Embed Size (px)
DESCRIPTION
Evaluation of a new Health Code requirement for discharging infectious tuberculosis patients from NYC hospitals. Michelle M. Macaraig, MPH Assistant Director for Planning and Policy Bureau of Tuberculosis Control NYC Department of Health and Mental Hygiene. Today’s presentation. Background - PowerPoint PPT Presentation
Citation preview

Evaluation of a new Health Code requirement for discharging infectious
tuberculosis patients from NYC hospitals
Michelle M. Macaraig, MPHAssistant Director for Planning and Policy
Bureau of Tuberculosis ControlNYC Department of Health and Mental Hygiene

Today’s presentation
• Background• Describe the new health code hospital
discharge requirements• Describe the Bureau of TB Control
(BTBC) implementation process• Provide preliminary evaluation results• Discuss common issues related to
hospital discharges

Background

Outpatient treatment of TB
• TB patients could be treated successfully as outpatients
• No significant difference between hospital and outpatient treatment
• Requirements for successful treatment include:– Prescription of the correct chemotherapy– Compliance with medication doses
• Directly observed therapy• Completion of a minimum number of doses

BTBC criteria for discharging patients with suspected or confirmed TB from the hospital
Assess if patientcan be treated as an outpatient
Begin treatment appropriate regimen
Obtain approval from BTBC to discharge patient

NYC Health Code Amendment

Rationale
• In 2009, 83% (255/308) of respiratory smear positive TB patients were hospitalized
• BTBC has observed private practitioners deviate from recommended TB management practices
• BTBC must be able to influence and ensure TB practices conform with accepted standards
• Legal and regulatory approach would be effective

NYC Health Code amendment
• New York City Health Code Article 11 Section 21(4)
– Hospitals/providers must obtain approval from health department at least 72 business hours before discharging infectious* TB patients
– DOHMH [through BTBC] must respond to the request for approval within one business day
• New requirement was implemented in November 2010
*positive sputum smear from a pulmonary or laryngeal source

Implementation and Process for Submitting
Hospital Discharge Plans

Implementation
• Communicated the health code amendment– Announcement made to public hospitals– Letters sent to health care providers– Memo sent to BTBC staff
• Developed forms and guides• Developed a plan to review and provide feedback to
providers• Trained BTBC staff• Modified sections of the TB registry to track
discharge requests

Hospital discharge forms
Available on NYC Health Department’s website: www.nyc.gov/health/tb

Discharge plan approval process
Determination72 hour before discharge Within 1 business day
Provider • discusses discharge plan issues with DOHMH • revises plan• informs DOHMH
Provider submits Hospital Discharge Approval Request Form to BTBCvia fax
BTBC physician • Reviews discharge plan • Makes determination• Communicates withhospital provider
Not Applicable
Approved
Not approved

Determination
• Approved: criteria for discharge met• Not approved: additional actions or
information needed • Not applicable: extrapulmonary TB
cases, noninfectious cases, atypical mycobacterium (NTM)

Evaluation

Evaluation questions
• Are hospitals/providers compliant with the new health code requirement?
• What proportion of discharge requests met criteria for discharge?
• What were the reasons discharges were not approved?

Analysis
• Identified all hospitalized infectious TB patients who were reported to BTBC between November 1, 2010-March 1, 2011
• Reviewed discharge plans• Obtained data from the NYC TB registry

Results

Submission of hospital discharge plans
Sputum smear positive TB patients *
97
*Suspected and confirmed
Discharged smear positive
48 (50%)
Still in hospital33 (34%)
Discharged smear negative
16 (17%)
Plan submitted22 (46%)
No plan submitted26 (54%)
Plan submitted
9 (56%)
No plan submitted
7 (44%)
Plan submitted10 (30%)
No plan submitted23 (70%)

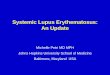
Patients discharged from the hospital while acid fast bacilli sputum smear positive, by
submission of discharge plan (n=48)
H1
H2
H3
H4
H5
H6
H7
H8
H9
H10
H11
H12
H13
H14
H15
H16
H17
H18
H19
H20
H21
H22
H23
H24
H25
H26
H27
0
1
2
3
4
5
6Plan submitted No plan submitted
Hospital
Nu
mb
er o
f p
atie
nts

Compliance with Health Code time requirements
• Median days from discharge plan submission to planned discharge was 1 day (range: -4 to 5)– 23% (9/41) of plans submitted did not have
a planned discharge date• Median number of days for BTBC physician to
respond to treating provider was 0 days (range: <1-3)

Initial determination for discharge plans submitted to BTBC
Not approved 14 (35%)
Approved24 (60%)
Not Applicable2 (5%)

Primary reasons for initial determination of “Not Approved” among discharge plans (n=14)*
Reasons # %
Home assessment not complete 6 43
Discharge plan form incomplete 3 22
DOT not offered/agreed 2 14
Discharged to congregate setting/unstable residence
1 7
Inadequate treatment regimen 1 7
Children <5 in house not evaluated 1 7
*Some submitted plans had multiple issues that may have contributed to “not approved” determination

Conclusion
• Compliance with the new Health Code provision was low
• Timeframe requirements for submission of discharge plans were not met
• Over half of discharge plans were approved at initial review
• Most common reason for disapproval of a request was incomplete home assessment followed by incomplete discharge request form

Future Considerations
• Continue collaboration with hospitals• Monitor submission of hospital discharge
plans• Outreach to hospitals/providers
experiencing issues with plans• Evaluate impact of initiative at one year

Acknowledgements
• NYC DOHMH Bureau of TB Control Provider Outreach Project Working Group
• NYC DOHMH Bureau of TB Control Staff• NYC Infection Control Nurses and
Practitioners

Thank You!
Questions?

Extra slides

Discharge of NYC Residents from Non-NYC Hospital
•NYC DOHMH will work with discharging hospital &/or the local public health authorities to ensure discharge plans conform to NYC standards

Responsibilities of providers
• Complete and legible forms • Appropriate contact information for the treating
physician/attending MD • Notification of any issues with medications, side
effects or abnormal lab values• Specialized nursing needs : PICC lines, injections• Discharges to congregate settings or home care
agency referrals• Discharges to other jurisdictions requiring interstate
notification• How many days of medication provided to patient• Follow-up appointment date –should be close to date
of discharge

Responsibilities of BTBC
• Field staff need to interview patient to elicit contacts
• Home assessment should be done• Patient to agree to home isolation and
DOT– Sign agreements for both
• Follow up appointment is made

Treatment of TB in India
• Tuberculosis Chemotherapy Centre, Madras, compared home treatment of TB with sanatorium – Treatment at home is satisfactory
• Crowded living conditions, low nutritional standards, low income
• Major risk to contacts lies in exposure to the infectious case BEFORE diagnosis
Tuberculosis Chemotherapy Centre, Madras. Bull WHO 1960, 23; 463-510

Successful Treatment of TB
Requirements for successful treatment include:
• Prescription of the correct chemotherapy• Compliance with medication doses
– Achieved as outpatient with DOT• Completion of a minimum number of doses
All of which can be done as an outpatient!

Risks of Hospitalization
• Nosocomial transmission to:– Health care workers– Vulnerable patients
• Anxiety for the patient who is isolated– Feeling of isolation – Removal from social supports– Loss of control over one’s life