Embed Size (px)
Citation preview

72 Solitary lung nodule—Saraiva et al
Metastatic choroidal melanoma presenting as asolitary pulmonary nodule
Vinicius S. Saraiva,* MD; Abelardo A. Rodriguez-Reyes,* MD; Moy F. Chen,† MD;Eun Joo Park Saraiva,‡ MD; Miguel N. Burnier, Jr.,* MD, PhD, FRCSC
Uveal melanoma is the most common primaryintraocular tumour in adults. When metastatic dis-
semination occurs, the liver is the most frequent site ofinvolvement; the lungs are the next most frequent site.When lung metastasis occurs it is usually characterizedby numerous nodules. Isolated lung involvement isuncommon, and a solitary pulmonary nodule is anexceedingly rare presentation. To our knowledge, onlysix cases of metastatic choroidal melanoma presentingas a solitary pulmonary nodule have been previouslydescribed, of which four were treated with enucle-ation1–4 and two with plaque radiotherapy.5
CASE REPORT
A 48-year-old white man was referred with an asymp-tomatic peripapillary pigmented choroidal mass in hisright eye. Ultrasound examination showed a choroidaltumour measuring 10 mm by 6 mm by 2 mm withmedium to low internal reflectivity. Ten months later,follow-up ultrasound examinations revealed tumourgrowth (10 mm by 8 mm by 3 mm) associated withserous retinal detachment. Systemic evaluation was unre-markable. The patient was treated with proton beamradiotherapy (total dose 60 cobalt-gray equivalent).
There was no sign of tumour enlargement for thenext 6 years, after which tumour regrowth was diag-
nosed on ultrasonography (13 mm by 12 mm by3 mm). Uneventful enucleation was performed. Histo-pathological examination of the enucleated eyeshowed a mixed-cell-type choroidal melanoma withareas of necrosis and intrascleral and extraocular inva-sion (Fig. 1, left).
Four years later a solitary nodule measuring 15 mmin diameter in the superior lobe of the right lung wasincidentally discovered on chest radiography and wasconfirmed by computed tomography (Fig. 2). Thenodule was surgically resected, and the histopatholog-ical diagnosis was metastatic melanoma (Fig. 1, right).Immunohistochemical staining of the nodule gave pos-itive results for S-100 protein and HMB-45. No othersites of metastatic disease were found. Despite chemo-therapy (first with bryostatin and later with dacarba-zine), recurrent metastatic disease developed in theright hemithorax. There was extrinsic compression ofthe lower esophagus, leading to progressive dysphagiaand severe wasting. The patient died 16 months afterlung metastasis was initially diagnosed.
A complete autopsy was performed. There was noevidence of cutaneous malignant melanoma. The righthemithorax was completely replaced by metastaticuveal melanoma, and the overlying skin and subcuta-neous tissue of the lateral chest wall were involved, aswere the hilar lymph nodes. There were no othermetastatic sites.
COMMENTS
In comparison with the previously reported cases,1–5
the distinctive feature of our case is the initial treatmentwith proton beam irradiation. Furthermore, there was a6-year interval between radiotherapy and diagnosis oflocal recurrence, and a 10-year interval between radio-therapy and diagnosis of the metastatic lung nodule.
Failure of proton beam radiotherapy is uncommon.However, tumour-specific survival is known to be sub-stantially decreased in patients with recurrent uvealmelanoma after proton beam irradiation.6
In any patient with a solitary pulmonary nodule and
From *the Henry C. Witelson Ophthalmic Pathology Laboratoryand Registry and the Departments of †Pathology and ‡DiagnosticRadiology, McGill University, Montreal, Que.
Originally received Mar. 26, 2004Accepted for publication Sept. 3, 2004
Correspondence to: Dr. Vinicius S. Saraiva, Henry C. WitelsonOphthalmic Pathology Laboratory, Room 216, 3775 University St.,Montreal QC H3A 2B4; fax (514) 398-5728; [email protected]
This article has been peer-reviewed.
Can J Ophthalmol 2005;40:72–4

a previous history of malignant disease, it is of para-mount importance to rule out metastasis from theprimary site. Therefore, surgical resection should beperformed in order to obtain a definitive histopatho-logical diagnosis.7
Surgical removal of tumours metastatic to the lungoffers improved palliation and extended survival, par-ticularly in cases in which the pulmonary lesion is soli-tary and there is no extrathoracic disease.8 Kath andcolleagues9 found that the median survival of patientswith uveal melanoma who experienced metastasiswithout liver involvement was better than that ofpatients with liver involvement (19 versus 7 months).Aoyama and associates5 reported longer survival after
complete surgical removal of metastatic uveal mela-noma in selected patients, including two with a solitarylung nodule.
In conclusion, although rare, a solitary pulmonarynodule may be the first clinical manifestation ofmetastatic choroidal melanoma and may occur afterfailed proton beam radiotherapy.
REFERENCES
1. Reed RJ 3rd, Kent EM. Solitary pulmonary mela-nomas: two case reports. J Thorac Cardiovasc Surg1964;48:226–31.
2. Harada S, Kuwahara T, Kido M, Kajiki A, Ishikura Y,Koide O. Solitary pulmonary metastasis of choroidalmalignant melanoma: report of an unusual case.Endoscopy 1983;15(6):363–4.
3. Tishler M, Greif J, Topilsky M. Solitary pulmonarymetastasis of choroidal malignant melanoma simulat-ing primary lung cancer. Eur J Respir Dis 1986;68(3):215–7.
4. Keller H, Hacker R, Stolte M. [Simultaneous enucle-ation of a pulmonary melanoma metastasis andmyocardial revascularization.] Med Klin (Munich)1997;92(11):683–5.
5. Aoyama T, Mastrangelo MJ, Berd D, Nathan FE,Shields CL, Shields JA, et al. Protracted survival afterresection of metastatic uveal melanoma. Cancer2000;89(7):1561–8.
6. Egger E, Schalenbourg A, Zografos L, Bercher L,Boehringer T, Chamot L, et al. Maximizing localtumor control and survival after proton beam radio-therapy of uveal melanoma. Int J Radiat Oncol Biol
Solitary lung nodule—Saraiva et al
CAN J OPHTHALMOL—VOL. 40, NO. 1, 2005 73
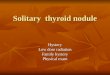
Fig. 1—Left: Photomicrograph of choroidal melanoma, showing (from top to bottom) degenerated overlying retina, peripapillarychoroidal melanoma, and intrascleral and extraocular invasion (hematoxylin–eosin; magnification ×25). Right: Photomicrograph ofsolitary pulmonary nodule, showing normal alveoli at top and replacement of lung parenchyma by metastatic choroidal melanomaat bottom (hematoxylin–eosin; magnification ×200).
Fig. 2—Axial computed tomography scan of chest, showingsolitary pulmonary nodule (black arrow).

Phys 2001;51(1):138–47.7. Ost D, Fein A. Evaluation and management of the
solitary pulmonary nodule. Am J Respir Crit Care Med2000;162(3 Pt 1):782–7.
8. Greelish JP, Friedberg JS. Secondary pulmonary ma-lignancy. Surg Clin North Am 2000;80(2):633–57.
9. Kath R, Hayungs J, Bornfeld N, Sauerwein W, HoffkenK, Seeber S. Prognosis and treatment of disseminateduveal melanoma. Cancer 1993;72(7):2219–23.
Key words: solitary pulmonary nodule, choroidal neo-plasm, melanoma
Solitary lung nodule—Saraiva et al
74 CAN J OPHTHALMOL—VOL. 40, NO. 1, 2005
IN THE NEXT ISSUE • DANS LE PROCHAIN NUMÉRO
IOP control in patients with glaucoma or ocular hypertension receiving treatment
Effect of the menstrual cycle on the optic nerve head in women with diabetes mellitus
Lymphoproliferative lesions of the lacrimal gland:clinicopathological, immunohistochemical and
molecular genetic analysis