Embed Size (px)
DESCRIPTION
metabolisme lipid
Citation preview

PROGRAM KBKPROGRAM KBKFK-UKIFK-UKI
LIPID METABOLISM
Prof. Dr. drh. Maria Bintang, MSGURU BESAR BIOKIMIA

REFERENCESREFERENCES
Lehninger. 2000. Lehninger. 2000. Principles of biochemistryPrinciples of biochemistry 3 3rdrd Ed. Ed. Michael W. KingMichael W. King. 2006. . 2006. Medical BiochemistryMedical Biochemistry.. Murray R K, Granner D k, Mayers P a & Rodwell V w. Murray R K, Granner D k, Mayers P a & Rodwell V w.
2003. Harper’s Illustrated Biochemistry. 2003. Harper’s Illustrated Biochemistry. 2626th th Ed.Ed. Pratt,C.W.and Cornely K. 2004. Pratt,C.W.and Cornely K. 2004. Essential Essential
BiochemistryBiochemistry. Wiley International Edition.. Wiley International Edition. Stryer, Lubert 1995. Biochemistry.4Stryer, Lubert 1995. Biochemistry.4thth Ed. Sung Hee Um. 2004. The Role of S6K1 in
Development and Maintenance of Nutrient Homeostasis.[dessertation]. Basel.

Lipids Lipids Lipids include Lipids include oils, fatty acids, waxes, steroids oils, fatty acids, waxes, steroids
(such as (such as cholesterol cholesterol andand estrogen estrogen), and other related ), and other related compounds.compounds.
The functions of lipids areThe functions of lipids are::Fats (lipids) are an important source of energy Fats (lipids) are an important source of energy
for the body, as for the body, as ATP.ATP.Lipids are fat-like substances that are important Lipids are fat-like substances that are important
parts of the membranes found within and parts of the membranes found within and between each cell between each cell
IIn the n the myelin sheath myelin sheath that coats and protects the that coats and protects the nerves.nerves.

Adipocytes at the crossroads of energy homeostasisAdipocytes at the crossroads of energy homeostasis
Adipose tissue, which is the Adipose tissue, which is the main energy storage site, is main energy storage site, is responsive to both central and responsive to both central and peripheral metabolic signals peripheral metabolic signals by regulating lipid storage and by regulating lipid storage and mobilization. mobilization.
Dietary fat is absorbed Dietary fat is absorbed through the gastrointestinal through the gastrointestinal tract in the form of circulating tract in the form of circulating chylomicrons and very-low-chylomicrons and very-low-density lipoprotein (density lipoprotein (VLDLVLDL), ), part of which is metabolized part of which is metabolized to provide energy and the rest to provide energy and the rest of which enters the liver and of which enters the liver and adipose tissues for short- and adipose tissues for short- and long-term storage, long-term storage, respectively.respectively.

As a gauge of the level of energy reserves, adipose tissues secrete As a gauge of the level of energy reserves, adipose tissues secrete several adipokines, such as leptin, which regulates energy several adipokines, such as leptin, which regulates energy homeostasis by signalling to the brain and peripheral tissues. homeostasis by signalling to the brain and peripheral tissues.
Adipose tissues, through the lipolysis and re-esterification process, Adipose tissues, through the lipolysis and re-esterification process, are also the main sites for fatty-acid cycling, thereby securing the are also the main sites for fatty-acid cycling, thereby securing the energy supply to oxidative tissues, such as skeletal muscle and the energy supply to oxidative tissues, such as skeletal muscle and the heart. The liver has an important role as a homeostat for transient heart. The liver has an important role as a homeostat for transient energy fluctuation; it protects other tissues from energy fluctuation; it protects other tissues from POSTPRANDIAL TRIGLYCERIDAEMIA by temporarily storing by temporarily storing FAs from the circulation as a benign derivative, triacylglycerol FAs from the circulation as a benign derivative, triacylglycerol (TAG), (TAG), and secreting them as and secreting them as VLDLVLDL when the period of when the period of maximum lipid load has passed. maximum lipid load has passed.
The liver is also an important site for energy conversion, The liver is also an important site for energy conversion, exchanging energy sources from one form to another, such as exchanging energy sources from one form to another, such as glycogen to glucose, fatty acid to TAG and saturated fatty acid to glycogen to glucose, fatty acid to TAG and saturated fatty acid to unsaturated fatty acid. CNS, central nervous system. unsaturated fatty acid. CNS, central nervous system.

The process of dietary lipid digestion and absorptionThe process of dietary lipid digestion and absorption
triacylglycerol (TAG) phospholipids (PLs)FA-transport protein-4 (FATP4). Fatty acid transferase (FAT=CD36)bile salts (BS) lysophosphatidic acid (LPA) cholesterol (CL) intestinal FA-binding protein (IFABP)
FA-transport protein-4 (FATP4). glycerol-3-phosphate acyltransferase (GPAT) acyl-CoA:cholesterol acyltransferase (ACAT) cholesterol esters (CE).
chylomicrons (CM) microsomal triglyceride transfer protein (MTP),

A. Dietary lipid digestion begins in the stomach.A. Dietary lipid digestion begins in the stomach. Where lipids are subjected to partial digestion by gastric Where lipids are subjected to partial digestion by gastric lipaselipase
and form large fat globules with hydrophobic triacylglycerol and form large fat globules with hydrophobic triacylglycerol (TAG) cores surrounded by polar molecules, including (TAG) cores surrounded by polar molecules, including phospholipids (PLs), cholesterol (CL), fatty acids (FAs) and phospholipids (PLs), cholesterol (CL), fatty acids (FAs) and ionized proteins. ionized proteins.
The digestive processes are completed in the intestinal lumen, The digestive processes are completed in the intestinal lumen, where large emulsions of fat globules are mixed with bile salts where large emulsions of fat globules are mixed with bile salts (BS) and pancreatic juice containing lipid digestive enzymes to (BS) and pancreatic juice containing lipid digestive enzymes to form an aqueous suspension of small fatty droplets to maximize form an aqueous suspension of small fatty droplets to maximize exposure to the pancreatic exposure to the pancreatic lipaseslipases for lipid hydrolysis. for lipid hydrolysis.
Monoacylglycerol (MAG), diacylglycerol (DAG) and free FAs Monoacylglycerol (MAG), diacylglycerol (DAG) and free FAs that are released by lipid hydrolysis join BS, CL, that are released by lipid hydrolysis join BS, CL, lysophosphatidic acid (LPA) and fat-soluble vitamins to form lysophosphatidic acid (LPA) and fat-soluble vitamins to form mixed micelles that provide a continuous source of digested mixed micelles that provide a continuous source of digested dietary products for absorption at the brush-border membranes dietary products for absorption at the brush-border membranes of the enterocytes. of the enterocytes.

B. FAs and MAG enter the enterocytes by passive diffusion and are B. FAs and MAG enter the enterocytes by passive diffusion and are facilitated by transporters, such as intestinal FA-binding protein facilitated by transporters, such as intestinal FA-binding protein (IFABP), CD36 and FA-transport protein-4 (FATP4). (IFABP), CD36 and FA-transport protein-4 (FATP4). They are then re-esterified sequentially inside the They are then re-esterified sequentially inside the
endoplasmic reticulum by MAG acyltransferase (MGAT) and endoplasmic reticulum by MAG acyltransferase (MGAT) and diacylglycerol acyltransferase (DGAT) to form TAG. diacylglycerol acyltransferase (DGAT) to form TAG.
Phospholipids from the diet as well as bile - mainly LPA - are Phospholipids from the diet as well as bile - mainly LPA - are acylated by 1-acyl-glycerol-3-phosphate acyltransferase acylated by 1-acyl-glycerol-3-phosphate acyltransferase (AGPAT) to form phosphatidic acid (PA), which is also (AGPAT) to form phosphatidic acid (PA), which is also converted into TAG.converted into TAG.
Dietary CL is acylated by acyl-CoA:cholesterol Dietary CL is acylated by acyl-CoA:cholesterol acyltransferase (ACAT) to cholesterol esters (CE). acyltransferase (ACAT) to cholesterol esters (CE).
Facilitated by microsomal triglyceride transfer protein Facilitated by microsomal triglyceride transfer protein (MTP), TAG joins CE and apolipoprotein B (ApoB) to form (MTP), TAG joins CE and apolipoprotein B (ApoB) to form chylomicrons (CM) that enter circulation through the lymph chylomicrons (CM) that enter circulation through the lymph

Lipid storage and mobilization in adipocytesLipid storage and mobilization in adipocytes
lipoprotein lipase (LPL) acyl-CoA synthase (ACS)glycerol-3-phosphate acyltransferase (GPAT) MAG acyltransferase (MGAT). 1-acylglycerol-3-phosphate acyltransferase (AGPAT) diacylglycerol acyltransferase (DGAT). free fatty acids (FFAs) lipoprotein lipase (LPL) phosphatidic-acid phosphohydrolase (PAP) adipose differentiation-related protein (ADRP)perilipin (PER) tail-interacting protein of 47 kDa (TIP47)phosphate acyltransferase (PAT) hormone-sensitive lipase (HSL).protein kinase A (PKA) lysophosphatidic acid (LPA)

The main metabolic functions of adipose tissue are the accumulation of The main metabolic functions of adipose tissue are the accumulation of surplus energy through triacylglycerol (TAG) synthesis and deposition surplus energy through triacylglycerol (TAG) synthesis and deposition (lipogenesis), and lipid mobilization by releasing free fatty acids (FFAs) (lipogenesis), and lipid mobilization by releasing free fatty acids (FFAs) under conditions of negative energy balance (lipolysis). under conditions of negative energy balance (lipolysis).
FFAs that are released from lipoprotein — chylomicrons and very-low-FFAs that are released from lipoprotein — chylomicrons and very-low-density lipoprotein (VLDL) — catalysed by lipoprotein lipase (LPL) density lipoprotein (VLDL) — catalysed by lipoprotein lipase (LPL) enters the adipocytes through both passive diffusion and active enters the adipocytes through both passive diffusion and active transport. Intracellular FFA is first converted to acyl-CoA by acyl-CoA transport. Intracellular FFA is first converted to acyl-CoA by acyl-CoA synthase (ACS), and is then used as a substrate by two parallel TAG-synthase (ACS), and is then used as a substrate by two parallel TAG-synthetic pathways in the (ER). synthetic pathways in the (ER).
Glycerol-3-phosphate (G3P) that is generated by glucose metabolism is Glycerol-3-phosphate (G3P) that is generated by glucose metabolism is acylated sequentially by glycerol-3-phosphate acyltransferase (GPAT) acylated sequentially by glycerol-3-phosphate acyltransferase (GPAT) and sn-1-acylglycerol-3-phosphate acyltransferase (AGPAT), and and sn-1-acylglycerol-3-phosphate acyltransferase (AGPAT), and converted to diacylglycerol (DAG) by phosphatidic-acid converted to diacylglycerol (DAG) by phosphatidic-acid phosphohydrolase (PAP); by contrast, the alternative pathway involves phosphohydrolase (PAP); by contrast, the alternative pathway involves the acylation of monoacylglycerol (MAG) by MAG acyltransferase the acylation of monoacylglycerol (MAG) by MAG acyltransferase (MGAT). The two pathways merge with the acylation of DAG to TAG (MGAT). The two pathways merge with the acylation of DAG to TAG by diacylglycerol acyltransferase (DGAT). by diacylglycerol acyltransferase (DGAT).

Nascent lipid droplets that are generated from the ER are coated Nascent lipid droplets that are generated from the ER are coated by at least one of the PAT family proteins (which includes by at least one of the PAT family proteins (which includes perilipin (PER), adipose differentiation-related protein (ADRP) perilipin (PER), adipose differentiation-related protein (ADRP) and tail-interacting protein of 47 kDa (TIP47)) and S3-12, and tail-interacting protein of 47 kDa (TIP47)) and S3-12, whereas mature lipid drops are mainly coated with perilipin. whereas mature lipid drops are mainly coated with perilipin.
The mechanism by which other PAT proteins are replaced with The mechanism by which other PAT proteins are replaced with perilipin is unclear. The relative rate of lipogenesis and perilipin is unclear. The relative rate of lipogenesis and lipolysis is determined by nutritional states and is regulated by lipolysis is determined by nutritional states and is regulated by endocrine factors, such as catecholamines and insulin, which endocrine factors, such as catecholamines and insulin, which impose their effect by the phosphorylation of perilipin and impose their effect by the phosphorylation of perilipin and hormone-sensitive lipase (HSL).hormone-sensitive lipase (HSL).
The phosphorylation of perilipin allows HSL to access lipid The phosphorylation of perilipin allows HSL to access lipid droplets, which results in the hydrolysis of TAG to FFAs that droplets, which results in the hydrolysis of TAG to FFAs that are then released from the adipocytes. PA, phosphatidic acid; are then released from the adipocytes. PA, phosphatidic acid; PKA, protein kinase A; LPA, lysophosphatidic acid. PKA, protein kinase A; LPA, lysophosphatidic acid.

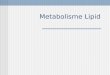
Interconnection of metabolic pathways involved in lipid synthesis in the endoplasmic Interconnection of metabolic pathways involved in lipid synthesis in the endoplasmic reticulum and lipid oxidation in mitochondria of liver and skeletal musclereticulum and lipid oxidation in mitochondria of liver and skeletal muscle
carnitine palmitoyl transferase (CPT) Stearoyl-CoA desaturase-1 (SCD1)acyl-carrier protein (ACP) acyl-CoA synthase (ACS)malonyl-CoA decarboxylase (MCD) phosphatidylglycerophosphate synthase (PGPS)acetyl-CoA carboxylase (ACC) fatty-acid synthase (FAS)

Among the lipid metabolic enzymes, acetyl-CoA Among the lipid metabolic enzymes, acetyl-CoA carboxylase (ACC), fatty-acid synthase (FAS) and carboxylase (ACC), fatty-acid synthase (FAS) and carnitine palmitoyl transferase (CPT) are the three main carnitine palmitoyl transferase (CPT) are the three main enzymes that regulate the synthesis of malonyl-CoA, enzymes that regulate the synthesis of malonyl-CoA, which is the principal inhibitor of fatty-acid entry into which is the principal inhibitor of fatty-acid entry into mitochondria for -oxidation. Stearoyl-CoA desaturase-mitochondria for -oxidation. Stearoyl-CoA desaturase-1 (SCD1) regulates lipid oxidation by converting stearic 1 (SCD1) regulates lipid oxidation by converting stearic acid (18:0) to oleic acid (18:1). acid (18:0) to oleic acid (18:1).
The saturated fatty acyl-CoAs are known to The saturated fatty acyl-CoAs are known to allosterically inhibit ACC1, whereas monounsaturated allosterically inhibit ACC1, whereas monounsaturated fatty acyl-CoAs are the preferred substrates for the lipid fatty acyl-CoAs are the preferred substrates for the lipid synthesis of triacylglycerol (TAG) in the endoplasmic synthesis of triacylglycerol (TAG) in the endoplasmic reticulum (ER). reticulum (ER).
Malonyl-CoA and stearic acid reciprocally regulate the Malonyl-CoA and stearic acid reciprocally regulate the entry of acyl-CoA into mitochondria by modulating the entry of acyl-CoA into mitochondria by modulating the activity of CPT. activity of CPT.

Lysophosphatidic acid (LPA) and phosphatidic acid (PA) are Lysophosphatidic acid (LPA) and phosphatidic acid (PA) are synthesized in the ER; they are also produced in mitochondria synthesized in the ER; they are also produced in mitochondria and transported to the ER where the terminal enzymes for and transported to the ER where the terminal enzymes for TAG synthesis are located. TAG synthesis are located.
Mitochondrial FAS (FAS II) and acyl-carrier protein (ACP) Mitochondrial FAS (FAS II) and acyl-carrier protein (ACP) are involved in fatty-acid synthesis, but their role in lipid are involved in fatty-acid synthesis, but their role in lipid metabolism remains elusive. metabolism remains elusive.
ACS, acyl-CoA synthase; AGPAT, acylglycerol-3-phosphate ACS, acyl-CoA synthase; AGPAT, acylglycerol-3-phosphate acyltransferase; CLS, cardiolipin (CL) synthase; DGAT, acyltransferase; CLS, cardiolipin (CL) synthase; DGAT, diacylglycerol (DAG) acyltransferase; GPAT, glycerol-3-diacylglycerol (DAG) acyltransferase; GPAT, glycerol-3-phosphate (G-3-P) acyltransferase; MCD, malonyl-CoA phosphate (G-3-P) acyltransferase; MCD, malonyl-CoA decarboxylase; MGAT, monoacylglycerol (MAG) decarboxylase; MGAT, monoacylglycerol (MAG) acyltransferase; PAP, phosphatidic-acid phosphohydrolase; acyltransferase; PAP, phosphatidic-acid phosphohydrolase; PGPS, phosphatidylglycerophosphate (PGP) synthase; TAG, PGPS, phosphatidylglycerophosphate (PGP) synthase; TAG, triacylglycerol; TCA, tricarboxylic-acid cycle.triacylglycerol; TCA, tricarboxylic-acid cycle.

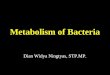
Pathways of lipid absorption and pooling within the enterocytePathways of lipid absorption and pooling within the enterocyte
monoglyceride (MG) glycerol-3 phosphate (G3P)
chylomicron (CM) smooth endoplasmic reticulum (SER)
rough endoplasmic reticulum (RER) lipoproteins (LPs)

Following uptake across the apical membrane of the enterocyte, Following uptake across the apical membrane of the enterocyte, the products of gastrointestinal (GI) lumen lipid digestion — the products of gastrointestinal (GI) lumen lipid digestion — monoglyceride (MG) and fatty acid (FA) — can either diffuse monoglyceride (MG) and fatty acid (FA) — can either diffuse across the enterocyte and enter the portal vein blood or be re-across the enterocyte and enter the portal vein blood or be re-synthesized to triglyceride (TG) by either the 2-monoglyceride synthesized to triglyceride (TG) by either the 2-monoglyceride (2-MG) pathway associated with the smooth endoplasmic (2-MG) pathway associated with the smooth endoplasmic reticulum (SER) or the a-glycerol-3 phosphate (G3P) pathway reticulum (SER) or the a-glycerol-3 phosphate (G3P) pathway associated with the rough endoplasmic reticulum (RER). associated with the rough endoplasmic reticulum (RER).
TG formed by these pathways typically enters the ER lumen and TG formed by these pathways typically enters the ER lumen and is assembled into lipoproteins (LPs; represented by orange is assembled into lipoproteins (LPs; represented by orange circles). circles).
LPs are then transported to the Golgi, exocytosed from the LPs are then transported to the Golgi, exocytosed from the enterocyte and taken up into the intestinal lymphatic system.enterocyte and taken up into the intestinal lymphatic system.
As lipid contained within the lipoprotein assembly pathways and As lipid contained within the lipoprotein assembly pathways and the Golgi is destined for transport to the systemic circulation by the Golgi is destined for transport to the systemic circulation by the intestinal lymphatic system, this pool of lipids is referred to the intestinal lymphatic system, this pool of lipids is referred to as the lymph lipid precursor pool.as the lymph lipid precursor pool.

A cytosolic poolA cytosolic pool of lipids of lipids is also located within the enterocyte. is also located within the enterocyte. This lipid pool comprises excess TG formed by the G3P pathway This lipid pool comprises excess TG formed by the G3P pathway and endogenous lipids taken up from the intestinal blood supply and endogenous lipids taken up from the intestinal blood supply in the form of either FA or chylomicron (CM) remnants. in the form of either FA or chylomicron (CM) remnants.
The cytosolic lipids are subject to hydrolysis by cytosolic lipase The cytosolic lipids are subject to hydrolysis by cytosolic lipase and the digestion products formed can be re-circulated into TG and the digestion products formed can be re-circulated into TG assembly pathways. However, the majority of lipids from this assembly pathways. However, the majority of lipids from this pool exit the enterocyte in the form of TG or free FA and are pool exit the enterocyte in the form of TG or free FA and are taken up into portal vein blood. taken up into portal vein blood.
The pool of lipids that is transported from the enterocyte by the The pool of lipids that is transported from the enterocyte by the portal vein is therefore referred to as the portal lipid precursor portal vein is therefore referred to as the portal lipid precursor pool (dashed red line). pool (dashed red line).
Recent evidence suggests that the trafficking and pooling of Recent evidence suggests that the trafficking and pooling of lipids within the enterocyte have a significant influence on the lipids within the enterocyte have a significant influence on the intracellular disposition of lipophilic drugs intracellular disposition of lipophilic drugs

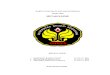
Schematic of Metabolic PPARß/δ Action
Enzymes and functions found to be activated by PPARß/δ peroxisome proliferator-activated receptor δ (PPARδ) agonist are marked in green. Red indicates inhibition of pathways. The green arrows underline FA uptake and oxidation, followedby uncoupling oxidation from ATP synthesis.
ABC : ATP-binding cassette transporter GLUT : Glucose transporterADRP : adipose differentiation-related protein SCD : Stearoyl-CoA desaturaseACS : acyl-CoA synthase CPT : carnitine palmitoyl transferasePDK : phosphoinositide-dependent protein kinase PDC : pyruvate dehydrogenase complexUCP : uncoupling protein GYG1 : glycogenin 1 FABP : Fatty acid binding protein MUFAs : monounsaturated fatty acid

The sequence of events postulated to occur during the development of dietinduced obesity and metabolic syndrome
Note: SREBP-1c: Sterol regulatory element binding protein-1c, also known as adipocyte determination and differentiation factor-1, ADD-1

Pathway for the movement of acetyl-CoA units from within the mitochondrion to the cytoplasm for use in lipid and cholesterol biosynthesis

mitokondria
cytosol














Lehninger. 2000Lehninger. 2000



CHOLESTEROLCHOLESTEROL Cholesterol is an extremely important biological Cholesterol is an extremely important biological
molecule that has roles in membrane structure as molecule that has roles in membrane structure as well as being a precursor for the synthesis of the well as being a precursor for the synthesis of the steroid hormones and bile acids. Both dietary and bile acids. Both dietary cholesterol and that synthesized cholesterol and that synthesized de novode novo are are transported through the circulation in transported through the circulation in lipoprotein particle
The synthesis and utilization of cholesterol must The synthesis and utilization of cholesterol must be tightly regulated in order to prevent over-be tightly regulated in order to prevent over-accumulation and abnormal deposition within the accumulation and abnormal deposition within the body. Of particular importance clinically is the body. Of particular importance clinically is the abnormal deposition of cholesterol and abnormal deposition of cholesterol and cholesterol-rich lipoproteins in the coronary cholesterol-rich lipoproteins in the coronary arteries. Such deposition, eventually leading to arteries. Such deposition, eventually leading to atherosclerosisatherosclerosis,, is the leading contributory factor is the leading contributory factor in diseases of the coronary arteries. in diseases of the coronary arteries.

Biosynthesis of Biosynthesis of CholesterolCholesterol

Regulating Cholesterol Regulating Cholesterol SynthesisSynthesis

Regulation of HMGR by covalent modification. HMGRRegulation of HMGR by covalent modification. HMGR ((HydroxymethylglutarylHydroxymethylglutaryl CoA reduktase CoA reduktase)) is most active in the is most active in the dephosphorylated state. dephosphorylated state. Phosphorylation is catalyzed by AMP-activated protein kinase, Phosphorylation is catalyzed by AMP-activated protein kinase, AMPK, (used to be termed HMG kinase), an enzyme whose activity AMPK, (used to be termed HMG kinase), an enzyme whose activity is also regulated by phosphorylation. is also regulated by phosphorylation. Phosphorylation of AMPK is catalyzed by AMPK kinase (AMPKK).Phosphorylation of AMPK is catalyzed by AMPK kinase (AMPKK).Hormones such as glucagon and epinephrine negatively affect Hormones such as glucagon and epinephrine negatively affect cholesterol biosynthesis by increasing the activity of the inhibitor of cholesterol biosynthesis by increasing the activity of the inhibitor of phosphoprotein phosphatase inhibitor-1, PPI-1. phosphoprotein phosphatase inhibitor-1, PPI-1. Conversely, insulin stimulates the removal of phosphates and, Conversely, insulin stimulates the removal of phosphates and, thereby, activates HMGR activity. thereby, activates HMGR activity. Additional regulation of HMGR occurs through an inhibition of its' Additional regulation of HMGR occurs through an inhibition of its' activity as well as of its' synthesis by elevation in intracellular activity as well as of its' synthesis by elevation in intracellular cholesterol levels.cholesterol levels. This latter phenomenon involves the transcription factor SREBP This latter phenomenon involves the transcription factor SREBP (sterol regulatory element binding proteins) described below. (sterol regulatory element binding proteins) described below.

Bile Acids Synthesis and UtilizationBile Acids Synthesis and Utilization The end products of cholesterol utilization are the bile acids, The end products of cholesterol utilization are the bile acids,
synthesized in the liver. Synthesis of bile acids is one of the synthesized in the liver. Synthesis of bile acids is one of the predominant mechanisms for the excretion of excess cholesterol. predominant mechanisms for the excretion of excess cholesterol. However, the excretion of cholesterol in the form of bile acids is However, the excretion of cholesterol in the form of bile acids is insufficient to compensate for an excess dietary intake of cholesterol.insufficient to compensate for an excess dietary intake of cholesterol.
Bile acids perform four physiologically significant functions: Bile acids perform four physiologically significant functions: 1.1. Their synthesis and subsequent excretion in the feces represent the Their synthesis and subsequent excretion in the feces represent the
only significant mechanism for the elimination of excess only significant mechanism for the elimination of excess cholesterol. cholesterol.
2.2. Bile acids and phospholipids solubilize cholesterol in the bile, Bile acids and phospholipids solubilize cholesterol in the bile, thereby preventing the precipitation of cholesterol in the thereby preventing the precipitation of cholesterol in the gallbladder. gallbladder.
3.3. They facilitate the digestion of dietary triacylglycerols by acting as They facilitate the digestion of dietary triacylglycerols by acting as emulsifying agents that render fats accessible to pancreatic lipases. emulsifying agents that render fats accessible to pancreatic lipases.
4.4. They facilitate the intestinal absorption of fat-soluble vitamins.They facilitate the intestinal absorption of fat-soluble vitamins.

Lipoprotein Lipoprotein A A lipoproteinlipoprotein is a biochemical assembly that contains both is a biochemical assembly that contains both
proteins and lipids. The lipids or their derivatives may be proteins and lipids. The lipids or their derivatives may be covalently or non-covalently bound to the proteins. covalently or non-covalently bound to the proteins.
Many enzymes, transporters, structural proteins, antigens, Many enzymes, transporters, structural proteins, antigens, adhesins and toxins are lipoproteins. Examples include the adhesins and toxins are lipoproteins. Examples include the high density and low density lipoproteins of the blood, the high density and low density lipoproteins of the blood, the transmembrane proteins of the mitochondrion and the transmembrane proteins of the mitochondrion and the chloroplast, and bacterial lipoproteins chloroplast, and bacterial lipoproteins
Lipoproteins in the blood, carry fats around the body. The Lipoproteins in the blood, carry fats around the body. The protein particles have charged groups aimed outward so as to protein particles have charged groups aimed outward so as to attract water molecules; this makes them soluble in the salt attract water molecules; this makes them soluble in the salt water based blood pool. water based blood pool.

Triglyceride-fats and cholesterol are carried internally, Triglyceride-fats and cholesterol are carried internally, shielded by the protein particle from the water.shielded by the protein particle from the water.
The interaction of the proteins forming the surface of the The interaction of the proteins forming the surface of the particles with (a) enzymes in the blood, (b) with each other particles with (a) enzymes in the blood, (b) with each other and (c) with specific proteins on the surfaces of cells and (c) with specific proteins on the surfaces of cells determinedetermine
TTriglycerides and cholesterol will be added to or removed riglycerides and cholesterol will be added to or removed from the lipoprotein transport particles.from the lipoprotein transport particles.

Classification Classification of Lipoproteinof Lipoprotein General categories of lipoproteins, listed in order from larger General categories of lipoproteins, listed in order from larger
and less dense (more fat than protein) to smaller and more and less dense (more fat than protein) to smaller and more dense (more protein, less fat): dense (more protein, less fat):
A.A. Chylomicrons - carry triacylgycerol (fat) from the Chylomicrons - carry triacylgycerol (fat) from the intestines to the liver and to adipose tissueintestines to the liver and to adipose tissue . .
B.B. Very low density lipoproteins - carry (newly synthesised) Very low density lipoproteins - carry (newly synthesised) triacylglycerol from the liver to adipose tissue. triacylglycerol from the liver to adipose tissue.
C.C. Intermediete density lipoproteins - are intermediate between Intermediete density lipoproteins - are intermediate between VLDL and LDL. They are not usually detectable in the VLDL and LDL. They are not usually detectable in the blood. blood.
D.D. Low density lipoproteins - carry cholesterol from the liver to Low density lipoproteins - carry cholesterol from the liver to cells of the body. Sometimes referred to as the "bad cells of the body. Sometimes referred to as the "bad cholesterol" lipoprotein. cholesterol" lipoprotein.
E.E. High density lipoproteins - collects cholesterol from the High density lipoproteins - collects cholesterol from the body's tissues, and brings it back to the liver. Sometimes body's tissues, and brings it back to the liver. Sometimes referred to as the "good cholesterol" lipoprotein referred to as the "good cholesterol" lipoprotein

A.A. Low-density lipoproteinLow-density lipoprotein ( (LDLLDL) ) • Its size is approx. 22 nm. Each native LDL particle contains Its size is approx. 22 nm. Each native LDL particle contains
a single apolipoprotein B-100 molecule (Apo B-100, a a single apolipoprotein B-100 molecule (Apo B-100, a protein with 4536 amino acid residues) that circles the fatty protein with 4536 amino acid residues) that circles the fatty acids keeping them soluble in the aqueous environmen acids keeping them soluble in the aqueous environmen
• Generally, LDL transports cholesterol and triglycerides from Generally, LDL transports cholesterol and triglycerides from the liver the liver
• Because LDLs transport cholesterol to the arteries and can Because LDLs transport cholesterol to the arteries and can be retained there by arterial proteoglycans starting the be retained there by arterial proteoglycans starting the formation of plaques, increased levels are associated with formation of plaques, increased levels are associated with atherosclerosis, and thus heart attack, stroke and peripheral atherosclerosis, and thus heart attack, stroke and peripheral vascular disease. This is why cholesterol inside LDL vascular disease. This is why cholesterol inside LDL lipoproteins is called lipoproteins is called ““badbad cholesterol cholesterol”. ”.

High concentrations of small LDL particles correlates with much faster growth of atheroma, progression of atherosclerosis and earlier and more severe cardiovascular disease events and death.
LDL is formed as VLDL lipoproteins lose triglyceride through the action of lipoprotein lipase (LPL) and become smaller and denser, containing a higher proportion of cholesterol.
A hereditary form of high LDL is familial hypercholesterolemia (FH). Increased LDL is termed hyperlipoproteinemia type II with symptom abdominal pain, enlarged liver, enlarged spleen, increased blood cholesterol, and LDL

LDL import to the cell When a cell requires cholesterol, it synthesises the
necessary LDL receptors, and inserts them into the plasma membrane. The LDL receptors diffuse freely until they associate with clathrin coated pits. LDL particles in the blood stream bind to these extracellular LDL receptors. The clathrin coated pits then form vesicles which are endocytosed into the cell.
After the clathrin coat is shed the vesicles deliver the LDL and their receptors to early endosomes, onto late endosomes to lysosomes. Here the cholesterol esters in the LDL are hydrolysed. The LDL receptors are recycled back to the plasma membrane

Recommended range; changing targetsRecommended range; changing targets. . The The American Heart Association, provide a set of guidelines for , provide a set of guidelines for fasting LDL-Cholesterol levels, estimated or measured, and fasting LDL-Cholesterol levels, estimated or measured, and risk for heart disease. As of 2003, these guidelines were:risk for heart disease. As of 2003, these guidelines were:
Borderlinehigh LDL level
High LDL level, corresponding to highestincreased risk of heart disease
> 4.9> 190Very
High LDL level4.1 to 4.9160 to 189
3.3 to 4.1130 to 159
Near optimal LDL level2.6 to 3.3100 to 129
Optimal LDL cholesterol, corresponding to reduced, but not zero, risk for heart disease
< 2.6< 100
InterpretationLevel mmol/LLevel (mg/dL)

B. B. High density lipoproteinHigh density lipoprotein
TTheir size (8–11 nm in diameter), that carry cholesterol heir size (8–11 nm in diameter), that carry cholesterol from the body's tissues to the liver. About thirty percent of from the body's tissues to the liver. About thirty percent of blood cholesterol is carried by HDL.blood cholesterol is carried by HDL.
It is hypothesised that HDL can remove cholesterol from It is hypothesised that HDL can remove cholesterol from atheroma within arteries and transport it back to the liver atheroma within arteries and transport it back to the liver for excretion or re-utilization—which is the main reason for excretion or re-utilization—which is the main reason why HDL-bound cholesterol is sometimes called why HDL-bound cholesterol is sometimes called "good "good cholesterol"cholesterol", or HDL-C. A high level of HDL-C seems to , or HDL-C. A high level of HDL-C seems to protect against cardiovascular diseases, and low HDL protect against cardiovascular diseases, and low HDL cholesterol levels (less than 40 mg/dL) increase the risk for cholesterol levels (less than 40 mg/dL) increase the risk for heart diseaseheart disease..
When measuring cholesterol, any contained in HDL When measuring cholesterol, any contained in HDL particles is considered as protection to the body's particles is considered as protection to the body's cardiovascular healthcardiovascular health..

Level mg/dLLevel mg/dL Level mmol/LLevel mmol/L InterpretationInterpretation
<40<40 < 1.03< 1.03 Low HDL cholesterol, heightened Low HDL cholesterol, heightened risk for heart disease, < 50 is the risk for heart disease, < 50 is the value for womenvalue for women
40–5940–59 1.03–1.521.03–1.52 Medium HDL levelMedium HDL level
>60>60 diseasedisease >1.55>1.55 High HDL level, optimal condition High HDL level, optimal condition considered protective against heartconsidered protective against heart
Recommended range. The American Heart Association, provides a set of guidelines for male fasting HDL levels and risk for heart disease.

Obesity Obesity ObesityObesity is a condition in which the natural energy reserve, is a condition in which the natural energy reserve,
stored in the fatty tissue of humans and other mammals, is stored in the fatty tissue of humans and other mammals, is increased to a point where it is associated with certain health increased to a point where it is associated with certain health conditions or increased mortality.conditions or increased mortality.
Although obesity is an individual clinical condition, it is Although obesity is an individual clinical condition, it is increasingly viewed as a serious and growing public health increasingly viewed as a serious and growing public health problem: excessive body weight has been shown to predispose problem: excessive body weight has been shown to predispose to various diseases, particularly cardiovascular diseases, to various diseases, particularly cardiovascular diseases, diabetes mellitus type 2, sleep apnea, and osteoarthritisdiabetes mellitus type 2, sleep apnea, and osteoarthritis
BMI, or body mass index, is a simple and widely used method BMI, or body mass index, is a simple and widely used method for estimating body fat. In epidemiology BMI alone is used as for estimating body fat. In epidemiology BMI alone is used as an indicator of prevalence and incidence.an indicator of prevalence and incidence.

BMI was developed by the Belgian statistician and BMI was developed by the Belgian statistician and anthropometrist Adoplhe Quetelet.It is calculated by anthropometrist Adoplhe Quetelet.It is calculated by dividing the subject's weight by the square of his/her dividing the subject's weight by the square of his/her height, typically expressed either in metric or US height, typically expressed either in metric or US “Customary” units:“Customary” units: Metric: Metric: BMIBMI = = kgkg / / mm
Where Where kgkg is the subject's weight in Kg and is the subject's weight in Kg and mm is the subject's height in metres.is the subject's height in metres.
US/Customary: US/Customary: BMIBMI = = lblb * 703 / * 703 / ininWhere Where lblb is the subject's weight in pounds and is the subject's weight in pounds and inin is the subject's height in inches. is the subject's height in inches.

BMI less than 18.5 is BMI less than 18.5 is underweightunderweight BMI of 18.5–24.9 is BMI of 18.5–24.9 is normal weightnormal weight BMI of 25.0–29.9 is BMI of 25.0–29.9 is overweightoverweight BMI of 30.0–39.9 is BMI of 30.0–39.9 is obeseobese BMI of 40.0 or higher is BMI of 40.0 or higher is severely (or morbidly) obeseseverely (or morbidly) obese BMI of 35.0 or higher BMI of 35.0 or higher in the presence of at least one in the presence of at least one
other other significant comorbiditysignificant comorbidity is also is also classified by classified by some odies as some odies as morbid obesmorbid obesityity
The current definitions commonly in use establish the following The current definitions commonly in use establish the following values, agreed in 1997 and published in 2000values, agreed in 1997 and published in 2000:

A large number of medical conditions have been associated with obesity:
Cardiovascular, congestive heart failure, enlarged heart
and its associated arrhythmias and dizziness, cor pulmonale, varicose veins, and pulmonary embolisme
Endocrine: polycystic ovarian syndrome (PCOS), menstrual disorders, and infertility
Gastrointestinal : gastroesophageal reflux disease (GERD), fatty liver disease, cholelithiasis (gallstones), hernia, and colorectal cancer
Renal and genitourinary : erectile dysfunction, urinary incontinence, chronic renal failure, hypogonadism (male), breast cancer (female), uterine cancer (female), stillbirth
Integument (skin and appendages): stretch marks, acanthosis nigricans, lymphedema, cellulitis, carbuncles, intertrigo

Musculoskeletal: hyperuricemia (which predisposes to gout), immobility, osteoarthritis, low back pain
NeurologicNeurologic: stroke, meralgia paresthetica, headache, carpal : stroke, meralgia paresthetica, headache, carpal tunnel syndrome, dementiatunnel syndrome, dementia
Respiratory : dyspnea, obstructive sleep apnea, Respiratory : dyspnea, obstructive sleep apnea, hypoventilation hypoventilation syndrome, Pickwickian syndrome, asthma syndrome, Pickwickian syndrome, asthma
Psycholoical : depressionPsycholoical : depression, low self esteem, body , low self esteem, body dysmorphic disorder, social stigmatizationdysmorphic disorder, social stigmatization
Causes and mechanisms Causes and mechanisms Lifestyle Lifestyle ((excessive nutrient intake)excessive nutrient intake) GeneticsGenetics ((genes controlling appetite, metabolism, and genes controlling appetite, metabolism, and
adipokine release predispose to obesity) adipokine release predispose to obesity) Medical illnessMedical illness ((hypothyroidism, Cushing’syndrome, hypothyroidism, Cushing’syndrome,
growth hormone deficiency)growth hormone deficiency) Social determinantsSocial determinants ((fast foodfast food))

TherapyTherapy, , In a In a clinical practice guideline by the by the American College of Physicians, the following five , the following five recommendations are madrecommendations are mad: :
People with a BMI of over 30 should be counseled on diet, People with a BMI of over 30 should be counseled on diet, exercise and other relevant behavioral interventions, and set exercise and other relevant behavioral interventions, and set a realistic goal for weight loss. a realistic goal for weight loss.
If these goals are not achieved, pharmacotherapy can be If these goals are not achieved, pharmacotherapy can be offered. The patient needs to be informed of the possibility offered. The patient needs to be informed of the possibility of side-effects and the unavailability of long-term safety and of side-effects and the unavailability of long-term safety and efficacy data. efficacy data.
Drug therapy may consist of sibutramine, orlistat, Drug therapy may consist of sibutramine, orlistat, phentermine, diethylpropion, fluoxetine, and bupropion. For phentermine, diethylpropion, fluoxetine, and bupropion. For more severe cases of obesity, stronger drugs such as more severe cases of obesity, stronger drugs such as amphetamine and methamphetamine may be used on a amphetamine and methamphetamine may be used on a selective basis. Evidence is not sufficient to recommend selective basis. Evidence is not sufficient to recommend sertraline, topiramate, or zonisamide. sertraline, topiramate, or zonisamide.

In patients with BMI > 40 who fail to achieve their weight In patients with BMI > 40 who fail to achieve their weight loss goals (with or without medication) and who develop loss goals (with or without medication) and who develop obesity-related complications, referral for bariatric surgery obesity-related complications, referral for bariatric surgery may be indicated. The patient needs to be aware of the may be indicated. The patient needs to be aware of the potential complications. potential complications.
Those requiring bariatric surgery should be referred to Those requiring bariatric surgery should be referred to high-volume referral centers, as the evidence suggests that high-volume referral centers, as the evidence suggests that surgeons who frequently perform these procedures have surgeons who frequently perform these procedures have fewer complications. fewer complications.

Lipid storage disorder Lipid storage disorder
The body's store of fat is constantly broken down and The body's store of fat is constantly broken down and reassembled to balance the body's energy needs with the food reassembled to balance the body's energy needs with the food available. available. Groups of specific enzymes help the body break down and Groups of specific enzymes help the body break down and process fats. Certain abnormalities in these enzymes can lead process fats. Certain abnormalities in these enzymes can lead to the buildup of specific fatty substances that normally would to the buildup of specific fatty substances that normally would have been broken down by the enzymes. have been broken down by the enzymes. Over time, accumulations of these substances can be harmful Over time, accumulations of these substances can be harmful to many organs of the body. to many organs of the body. Disorders caused by the accumulation of lipids are called Disorders caused by the accumulation of lipids are called lipidosis. Other enzyme abnormalities result in the body being lipidosis. Other enzyme abnormalities result in the body being unable to properly convert fats into energy. These unable to properly convert fats into energy. These abnormalities are called fatty acid oxidation disorders abnormalities are called fatty acid oxidation disorders

Lipid storage disorders (or lipidoses) are a group of inherited Lipid storage disorders (or lipidoses) are a group of inherited metabolic disorders in which harmful amounts of metabolic disorders in which harmful amounts of lipids lipids (fats) (fats) accumulate in some of the body’s accumulate in some of the body’s cells cells and tissues. and tissues. Types Lipid storage disorders Types Lipid storage disorders
Gauser diseaseGauser diseaseNiemann-Pick disease Niemann-Pick disease Fabry disease Fabry disease Farber’s disease Farber’s disease Gangliosidoses = Tay-Sachs diseaseGangliosidoses = Tay-Sachs disease Krabbé disease Krabbé disease Metachromatic leukodystrophy Metachromatic leukodystrophy Wolman’s disease Wolman’s disease

Gaucher diseaseGaucher disease Gaucher disease is the most common of the lipid storage Gaucher disease is the most common of the lipid storage
diseases. diseases. It is caused by a deficiency of the enzyme It is caused by a deficiency of the enzyme
glucocerebrosidase. glucocerebrosidase. Fatty material can collect in the spleen, liver, kidneys, lungs, Fatty material can collect in the spleen, liver, kidneys, lungs,
brain, and bone marrow.brain, and bone marrow. Gaucher disease has three common clinical subtypes: Gaucher disease has three common clinical subtypes:
o Type 1 (or nonneuropathic type) is the most common form of the Type 1 (or nonneuropathic type) is the most common form of the disease. It occurs most often among persons of Ashkenazi Jewish disease. It occurs most often among persons of Ashkenazi Jewish heritage. Symptoms may begin early in life or in adulthood and heritage. Symptoms may begin early in life or in adulthood and include enlarged liver and grossly enlarged spleen, which can rupture include enlarged liver and grossly enlarged spleen, which can rupture and cause additional complications. Skeletal weakness and bone and cause additional complications. Skeletal weakness and bone disease may be extensive. The brain is not affected, but there may be disease may be extensive. The brain is not affected, but there may be lung and, rarely, kidney impairment. Patients in this group usually lung and, rarely, kidney impairment. Patients in this group usually bruise easily and experience fatigue due to low blood platelets bruise easily and experience fatigue due to low blood platelets

o Type 2 (or acute infantile neuropathic Gaucher disease) typically Type 2 (or acute infantile neuropathic Gaucher disease) typically begins within 3 months of birth. Symptoms include an enlarged begins within 3 months of birth. Symptoms include an enlarged liver and spleen, extensive and progressive brain damage, eye liver and spleen, extensive and progressive brain damage, eye movement disorders, movement disorders, spasticity, , seizures, limb rigidity, and a poor , limb rigidity, and a poor ability to suck and swallow. Affected children usually die by age 2 ability to suck and swallow. Affected children usually die by age 2 platelets platelets
o Type 3 (the chronic neuronopathic form) can begin at any time in Type 3 (the chronic neuronopathic form) can begin at any time in childhood or even in adulthood. It is characterized by slowly childhood or even in adulthood. It is characterized by slowly progressive but milder neurologic symptoms compared to the acute progressive but milder neurologic symptoms compared to the acute or type 2 version. Major symptoms include an enlarged spleen or type 2 version. Major symptoms include an enlarged spleen and/or liver, seizures, poor coordination, skeletal irregularities, eye and/or liver, seizures, poor coordination, skeletal irregularities, eye movement disorders, blood disorders including anemia and movement disorders, blood disorders including anemia and respiratory problems. Patients often live to their early teen years respiratory problems. Patients often live to their early teen years and often into adulthood. and often into adulthood.
For type 1 and most type 3 patients, enzyme replacement For type 1 and most type 3 patients, enzyme replacement treatment given intravenously every two weeks can treatment given intravenously every two weeks can dramatically decrease liver and spleen size, reduce skeletal dramatically decrease liver and spleen size, reduce skeletal abnormalities, and reverse other manifestations. abnormalities, and reverse other manifestations.

Niemann-Pick disease Niemann-Pick disease Niemann-Pick disease is actually a group of autosomal is actually a group of autosomal
recessive disorders caused by an accumulation of fat and recessive disorders caused by an accumulation of fat and cholesterol in cells of the liver, spleen, bone marrow, cholesterol in cells of the liver, spleen, bone marrow, lungs, and, in some patients, brain, because of lungs, and, in some patients, brain, because of sphingomyelinase deficiency. sphingomyelinase deficiency.
Neurological complications may include ataxia,eye Neurological complications may include ataxia,eye paralysis, brain degeneration, learning problems, paralysis, brain degeneration, learning problems, spasticity, feeding and swallowing difficulties, slurred spasticity, feeding and swallowing difficulties, slurred speech, loss of muscle tone, hypersensitivity to touch, and speech, loss of muscle tone, hypersensitivity to touch, and some corneal clouding. some corneal clouding.
A characteristic cherry-red halo develops around the A characteristic cherry-red halo develops around the center of the retina in 50 % of patients. center of the retina in 50 % of patients.

Niemann-Pick disease is currently subdivided into four Niemann-Pick disease is currently subdivided into four categories:categories:
o Onset of type A, the most severe form, is in early infancy. Infants Onset of type A, the most severe form, is in early infancy. Infants appear normal at birth but develop an enlarged liver and spleen, appear normal at birth but develop an enlarged liver and spleen, swollen lymph nodes, nodes under the skin (xanthemas), and swollen lymph nodes, nodes under the skin (xanthemas), and profound brain damage by 6 months of age. The spleen may enlarge profound brain damage by 6 months of age. The spleen may enlarge to as much as 10 times its normal size and can rupture. These to as much as 10 times its normal size and can rupture. These children become progressively weaker, lose motor function, may children become progressively weaker, lose motor function, may become anemic, and are susceptible to recurring infection. They become anemic, and are susceptible to recurring infection. They rarely live beyond 18 months. This form of the disease occurs most rarely live beyond 18 months. This form of the disease occurs most often in Jewish families often in Jewish families
o type B (or juvenile onset), enlargement of the liver and spleen type B (or juvenile onset), enlargement of the liver and spleen characteristically occurs in the pre-teen years. Most patients also characteristically occurs in the pre-teen years. Most patients also develop ataxia, peripheral neuropathy, and pulmonary difficulties develop ataxia, peripheral neuropathy, and pulmonary difficulties that progress with age, but the brain is generally not affected. Type B that progress with age, but the brain is generally not affected. Type B patients may live a comparatively long time but many require patients may live a comparatively long time but many require supplemental oxygen because of lung involvement supplemental oxygen because of lung involvement

o Niemann-Pick disease types C and D are not caused by a Niemann-Pick disease types C and D are not caused by a deficiency of deficiency of sphlingomyelinasesphlingomyelinase but by a lack of the NPC1 or but by a lack of the NPC1 or NPC2 proteins. As a result, various lipids and cholesterol NPC2 proteins. As a result, various lipids and cholesterol accumulate inside nerve cells and cause them to malfunction. accumulate inside nerve cells and cause them to malfunction. Patients with types C and D have only moderate enlargement of Patients with types C and D have only moderate enlargement of their spleens and livers. Brain involvement may be extensive, their spleens and livers. Brain involvement may be extensive, leading to inability to look up and down, difficulty in walking and leading to inability to look up and down, difficulty in walking and swallowing, and progressive loss of vision and hearing.swallowing, and progressive loss of vision and hearing.Type D patients typically develop neurologic symptoms later than Type D patients typically develop neurologic symptoms later than those with type C and have a progressively slower rate of loss of those with type C and have a progressively slower rate of loss of nerve function. Most type D patients share a common ancestral nerve function. Most type D patients share a common ancestral background in Nova Scotia. The life expectancies of patients with background in Nova Scotia. The life expectancies of patients with types C and D vary considerably. Some patients die in childhood types C and D vary considerably. Some patients die in childhood while others who appear to be less severely affected live into while others who appear to be less severely affected live into adulthood. adulthood.

Fabry diseaseFabry disease Fabry disease, also known as , also known as alpha-galactosidase-A deficiency, causes a deficiency, causes a
buildup of fatty material in the autonomic nervous system, eyes, kidneys, buildup of fatty material in the autonomic nervous system, eyes, kidneys, and cardiovascular system and cardiovascular system
Fabry disease is the only x-linked lipid storage disease. Males are Fabry disease is the only x-linked lipid storage disease. Males are primarily affected although a milder form is common in females, some of primarily affected although a milder form is common in females, some of whom may have severe manifestations similar to those seen in affected whom may have severe manifestations similar to those seen in affected males. males.
Fatty storage in blood vessel walls may impair circulation, putting the Fatty storage in blood vessel walls may impair circulation, putting the patient at risk for patient at risk for stroke or or heart attack. Other symptoms include heart . Other symptoms include heart enlargement, progressive kidney impairment leading to enlargement, progressive kidney impairment leading to renal failure, , gastrointestinal difficulties, decreased difficulties, decreased sweating, and , and fever. . Angiokeratomas (small, non-cancerous, reddish-purple elevated spots on (small, non-cancerous, reddish-purple elevated spots on the skin) may develop on the lower part of the trunk of the body and the skin) may develop on the lower part of the trunk of the body and become more numerous with age become more numerous with age
Patients with Fabry disease often die prematurely of complications from Patients with Fabry disease often die prematurely of complications from heart disease, renal failure, or stroke. Drugs such as heart disease, renal failure, or stroke. Drugs such as phenytoin and and carbamazepine are often prescribed to treat pain that accompanies Fabry are often prescribed to treat pain that accompanies Fabry disease disease

Farber’s disease Farber’s disease, also known as Farber’s lipogranulomatosis or Farber’s disease, also known as Farber’s lipogranulomatosis or
ceramidase deficiency, describes a group of rare autosomal recessive ceramidase deficiency, describes a group of rare autosomal recessive disorders that cause an accumulation of fatty material in the joints, disorders that cause an accumulation of fatty material in the joints, tissues, and central nervous system tissues, and central nervous system
The disorder affects both males and females. Disease onset is typically The disorder affects both males and females. Disease onset is typically in early infancy but may occur later in life. Children who have the in early infancy but may occur later in life. Children who have the classic form of Farber’s disease develop neurological symptoms within classic form of Farber’s disease develop neurological symptoms within the first few weeks of life. These symptoms may include moderately the first few weeks of life. These symptoms may include moderately impaired mental ability and problems with swallowing. The liver, impaired mental ability and problems with swallowing. The liver, heart, and kidneys may also be affected. heart, and kidneys may also be affected.
Other symptoms may include vomiting, arthritis, swollen lymph nodes, Other symptoms may include vomiting, arthritis, swollen lymph nodes, swollen joints, joint contractures (chronic shortening of muscles or swollen joints, joint contractures (chronic shortening of muscles or tendons around joints), hoarseness, and xanthemas which thicken tendons around joints), hoarseness, and xanthemas which thicken around joints as the disease progresses. Patients with breathing around joints as the disease progresses. Patients with breathing difficulty may require insertion of a breathing tube. Most children with difficulty may require insertion of a breathing tube. Most children with the disease die by age 2, usually from lung disease. In one of the most the disease die by age 2, usually from lung disease. In one of the most severe forms of the disease, an enlarged liver and spleen severe forms of the disease, an enlarged liver and spleen (hepatosplenomegaly) can be diagnosed soon after birth. Children born (hepatosplenomegaly) can be diagnosed soon after birth. Children born with this form of the disease usually die within 6 months. with this form of the disease usually die within 6 months.

Krabbé disease Krabbé disease Krabbé disease (also known as globoid cell leukodystrophy and Krabbé disease (also known as globoid cell leukodystrophy and
galactosylceramide lipidosis) is an autosomal recessive disorder galactosylceramide lipidosis) is an autosomal recessive disorder caused by deficiency of the enzyme galactosylceramidase. caused by deficiency of the enzyme galactosylceramidase.
The disease most often affects infants, with onset before age 6 The disease most often affects infants, with onset before age 6 months, but can occur in adolescence or adulthood. The buildup of months, but can occur in adolescence or adulthood. The buildup of undigested fats affects the growth of the nerve’s protective myelin undigested fats affects the growth of the nerve’s protective myelin sheath and causes severe degeneration of mental and motor skills. sheath and causes severe degeneration of mental and motor skills.
Other symptoms include muscle weakness, hypertonia (reduced Other symptoms include muscle weakness, hypertonia (reduced ability of a muscle to stretch), myoclonic seizures (sudden, shock-ability of a muscle to stretch), myoclonic seizures (sudden, shock-like contractions of the limbs), spasticity, irritability, unexplained like contractions of the limbs), spasticity, irritability, unexplained fever, deafness, optic atrophy and blindness, paralysis, and fever, deafness, optic atrophy and blindness, paralysis, and difficulty when swallowing. Prolonged weight loss may also occur.difficulty when swallowing. Prolonged weight loss may also occur.
The disease may be diagnosed by its characteristic grouping of The disease may be diagnosed by its characteristic grouping of certain cells, nerve demyelination and degeneration, and destruction certain cells, nerve demyelination and degeneration, and destruction of brain cells. In infants, the disease is generally fatal before age 2. of brain cells. In infants, the disease is generally fatal before age 2. Patients with a later onset form of the disease have a milder course Patients with a later onset form of the disease have a milder course of the disease and live significantly longer. of the disease and live significantly longer.

Metachromatic leukodystrophy Metachromatic leukodystrophy Metachromatic leukodystrophyMetachromatic leukodystrophy, or MLD, is a group of disorders , or MLD, is a group of disorders
marked by storage buildup in the white matter of the central marked by storage buildup in the white matter of the central nervous system and in the peripheral nerves and to some extent in nervous system and in the peripheral nerves and to some extent in the kidneys the kidneys
Similar to Krabbé disease, MLD affects the myelin that covers Similar to Krabbé disease, MLD affects the myelin that covers and protects the nerves. This autosomal recessive disorder is and protects the nerves. This autosomal recessive disorder is caused by a deficiency of the enzyme arylsufatase A. Both males caused by a deficiency of the enzyme arylsufatase A. Both males and females are affected by this disorder. and females are affected by this disorder.
The most common form of the disease is late infantile, with onset The most common form of the disease is late infantile, with onset typically between 12 and 20 months following birth. Infants may typically between 12 and 20 months following birth. Infants may appear normal at first but develop difficulty in walking and a appear normal at first but develop difficulty in walking and a tendency to fall, followed by intermittent pain in the arms and tendency to fall, followed by intermittent pain in the arms and legs, progressive loss of vision leading to blindness, legs, progressive loss of vision leading to blindness, developmental delays, impaired swallowing, convulsions, and developmental delays, impaired swallowing, convulsions, and dementia before age 2. dementia before age 2.
Death generally occurs within 6 to 14 years after onset of Death generally occurs within 6 to 14 years after onset of symptoms.symptoms.

Wolman’s disease Wolman’s disease Wolman’s disease, also known as acid lipase deficiency, is Wolman’s disease, also known as acid lipase deficiency, is
a severe lipid storage disease that is usually fatal by age 1. a severe lipid storage disease that is usually fatal by age 1. This autosomal recessive disorder is marked by This autosomal recessive disorder is marked by accumulation of cholesteryl esters (normally a transport accumulation of cholesteryl esters (normally a transport form of cholesterol) and triglycerides (a chemical form in form of cholesterol) and triglycerides (a chemical form in which fats exist in the body) that can build up significantly which fats exist in the body) that can build up significantly and cause damage in the cells and tissues and cause damage in the cells and tissues
Both males and females are affected by this severe Both males and females are affected by this severe disorder. Infants are normal and active at birth but quickly disorder. Infants are normal and active at birth but quickly develop progressive mental deterioration, enlarged liver develop progressive mental deterioration, enlarged liver and grossly enlarged spleen, distended abdomen, and grossly enlarged spleen, distended abdomen, gastrointestinal problems including steatorrhea (excessive gastrointestinal problems including steatorrhea (excessive amounts of fats in the stools), jaundice, anemia, vomiting, amounts of fats in the stools), jaundice, anemia, vomiting, and calcium deposits in the adrenal glands, causing them to and calcium deposits in the adrenal glands, causing them to harden. harden.

Gangliosidoses = Tay-Sachs diseaseGangliosidoses = Tay-Sachs disease Tay-Sachs diseaseTay-Sachs disease (abbreviated (abbreviated TSDTSD, also known as , also known as
GM2 Gene map locusGM2 Gene map locus.. Hexosaminidase A deficiencyHexosaminidase A deficiency or or SphingolipidosisSphingolipidosis) is a genetic disorder, fatal in its ) is a genetic disorder, fatal in its most common variant known as most common variant known as Infantile Tay-Sachs Infantile Tay-Sachs diseasedisease. TSD is inherited in an autosomal recessive . TSD is inherited in an autosomal recessive pattern. The disease occurs when harmful quantities of a pattern. The disease occurs when harmful quantities of a fatty acid derivative called a ganglioside accumulate in fatty acid derivative called a ganglioside accumulate in the nerve cells of the brain. Gangliosides are lipids, the nerve cells of the brain. Gangliosides are lipids, components of cellular membranes, and the ganglioside components of cellular membranes, and the ganglioside GM2, implicated in Tay-Sachs disease, is especially GM2, implicated in Tay-Sachs disease, is especially common in the nervous tissue of the brain.common in the nervous tissue of the brain.

Tay-Sachs disease is a rare disease. Other Tay-Sachs disease is a rare disease. Other autosomal disorders such as cystic fibrosis and sickle autosomal disorders such as cystic fibrosis and sickle cell anemia are far more common. The importance of cell anemia are far more common. The importance of Tay-Sachs lies in the fact that an inexpensive enzyme Tay-Sachs lies in the fact that an inexpensive enzyme assay test was discovered and subsequently assay test was discovered and subsequently automated, providing one of the first "mass screening" automated, providing one of the first "mass screening" tools in medical genetics. tools in medical genetics.
Gangliosides are lipids, components of cellular Gangliosides are lipids, components of cellular membranes, and the ganglioside GM2, implicated in membranes, and the ganglioside GM2, implicated in Tay-Sachs disease, is especially common in the Tay-Sachs disease, is especially common in the nervous tissue of the brainnervous tissue of the brain..