Embed Size (px)
Citation preview

39
1 Department of Nutritional Sciences and 3Department of Kinesiology, University of Connecticut, Storrs, Connecticut.
2 Department of Internal Medicine, Faculty of Medicine and Health Sciences, United Arab Emirate University, Al-Ain,
United Arab Emirates.
Metabolic Syndrome Prevalence, Dietary Intake, and Cardiovascular Risk Profile Among Overweight and Obese
Adults 18–50 Years Old From the United Arab Emirates
Taif Al-Sarraj, Ph.D.,1 Hussein Saadi, M.D.,2 Jeff S. Volek, Ph.D., R.D.,3 and Maria Luz Fernandez, Ph.D.1
Abstract
Background: The prevalence of diabetes mellitus is among the highest worldwide, and metabolic syndrome predisposes to diabetes.Methods: We recruited 227 overweight/obese Emirati adults living in the city of Al-Ain, Emirati of Abu Dhabi to screen for the metabolic syndrome and to assess for the most relevant criteria for the metabolic syndrome in this population. We identifi ed subjects as having the metabolic syndrome if they had three of the following charac-teristics: Waist circumference (WC) >88 cm in women and >102 cm in men; plasma glucose >5.5 mmol/L; blood pressure >130/85 mmHg, triglycerides (TG) >1.7 mmol/L, and high-density lipoprotein cholesterol (HDL-C) <1.0 mmol/L in men and <1.3 mmol/L in women. In addition to features of metabolic syndrome, lipoprotein subfractions and 24-hour dietary recalls were assessed in a random sample of participants.Results: A total of 92 subjects (40.5%) were classifi ed as having metabolic syndrome. The most relevant clinical criteria associated with metabolic syndrome were large WC, high blood pressure, and low HDL-C. Only 7% of subjects had TG >1.7 mmol/L, whereas 95% had plasma LDL-C >2.6 mmol/L. In addition, subjects presented low concentrations of medium very-low-density lipoprotein (VLDL) and small HDL subfractions in agreement with low concentrations of HDL-C and TG. Dietary analysis revealed high-energy consumption, with diets high in total carbohydrates, fat, and simple sugars. In addition, subjects were sedentary with only 14% of the popula-tion engaged in physical activity.Conclusions: The high prevalence of metabolic syndrome among overweight/obese Emirati adults predisposes this population to increased risk for developing diabetes and cardiovascular disease. Public health involvement targeting poor dietary habits and exercise programs among Emirati citizens is urgently needed.
Introduction
The obesity epidemic has led to a marked increase in the prevalence of the metabolic syndrome over the past two
decades.1 The metabolic syndrome is a clustering of metabolic
abnormalities characterized by abdominal obesity, dyslipi-demia (elevated apolipoprotein B [ApoB]), high triglyceride (TG) levels, elevated small, dense low-density lipoprotein (LDL) particles, low high-density lipoprotein-cholesterol (HDL-C) levels, hypertension, insulin resistance, hypergly-cemia, and a systemic proinfl ammatory state.2 The National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) report has identifi ed fi ve criteria for the
clinical diagnosis of metabolic syndrome. These include waist circumference (WC) >102 cm for men and >88 cm for women; TG ≥1.7 mmol/L (150 mg/dL); HDL-C <1.0 mmol/L (40 mg/dL) for men and <1.3 mmol/L (50 mg/dL) for women; blood pressure ≥130/85 mmHg; and fasting glucose ≥100 mg/dL. When three out of fi ve identifi ed characteristics are presented, a diagnosis of metabolic syndrome is made.2 Individuals with the metabolic syndrome, with or without insulin resistance, are at an increased risk for developing type 2 diabetes melli-tus (T2DM) and cardiovascular disease (CVD).3
The prevalence of T2DM in the United Arab Emirates (UAE) is considered one of the highest worldwide.4 It is
METABOLIC SYNDROME AND RELATED DISORDERSVolume 8, Number 1, 2010© Mary Ann Liebert, Inc.Pp. 39–46DOI: 10.1089/met.2009.0035
06_MET-2009_0035.indd 39 1/27/2010 5:08:03 PM

AL-SARRAJ ET AL.40
Technology students, in addition to random governmental schools and institutions in Al-Ain City. Exclusion criteria were non-UAE citizens, being younger than 18 or older than 50 years old, pregnancy and lactation, thyroid problems, use of medication relevant to T2DM and CVD, such as hypoglycemic agents or cholesterol-lowering medication, T2DM or fasting blood glucose greater than 126 mg/dL, stroke, or heart dis-ease. A total of 227 adult UAE citizens, were screened for met-abolic syndrome. All human protocols were approved by the Institutional Review Board of the University of Connecticut and the Human Research and Ethics Committee, Faculty of Medicine and Health Science, UAE University.
Physical examination and anthropometric measurement
After obtaining a consent agreement from each partici-pant, a 24-hour dietary record was recorded on random sub-jects by a hospital dietitian. In addition, a general physical activity questionnaire was obtained to determine type, time per session, and number of physical activities performed per week. Weight and height were measured using a profes-sional digital body composition analyzer scale/stadiometer (TANITA–Body Composition Analyzer TBF-215). Waist and hip circumference were measured using a fl exible tape over a loose single layer of light clothing due to cultural barriers. Blood pressure (systolic and phase-V diastolic) was measured on the right arm with subjects seated, after at least 10 min-utes rest, using a validated electronic sphygmomanometer (CRITICARE Systems, Inc. Model 506 DXNT2 series). Three separate recordings were made and the mean was used.
Diet analysis
A subset of subjects (13 men and 26 women) were given a 24-hour dietary recall by the same registered dietitian to assess energy intake, carbohydrate, fat, protein, fi ber, and cholesterol intake. Dietary recalls were analyzed using The Nutritional Data System 9.0 (Minneapolis, MN). Specifi c recipes and food preparation associated with UAE culture were included in the Data System for a more accurate dietary intake.
Laboratory measurements
After a 12-hour overnight fast, blood samples were col-lected from all participants for determination of lipid profi le and glucose. Fasting serum glucose was determined using the UniCel® DxC 600/800 System and SYNCHRON® Systems Multi Calibrator.10 Plasma cholesterol was assayed by a col-orimetric method.11 HDL-C was measured in human serum after precipitation of the ApoB-containing lipoproteins by centrifugation.12 LDL-C was measured by a direct homoge-neous assay, which solubilizes only the non-LDL lipoprotein particles and releases cholesterol to react with cholesterol esterase and cholesterol oxidase to produce a non-color-forming reaction. A second detergent solubilizes the remain-ing LDL particles, and a chromogenic coupler allows for color formation.10 TGs were measured by enzymatic methods.13
Lipoprotein subfractions and size
Hydrogen nuclear magnetic resonance (H-NMR) analy-sis was performed on a 400-MHz NMR analyzer (Bruker
unclear whether this is due to changes in lifestyle or genetic propensity or a combination of both. In 1971, the UAE was established as a federation of seven Emirates (or states) lo-cated on the Arabian Gulf and bordering Oman and Saudi Arabia. Since that time and along with the discovery of oil, the UAE has experienced a tremendously rapid urbaniza-tion that has transformed the country from a land of desert with minimal natural resources to a land of oil production, trading, and tourism. Accordingly, lifestyle and dietary hab-its have changed dramatically among Emirati citizens from a highly physical active lifestyle with less food and caloric intake to a sedentary lifestyle with much more food avail-ability and higher caloric intake.5 This has led to the devel-opment of obesity and diabetes among the UAE population.6 A national survey by the Emirates National Diabetes and Coronary Artery Disease Risk Factor (ENDCAD) reported that the prevalence of diabetes in the adult multiethinic pop-ulation of UAE is over 20%.7 Interestingly, the prevalence was higher among the Emirati population (24%) compared to non-Emirati (expatriates) population (17.4%).7 A more re-cent study by Saadi and co-researchers1 showed a T2DM prevelance of 24.5% among Emirati adults, whereas 18.5% had impaired glucose tolerance.8 These fi ndings place the UAE as the second country with the highest prevalence of diabetes in the world after Nauru.4
Metabolic syndrome is a major risk factor that predis-poses to T2DM. Recently, Malik and Razig9 evaluated for the fi rst time the prevalence of metabolic syndrome among the multiethnic population of the UAE using data from the 2000 ENDCAD Study. Their results indicate a prevalence of 39.6% among 4097 multiethnic men and women aged 20 and above using the ATP III criteria, and a rate of 40.5% using the International Diabetes Federation (IDF) defi nition. Among 729 Emirate citizens, the prevalence of metabolic syndrome was 42.4% according to ATP III criteria, and 41.8% accord-ing to IDF defi nition. The high prevalence of metabolic syn-drome was associated with increasing age (≥40 years old) but not with body mass index (BMI).9 These fi ndings prompted our interest in evaluating the prevalence of metabolic syn-drome among overweight and obese Emirati citizens resid-ing in the city of Al-Ain, one of the major cities located in the Emirate of Abu Dhabi.
The aim of this study was to screen overweight and obese adult Emirati citizens, aged 18–50 years, to determine the prevalence of metabolic syndrome and to assess the most relevant criteria associated with metabolic syndrome in this population. A second objective was to evaluate in more detail the contribution of lipoprotein subfractions to the distinctive plasma lipids characterized by high LDL-C, low HDL-C, and low TG in a subset of this population.
Materials and Methods
Study design and sampling
The study was conducted at Tawam hospital, one of the major tertiary hospitals in the UAE that is affi liated with Johns Hopkins Medicine International and the Faculty of Medicine and Health Sciences, UAE University.
Written and word-by-mouth advertisement for the met-abolic sydrome screening program was circulated among the hospital Emirati employees and their relatives, UAE University, and Faculty of Medicine and Higher College of
06_MET-2009_0035.indd 40 1/27/2010 5:08:04 PM

OBESITY, METABOLIC SYNDROME, AND HEART DISEASE RISK IN UAE 41
to the expected higher values for WC and blood pressure for those subjects with the metabolic syndrome, individuals classifi ed with the metabolic syndrome were older (P < 0.01), heavier (P < 0.01), and with a higher BMI (P < 0.01) com-pared to those overweight/obese subjects with no metabolic syndrome (Table 1). The percentage of obese subjects classi-fi ed with the metabolic syndrome was 91% compared to 61% in those individuals with no metabolic syndrome.
Both gender and metabolic syndrome signifi cantly mod-ulated plasma lipids in this population of overweight/obese Emirati subjects. Men had higher LDL-C (P < 0.05) and lower HDL (P < 0.01) compared to women, whereas plasma TG lev-els were higher in men compared to women only if there was no metabolic syndrome present (P < 0.01) (Table 1). Subjects classifi ed with metabolic syndrome had the expected higher TG and lower HDL-C and in addition had higher concen-trations of total cholesterol (P < 0.01) and LDL-C (P < 0.01) compared to those with no metabolic syndrome.
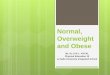
The most relevant ATP III clinical criteria associated with the metabolic syndrome in both men and women from the whole population of 227 subjects was large WC (60% of men and 70% of women), high systolic blood pressure (30% of men and 62% of women), and low HDL-C (75% of men and 62% of women) (Fig. 1A). Plasma TG concentrations were not a contributing factor for metabolic syndrome in this popu-lation because less than 10% of the subjects presented TG >150 mg/dL (1.7 mmol/L) (Fig. 1). In contrast, although not a criterion for metabolic syndrome, elevated LDL-C was present in almost all 227 subjects. Among overweight and obese individuals, there was a high percentage (35–40%) of subjects with total cholesterol higher than 5.6 mmol/L (Fig. 1B). In addition, 85–90% of the subjects had an LDL-C higher than 2.6 mmol/L, placing the majority of these subjects at very high risk for CVD (Fig. 1B)
We analyzed diet intake from a subgroup of subjects classifi ed with the metabolic syndrome (n = 13 men and 26 women) to determine caloric intake and diet composition of this population. Total energy intake was very high both for men (20,971 ± 5,466 kJ) and women (17,180 ± 5,138 kJ)
BioSpin Corp, Billerica, MA) as previously described.14 Briefl y, lipoprotein subclasses of different sizes produce a distinct lipid methyl signal whose amplitude is directly proportional to lipoprotein particle concentration. NMR simultaneously quantifi es >30 lipoprotein subclasses that are empirically grouped into nine smaller subclasses based on particle diameters: large very-large-density lipoprotein (VLDL) (35–60 nm), medium VLDL (27–35 nm), small VLDL (23–27 nm), large LDL (21.2–23 nm), medium LDL (19.8–21.2), small LDL (18–19.8 nm), large HDL (8.8–13 nm), medium HDL (8.2–8.8 nm), and small HDL (7.3–8.2 nm). Weighted average lipoprotein particle sizes in diameters were calcu-lated based on the diameter of each lipoprotein subclass multiplied by its respective relative concentration.
Statistical analysis
Two-way analysis of variance (ANOVA) (gender, meta-bolic syndrome) was used to analyze plasma lipids, glucose, and anthropometric parameters among men and women with or without metabolic syndrome. P < 0.05 was consid-ered statistically signifi cant. A subset of 39 samples (13 men and 26 women) was used to determine dietary intake and lipoprotein subfraction number and average size. An inde-pendent t-test was used to evaluate differences between men and women.
Results
Among 227 Emirati adults, 92 participants were diag-nosed with metabolic syndrome (7 overweight and 85 obese), with a prevalence of 40.5%. When comparisons were made between men and women with and without the met-abolic syndrome, signifi cant gender and group effects were found. Overall, men were younger (P < 0.01), heavier (P < 0.01), and had higher systolic blood pressure (P < 0.01) com-pared to women (Table 1). Interestingly women not classifi ed with the metabolic syndrome also had a high WC (93.9 ± 11.9 cm), whereas men did not (98.7 ± 10.9 cm). In addition
Table 1. Anthropometrics, Blood Pressure, and Plasma Lipids of 227 Overweight/Obese Men and Women From the United Arab Emirates With or Without Metabolic Syndrome
Parameter
No metabolic syndrome Metabolic syndrome P value
Men (n = 38)
Women(n = 96)
Men(n = 36)
Women(n = 57)
Gender effect
Metabolic syndrome effect
Age (years) 27.0 ± 8.5 30.9 ± 8.0 28.8 ± 8.9 33.7 ± 8.9 <0.01 <0.05Weight (kg) 91.8 ± 15.0 81.6 ± 15.0 108.3 ± 17.3 92.0 ± 16.4 <0.01 <0.01BMI (kg/m2) 32.2 ± 4.3 32.5 ± 5.7 37.6 ± 6.9 35.9 ± 5.7 <0.01 <0.01WC (cm) 98.7 ± 10.9 93.9 ± 11.9 113.0 ± 12.2 104.1 ± 11.5 <0.01 <0.01Systolic blood pressure (mmHg) 132.4 ± 11.9 122.0 ± 13.7 137.3 ± 10.8 134.6 ± 13.0 <0.01 <0.01Diastolic blood pressure (mmHg) 79.6 ± 9.3 77.4 ± 10.0 86.1 ± 9.5 84.0 ± 10.8 <0.01 <0.01TC (mmol/L) 5.37 ± 1.01 5.22 ± 0.77 5.66 ± 1.27 5.59 ± 0.94 NS <0.05LDL-C (mmol/L) 3.87 ± 0.91 3.63 ± 0.67 4.14 ± 1.00 3.92 ± 0.80 <0.05 <0.01HDL-C (mmol/L) 1.10 ± 0.23 1.28 ± 0.26 0.90 ± 0.14 1.07 ± 0.20 <0.01 <0.01TG (mmol/L) 0.91 ± 0.47 0.77 ± 0.48 1.09 ± 0.62 1.23 ± 0.83 <0.01 <0.01Glucose (mmol/L) 5.07 ± 0.50 5.04 ± 0.45 5.56 ± 0.52 5.49 ± 0.68 NS <0.01
Values are mean ± SD for the number of subjects indicated in parentheses.
Abbreviations: BMI, body mass index; WC, waist circumference; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol;
HDL-C, high-density lipoprotein cholesterol; TG, triglyceride; NS, not signifi cant; SD, standard deviation.
06_MET-2009_0035.indd 41 1/27/2010 5:08:04 PM

AL-SARRAJ ET AL.42
more grams/day of fat (P < 0.01) than women, although the consumption of both carbohydrate and protein was not dif-ferent between groups (Table 2). All subjects also had very high consumption of trans-fatty acids, dietary cholesterol, and dietary fi ber. Dietary intake was also very high in simple sugars and saturated fat. Mean intake of total sugars was 213 grams/day, whereas the mean energy contribution from sat-urated fat was 10.6% (Table 2). Fiber intake was also higher in men compared to women (P < 0.01). Most participants led a sedentary lifestyle and only a minority (14 subjects among 227) reported walking for 20–30 minutes at least once in the previous 1–2 weeks.
Pearson correlations were performed between BMI, age, and energy intake and the parameters of the meta-bolic syndrome. In men, BMI was signifi cantly and pos-itively correlated with WC, blood pressure, and LDL-C (Table 3), whereas in women all parameters of the meta-bolic syndrome were positively correlated with BMI except for HDL-C, which was negatively correlated (P < 0.01). Age also was a determinant of metabolic syndrome parameters. In men, age was positively correlated with systolic blood pressure, TG, and LDL-C (P < 0.01), whereas in women age was positively correlated with WC, TG, and LDL-C (Table 3). Although we only have diet records for 59 subjects, en-ergy intake was positively correlated with WC for both men (r = 0.768, P < 0.01) and women (r = 0.545, P < 0.01) (Table 3).
Regarding lipoprotein subclasses, no signifi cant differ-ences were found between men and women in the number of large, medium, or small VLDL subclasses (Table 4). Similarly, no signifi cant differences were observed in the number of the different LDL subclasses between men and women. However, subjects presented high concentrations of small LDL, characteristic of a more atherogenic lipid pro-fi le. In addition, women had more large and medium HDL particles compared to men (P < 0.05), whereas men had a higher number of the small HDL particles compared to
(Table 2) with men having a higher energy intake (P < 0.05). The consumption of carbohydrate, fat, and protein in grams/day was high both for men and for women. Men consumed
Perc
ent S
ubje
cts
0
0
20
40
60
80
100
WCcm
Total Overweight
Number of Subjects
Obese Metsyn
BPmmHg
Glucosemmol/L
TGmmol/L
HDLmmol/L
10203040506070
Men
LDL
Women
TC
80
A
B
FIG. 1. Percent of subjects with WC >88 cm for women and 102 cm for men; BP >130/85 mmHg; plasma glucose higher than 100 mg/dL (5.6 mmol/L); TGs higher than 150 mg/dL (1.7 mmol/L); and HDL-C <40 mg/dL (1.1 mmol/L) for men and <50 mg/dL (1.3 mmol/L) for women among the 227 overweight/obese Emirati subjects (A). Percent of total indi-viduals, those classifi ed as metabolic syndrome, overweight, or obese with total cholesterol >200 mg/dL (5.5 mmol/L) or LDL-C >100 mg/dL (2.6 mmol/L) (B). Abbreviations: BP, blood pressure; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TG, plasma trig-lycerides; WC, waist circumference.
Table 2. Total Energy, Fat, Carbohydrate, Protein, Dietary Cholesterol, and Dietary Fiber Intake Based on a 24-Hour Dietary Recall of a Randomly Selected Group of
Participants Classified With Metabolic Syndrome
Parameter Men (n = 13) Women (n = 26)
Total energy (Kjoules/day) 20971 ± 5466a 17180 ± 5138b
Total fat (grams/day) 207.5 ± 80.7a 150.1 ± 49.0b
Total fat (% energy) 36.3 ± 7.0 34.2 ± 7.9Saturated fat (% energy) 10.8 ± 2.5 10.5 ± 2.8Monounsaturated fat (% energy) 13.1 ± 3.7 12.0 ± 3.2Polyunsaturated fat (% energy) 9.6 ± 3.3 7.7 ± 2.3Trans-fatty acids (grams/day) 6.7 ± 4.7 4.0 ± 4.0Omega-3 fatty acids (grams/day) 3.1 ± 1.7a 2.0 ± 0.8b
Total carbohydrate (grams/day) 627.3 ± 139.2 549.7 ± 193.6Total sugars (grams/day) 224.4 ± 81.5 202.0 ± 73.4Carbohydrate (% energy) 50.7 ± 6.7 53.1 ± 7.3Total protein (grams/day) 175.5 ± 63.4 151.5 ± 46.3Protein (% energy) 14.1 ± 2.7 15.0 ± 2.7Dietary cholesterol (mg/day) 755.7 ± 428.7 667.8 ± 305.7Total fi ber (grams/day) 44.4 ± 18.0a 33.3 ± 14.3b
Soluble fi ber (grams/day) 10.1 ± 3.9a 6.7 ± 2.9b
Insoluble fi ber (grams/day) 34.7 ± 15.3a 25.4 ± 11.2b
Values are mean ± SD. Values in a row with different superscripts are signifi cantly different (P < 0.01).
Abbreviation: SD, standard deviation.
06_MET-2009_0035.indd 42 1/27/2010 5:08:04 PM

OBESITY, METABOLIC SYNDROME, AND HEART DISEASE RISK IN UAE 43
the population becomes older, the number of individuals with metabolic syndrome will increase. In other Arabian Gulf countries such as Saudi Arabia, a country bordering UAE that shares many similarities in terms of lifestyle and culture, the prevalence of metabolic syndrome among native Saudi popu-lation was 39.3%, which is almost similar to our fi ndings.16
The prevalence of metabolic syndrome has largely in-creased worldwide and it seems to be primarily due to obesity and sedentary lifestyle.2 The high prevalence of metabolic syndrome among this Emirati population could be explained by the high rate of obesity in the UAE that has increased over the past few decades.6,7 For example, in 1995, El-Mugamer et al.6 found an obesity prevalence of 27% among Emirati adults aged 20 and above. This prevalence increased to 37% in 2000.7 A similar fi nding was reported in 2004 among urban Emirati women, aged 19 and above, with a prevalence of 35%.17
women (P < 0.05) (Table 4). When lipoprotein subfraction size was analyzed, VLDL size was not different between men and women; both mean LDL and HDL size were larger in women compared to men (P < 0.05) (Table 4).
Discussion
Our results show a prevalence of 40.5% metabolic syn-drome among this sample of 227 overweight/obese urban Emirati adults aged 18–50 years. This prevalence is consis-tent with the 42.4% rate reported recently by Malik and Razig among Emirati adults of all ages9 and by Saadi et al.15 This high rate of metabolic syndrome may represent a strong pre-disposition for T2DM and CVD and may epitomize a signif-icant predictor of future health problems in this population. The positive correlation found between age and some of the parameters of metabolic syndrome clearly indicates that as
Table 3. Correlations Between Age, BMI, and Energy Intake and the Parameters of the Metabolic Syndrome and LDL-C For Men and Women
Parameter
BMI Age Energy
Men(n =64)
Women(n =153)
Men(n =64)
Women(n =153)
Men(n =13)
Women(n =36)
Waist circumference 0.818a 0.782a — 0.223a 0.768a 0.545a
Systolic blood pressure 0.286a 0.252a 0.225b NS NS NSDiastolic blood pressure 0.319a 0.235a NS NS NS NSHDL-C NS –0.525a NS NS NS NSTriglycerides NS 0.268a 0.328a 0.274a NS NSLDL-C 0.286a 0.172b 0.399a 0.180b NS NS
aSignifi cant at P < 0.01.bSignifi cant at P < 0.05.
Abbreviations: BMI, body mass index; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein
cholesterol; NS, not signifi cant.
Table 4. Number of VLDL, IDL, LDL, and HDL Particles According to Size in Men and Women Classified With Metabolic Syndrome
Parameter Men (n = 13) Women (n = 26)
VLDL diameter (nm) 46.5 ± 7.0 48.0 ± 6.4Total VLDL (mmol/L) 75 ± 31 81 ± 66Large VLDL (mmol/L) 2.4 ± 2.2 2.6 ± 2.2Medium VLDL (mmol/L) 20.6 ± 16.6 17.4 ± 3.4Small VLDL (mmol/L) 52.1 ± 19.2 45.6 ± 14.4IDL (mmol/L) 39.5 ± 33.3 45.1 ± 34.2LDL diameter (nm) 20.8 ± 0.7a 21.1 ± 0.4b
Total LDL (mmol/L) 1432 ± 405 1278 ± 390Large LDL (mmol/L) 426 ± 208a 488 ± 125b
Medium LDL (mmol/L) 193 ± 101 160 ± 79Small LDL (mmol/L) 767 ± 362 624 ± 294HDL diameter (nm) 8.5 ± 0.2a 8.9 ± 0.3b
Total HDL (mmol/L) 27.3 ± 4.4 28.8 ± 5.8Large HDL (mmol/L) 3.1 ± 1.3a 5.3 ± 2.1b
Medium HDL (mmol/L) 2.2 ± 2.6 4.4 ± 3.9Small HDL (mmol/L) 22.0 ± 3.1 19.0 ± 5.2
Values are mean ± SD. Values in a row with different superscripts are signifi cantly different (P < 0.01).
Abbreviations: VLDL, very-low-density lipoprotein; IDL, intermediate-density lipoprotein; LDL, low-
density lipoprotein; HDL, high-density lipoprotein.
06_MET-2009_0035.indd 43 1/27/2010 5:08:05 PM

AL-SARRAJ ET AL.44
with obesity and common in persons with insulin resistance, we were not surprised that high systolic blood pressure was a main common component of metabolic syndrome among these overweight and obese subjects. In contrast, high levels of fasting blood glucose were not an important component of the metabolic syndrome in this population.
Perhaps the most interesting fi nding in our study is the low plasma TG concentrations in these subjects. TG value was not a signifi cant contributing factor for the diagnosis of metabolic syndrome in this population. Mean plasma TG value for the whole population was 0.97 ± 0.63 mmol/L (85.5 ± 55.0 mg/dL), despite the fact that TG is inversely associated with low HDL-C and positively associated with elevated blood pressure.23 Only 7% of the 227 subjects had TG higher than 1.7 mmol/L (150 mg/dL). This could be an interesting area of research to study genetic factors and lipid profi les among the Emirati population.
Although not a criteria for the metabolic syndrome, LDL-C is one of the major risk factors for CVD.2 Our results show that 95% the 227 participants had LDL-C levels higher than 2.6 mmol/L (100 mg/dL), placing these subjects at high risk for CVD. The analysis of lipoprotein subfractions was used as a means to interpret the very distinctive lipoprotein profi le observed in overweight/obese young Emirati. One of the interesting fi ndings was that both men and women present lower concentrations of the medium VLDL particle compared to other reports in overweight14,24 and normal-weight subjects.25 In addition and relative to the observed high LDL-C, these subjects have a higher number of total LDL particles (12%), associated with the 21% higher num-ber of small LDL particles compared to Caucasian popula-tions.14,24,25 It is well known that smaller LDL particles are associated with an increased risk for coronary heart dis-ease.26 Thus, this Emirati population presents numerous risk factors that are associated with both heart disease and T2DM.
Interestingly, low HDL-C and the prevalence of small LDL particles are commonly associated with high plasma triglycerides.27 In T2DM, it is frequent to observe both low HDL-C and high plasma TG.28,29 Furthermore, a recent study in obese and normal-weight subjects demonstrated a strong correlation between Apo A-I catabolism and VLDL Apo B production rates.30 In other words, the removal of HDL from plasma leading to lower concentrations of HDL-C was associated with increased VLDL production or higher plasma TG. In contrast to all these reports, our population of overweight/obese Emirati presents high plasma LDL-C, increased small LDL, and low HDL-C in combination with low plasma TG. A recent report in mice lacking the enzyme stearoyl coenzyme A (CoA) desaturare indicated that in spite of low plasma TG these animals possessed abnormally low HDL.31 It is possible that a genetic polymorphism could be responsible for this unusual lipoprotein profi le that in spite of the low plasma TG is highly atherogenic and predisposes to T2DM. These fi ndings warrant further investigation.
Limitations
This is a unicenter study conducted in the city of Al-Ain only. The prevalence of metabolic syndrome may not be well representative of all eligible Emirati citizens in Al-Ain. Furthermore, results from Emirati citizens living in Al-Ain City may not be typical for all cities or Emirates (states) in
Another explanation for the high prevalence of metabolic syndrome is the unique fi nding of the high daily energy in-take (~18,000 kJ/day), elevated carbohydrate consumption (mainly sugar), and total fat that may have led to overweight and obesity status among this population and therefore to metabolic syndrome, as suggested by the strong correla-tion between energy intake and WC in the subset sample of men and women. It becomes obvious that robust dietary interventions18,19 need to be prescribed to these Emirati sub-jects to avoid major future public health problems.
The high rate of metabolic syndrome amid this popula-tion can also be due to lack of physical activity Only 14 sub-jects (6%) reported occasional walking of 20–30 minutes at either work place or neighborhood area, yet this was not part of a scheduled or routine physical activity program. Similar fi ndings were recently reported regarding minimal physical activities among the Emirati population.9 In a cross-sectional survey using a self-administered questionnaire among 175 medical male and female students aged 19–27 years, who were studying at the faculty of medicine and health science of UAE University, 77% believed their activity levels were insuffi cient and 33% were not active enough to meet min-imal recommended level.20 Among those who felt that they did not get enough activity levels, 75% referred it to lack of time and 17% referred it to poor motivation. In contrast, a more recent cross-sectional survey on 553 urban Emirati women aged 19 and above showed that 84% of 460 women reported they were suffi ciently active to meet the export recommendations.17 However, errors of self-reporting vari-able could be a limitation of this survey because the study reported a very high rate of obesity (35%) in this population, particularly young women (20–29 years old) with a rate of 21%. In addition to the poor dietary habits and low physical activity, the high prevalence of metabolic syndrome among native Emirati subjects may be due to other key aspects that remain unknown in this population, such as genetic suscep-tibility and the interaction between genes and environmen-tal factors.21
Our fi ndings indicate that the clinical criteria contribut-ing most to metabolic syndrome, as defi ned by ATP III, in both men and women were large WC (mean 107.4 ± 12.5 cm), high systolic blood pressure (135.8 ± 12.1 mmHg), and low HDL-C (1.0 ± 0.2 mmol/L). According to ATP III, abdomi-nal obesity has been well recognized as an underlying risk factor in the defi nition of metabolic syndrome.2 Central adipose tissue correlates with other metabolic risk factors (e.g., insulin resistance, proinfl ammatory and prothrom-botic states) through their production of nonesterifi ed fatty acids (NEFA), cytokines, plasminogen activator inhibitor-1 (PAI-1), and adiponectin.2 On the other hand, HDL-C has been considered as a major risk factor for the defi nition of metabolic syndrome.2 Our results are consistent with other studies in UAE and other Gulf-region countries. Larger WC and low HDL-C were the two major contributors to meta-bolic syndrome among the multiethnic population of UAE.9 In a study among the Saudi Arabian population, Al-Nozha et al.16 reported that low HDL-C was the factor contributing most to metabolic syndrome, regardless of the age groups. Furthermore, in Oman, another country bordering the UAE, Al-Lawati et al.22 addressed the two most common criteria for the defi nition of metabolic syndrome among 1419 Omani adults aged ≥20 years to be low HDL-C (75.4%) followed by WC (24.6%). Because blood pressure is strongly associated
06_MET-2009_0035.indd 44 1/27/2010 5:08:05 PM

OBESITY, METABOLIC SYNDROME, AND HEART DISEASE RISK IN UAE 45
8. Saadi H, Carruthers SG, Nagelkerke N, Al-Maskari F, Afandi B,
Reed R, Lukic M, Nicholls MG, Kazam E, Algawi K, Al-Kaabi
J, Leduc C, Sabri S, El-Sadig M, Elkhumaidi S, Agarwal M,
Benedict S. Prevalence of diabetes mellitus and its complica-
tions in a population-based sample in Al Ain, United Arab
Emirates. Diabetes Res Clin Pract 2007;78:369–377.
9. Malik M, Razig SA. The Prevalence of the Metabolic Syndrome
among the Multiethnic Population of the United Arab Emirates.
Metab Syndr Relat Disord 2008;6:177–186.
10. Centers for Disease Control and Prevention. A proposed
method for determining glucose using hexokinase and glucose
6-phosphatase dehydrogenase. Public Health Service. Centers
for Disease Control and Prevention, 1976.
11. Allain CC, Poon LS, Chan CSG, Richmond W, Fu PC.
Enzymatic determination of total Serum cholesterol. Clin Chem
1974;20:470–475.
12. Assmann G, Schriewer H, Schmitz G, Hagele EO. Quantifi cation
of high density lipoprotein cholesterol by precipitation with
phosphotungstic acid/MgCl2. Clin Chem 1983;29:2026.
13. Bucolo G, Yabut J, Chang TY. Mechanical enzymatic determina-
tion of triglycerides in serum. Clin Chem 1975;21:420–424.
14. Wood RJ, Volek JS, Liu Y, Shachter NS, Contois JH, Fernandez
ML. Carbohydrate restriction alters lipoprotein metabolism by
modifying VLDL, LDL and HDL subfraction distribution and
size in overweight men. J Nutr 2006;136:384–389.
15. Saadi H, Nagelkerke N, Carruthers SG, Benedict S, Abdulkhalek
S, Reed R, Lukic M, Nicholls MG. Association of TCF7L2 poly-
morphism with diabetes mellitus, metabolic syndrome, and
markers of beta cell function and insulin resistance in a popu-
lation-based sample of Emirati subjects. Diabetes Res Clin Pract 2008;80:392–398.
16. Al-Nozha M, Al-Khadra A, Arafah MR, Al-Maatouq MA,
Khalil MZ, Khan NB, Al-Mazrou YY, Al-Marzouki K, Al-Harthi
SS, Abdulla M, Al-Shahib MS, Al-Mobeireek A, Nouh MS.
Metabolic syndrome in Saudi Arabia. Saudi Med J 2006;27:
1087.
17. Carter AO, Saadi HF, Reed RL, Dunn EV. Assessment of obesity,
lifesty le, and reproductive health needs of female citizens of
Al-Ain, United Arab Emirates. J Health Publ Nutr 2004;22:75–83.
18. Pirozzo S, Summerbell C, Cameron C, Glasziou P. Should we
recommend low-fat diets for obesity? Obes Rev 2003;4:83–90.
19. Wood RJ, Fernandez ML. Carbohydrate restriction versus low
glycemic index diets: Which is a better option for the treatment
of insulin resistance and the metabolic syndrome? Nutr Rev
2009;67:179–183.
20. Carter AO, Elzubeir M, Abdulrazzaq YM, Revel AD, Townsend
A. Health and lifestyle needs assessment of medical students in
the United Arab Emirates. Med Teacher 2003;25:492–496.
21. Ordovas JM, Shen J. Gene-environment interactions and sus-
ceptibility to metabolic syndrome and other chronic diseases.
J Periodontol 2008;79:1508–1513.
22. Al-Lawati JA, Mohammed AJ, Al-Hinai HQ, Jousilahti P.
Prevalence of the Metabolic Syndrome among Omani Adults.
Diabetes Care 2003;26:1781–1785.
23. Grundy SM. Hypertriglyceridemia, atherogenic dyslipidemia,
and the metabolic syndrome. Am J Cardiol 1998;81:18B–25B.
24. Mutungi G, Waters D, Ratliff J, Puglisi MJ, Clark RM, Volek JS,
Fernandez ML. Eggs distinctly modulate plasma carotenoid
and lipoprotein subclasses in adult men following a carbohy-
drate restricted diet. J Nutr Biochem 2009;(Epub ahead of print).
25. Greene CM, Waters D, Clark RM, Contois JH, Fernandez ML.
Plasma LDL and HDL characteristics and carotenoid content
are positively infl uenced by egg consumption in an elderly
population. Nutr Met 2006;3:6.
26. Austin MA, Breslow JL, Hennekens CH, Buring JE, Willett WC,
Krauss RM: Low-density lipoprotein subclass patterns and risk
of myocardial infarction. JAMA 1988;260:1917–1921.
27. Krauss RM, Siri PW. Metabolic abnormalities: Triglyceride and low-
density lipoprotein. Endocrinol Metab Clin N Am 2004;33:405–415.
the UAE, especially major Emirates, such as Abu Dhabi and Dubai, or smaller cities in the north Emirates of the UAE where land geography, lifestyle, eating habits, and perhaps genetic factors could be slightly different. In addition, we are not presenting dietary habits or lipoprotein subfrac-tions from those subjects not classifi ed with the metabolic syndrome. Despite these limitations, however, these results provide solid data on the prevalence of metabolic syndrome among young overweight and obese Emirati population and may explain some of the reasons behind the high prevalence of T2DM in UAE.
Conclusion
In this study, about 41% of adult overweight/obese Emirati men and women, aged 18–50 years were classifi ed with met-abolic syndrome according to ATP III criteria. In addition, this population also presents several fi ndings associated with increased risk for CVD, including elevated concentra-tions of LDL-C, high number of small LDL particles, and low HDL-C. These fi ndings emphasize the urgency for public health programs aiming at lifestyle modifi cation to reduce the risk for T2DM and CVD later in life.
Acknowledgments
This study was supported by the Health Authority for the Emirate of Abu Dhabi (HAAD). We are grateful to Mrs. Fatima H. Al-Noaimi, dietitian, Department of Clinical Nutrition, at Tawam Hospital, for her help with data collec-tion and dietary records, and to Mr. Luisito Velasco, trained orderly, Department of Clinical Nutrition, for his help with data collection and clerical support. We also thank the hos-pital’s laboratory department, mainly the Chemistry sec-tion and the phlebotomist team for their blood draw and collection.
References
1. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic
syndrome among US adults: Findings from the third National
Health and Nutrition Examination Survey. JAMA 2002;287:
356–359.
2. Third Report of the National Cholesterol Education Program
(NCEP) expert panel on detection, evaluation, and treatment
of high blood cholesterol in adults (Adult Treatment Panel III).
Final report. Circulation 2002;106:3143–3421.
3. Wilson PW, D’Agostino RB, Parise H, Sullivan L, Meigs
JB. Metabolic syndrome as a precursor of cardiovascular
disease and type 2 diabetes mellitus. Circulation
2005;112:3066–3072.
4. International Diabetes Federation, Diabetes Atlas, 3rd edition,
2006. Accessed at www.idf.org/.
5. Badrinath P, Al-Shboul QA, Zoubeidi T, Gargoum AS, Ghubash
R, El-Rufaie OE (eds.). Measuring the health of the nation: United
Arab Emirates health and lifestyle survey, 2000. Accessed at
www.fmhs.uaeu.ae/cmd/UAEHALS2000.htm/.
6. El Mugamer IT, Ali Zayat AS, Hossain MM, Pugh RN. Diabetes,
obesity and hypertension in urban and rural people of bed-
ouin origin in the United Arab Emirates, J. Trop. Med. Hyg
1995;98:407–415.
7. Malik M, Bakir A, Abi Saab B, Roglic G, King H. Glucose intol-
erance and associated factors in the multi-ethnic population of
the United Arab Emirates: results of a national survey, Diabetes Res. Clin. Pract. 2005; 69:188–195.
06_MET-2009_0035.indd 45 1/27/2010 5:08:06 PM

AL-SARRAJ ET AL.46
Address correspondence to:Maria Luz Fernandez, Ph.D.
Department of Nutritional SciencesUniversity of Connecticut
3624 Horsebarn Road Ext, U 4017Storrs, CT 06269
E-mail: [email protected]
28. Fortmeier-Saucier L, Savrin C, Heinzer M, Hudak C. BMI and
lipid levels in Mexican American children diagnosed with type
2 diabetes. Worldview Evid Based Nurs 2008;5:142–147.
29. Krauss RM. Lipids and lipoproteins in patients with type 2
Diabetes. Diabetes Care J Clin Endocrinol Metab 2009;94:989-97.
30. Chan DC, Barrett PH, Ooi EM, Ji J, Chan DT, Watts GF. Very-low
density lipoprotein metabolism and plasma adiponectin as pre-
dictors of high-density lipoprotein apolipoprotein A-I kinetics in
obese and non-obese men. J Clin Endrocrinol Metab
2009;94:989–997.
31. Macdonald ML, van Eck M, Hildebrand RB, Wong BW, Bissada
N, Ruddle P, Kontush A, Hussein H, Pouladi MA, Chapman
MJ, Fievet C, van Berkel TJ, Staels B, McManus BM, Hayden
MR. Despite antiatherogenic metabolic characteristics, SCD1-
defi cient mice have increased infl ammation and atherosclerosis.
Arterioscler Thromb Vasc Biol 2008;Dec 18[Epub ahead of print].
06_MET-2009_0035.indd 46 1/27/2010 5:08:06 PM