Embed Size (px)
Citation preview

O
Mi
JD
a
ARAA
KCDIMP
1
rfepCrvSimgTf
tS
1h
Digestive and Liver Disease 44 (2012) 1042– 1047
Contents lists available at SciVerse ScienceDirect
Digestive and Liver Disease
jou rn al h om epage: www.elsev ier .com/ locate /d ld
ncology
etformin use is associated with a decreased incidence of colorectal adenomasn diabetic patients with previous colorectal cancer
in Ha Lee, Soung Min Jeon, Sung Pil Hong, Jae Hee Cheon, Tae Il Kim ∗, Won Ho Kimepartment of Internal Medicine and Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Republic of Korea
r t i c l e i n f o
rticle history:eceived 22 November 2011ccepted 11 June 2012vailable online 11 July 2012
eywords:olorectal adenomaiabetes mellitus
ncidenceetformin
revious Colorectal cancer
a b s t r a c t
Background: Metformin use has been associated with decreased cancer risk and mortality. However, theeffects of metformin on the development of colorectal adenomas, the precursors of colorectal cancers,are not defined.Aims: This study aimed to evaluate the potential effect of metformin on the incidence of colorectaladenomas in diabetic patients with previous colorectal cancer.Methods: Among 488 consecutive diabetic patients who underwent colonoscopic surveillance after cura-tive resection of colorectal cancer between 1998 and 2008, 240 patients were enrolled in this study andwere compared in two groups: 114 patients taking metformin and 126 patients not taking metformin.Patient demographics, clinical characteristics, and colorectal adenoma incidence rate were analysed.Results: After a median follow-up of 58 months, a total of 33 patients (28.9%) exhibited adenomatouscolorectal polyps among the 114 patients who used metformin, compared with 58 (46.0%) patients with
colorectal adenomas among the 126 patients who did not use metformin (odds ratio = 0.48, 95% confi-dence interval = 0.280–0.816, P = 0.008). After adjustment for clinically relevant factors, metformin usewas found to be associated with a decreased incidence of colorectal adenomas (odds ratio = 0.27, 95% con-fidence interval = 0.100–0.758, P = 0.012) in diabetic patients with previous colorectal cancer. Metforminuse in diabetic patients with previous colorectal cancer is associated with a lower risk of colorectaladenoma.Gast
© 2012 Editrice. Introduction
Colorectal cancer (CRC) is the third leading cause of cancer-elated death, with a lifetime risk of 5% [1,2]. Most CRCs developrom adenomas; it takes 10–15 years for an adenomatous polyp tovolve into clinically invasive cancer [3]. Therefore, screening andrevention are important strategies to lower the burden of CRC.hemoprevention is one of the primary preventive strategies andefers to long-term use of a variety of oral agents that can delay, pre-ent, or even reverse the development of adenomas in the colon.ubstantial evidence has shown that NSAIDs and selective COX-2nhibitors can reduce the incidence of CRC and colorectal adeno-
as [4–6]; however, reports have revealed an increased risk ofastrointestinal bleeding and serious cardiovascular events [7,8].
herefore, novel drugs that are both safe and effective are neededor CRC prevention.∗ Corresponding author at: Department of Internal Medicine and Institute of Gas-roenterology, Yonsei University College of Medicine, 50, Yonsei-ro, Seodaemun-gu,eoul 120-752, Republic of Korea. Tel.: +82 2 2228 1965; fax: +82 2 393 6884.
E-mail address: [email protected] (T.I. Kim).
590-8658/$36.00 © 2012 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevierttp://dx.doi.org/10.1016/j.dld.2012.06.007
roenterologica Italiana S.r.l. Published by Elsevier Ltd. All rights reserved.
Metformin, a biguanide derivative, is an oral drug widely usedas a first-line therapy for type 2 diabetes. Metformin decreasesbasal glucose output by inhibiting hepatic gluconeogenesis andperipheral glycogenolysis. The molecular mechanism of metformininvolves liver kinase B1 (LKB1)-dependent activation of AMP-activated protein kinase (AMPK) [9]. Activated AMPK inhibits themammalian target of the rapamycin (mTOR) pathway, which playsa key role in cell growth and proliferation. Therefore, AMPK activa-tion by metformin may have a suppressive effect on tumourigenesisand cancer cell growth. Interestingly, several experimental stud-ies in animals suggest that metformin use may decrease the riskof colorectal adenomas [10,11]. They have shown that metformininduces AMPK activation and inhibits tumour development andgrowth, including colon carcinogenesis. In addition, populationstudies have shown that patients with type 2 diabetes who are tak-ing metformin have a lower risk of cancer compared with patientswho do not take metformin [12]. Recently, we found that met-formin use is associated with lower risk of mortality in CRC patientswith diabetes [13].
Although there has been substantial evidence from in vivo andin vitro studies supporting the potential efficacy of metformin as achemopreventive agent, there have been no clinical studies inves-tigating the effect of metformin on the prevention of colorectal
Ltd. All rights reserved.

iver D
awaa
2
2
clUmpomsc6tsspaami
afsroAimdsabc
U
2
rocwetaTtcf
ohwPw
J.H. Lee et al. / Digestive and L
denomas. We undertook a retrospective cohort study of patientsith a history of CRC, a high-risk group for adenomas, to evalu-
te the effect of metformin on the occurrence of new colorectaldenomas in diabetic patients.
. Methods
.1. Patients
Between January 1998 and December 2008 we identified 488onsecutive diabetic patients who underwent colonoscopic surveil-ance after curative resection of CRC at Severance Hospital, Yonseiniversity College of Medicine in Seoul, Korea. We obtained theedication data from the chart review based on self-report and
harmacy records. Among them, 248 patients were excluded basedn the following exclusion criteria: incomplete records (includingedication records); stage 4 patients, history of familial polyposis
yndrome; known inflammatory bowel disease; other invasive can-er; incomplete colonoscopy before colorectal resection or within
months after operation; and localized tumour recurrences athe anastomotic site. Finally, 240 patients were enrolled in thistudy and were divided into two groups: 114 patients with con-istent metformin use before and after CRC diagnosis and 126atients not taking metformin. Patient demographics, clinical char-cteristics, surveillance colonoscopic findings, and the colorectaldenoma incidence rate were analysed. The use of other diabeticedications (sulfonylureas, thiazolidinediones, alpha-glucosidase
nhibitors, insulin, and so on) and aspirin was also investigated.Patient demographics and clinical characteristics including age
t diagnosis, gender, follow-up duration, duration of diabetes,amily history of colorectal malignancy, body mass index (BMI),moking history, and drinking history were obtained from medicalecords. Laboratory findings included pretreatment carcinoembry-nic antigen (CEA) levels, plasma glucose levels, and haemoglobin1c levels, as well as information pertaining to the CRC diagnosis,
ncluding stage, location, histology, differentiation, and treatmentodality. The date of diagnosis of CRC was the day of pathologic
iagnosis. All patients were assessed by the 6th version of the AJCCtaging system derived from a synthesis of clinical, pathological,nd imaging information. Treatment modality was decided upony extension and location of the tumour. All patients underwenturative intent surgical resection for stage I, II, or III CRCs.
The institutional review board of Severance Hospital, Yonseiniversity in Seoul, Korea approved this study.
.2. Colonoscopic surveillance
All patients received a baseline colonoscopy before colorectalesection or within 6 months after colorectal resection. In casesf obstructing CRCs, additional colonoscopic examinations werearried out within 6 months after operation and these findingsere included as part of the baseline colonoscopic findings. We
xcised all adenomas detected during preoperative and postopera-ive colonoscopies. Follow-up colonoscopy was done at least oncend up to three times after operation during the follow-up period.he surveillance interval varied among patients from 6 monthso 12 years. Given this diversity in the number of surveillanceolonoscopies and surveillance intervals, we considered the totalollow-up period and the timing of the first follow-up colonoscopy.
An advanced adenoma was defined as a tubular adenoma 10 mmr greater in diameter, an adenoma with villous or tubulovillous
istology, or with high-grade dysplasia or carcinoma [14]. Patientsere classified according to their most advanced histologic lesions.atients with hyperplastic polyps and other benign mucosal lesionsere not considered to have adenomas.
isease 44 (2012) 1042– 1047 1043
2.3. Statistical analysis
The primary endpoint of the current study was colorectal ade-noma incidence rate. Secondary analyses compared the two groupswith respect to the proportion of patients with advanced adenomas.The baseline demographics and characteristics of the patients wereanalysed with descriptive statistics. Continuous data were analysedusing Student’s t-test and categorical data were compared usingPearson’s �2 test. Univariate logistic regression analysis was usedfor univariate analysis of the colorectal adenoma incidence rate. Amultivariate logistic regression model was used to evaluate the col-orectal adenoma incidence rate to adjust for various confounders.A Kaplan–Meier model was used to evaluate the cumulative prob-ability of colorectal adenoma development; the survival curves ofeach group were compared by a log-rank test. A value of P < 0.05was considered significant. All statistical analyses were performedusing SPSS version 13.0 (SPSS, Inc., Chicago, IL, USA).
3. Results
3.1. Patient demographics and clinical characteristics
Patient demographics and clinical characteristics are sum-marised in Table 1. The median patient age was 62 years (range,33–82 years). Baseline characteristics including age at diagnosis,sex, follow-up duration, family history of CRC, BMI, smoking his-tory, history of alcohol consumption, number of baseline colorectaladenoma, tumour stage, tumour location (colon or rectum), aspirinuse, and pretreatment CEA level were not significantly differ-ent between the metformin group and the non-metformin group.Severity of diabetes as judged by haemoglobin A1c levels, pre-mealglucose levels, and duration of diabetes were not different betweenthe two groups. We also evaluated the use of other diabetic medi-cations because there is evidence that these medications, includinginsulin and thiazolidinediones, may affect the development of col-orectal adenomas [15,16]. Insulin and thiazolidinedione use werenot significantly different between the two groups. In addition, acomparison of the treatment modality for CRC and the operationmethod in the two groups showed no significant difference.
3.2. Colonoscopic surveillance
In our study group, 177 patients (73.8%), 54 patients (22.5%), and9 patients (3.8%) underwent follow-up colonoscopy once, twice,and three times, respectively. The number of follow-up colono-scopies was not significantly different between the metformingroup and the non-metformin group (P = 0.069). The interval to thefirst follow-up colonoscopy was not significantly different betweenthe two groups (24.4 months vs. 24.5 months, P = 0.979) (Table 2).
3.3. Findings of follow-up colonoscopy
The number of polyps and colorectal adenoma positive ratewere examined in each follow-up colonoscopy, and in the 1stfollow-up colonoscopy, colorectal adenoma positive rate of thenon-metformin group was higher than that of the metformin group(43.7% vs. 28.1%, P = 0.015) (Table 3). Although there was no sta-tistical significance, the non-metformin group still showed highercolorectal adenoma positive rates in the 2nd and 3rd follow-upcolonoscopies.
3.4. Metformin use and colorectal adenoma incidence rate
The median follow-up duration was 48 months (range, 19–170).In the entire cohort, 91 (37.9%) patients exhibited colorectal ade-noma development and 2 (0.8%) patients showed metachronous

1044 J.H. Lee et al. / Digestive and Liver Disease 44 (2012) 1042– 1047
Table 1Patient demographics and clinical characteristics.
Metformin group (n = 114) Non-metformin group (n = 126) P-value
Age at diagnosis, mean±S.D., years 61.5 ± 8.0 62.3 ± 7.9 0.439<50 5 (4.4%) 8 (6.3%)≥50 109 (95.6%) 118 (93.7%)
Sex 0.886Male 81 (71.1%) 91 (72.2%)Female 33 (28.9%) 35 (27.8%)
Follow-up duration, median (range), months 45.5 (19–170) 54(22–127) 0.084DM duration, median (range), years 8(1–120) 8(1–30) 0.290Family history of CRC 7 (6.1%) 6 (4.8%) 0.777BMI, mean ± S.D., kg/m2 23.7 ± 3.7 24.1 ± 2.9 0.420
Normal (≤25) 73 (64.0%) 80 (63.5%)Overweight (25–30) 37 (32.5%) 42 (33.3%)Obesity (≥30) 4 (3.5%) 4 (3.2%)
Smoking 0.971Never-smoker 55 (48.2%) 63 (50.0%)Ex-smoker 27 (23.7%) 28 (22.2%)Current smoker 32 (28.1%) 35 (27.8%)
Alcohol 0.888None 47 (41.2%) 56 (44.4%)<1 drink/day 23 (23.1%) 25 (19.8%)≥1 drink/day 44 (38.6%) 45 (35.7%)
Aspirin use 25 (21.9%) 18 (14.3%) 0.133Insulin use 9 (7.9%) 18 (14.3%) 0.152Thiazolidinedione use 12 (10.5%) 7 (5.6%) 0.231CEA, median (range), ng/mL 2.5 (0.1–97.3) 3.1 (0.1–99) 0.237HbA1c, mean ± S.D., % 7.3 ± 1.4 7.2 ± 1.3 0.713Glucose, AC, mean ± S.D., mg/dL 133.0 ± 42.5 137.3 ± 34.0 0.393Cholesterol, total, mean ± S.D., mg/dL 169.4 ± 41.9 161.1 ± 36.9 0.125Tumour stage 0.568
I 19 (16.7%) 24 (19.0%)II 39 (34.2%) 49 (38.9%)III 56 (49.1%) 53 (42.1%)
Tumour site 0.146Colon 63 (54.2%) 82 (62.4%)Rectum 51 (45.8%) 44 (37.6%)
Number of baseline colorectal adenoma 141 154 0.843Treatment modality 0.942
Resection only 25 (21.2%) 29 (21.8%)Resection + adjuvant chemotherapy 67 (60.2%) 73 (58.6%)Resection + chemoradiotherapy 12 (10.2%) 11 (9.0%)Neoadjuvant chemotherapy + resection 10 (8.5%) 13 (10.5%)
Operation methods 0.252Right hemicolectomy 26 (22.8%) 30 (26.3%)Anterior resection (AR)/lower AR 82 (71.9%) 82 (65.1%)Left hemicolectomy 5 (4.4%) 6 (4.8%)Local resection 1 (0.9%) 6 (4.8%)
S
cpuaTdct(
TCm
P = 0.008).After adjustment for age at diagnosis, sex, stage of cancer, BMI,
family history of CRC, follow-up duration, number of total colono-
Subtotal colectomy 0
.D., standard deviation; DM, diabetes mellitus; Hb, haemoglobin; AC, ante cibum.
ancer development. With respect to metformin use, 8 (7.0%)atients had advanced adenomas among the 114 patients whosed metformin, and 13 patients (10.3%) demonstrated advanceddenomas among the 126 patients who did not use metformin.he advanced adenoma development rate was not significantlyifferent between the two groups (P = 0.371). However, the total
olorectal adenoma development rate was significantly lower inhe metformin group compared with the non-metformin groupTable 4). Thirty-three (28.9%) patients had colorectal adenomasable 2omparison of total number and interval of follow-up colonoscopies between theetformin and non-metformin groups.
Metformin group (n = 114) Non-metformin group(n = 126)
P-value
Number of follow-up colonoscopies 0.0691 92 (80.7%) 85 (67.5%)2 19 (16.7%) 35 (27.8%)3 3 (2.6%) 6 (5.0%)
Interval to first follow-up colonoscopy, mean ± S.D., months 0.97924.4 ± 19.7 24.5 ± 18.2
2 (1.6%)
among the 114 patients who used metformin, meanwhile, 58(46.0%) patients had colorectal adenomas among the 126 patientswho did not use metformin (OR = 0.48, 95% CI = 0.280–0.816;
scopies, interval to first follow-up colonoscopy, number of baseline
Table 3Comparison of the findings of follow up colonoscopy between the metformin andnon-metformin groups.
F/U colonoscopy Metformin group Non-metformin group P-value
1stNumber of polyps 58 93Positive patients 32/114 (28.1%) 55/126 (43.7%) 0.015
2ndNumber of polyps 9 10Positive patients 4/22 (18.2%) 10/41 (24.4%) 0.753
3rdNumber of polyps 0 3Positive patients 0/3 1/6 (16.7%) 1.000
F/U, follow-up.

J.H. Lee et al. / Digestive and Liver Disease 44 (2012) 1042– 1047 1045
Table 4Comparison of adenoma incidence rate between the metformin and non-metformin groups.
Metformin group (n = 114) Non-metformin group (n = 126) OR 95%CI P-value
Total adenoma 33 (28.9%) 58 (46.0%)
Advanced adenoma 8 (7.0%) 13 (10.3%)
Metachronous cancer 0 2 (1.6%)
Table 5Multivariate analysis of total adenoma incidence rate.
OR 95% CI P-value
Metformin use (yes vs. no) 0.27 0.100–0.758 0.012Age at diagnosis (<50 vs.
≥50)0.15 0.013–1.662 0.121
Sex (male vs. female) 1.06 0.600–7.690 0.920BMI (normal vs.
overweight/obese)0.13 0.010–1.701 0.121
Family history (yes vs. no) 1.7 0.204–14.165 0.623Aspirin use (yes vs. no) 0.85 0.272–2.678 0.786Thiazolidinedione use (yes
vs. no)0.6 0.083–4.347 0.612
Insulin use (yes vs. no) 1.97 0.491–8.230 0.353Tumour stage (I vs. II/III/IV) 0.28 0.022–3.546 0.111Treatment modality
(surgery only vs.combined treatment)
0.87 0.065–10.206 0.415
Follow-up duration 1.0 0.980–1.025 0.834Number of baseline
colorectal adenoma0.73 0.506–1.048 0.088
Interval to first follow-upcolonoscopy
1.04 1.003–1.084 0.034
ciw9Cuiiit(
Ff
Number of total follow-upcolonoscopies (1 vs. 2/3)
0.81 0.021–1.571 0.355
olorectal adenoma, treatment modality, use of aspirin, use ofnsulin, and use of thiazolidinediones, metformin was associated
ith a lower incidence rate for colorectal adenomas (OR = 0.27,5% CI = 0.100–0.758; P = 0.012) in diabetic patients with previousRC (Table 5). Metformin use and interval to the first follow-p colonoscopy (OR = 1.04, 95%CI = 1.003–1.084; P = 0.034) were
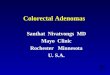
ndependent predictive factors for colorectal adenoma incidencen diabetic patients with previous CRC. The cumulative probabil-ty of colorectal adenoma development was significantly lower in
he metformin group compared with the non-metformin groupP = 0.041, Fig. 1).ig. 1. Cumulative development rate of colorectal adenomas according to met-ormin use.
0.48 0.280–0.816 0.0080.6 0.243–1.497 0.371
0.499
In addition, we performed sub-analysis by the length of follow-up and baseline number of polyp. When subgrouping by lengthof follow-up, metformin use was still associated with decreasedcolorectal adenoma development in both groups (follow-up dura-tion < 50 months; OR = 0.27, 95%CI 0.100–0.727, P = 0.046 andfollow-up duration ≥ 50 months; OR = 0.38, 95%CI 0.145–0.981,P = 0.010). When subgrouping by baseline number of polyp, thepatients receiving metformin had a lower colorectal adenoma inci-dence rate in only patients with more than 2 adenomas at baselinestudy (OR = 0.05, 95%CI 0.010–0.285, P = 0.001).
We also performed a subgroup analysis based on the operationmethod because the location of remaining colon differs accordingto the operative method and could therefore affect the occurrenceof colorectal adenomas. While the colorectal adenoma incidencerate was not significantly different according to metformin usein patients who underwent right hemicolectomy, patients whounderwent anterior resection or lower anterior resection exhib-ited a significantly lower colorectal adenoma incidence rate in themetformin group (24/82, 29.3%) compared to the non-metformingroup (40/82, 48.8%) (OR = 0.43, 95%CI = 0.228–0.826; P = 0.011).
4. Discussion
In the present study we found that diabetic patients with pre-vious CRC who took metformin had a lower rate of colorectaladenoma development compared to those who did not take met-formin. In addition, metformin use was associated with a lowercumulative colorectal adenoma incidence rate after adjustment forage at diagnosis, sex, stage of cancer, BMI, family history of CRC,follow-up duration, total number of colonoscopies, interval to firstfollow-up colonoscopy, number of baseline colorectal adenoma,treatment modality, use of aspirin, use of insulin, and use of thi-azolidinediones in diabetic patients with previous CRC.
Previous studies have suggested that metformin decreases theincidence of cancer in diabetic patients [12,17]. In addition, animalstudies have shown that metformin use may decrease the risk ofcolorectal adenomas, the precursor of CRC [10,11]. However, therehave been no clinical studies investigating the effect of metforminon the prevention of colorectal adenomas. Thus, our study is thefirst to show the chemopreventive effect of metformin in diabeticpatients with previous CRC. In general, it is very difficult to demon-strate the chemopreventive effect of some materials because manyyears of study are required and low compliance may affect studyresults. To overcome these problems, we chose patients with ahistory of CRC who might constitute a group at higher risk foradenomas.
Metformin has been widely used for a long time in the treatmentof type 2 DM and is generally considered to be a safe and economicdrug. There are several possible mechanisms for the antitumoureffects of metformin, including an antiproliferative effect via reduc-ing insulin-like growth factor [18]; inhibition of the mTOR pathway[19]; blockage of HER-2 signalling [20]; inhibition of angiogen-esis [21]; apoptosis [22]; and induction of cell cycle arrest [23].Among these, the majority of metformin’s antitumour effects may
be through the inhibition of the mTOR signalling [24]. Specifically,mTOR phosphorylates down-stream mediators regulating cell cycleprogression, cell growth, and angiogenesis. As the mTOR pathwayis frequently deregulated in a variety of tumours, and activation of
1 iver D
mpao
tcaTindaPteotdmsewgbt
fecAmhtcrnacrwgo
tipmhngdseeodfm
owpHti
046 J.H. Lee et al. / Digestive and L
TOR-dependent protein translation is associated with an adverserognosis and resistance to both chemotherapy and targeted ther-py, inhibition of mTOR signalling is regarded as a promising targetf cancer therapy [25].
In previous studies, other diabetic drugs such as insulin andhiazolidinediones have been shown to affect the development ofolorectal adenomas [26,27]. Therefore, we performed analysis fordenoma detection rate according to insulin and thiazolidinedione.he adenoma detection rate was 10/27 (37%) in patients receiv-ng insulin and 81/213(38%) in not receiving insulin. There waso difference between the two groups (P = 1.000). The adenomaetection rate was neither different between the group taking thi-zolidinedione and those not (10/19 (52.6%) vs. 81/221 (36.7%),
= 0.218). However, the number of patients receiving insulin orhiazolidinedione was too small for meaningful evaluation of theirffect in our study. In addition, we adjusted for these variables inur analysis, and use of metformin remained an independent fac-or of lower risk for colorectal adenomas. We also examined theuration of diabetes, glycosylated haemoglobin levels, and pre-eal glucose levels at the time of CRC diagnosis, which represent
everity and patient control of diabetes, in order to exclude theffects of improved diabetic control. In our study, these variablesere not different between the metformin and non-metformin
roups; therefore, the chemopreventive effect of metformin maye due to metformin itself rather than improved diabetes con-rol.
To confirm that the follow-up colonoscopies for the met-ormin group and the non-metformin group were conducted underqual conditions, we analysed the total number of follow-upolonoscopies and the interval to the first follow-up colonoscopy.lthough there was no statistical significance, the number of 2 orore follow-up colonoscopies in the non-metformin group was
igher than the metformin group. For clarify the cause, we analysedhe findings of each follow-up colonoscopy. In the first follow-upolonoscopy, the non-metformin group showed a higher positiveate of adenoma than the metformin group. Although there waso statistical significance, the non-metformin group still showed
higher positive rate of adenoma in the 2nd and 3rd follow-upolonoscopies. These results suggest that since adenoma positiveate in the first follow-up colonoscopy of the non-metformin groupas higher than that of the metformin group, the non-metformin
roup required more follow-up colonoscopies in the same periodf time.
Interestingly, we found that the effect of metformin onhe prevention of colorectal adenomas was different accord-ng to the adenoma location. Specifically, when we divided theatients according to surgical method, the positive effect ofetformin was not observed in patients who underwent right
emicolectomy, namely, patients with intact left colons. Colorectaleoplasms exhibit different clinical characteristics and tumouri-enic pathways according to the location of the tumour, includingifferent molecular pathways, microsatellite stability, and progno-is [28–30]. However, we could not determine if these differentffects are due to different tumourigenic pathways or differentffect of metformin according to colonic locations. Furthermore,ur sample size was too small to generalize these results. A moreetailed examination of the molecular pathways targeted by met-ormin and their association with known tumourigenic pathway
odels is necessary.Although aspirin use is known to decrease the incidence of col-
rectal adenomas in patients with previous CRC [5], aspirin useas not an independent predictive factor for colorectal adenoma
revention in diabetic patients with previous CRC in our study.owever, the number of aspirin users in our study may have beenoo small to demonstrate the effect of aspirin on colorectal polypncidence.
[
[
isease 44 (2012) 1042– 1047
There are several limitations to this study. First, we had inher-ent limitations associated with the retrospective study design andthe inclusion of non-randomly distributed patients. In addition,the frequency and interval of follow-up colonoscopies were dif-ferent among the study patients. We adjusted for these problemsby including total follow-up period, timing of the first follow-upcolonoscopy, and total number of follow-up colonoscopies in mul-tivariate analysis, and these factors were not different betweenthe metformin and the non-metformin groups. Second, in ourstudy, consistent metformin use before and after CRC diagno-sis was included. Therefore, it is unclear if the observed benefitwas from prediagnosis and/or postdiagnosis metformin use. Third,we had a limited sample size, especially in the subgroup analy-sis based on operative method, and there was a potential risk fortype II errors (false positive results). Fourth, our study sample con-sisted of diabetic patients; therefore, it is difficult to generalize thechemopreventive effect of metformin to non-diabetic patients. Toovercome these limitations, further large-scale, prospective, obser-vational studies and interventional trials are required. Finally, wecould not completely exclude the possibility that metformin usemay be related to other prognostic factors, including other medi-cations such as insulin and metabolic status. However, our findingsremained unchanged after adjusting for these potential factors andthere were no significant differences between the metformin andnon-metformin groups with respect to BMI, plasma total choles-terol, pre-meal glucose, duration of diabetes, or haemoglobin A1clevels, which serve as proxies for metabolic status and diabetesseverity.
In conclusion, diabetic patients with previous CRC receiv-ing metformin had a lower colorectal adenoma incidence ratecompared to those not receiving metformin. To the best of ourknowledge, this is the first study to demonstrate a protective effectof metformin against colorectal adenomas in diabetic patients withprevious CRC. While the exact mechanisms underlying this effectneed further elucidation, metformin may have the potential to beused as a chemopreventive agent for CRC. Further studies are war-ranted to evaluate the potential of metformin as a chemopreventiveagent.
Conflict of interestThe authors declare that there is no conflict of interest.
References
[1] Andrieu N, Launoy G, Guillois R, et al. Familial relative risk of colorec-tal cancer: a population-based study. European Journal of Cancer 2003;39:1904–11.
[2] Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA: A Cancer Journal forClinicians 2010;60:277–300.
[3] Morson B. President’s address. The polyp-cancer sequence in the large bowel.Proceedings of the Royal Society of Medicine 1974;67:451–7.
[4] Tuynman JB, Peppelenbosch MP, Richel DJ. COX-2 inhibition as a tool totreat and prevent colorectal cancer. Critical Reviews in Oncology/Hematology2004;52:81–101.
[5] Baron JA, Cole BF, Sandler RS, et al. A randomized trial of aspirin to preventcolorectal adenomas. New England Journal of Medicine 2003;348:891–9.
[6] Thun MJ, Henley SJ, Patrono C. Nonsteroidal anti-inflammatory drugs as anti-cancer agents: mechanistic, pharmacologic, and clinical issues. Journal of theNational Cancer Institute 2002;94:252–66.
[7] Ballinger A, Smith G. COX-2 inhibitors vs. NSAIDs in gastrointestinal damageand prevention. Expert Opinion on Pharmacotherapy 2001;2:31–40.
[8] Solomon SD, McMurray JJ, Pfeffer MA, et al. Cardiovascular risk associated withcelecoxib in a clinical trial for colorectal adenoma prevention. New EnglandJournal of Medicine 2005;352:1071–80.
[9] Shaw RJ, Lamia KA, Vasquez D, et al. The kinase LKB1 mediates glucosehomeostasis in liver and therapeutic effects of metformin. Science 2005;310:1642–6.
10] Hosono K, Endo H, Takahashi H, et al. Metformin suppresses azoxymethane-induced colorectal aberrant crypt foci by activating AMP-activated proteinkinase. Molecular Carcinogenesis 2010;49:662–71.
11] Tomimoto A, Endo H, Sugiyama M, et al. Metformin suppresses intestinal polypgrowth in ApcMin/+ mice. Cancer Science 2008;99:2136–41.

iver D
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
J.H. Lee et al. / Digestive and L
12] Evans JM, Donnelly LA, Emslie-Smith AM, et al. Metformin and reduced risk ofcancer in diabetic patients. British Medical Journal 2005;330:1304–5.
13] Lee JH, Kim TI, Jeon SM, et al. The effects of metformin on the survival of col-orectal cancer patients with diabetes mellitus. International Journal of Cancer2011;131:752–9.
14] Winawer SJ, Zauber AG, O’Brien MJ, et al. Randomized comparison of surveil-lance intervals after colonoscopic removal of newly diagnosed adenomatouspolyps. The National Polyp Study Workgroup. New England Journal of Medicine1993;328:901–6.
15] Chung YW, Han DS, Park KH, et al. Insulin therapy and colorectal adenoma riskamong patients with Type 2 diabetes mellitus: a case–control study in Korea.Diseases of the Colon and Rectum 2008;51:593–7.
16] Saez E, Tontonoz P, Nelson MC, et al. Activators of the nuclear recep-tor PPARgamma enhance colon polyp formation. Nature Medicine1998;4:1058–61.
17] Bodmer M, Meier C, Krahenbuhl S, et al. Long-term metformin use is associatedwith decreased risk of breast cancer. Diabetes Care 2010;33:1304–8.
18] Pollak M. Insulin and insulin-like growth factor signalling in neoplasia. NatureReviews Cancer 2008;8:915–28.
19] Zakikhani M, Dowling R, Fantus IG, et al. Metformin is an AMP kinase-dependent growth inhibitor for breast cancer cells. Cancer Research
2006;66:10269–73.20] Vazquez-Martin A, Oliveras-Ferraros C, Menendez JA. The antidiabetic drugmetformin suppresses HER2 (erbB-2) oncoprotein overexpression via inhibi-tion of the mTOR effector p70S6K1 in human breast carcinoma cells. Cell Cycle2009;8:88–96.
[
[
isease 44 (2012) 1042– 1047 1047
21] Ersoy C, Kiyici S, Budak F, et al. The effect of metformin treatment on VEGF andPAI-1 levels in obese type 2 diabetic patients. Diabetes Research and ClinicalPractice 2008;81:56–60.
22] Ben Sahra I, Laurent K, Giuliano S, et al. Targeting cancer cell metabolism:the combination of metformin and 2-deoxyglucose induces p53-dependentapoptosis in prostate cancer cells. Cancer Research 2010;70:2465–75.
23] Ben Sahra I, Laurent K, Loubat A, et al. The antidiabetic drug metformin exertsan antitumoral effect in vitro and in vivo through a decrease of cyclin D1 level.Oncogene 2008;27:3576–86.
24] Jalving M, Gietema JA, Lefrandt JD, et al. Metformin: taking away the candy forcancer? European Journal of Cancer 2010;46:2369–80.
25] Morgensztern D, McLeod HL. PI3K/Akt/mTOR pathway as a target for cancertherapy. Anti-Cancer Drugs 2005;16:797–803.
26] Campbell PT, Deka A, Jacobs EJ, et al. Prospective study reveals associationsbetween colorectal cancer and type 2 diabetes mellitus or insulin use in men.Gastroenterology 2010;139:1138–46.
27] Okumura T. Mechanisms by which thiazolidinediones induce anti-cancer effects in cancers in digestive organs. Journal of Gastroenterology2010;45:1097–102.
28] Yamaji Y, Mitsushima T, Ikuma H, et al. Right-side shift of colorectal adenomaswith aging. Gastrointestinal Endoscopy 2006;63:453–8, quiz 64.
29] Elsaleh H, Joseph D, Grieu F, et al. Association of tumour site and sex withsurvival benefit from adjuvant chemotherapy in colorectal cancer. Lancet2000;355:1745–50.
30] Patel K, Hoffman NE. The anatomical distribution of colorectal polyps atcolonoscopy. Journal of Clinical Gastroenterology 2001;33:222–5.