Embed Size (px)
Citation preview

Metallic ion content and damage to the DNA in oral mucosa cellspatients treated dental implants
Pıa Lopez-Jornet • Francisco Parra Perrez •
Jose Luis Calvo-Guirado • Irene LLor-Ros •
Piedad Ramırez-Fernandez
Received: 24 December 2013 / Accepted: 19 March 2014 / Published online: 29 March 2014
� Springer Science+Business Media New York 2014
Abstract The aim of this study was to assess the potential
genotoxicity of dental implants, evaluating biomarkers of
DNA damage (micronuclei and/or nuclear buds), cytokinetic
defects (binucleated cells) and the presence of trace metals in
gingival cells of patients with implants, comparing these with
a control group. A total of 60 healthy adults (30 patients with
dental implants and 30 control patients without) were included
in the study. Medical and dental histories were made for each
including life-style factors. Genotoxicity effects were asses-
sed by micronucleus assays in the gingival epithelial cells of
each patient; 1,000 epithelial cells were analyzed, evaluating
the frequency of micronucleated cells and other nuclear
anomalies. The concentration of metals (Al27, Ag107, Co 59, Cr52, Cu63, Fe56, Sn118, Mn55, Mo92, Ni60, Pb208, Ti47) were
assayed by means of coupled plasma-mass spectrophotometry
(ICP-MS). The frequency of micronuclei in the patient group
with implants was higher than in the control group but without
statistically significant differences (P [ 0.05). Similar results
were found for binucleated cells and nuclear buds (P [ 0.05).
For metals assayed by ICP-MS, significant differences were
found for Ti47 (P B 0.045). Univariate analysis identified a
significant association between the presence of micronuclei
and age. Dental implants do not induce DNA damage in
gingival cells, the slight effects observed cannot be indicated
as biologically relevant.
1 Introduction
Dental implants restore patients’ oral health as well as
function, esthetics and comfort. The soft tissues sur-
rounding implants must adapt to their presence and peri-
odontal and peri-implant tissues are important for
establishing a protective barrier [1–3]. It has already been
documented in both in vitro and in vivo research that dental
metals can produce alterations in surrounding cells arising
mainly from corrosion [4–7]. The oral mucosa is covered
by a stratified epithelium composed of multiple layers of
cells that show various patterns of differentiation between
the deepest cell layer and the surface [8].
Biocompatibility is a fundamental requirement for the
success of dental implant treatments; the release of elements
from a biomaterial, whether this is through metal ions
released by alloy corrosion or peroxide degradation, is a
fundamental factor in the production of adverse biological
effects such as toxicity, allergy and mutagenicity [9–14].
Titanium is widely used in implant dentistry due to its
good physical, chemical and mechanical properties as well
as its resistance to corrosion [14–17]. Nevertheless, the oral
environment is an ideal medium for the biodegradation of
metals (pH variation, temperature, salivary conditions,
microbiological and enzymatic activity) and the release of
metal ions can cause a wide variety of biological responses.
However, understanding of the mechanisms of biological
interactions between metallic dental and oral or systemic
tissues remains limited [3, 7].
The Micronuclei test (MN) on human oral gingival cells
is a minimally-invasive and simple technique to detect
P. Lopez-Jornet � F. P. Perrez � I. LLor-Ros
Oral Medicine Department, Faculty of Medicine and Dentistry,
Ageing Research Institute, University of Murcia, Murcia, Spain
P. Lopez-Jornet (&)
Clınica Odontologica Universitaria, Hospital Morales Meseguer,
Adv. Marques de los Velez s/n, 30008 Murcia, Spain
e-mail: [email protected]
J. L. Calvo-Guirado � P. Ramırez-Fernandez
Department of Implant Dentistry, School of Medicine and
Dentistry, University of Murcia, Murcia, Spain
123
J Mater Sci: Mater Med (2014) 25:1819–1824
DOI 10.1007/s10856-014-5203-7

genotoxic damage. The MN in oral epithelial cells is being
used as a biomarker of exposure to genotoxic agents [18].
Some reports in the literature have shown that metal can
affect the close contact between implant and tissue. The
hypothesis of this study was that the titanium alloy used for
fabricating dental implants releases fewer metallic ions but
might nevertheless produce changes to the DNA of the oral
gingival mucosa. Olmedo et al. [10] measured the presence
of metal particles in cells exfoliated from peri-implant oral
mucosa around titanium dental implants; the concentration
of titanium was higher in patients with peri-implantitis.
The detection of metal ions in relation to genotoxic and
mutagenic effects has been studied in depth in vitro and in
animal studies [4, 16, 18], but in vivo research into metal
release in patients with dental implants and possible DNA
damage to gingival mucosa cells is scarce.
In this way, the aim of the present study was to assess
the potential genotoxicity of dental implants, evaluating
biomarkers of DNA damage (micronuclei and/or nuclear
buds), cytokinetic defects (binucleated cells) and the pre-
sence of metal particles in subjects with dental implants,
comparing these with a control group.
2 Materials and methods
The study protocol was designed and performed following
Spanish Ethical Guidelines and the Declaration of Helsinki
for research involving humans; it was approved by the
Bioethical Committee of the University of Murcia. All
subjects were fully informed of the purpose of the study
and gave their consent to take part.
This cohort study included 60 patients attending the
University of Murcia dental clinic. Thirty subjects were
selected consecutively who had received dental implants
more than one year previously without any associated
pathologies. A further 30 control subjects with the same
age and gender characteristics as the study group were
selected from the same local area. Medical and dental
histories were prepared including information about dietary
habits, alcohol consumption, smoking and exposure to
chemical carcinogens or radiation.
2.1 Inclusion criteria
Healthy subjects older than 18 years, in good general
health and without oral disease.
2.2 Exclusion criteria
The study excluded edentulous subjects, regular mouth-
wash users, taking antioxidant dietary supplements,patients
receiving local or systemic therapy or suffering any illness
(sensitivity to metals, oral lesions or ulcers, dental
pathologies, diabetics or subjects with a previous history of
cancer) or pregnant women. Subjects wearing complete
fixed or removable dental prostheses were also excluded, as
well as subjects with piercings, dental amalgams, previous
orthodontic treatment or with any clinical signs of mucosal
metallosis in the mucosa. None of the participants had
received radiological diagnosis during the six months prior
to sample collection.
2.3 Micronucleus assay technique [18–20]
(a) Cell Sampling and Preparation: Exfoliated oral
mucosal cells were collected from each subject by a
single practitioner (FP). According to the technique
proposed by Thomas et al. [18] in 2009 , the mouth
was rinsed with water to remove saliva, food particles
and any other debris prior to cell collection. Samples
were collected from the gingival margin of the sul-
cular epithelium with a conventional toothbrush,
applying a circular motion 20 times, covering a wide
area without damaging the gingival mucosa. Sample
sites for cell collection were uniform for all subjects.
Two 30-ml yellow-capped containers were prepared
containing 20 ml of gingival mucosal cell buffer
(EDTA 0.1 M, Tris–HCl 0.01 M, NaCl 0.02 M,
pH 7) (Sigma-Aldrich E6758, USA). The brushes
were placed in their respective buffer containers and
rotated repeatedly to dislodge the cells and release
them into the buffer medium. The cells were then
transferred to centrifuge tubes and centrifuged for
10 min. at 1,500 rpm. After centrifuging, the super-
natant was aspirated and the cells were resuspended in
another 5 ml of oral mucosal cell buffer, followed by
repeat centrifugation. The process was repeated once
again to eliminate bacteria and inactivate enzymes.
The cells were transferred using a pipette, placing
120–150 ll of cell suspension onto two clean and
labeled microscope slides. After drying, the slides
were placed in an oven at 55 �C for 15 min. and were
then fixed with 50 % methanol (Panreac SAU,
E-08211, Barcelona, Spain) at 0 �C for 15 min.
(b) DAPI Staining: Cell samples were stained with
DAPI (40,6-diamidino-2-phenylindole dihydrochlo-
ride) (Sigma-Aldrich, D9542, USA) at a concentra-
tion of 200 lg/ml, for 15 min. The slides were then
washed in Milli-Q water. Slides were scored using a
Leica DRMB fluorescence microscope equipped
with a DAPI band filter (excitation wavelength filter
set [BP340-380], dichroic filters RKP 400 and
emission filters LP 425) under 1009 magnifications.
(c) Scoring Method: Gingival buccal cell samples were
collected and processed following recommendations
1820 J Mater Sci: Mater Med (2014) 25:1819–1824
123
made by Thomas et al. [18] by a single practitioner
blinded to study group assignation.
Micronuclei, nuclear buds and other nuclear anomalies
were scored over 1,000 cells; they were identified by the
following characteristics:
Normal differentiated cells have a uniformly stained
nucleus and are distinguished from basal cells by their
larger size and by a smaller nucleus-to-cytoplasm ratio.
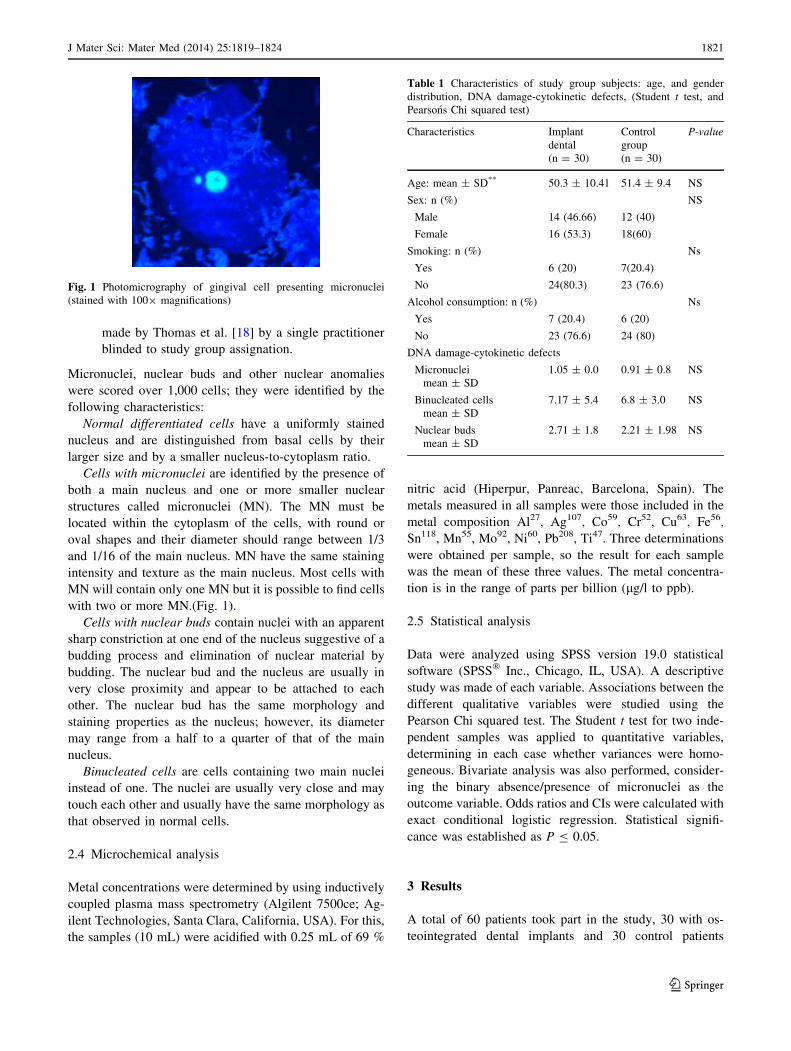
Cells with micronuclei are identified by the presence of
both a main nucleus and one or more smaller nuclear
structures called micronuclei (MN). The MN must be
located within the cytoplasm of the cells, with round or
oval shapes and their diameter should range between 1/3
and 1/16 of the main nucleus. MN have the same staining
intensity and texture as the main nucleus. Most cells with
MN will contain only one MN but it is possible to find cells
with two or more MN.(Fig. 1).
Cells with nuclear buds contain nuclei with an apparent
sharp constriction at one end of the nucleus suggestive of a
budding process and elimination of nuclear material by
budding. The nuclear bud and the nucleus are usually in
very close proximity and appear to be attached to each
other. The nuclear bud has the same morphology and
staining properties as the nucleus; however, its diameter
may range from a half to a quarter of that of the main
nucleus.
Binucleated cells are cells containing two main nuclei
instead of one. The nuclei are usually very close and may
touch each other and usually have the same morphology as
that observed in normal cells.
2.4 Microchemical analysis
Metal concentrations were determined by using inductively
coupled plasma mass spectrometry (Algilent 7500ce; Ag-
ilent Technologies, Santa Clara, California, USA). For this,
the samples (10 mL) were acidified with 0.25 mL of 69 %
nitric acid (Hiperpur, Panreac, Barcelona, Spain). The
metals measured in all samples were those included in the
metal composition Al27, Ag107, Co59, Cr52, Cu63, Fe56,
Sn118, Mn55, Mo92, Ni60, Pb208, Ti47. Three determinations
were obtained per sample, so the result for each sample
was the mean of these three values. The metal concentra-
tion is in the range of parts per billion (lg/l to ppb).
2.5 Statistical analysis
Data were analyzed using SPSS version 19.0 statistical
software (SPSS� Inc., Chicago, IL, USA). A descriptive
study was made of each variable. Associations between the
different qualitative variables were studied using the
Pearson Chi squared test. The Student t test for two inde-
pendent samples was applied to quantitative variables,
determining in each case whether variances were homo-
geneous. Bivariate analysis was also performed, consider-
ing the binary absence/presence of micronuclei as the
outcome variable. Odds ratios and CIs were calculated with
exact conditional logistic regression. Statistical signifi-
cance was established as P B 0.05.
3 Results
A total of 60 patients took part in the study, 30 with os-
teointegrated dental implants and 30 control patients
Fig. 1 Photomicrography of gingival cell presenting micronuclei
(stained with 1009 magnifications)
Table 1 Characteristics of study group subjects: age, and gender
distribution, DNA damage-cytokinetic defects, (Student t test, and
Pearsons Chi squared test)
Characteristics Implant
dental
(n = 30)
Control
group
(n = 30)
P-value
Age: mean ± SD** 50.3 ± 10.41 51.4 ± 9.4 NS
Sex: n (%) NS
Male 14 (46.66) 12 (40)
Female 16 (53.3) 18(60)
Smoking: n (%) Ns
Yes 6 (20) 7(20.4)
No 24(80.3) 23 (76.6)
Alcohol consumption: n (%) Ns
Yes 7 (20.4) 6 (20)
No 23 (76.6) 24 (80)
DNA damage-cytokinetic defects
Micronuclei
mean ± SD
1.05 ± 0.0 0.91 ± 0.8 NS
Binucleated cells
mean ± SD
7.17 ± 5.4 6.8 ± 3.0 NS
Nuclear buds
mean ± SD
2.71 ± 1.8 2.21 ± 1.98 NS
J Mater Sci: Mater Med (2014) 25:1819–1824 1821
123

without implants Their average age was 50.61 ±
6.15 years. Table 1 shows the characteristics of the two
groups.
In patients wearing implants, the average time since
implant placement was 2.6 ± 1.13 years. The average
number of implants per patient was three with a range of
one to ten. Micronuclei frequency (mean ± standard
deviation) per 1,000 gingival epithelial cells quantified for
each subject in the dental implant group was higher than
for control group subjects but without statistically signifi-
cant differences (P [ 0.05). Similar results were found for
binucleated cells and nuclear buds. (Table 1) (Fig. 1).
When the presence of metals was assayed by means of
ICP-MS, a significant difference was found between the
groups for titanium alloy, 2.42 ± 5.049 versus 0.461 ±
1.13 (P B 0.045) (Table 2).
Univariate analysis (Table 3) showed that age was sig-
nificantly associated with the presence of micronuclei in
the gingival epithelial (P = 0.048).
4 Discussion
Gingival epithelial cells are a useful target for biomoni-
toring due to their accessibility [19]; the micronucleus
(MN) assay is one of the most widely applied used in
genotoxicity studies and has become one of the most
important tests used for the evaluation of mutagenicity and
carcinogenicity [18, 19]. The results of the present study
were negative in that no statistically significant effect
relating to exposure to dental implants was observed on the
induction of MN and/or BN in the gingival epithelium. In
this way, the present study did not produce any evidence to
suggest that titanium alloy dental interventions increase
mutagenic and carcinogenic risks in humans.
The significance of binucleated cells remains uncertain,
though the phenomenon appears to indicate failed cytoki-
netics following the last step in nuclear division. The
binucleated/mononucleated cell ratio could be an important
biomarker indicating failed cytokinetics due to an increase
in aneuploid DNA rates [20, 21].
When considering DNA damage, factors such as sex,
age, smoking and alcohol consumption must be taken into
account [22–28]. According to Barnett and King [22], the
influence of age on genotoxic and cytotoxic endpoints may
reflect the increase in spontaneous chromosome instability
associated with an accumulation of DNA damage due to
progressive impairment of overall DNA-repair capacity.
Tissue repair capacity decreases with age and so the oral
mucosa becomes more permeable to nocive substances and
more vulnerable to damage produced by mechanical agents
[20]. In this way, the present results showed a significant
association between age and MN frequency.
Biomaterials used in dental medicine may release dif-
ferent cytotoxic elements that can cause toxic reactions,
allergy, mutagenic or inflammatory effects on cells [9, 29,
30](Fig. 2). The release of elements from a biomaterial,
whether from metal ions released through from alloy
Table 2 Concentration of metal ions (lg/l) detected in patients’
gingival cells: mean, standard deviation (SD)
Elements Implants (N = 30) Control (N = 30) P-value
Mean ± SD Mean ± SD
Al27 1.40 ± 2.2 1.390 ± 2.50 P [ 0.05
Ag107 0 .00 ± 0.0 0 .00 ± 0.0
Co59 0 ± 0 0 ± 0
Cr52 0.340 ± 0.31 0.010 ± 0.02 P [ 0.05
Cu63 0.160 ± 0.18 0.141 ± 0.14 P [ 0.05
Fe56 4.007 ± 3.96 3.570 ± 2.97 P [ 0.05
Sn118 0.001 ± 0.001 0.001 ± 0.001 P [ 0.05
Mn55 0.193 ± 0.16 0.187 ± 0.10 P [ 0.05
Mo92 0.004 ± 0.015 0 .001 ± 0.01 P [ 0.05
Ni60 0.106 ± 0.171 0.100 ± 0.03 P [ 0.05
Pb208 0.080 ± 0.062 0.019 ± 0.02 P [ 0.05
Ti47 2.42 0 ± 5.049 0.461 ± 1.13 0.0450
Table 3 Association with study subjects’ characteristics:Logistic
regression model for ‘‘presence of micronucleus/1,000 cells
gingival.’’
Variables Odds
ratio
95 % Confidence
interval
P-
value
Age (\50 vs. [50) 1.02 1.00–1.22 0.048
Sex (male vs. females) 1.32 0.61–1.90 0.150
Smoking (Yes/No) 1.74 0.29–3.69 0.670
Alcohol (Yes/NO) 0.09 0.01–1.85 0.303
Metal (Yes/No) 0.40 0.83–2.01 0.272
Year implant (\3
vs. [3)
2.6 0.61–2.10 0.122
Fig. 2 Failed human dental implant showing tissue in contact with
the metallic surface
1822 J Mater Sci: Mater Med (2014) 25:1819–1824
123

corrosion or from peroxide degradation, is fundamental to
the production of adverse biological effects such as toxic-
ity, allergy and mutagenicity. In an experimental study in
rat tibia, Piozzi et al. [13] observed an absence of cyto-
toxicity and genotoxicity from titanium. Thirty, 90, and
180 days after implantation, no statistically significant
differences in DNA damage were found in any study
groups, for any of the organs evaluated when compared
with the negative control group.
Flatebø, et al. [12] made a histological evaluation of
non-perforated mucosas covering maxillary submerged
titanium implants, finding no tissue sensitivity to the tita-
nium implants in spite of the fact that all the biopsies taken
at six months contained dense metal particles.
Olmedo et al. [10] measured the presence of metal
particles in cells exfoliated from peri-implant oral mucosas
around titanium dental implants. The concentration of
titanium was higher in the group of patients with peri-
implantitis compared to the group without peri-implantitis;
no traces of titanium were observed in control subjects.
In metal detection it should be remembered that in some
cases metal levels can be below the lower detection limit of
the instruments used for analysis; in other words, they are
present but undetectable. This may be the case even when the
ICP-MS technique is used, which can quantify parts per
billion. Furthermore, some titanium particles present in the
epithelium might not have anything to do with the implant
but originate from quite different sources. For example, TiO2
is widely used in food products, in toothpaste, prophylactic
pastes, etc. In vitro research has reported that various metal
elements such as Ni, Co and Cr can modulate immune
responses. Furthermore, human fibroblast and epithelial cell
cultures show that Cu, Co and Zn significantly increase
prostaglandin synthesis, a proinflammatory mediator
derived from arachidonic acid [14]. Nevertheless, while
in vitro tests are quick and simple and ensure controlled
laboratory conditions, they do not exactly reflect phenomena
occurring in the oral environment. In this way, actual oral
tissues might show the cumulative effects of metal release.
The results obtained in the present study correspond to
the data analyzed by Di Pietro et al. [31] who observed the
effects of dental restorative materials on peripheral blood
lymphocytes in patients with composite restorations com-
pared to those without restorations, whereby comet assay
results showed that DNA damage was two times higher in
the exposed group than in the control group. Furthermore,
DNA damage increased with the time of exposure and
number of restorations.
Soft tissues around teeth and implants present anatomic
similarities represented by the presence of an oral epithelium,
continuous with a junctional epithelium. The present study
assayed gingival cells in patients with natural teeth in good
periodontal health (control subjects) and gingival cells in
patients with dental implants (without mucositis or peri-im-
plantitis). Differences were observed in the positioning of the
most apical portion of the junctional epithelium, which in
tooth sections was close to the level of the cementoenamel
junction but in implant sections was at a variable distance from
the gingival margin. Another difference concerns the peri-
implantar absence of cementum layer or Sharpey’s fibers.
Consequently, collagen fiber bundles in teeth (dentogingival
fibers, dento-periodontal fibers and circular fibers) are inserted
perpendicular to the surface, while at implant sites, a dense
network of collagen fibers is observed extending from the
alveolar bone crest to the gingival margin, arranged parallel to
the implant surface [32]. Such anatomical variations should be
considered when contemplating the results of an assay such as
the present one, given that research involving gingival epi-
thelial cells in patients with implants is scarce and so it is
difficult to compare results.
There seems to be a consensus that, immediately fol-
lowing the placement of metals in the mouth, ion release
peaks as a result of corrosion, which is followed by sta-
bilization and a reduction in ion release due to the for-
mation of a protective biofilm over the metal surface [32].
For this reason, in order to assay accumulated DNA dam-
age, cytogenetic defects and trace metals, the present study
avoided the initial ion release peak period and assayed
responses during the stabilized phase.
Most studies have evaluated the metal ions in saliva [33,
34]. However, Mikulewicz and Chojnacka [35], in a system-
atic literature review, suggest that this procedure may have
limitations since the saliva is continuously washed and
swallowed and so will give information at the moment of
sampling only. For the purposes of the present study, it was
decided to use gingival mucosa cells since they are in direct
contact with implants and it has been reported that oral tissues
take up the metal ions released by an adjacent implant [29].
Given its design, the present study had certain limita-
tions and prospective studies with larger case numbers that
assay metal concentrations are needed to confirm findings.
It should also be remembered that metal degradation not
only alters the implants integral structure but brings about
systemic metal release. The microorganisms of the oral
flora must play an important role, which has not been
assayed in this study.
The method used for sample collection was simple, non-
invasive and well tolerated by the participants and so useful
for evaluating biomarkers of DNA damage and detecting
trace metals in gingival cells. Dental implants do not
induce DNA damage in gingival cells, the slight effects
observed cannot be indicated as biologically relevant.
Conflict of interest The authors declare no conflicts of interest
J Mater Sci: Mater Med (2014) 25:1819–1824 1823
123

References
1. Faggion CM Jr, Atieh MA, Park S. Search strategies in system-
atic reviews in periodontology and implant dentistry. J Clin Pe-
riodontol. 2013;40(9):883–8.
2. Sjostrom T. Brydone AS, Meek RM, Dalby MJ, Su B, McNamara
LE Titanium nanofeaturing for enhanced bioactivity of implanted
orthopedic and dental devices. Nanomedicine (Lond).
2013;8:89–104.
3. Louropoulou A, Slot DE, Van der Weijden FA. Titanium surface
alterations following the use of different mechanical instruments:
a systematic review Clin. Oral Impl Res. 2012;23:643–58.
4. Velasco-Ortega E, Jos A, Camean AM, Pato-Mourelo J, Segura-
Egea JJ. In vitro evaluation of cytotoxicity and genotoxicity of a
commercial titanium alloy for dental implantology. Mutation
Res. 2010;702:17–23.
5. Valko M, Morris H, Cronin MT. Metals, toxicity and oxidative
stress. Curr Med Chem. 2005;12:1161–208.
6. Simon M, Lagneau J, Moreno M, Lissac F, Dalard B. Grosgogeat
Corrosion resistance and biocompatibility of a new porous sur-
face for titanium implants Eur. J Oral Sci. 2005;113:537–45.
7. Ribeiro DA, Matsumoto MA, Padovan LE, Marques ME, Sal-
vadori DM. Genotoxicity of corrosion eluates obtained from
endosseous implants. Implant Dent. 2007;16:101–9.
8. Squier CA, Kremer MJ. Biology of oral mucosa and esophagus.
J Natl Cancer Inst Monogr. 2001;29:7–15.
9. Olmedo DG, Paparella ML, Spielberg M, Brandizzi D, Gug-
lielmotti MB, Cabrini RL. Oral mucosa tissue response to tita-
nium cover screws. J Periodontol. 2012;83(8):973–80.
10. Olmedo DG, Nalli G, Verdu S, Paparella ML, Cabrini RL. Ex-
foliative cytology and titanium dental implants: a pilot study.
J Periodontol. 2013;84:78–83.
11. Sicilia A, Cuesta S, Coma G, Arregui I, Guisasola C, Ruiz E,
Maestro A. Titanium allergy in dental implant patients: a clinical
study on 1500 consecutive patients. Clin Oral Impl Res.
2008;19:823–35.
12. Flatebø RS, Johannessen AC, Grønningsaeter AG, Bøe OE,
Gjerdet NR, Grung B, Leknes KN. Host response to titanium
dental implant placement evaluated in a human oral model.
J Periodontol. 2006;77:1201–10.
13. Piozzi R, Araki D, Marques LE, Nary H, Akemi M. Genotoxicity
and cytotoxicity in multiple organs induced by titanium mini-
plates in Wistar rats. J Biomed Mater Res. 2008;88:342–7.
14. Schmalz G, Garhammer P. Biological interactions of dental cast
alloys with oral tissues. Dent Mat. 2002;18:396–406.
15. ADA Council on Scientific Affairs. Titanium applications in
dentistry. J Am Dent Assoc. 2003;134:347–9.
16. Tomakidi P, Koke U, Kern R, Erdinger L, Kruger H, Kohl A,
et al. Assessment of acute cyto- and genotoxicity of corrosion
eluates obtained from orthodontic materials using monolayer
cultures of immortalized human gingival keratinocytes. J Orofac
Orthop. 2000;61:2–19.
17. Ortiz AJ, Fernandez E, Vicente A, Calvo JL, Ortiz C. Metallic
ions released from stainless steel, nickel-free, and titanium
orthodontic alloys: toxicity and DNA damage. Am J Orthod
Dentofac Orthop. 2011;140:e115–22.
18. Thomas P, Holland N, Bolognesi C, Kirsch-Volders M, Bonassi
S, Zeiger E, Knasmueller S, Fenech M. Buccal micronucleus
cytome assay. Nat Protoc. 2009;4:825–37.
19. Holland N, Bolognesi C, Kirsch-Volders M, Bonassi S, Zeiger E,
Knasmueller S, et al. The micronucleus assay in human buccal
cells as a tool for biomonitoring DNA damage: the HUMN
project perspective on current status and knowledge gaps. Mutat
Res. 2008;659:93–108.
20. Bonassi M, Fenech C, Lando YP, Lin M, Ceppi WP, Chang N,
et al. Human micronucleus project: international database com-
parison for results with the cytokinesis-block micronucleus assay
in human lymphocytes. I. Effect of laboratory protocol, scoring
criteria, and host factors on the frequency of micronuclei. Envi-
ron Mol Mutagen. 2001;37:31–45.
21. Sanchez-Siles M, Ros-Llor I, Camacho-Alonso F, Lopez-Jornet
P. A novel application of the buccal micronucleus cytome assay
in oral lichen planus: a pilot study. Arch Oral Biol. 2011;56:
1148–53.
22. Barnett YA, King CM. An investigation of antioxidants status,
DNA repair capacity and mutation as a function of age in
humans. Mutat Res. 1995;338:115–28.
23. Fenech M, Holland N, Zeiger E, Chang WP, Burgaz S, Thomas P,
Bolognesi C, Knasmueller S, Kirsch-Volders M, Bonassi S. The
HUMN and HUMNxL international collaboration projects on
human micronucleus assays in lymphocytes and buccal cells-past,
present and future. Mutagenesis. 2011;26:239–45.
24. Migliore L, Parrini M, Sbrana I, Biagini C, Battaglia A, Loprieno
N. Micronucleated lymphocytes in people occupationally
exposed to potential environmental contaminants: the age effect.
Mutat Res. 1991;256:13–20.
25. Milosevic-Djordjevic O, Grujicic D, Novakovic T, Arsenijevic S,
Marinkovic D. Micronuclei and ageing in a sample of Yugosla-
vian population. Russ J Genet (Genetika). 2002;37:201–4.
26. Fenech M, Chang WP, Kirsch-Volders M, Holland N, Bonassi S,
Zeiger E. HUMN project: detailed description of the scoring
criteria for the cytokinesis block micronucleus assay using iso-
lated human lymphocyte cultures. Mutat Res. 2003;534:65–75.
27. Bonassi S, Znaor A, Ceppi M, et al. An increase micronucleus
frequency in peripheral blood lymphocytes predicts the risk of
cancer in humans. Carcinogenesis. 2007;28:625–31.
28. Sarto F, Finotto S, Giacomelli L, Mazzotti D, Tomanin R, Levis
AG. The micronucleus assay in exfoliated cells of the human
buccal mucosa. Mutagenesis. 1987;2(1):11–7.
29. Garhammer P, Schmalz G, Hiller KA, Reitinger T. Metal content
of biopsies adjacent to dental cast alloys. Clin Oral Invest.
2003;7:92–7.
30. Baricevic M, Ratkaj I, Mladinic M, Zeljezic D, Kraljevic SP,
Loncar B, Stipetic MM. In vivo assessment of DNA damage
induced in oral mucosa cells by fixed and removable metal
prosthodontic appliances. Clin Oral Invest. 2012;16:325–31.
31. Di Pietro A, Visalli G, La Maestra S, Micale R, Baluce B,
Matarese G, Cingano L, Scoglio ME. Biomonitoring of DNA
damage in peripheral blood lymphocytes of subjects with dental
restorative fillings. Mutat Res. 2008;650:115–22.
32. Piatelli A, Scarano A, Piatelli M, Bertolai R, Panzoni E. Histo-
logic aspects of the bone and soft tissues surrounding three tita-
nium non-submerged plasma-sprayed implants retrieved at
autopsy: a case report. J Periodontol. 1997;68:694–700.
33. de Souza Matos. R, Macedo de Menezes L. Nickel, chromium
and iron levels in saliva of patients with simulated fixed ortho-
dontic appliances. Angle Orthod. 2008;78:345–50.
34. Eliades T, Trapalis C, Eliades G, Katsavarias E. Salivary metal
levels of orthodontic patients: a novel methodological and ana-
lytical approach. Eur J Orthod. 2003;25:103–6.
35. Mikulewicz M, Chojnacka K. Trace metal release from ortho-
dontic appliances by in vivo studies: a systematic literature
review. Biol Trace Elem Res. 2010;137:127–38.
1824 J Mater Sci: Mater Med (2014) 25:1819–1824
123








![Histological assessment of the palatal mucosa and greater ... · exposed root, alveolar ridge, or soft tissue around implants [2, 3]. Successful surgery depends on several factors,](https://img.pdfslide.us/doc/110x75/5e070bb6a07c0d7ce307230d/histological-assessment-of-the-palatal-mucosa-and-greater-exposed-root-alveolar.jpg)
![New Metallic Alloys Used for Dental Implants Manufacturing · realization of dental crowns, analogues implants (Fig. 6), dental bridges and implants [9]-[11]. TABLE II: MECHANICAL](https://img.pdfslide.us/doc/110x75/5f0acbe27e708231d42d62d3/new-metallic-alloys-used-for-dental-implants-realization-of-dental-crowns-analogues.jpg)



















