Embed Size (px)
Citation preview
Methicillin Resistant Staphylococcus aureus (MRSA):
Proposed Revision of ICD-9 Codes
Rachel Gorwitz, MD, MPHDivision of Healthcare Quality Promotion
Centers for Disease Control and Prevention
Staphylococcus aureus Common human colonizer Common cause of skin infections Potential to cause severe / invasive
infections Transmission: Direct contact
Methicillin-Resistant Staphylococcus aureus (MRSA)
Resistant to all currently available β-lactam antibiotics (penicillins, cephalosporins)
Accounts for majority of S. aureus infections in healthcare settings– Associated with increased morbidity,
mortality, and healthcare costs as compared to methicillin-susceptible S. aureus (MSSA)
1990s: Emerged as a community pathogen– Mainly skin infections– Occasionally severe / life-threatening
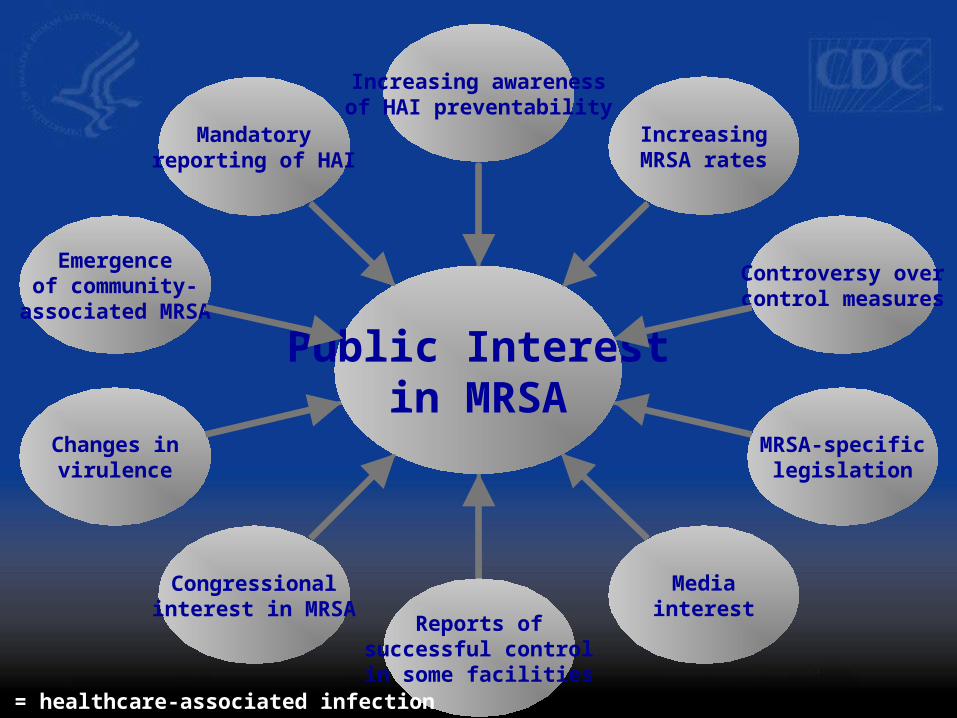
Mandatoryreporting of HAI
Emergenceof community-
associated MRSA
Changes invirulence
Congressionalinterest in MRSA
Reports ofsuccessful controlin some facilities
Mediainterest
MRSA-specificlegislation
Controversy overcontrol measures
IncreasingMRSA rates
Increasing awarenessof HAI preventability
Public Interestin MRSA
HAI = healthcare-associated infection
Sources of MRSA Surveillance Data
Active Bacterial Core Surveillance Project National Healthcare Safety Network (NHSN) National surveys using ICD-9 codes Specialized Projects
– EMERGEncy ID Net– National Health and Nutrition Examination Survey
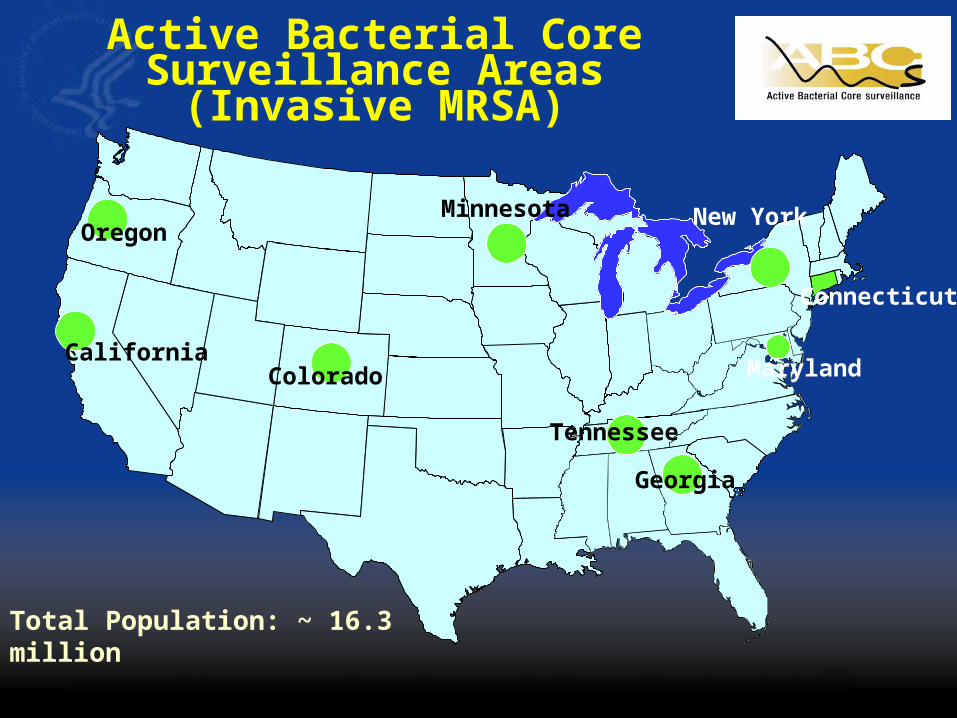
Active Bacterial Core Surveillance Areas (Invasive MRSA)
Total Population: ~ 16.3 million
Oregon
CaliforniaColorado
Tennessee
Georgia
Maryland
Connecticut
New YorkMinnesota
ABCs MRSA Case Categorization Healthcare-associated:
– Hospital-onset: Cases with positive culture obtained >48 hrs after hospital admission (may also have risk factors)
– Community-onset: Cases with at least 1 of the following risk factors:
• Invasive device at time of admission; h/o MRSA infection or colonization; h/o surgery, hospitalization, dialysis, or residence in a LTC facility in 12 mos preceding culture
Community-associated: Cases with community-onset and none of above risk factors documented
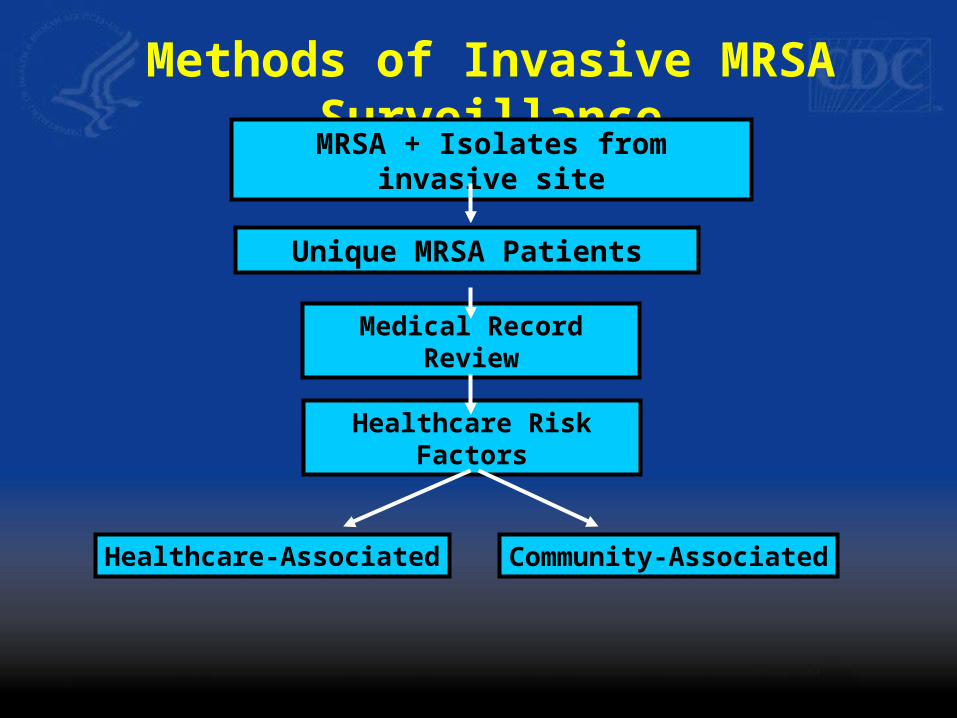
Unique MRSA Patients
Medical Record Review
Methods of Invasive MRSA Surveillance
MRSA + Isolates from invasive site
Healthcare Risk Factors
Healthcare-Associated Community-Associated
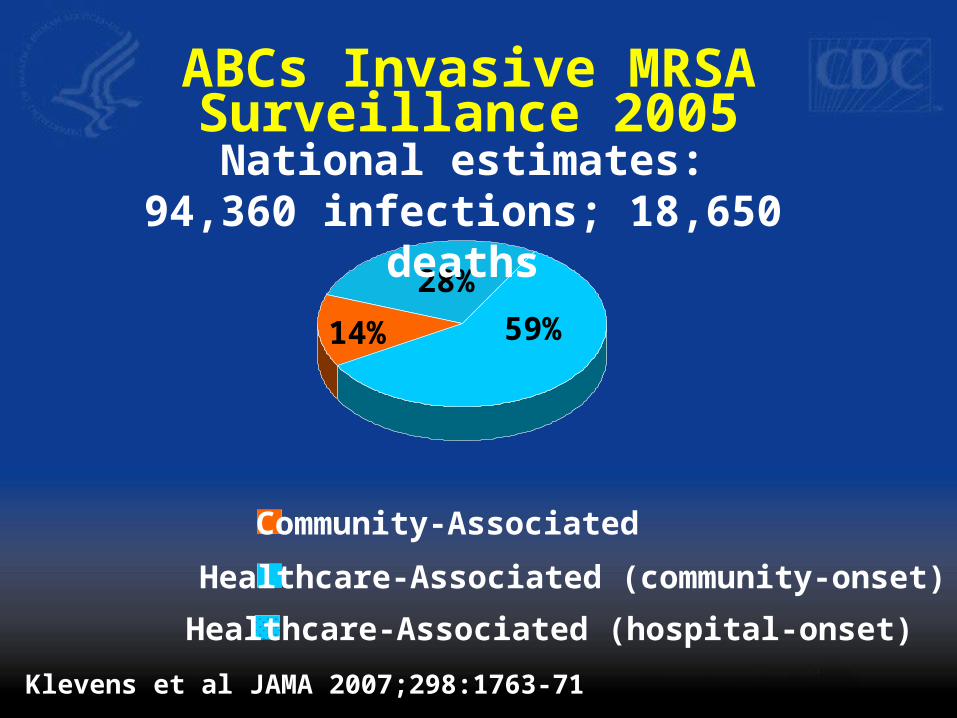
ABCs Invasive MRSA Surveillance 2005
Healthcare-Associated (community-onset)
Community-Associated
Klevens et al JAMA 2007;298:1763-71
14% 59%
28%
Healthcare-Associated (hospital-onset)
National estimates:94,360 infections; 18,650 deaths
National Healthcare Safety Network (NHSN)
Voluntary, confidential, internet-based system for monitoring healthcare-associated events and processes (including HAIs)
Purposes:– Provide national estimates of magnitude of adverse
events, trends– Provide risk-adjusted data for interfacility comparisons– Assist facilities in developing surveillance and analysis
methods Facility-associated infection:
– No evidence infection was present or incubating at time of admission (as assessed by trained infection control professional)

Use of ICD-9 Data to Monitor Burden and Trends in S. aureus Infections
Nationally representative surveys of hospitalizations and ambulatory care visits
Utilize:– Specific S. aureus infection codes (038.11
septicemia, 482.41 pneumonia)– S. aureus organism code (041.11)– Codes for syndromes typical of S. aureus (e.g.,
682 cellulitis and abscess) Methicillin resistance data from V codes
(V09.0) or external data sources
Use of ICD-9 Data to Monitor Burden and Trends in S. aureus Infections
Kuehnert et al, Emerg Infect Dis 2005– 291,542 annual hospital discharges with S.
aureus infection-related diagnoses 1999-00– 125,969 MRSA
Klein et al, Emerg Infect Dis 2007– 62% in S. aureus-related hospitalizations
1999-2005; >2-fold in MRSA-related hospitalizations
McCaig et al, Emerg Infect Dis 2006– 11.6 million annual ambulatory care visits for
skin infections typical of S. aureus 2001-03
Use of ICD-9 Data to Monitor Burden and Trends in S. aureus Infections:
Challenges With exception of septicemia and pneumonia, S.
aureus organism code not linked to clinical syndrome Resistance code (V09.0) not linked to clinical
syndrome or S. aureus organism code (041.11) National surveys contain a limited number of ICD-9
fields → organism codes and resistance codes may be deleted
Current resistance code (V09.0) not specific for S. aureus or for methicillin-resistance
Currently no colonization code specific for S. aureus or MRSA (falls under V02.59 – Other specified bacterial diseases)

Proposal: Modification of ICD-9 Codes for MRSA
Pages 17-18 of agenda

Acknowledgements Kate Ellingson Scott Fridkin Jeffery Hageman Michael Jhung John Jernigan Monina Klevens Cliff McDonald Cathy Rebmann Chesley Richards Melissa Schaefer Arjun Srinivasan
IL
NYJan-2007
MS
OR
ID
MT
NV
AZ
COJan-2008
NMOK
Jul-2008
MO
AR2008
TXLA
ND
SD
IANE
DC
KY
ME
NJ Jan-2009?
MD Jul-2008
TNJan-2008
WYMI
SCJul-2007
FL
HI
AK
MA Jul-2008
VTFeb-2007
WAJul-2008
CAJan-2008
WI
PAFeb-2008
VAJul-2008
NH
AL GA
UT
KS
MN
OH
NC
RI
DE Feb-2008
WV
IN
CT Jan-2008
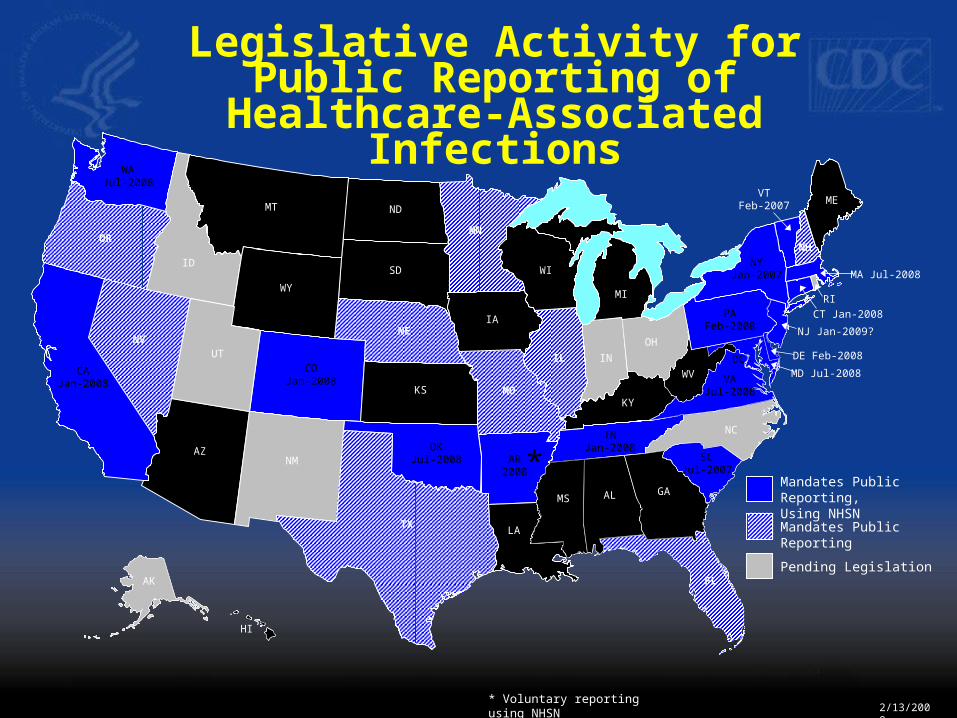
*Mandates Public Reporting,Using NHSN
Mandates Public Reporting
Pending Legislation
* Voluntary reporting using NHSN2/13/2008
Legislative Activity for Public Reporting of Healthcare-Associated
Infections