Disclosures We have no relevant financial disclosures. We will not be discussing any unapproved or off-label uses of therapeutic agents of products.
Michael D. Warren, MD MPH FAAP Division of Family Health and
Wellness
Tiny Victims of a Massive Problem: Neonatal Abstinence Syndrome and
Tennessees Prescription Drug Epidemic Michael D. Warren, MD MPH
FAAP Division of Family Health and Wellness Sheri Smith, RN Nursing
Director, Critical Care Services Disclosures We have no relevant
financial disclosures.
We will not be discussing any unapproved or off-label uses of
therapeutic agents of products. Objectives Review signs, symptoms,
and treatment related to Neonatal Abstinence Syndrome. Describe the
scope of the NAS epidemic and the larger prescription drug problem
in Tennessee. Identify state-level initiatives to prevent NAS.
Discuss collaboration between state and community partners on this
topic. Neonatal Abstinence Syndrome: Signs, Symptoms, and Treatment
NAS Background Describes withdrawal symptoms in neonates associated
with exposure to: Alcohol Barbiturates Benzodiazepines Opioids
Caffeine Anti-depressants Etc.. NAS Background NAS Background NAS
can be associated with:
Prescription drugs obtained with prescription Includes women on
pain therapy or replacement therapy Prescription drugs obtained
without prescription Illicit drugs NAS Background Opioid withdrawal
symptoms primarily related to:
Central Nervous System: Seizures Hyperactivity Tremors
Gastrointestinal System: Poor feeding Vomiting Poor weight gain
Diarrhea Uncoordinated sucking NAS Background Opioid withdrawal
symptoms:
May appear as early as within the first 24 hours May take as many
as 4-5 days to appear Occur in 55-94% of exposed infants NAS
Identification NAS is a clinical diagnosis NAS diagnosis based
on:
History of exposure Evidence of exposure: Maternal drug screen
Infant urine, meconium, hair, or umbilical samples Clinical signs
of withdrawal (symptom rating scale) NAS Treatment Initial
treatment: Pharmacologic therapy may be needed
Minimize environmental Stimuli Respond early to signals Support
adequate growth Pharmacologic therapy may be needed NAS Outcomes
Prenatal drug exposure associated with increased risks:
Cesarean delivery (OR ) Pre-term birth (OR ) Low birth weight (OR )
Feeding problems (OR ) Respiratory distress syndrome (OR ) Prenatal
opioid use associated with increased risk of: Spina bifida (OR )
Gastroschisis (OR ) Any heart defect (OR ) Creanga AA, et
al.Maternal drug use and its effect on neonatesa population-based
study in Washington state.Obstetrics and Gynecology (5): Broussard
CS, Rasmussen SA, Reefhuis J, et al. Maternal treatment with opioid
analgesics and risk for birth defects. Am J Obstet Gynecol
2011;204:314.e1-11. NAS Outcomes No definitive long-term syndrome
associated with neonatal opioid withdrawal Limited studies show:
Mixed outcomes of developmental assessment scores (hyperactivity,
short attention span, memory and perceptual problems) Resolution of
seizures Confounding by social/environmental variables Neonatal
Abstinence Syndrome: Scope of the Problem in US & TN NAS
Epidemiology (US) Over the past decade:
2.8-fold increase in NAS incidence 4.7-fold increase in maternal
opioid use Increase in hospital costs $39,400$53,400 78% charges to
state Medicaid programs Source:Patrick SW et al.Neonatal Abstinence
Syndrome and Associated Health Care Expenditures, United States,
Journal of the American Medical Association. 2012;307(18): NAS
Hospitalizations in TN: 1999-2011
Data sources: Tennessee Department of Health; Office of Health
Statistics; Hospital Discharge Data System (HDDS) and Birth
Statistical System. Analysis includes inpatient hospitalizations
with age less than 1 and any diagnosis of drug withdrawal syndrome
of newborn (ICD-9-CM 779.5). HDDS records may contain up to 18
diagnoses.Infants were included if any of these diagnosis fields
were coded Note that these are discharge-level data and not unique
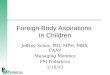
patient data. TN NAS Hospitalizations (2010)
Data sources: Tennessee Department of Health; Office of Health
Statistics; Hospital Discharge Data System (HDDS) and Birth
Statistical System. Numerator is number of inpatient
hospitalizations with age less than one and any diagnosis of
neonatal abstinence syndrome (ICD-9-CM 779.5). HDDS records may
contain up to 18 diagnoses.Infants were included if any of these
diagnosis fields were coded Note that these are discharge-level
data and not unique patient data.Denominator is number of live
births.For BSS data, county is mothers county of residence. TNs
Prescription Drug Problem
In 2011, Tennessee ranked 49th highest in the country for the
number of prescriptions filled per capita 17.6 prescriptions filled
per person National average:12.1 Kentucky and West Virginia tied
for highest (19.3 prescriptions per person) Data source: Henry J.
Kaiser Family Foundation.Retail Prescription Drugs Filled at
Pharmacies (Annual Per Capita), 2011. TNs Prescription Drug
Problem
Prescription Painkillers Sold By State, 2010 TN:2nd highest in
country for kilograms of prescription painkillers sold per 10,000
people Data source: CDC, Policy Impact Brief:Prescription
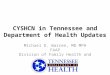
Painkiller Overdoses.Available at: Opioid Prescription Rates by
CountyTN, 2007-2011
2008 2009 2010 2011 Data source: Tennessee Department of Health;
Controlled Substance Monitoring Database. TNs Prescription Drug
Problem
Increase in TN deaths due to prescription drug overdose 422 in 2001
1,062 in 2011 More than deaths from: Motor vehicle accidents,
homicide, or suicide Opioids (methadone, oxycodone, and
hydrocodone) are by far the most-abused prescription drugs TNs
Prescription Drug Problem
51 pills per every Tennessean over age 12 275.5 Million Hydrocodone
Pills 22 pills per every Tennessean over age 12 116.6 Million Xanax
Pills The top three most prescribed controlled substances in
Tennessee in 2010 were: 275.5 million pills of hydrocodone (e.g.,
Lortab, Lorcet, Vicodin) 51 pills per every Tennessean over age of
12 116.6 million pills prescribed for alprazolam (e.g., Xanax: used
to treat anxiety) 22 pills per every Tennessean over age of 12
113.5 million pills prescribed for oxycodone (e.g., OxyContin,
Roxicodone) 21 pills for every Tennessean over age of 12 21 pills
per every Tennessean over age 12 113.5 Million Oxycodone Pills Data
source: Tennessee Department of Health; Controlled Substance
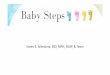
Monitoring Database. US Prescription Drug Problem
Rates of prescription painkiller sales, deaths and substance abuse
treatment admissions ( ) Graphic Source:CDC. Vital Signs, November
Prescription Painkiller Overdoses in the US.Available at: US
Prescription Drug Problem
Graphic Source:CDC. QuickStats: Number of Deaths From Poisoning,
Drug Poisoning, and Drug Poisoning Involving Opioid
AnalgesicsUnited States, 1999 Available at: Narcotics and
Contraceptive Use: TennCare Women, CY2012*
Demographics TennCare Women Women PrescribedNarcotics (>30 days
supplied) Narcotic Users Rate per 1,000 Women Prescribed
Contraceptives and Narcotics % of Women on Narcotics and
Contraceptives Women Prescribed Narcotics without Contraceptives %
of Women on Narcotics Not on Contraceptives All Women 296,687
42,082 141.8 7.538 18% 34,544 82% 84,398 2,054 24.3 987 48% 1,067
52% 44,620 3,897 87.3 1,432 37% 2,465 63% 53,333 8,689 162.9 2,199
25% 6,490 75% 48,912 10,442 213.5 1,699 16% 8,743 84% 37,483 9,319
248.6 805 9% 8,514 91% 27,940 7,681 274.9 416 5% 7,265 95% Data
source: Division of Health Care Finance and Administration, Bureau
of TennCare.*CY2012 data is provisional. Unintended Pregnancy Among
All Women & Opioid Abusers
Data source: For general population:Tennessee Department of
Health.Pregnancy Risk Assessment Monitoring System, 2009 Summary
Report.Available at:.For opioid-abusing women:Heil SH et
al.Unintended pregnancy in opioid-abusing women.Journal of
Substance Abuse Treatment March; 40(2): TennCare NAS Costs, CY2012*
Metric TennCare Paid Live Births1
TennCare non-LBWT Births TennCare Live LBWT Births2 NAS Infants
Number of Births 42,171 37,576 4,595 736 Cost for Infant in first
year of life $352,516,166 $177,959,049 $174,557,118 $45,870,410
Average Cost per child $8,359 $4,736 $37,988 $62,324 Average length
of stay (days) 3.5 2.0 15.8 26.2 Data source: Division of Health
Care Finance and Administration, Bureau of TennCare.*CY2012 data is
provisional. 1.This sample contains only children that were
directly matched to TennCares records based on Social Security
Number. 2 .Any infant weighing under 2,500g at the time of birth
was considered low birth weight (LBWT). TennCare Infants in DCS
Custody Within 1 Year of Birth, CY2012*
Infants born in CY 2012 NAS infants Total # of Infants 54,984 736
Total # infants in DCS 906 179 % in DCS 1.6% 24.3% Data source:
Division of Health Care Finance and Administration, Bureau of
TennCare.*CY2012 data are provisional. This sample contains only
children that were directly matched to TennCares records based on
Social Security Number. Neonatal Abstinence Syndrome: State-Level
Efforts NAS Subcabinet Working Group
Convened in late Spring 2012 Committed to meeting every 3-4 weeks
Cabinet-level representation from Departments: Public Health (TDH)
Childrens Services (DCS) Human Services (DHS) Mental Health and
Substance Abuse Services (DMHSAS) Medicaid (TennCare) Childrens
Cabinet The Levels of Prevention
PRIMARY Prevention SECONDARY Prevention TERTIARY Prevention
Definition An intervention implemented before there isevidence of a
disease or injury An intervention implemented after a disease has
begun, but before it is symptomatic. An intervention implemented
after a diseaseor injury is established Intent Reduce or eliminate
causative risk factors (risk reduction) Early identification
(through screening) and treatment Prevent sequelae (stop bad things
from getting worse) NAS Example Prevent addiction from occurring
Prevent pregnancy Screen pregnant women for substance use during
prenatal visits and refer for treatment Treat addicted women Treat
babies with NAS Adapted from:Centers for Disease Control and
Prevention.A Framework for Assessing the Effectiveness of Disease
and Injury Prevention.MMWR ; 41(RR-3); Available at: TennCare Prior
Authorization Form
Form available at:
https://tnm.providerportal.sxc.com/rxclaim/TNM/TC%20PA%20Request%20Form%20(Long%20Acting%20Narcotics).pdf
NASReportable Disease
Previous estimates of NAS incidence came from: Hospital discharge
data (all payers but ~18 month lag) Medicaid claims data (only ~9
month lag but only includes Medicaid) Need more real-time
estimation of incidence in order to drive policy and program
efforts NASReportable Disease
Add NAS to states Reportable Disease list Effective January 1, 2013
Collaborated with state perinatal quality collaborative (TIPQC) to
define reporting elements Align required reporting elements with
same data elements reported in hospital QI projects Drug Dependent
Newborns (Neonatal Abstinence Syndrome) Surveillance Summary For
the Week of November 10-November 16, 2013 (Week 46)1 Reporting
Summary (Year-to-date) Cases Reported:752 Male:441 Female:311
Unique Hospitals Reporting:50 Maternal County of Residence (By
Health Department Region) # Cases % Cases Davidson 33 4.4% East 204
27.1% Hamilton 13 1.7% Jackson/Madison 2 0.3% Knox 86 11.4%
Mid-Cumberland 49 6.5% North East 116 15.4% Shelby 15 2.0% South
Central 23 3.1% South East 11 1.5% Sullivan 79 10.5% Upper
Cumberland 98 13.0% West Total 752 100% Source of Maternal
Substance (if known)2 # Cases2 % Cases Supervised replacement
therapy 344 45.7% Supervised pain therapy 147 19.5% Therapy for
psychiatric or neurological condition 58 7.7% Prescription
substance obtained WITHOUT a prescription 294 39.1%
Non-prescription substance 214 28.5% No known exposure but clinical
signs consistent with NAS 11 1.5% No response 19 2.5% 1.Summary
reports are archived weekly at: 2.Multiple maternal substances may
be reported; therefore the total number of cases in this table may
not match the total number of cases reported. NASReportable
Disease
Maternal County of Residence (By HD Region) # Cases % Cases
Davidson 33 4.4% East 204 27.1% Hamilton 13 1.7% Jackson/Madison 2
0.3% Knox 86 11.4% Mid-Cumberland 49 6.5% North East 116 15.4%
Shelby 15 2.0% South Central 23 3.1% South East 11 1.5% Sullivan 79
10.5% Upper Cumberland 98 13.0% West Total 752 100% 64% of cases in
East and Northeast TN 24% of cases in Middle TN and Plateau
NASReportable Disease
Only substances prescribed to mother 41.7% Substance exposure
unknown 4.0% Only illicit or diverted substances 33.4% Mix of
prescribed and non-prescribed substances 20.9% Data
source:Tennessee Department of Health, Neonatal Abstinence Syndrome
Reporting Data.Data through 10/26/2013. NASReportable Disease
Important caveat: Reporting is for surveillance purposes only. Does
not constitute a referral to any agency other than the Tennessee
Department of Health. Does not replace requirement to report
suspected abuse/neglect. Controlled Substance Monitoring
Database
Established in 2006 Monitor prescribing of controlled
substancesdrugs illegal to use except with prescription Drug
Enforcement Agency (DEA) Schedule IIV Provider participation was
previously voluntary Controlled Substance Monitoring Database
Prescription Safety Act of 2012 All prescribers required to
register by 1/1/13 Starting 4/1/2013, prescribers required to check
the database before prescribing any opioid or benzodiazepine as a
new course of treatment and at least annually when said controlled
substance remains part of the treatment Dispensers must report at
least every 7 days to CSMD Controlled Substance Monitoring
Database
Provider Opioid Prescription Tennessee Pharmacy I will now walk you
through the algorithm of how data gets into the TNCSMP. A provider
writes an opioid prescription for a patient. The patient takes the
prescription to a pharmacy in Tennessee. The pharmacist dispenses
the medication, manually logs onto the TNCSMP database and enters
information about the prescription, the provider, the patient, and
the pharmacy. Providers and pharmacies logging into the database
now has access to patient prescription histories in the database.
TNCSMP database Controlled Substance Monitoring Database
When a provider logs in the TNCSMP database to look up a patient,
they are able to see the following information on their patient.
CLICK Patient demographics, including name, date of birth and
address, Prescription information, including type of controlled
substance, date and quantity prescribed, prescriber and pharmacy at
which prescription was dispensed. Controlled Substance Monitoring
Database
Top 10 Prescriptions reported to CSMD, 2012 When a provider logs in
the TNCSMP database to look up a patient, they are able to see the
following information on their patient. CLICK Patient demographics,
including name, date of birth and address, Prescription
information, including type of controlled substance, date and
quantity prescribed, prescriber and pharmacy at which prescription
was dispensed. Controlled Substance Monitoring Database
Risk Factor Cases N=592 Number (%) Controls N=11,840 AORs 95%
Confidence Interval Provider shopping 227 (38) 513 (4) 5.1 Pharmacy
shopping 145 (24) 196 (2) 4.5 High dosage use 140 (24) 172 (1) 13.2
Source:Dr. Jane Baumblatt, TN Department of Health.Case control
analysis of TN Controlled Substance Monitoring Database Neonatal
Abstinence Syndrome: Opportunities for Prevention and Collaboration
NASPrimary Prevention
Prevent pregnancy from occurring Provider education Counseling by
providers at initial prescription Promotion of contraceptives,
particularly long-acting reversible contraceptives (LARCs) Work
with non-traditional partners to promote counseling re: addition
during pregnancy and contraceptives A&D Pain clinics Drug
courts NASSecondary Prevention
Identify pregnant women who may be opioid addicted Identify
reproductive-aged women via CSMD whose fill patterns suggest risk
of dependence Referral to TennCare managed care organization case
management programs Screen women for drug use Consent of patient
Supportive rather than punitive approach NASTertiary
Prevention
Minimize complications for women who are addicted (and their
neonates) Can addicted pregnant women be weaned? What are best
strategies for treating NAS infants? NASWhat Can You Do? Connect
family with: Primary care medical home
TennCare or other insurance TN Early Intervention Services (TEIS)
Help Us Grow Successfully (HUGS) Childrens Special Services (CSS)
Family Planning WIC NASWhat Can You Do? Promote long-acting
reversible contraceptives (LARCs) Intrauterine devices Subdermal
implant Collaborate with local prescription drug drop-off efforts
For prescribers:Register for and use CSMD NASWhat Can You Do?
Decide whether referral to Department of Childrens Services is
appropriate State law requires all persons to make a report when
they suspect abuse, neglect or exploitation of children NAS
Resources NAS Main Page Weekly Surveillance Summary Archive
Weekly Surveillance Summary Archive Contact Information Michael D.
Warren, MD MPH FAAP Director, Division of Family Health and
Wellness Tennessee Department of Health Sheri Smith, RN Nursing
Director, Critical Care Services East TN Childrens Hospital