Embed Size (px)
Citation preview

METASTATIC THYMOMA PRESENTING AS A SOLITARY PULMONARY NODULE
VICTOR J. ROSEN, MD, THORWALD 1%'. CHRISTIANSEN, AID,*
AND RICHARD K. HUGHES, M D ~
A 74-year-old man underwent an exploratory thoracotomy for what was thought to be a solitary peripheral pulmonary nodule. Microscopic exam- ination revealed a tumor consistent with a thymoma and mediastinal explora- tion revealed thymoma. Additional nodules were noted within the substance of the lung. The patient died of a coronary occlusion one month following sur- gery. Autopsy revealed metastatic thymoma in the liver and spleen. The medias- tinal mass showed extensive venous invasion. The case represents a very unusual clinical manifestation of a thymic neoplasm.
ORKABLE CLASSIFICATIONS OF THYhIOMA
have been described in recent years by Castleman, Iverson and Lattes for most neo- plasms of the thymus which readily are rec- ognized microscopically.2, 4 ~ 6 , 7 Clinical man- agement usually involves local treatment although systemic treatment sometimes is re- quired as hematologic and bizarre manifesta- tions and myasthenia gravis3. 5 , 8 often are ascribed to these tumors. Its unusual occur- rence in association with other neoplasms also has been reported. True metastatic spread is very infrequent but local mediastinal and pleural invasion may suggest clinical malig- nancy. Castleman reported a case of thymoma that appeared as an intrapulmonary nodule 5 years after surgery and radiation to the mediastinum for a lung carcinoma.1 Splenic and renal metastases from the thymoma were found at necropsy. The case to be described concerns a patient with a solitary, slowly growing, peripheral intrapulmonary nodule which was determined to be a metastatic thy- moma. A separate anterior mediastinal thy- moma was discovered at thoracotomy.
From the Departments of Pathology and Thoracic Surgery, Wadsworth Hospital, Veterans Administration Center, Los Angeles, 90073 and the University of Cali- fornia, Los Angeles, Center for the Health Sciences, Departments of Surgery and Pathology.
Address for reprints: Victor J. Rosen, MD, Chief, Anatomic Pathology Section, Wadsworth Hospital, Wil- shire and Sawtelle Boulevards, Los Angeles, Calif. 90073.
* Chief Thoracic Surgical Resident, Wadsworth Hos- pital, and Clinical Associate in Surgery, University of California, Los Angeles, Calif.
t Chief of Thoracic Surgery, Wadsworth Hospital, and Assistant Professor-in-Residence (Surgery), Univer- sity of California, Los Angeles, Calif.
CASE REPORT
A 74-year-old veteran entered Wadsworth Hospital because of recurrent hoarseness for 2 years, dull substernal pain for one year and dysphagia for one month associated with a loss of 20 pounds of weight. An x-ray film of the chest revealed a 2 cm nodular density in the base of the left lung. Past medical his- tory was unremarkable except for a rectal polypectomy 8 years earlier. Infectious syphilis had been treated with Salvarsan in 1919.
Physical examination showed an obese eld- erly man in no distress. Blood pressure was 122 mm Hg systolic, 60 mm Hg diastolic. The lungs were clear to auscultation. A grade I1 systolic murmur was present over the precord- ium, loudest at the apex. Some reduction in mobility of the right vocal cord was seen at laryngoscopy. Results of neurological examina- tion were normal.
Laboratory studies were performed. An electrocardiographic tracing was normal. Four sputum specimens contained atypical cells which did not appear to be malignant. Alka- line phosphatase, serum transaminase, total proteins and cephalin flocculation were nor- mal; white blood count was normal. Hemato- crit was 44.5%. A serologic test for syphilis was nonreactive. Coccidioidin, histoplasmin and tuberculin tests were negative. When esopha- goscopy showed a small lesion just proximal to the cricopharyngeus, a biopsy was performed which revealed chronic inflammation. Two gastric cytologies were interpreted as showing atypical cells not suggestive of malignant change. The patient was discharged from the
527

528 CANCER April 1966
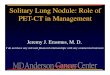
FIG. 1. Resected pulmonary nodule showing sheets of spindly epithelioid cells admixed with nests of lymphocytes. One small nodule of tumor partially fills the lumen of a bronchiole ( ~ 8 7 ) .
FIG. 2. Detail of Figure 1 showing the lobulated epithelial aggregates with pale cytoplasm and oval nuclei generously admixed with lymphoid elements (~200).

h v . 4 hlETA5TATIC THYMOMA AS SOLlTARY PULMONARY S 0 U L L . E - 1<OSC'll el Ul.
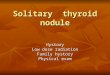
FIG. 3. Biopsy of mediastinal mass obtained a t time of pulmonary resection. Note the char- acteristic dense fibrous trabecula separating generously admixed patterns of thymoma ( ~ 8 7 ) .
hospital and antacids were prescribed. Cytol- ogy of a gastric lavage 4 weeks later was read as "positive for malignant cells."
The patient was readmitted to the hospital 5 weeks later. Results of the physical examina- tion were unchanged. Upper radiographic gastro-intestinal studies and repeat gastric cy- tology studies were interpreted as consistent with atrophic gastritis.
The patient was readmitted to the hospital 4 months later for evaluation of his pulmo- nary lesion. Bronchoscopy was unremarkable and right scalene lymph node biopsy showed thyroid follicles in a peripheral lymph node sinus. Thyroid scan was normal (12% uptake in 24 hours). Thoracotomy was performed and the 2 cm lesion was excised from deep within the central portion of the left lower lobe. An additional one cm nodule was removed from the medial surface of the left upper lobe. Frozen section examination of both nodules revealed tumor microscopically consistent with thymoma. Exploration of the anterior mediastinum then revealed a mass 8 x 2 x 3 cm which was examined by biopsy and inter-
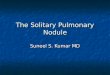
* FIG. 4. The mediastinal mass, multisected at autopsy.
Notc the coalescing nodular focally scarred pattern.

530 C A ~ C E K April 1966 Vol. I n
FIG. 5. Two distinctive patterns of thymoma. The left side of the field shows predominantly lymphoid elements whereas the right portion is composed predominantly of epithelial cells and contains typical cleftlike spaces ( ~ 8 7 ) .
FIG. 6 . Epithelial elements in the mediastinal mass show sharp cell margins and a “mosaic tile” pattern ( ~ 2 1 5 ) .

preted as thymonia. A mass in the spleen was palpated. The tumors microscopically were composed of spindly and ovoid epithelial ele- ments admixed with generous numbers of lymphocytes (Fig. 1-3). The patient was dis- charged on the sixteenth postoperative day. He was readmitted to the hospital 2 weeks later because of shortness of breath. Circula- tion time was 25 seconds. Digoxin was started. An electrocardiogram showed left ventricular hypertrophy and premature atrial contrac- tions. Two days after admission he became tlyspneic, developed a severe tachycardia and died shortly thereafter.
Autopsy revealed a well-developed large statured man with a healing left thoracotomy incision. The heart weighed 470 Gm. There was severe atherosclerosis of the coronary ar- teries and a fresh thrombus totally occluded the left anterior descending branch, 1.5 cm distal to its origin. The myocardium showed white and silvery focal streaking and fibrosis. Within the anterior mediastinal fat was a firm gritty white and yellow mottled tumor streaked with broad fibrous septa and measuring 8 X 4 x 2.5 cm. Numerous pseudopodlike exten- sions projected into the right pleural space and through the pericardium (Fig. 4). Multi-
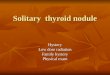
FIG. 7. Solitary hepatic metastasis within dome of right lobe showing the finely lobulated border.
ple sections revealed invasion of the innomi- nate vein system and constriction of the su- perior vena cava by stony hard gritty tumor. The lungs contained multiple small firm white to gray tumor nodules measuring up to 1.5 cm in diameter. The liver weighed 1,750 Gm and within the substance of the right lobe was a 4.5 cm “cauliflower-like” peripherally scalloped nodular white tumor mass. The spleen weighed 240 Gm. A 2.8 cm red some- what spongy pink and white tumor nodule was found in the parenchyma. Histolo,. WIC ex- amination of the mediastinal mass revealed epithelial and lymphoid thymic elements ex- isting in pure “culture” in some fields and
FIG. 8. Hcpatic metastasis demonstrating predominant lymphocyte population ( ~ 1 8 0 ) .

532 CANCER Apri l 1966 Vol. 19
admixture in other areas. Solid nests of cells resembling pure squamous epithelium were seen. Much necrosis and degeneration were seen (Fig. 5, 6) and dense fibrous septa oc- curred through the mass. The epithelial por- tion contained characteristic clefts and wide vascular spaces. Mitotic activity was seen within some fields. The pulmonary nodules revealed inixed spindly epithelial elements and lymphocytes. Bronchiolar invasion was observed. The hepatic and splenic nodules were composed predominantly of lymphoid cells with only a few plump and spindly epi- thelial elements recognizable (Fig. 7, 8). The examination of bone marrow failed to reveal thymic elements.
DISCUSSION
There are several interesting features to this
case. The primary th) nioma was composed of spindle cell and ovoid epithelial elements and lymphocytes existing in some fields as pure elements and in others as mixed elements. T h e pulmonary metastases were of mixed type, predominantly spindle and lymphoid with a few plump epithelial cells. Both the surgical specimen and autopsy examination revealed evidence of invasion of bronchial walls. The bizarre cells reported in cytological examination of sputum may have represented thymocytes. Perhaps some of the pulmonary dissemination could hake been a consequence of endobronchial implantation. The splenic and hepatic masses were almost pure lymphoid type of thymoma. The primary thymoma showed evidence of direct invasion of innom- inate vein structures. There is still a question as to whether the pulmonary mass had been present for many years prior to exploration.
REFERENCES
1. Castleman, B., ed.: Case Records of the Massa- chusetts General Hospital (Case 14-1966). New Eng. J . Med . 266:458-465, 1962.
2. - : Tumors of the thymus gland. Atlas of Tumor Pathology, sec. 5, fasc. 19. Washington, D.C., .4rmed Forces Institute of Pathology, 1955.
3. Clarkson, B., and Prockop, D. J.: Aregenerative anemia associated with benign thymoma. New Eng. J . M e d . 259:253-258, 19%.
4. Iverson, L.: Thymoma-Review and rerlassifica- tion. Am. J. Path. 32:695-719, 1956.
5. Josse, J. W., and Zacks, S. I.: Thymoma and pati- cytopenia. New E71g. J . Med. 259:113-117, 1958.
6. Lattes, R.: Thymoma and other tumors of thc thymus. Cancer 15:1224-1260, 1962.
7. O'Gara, R. W., Horn, R. C., Jr., and Enterline, H. T.: Tumors of the anterior mediastinum. Zbid. 11: 562:590, 1958.
8. Scholz, D. A., and Bahn, R. C.: Thymic tumors associated with Cushing's syndrome-Review of 3 cases. Proc. Mayo Clin. 34:433-441, 1959.