Embed Size (px)
Citation preview

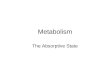
MetabolismFOOD
proteinssugars
fats
amino acids fatty acidssimple sugars(glucose)
muscle
proteins
liver
glycogen
fat
lipids
glucose
glucose glucose
glucose
glucose

Mammalian PancreasGall bladder
duodenum
liver
Bile Duct
Pancreas
Pancreatic duct
-Exocrine Pancreas: secretes digestive enzymes, alkaline pancreatic fluid
-Endocrine Pancreas: secretes hormones that regulate carbohydrate, lipid, and protein metabolism

Endocrine Pancreas
• Islets of Langerhans: 4 cell types cells: secrete glucagon cells: secrete insulin cells: secrete somatostatin
– F cells: secrete pancreatic polypeptide
Islets of Langerhans
Exocrine cells
capillaries

Pancreatic Hormones
• Insulin
• Glucagon
• Somatostatin

INSULIN• Regulation of Secretion
– Hyperglycemia stimulates release• Glucose sensors in cells
– Gastric Inhibitory Peptide• Released from cells of the small intestine
• Potent stimulator of insulin secretion
– Somatostatin: inhibits insulin release (paracrine)– Autonomic nervous system
• Parasympathetic activation increases insulin release
• Sympathetic activation blocks insulin release
• Epinephrine (from adrenal) blocks insulin release

INSULIN• Action at Target Tissues
– Activation of insulin receptor:• Increases transport of glucose, amino acids, and fatty
acids into cells
Glucose transporter:

INSULIN• Action at Target Tissues
– Activation of insulin receptor:• Increases transport of glucose (glucose transporter),
amino acids, and fatty acids into cells
– Enhancement of anabolic pathways, decrease in catabolic pathways
– Increases enzymes that activate:• Glycogen formation (liver)
• Lipogenesis (fat)
• Protein Synthesis (muscle)

Pancreatic Hormones
• Insulin– Hypoglycemic, glycogenic, lipogenic, anabolic
• Glucagon
• Somatostatin

Glucagon
• Hyperglycemic (increases plasma glucose)– (one of many in the body)
• Actions at target cells– Liver
• Promotes glycogenolysis
• Promotes gluconeogenesis
– Fat Tissue• Promotes lipolysis

Pancreatic Hormones
• Insulin– Hypoglycemic, glycogenic, lipogenic, anabolic
• Glucagon– Hyperglycemic, lipolytic
• Somatostatin– Paracrine agent– Believed to inhibit insulin and glucagon release– Inhibits digestion through several pathways

Glucose Regulation
Insulin: decreases blood glucose levels
Glucagon: increases blood glucose levels
Somatostatin: inhibits insulin and glucagon levels (paracrine) and
digestive processes

DIABETES MELLITUS
• Type 1—juvenile onset—insulin dependent– IDDM
– Underproduction of insulin
• Type 2—adult onset—non-insulin dependent– NIDDM
– Insulin receptor resistance
– Post-receptor mechanism problem

Type 1 DiabetesInsulin Dependent: IDDM
• Likely results from autoimmune reaction– The body’s immune system attacks the cells
• Pancreatic markedly reduced– Symptoms only appear after ~80% loss of cells
• No insulin……physiological repercussions?
• Treatment – Insulin injections or insulin pump– Recent methods

Islet Transplantation
Inside the patient
Separate islets from exocrine pancreasEncapsulate islets (immune protection)
Inject into liver portal veinhttp://diabetes.niddk.nih.gov/dm/pubs/pancreaticislet/

Type 2 Diabetes:Non-Insulin Dependent: NIDDM• Accounts for 90-95% of all Diabetes cases• Usually occurs in overweight individuals over 40
years of age– But ages are getting younger and younger– Associated with abdominal fat in women
• Target cells become resistant to insulin– insulin receptor
• Fewer receptors• Receptors have lower affinity• Receptor blocked (possibly by antibody)
– Post-receptor mechanisms

Diabetes Prevelence in US
%
Incidence of diagnosed diabetes
1980 1990 2000 2007

2007
2004
% of adults >20

New Cases in <20 yrs old

Type 2 Risks 2006
• 7th leading cause of death
• With Type 2 diabetes– 2 to 4-fold increase in heart disease related death– 2-fold risk of death
• Type 2 associated complications– 2-4 fold risk of stroke– 75% of adults with Type 2 have high blood pressure– leading cause of blindness in adults aged 20-74– Leading cause of kidney failure























![CITRIC ACID CYCLE [1] Organic fuels (glucose, amino acids, fats](https://img.pdfslide.us/doc/110x75/61fb3bf82e268c58cd5bc0d0/citric-acid-cycle-1-organic-fuels-glucose-amino-acids-fats.jpg)




