplementation 1.00 1.44 2.55
1991-1994
Post-supplementation .82 1.60 2.61
Pre-fortification 1995-1997
*RR0.82,95%CI 0.51-1.32; p=0.49
**RR1.11,95%CI 0.79-1.60; p=0.64
***RR1.02,95%CI 0.77-1.35; p=0.87
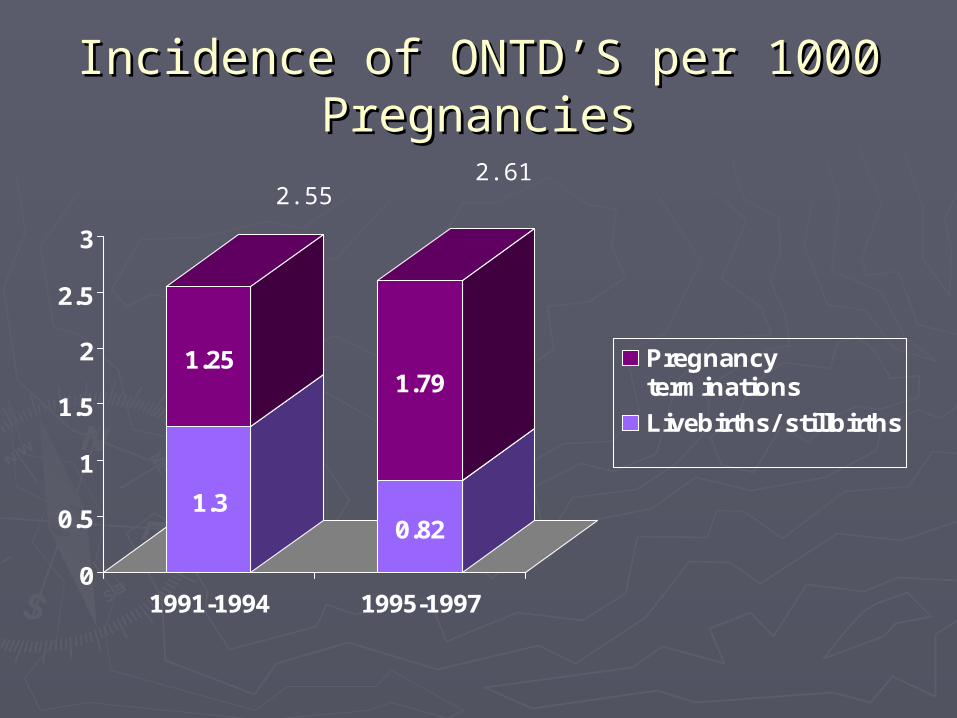
Incidence of ONTD’S per 1000 Incidence of ONTD’S per 1000 PregnanciesPregnancies
1.3
1.25
0.82
1.79
0
0.5
1
1.5
2
2.5
3
1991-1994 1995-1997
Pregnancyterminations
Livebirths/ stillbirths
2.552.61
Folic Acid Folic Acid Supplementation/FortificationSupplementation/Fortification
Spina Total
Anencephaly* Bifida** NTDs***
Pre-fortification .93 1.52 2.58
1991-1997
Post-fortification .38 .62 1.17
* RR 0.41, 95% CI 0.22-0.77; p=0.004
** RR 0.40, 95% CI 0.25-0.67; p<0.001
***RR 0.46, 95% CI 0.32-0.66; p<0.001
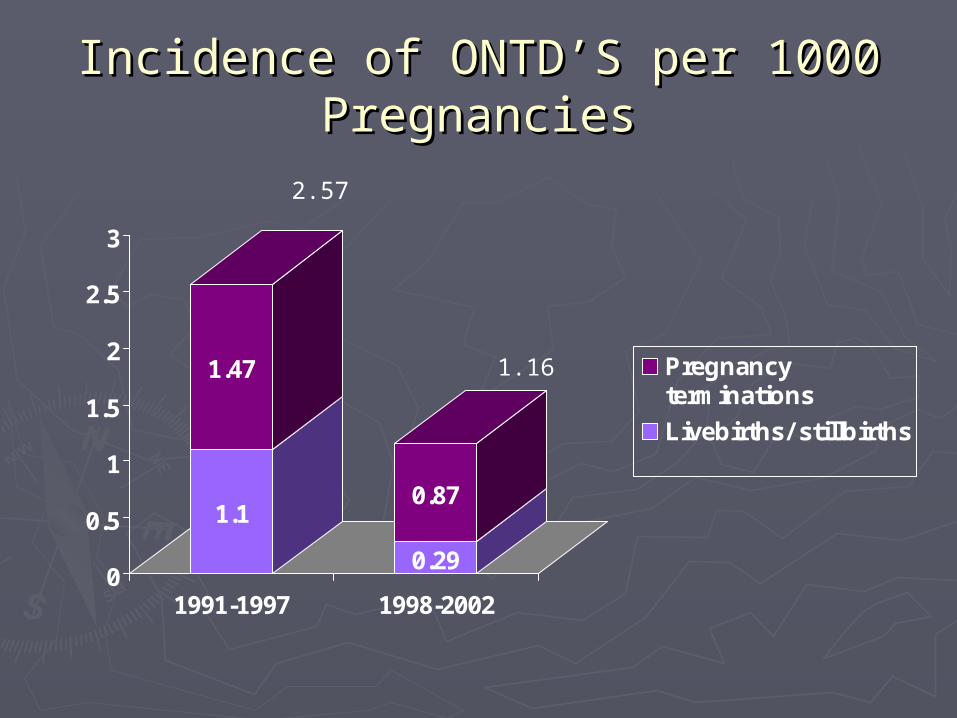
Incidence of ONTD’S per 1000 Incidence of ONTD’S per 1000 PregnanciesPregnancies
1.1
1.47
0.29
0.87
0
0.5
1
1.5
2
2.5
3
1991-1997 1998-2002
Pregnancyterminations
Livebirths/ stillbirths
1.16
2.57
Folic Acid Folic Acid Supplementation/FortificationSupplementation/Fortification
With the introduction of folic acid fortification, there was a 59% reduction in anencephaly
59% reduction in spina bifida
and a 54% reduction in all NTDs.
Calculated reduction ~ 20%
Folic Acid Folic Acid Supplementation/FortificationSupplementation/Fortification
Can prevention be further reduced?
Chinese study suggested ~ .6/1000 in both high and low-risk population.
Thus, further reduction may be possible,
1.0 .6 (40%).
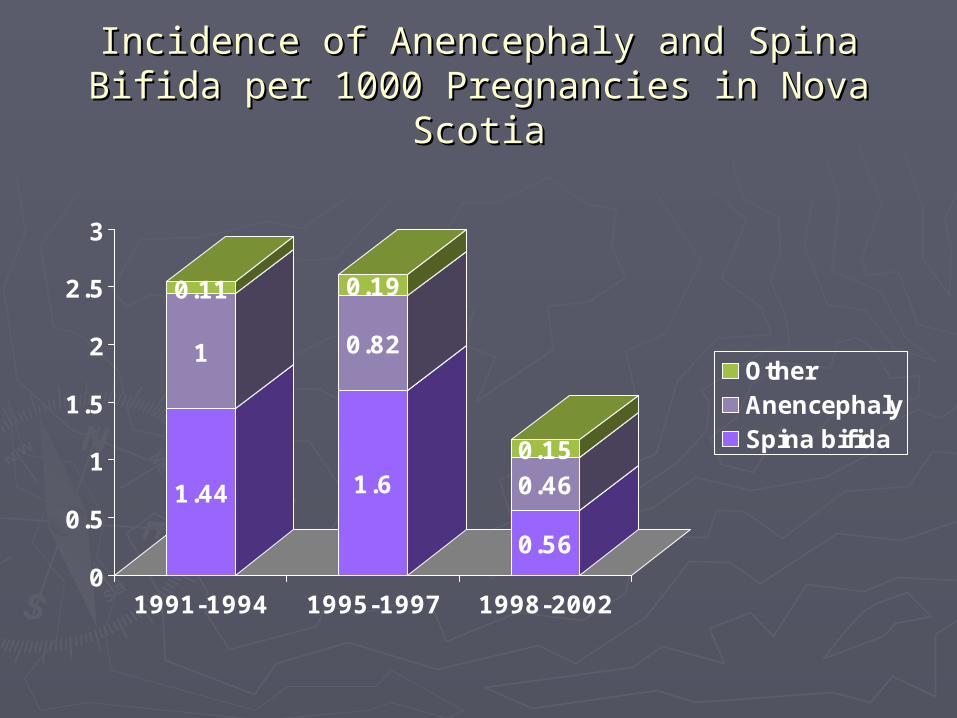
Incidence of Anencephaly and Spina Bifida per Incidence of Anencephaly and Spina Bifida per 1000 Pregnancies in Nova Scotia1000 Pregnancies in Nova Scotia
1.44
1
0.11
1.6
0.82
0.19
0.56
0.460.15
0
0.5
1
1.5
2
2.5
3
1991-1994 1995-1997 1998-2002
OtherAnencephalySpina bifida