Embed Size (px)
Citation preview
75
The management of hepatic metastases has becomemore and more complex, and the role of the surgicaloncologist in directing care has become increasinglyimportant. Patients with metastatic colorectal cancerrepresent the majority in whom resection may beindicated, but other tumor types are also appropri-ately resected in some cases. Diagnostic methodsare increasingly sensitive and provide improveddelineation of extrahepatic disease and the relation-ship of metastatic tumors to the relevant normalanatomy of the liver. Intraoperative ultrasonographyand laparoscopy are two areas that are especially rel-evant to the hepatic surgeon. Multimodality therapyis often employed in the management of metastaticdisease in the liver. In addition to resection, radia-tion, and chemotherapy, modern treatment algo-rithms involve a variety of novel therapies, includingembolization, hepatic artery infusion of chemother-apy, cryotherapy, and radio-frequency ablation.Despite the multitude of therapeutic options, resec-tion of metastatic disease to the liver remains themost effective therapy in selected patients and ispotentially curative, unlike other modalities.
The range of treatments available for the man-agement of liver metastases has underlined theimportance of instituting a multidisciplinary plan-ning conference in any institution that treats a sig-nificant volume of patients with hepatic metastases.Such a forum allows for the appropriate selection ofthe best therapy for individual patients. In a subsetof patients, resection is indicated. Increasingly,resection is combined with other modalities to pro-
4
Metastatic Liver CancerANDREW J. SMITH, MD, FRCSCRONALD P. DEMATTEO, MDYUMAN FONG, MD, FACSLESLIE H. BLUMGART, MD, FACS, FRCS (ENG, EDIN, GLAS)
vide the best management of hepatic metastatic dis-ease. For example, experience is increasing regard-ing the efficacy of resection followed by adjuvantchemotherapy or hepatic artery infusion therapy orof resection combined with cryoablation of unre-sectable lesions. The purpose of this chapter is toreview the data supporting resection in differenttumor types. In addition, the indications, applica-tions, and limitations of hepatic resection formetastatic disease will be presented.
COLORECTAL CANCER METASTASES
Hepatic metastases from colorectal cancer (CRC) areidentified at some point in nearly half of all patientswith this disease. A large body of evidence supportsthe role of resection in the management of CRCmetastatic to the liver in selected patients.1 Resectionis accepted as the treatment of choice when all hepaticdisease can be removed and when there is no evidenceof extrahepatic metastatic disease. In the appropriatesetting, resection results in a 30 to 40 percent 5-yearsurvival rate, which is much greater than thatobserved with chemotherapy alone. Thus, althoughno prospective comparison of resection withchemotherapy has been performed, resection hasemerged as the most effective treatment, based onmarkedly improved survival in several large series.1–3
Recognition of the biologic and technical factorsthat govern success or failure is expected to allowimproved application of hepatic resection for CRC.2
Additionally, enhanced approaches to assessing dis-
76 HEPATOBILIARY CANCER
an uncommon phenomenon. Other gastrointestinaltumors such as esophageal, gastric, and pancreatictumors do not display this favorable pattern; conse-quently, hepatic resection has never been found to bea useful therapeutic option in these diseases. Ulti-mately, biologic factors, rather than technicalprowess, are the reason that hepatic resection hasemerged as a successful strategy in large numbers ofpatients with CRC metastases. Further improvementsin results can be expected as the understanding of thebiology of metastasis increases and as existing andnovel therapies are applied in a thoughtful manner.5
Diagnosis
A variety of modalities, including laboratory tests,radiologic examinations, and laparoscopy, are rele-vant in diagnosing patients with CRC hepatic metas-tases.6 These studies are done to initially identify
ease extent preoperatively have resulted in betterpatient selection and improved planning of resectionfor complex cases. Improvements in radiologicimaging technology and the use of laparoscopy min-imize unnecessary laparotomies. Furthermore, clin-ically identified risk factors may help identify thosepatients who will benefit from neoadjuvant, adju-vant, or alternative therapies. Toward that end, wehave developed a scoring system designed to givethe clinician a better estimate of the likelihood ofsuccess following hepatic resection2 (see below).
Epidemiology
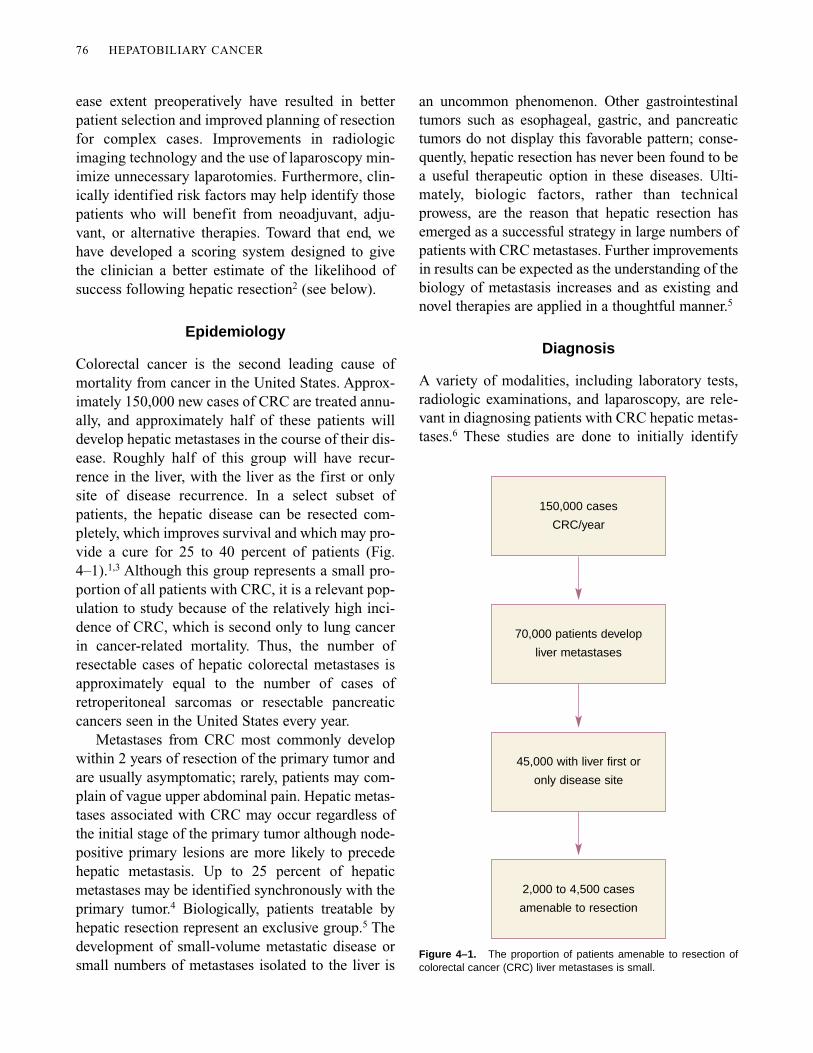
Colorectal cancer is the second leading cause ofmortality from cancer in the United States. Approx-imately 150,000 new cases of CRC are treated annu-ally, and approximately half of these patients willdevelop hepatic metastases in the course of their dis-ease. Roughly half of this group will have recur-rence in the liver, with the liver as the first or onlysite of disease recurrence. In a select subset ofpatients, the hepatic disease can be resected com-pletely, which improves survival and which may pro-vide a cure for 25 to 40 percent of patients (Fig.4–1).1,3 Although this group represents a small pro-portion of all patients with CRC, it is a relevant pop-ulation to study because of the relatively high inci-dence of CRC, which is second only to lung cancerin cancer-related mortality. Thus, the number ofresectable cases of hepatic colorectal metastases isapproximately equal to the number of cases ofretroperitoneal sarcomas or resectable pancreaticcancers seen in the United States every year.
Metastases from CRC most commonly developwithin 2 years of resection of the primary tumor andare usually asymptomatic; rarely, patients may com-plain of vague upper abdominal pain. Hepatic metas-tases associated with CRC may occur regardless ofthe initial stage of the primary tumor although node-positive primary lesions are more likely to precedehepatic metastasis. Up to 25 percent of hepaticmetastases may be identified synchronously with theprimary tumor.4 Biologically, patients treatable byhepatic resection represent an exclusive group.5 Thedevelopment of small-volume metastatic disease orsmall numbers of metastases isolated to the liver is
Figure 4–1. The proportion of patients amenable to resection ofcolorectal cancer (CRC) liver metastases is small.
150,000 cases
CRC/year
70,000 patients develop
liver metastases
45,000 with liver first or
only disease site
2,000 to 4,500 cases
amenable to resection
Metastatic Liver Cancer 77
hepatic metastases, determine suitability of resec-tion, and as follow-up after resection. In general,laboratory tests are done to screen for metastases.Serial carcinoembryonic antigen (CEA) levelassessment is useful for detecting recurrence inmany patients. Radiology has been progressivelyrefined such that ultrasonography (US), computedtomography (CT), and (to a lesser extent) magneticresonance imaging (MRI) provide the cornerstone ofidentification and assessment of CRC metastasis.Nuclear medicine scans such as CEA scans andOncoScint scanning have not proved useful and arenot done routinely. Positron emission tomography(PET) may prove useful, but its role remains to bedefined. Finally, laparoscopy has increasingly foundapplication in the assessment of resectability.
Screening for Hepatic Metastases
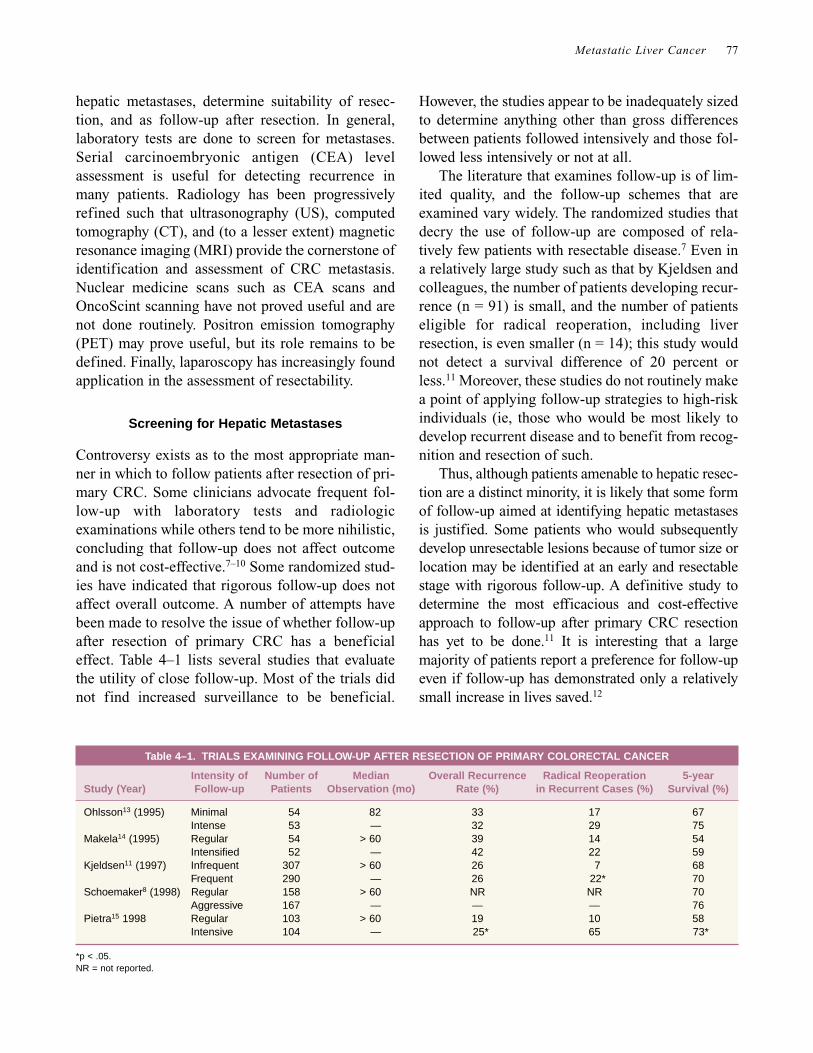
Controversy exists as to the most appropriate man-ner in which to follow patients after resection of pri-mary CRC. Some clinicians advocate frequent fol-low-up with laboratory tests and radiologicexaminations while others tend to be more nihilistic,concluding that follow-up does not affect outcomeand is not cost-effective.7–10 Some randomized stud-ies have indicated that rigorous follow-up does notaffect overall outcome. A number of attempts havebeen made to resolve the issue of whether follow-upafter resection of primary CRC has a beneficialeffect. Table 4–1 lists several studies that evaluatethe utility of close follow-up. Most of the trials didnot find increased surveillance to be beneficial.
However, the studies appear to be inadequately sizedto determine anything other than gross differencesbetween patients followed intensively and those fol-lowed less intensively or not at all.
The literature that examines follow-up is of lim-ited quality, and the follow-up schemes that areexamined vary widely. The randomized studies thatdecry the use of follow-up are composed of rela-tively few patients with resectable disease.7 Even ina relatively large study such as that by Kjeldsen andcolleagues, the number of patients developing recur-rence (n = 91) is small, and the number of patientseligible for radical reoperation, including liverresection, is even smaller (n = 14); this study wouldnot detect a survival difference of 20 percent orless.11 Moreover, these studies do not routinely makea point of applying follow-up strategies to high-riskindividuals (ie, those who would be most likely todevelop recurrent disease and to benefit from recog-nition and resection of such.
Thus, although patients amenable to hepatic resec-tion are a distinct minority, it is likely that some formof follow-up aimed at identifying hepatic metastasesis justified. Some patients who would subsequentlydevelop unresectable lesions because of tumor size orlocation may be identified at an early and resectablestage with rigorous follow-up. A definitive study todetermine the most efficacious and cost-effectiveapproach to follow-up after primary CRC resectionhas yet to be done.11 It is interesting that a largemajority of patients report a preference for follow-upeven if follow-up has demonstrated only a relativelysmall increase in lives saved.12
Table 4–1. TRIALS EXAMINING FOLLOW-UP AFTER RESECTION OF PRIMARY COLORECTAL CANCER
Intensity of Number of Median Overall Recurrence Radical Reoperation 5-year Study (Year) Follow-up Patients Observation (mo) Rate (%) in Recurrent Cases (%) Survival (%)
Ohlsson13 (1995) Minimal 54 82 33 17 67Intense 53 — 32 29 75
Makela14 (1995) Regular 54 > 60 39 14 54Intensified 52 — 42 22 59
Kjeldsen11 (1997) Infrequent 307 > 60 26 7 68Frequent 290 — 26 22* 70
Schoemaker8 (1998) Regular 158 > 60 NR NR 70Aggressive 167 — — — 76
Pietra15 1998 Regular 103 > 60 19 10 58Intensive 104 — 25* 65 73*
*p < .05.NR = not reported.
78 HEPATOBILIARY CANCER
Carcinoembryonic antigen (CEA) is a glycopro-tein that is found on the surface of CRC cells andthat can be secreted into the bloodstream.16,17 Usedas a screening tool, an elevated CEA level serves toprompt further investigation with radiologic studies.Several studies have shown that elevated CEA ishighly sensitive for the identification of hepaticmetastases. Although some authors have argued thatonly a small number of patients benefit from sur-veillance of CEA levels, other investigators haveconcluded that CEA-based follow-up strategies areefficacious and cost-effective.18 A study from theMayo Clinic found that patient survival nearly dou-bled when hepatic metastases were identified on thebasis of CEA elevation rather than tumor-relatedsymptoms.19 Because CEA-based strategies areassociated with survival benefit, the American Soci-ety of Clinical Oncology (ASCO) recommendations
indicate that CEA levels should be assessed every 2to 3 months in patients with stage 2 or 3 CRC for atleast 2 years after diagnosis (Table 4–2). Unfortu-nately, CEA-based strategies are of limited benefitin the 30 percent of patients whose tumors do notsecrete CEA as these patients are not expected tomanifest an elevation in CEA level, even with pro-gression of disease.
In addition to its utility in identifying hepaticmetastases, CEA level is predictive of prognosis fol-lowing hepatic resection; high levels of CEA areassociated with worse outcomes.2,5,20,21 There is littleevidence that other biochemical tests such as alka-line phosphatase or transaminase tests contribute tothe early identification of resectable tumors or to theprediction of outcomes following resection.1
Presently, there are no firm guidelines regardingthe use of radiologic investigations to screen for
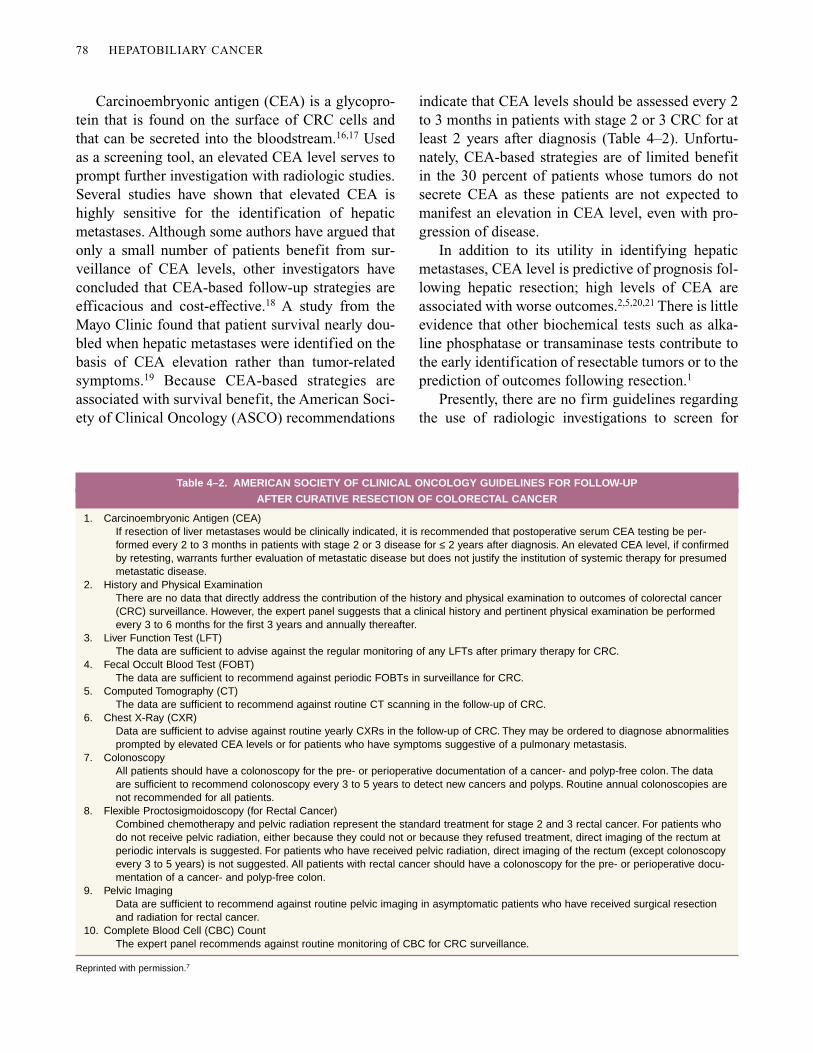
Table 4–2. AMERICAN SOCIETY OF CLINICAL ONCOLOGY GUIDELINES FOR FOLLOW-UP
AFTER CURATIVE RESECTION OF COLORECTAL CANCER
1. Carcinoembryonic Antigen (CEA)If resection of liver metastases would be clinically indicated, it is recommended that postoperative serum CEA testing be per-formed every 2 to 3 months in patients with stage 2 or 3 disease for ≤ 2 years after diagnosis. An elevated CEA level, if confirmedby retesting, warrants further evaluation of metastatic disease but does not justify the institution of systemic therapy for presumedmetastatic disease.
2. History and Physical ExaminationThere are no data that directly address the contribution of the history and physical examination to outcomes of colorectal cancer(CRC) surveillance. However, the expert panel suggests that a clinical history and pertinent physical examination be performedevery 3 to 6 months for the first 3 years and annually thereafter.
3. Liver Function Test (LFT)The data are sufficient to advise against the regular monitoring of any LFTs after primary therapy for CRC.
4. Fecal Occult Blood Test (FOBT)The data are sufficient to recommend against periodic FOBTs in surveillance for CRC.
5. Computed Tomography (CT)The data are sufficient to recommend against routine CT scanning in the follow-up of CRC.
6. Chest X-Ray (CXR)Data are sufficient to advise against routine yearly CXRs in the follow-up of CRC. They may be ordered to diagnose abnormalitiesprompted by elevated CEA levels or for patients who have symptoms suggestive of a pulmonary metastasis.
7. Colonoscopy All patients should have a colonoscopy for the pre- or perioperative documentation of a cancer- and polyp-free colon. The dataare sufficient to recommend colonoscopy every 3 to 5 years to detect new cancers and polyps. Routine annual colonoscopies arenot recommended for all patients.
8. Flexible Proctosigmoidoscopy (for Rectal Cancer) Combined chemotherapy and pelvic radiation represent the standard treatment for stage 2 and 3 rectal cancer. For patients whodo not receive pelvic radiation, either because they could not or because they refused treatment, direct imaging of the rectum atperiodic intervals is suggested. For patients who have received pelvic radiation, direct imaging of the rectum (except colonoscopyevery 3 to 5 years) is not suggested. All patients with rectal cancer should have a colonoscopy for the pre- or perioperative docu-mentation of a cancer- and polyp-free colon.
9. Pelvic ImagingData are sufficient to recommend against routine pelvic imaging in asymptomatic patients who have received surgical resectionand radiation for rectal cancer.
10. Complete Blood Cell (CBC) CountThe expert panel recommends against routine monitoring of CBC for CRC surveillance.
Reprinted with permission.7

Metastatic Liver Cancer 79
metastatic disease following colorectal resection forcancer. The ASCO recommendations do not includestandard follow-up with imaging following primaryresection. The argument is that CT or US rarelydetects recurrence before CEA levels are elevated.7
However, this fails to address the issue of non-CEA-secreting tumors, and it is likely that selectedpatients benefit from periodic imaging.
Liver US is a versatile tool in the evaluation of thepatient with suspected hepatic colorectal metastases.6
This modality has the advantage of being inexpen-sive, widely available, noninvasive, and sensitive forthe definition of hepatic metastases. Its limitationsinclude an inability to specifically characterize solidlesions as metastases as opposed to other benignlesions. Moreover, US is operator dependent and isnot as easily interpreted by nonradiologists as areother cross-sectional imaging techniques. Despitethis, it remains the most widely used screeningmethod worldwide for detection of hepatic metas-tases. Computed tomography is more sensitive andless operator dependent than US. Nonetheless, CTinvolves increased expense, the use of radiation, andthe risk of nephrotoxic and allergic reactions, thuslimiting its application as a routine screening tool.
The ideal radiologic approach to screening forhepatic CRC metastases remains to be established.Any algorithms used should be sensitive and cost-effective, and should have an impact on patient out-come. At present, approximately 25 percent of clin-icians routinely follow up patients by usingradiologic tests designed to detect metastases.9
Although the evidence does not exist to fully recom-mend follow-up investigations after primary col-orectal resection for cancer, neither does existingevidence exclude imaging as being worthwhile atsome interval in selected patients.
Unlike follow-up after resection of the primarylesion, follow-up imaging (CT or US) after hepaticresection is indicated for patients undergoing suc-cessful hepatic resection for CRC metastases.Although a majority of lesions will recur at hepaticand extrahepatic sites and be incurable, there is theoccasional opportunity to successfully resect recur-rent hepatic disease in some patients.22–26 Studieshave confirmed long-term survival in some patientsafter repeat hepatic resection.
Determining Resectability
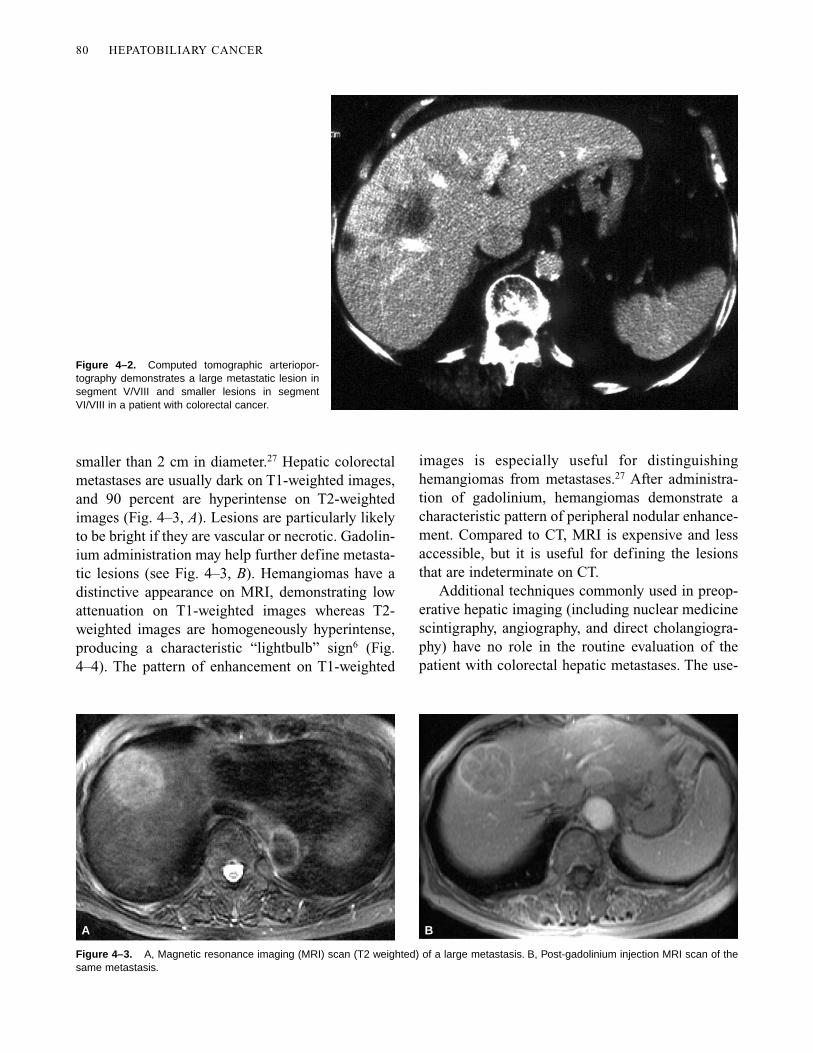
The majority of patients with hepatic metastaseshave unresectable disease either because of theextent of disease in the liver or because of the pres-ence of extrahepatic disease. In general, radiologicexaminations are the primary tools that guide deci-sions regarding resectability,6 and the CT scan is themost widely used study because it can define therelationship of the tumor to its surrounding vascularand biliary structures, reveal the extent of diseasewithin the liver, and allow assessment of extrahep-atic disease. Imaging studies with enhanced andnon-enhanced views are critical to obtain maximalassessment of the liver parenchyma. The spiral orhelical CT scan allows the rapid acquisition of datawith decreased artifact as well as decreased require-ments for intravenous contrast. This technique isassociated with a reduction in partial-volume aver-aging and a consequently improved detection ofsmaller metastases. Computed tomographic arterio-portography (CTAP) is a more invasive procedurebut represents the “gold standard” for the detectionand preoperative assessment of liver metastases. Thisprocedure involves the injection of contrast into themesenteric circulation and the acquisition of imagedata during the portal phase, when the liverparenchyma tends to be more vascular compared tothe surrounding tumor that is supplied by the hepaticarterial system. This technique is particularly sensi-tive for the detection of lesions less than 2 cm in size;overall, it detects hepatic metastases at a rate ofgreater than 90 percent (Fig. 4–2). The arteriographobtained during this procedure is also of value inpatients who will undergo placement of a hepaticartery infusion pump. Information obtained duringthis stage of the study is valuable for identifyingaberrant arterial anatomy. As noninvasive imagingmodalities (MRI and CT) advance, they will likelysupplant angiography for this purpose.
Magnetic resonance imaging of the abdomenoccasionally gives additional information beyondthat provided by high-quality CT. It is especiallyuseful in differentiating hemangiomas from metas-tases and may accurately characterize lesions ashemangiomas in 84 to 95 percent of cases. More-over, MRI is helpful in characterizing lesions
80 HEPATOBILIARY CANCER
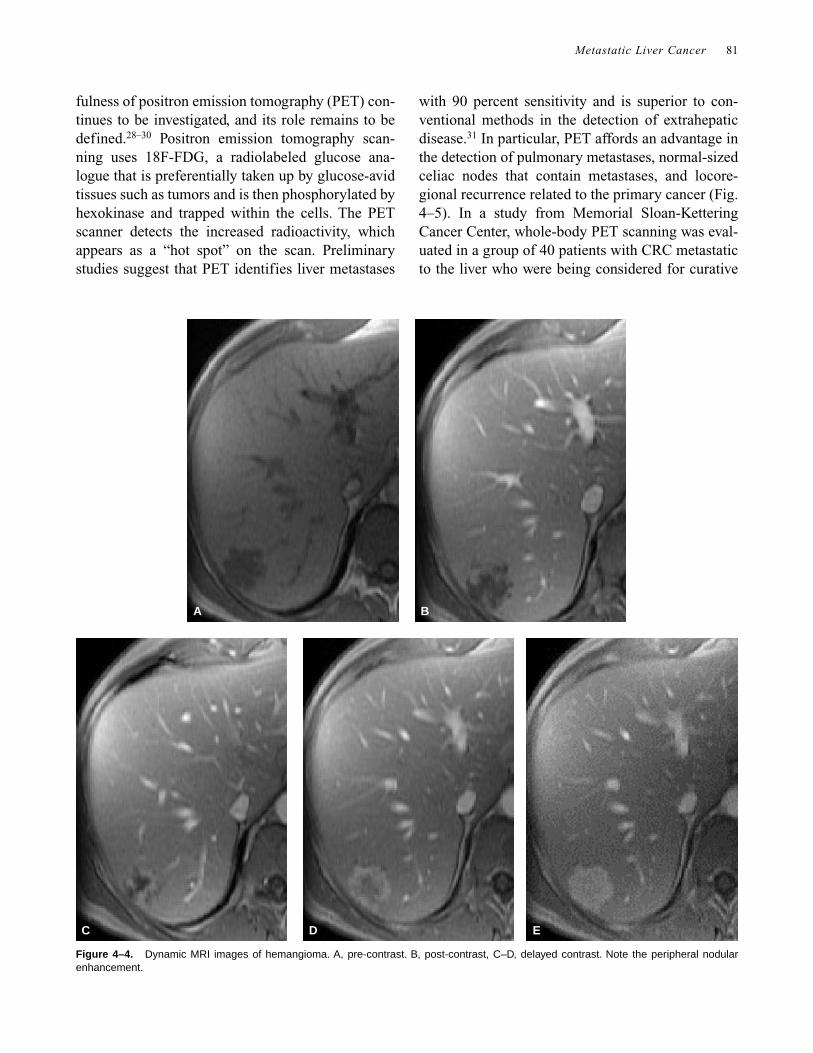
smaller than 2 cm in diameter.27 Hepatic colorectalmetastases are usually dark on T1-weighted images,and 90 percent are hyperintense on T2-weightedimages (Fig. 4–3, A). Lesions are particularly likelyto be bright if they are vascular or necrotic. Gadolin-ium administration may help further define metasta-tic lesions (see Fig. 4–3, B). Hemangiomas have adistinctive appearance on MRI, demonstrating lowattenuation on T1-weighted images whereas T2-weighted images are homogeneously hyperintense,producing a characteristic “lightbulb” sign6 (Fig.4–4). The pattern of enhancement on T1-weighted
Figure 4–3. A, Magnetic resonance imaging (MRI) scan (T2 weighted) of a large metastasis. B, Post-gadolinium injection MRI scan of thesame metastasis.
A B
images is especially useful for distinguishinghemangiomas from metastases.27 After administra-tion of gadolinium, hemangiomas demonstrate acharacteristic pattern of peripheral nodular enhance-ment. Compared to CT, MRI is expensive and lessaccessible, but it is useful for defining the lesionsthat are indeterminate on CT.
Additional techniques commonly used in preop-erative hepatic imaging (including nuclear medicinescintigraphy, angiography, and direct cholangiogra-phy) have no role in the routine evaluation of thepatient with colorectal hepatic metastases. The use-
Figure 4–2. Computed tomographic arteriopor-tography demonstrates a large metastatic lesion insegment V/VIII and smaller lesions in segmentVI/VIII in a patient with colorectal cancer.
Metastatic Liver Cancer 81
fulness of positron emission tomography (PET) con-tinues to be investigated, and its role remains to bedefined.28–30 Positron emission tomography scan-ning uses 18F-FDG, a radiolabeled glucose ana-logue that is preferentially taken up by glucose-avidtissues such as tumors and is then phosphorylated byhexokinase and trapped within the cells. The PETscanner detects the increased radioactivity, whichappears as a “hot spot” on the scan. Preliminarystudies suggest that PET identifies liver metastases
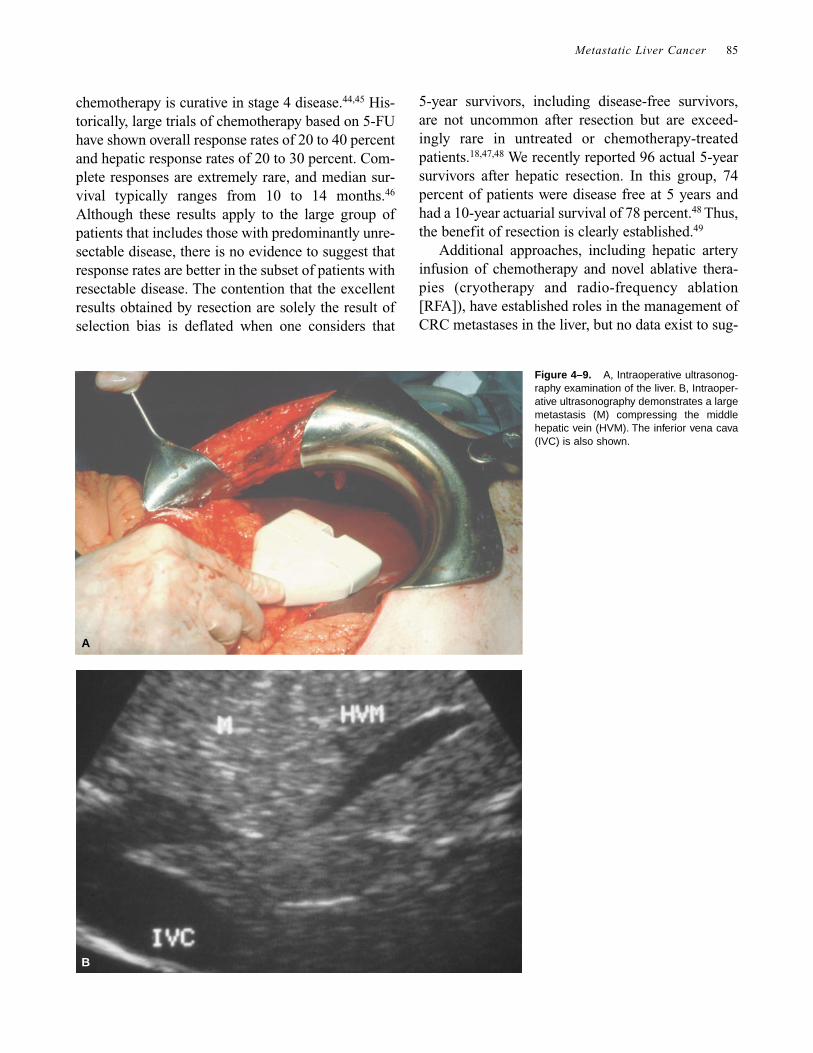
with 90 percent sensitivity and is superior to con-ventional methods in the detection of extrahepaticdisease.31 In particular, PET affords an advantage inthe detection of pulmonary metastases, normal-sizedceliac nodes that contain metastases, and locore-gional recurrence related to the primary cancer (Fig.4–5). In a study from Memorial Sloan-KetteringCancer Center, whole-body PET scanning was eval-uated in a group of 40 patients with CRC metastaticto the liver who were being considered for curative
A B
C D E
Figure 4–4. Dynamic MRI images of hemangioma. A, pre-contrast. B, post-contrast, C–D, delayed contrast. Note the peripheral nodularenhancement.
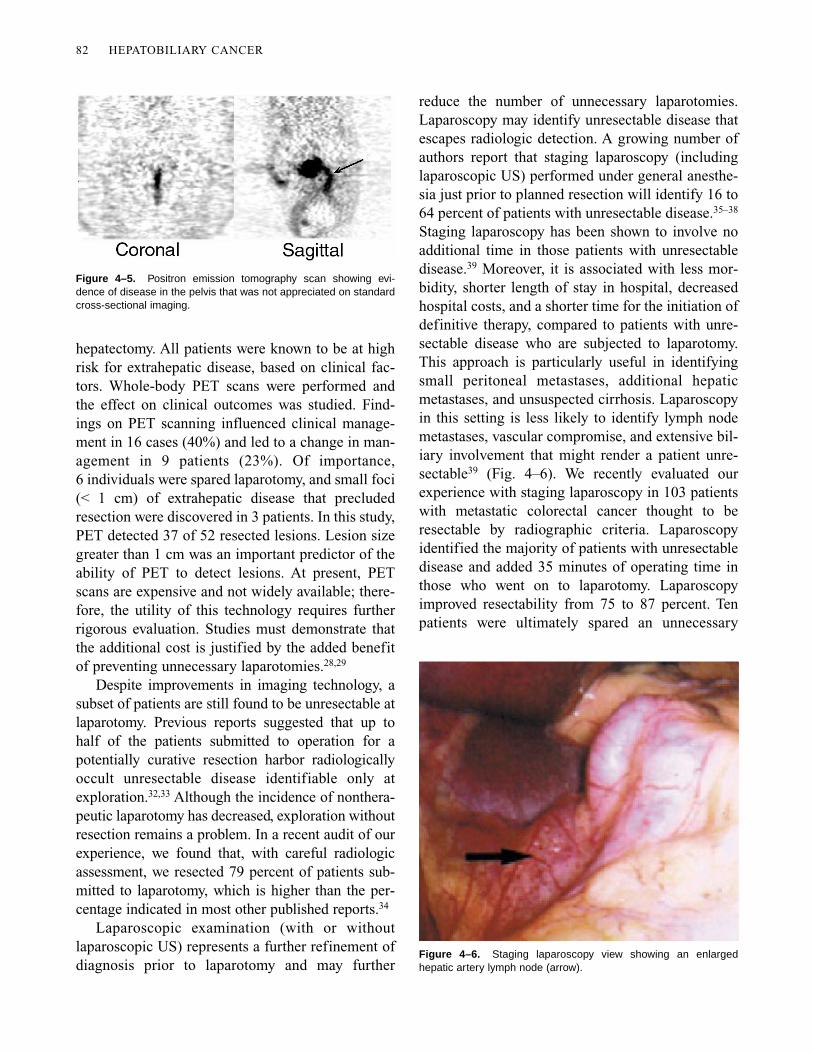
Figure 4–6. Staging laparoscopy view showing an enlargedhepatic artery lymph node (arrow).
Figure 4–5. Positron emission tomography scan showing evi-dence of disease in the pelvis that was not appreciated on standardcross-sectional imaging.
82 HEPATOBILIARY CANCER
hepatectomy. All patients were known to be at highrisk for extrahepatic disease, based on clinical fac-tors. Whole-body PET scans were performed andthe effect on clinical outcomes was studied. Find-ings on PET scanning influenced clinical manage-ment in 16 cases (40%) and led to a change in man-agement in 9 patients (23%). Of importance,6 individuals were spared laparotomy, and small foci(< 1 cm) of extrahepatic disease that precludedresection were discovered in 3 patients. In this study,PET detected 37 of 52 resected lesions. Lesion sizegreater than 1 cm was an important predictor of theability of PET to detect lesions. At present, PETscans are expensive and not widely available; there-fore, the utility of this technology requires furtherrigorous evaluation. Studies must demonstrate thatthe additional cost is justified by the added benefitof preventing unnecessary laparotomies.28,29
Despite improvements in imaging technology, asubset of patients are still found to be unresectable atlaparotomy. Previous reports suggested that up tohalf of the patients submitted to operation for apotentially curative resection harbor radiologicallyoccult unresectable disease identifiable only atexploration.32,33 Although the incidence of nonthera-peutic laparotomy has decreased, exploration withoutresection remains a problem. In a recent audit of ourexperience, we found that, with careful radiologicassessment, we resected 79 percent of patients sub-mitted to laparotomy, which is higher than the per-centage indicated in most other published reports.34
Laparoscopic examination (with or withoutlaparoscopic US) represents a further refinement ofdiagnosis prior to laparotomy and may further
reduce the number of unnecessary laparotomies.Laparoscopy may identify unresectable disease thatescapes radiologic detection. A growing number ofauthors report that staging laparoscopy (includinglaparoscopic US) performed under general anesthe-sia just prior to planned resection will identify 16 to64 percent of patients with unresectable disease.35–38
Staging laparoscopy has been shown to involve noadditional time in those patients with unresectabledisease.39 Moreover, it is associated with less mor-bidity, shorter length of stay in hospital, decreasedhospital costs, and a shorter time for the initiation ofdefinitive therapy, compared to patients with unre-sectable disease who are subjected to laparotomy.This approach is particularly useful in identifyingsmall peritoneal metastases, additional hepaticmetastases, and unsuspected cirrhosis. Laparoscopyin this setting is less likely to identify lymph nodemetastases, vascular compromise, and extensive bil-iary involvement that might render a patient unre-sectable39 (Fig. 4–6). We recently evaluated ourexperience with staging laparoscopy in 103 patientswith metastatic colorectal cancer thought to beresectable by radiographic criteria. Laparoscopyidentified the majority of patients with unresectabledisease and added 35 minutes of operating time inthose who went on to laparotomy. Laparoscopyimproved resectability from 75 to 87 percent. Tenpatients were ultimately spared an unnecessary

Metastatic Liver Cancer 83
laparotomy while 4 had alternative palliative proce-dures. Nevertheless, hospital stay and charges weresignificantly decreased for those with unresectabledisease seen at laparoscopy rather than at laparo-tomy. Outcomes in the cohort managed withlaparoscopy are summarized in Figure 4–7.
The addition of laparoscopic US has beenreported to add to the laparoscopic staging examina-tion.35–38 High-quality images showing tumor-vesselrelationships can be obtained (Fig. 4–8). In ourexperience, however, laparoscopic US had a loweryield than that reported by others. In our experience,10 percent of patients had additional tumors identi-fied by laparoscopic US but the majority of patientsunderwent resection despite these findings. Overall,laparoscopic US by itself identified unresectabledisease in 3 of 103 patients.39 Clearly, the yield ofboth laparoscopy and laparoscopic US depends onthe quality of preoperative imaging, and the rela-tively small yield that we observed is almost cer-tainly related to improved radiographic techniques.
Intraoperative ultrasonography (IOUS), per-formed at laparotomy, has been an important tool forassessing resectability, and it remains in wide use.The sensitivity of open IOUS for detecting metas-tases is 96 percent, compared to 91 percent for CTportography. Moreover, IOUS may alter manage-ment in 10 to 48 percent of cases.40–42 In some cases,it causes the surgeon to change the planned resectionbecause new lesions are identified or because unan-ticipated vascular involvement is detected (Fig.4–9). There is a significant learning curve for thenovice using IOUS. However, once the surgeongains facility with it, the technique is especially use-ful in clarifying the relationship of tumors to theportal structures and hepatic veins. This feature isparticularly important when planning segmental orsectoral resections43 (Fig. 4–10). Many hepatic sur-geons have found it useful to arrange to have a des-ignated radiologist in the operating room for IOUS.The procedure can usually be completed in about15 minutes, thus minimizing the amount of time the
Unresectable diseaseseen at laparoscopy
14 patients
Avoided laparotomy
10 patients
Other proceduresperformed*
4 patients
Additional findings seenat laparoscopy
Planned resection changed
4 patients
Not helpful
68 patients
No additional findings confirmed preop impression
Resected as planned
54 patients
Additional findings missed at laparoscopy
Resected (plan changed in 6)
8 patients
Additional findings seenat laparoscopy
No change in planned resection
8 patients
Unresectable diseasemissed at laparoscopy
8 patients(7 biopsy only, 1 HA pump)
Laparoscopy unsuccessful
9 patients(5 resected, 4 biopsy only)
103 patients
Figure 4–7. Outcome with staging laparoscopy in patients with hepatic colorectal cancer metastases. (HA = hepatic artery;preop = preoperative.) Reproduced with permission from Jarnagin WR, Bodniewicz J, Dougherty, E, et al. A prospective analy-sis of staging laparoscopy in patients with primary and secondary hepatobiliary malignancies. Ann Surg Oncol [In press].
*hepatic artery pump (2),colostomy, colectomy

84 HEPATOBILIARY CANCER
radiologist is out of the radiology department butensuring that the maximum benefit from the IOUSis obtained. Open US, like laparoscopic US, contin-ues to be used routinely, but it is likely that the yieldwill continue to decrease as better imaging becomeswidely available.
Outcomes of Resection
Natural History of Colorectal Cancer Metastases
An understanding of the impact of surgical resectionin patients with hepatic CRC metastases requires anunderstanding of the natural history of colorectalmetastases to the liver (Table 4–3). Although a ran-domized study comparing survival in treated anduntreated patients has never been done, a number ofretrospective studies have addressed the issue of out-comes in patients with unresected liver metastases.Survival after resection is better than that foruntreated hepatic metastases, even when only themost favorable unresected cases are considered.Median survival in patients with unresectable diseaseconsistently ranges from 3 to 21 months, and 5-yearsurvival is rare, occurring in less than 2 percent ofpatients.1,3 Survival is most dependent on the extentof hepatic involvement: the more extensive theinvolvement, the worse the survival. Some authorshave attempted to identify retrospectively patients
who are not offered resection but who have poten-tially resectable disease, as determined from data inthe clinical record. Wood and colleagues identified13 patients with disease inferred to be resectablefrom a total of 126 patients with hepatic metas-tases.41 Survival was markedly better in this group of13, compared to those with unresectable disease. The1-year survival was 77 percent, compared to 15 per-cent in the unresectable group; 3-year survival was23 percent, compared to 0 percent; and 5-year sur-vival was 8 percent. Similarly, a report from theMayo Clinic compared 141 patients who had resec-tions of CRC hepatic metastases with 70 patientswho had potentially resectable tumors treated nonop-eratively.42 Five-year survival in the resection groupwas 25 percent, compared to 2.5 percent in the unre-sected group. Scheele compared three groups: 183patients with resected metastases, 62 patients whohad resectable lesions that were not removed, and921 patients with unresectable disease.43 The 5-yearsurvival in the resected group was 38 percent whilethere were no 5-year survivors in the nonoperatedgroups. Moreover, patients in the resectable but non-operated group had a median survival of 14 months,compared to 6.9 months for the unresectable group.Conceding the limitations of these retrospective stud-ies, it appears that a patient with disease that is poten-tially resectable probably has a more favorable tumorbiology and a better prognosis than a patient withunresectable disease. However, these data alsostrongly suggest that resection improves survival,even in the group with favorable biology. Extendedsurvival is associated only with resection, and 5-yearsurvivors represent less than 3 percent of patients inall series of unresected colorectal hepatic metastases.
Alternative Treatments
Extensive experience in treating metastatic CRCwith chemotherapy has been obtained over the pasttwo decades. Regimens including 5-fluorouracil (5-FU) with or without the modulation of folinic acid(leucovorin) have been the mainstay of chemother-apy in stage 4 disease. Despite progress in under-standing the best timing of dose administration andthe emergence of new active agents against metasta-tic CRC, there are no data to suggest that systemic
Figure 4–8. Image from a laparoscopic ultrasound examinationshowing a metastatic colorectal cancer lesion at the hilus, encroach-ing on the left hepatic duct.
Metastatic Liver Cancer 85
chemotherapy is curative in stage 4 disease.44,45 His-torically, large trials of chemotherapy based on 5-FUhave shown overall response rates of 20 to 40 percentand hepatic response rates of 20 to 30 percent. Com-plete responses are extremely rare, and median sur-vival typically ranges from 10 to 14 months.46
Although these results apply to the large group ofpatients that includes those with predominantly unre-sectable disease, there is no evidence to suggest thatresponse rates are better in the subset of patients withresectable disease. The contention that the excellentresults obtained by resection are solely the result ofselection bias is deflated when one considers that
5-year survivors, including disease-free survivors,are not uncommon after resection but are exceed-ingly rare in untreated or chemotherapy-treatedpatients.18,47,48 We recently reported 96 actual 5-yearsurvivors after hepatic resection. In this group, 74percent of patients were disease free at 5 years andhad a 10-year actuarial survival of 78 percent.48 Thus,the benefit of resection is clearly established.49
Additional approaches, including hepatic arteryinfusion of chemotherapy and novel ablative thera-pies (cryotherapy and radio-frequency ablation[RFA]), have established roles in the management ofCRC metastases in the liver, but no data exist to sug-
Figure 4–9. A, Intraoperative ultrasonog-raphy examination of the liver. B, Intraoper-ative ultrasonography demonstrates a largemetastasis (M) compressing the middlehepatic vein (HVM). The inferior vena cava(IVC) is also shown.
A
B
86 HEPATOBILIARY CANCER
Table 4–3. LARGE SERIES EXAMINING
THE NATURAL HISTORY OF UNRESECTED
UNTREATED COLORECTAL CANCER METASTASES
Number of Median 5-yr SurvivalAuthor Patients Survival (months) (%)
Pestana50 353 9.0 3Cady51 269 13.0 1Lahr52 175 6.1 1Wagner53 252 19.0 2Scheele54 921 6.9 0Stangl55 484 7.5 1Rougier56 318 5.7 —
gest that any of these modalities should supplantresection as the treatment gold standard. The appli-cation of cryotherapy and RFA remain limited bytumor size and location. Lesions adjacent to major
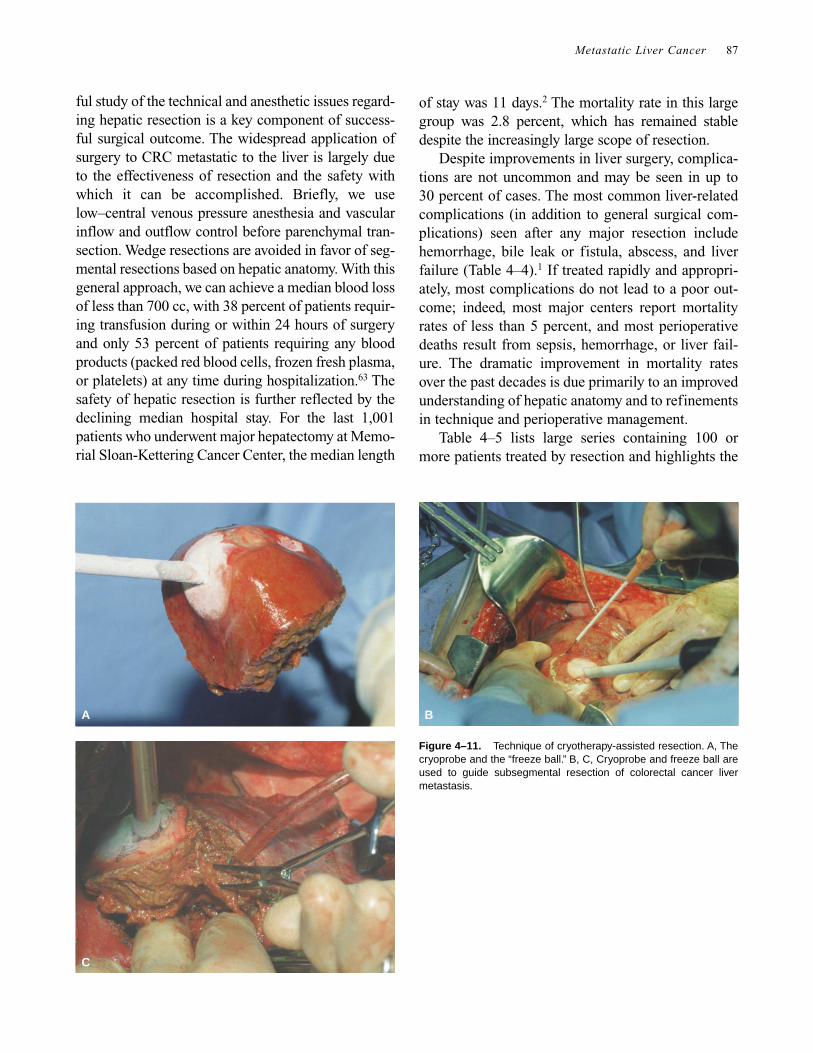
vascular structures cannot be completely ablated.The potential advantage of RFA is that it is moresuited to percutaneous application. On the otherhand, RFA is more limited by tumor size than iscryotherapy, and following the progress of the abla-tion by US is more difficult and imprecise. Cryother-apy should be reserved for those patients who cannotundergo resection although it may have a role inselected cases as an adjunct to resection57,58 (Fig.4–11). Cryotherapy combined with hepatic arteryinfusion,59 cryotherapy for close resection margins,60
cryotherapy-assisted resections,61 and combinedresection and cryotherapy for multiple lesions areexamples of novel ways in which resection may becomplemented with emerging ablative technologies.Details of these approaches are discussed in otherchapters. The increasing complexity of decisionmaking in these cases underscores the benefit of amultidisciplinary planning conference to optimizethe planning of treatment for individual patients.62
Resection of Colorectal Hepatic Metastases
Numerous reports have shown that selected patientsbenefit from resection, resulting in 5-year survivalin 20 to 40 percent of patients and disease-free sur-vival in up to 30 percent of patients. Moreover, tech-nical advances and the increasing application ofmultimodality management to hepatic CRC metas-tases have expanded the group of patients in whomsurgical therapy may be appropriate. Long-term sur-vival and cure are now possible for patients previ-ously considered unresectable.1
Our approach to resection is described elsewherein this book. It should be stressed, however, that care-
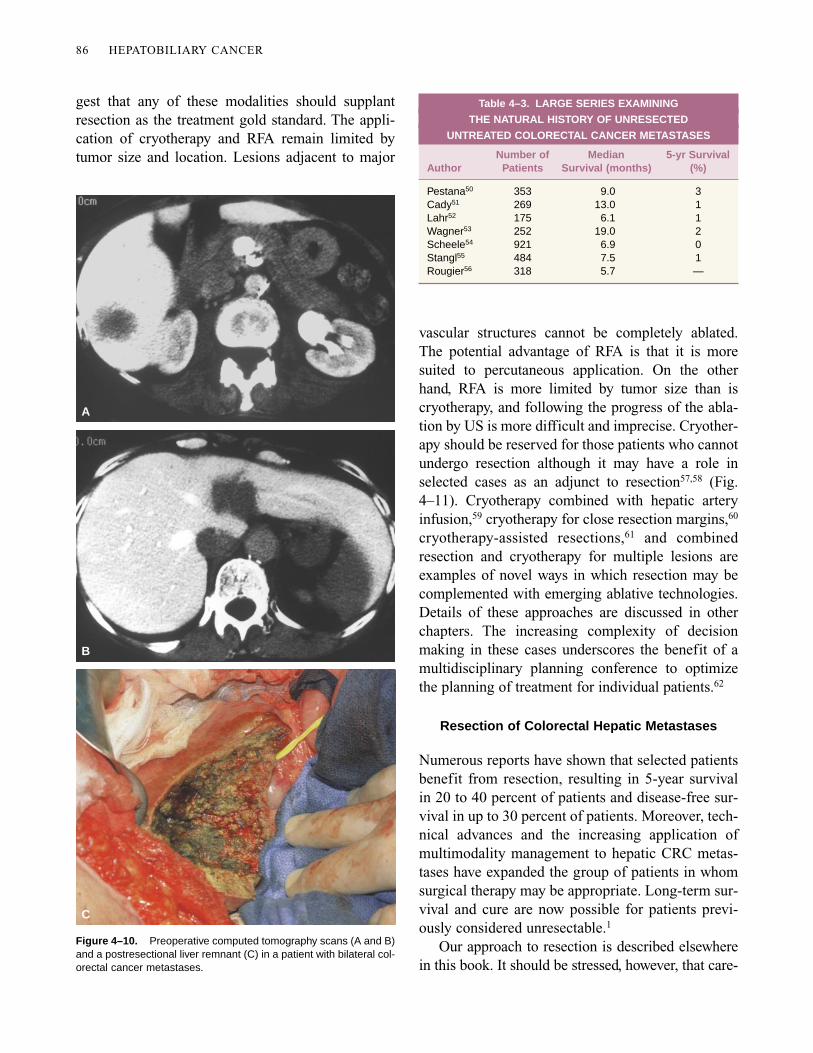
Figure 4–10. Preoperative computed tomography scans (A and B)and a postresectional liver remnant (C) in a patient with bilateral col-orectal cancer metastases.
B
A
C
Metastatic Liver Cancer 87
ful study of the technical and anesthetic issues regard-ing hepatic resection is a key component of success-ful surgical outcome. The widespread application ofsurgery to CRC metastatic to the liver is largely dueto the effectiveness of resection and the safety withwhich it can be accomplished. Briefly, we uselow–central venous pressure anesthesia and vascularinflow and outflow control before parenchymal tran-section. Wedge resections are avoided in favor of seg-mental resections based on hepatic anatomy. With thisgeneral approach, we can achieve a median blood lossof less than 700 cc, with 38 percent of patients requir-ing transfusion during or within 24 hours of surgeryand only 53 percent of patients requiring any bloodproducts (packed red blood cells, frozen fresh plasma,or platelets) at any time during hospitalization.63 Thesafety of hepatic resection is further reflected by thedeclining median hospital stay. For the last 1,001patients who underwent major hepatectomy at Memo-rial Sloan-Kettering Cancer Center, the median length
of stay was 11 days.2 The mortality rate in this largegroup was 2.8 percent, which has remained stabledespite the increasingly large scope of resection.
Despite improvements in liver surgery, complica-tions are not uncommon and may be seen in up to30 percent of cases. The most common liver-relatedcomplications (in addition to general surgical com-plications) seen after any major resection includehemorrhage, bile leak or fistula, abscess, and liverfailure (Table 4–4).1 If treated rapidly and appropri-ately, most complications do not lead to a poor out-come; indeed, most major centers report mortalityrates of less than 5 percent, and most perioperativedeaths result from sepsis, hemorrhage, or liver fail-ure. The dramatic improvement in mortality ratesover the past decades is due primarily to an improvedunderstanding of hepatic anatomy and to refinementsin technique and perioperative management.
Table 4–5 lists large series containing 100 ormore patients treated by resection and highlights the
Figure 4–11. Technique of cryotherapy-assisted resection. A, Thecryoprobe and the “freeze ball.” B, C, Cryoprobe and freeze ball areused to guide subsegmental resection of colorectal cancer livermetastasis.
A B
C
88 HEPATOBILIARY CANCER
5-year survival rates. Of importance, the majority ofpatients treated with liver resection will developrecurrence. Experience with resection has shown thatstrategy and technique are ultimately limited by bio-logic factors. Technical issues that affect patient out-come have been better described than have biologicfactors, which are difficult to modulate presently.
An important goal of the ongoing investigationinto the natural history of this disease is to betterdelineate patients who will benefit from resection andto distinguish them from patients with disease that islikely to recur even after complete resection.31 Withidentification of the latter group, it would be possibleto use adjuvant therapies with resection to eradicatemicroscopic residual disease and improve results.
Several studies have identified a number of fac-tors that influence outcome after hepatic resectionfor CRC metastases. The “tumor biology” ispresently defined by standard clinical and pathologicfeatures of patients and their cancers. This relativelysimple approach may change in the near future asvarious molecular markers are rigorously studied.64,65
Patient factors limiting the application of hepaticresection are few. Medically infirm patients are notconsidered for hepatic resection although age aloneis not a contraindication. We and others have demon-strated that excellent results can be achieved in olderpatients, with acceptable mortality.66 Most studiesshow no effect of the sex of the patient on outcome.1
Factors related to the primary tumor help definethe tumor biology and influence outcome.1,2 The siteof the initial tumor does not have an impact on out-come. There is an adverse relationship between thepresence of lymph node metastases associated withthe primary tumor and survival following the resec-tion of subsequent liver metastases.1,2 Most studiessuggest that liver metastases diagnosed synchro-nously with the primary tumor have a worse out-come, compared to those metastases diagnosed
metachronously. Furthermore, analysis of someseries suggests that longer disease-free intervals areassociated with a better outcome.1
The characteristics of metastases in the liver alsoshed light on the biology of the disease. The numberof metastases in the liver affects outcome: patientswith solitary metastases fare better than those withmultiple metastases. Nonetheless, the presence ofmultiple metastases or bilateral disease is not a con-traindication to resection. Although resection ofhepatic metastases was initially reserved for patientswith solitary metastases, it is now evident that mul-tiple metastases can be resected with the expectationof good results for patients with bilobar and unilobarmetastases.3,43 Tumor size and CEA levels have alsobeen identified as prognostic factors. Completeexcision, with negative margins, of all disease is themost significant predictor of outcome.2,15
There are now sufficient data to identify factorsassociated with a high risk of recurrence followinghepatic resection.2 Despite this, no single factorshould be used to deny resection, because resectionaffords the possibility of cure and because there is alack of effective alternatives. In otherwise healthypatients, extrahepatic disease and the inability toresect all disease safely are the generally acceptedcontraindications. However, even this has been chal-lenged as selected patients with limited metastaticdisease to the lungs and liver may also benefit fromresection of all disease at both sites. Despite thesecaveats, it is clear that some patients will benefitmore than others from resection. In an effort to iden-tify such patients, we have devised a clinical-riskscore that includes five preoperative factors that areindependent predictors of survival. This system was
Table 4–4. LIVER-RELATED COMPLICATIONS
FOLLOWING MAJOR RESECTION
Complication Rate (%)
Liver failure 3–8 Bile leak, biliary fistula 4Perihepatic abscess 2–10Severe hemorrhage 1–3
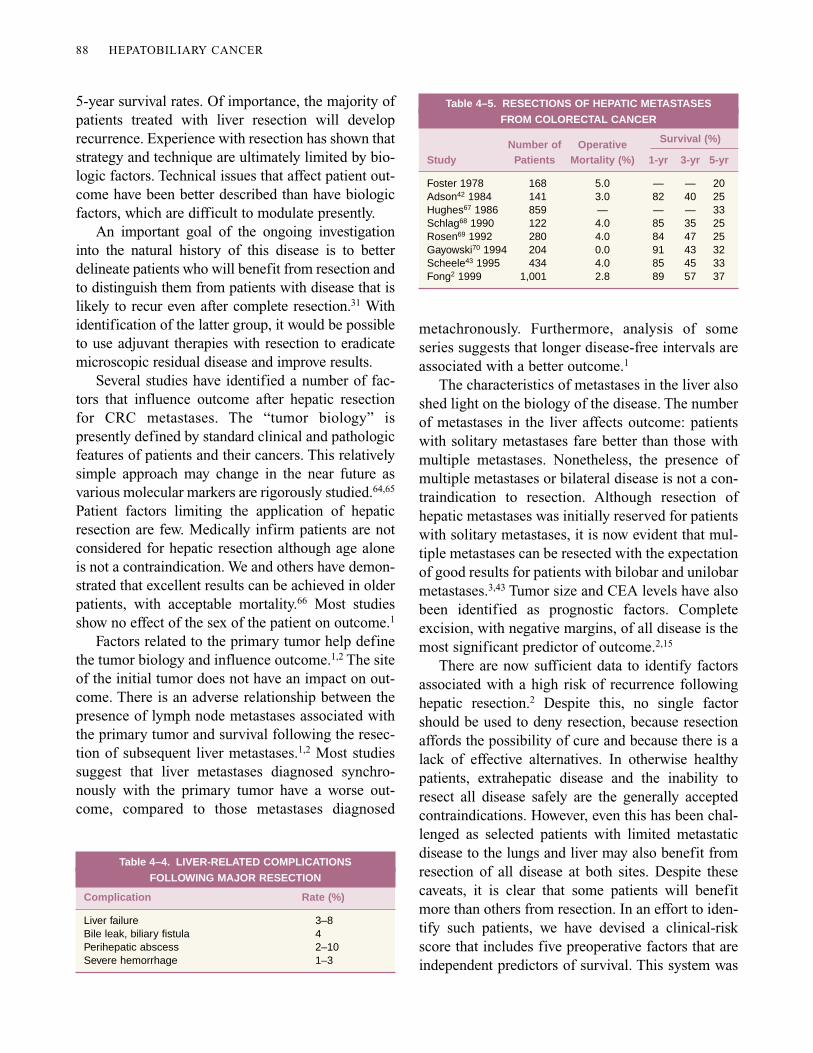
Table 4–5. RESECTIONS OF HEPATIC METASTASES
FROM COLORECTAL CANCER
Number of Operative Survival (%)
Study Patients Mortality (%) 1-yr 3-yr 5-yr
Foster 1978 168 5.0 — — 20Adson42 1984 141 3.0 82 40 25Hughes67 1986 859 — — — 33Schlag68 1990 122 4.0 85 35 25Rosen69 1992 280 4.0 84 47 25Gayowski70 1994 204 0.0 91 43 32Scheele43 1995 434 4.0 85 45 33Fong2 1999 1,001 2.8 89 57 37

Metastatic Liver Cancer 89
devised after review of clinical, pathologic, and out-come data for 1,001 consecutive patients undergoingliver resection for metastatic CRC.2 This groupincluded 237 trisegmentectomies, 394 lobectomies,and 370 resections of less than a lobe. In this group,the operative mortality was 2.8 percent, the 5-yearsurvival rate was 37 percent, and the 10-year survivalrate was 22 percent. Multivariate analysis identifiedseven factors as significant predictors of poor out-come: (1) positive hepatic resection margins, (2)extrahepatic disease, (3) a node-positive primarytumor, (4) a disease-free interval from primary can-cer to metastasis of < 12 months, (5) multiple hepatictumors, (6) the largest hepatic tumor being > 5 cm indiameter, and (7) a CEA level > 200 ng/mL. The lastfive of these features can be easily identified preop-eratively and serve as the basis of a clinical-risk scor-ing system.2 Each adverse factor is worth 1 point,and the final clinical-risk score is the sum. We haveshown that this scoring system significantly pre-dicted survival, which was 74 months (median) inpatients with a score of 0 and 22 months in patientswith a score of 5 (Table 4–6).2
Prognostic systems such as this serve mainly toprovide the clinician with a more sophisticatedmeans of assessing the potential benefit of resection.Staging patients in this way allows a more cogentdiscussion between doctor and patient with respectto the risks and benefits of surgery. In addition, itmay delineate those patients who make up a high-risk group and who may be served well by adjuvanttherapy. Most important, this system can be used tostratify patients in clinical trials. It should bestressed that this system is meant not to excludeindividuals from hepatic resection that represents apotentially curative option, but rather to assess the
risk of recurrence and to perhaps select those whoshould receive additional treatment.
The presence of extrahepatic disease is generallyan indication that the patient has diffuse disease andis therefore unlikely to benefit from hepatic resec-tion. However, this tenet has been challenged in thecontext of pulmonary and liver metastases fromCRC.72 At Memorial Sloan-Kettering Cancer Cen-ter, we have shown that resection of pulmonary andhepatic CRC metastases is associated with extendedsurvival in highly selected patients. A review of81 patients showed extended survival in a group ofpatients with hepatic and pulmonary metastaticCRC. With a median follow-up of 3.7 years fromresection of the first metastasis and a median fol-low-up of 2.5 years once a liver and a lung resectionhad been performed, median survival was 6.0 and3.8 years, respectively.72 This report represents ahighly selected group but shows that some patientscan be salvaged.
Recurrent disease after hepatic resection gener-ally portends a poor outcome, but some patients maybe appropriate for repeat resection. Recurrence ofCRC develops in 56 to 78 percent of patients afterpartial hepatectomy; in approximately half of thesepatients, the disease is isolated to the liver.48 A selectfew will be eligible for repeat resection after they areshown to have no extrahepatic disease.19–23 This pro-cedure may be more technically difficult due to thepresence of adhesions and to hypertrophy of theliver remnant. Nonetheless, when done in experi-enced units, the morbidity and mortality of repeatresection is similar to that of primary resection. In aseries of long-term survivors, 43 percent were ren-dered disease free following repeat hepatectomy forrecurrent hepatic CRC. A multi-institutional study
Table 4–6. CLINICAL-RISK SCORES FOR TUMOR RECURRENCE
Survival (%)
Score 1 yr 2 yr 3 yr 4 yr 5 yr Median Survival (mo)
0 93 79 72 60 60 741 91 76 66 54 44 512 89 73 60 51 40 473 86 67 42 25 25 334 70 45 38 29 20 205 71 45 27 14 14 22
Risk factors are node-positive primary; disease-free interval < 12 months; > 1 tumor; size > 5 cm; carcinoembryonic antigen level > 200 ng/mL. Each risk factorequals 1 point in scoring.

90 HEPATOBILIARY CANCER
of 170 patients demonstrated that a 3-year survivalof 37 percent and a 5-year survival of 26 percent fol-lowing reresection can be expected in this group.19
Technical surgical advances have had an impacton prognosis following resection of CRC metas-tases. These advances specifically relate to thesafety of resection and to the achievement of nega-tive margins. The need to achieve negative surgicalmargins cannot be overemphasized. Resection thatleaves a positive margin generally results in recur-rence although occasional long-term survivors havebeen reported.3,18,40,47,48 The Gastrointestinal TumorStudy Group showed that curative resection resultedin significantly longer median survival (37 vs21 months) compared to palliative resection, whichyielded results similar to those in unresectedpatients.73 Although some authors have maintainedthat margins of at least 1 cm are necessary, we havefound that this is not necessarily the case and thatnegative histologic margins of any depth are accept-able and associated with good outcome.3,18,47
Anatomic resections afford the best chance ofachieving negative margins. Lobar and extendedlobar resections have typically been used to achievethis end. However, techniques of segmental resec-tion also allow resection of multiple lesions whilepreserving liver parenchyma.40 This has allowed amore aggressive approach to bilobar disease. Wehave shown that segmental resections are associatedwith a much lower incidence of positive histologicmargins and consequently with better survival.75
Wedge resection, therefore, should be discouragedfor all but the smallest, most peripheral lesions. Thishas implications for the patient with liver metastasesdiscovered incidentally at operation for primaryCRC. In general, attempts at resection in such a con-text should be avoided, with a plan for further post-operative imaging to fully assess disease extent.
The remarkable regenerative capacity of the liverenables the hepatic surgeon to perform resections ofup to 80 percent of hepatic parenchyma in a normalliver without causing hepatic failure. Nonetheless,there are scenarios in which performing extendedhepatectomy can be expected to cause hepatic failureif the remnant liver is too small or is abnormal (fatty,fibrotic, or cirrhotic). This is particularly worrisomein the case of a small deep lesion that would require
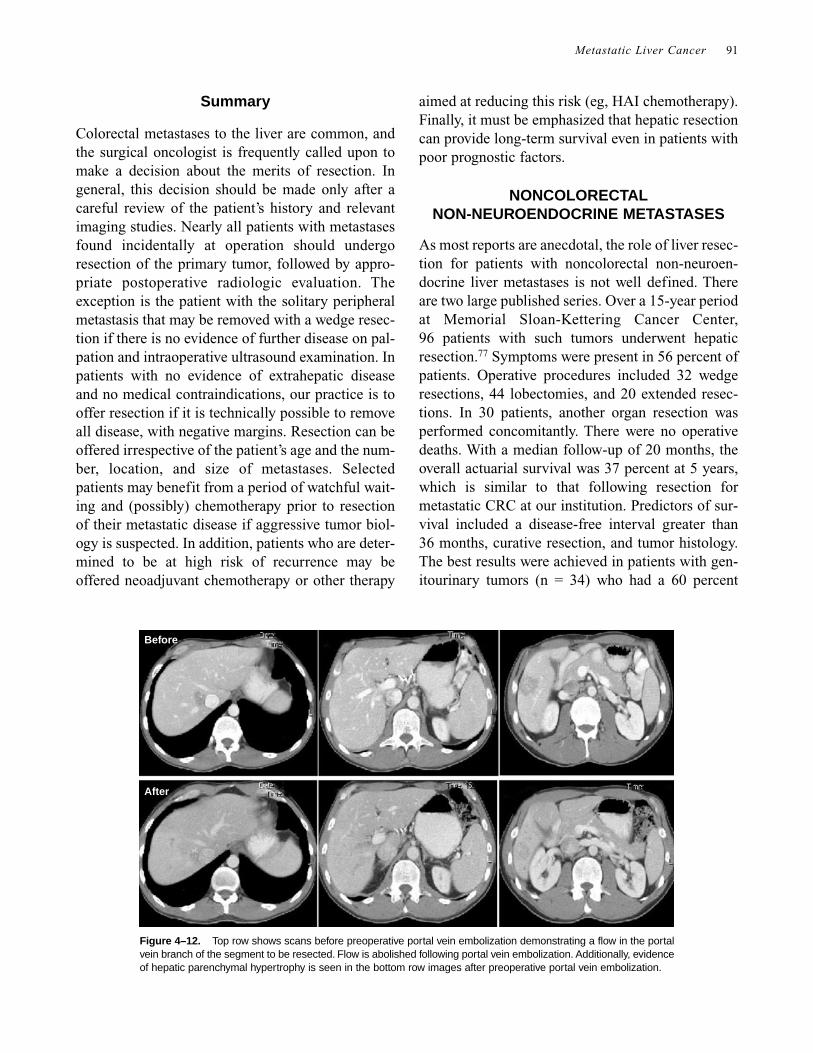
sacrificing a large amount of normal liver tissue.Recently, some investigators reported their experi-ence with preoperative portal vein embolization in aneffort to overcome this limitation. With this tech-nique, the portal vein supplying the parenchyma tobe resected is embolized before operation. After 2 to4 weeks, compensatory hypertrophy of the unin-volved side of the liver occurs, thus reducing theamount of functional parenchyma resected.74,75 It ishoped that by inducing hypertrophy of the liver rem-nant preoperatively, the risk of postoperative hepaticfailure will be lowered (Fig. 4–12). It must beemphasized, however, that experience with portalvein embolization is limited, that the indications arenot clearly defined, and that no prospective compar-ison studies have been performed. It remains to beseen whether this technique will find a role inpatients with metastatic CRC, especially given thelow operative mortality in most large centers.
It is likely that we are approaching the limits ofwhat can be achieved with resection of hepaticmetastases. Two challenges for the future are toselect patients for resection in the best manner andto determine which patients are at prohibitive risk ofrecurrence following operation. High-risk individu-als may be better served by a strategy that alsoaddresses their risk of micrometastatic disease.Although there is no standard approach to neoadju-vant chemotherapy in high-risk patients, there aredata to recommend that approach.74 Some authorshave found that patients initially deemed unre-sectable became subsequently resectable following acourse of aggressive chemotherapy.44 More recentapproaches to aggressive adjuvant therapy followinghepatic resection include hepatic arterial infusion(HAI) and systemic therapy after resection ofhepatic metastases from CRC. Kemeny and col-leagues have reported that HAI with floxuridine anddexamethasone followed by systemic 5-FU and leu-covorin produces better 2-year survival and disease-free survival than systemic therapy alone.76 Finally,the emergence of a newer systemic chemotherapythat has improved activity over chemotherapy basedon 5-FU may mean that these agents (eg, CPT-11,oxaliplatin) will find an application in liver resectionfor CRC. Indeed, trials are under way to test thesedrugs in this setting.
Metastatic Liver Cancer 91
Summary
Colorectal metastases to the liver are common, andthe surgical oncologist is frequently called upon tomake a decision about the merits of resection. Ingeneral, this decision should be made only after acareful review of the patient’s history and relevantimaging studies. Nearly all patients with metastasesfound incidentally at operation should undergoresection of the primary tumor, followed by appro-priate postoperative radiologic evaluation. Theexception is the patient with the solitary peripheralmetastasis that may be removed with a wedge resec-tion if there is no evidence of further disease on pal-pation and intraoperative ultrasound examination. Inpatients with no evidence of extrahepatic diseaseand no medical contraindications, our practice is tooffer resection if it is technically possible to removeall disease, with negative margins. Resection can beoffered irrespective of the patient’s age and the num-ber, location, and size of metastases. Selectedpatients may benefit from a period of watchful wait-ing and (possibly) chemotherapy prior to resectionof their metastatic disease if aggressive tumor biol-ogy is suspected. In addition, patients who are deter-mined to be at high risk of recurrence may beoffered neoadjuvant chemotherapy or other therapy
aimed at reducing this risk (eg, HAI chemotherapy).Finally, it must be emphasized that hepatic resectioncan provide long-term survival even in patients withpoor prognostic factors.
NONCOLORECTAL NON-NEUROENDOCRINE METASTASES
As most reports are anecdotal, the role of liver resec-tion for patients with noncolorectal non-neuroen-docrine liver metastases is not well defined. Thereare two large published series. Over a 15-year periodat Memorial Sloan-Kettering Cancer Center,96 patients with such tumors underwent hepaticresection.77 Symptoms were present in 56 percent ofpatients. Operative procedures included 32 wedgeresections, 44 lobectomies, and 20 extended resec-tions. In 30 patients, another organ resection wasperformed concomitantly. There were no operativedeaths. With a median follow-up of 20 months, theoverall actuarial survival was 37 percent at 5 years,which is similar to that following resection formetastatic CRC at our institution. Predictors of sur-vival included a disease-free interval greater than36 months, curative resection, and tumor histology.The best results were achieved in patients with gen-itourinary tumors (n = 34) who had a 60 percent
Figure 4–12. Top row shows scans before preoperative portal vein embolization demonstrating a flow in the portalvein branch of the segment to be resected. Flow is abolished following portal vein embolization. Additionally, evidenceof hepatic parenchymal hypertrophy is seen in the bottom row images after preoperative portal vein embolization.
Before
After

92 HEPATOBILIARY CANCER
5-year survival, with 7 (2 adrenal, 3 renal, 1 testicu-lar, and 1 ovarian) actual 5-year survivors. Hepatec-tomy was performed in 41 patients with soft-tissuetumors (7 melanomas [1 ocular], 7 breast cancers, and27 sarcomas), with a 5-year survival of 26 percent.Two-thirds of the sarcomas were leiomyosarcomas;the median survival for these patients was 31 months.Resection of gastrointestinal primaries (n = 7) result-ed in a median survival of 21 months but no 5-yearsurvivors. Patients with an unknown primary tumor(n = 8) did particularly poorly; all died of diseasewithin 1 year. Similar results were reported in a seriesof 120 resections for noncolorectal non-neuroen-docrine liver metastases.78 The overall 5-year survivalrate was 36 percent; it was 20 percent for breast can-cers (n = 35), 46 percent for testicular cancers(n = 20), and > 20 percent for gynecologic tumors.Patients with sarcomas, gastrointestinal malignancies,melanomas, head and neck tumors, and unknown pri-maries all had poor outcomes.
In other reports, 15 patients with Wilms’ tumorhad a median survival of 24 months; at 5 years, therewere 4 survivors79 after resection. In a study of 13patients with metastatic melanoma to the liver, therewas a median survival of 10 months, and only 1 per-son survived for 5 years.79 Ocular melanoma repre-sents an important subgroup with a more favorableprognosis. Ocular melanoma has a propensity tometastasize to the liver, which is often the first site ofrecurrence in some patients. In 19 patients with ocu-lar melanoma who underwent complete resection ofall gross liver disease and who received postopera-tive intra-arterial chemotherapy, there was a mediansurvival of 22 months.80 However, 16 patients hadrecurrences at a mean of 14 months.
Resection of noncolorectal non-neuroendocrineliver metastases is rarely indicated. However, inhighly selected patients with a long disease-freeinterval, resection may be reasonable, and prolongedsurvival may be achieved. A period of observationprior to surgery may reveal the biology of the tumorto determine the suitability of resection (ie, somepatients’ cancer may rapidly progress during a shortperiod of observation, indicating that their tumorsare biologically unfavorable and not amenable tobenefit from surgical resection). Hepatectomy maybe indicated to palliate symptoms, accurately stage
or diagnose a patient, or debulk disease prior toadjuvant therapy. Concomitant resection of extra-hepatic disease may also be necessary. Patients withtesticular or ovarian liver metastases appear to havethe best outcome after partial hepatectomy andshould be considered for resection to remove resid-ual disease after systemic chemotherapy. Patientswith metastatic disease from other primary lesions(melanoma, breast, and gastrointestinal) should beapproached with caution, given the high rates ofrecurrence in these patients. Patients with metastaticsarcoma may benefit more from hepatic resectionthan previously reported. Given the lack of effectivealternative treatments, this group of patients is diffi-cult to manage. Chemotherapy and other interven-tions have not proven effective. Furthermore, trans-plantation in these patients should not beconsidered; less than half of 27 patients in one studysurvived 1 year.81
REFERENCES
1. Blumgart LH, Fong Y. Surgical options in the treatmentof hepatic metastasis from CRC. Curr Probl Surg1995;32:333–421.
2. Fong Y, Fortner JG, Sun R, et al. Clinical score for pre-dicting recurrence after hepatic resection: analysisof 1001 consecutive resections for metastatic CRC.Ann Surg 1999;230:309–18.
3. Fong Y, Cohen AM, Fortner JG, et al. Liver resection forcolorectal metastases. J Clin Oncol 1997;15:938–46.
4. Bengmark S, Hafstrom L. The natural history of pri-mary and secondary malignant tumors of the liver.I. The prognosis for patients with hepatic metastasesfrom colonic and rectal carcinoma by laparotomy.Cancer 1969;23:198–202.
5. Cady B, Stone MD, McDermott WVJ, et al. Technicaland biological factors in disease-free survival afterhepatic resection for CRC metastases. Arch Surg1992;127:561–8.
6. DeMatteo RP, Fong Y. Imaging of hepatobiliary neo-plasms. Surg Oncol Clin N Am 1999;8:59–89.
7. Desch CE, Benson AB, Smith TJ, et al. Recommendedcolorectal cancer surveillance guidelines by theAmerican Society of Clinical Oncology. J Clin Oncol1999;17:1312–21.
8. Schoemaker D, Black R, Giles L, Toouli J. Yearlycolonoscopy, liver CT, and chest radiography do notinfluence 5-year survival of CRC patients. Gas-troenterology 1998;114:7–14.
Metastatic Liver Cancer 93
9. Virgo KS, Wade TP, Longo WE, et al. Surveillanceafter curative colon cancer resection: practice pat-terns of surgical subspecialists. Ann Surg Oncol1995;2:472–82.
10. Virgo KS, Vernava AM, Longo WE, et al. Cost ofpatient follow-up after potentially curative CRCtreatment. JAMA 1995;273:1837–41.
11. Kjeldsen BJ, Kronborg O, Fenger C, Jorgensen OD. Aprospective randomized study of follow-up afterradical surgery for colorectal cancer. Br J Surg1997:84:666–9.
12. Stiggelbout AM, de Haes JCM, Vree R, et al. Followup of colorectal cancer patients: quality of life andattitudes towards follow-up. Br J Cancer 1997;75:914–20.
13. Ohlsson B, Breland U, Ekberg H, et al. Follow-up aftercurative surgery for colorectal carcinoma: random-ized comparison with no follow-up. Dis Colon Rec-tum 1995;38:619–26.
14. Makela JT, Laitinen SO, Kairaluama MI. Five year fol-low-up after radical surgery for colorectal cancer.Arch Surg 1995;130:1062–7.
15. Pietra N, Sarli L, Costi R, et al. Role of follow-up inmanagement of local recurrences of colorectal can-cer: a prospective, randomized study. Dis ColonRectum 1998;41:1127–33.
16. Vauthey JN, Dudrick PS, Lind DS, Copeland EM.Management of recurrent CRC: another look at car-cinoembryonic antigen-detected recurrence. DigDis 1996;14:5–13.
17. Mitchell EP. Role of carcinoembryonic antigen in themanagement of advanced CRC. Semin Oncol1998;25:(5Suppl 11):12–20.
18. Jaeck D, Bachellier P, Guiguet M, et al. Long-term sur-vival following resection of colorectal hepaticmetastases. Association Francaise de Chirurgie. BrJ Surg 1997;84:977–80.
19. Fernandez-Trigo V, Shamsa F, Sugarbaker PH. Repeatliver resections from colorectal metastasis. RepeatHepatic Metastases Registry. Surgery 1995;117:296–304.
20. Fong Y, Blumgart LH, Cohen A, et al. Repeat hepaticresections for metastatic CRC. Ann Surg 1994;220:657–62.
21. Jaeck D, Bachellier P, Guiguet M, et al. Survival bene-fit of repeat liver resection for recurrent colorectalmetastases: 143 cases. Wiad Lek 1997;50 (Suppl 1,Pt. 1):102–4.
22. Nordlinger B, Vaillant JC. Repeat resections for recur-rent colorectal liver metastases. Cancer Treat Res1994;69:57–61.
23. Wanebo HJ, Chu QD, Avradopoulos KA, Vezeridis MP.Current perspectives on repeat hepatic resection for
colorectal carcinoma: a review. Surgery 1996;119:361–71.
24. Mitchell DG, Saini S, Weinreb J, et al. Hepatic metas-tases and cavernous hemangiomas: distinction withstandard- and triple-dose gadoteridol-enhanced MRimaging. Radiology 1994;193:49–57.
25. Beets G, Penninckx F, Schiepers C, et al. Clinical valueof whole-body positron emission tomography with[18F]fluorodeoxyglucose in recurrent CRC. Br JSurg 1994;81:1666–70.
26. Lai DT, Fulham M, Stephen MS, et al. The role of whole-body positron emission tomography with [18F]fluo-rodeoxyglucose in identifying operable CRC metas-tases to the liver. Arch Surg 1996;131:703–7.
27. Ogunbiyi OA, Flanagan FL, Dehdashti F, et al. Detec-tion of recurrent and metastatic CRC: comparisonof positron emission tomography and computedtomography. Ann Surg Oncol 1997;4:613–20.
28. Fong Y, Saldinger PF, Akhurst T, et al. Utility of F-FDGpositron emission tomography scanning on selec-tion of patients for resection of hepatic colorectalmetastases. Am J Surg 1999;178:282–7.
29. Babineau TJ, Lewis WD, Jenkins RL, et al. Role ofstaging laparoscopy in the treatment of hepaticmalignancy. Am J Surg 1994;167:151–4.
30. Callery MP, Strasberg SM, Doherty GM, et al. Staginglaparoscopy with laparoscopic ultrasonography:optimizing resectability in hepatobiliary and pan-creatic malignancy. J Am Coll Surg 1997;185:33–9.
31. Jarnagin WR, Fong Y, Ky A, et al. Liver resection formetastatic CRC: assessing the risk of occult irre-sectable disease. J Am Coll Surg 1999;188:33–42.
32. Lo CM, Lai EC, Liu CL, et al. Laparoscopy andlaparoscopic ultrasonography avoid exploratorylaparotomy in patients with hepatocellular carci-noma. Ann Surg 1998;227:527–32.
33. Babineau T, Lewis D, Jenkins R, et al. Role of staginglaparoscopy in the treatment of hepatic malignancy.Am J Surg 1994;167:151–5.
34. Callery MP, Strasberg SM, Doherty GM, et al. Staginglaparoscopy with laparoscopic ultrasonography:optimizing resectability in hepatobiliary and pan-creatic malignancy. J Am Coll Surg 1997;185:33–9.
35. John TG, Greig JD, Crosbie JL, et al. Superior stagingof liver tumors with laparoscopy and laparoscopicultrasound. Ann Surg 1994;220:711–9.
36. Jarnagin WR, Bodniewicz J, Dougherty E, et al. Aprospective analysis of staging laparoscopy inpatients with primary and secondary hepatobiliarymalignancies. J Gastrointest Surg 2000;4:34–43.
37. Castaing D, Emond J, Kunstlinger F, Bismuth H. Util-ity of operative ultrasound in the surgical manage-ment of liver tumors. Ann Surg 1986;204:600–5.
94 HEPATOBILIARY CANCER
38. Rifkin MD, Rosato FE, Branch HM, et al. Intraopera-tive ultrasound of the liver. An important adjunctivetool for decision making in the operating room. AnnSurg 1987;205:466–72.
39. Ravikumar TS. Laparoscopic staging and intraopera-tive ultrasonography for liver tumor management.Surg Oncol Clin N Am 1996;5:271–82.
40. Billingsley KG, Jarnagin WR, Fong Y, Blumgart LH.Segment-oriented hepatic resection in the manage-ment of malignant neoplasms of the liver. J Am CollSurg 1998;187:471–81.
41. Wood CB, Gillis CR, Blumgart LH. A retrospectivestudy of the natural history of patients with livermetastases from CRC. Clin Oncol 1976;2:285–8.
42. Adson MA, van Heerden JA, Adson MH, et al. Resec-tion of hepatic metastases from CRC. Arch Surg1984;119:647–51.
43. Scheele J, Stang R, Altendorf-Hofmann A, Paul M.Resection of colorectal liver metastases. World JSurg 1995;19:59–71.
44. Levi F, Zidani R, Misset JL. Randomised multicentretrial of chronotherapy with oxaliplatin, fluorouracil,and folinic acid in metastatic CRC. InternationalOrganization for Cancer Chronotherapy. Lancet1997;350:681–6.
45. Cunningham D, Pyrhonen S, James RD, et al. Ran-domised trial of irinotecan plus supportive care ver-sus supportive care alone after fluorouracil failurefor patients with metastatic CRC. Lancet 1998;352:1413–8.
46. Advanced CRC Meta-Analysis Project. Modulation offluorouracil by leucovorin in patients with advancedCRC: evidence in terms of response rate. J ClinOncol 1992;10:896–903.
47. Geoghegan JG, Scheele J. Treatment of colorectal livermetastases. Br J Surg 1999;86:158–69.
48. D’Angelica M, Brennan MF, Fortner JG, et al. Ninety-six five-year survivors after liver resection formetastatic CRC. J Am Coll Surg 1997;185:554–9.
49. Goldberg RM, Fleming TR, Tangen CM, et al. Surgeryfor recurrent colon cancer: strategies for identifyingresectable recurrence and success rates after resec-tion. Eastern Cooperative Oncology Group, theNorth Central Cancer Treatment Group, and theSouthwest Oncology Group. Ann Intern Med1998;129:27–35.
50. Pestana C, Reitemeier R, Moertel CG, et al. The nat-ural history of carcinoma of the colon and rectum.Am J Surg 1964;108:826–29.
51. Cady B, Monson DO, Swinton NW. Survival ofpatients after colonic resection for carcinoma withsimultaneous liver metastases. Surg Gynecol Obstet1970:131:697–700.
52. Lahr CJ, Soong SJ, Cloud G, et al. A multifactorialanalysis of prognostic factors in patients with livermetastases from colorectal carcinoma. J Clin Oncol1983;1:720–6.
53. Wagner JS, Adson MA, van Heerden JA, Adson MH,Ilstrup DM. The natural history of hepatic metas-tases from colorectal cancer. A comparison withresective treatment. Ann Surg 1984;199:502–8.
54. Scheele J, Stangl R, Altendorf-Hofmann A. Hepaticmetastases from colorectal carcinoma: impact ofsurgical resection on the natural history. Br J Surg1990;77:1241–6.
55. Stangl R, Altendorf-Hoffmann A, Charnley Rm, ScheeleJ. Factors influencing the natural history of colorec-tal liver mestastases. Lancet 1994;343:1405–10.
56. Rougier P, Milan C, Lazorthes F, et al. Prospectivestudy of prognostic factors in patients with unre-sected hejpatic metastases from colorectal cancer.Fondation Francaise de Cancerologie Digestive. BrJ Surg 1995;82:1397–400.
57. McCarty TM, Kuhn JA. Cryotherapy for liver tumors.Oncology 1998;12:979–87.
58. Seifert JK, Junginger T, Morris DL. A collectivereview of the world literature on hepatic cryother-apy. J R Coll Surg Edinb 1998;43:141–54.
59. Stubbs RS, Alwan MH, Booth MW. Hepatic cryother-apy and subsequent hepatic arterial chemotherapyfor colorectal metastases to the liver. HPB Surg1998;11:97–104.
60. Seifert JK, Morris DL. Cryotherapy of the resectionedge after liver resection for CRC metastases. AustN Z J Surg 1998;68:725–8.
61. Welling RE, Lamping K. Cryoprobe as a “handle” forresection of metastatic liver tumors. J Surg Oncol1990;45:227–8.
62. Hugh TJ, Kinsella AR, Poston GJ. Management strate-gies for colorectal liver metastases—Part I. SurgOncol 1997;6:19–30.
63. Melendez JA, Arslan V, Fischer ME, et al. Perioperativeoutcomes of major hepatic resections under low cen-tral venous pressure anesthesia: blood loss, bloodtransfusion, and the risk of postoperative renal dis-function. J Am Coll Surg 1998;187:620–5.
64. Belluco C, Guillem JG, Kemeny N, et al. p53 nuclearprotein overexpression in CRC: a dominant predic-tor of survival in patients with advanced hepaticmetastases. J Clin Oncol 1996;14:2696–701.
65. Nitti D, Belluco C, Montesco MC, et al. Nuclear p53protein expression in resected hepatic metastasesfrom CRC: an independent prognostic factor of sur-vival. Eur J Cancer 1998;34:851–5.
66. Fong Y, Brennan MF, Cohen AM, et al. Liver resectionin the elderly. Br J Surg 1997;84:1386–90.
Metastatic Liver Cancer 95
74. Bismuth H, Adam R, Levi F, et al. Resection of nonre-sectable liver metastases from CRC after neoadju-vant chemotherapy. Ann Surg 1996;224:509–20.
75. Elias D, Lasser P, Rougier P, et al. Frequency, technicalaspects, results, and indications of major hepatec-tomy after prolonged intra-arterial hepaticchemotherapy for initially unresectable hepatictumors. J Am Coll Surg 1995;180:213–9.
76. Kemeny N, Huang Y, Cohen AM, et al. Hepatic arter-ial infusion of chemotherapy after resection ofhepatic metastases from colorecal cancer. N Engl JMed 1999;341:2039–48.
77. Harrison LE, Brennan MF, Newman E, et al. Hepaticresection for noncolorectal, nonneuroendocrinemetastases: a fifteen-year experience with ninety-six patients. Surgery 1997;121:625–32.
78. Elias D, Cavalcanti de Albuquerque A, Eggenspieler P, etal. Resection of liver metastases from a noncolorectalprimary: indications and results based on 147 mono-centric patients. J Am Coll Surg 1998;187:487–93.
79. Foster JH. Survival after liver resection for secondarytumors. Am J Surg 1978;135:389–94.
80. Salmon RJ, Levy C, Plancher C, et al. Treatment ofliver metastases from uveal melanoma by combinedsurgery-chemotherapy. Eur J Surg Oncol 1998;24:127–30.
81. Penn I. Hepatic transplantation for primary and metasta-tic cancers of the liver. Surgery 1991;110:726–34.
67. Hughes KS, Simon R, Songhorabodi S, et al. Resectionof the liver for colorectal carcinoma metastases: amulti-institutional study of patterns of recurrence.Surgery 1986; 100: 278-84.
68. Schlag P, Hohenberger P, Herfarth C. Resection ofliver metastases in colorectal cancer: competitiveanalysis of treatment results in synchronous versusmetachronous metastases. Eur J Surg Oncol 1990;16: 360-5.
69. Rosen CB, Nagorney DM, Taswell HF, et al. Perioper-ative blood transfusion and determinants of survivalafter liver resection for metastatic colorectal carci-noma. Ann Surg 1992;216:493–504.
70. Gayowski TJ, Iwatsuki S, Madariaga JR. Experience inhepatic resection for metastatic colorectal cancer:analysis of clinical and pathologic risk factors. Surg1994;116:703–10.
71. Lehnert T, Knaebel HP, Duck M, et al. Sequentialhepatic and pulmonary resections for metastaticCRC. Br J Surg 1999;86:241–3.
72. DeMatteo RP, Minnard EA, Kemeny N, et al. Surgicalresection of both hepatic and pulmonary metastasesin patients with CRC. (submitted)
73. Steele GJ, Bleday R, Mayer RJ, et al. A prospectiveevaluation of hepatic resection for colorectal carci-noma metastases to the liver: GastrointestinalTumor Study Group Protocol 6584. J Clin Oncol1991;9:1105–12.



























![Liver resection for metastatic colorectal cancer - [email protected]](https://img.pdfslide.us/doc/110x75/620633768c2f7b1730055cf8/liver-resection-for-metastatic-colorectal-cancer-emailprotected.jpg)
