Embed Size (px)
Citation preview

The Advance Directive Hot Potato : The Why, When and How for the Conversation
Michael D. Harrington, M.D.
Division of Geriatrics and Palliative Care
MetroHealth Medical Center
April 8. 2016

�Absolutely no finances thus
�No financial conflicts to disclose
Disclosures

Objectives: Learners will…
� Appreciate the value and impact these discussions
can have for their patients, families and medical
team
� Gain understanding on timing on when to have
these conversations and the framework needed.
� Replace the medically indoctrinated advance
directive vocabulary with a more productive and
supportive vocabulary.

The Patient’s Good and the Ends of
Medicine
If medicine takes aim at death prevention, rather than at health and relief of suffering, if it regards every death as premature, as a failure of today’s medicine- but avoidable by tomorrow’s- then it is tacitly asserting that its true goal is bodily immortality… Physicians should try to keep their eyes on the main business, restoring and correcting what can be corrected and restored, always acknowledging that death will and must come, that health is a mortal good, and that as embodied beings we are fragile beings that must stop sooner or later, medicine or no medicine.
Kass LR. JAMA 1980;244:1947

The Nature of Suffering and the Goals of Medicine - Eric J. Cassell
The relief of suffering and the cure of disease must be seen as twin obligations of a medical profession that is truly dedicated to the care of the sick. Physicians’ failure to understand the nature of suffering can result in medical intervention that (though technically adequate) not only fails to relieve suffering but becomes a source of suffering itself.

“Seatbelts are carcinogenic”
� Prevention of one way of dying, in effect creates another way of death
� Increase probability of growing older and dying from another disease
� Newer, powerful medical tools often create new forms of suffering
� Society must recognize and take responsibility for these new forms of illness and associated dying
� James Hallenbeck “Palliative Care Perspectives”


Appreciate the value and impact these discussions can have for their patients,
families and medical team

What is Advance Care Planning?
� Planning for future medical care in the event patient is unable to make own decisions� Needs to be updated regularly
� Empowers patient to explore and express their own values and goals
� Determine proxy decision-maker
� It is a process, not an event
� Proper documentation avoids confusion & conflict

Patient Barriers to Completion of Advance Directives
� Belief that physicians should initiate discussions*� Patients felt discussions should occur earlier than MDs. At earlier age, earlier in disease history, earlier in patient-doctor relationship.
� Procrastination
� Apathy
� Belief that family should decide
� Family would be upset by the planning process
� Fear of burdening family members
� Discomfort with the topic
(*Johnston et al. Arch Intern Med, 1995)

Physician Barriers to Advance Care Planning
� Patients should initiate discussions� Physician lack of understanding of AD*� MD erroneous beliefs about appropriateness*� Lack of knowledge about AD’s*� Discomfort with the topic� Time constraints� Negative attitude� Prognostication avoidance
(* Morrison et al, Arch Intern Med, 1994)

Durable Power of Attorney for Health Care
Who is legally recognized by the State of Ohio to make health care
decisions for a patient?
� Guardian
� DPOA
� Familiar order
� What about significant others?

Non-decisional patients
1. Advanced directive – Living will supercedes proxy or guardian
2. Legal guardian or health proxy
3. 1st order relative
4. Opinions of other relatives
5. Physician’s judgement

Living Will� A mechanism for patient to express wishes for their care in advance
� To be enacted patient must not be able to participate and need 2 physicians to determine:� terminal condition� permanently unconscious state
� Once enacted, then administer no life sustaining therapies or withdraw life sustaining therapies
� Separate section for artificial hydration and nutrition






Gain understanding on timing on when to have these conversations and the
framework needed

Timing of when to discuss
� Routine health care – Preventive Visit
� Review with any changes� New diagnosis� Advancing or worsening illness� Prior to surgeries� Post hospitalization � Death in families
� How did it go?� Have you thought about your own death?

Knowledge Base Deficiencies� Natural history of disease is not emphasized
� Little experience in symptom management
� Little experience in the continuum of a disease
� Nature of suffering not recognized
0
10
20
30
40
50
60
70
80
90
100
1/1
/19
97
2/1
/19
97
4/1
/19
97
6/1
/19
97
8/1
/19
97
10
/1/1
99
71
2/1
/19
97
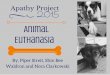
Function
CANCERCHF, COPDFRAILITY

Prognostication Pitfalls and Benefits
� No training or modeling
� Natural history of disease is new concept
� 37% of advanced chf told poor prognosis
� Markedly over-estimate prognosis
� Helps patient and family cope and plan
� Teach patient and family what to expect for illness
� 90% of patients want to discuss
� Advance directives
� Increase access to services like hospice

CPR is Therapeutic Treatment
� Goal of any therapy is to maintain or improve quality of life.
� No other therapy is treated in similar matter.
� Physicians need to guide patients and families.
� No legal or ethical obligation to provide

DNR Benefit vs. Burden
� General Public believes CPR works in 60-85%
� Over 60% success rate on TV
� AICD and AED confusion

History of CPR� Invented in 1960 to avoid open thoracotomy
� 1965 Monograph - CPR is indicated for the patient who, at the time of arrest, is not in the terminal stage of an incurable disease.
� Resuscitation will at best return them to the dying state.

American Heart AssociationFrom 1966 to present CPR guidelines remain the same
� Indicated in acute reversible situations
� Drowning, shock, drug effect, anesthesia, heart block, MI, surgery
� When CPR is not indicated, patients/proxies should be informed of the DNR order but not given a choice

CPR—contra-indications?� Chest wall pathology
� Myeloma, fractures
� Conditions in which the expected survival to discharge is close to 0%� Metastatic cancer with declining function
� Chronic renal failure on dialysis
� Multi-organ failure
� Sepsis
� Severe acute stroke

Survival and Complications
� Hospital patients: 15% survive to discharge
� Out-of-hospital arrest – 5%
� Chest wall trauma, aspiration: 25-50%
� Persistent Vegetative State: 10%
� MICU/SICU - 44% survive arrest, 5% survival to discharge
� Cost to family:
� Financial
� Emotional cost of prolonging dying
� Cost to health care team

Remember …
The procedure of CPR was never intended for use in patients dying an expected death from a chronic, fatal, medical illness.

Current Standards
� Full intervention is the default
� Rarely addressed when “healthier”
� When addressed --emergencies --obvious terminal decline
� Then often a cafeteria approach

Who Needs a DNR Discussion?
1. Inpatients w/ advanced life threatening illness
2. Inpatient w/ other “serious” chronic illnesses
3. Outpatients as part of routine advanced directive discussion or change in status
Note: In inpatients w/ non-life threatening diseases, CPR is assumed.

Decide if CPR is medically appropriate
� Before you meet with the patient, ask yourself this question:� Do you believe that CPR is an appropriate medical intervention for this patient at this time?
� Remember--CPR is a medical intervention—it has:� Indications and Contraindications
� Risks and Benefits
� Patients have no autonomous right to insist that you perform CPR
� Patient have decision making capacity?

Conducting the DNR Discussion
Physical Setting
� Quiet, comfortable room, beeper off
� Check personal appearance, sitting down
� Ask who patient wants to participate
� Are there others who you want to participate?
� Participants need to clearly define goals of meeting

Don’t Forget!!!
� If you recommend DNR status:1. Stress positive things that will be done:
� Pain and symptom relief
� Continued care to achieve goals
2. Reinforce that DNR doesnot mean “do not treat”


Replace the medically indoctrinated advance directive vocabulary with a more
productive and supportive vocabulary.

The “Goals of Care” need to drive the treatments, not diseases
� Patients must understand their diseases
� Patients must be told their prognosis
� Communication skills
� Commitment to patient and family
� Provider should not be afraid to help with decisions and give an opinion
� Burden versus benefit with all decisions
� “Hope for the best, prepare for the worse”

Unhelpful language inherent in our training
� If your heart stops, do you want to restart?
� Do you want us to do everything?
� If we do CPR we will break your ribs and you’ll need to be on a breathing machine, do you want us to do that?
� There is nothing more that we can do.
� Will you agree to discontinue care?
� It’s time we talk about pulling back
� I think we should stop aggressive therapy
� There is nothing more than can be done
� Avoid the term, “futility”

Language describing the goals of care� I want to give the best care possible until the day you die
� Based on what you said is important to you and advanced medical condition, I would recommend..
� We want to help you live meaningfully as long as you can
� We will aggressively treat your symptoms and support your goals
� I will aggressively treat you through the course of your disease and when your disease progresses I will recommend hospice services
� Hope for the best, but plan for the worse� I will be there for you and your family

Discussing Patient Goals is“GOOD”
�G – Goals
�O – Options/Objective Data
�O – Opinion
�D - Document

G – Goals� Set up meeting for success
� Seating position, pagers, supports
� Identify each member and stakeholders
� Get to know the patient� Hobbies, lifestyle, stories, values
� What are the stakeholders understanding and expectations?
� Identify option specific goals
� Clarify “big picture” first if needed

O – Options/Objective� Have a mental list of relevant options
� Benefits versus Burdens
� Probability - Framing Effect
� 1 in 5 better than 20%
� 15 % success rate = 85% failure rate
� Can Fill any objective data as well

O – Opinion
� Offer your opinion on treatment plan –more than just DNR
� Separate data from opinion –subconscious
� Opinion should reflect back to patient and family the goals established and reflect the patient values

D - Document
� List participants in the discussion/decision
� Recount the essence of discussion with attention to final decision
� Document patients wishes now and in event of future event.


























![Multidimensional Apathy: Evidence from Neurodegenerative … · 2018. 2. 12. · separate subtypes within neurodegenerative diseases: Dimensional Apathy Scale (DAS) [30]. These dimensions](https://img.pdfslide.us/doc/110x75/600fdcbf504842681322c1ba/multidimensional-apathy-evidence-from-neurodegenerative-2018-2-12-separate.jpg)