Embed Size (px)
Citation preview

Michael F. Michelis, M.D., F.A.C.P., F.A.S.N.Director, Division of Nephrology
Lenox Hill Hospital, New York
Clinical Professor of MedicineNew York University School of Medicine
Conventional and Novel Therapy
TREATMENT OF ACUTE HYPONATREMIA

Hyponatremia is the most common electrolyte disorder seen
in hospitalized patients.
Hyponatremia 21 %
Hypokalemia 12 %
Hyperkalemia 10 %
Hypernatremia 5 %

LECTURE GOALLECTURE GOAL
UNDERSTANDING UNDERSTANDING HYPONATREMIC HYPONATREMIC ENCEPHALOPATHY (HE) ENCEPHALOPATHY (HE)
•• Risk factorsRisk factors
•• Signs and symptomsSigns and symptoms
•• TherapyTherapy

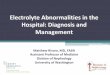
Anatomy of Hyponatremia
Glomerulus – Filtration
Proximal Tubule – Na Reabsorption
Loop of Henle – Na K 2 Cl Transport
Distal Nephron – AVP

DeFronzo RA, Arieff AI. Fluid Elec, A-B,pg 259, Churchill Livingstone, 1995

AVP RELEASE
Hypothalamus
Osmo Supraoptic &
Receptors Paraventricular nuclei
axonal flow to
Posterior pituitary ( or release)

AVP RELEASE
Baroreceptors and volume receptors
Volume Aortic arch, carotid sinus and atria
Receptors Parasympathetic afferent pathway
back to
Hypothalamus ( or release)
(can override osmolar)

Regulate Vascular Tone
Regulate H2 OReabsorption by the Kidney
AVP (ADH)
V1a Receptors V2 Receptors



RISK FACTORS FOR HERISK FACTORS FOR HE
•• PostPost--operative stateoperative state
•• Cortisol deficiencyCortisol deficiency
•• Nausea, emesis, pain, stressNausea, emesis, pain, stress
•• Female sex steroids Na/K/ATPaseFemale sex steroids Na/K/ATPase
•• HypoxiaHypoxia--limits adaptationlimits adaptation
•• CNS disease or surgeryCNS disease or surgery
•• Children < 16 yearsChildren < 16 yearsMoritz M. Ped Nephrol 2010; 25: 1225Moritz M. Ped Nephrol 2010; 25: 1225--12381238

SYMPTOMS AND SIGNS OF HESYMPTOMS AND SIGNS OF HE
HeadacheHeadache
Nausea and Nausea and vomitingvomiting
LethargyLethargy
WeaknessWeakness
ConfusionConfusion
AgitationAgitation
SeizuresSeizures
ComaComa
ApneaApnea
Pulmonary edemaPulmonary edema
PapilledemaPapilledema
Cardiac arrhythmiasCardiac arrhythmias

CHILDREN VS ADULTSCHILDREN VS ADULTS
Average serum sodium in children with Average serum sodium in children with hyponatremic encephalopathy is 120 mEq/L hyponatremic encephalopathy is 120 mEq/L vs adults is 111 mEq/L.vs adults is 111 mEq/L.
A childA child’’s brain reaches adult size by 6 years of s brain reaches adult size by 6 years of age but the skull does not reach adult size age but the skull does not reach adult size until 16 years of age. until 16 years of age.
Therefore, herniation occurs at higher serum Therefore, herniation occurs at higher serum sodium levels in children.sodium levels in children.

ACUTE HYPONATREMIA/TRAUMA ACUTE HYPONATREMIA/TRAUMA (CEREBRAL EDEMA) (CEREBRAL EDEMA)
VSVS
CHRONIC HYPONATREMIA (CHRONIC HYPONATREMIA (BRAIN BRAIN ADAPTATION, LOSS OF ELECTROLYTES ADAPTATION, LOSS OF ELECTROLYTES AND OSMOLYTES. MAY LEAD TO CPM AND OSMOLYTES. MAY LEAD TO CPM
SECONDARY TO DEHYDRATION IF SECONDARY TO DEHYDRATION IF OVERCORRECTION OCCURS)OVERCORRECTION OCCURS)

Diagnostic Approach for the Syndrome of Inappropriate Antidiuretic Hormone Release
Diagnostic CriteriaDecreased extracellular fluid effective osmolality(<270 mOsm/kg H2O)
Inappropriate urinary concentration(>100 mOsm/kg H2O)
Clinical euvolemia
Elevated urinary sodium concentration underconditions of a normal salt and water intake
Absence of adrenal, thyroid, pituitary, or renalinsufficiency or diuretic use

Diagnostic Criteria for SIADH
Supplemental
Abnormal H2O load test
Plasma AVP level inappropriately high relative to plasma osmolality
No significant correction of plasma [Na+] with volume expansion, but improvement after fluid restriction
SIADH=syndrome of inappropriate antidiuretic hormone secretionJanicic N et al. Endocrinol Metab Clin N Am. 2003;23:459-481Kumar S et al. In: Atlas of Diseases of the Kidney. 1999:1.1-1.21

CASE 1CASE 1Healthy 3 year old brought to ER with 1 day Healthy 3 year old brought to ER with 1 day
history N&V. Blood pressure 85/60 mm Hg. history N&V. Blood pressure 85/60 mm Hg. ExamExam--dry. Chemistries normal except dry. Chemistries normal except increased BUN. Child received 2 boluses of increased BUN. Child received 2 boluses of normal saline IV. Child admitted and then normal saline IV. Child admitted and then treated with treated with ““2/3 and 1/32/3 and 1/3”” at 130 mL per hr IV. at 130 mL per hr IV. The child voided about 110 mL urine and The child voided about 110 mL urine and received 1.5 liters IV fluid. The child received 1.5 liters IV fluid. The child developed lethargy, incontinence and serum developed lethargy, incontinence and serum sodium now 120 mEq/L. Seizures developed, sodium now 120 mEq/L. Seizures developed, and mannitol and saline were given prior to and mannitol and saline were given prior to demise. What went wrong? Therapy?demise. What went wrong? Therapy?Koczmara C. CJHP 2009; 62: 512Koczmara C. CJHP 2009; 62: 512--515515

CASE 2CASE 2
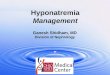
A 7 year old girl with cloacal exstrophy presented A 7 year old girl with cloacal exstrophy presented with 2 large bladder stones in association with with 2 large bladder stones in association with cutaneous fistulae after a prior gastriccutaneous fistulae after a prior gastric--ileal ileal augment, bladderaugment, bladder--neck reconstruction. During neck reconstruction. During the 35 minute procedure to remove the stones, the 35 minute procedure to remove the stones, a total of 2 liters of sterile water was used for a total of 2 liters of sterile water was used for bladder irrigation for stone fragment removal. bladder irrigation for stone fragment removal. Postoperatively, she was extubated but Postoperatively, she was extubated but became lethargic and irritable prior to became lethargic and irritable prior to respiratory arrest. Serum sodium 120 mEq/L. respiratory arrest. Serum sodium 120 mEq/L. CT showed massive cerebral edema. What CT showed massive cerebral edema. What went wrong? Therapy?went wrong? Therapy?Walker MR. JP Urol. 2008; 4:231Walker MR. JP Urol. 2008; 4:231--233233

SEVERE CEREBRAL EDEMA

SODIUM AND WATER SAMPLE SODIUM AND WATER SAMPLE CALCULATIONCALCULATION
18 L X 140 mEq/L 18 L X 140 mEq/L = 133 mEq/L= 133 mEq/L
19 L19 L

CASE 3CASE 3
13 year old boy admitted with depressed level of 13 year old boy admitted with depressed level of consciousness secondary to severe consciousness secondary to severe hyponatremia of 116 mEq/L. At age 3 months hyponatremia of 116 mEq/L. At age 3 months nasofrontal encephalocele repaired with nasofrontal encephalocele repaired with subsequent DI, hypothyroidism and AI. Treated subsequent DI, hypothyroidism and AI. Treated with corticosteroids, thyroid and DDAVP. with corticosteroids, thyroid and DDAVP. Following admission, serum sodium increased Following admission, serum sodium increased during 48 hours to 176 mEq/L. Neurologic during 48 hours to 176 mEq/L. Neurologic status worsened and MRI demonstrated status worsened and MRI demonstrated changes consistent with extrapontine changes consistent with extrapontine myelinolysis. What went wrong? Therapy?myelinolysis. What went wrong? Therapy?
Ranger A. Ped Neurosurg. 2010; 46:318Ranger A. Ped Neurosurg. 2010; 46:318--323323

AVOIDANCE OF AND MANAGEMENT AVOIDANCE OF AND MANAGEMENT OF DYSNATREMIASOF DYSNATREMIAS
Frequent monitoring and measurement Frequent monitoring and measurement of serum sodium levels in at risk of serum sodium levels in at risk patientspatients
Infusion of 3% saline for hyponatremic Infusion of 3% saline for hyponatremic encephalopathyencephalopathy

THREE PERCENT SALINE AND THREE PERCENT SALINE AND TRANSPORT (n=101)TRANSPORT (n=101)
Mean age 5.9 yMean age 5.9 y
Mean weight 27.6 kgMean weight 27.6 kg
MVA (n) 23MVA (n) 23
Hyponatremia (n) 6Hyponatremia (n) 6
Mean dose 5.3 mL/kg (1.2Mean dose 5.3 mL/kg (1.2--24)24)
Sodium change 135 Sodium change 135 --> 143 mEq/L> 143 mEq/L
range (115range (115--152) 152) --> (127> (127--183)183)
Access Peripheral line (central, osseous)Access Peripheral line (central, osseous)Luu JL. Ped Emerg Care. 2011; 27: 113Luu JL. Ped Emerg Care. 2011; 27: 113--117117

OUTLINE FOR USE OF 3% SALINE OUTLINE FOR USE OF 3% SALINE IN HEIN HE
•• 2 mL/kg of 3% NaCl over 10 minutes. 2 mL/kg of 3% NaCl over 10 minutes. Maximum 100 ccMaximum 100 cc
•• Repeat bolus 1Repeat bolus 1--2 times as needed until 2 times as needed until symptoms improve. Goal 5symptoms improve. Goal 5--6 mEq/L increase6 mEq/L increase
•• Recheck SNa following second bolus or Recheck SNa following second bolus or
Q 2 HQ 2 H
•• HE is unlikely if no improvementHE is unlikely if no improvement
•• Stop therapy if either symptom free or SNa Stop therapy if either symptom free or SNa increases > 10 mEq/Lincreases > 10 mEq/L
Moritz M. Ped Nephrol 2010; 25: 1225Moritz M. Ped Nephrol 2010; 25: 1225--12381238

Avoidance of Overcorrectionof Hyponatremia
R.H. Sterns et al. Kidney Int 2009;76:587-589
Goal: 4 - 6 mEq/L
Remedy: 5% D/W at 6 ml/kg over 1 - 2 Hr
DDAVP 2 µg q 6 - 8 Hrs

Change in serum sodium concentration
Infusate sodium concentration –Patient Serum Na concentration
with 1L of infusate = Total body water + 1
Adrogué-Madias. Intensive Care Med 1997;23:309-316
Adrogué-Madias Formula

H.K. Mohmand et al. Clin JASN 2007;2:1110-1117

VAPTANSVAPTANS
The safety and effectiveness of The safety and effectiveness of vaptans in pediatric patients have vaptans in pediatric patients have not been studied.not been studied.

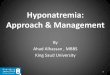
SERUM SODIUM RESPONDERS
B. Metzger, M. DeVita, M. Michelis. Int Urol Nephrol 2008;40:725-730
Day 0 Day 1
Serum Na
mEq/L
115
120
125
130
135

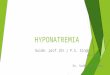
SERUM SODIUM RESPONDERS
B. Metzger, M. DeVita, M. Michelis. Int Urol Nephrol 2008;40:725-730
Day 0 Day 1
Urine Osm
mOsm/kg
100
200
300
400
500
600

CHF VS SIADHCHF VS SIADH
R. R. VaghasiyaVaghasiya, M. , M. DeVitaDeVita, M. Michelis. , M. Michelis. IntInt UrolUrol NephrolNephrol .2012; .2012; 44: 86544: 865--871871

TOLVAPTAN IN A SIX YEAR OLDTOLVAPTAN IN A SIX YEAR OLD
Ten kg male with CHF treated with furosemide,Ten kg male with CHF treated with furosemide,
thiazide and spironolactone gained weight andthiazide and spironolactone gained weight and
serum sodium decreased to 118 mEq/L. serum sodium decreased to 118 mEq/L.
Treated with tolvaptan 2Treated with tolvaptan 2--33--44--5 mg per day over5 mg per day over
30 days. Serum sodium increased to 13330 days. Serum sodium increased to 133
mEq/L and Uosm decreased to 216 mOsm/kg.mEq/L and Uosm decreased to 216 mOsm/kg.
Body weight decreased by 1.5 kg. Body weight decreased by 1.5 kg.
Horibate, et al. Card in the Young. 2013: 1Horibate, et al. Card in the Young. 2013: 1--33

HYPONATREMIA THERAPY HYPONATREMIA THERAPY SUMMARY:SUMMARY:
Boluses or infusions of 3% saline are Boluses or infusions of 3% saline are the most effective therapies for acute or the most effective therapies for acute or severe hyponatremic encephalopathysevere hyponatremic encephalopathy
Chronic hyponatremia with limited Chronic hyponatremia with limited symptoms and mild/moderate symptoms and mild/moderate decreases in serum sodium can be decreases in serum sodium can be managed by traditional and/or newer managed by traditional and/or newer therapeutic approachestherapeutic approaches

THANK YOUYOU