Embed Size (px)
Citation preview
MFP and Transition Coordination Refresher Training
Department of MedicalAssistance Services
Webinar
MFP and Transition Coordination Refresher Training Agenda
MFP – National Initiative New MFP Eligibility Criteria New Waiver Supports as a Result of MFP Outreach Efforts Keys to a Successful Transition Planning and Risk Assessment Transition Process, MFP Enrollment and Required Forms Consumer Direction Transition Services Administration and Reimbursement
for Rendering Waiver Services Additional Resources

An award from the Centers for Medicare and Medicaid Services Gives individuals of all ages and all disabilities who live in
Virginia LTC institutions options for community living
This Project has three Objectives:
Goal 1 - To give individuals who live in inpatient institutions more informed choices and options about where they can live and receive services;
Goal 2 - To transition individuals from institutions if they choose to live in the community; and
Goal 3 - To promote quality care through services that are person-centered, appropriate, and based on the individual’s needs.
MFP - National Initiative

MFP - National Initiative
MFP is the single largest investment in Medicaid Long Term Care 46 States have been awarded $4 Billion with a projected
number of over 70,000 individuals to be transitioned through calendar year 2016
Federal opportunity to further develop community integration strategies, systems, and infrastructure for individuals with long-term support needs
Emphasizes community living vs. institutional placement to help “rebalance” the system
A program that identifies individuals in institutions who wish to move back into the community and assists them with the transition process
MFP Eligibility
o New Eligibility Requirements – Effective June 1, 2011
o Have resided for at least 90 consecutive days in a hospital, nursing facility (any days spent in short-term skilled rehabilitation services do not count towards the 90 days), intermediate care facility for individuals with developmental disabilities (ICF-DD), long-stay hospital, institute for mental disorders (IMD), psychiatric residential treatment facility (PRTF), or a combination thereof;
o Be a resident of the Commonwealth of Virginia;
o Have received Medicaid benefits for inpatient services for at least one day prior to MFP enrollment;
MFP Eligibilityo Qualify for, and enroll into upon discharge, a Program for All-
inclusive Care for the Elderly (PACE) or one of the five following waiver programs:
o Elderly or Disabled with Consumer-Direction Waiver (EDCD) o Individual and Family Developmental Disabilities Support
Waiver (DD) o HIV/Aids Waiver (AIDS) o Intellectual Disabilities Waiver (ID) o Technology Assisted Wavier (TECH); and
o Move to a “qualified residence.” A qualified residence is: 1) a home that the individual or the individual’s family member owns or leases; 2) an apartment with an individual lease, with lockable access and egress, that includes living, sleeping, bathing and cooking areas over which the individual or the individual’s family has domain and control; or 3) a residence in a community-based residential setting in which no more than four (4) unrelated individuals reside.

MFP Eligibility
MFP Qualified InstitutionsHospital Nursing FacilityIntermediate Care Facility for Individuals
with Developmental Disabilities (ICF-DD) Long-stay Hospital Institute for Mental Disorders (IMD)Psychiatric Residential Treatment Facility
(PRTF)

MFP Eligibility
Certain days during a nursing facility stay must be excluded from the 90 day countAny days spent in short-term skilled
rehabilitation services are excludedConfirm with billing office
Have received Medicaid benefits for inpatient services for at least one day prior to MFP enrollment;

Waiver Services Added
Transition Services is a one-time, life-time benefit assisting with one-time, up-front household expenses. Added to EDCD, AIDS, TECH, ID and DD waivers. $5,000 maximum Time limited to 9 months Not available to individuals moving into provider-
operated living arrangements
Transition Coordination supports individuals who elect services through the EDCD waiver both before and after transitioning to the community. Time limited to 12 months from date of discharge

MFP Demonstration Services
Transition Services – Available to individuals participating in MFP up to 2 months prior to discharge
Transition Coordination – Available to individuals participating in MFP up to 2 months prior to discharge for a total 14 consecutive months in the EDCD waiver
Assistive Technology – Available to individuals participating in MFP who are in either the EDCD or HIV/AIDS waiver upon entry to the waiver
Environmental Modifications - Available to individuals participating in MFP who are in either the EDCD or HIV/AIDS waiver upon entry to the waiver
MFP Demonstration Services Supplemental Home Modifications
Supplemental Home Modifications through partnership with Department of Housing and Community Development Provides funds for “barrier” home modifications prior to
discharge for individuals participating in MFP Provides funds for home modifications that exceed $5000
post-discharge for individuals participating in MFP Administered by DHCD and five regionally-based Centers for
Independent Living• Blue Ridge Independent Living Center, Roanoke, 540-342-1231 • Endependence Center, Norfolk, 757-351-1595• Independence Empowerment Center, Manassas, 703-257-5400• Junction Center for Independent Living, Wise, 276-679-5988• Resources for Independent Living, Richmond, 804-353-6503
Outreach
Outreach is The first activity Critical to the success of a transition Varied in its forms Provided by many people
Levels of Outreach Agency Individual Regional

OutreachState Agency Led Outreach
The Department of Medical Assistance Services, the Virginia Health Care Association, the Virginia Association of Non-Profit Homes for the Aging, and Long-Term Care Ombudsman Office will
• Send information about MFP to all nursing facilities and long-stay hospitals
• Hold Informational Sessions• Incorporate educational and awareness information about the MFP
program into the annual resident review process
The Department of Medical Assistance Services, the Department of
Behavioral Health and Developmental Services, and the Virginia Association of Community Services Boards will
• Send information about MFP to all Intermediate Care Facilities for Individuals with Developmental Disabilities
Outreach Individual Led Outreach
Case Managers, Transition Coordinators, Health Care Coordinators, Human Rights Advocates, Long Term Care Ombudsman's will:• Contact facilities to:
• hold one-on-one meetings
• hold open informational sessions
Sources of Information
Information can be obtained through: DMAS DBHDS Local DSS Local Dept of Health Community Service Boards Area Agencies on Aging Centers for Independent Living On the Web
• http://www.DMAS.virginia.gov• http://www.DBHDS.virginia.gov• Virginia Easy Access www.easyaccess.virginia.gov• Olmstead http://www.olmsteadva.com/mfp
Referral Sources & Contacts
Professional Staff at Hospital Nursing Facility Intermediate Care Facility for Individuals with Developmental
Disabilities (ICF-DD) Long-stay Hospital Institute for Mental Disorders (IMD) Psychiatric Residential Treatment Facility (PRTF)
People in the community Family members Friends

Referral Sources & Contacts
Specific to Nursing Facilities MDS 3.0 Section Q Referrals
• Individuals who wish to seek additional information on community living and a list of Transition Coordination Agencies will be provided information from the local Area Agency on Aging
• Individuals will choose a Transition Coordination Agency• The Area Agency on Aging will contact the chosen
Transition Coordination Agency to arrange referral
Keys to a Successful Transition
More than someone changing residence Increasing self-direction Increasing decision-making Participating fully in community activities Developing informal and formal supports

Keys to a Successful TransitionTransition Coordinators
A DMAS-enrolled provider who is responsible for supporting the individual and family/caregiver, as appropriate, with activities associated with transitioning from an institution to the community
Transition Coordinators / Case Managers:
Work closely with individuals
Assist individuals to take a proactive role in the transition process
Recognize that a successful transition is dependent on the individuals themselves and their willingness to change
Keys to a Successful Transition Characteristics of the Transition Coordinator
Transition Coordinators / Case Managers will have multiple roles including Being an effective mentor Understanding circumstances of placement in
institutionBeing mindful of the individual’s potentialBeing knowledgeable of all community
resourcesBeing an active listener
Keys to a Successful Transition Characteristics of the Transition Coordinator
Recognizing that the individual’s emotions of fear, anger, and anxiety are real
Openly acknowledge and discuss emotions with the individual
Providing accurate information in a timely manner
Exploring all options with the individualAcknowledging and balancing risk

Keys to a Successful Transition Critical Components
Developing a trusting relationship Having a comprehensive assessment that clearly
reflects preferences and strengthsneeds concernspriorities
Developing and implementing a Transition Plan that addressesthe individual’s preferences and needscritical follow-up with post-transition activities
Keys to a Successful TransitionGuiding Principles
There are two important principles to keep in mind throughout the transition process
o self-determination
o the right to take risks
Keys to a Successful TransitionGuiding Principles
Self-Determinationo Is the right to make one’s own decisions without
interference from others
Right to Take Riskso Making choices about new experiences and
possibilitieso Individuals grow by making choices even if those
choices are viewed as poor choices o Individuals learn by both successes and failures o Taking risks is part of living for everyone
Keys to a Successful Transition Balancing Risk
Prudent risks vs. undue risks
Individuals should not be expected to face challenges that will result in failure
Planning & Risk Assessment Risk Assessment
Assessment elements for Person Centered PlanningAssessment is not a single meeting Assessment is a series of meetings
establishing• Trust • Individuals’ ability to manage risk• Determination of preferences and needs

Planning & Risk Assessment Risk Assessment (continued)
7 key componentsHealth ServicesSocial SupportsHousingTransportationVolunteering/ EmploymentAdvocacyFinancial Resources
Planning & Risk Assessment Risk Assessment (continued)
Risk assessments are integrated with the development of the support plan It determines the level of support needed for
• Health Services• Daily Living Activities• Housing• Transportation• Social Supports
It determines the plan’s ability to meet the personal goal of the individual
It determines the type of back-up plan
Planning & Risk Assessment Description of Required Tiers
Tier 1: Service Plan Backup Providers Required to have backup provider for each service
Tier 2: Informal Network Reaches out to the individual, family, friends, and
neighbors to provide interim supportsTier 3: 24-hour Response System
Call the toll-free call center, 2-1-1 Virginia Tier 4: Extreme Emergency
An immediate crisis involving a threat to the individual’s health, safety, or life, call 911
Planning & Risk Assessment Risk Assessment (continued)
Transition Coordinators are Mandated reporters for CPS & APS
Professional judgment is used to determine risk factors
Accessible and proper housing is critical to a individual’s success
Key elements to consider in helping the individual select the new home are: Location Affordability Access to transportation Personal security Opportunity for social activities Opportunity for employment
Planning & Risk Assessment Housing
Planning & Risk Assessment Housing and MFP Qualifying Criteria
Residences must meet one of the following requirements:
A home that the individual or the individual’s family member owns or leases
An apartment with an individual lease, lockable entry and exit and includes living, sleeping, bathing and cooking areas, over which either individual or the individual’s family has domain and control
A residence, in a community-based residential setting, in which no more than four unrelated individuals reside
Transition Process The key of the transition process
The ability to coordinate pre- and post- facility discharge transition planning and supports delivery
The ability to submit/ obtain waiver enrollment & prior authorization on the day of discharge from facility
3 Stages of the Transition Process
Planning Phase
Completed while in facility
Implementation Phase
Completed after transition and while individual is living in community
Discharge
Date
Stage 1 Stage 2 Stage 3

Pre-Discharge activity for Transition Coordinator/Case Manager
Educate and recruit individual Coordinate with discharge planner at facility to confirm individual
still meets nursing home level of care Ensure a copy of current UAI is available Complete MFP enrollment:
MFP Enrollment form (DMAS-222) MFP Informed Consent (DMAS-221)
Complete Prior Authorization Requests (DMAS-98) to enroll individual into MFP
Complete Prior Authorization Request (DMAS-98) for Transition Coordination prior to discharge as MFP demonstration services
Transition Coordination
Transition Process Stage 1 “Planning Phase”
Pre-Discharge activity for Transition Coordinator/ Case Manager (continued):
Complete MFP enrollment: Administer Quality of Life survey (DMAS-416) Develop Transition Plan which includes a risk assessment (DMAS-220)
Locate and secure qualified housing Schedule discharge date Complete Prior Authorization Requests (DMAS-98) for Transition
Services if needed prior to discharge as MFP demonstration services• Transition Services• Special Note: BE SURE HOUSING IS SECURED PRIOR TO
REQUESTING TRANSITION SERVICES Schedule transportation Confirm and ensure all is ready for discharge Plan for needed waiver supports upon discharge from facility
• Assistive Technology • Environmental Modifications • Transition Coordination • Personal assistance
Transition ProcessStage 1 “Planning Phase”

MFP Enrollment
Transition Coordinator/Case Manager must request MFP enrollment
MFP enrollment is available for as long as needed prior to discharge and 12 months from the date of discharge
Services available during the period of residence in an institution include Transition Coordination/Case Management Transition Services Environmental Modifications through DHCD

MFP Enrollment
The Transition Coordinator requesting the enrollment must:
Certify that the individual meets all MFP criteria
Determine with the individual if the individual can live safely in community
Complete needed forms• MFP Enrollment (DMAS-222) • Informed Consent (DMAS-221)• Administer Quality of Life Survey (DMAS-416)
Submit for MFP enrollment (DMAS-98) to KePRO
MFP Enrollment Prior Authorization Process
KePro Service Authorization Activities
•Confirms if individual meets MFP criteria
•Grants Prior Authorization / support plan approval
•Forwards letter of approval to provider & individual
•Enters individual in MMIS as participating in MFP
Insure waiver enrollment & PA’s are in place by Service Provider
Conduct home visit to ensure
Coordinate submission of DMAS-225 by both the institution and the accepting services provider to the local Department of Social Services
Service provider submits PA for services Service provider submits waiver enrollment Enroll for CD fiscal agent supports if appropriate (caution: a delay in CD services
may occur due to enrollment activities to become an employer) Monitor / coordinate delivery of goods for day of reentry Supports are in place and meeting needs Verify the back-up plan Verify delivery of Transition Services purchases Verify/schedule/completion of environmental modifications and/or assistive
technology
Transition Process Stage 2 “Day of Reentry”
A Critical Point
IMPORTANT!
Waiver enrollment MUST be coordinated with facility discharge
date

Activities Coordinate with service provider who provide needed waiver supports
Environmental Modifications Assistive Technology Personal Assistance Adult Day Health
Establish Transition Coordinator/ Case manager visit schedule for up to 12 months Be sensitive to individual’s stress Check appropriateness of supports being delivered Check individual’s view of how new life is progressing
Revise support plan as needed and before Transition Coordination ends
Transition Process Stage 3 “Implementation Phase”
Waiver Enrollment
On the day of discharge, the individual participating in MFP is enrolled into the appropriate waiver
Receive Authorization and begin delivery of identified, needed waiver supports
HIV/Aids
IFDDS
EDCD
ID
Tech
MFP Enrollment Completion of enrollment period
Individuals participating in MFP are permanently transferred to regular waiver status after MFP enrollment period ends
All waiver supports continue as long as waiver criteria is met

MFP Enrollment Disenrollment from MFP
Disenrollment from MFP due to hospitalization or institutionalization
Individual is hospitalized for more than 30 days• If re-admitted to a facility or hospital and stays
there for more than 30 days, the individual will be automatically dis-enrolled from MFP
MFP Enrollment Reenrollment Criteria
Individual does not have to meet the requirement for 90 consecutive days of institutional residency again
Reenrollment does not entitle the individual to Transition Services a second time Remaining Transition Services funding is
available for use if within the original 9-month period

MFP Enrollment Disenrollment – Returning to a facility
This will be a difficult decision to make because of the strong commitment to maintaining the individual in the community Decision should always be made with the individual Factors to use in determining
• How does the individual feel about the current situation?• Is the risk too great?• Are the basic living needs being met (food, shelter, clothing,
daily needs)?• Are supports meeting the individual’s needs?• Are the family and informal supports adequate to sustain the
individual?• Can the financial obligations be managed?

Can participation in MFP be withdrawn?
Yes Withdrawal Steps:
1. Individual will contact the Transition Coordinator2. Individual (with the Transition Coordinator) will
complete the MFP Withdrawal form 3. Transition Coordinator will make sure the form is
signed and dated by both the individual and themselves.
4. Be sure the effective date of the withdrawal is clear
5. Send the withdrawal form to KePRO agent6. Maintain copy for individual’s record and provide a
copy to the individual

MFP Enrollment Forms
All forms are on DMAS website: Search Services MFP enrollment forms:
MFP Enrollment (DMAS-222)• Provider Checklist to ensure individual meets MFP
eligibility criteria• Maintained in individual’s record
MFP Informed Consent (DMAS-221)• Ensures individuals are fully aware of their decision to
participate in MFP• Maintained in individual’s record
MFP Enrollment Forms
KePRO CBC Request for Services Form (DMAS-98) Enrolls individual into MFPMust be faxed to KePRO
• Box 12 - MFP Enrollment (PA Service Type 0909)• Box 13 – Individual Meets All MFP Eligibility
Criteria

MFP Demonstration Service Prior Authorization
KePRO CBC Request Services Form (DMAS-98) to request prior authorization for Transition Coordination (H2015) and/or Transition Services (T2038) Must be faxed to KePRO
• Box 12 - MFP Enrollment (PA Service Type 0909)• Box 15 – H2015 and/or T2038• Box 18 – 1 unit• Box 19 – H2015 = month T2038 = year• Box 22 – H2015 = up to 2 month prior and 12 months post
discharge T2038 = 9 months
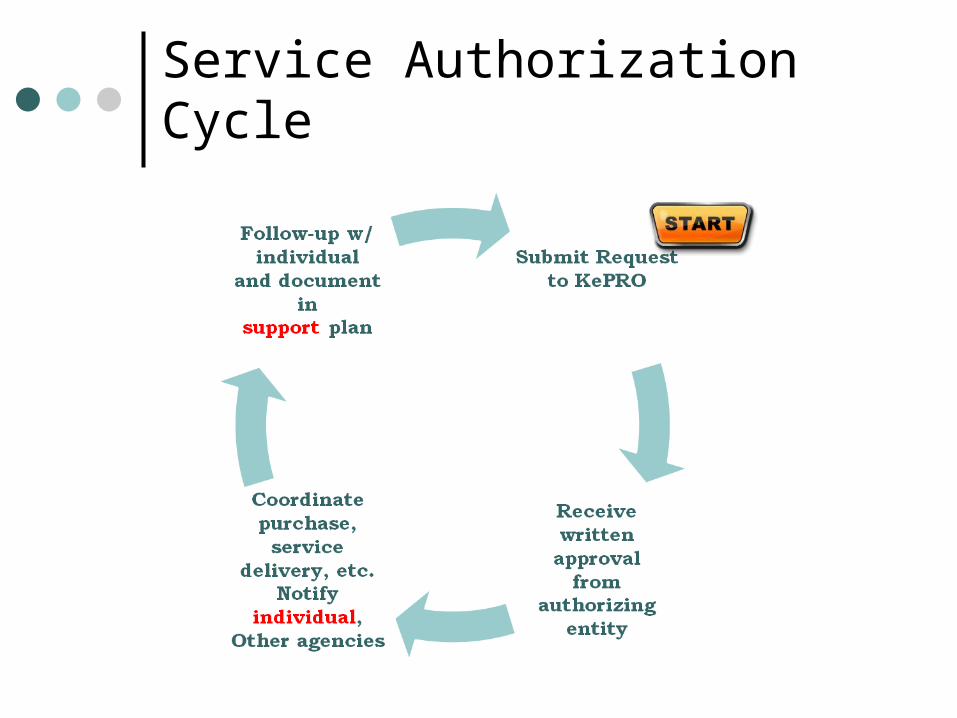
Service Authorization Cycle
MFP Enrollment Forms
Transition Coordination Services Plan for EDCD (DMAS-220) Used to develop individual’s transition plan including
assessing risk, developing back-up plan, listing of needed supports, and other aspects of community living
Maintained in individual’s record MFP Quality of Life Survey (DMAS-416)
Required of all individuals participating in MFP To be administered prior to individual’s discharge Omit questions preceded by “After Transition Only” Complete Supplemental Questions on page 18 Maintain copy in individual’s record and send original to
DMAS (see page 19 for address)
Consumer Direction “Consumer Direction” and “self direction” are terms used interchangeably.
Consumer Direction allows the individual to be the employer for their consumer-directed services.
As the employer, individuals are responsible for: advertising hiring training supervising firing their own consumer-directed services employees developing their own support plan
When supports are consumer-directed, individuals or their family or caregiver, as appropriate, decide
what support is needed who will provide it when it will be provided where it will be provided how it will be provided
Service limits for
Consumer Direction Apply
Family members & individuals who reside under the same roof cannot be employees, unless objective documentation is provided.
Pre discharge• Discuss the CD option• Provide a clear picture of the responsibilities of CD• Connect with Service Facilitator for services• Incorporate consumer direction into the support plan• Service Facilitators will confirm
• All IRS Employer forms complete (W9)• All employees are “ready to go”
Day Of Discharge• Coordinate with Service Facilitator that supports are ready to start• Support plan is understood by personal assistants
Post Discharge• Check on Service Facilitator services• Monitor supports meeting individual’s needs as defined in support plan and
adjust as needed
Transition Process Consumer Directed Option (CD)
Let the individual know that this
process can take up to 6 weeks

Transition Services Administration and Reimbursement
Transition Service reimbursement is unique to LTC home and community-based waivers
https://fms.publicpartnerships.com/VirginiaMFP
Step I – Obtain Prior Authorization (PA) from appropriate agent (PA will only be valid for 9 months from the date of authorization)
Step II – Determine with the individual the individual’s household needs essential for community living and generate estimate with Public Partnership, LLC (PPL) website
Step III – Local Agency will approve and purchase essential goods for transition to set-up the individual's household and arrange for delivery of services
Step IV – Local Agency will submit reimbursement requests via PPL website
Step V - Agency will retain documentation sufficient to explain purchase needs

Reimbursement Waiver Service Limits
The unit of service shall be specified by the DMAS fee schedule
To receive payment the services shall be explicitly detailed in the supporting documentation
Transition Coordination Service Transition coordination may not be billed solely for
monitoring purposes In-kind task or expenditure expenses within Transition are
not billable as separate items - examples include• Travel time• Written preparation • Telephone communication
Reimbursement Submission Process
Consult chapter 5 of your waiver manual for the details of submitting claims
Consumer Direction payroll will remain the same
DMAS training unit will be providing training on Transition Coordination, MFP services

Additional MFP Resources
MFP Operational Protocol Housing Waiver Supports Bridge rent Contact lists Quality of Life Survey Adult Foster Care Marketing info/ brochures Assisted Living Consumer Direction Transportation Providers Listings
ABC’s of Nursing Home Transition A publication of the IL Net
National Training & Technical Assistance Program at Independent Living Research Utilization
http://www.ilru.org – Click on “Publications” and Scroll down to “Olmstead Implementation”
On the WEB DMAS at
www.dmas.virginia.gov DBHDS at
www.dbhds.virginia.gov MFP SITE at
www.olmsteadva.com/mfp
MFP Transition Coordination Agency Monthly Conference Calls
Scheduled the last Tuesday of every month from 10:00 am to 11:00 am
Send request to be included on email distribution list to [email protected]
MFP Email DMAS will receive general
inquiries on the MFP project at [email protected]
Please enter “MFP Inquiries” in the subject line.
Contact InformationVirginia Department of Medical Assistance Services
Division of Policy and Research600 East Broad Street, Richmond, VA 23219
Jason Rachel, Ph.D.MFP Project Director
(804) [email protected]
Dana HicksMFP Analyst
(804) [email protected]
MFP website DMAS websitehttp://www.olmsteadva.com/mfp http://www.dmas.virginia.gov





























