-
1International Diabetes MonitorVolume 18, Number 5, 2006
Abstract
The metabolic syndrome is a cluster of meta-bolic abnormalities
associated with increasedrisk for cardiovascular disease and type
2diabetes.The most commonly used criteria todefine the metabolic
syndrome include the pres-ence of abdominal obesity, high blood
pressure,elevated fasting plasma glucose and dyslipidemia(high
triglyceride and/or decreased HDL choles-terol).There is great
variation in the prevalenceof the metabolic syndrome worldwide,
withincreasing trends related to the epidemic of obe-sity in most
countries. Insulin resistance and astate of chronic inflammation
are also underlyingfactors contributing to this syndrome.
C-reactiveprotein is an emerging biomarker that may beuseful for
risk stratification.The presence of themetabolic syndrome
identifies those with higherlong-term cardiovascular risk and thus
calls forintensified lifestyle therapy weight loss,increased
physical activity and antiatherogenicdiet. In some patients,
pharmacologic interven-tions may be indicated for the management
ofspecific components of this syndrome, mostlydepending upon the
severity of the abnormality.Further studies are needed to define
treatmentalgorithms for patients diagnosed with the meta-bolic
syndrome based on a particular combina-tion of its components.
Key words:Metabolic syndrome, cardiovascular disease,
diabetes,insulin resistance, obesity, inflammation, mortality
Historical background to definition of themetabolic syndrome
Investigators in the late 1980s, studying the rela-tionships
between dyslipidemia, obesity, insulinresistance, glucose
intolerance and the procoagu-lant state, independently recognized
that these
factors were associated with one another as wellas with
cardiovascular disease (CVD) [15].Thiscluster of CVD risk factors
began to be referredto as a syndrome using several different
names:the metabolic syndrome [68], the insulin resis-tance syndrome
[9], or syndrome X [3]. As evi-dence accumulated to indicate that
these riskfactors played an important role in the develop-ment of
CVD, the need to enhance awareness ofthem among health
professionals increased.Accordingly the term metabolic syndrome
wasformally adopted first by theWorld Health Orga-nization (WHO) in
1999 [10] and soon after bythe National Cholesterol Education
Program(NCEP)/AdultTreatment Panel III (ATP III) in2001 [11] and
then by others to describe a clus-ter of metabolic factors
associated with increasedrisk of type 2 diabetes and CVD [12,
13].
Diagnostic criteria
The most commonly used diagnostic criteriahave been those of
theWHO definition [10] andthe NCEP/ATP III definition [11], which
wasupdated in 2005 [13]. Recently the InternationalDiabetes
Federation (IDF) published its defini-tion of the metabolic
syndrome (Table I) [14].The latter two definitions are the more
easilyapplicable tools to assess the metabolic syndromein clinical
practice.It has been speculated that the predictive value
of the NCEP andWHO definitions may dependon the prevalence of
the core metabolic compo-nents (dyslipidemia, hypertension, obesity
andglycemia) in the population under investigation[15].Thus the
usefulness of the NCEP vs.WHOcriteria with a differing emphasis on
the compo-nents of the metabolic syndrome may varyaccording to the
background population towhich they are being applied. Prevalence
esti-mates for the NCEP/ATP III definition of the
REVIEW ARTICLES
Metabolic syndrome revisitedHermes Florez1,2,3 and Ron
Goldberg1
1University of Miami Miller School of Medicine;2Miami Veterans
Affairs Medical, Miami, FL, USA;
3University of Zulia School of Medicine, Maracaibo,
Venezuela([email protected]; [email protected])
-
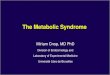
metabolic syndrome have been reported for sev-eral countries
(Fig. 1) [1631].These differ withrespect to the sample selection,
the year in whichthey were conducted, the precise definition
used,and the age and sex structure of the population.There is a
wide variation of prevalence by genderand race/ethnicity [22].Two
more criteria sets for the diagnosis of the
metabolic syndrome have been suggested by theAmerican
Association of Clinical Endocrinolo-gists [32] and by the European
Group for theStudy of Insulin Resistance [33].The key differ-ences
from the NCEP and IDF criteria are thatboth of these criteria sets
are totally foundedon insulin resistance and exclude patientswith
diabetes.The IDF clinical definition requires abdomi-
nal obesity for metabolic syndrome diagnosis, asa good surrogate
for the more cumbersome mea-surement of insulin resistance and to
reduce theamount of laboratory testing necessary for
iden-tification.When abdominal obesity is present,two additional
factors originally listed in theNCEP definition and now somewhat
modifiedare sufficient for diagnosis.The IDF emphasizedthe presence
of ethnic and national differences inthe abdominal obesity
threshold [14, 34]. Recentanalyses in the US population
(19992002)showed that the IDF definition leads to a
higherprevalence estimate of the metabolic syndrome(39%) than that
based on the updated NCEPdefinition (34.5%) [25], particularly in
MexicanAmerican men.
Underlying mechanisms: insulin resistanceand obesity
The predominant underlying risk factors for themetabolic
syndrome are thought to be insulinresistance [3, 35, 36] and
abdominal obesity [13,3739]. Reaven [3] postulated that insulin
resis-tance and its compensatory hyperinsulinemiapredispose
patients to hypertension, hyperlipid-emia and type 2 diabetes and
are thus the under-lying cause of much CVD.This constellation
ofinterrelated metabolic risk factors appears topromote the
development of atheroscleroticCVD (Fig. 2). Although obesity was
not includedin Reavens primary list of disorders caused byinsulin
resistance, he acknowledged that it, too,was correlated with
insulin resistance or hyper-insulinemia, and that the obvious
treatment forwhat he termed syndrome X was weight main-tenance (or
weight loss) and physical activity. Astate of mild chronic
inflammation has also beenrelated to features of the metabolic
syndrome,particularly obesity and insulin resistance [40],as
discussed below.
Insulin resistance
The metabolic syndrome is associated withinsulin resistance but
is not a consequence ofinsulin resistance alone nor of the lack of
insulinaction alone [41].Three mechanisms have beenproposed to
explain how insulin resistance mightgenerate other features of the
metabolic syn-
2 International Diabetes Monitor Volume 18, Number 5, 2006
Review articles
Table I: Criteria for clinical diagnosis of the metabolic
syndrome.
Clinical measurea WHOb (1999) [10] ATP III (2005) [13] IDFc
(2005) [14]
Abdominal obesity WHR >0.90 (M) Waist 102 cm (Asians 90
cm)(M)Waist 94 cm (Asians 90 cm)
(M)WHR >0.85 (F) Waist 88 cm (Asians 80 cm) (F) Waist 80 cm
(Asians 80 cm) (F)or BMI
-
drome: the effects of mild to moderate hyper-glycemia, the
effects of compensatory hyperinsu-linemia, and the effects of
unbalanced pathwaysof insulin action. In insulin resistance
condi-tions, the ability of insulin to augment glucoseuptake and
inhibit hepatic glucose production isimpaired.The resultant
hyperglycemia presentsa stimulus to the -cells, which secrete
largeamounts of insulin after meals. In individualsin whom -cell
dysfunction occurs, glucoseintolerance and type 2 diabetes may
develop,and the development of hyperglycemia is associ-ated with an
increasing prevalence of the meta-bolic syndrome.The two major
pathways for insulin signaling
are the phosphatidylinositol 3-kinase (PI3K) andthe
mitogen-activated protein (MAP) kinasepathways [42]. In the
metabolic syndrome thepathways leading to activation of PI3K
areimpaired, whereas the MAP kinase pathway,which mediates the
mitogenic and proinflamma-tory responses of insulin signaling, may
be over-stimulated [43], leading to unbalanced combina-tions of
both reduced as well as excessive
activation of metabolic targets via these twopathways of insulin
action.
Although insulin-resistant individualsneed not be clinically
obese, theynevertheless commonly have an
abnormal fat distribution characterizedby predominant upper
body
fat accompanied by an expandedvisceral fat depot
Obesity
During the last decade, newly discovered adipo-kinetic pathways
have suggested novel patho-physiologic mechanisms linking increased
adi-pose tissue mass with the development of insulinresistance and
other components of the meta-bolic syndrome [44]. In the Insulin
ResistanceAtherosclerosis Study [45], the strongest predic-tor of
the metabolic syndrome was waist circum-ference; thus, abdominal
obesity may precede
3International Diabetes MonitorVolume 18, Number 5, 2006
Review articles
Mexico (19971999)
Saudi Arabia (19952000)
Iran (19992001)
Turkey (2000)
USA (19992002)
Venezuela (19992001)
Portugal (2000)
USA (19881994)
Oman (2001)
Greece (2003)
Spain (20002003)
Italy (2000)
South Korea (1998)
India (2003)
Australia (19992000)
France (1996)
0 10 20 30 40 50 60
Prevalence (%)
WomenMen
Fig. 1: Prevalence of the metabolic syndrome in several
countries according to NCEP/ATP III criteria. Data from a recent
analysisof a national survey showed a prevalence of 34% in Mexico
(personal communication from Simon Barquera,MD, PhD).
-
the development of components of the metabolicsyndrome.
Likewise, in the San Antonio HeartStudy [46], one-third of subjects
with both alarge waist circumference and high BMI devel-oped the
metabolic syndrome during the 8-yearfollow-up. Adjusting for
fasting insulin concen-trations had only a minor effect on the
predictivevalue of the anthropometric indices.It is recognized that
some people who are not
obese or even overweight by traditional measuresare nevertheless
insulin-resistant and haveabnormal levels of metabolic risk factors
(nor-mal weight, metabolically obese) [47].This wasalso observed in
lean individuals with twodiabetic parents or one parent and a
first- orsecond-degree relative [48]. Although insulin-resistant
individuals need not be clinically obese,they nevertheless commonly
have an abnormalfat distribution characterized by predominantupper
body fat which is accompanied by anexpanded visceral fat depot (or
visceral adipos-ity) and which is associated with increasedrelease
of non-esterified fatty acids from adiposetissue [49, 50]; this
contributes to ectopic lipidaccumulation in muscle and liver, which
isthought to predispose to insulin resistance [51]and dyslipidemia
[52].The tendency to increasevisceral fat with only modest
increases in subcu-taneous fat and body weight is especially true
inpopulations from Asia [34].This has led to therecommendation in
the IDF and the AmericanHeart Association update on the NCEP
defini-tion of the metabolic syndrome that cut-pointsfor increased
waist circumference be set lowerfor these populations.Therefore
some investiga-tors regard insulin resistance as a mediating
fac-tor in the metabolic syndrome, but not as theprimary cause, and
consider dysfunctionalenergy storage to be a fundamental step
[41].Abnormalities in the processing and storage offatty acids and
triglycerides, the molecules that
account for most of the bodys energy utilizationand storage, are
observed when there is toomuch triglyceride or body fat (i.e.
obesity).When the capacity of adipocytes to store triglyc-eride is
exceeded, fat accumulates in hepato-cytes, skeletal myocytes and
other tissues. Exces-sive maldistribution of fat in visceral
tissuesappears to be a marker or perhaps a determinantof insulin
resistance.Visceral adiposity correlateswell with insulin
resistance and most features ofthe metabolic syndrome.The adipose
tissue of obesity exhibits abnor-
malities in the production of adipokines, whichmay separately
affect insulin resistance and/ormodify the risk of atherosclerotic
CVD.Theseinclude increased production of inflammatorycytokines [53,
54], plasminogen activatorinhibitor-1 [55] and other bioactive
products[44]; at the same time the potentially protectiveadipokine,
adiponectin, is reduced [56]. All ofthese changes have been
implicated in the gen-esis of metabolic risk factors. Indeed, as
men-tioned above, some individuals exhibit the meta-bolic syndrome
with only a moderate degree oftotal body obesity [47].
Inflammation and the metabolic syndrome
In recent years extensive studies have uncoveredthe importance
of systemic low-grade inflamma-tion in the initiation and
development of athero-sclerosis as well as acute CVD events
[5759].Several cytokines and acute-phase reactants havebeen shown
to be associated with and predictCVD, including C-reactive protein,
interleukin 6(IL-6), serum amyloid A, fibrinogen, whiteblood cell
count, D-dimer, plasminogen activa-tor, tumor necrosis factor-
(TNF), lipoproteinphospholipase A2, interleukin-18,
metallopro-teinase PAPP-A and secretory non-pancreaticphospholipase
A2 type IIA [6062]. In addition,systemic inflammation is also
associated withatherogenic changes in lipoprotein
metabolismincluding hypertriglyceridemia; elevated
triglyc-eride-rich lipoprotein; small, dense LDL; anddecreased HDL
cholesterol [63].C-reactive protein correlates with the
severity
of the metabolic syndrome [64] and, eventhough several studies
support the role ofinflammation in the development of the
meta-bolic syndrome, the nature of the relationshipsamong these
inflammatory markers, the pres-ence of dyslipidemia and the degree
of insulinresistance remain unclear [6567].There is evidence that
obesity and chronic
subclinical inflammation may play intermediary
4 International Diabetes Monitor Volume 18, Number 5, 2006
Review articles
Dyslipidemia
Hypertriglyceridemia
Small, dense LDL
Low HDL
Hypertension
HyperglycemiaHypercoagulability
Underlyingfactors
Metabolicfactors
Clinicaloutcomes
Cardiovasculardisease
Insulinresistance
Inflammation
Abdominalobesity
Type 2diabetes
Fig. 2:Metabolic syndrome pathways.
-
roles in the pathogenesis of CVD and type 2 dia-betes [68].The
levels of C-reactive protein andIL-6 increase with the degree of
adiposity andmay lead to higher insulin resistance and the riskof
developing type 2 diabetes [69].To the extentthat elevated IL-6 and
C-reactive protein levelsreflect adipocyte activation, the
availability ofthese markers represents an approach for
earlyidentification of individuals at increased riskof the
metabolic syndrome, type 2 diabetesand CVD.
The American Heart Associationrecommends the use of
C-reactive
protein as the best inflammatory markerin the clinical
assessment of CVD risk
Among a wide range of biomarkers, C-reactiveprotein is
considered to be the most applicablefor clinical use. In several
studies, C-reactiveprotein has actually predicted CVD better
thanother inflammatory biomarkers including inter-cellular adhesion
molecule-1 and vascular celladhesion molecule-1,TNF and IL-6, and
inde-pendently of LDL cholesterol and other lipopro-tein levels
[61]. In the general population, thelevel of C-reactive protein has
been found toconsistently predict incident myocardial infarc-tion,
stroke, peripheral arterial disease, suddencardiac death, and
recurrent ischemia and deathin patients with angina and acute
coronarysymptoms [70].The American Heart Associationrecommendations
state that, although inconclu-sive, evidence supports the use of
C-reactiveprotein as the best inflammatory marker in theclinical
assessment of CVD risk [60].
Association of the metabolic syndrome withmortality and CVD
There is uncertainty about the clinical and pub-lic health
importance of the metabolic syndrome[71, 72]. A recent report
summarizing its predic-tive value [73] concluded that the
population-attributable risk (PAR) associated with the meta-bolic
syndrome, based on the NCEP andWHOdefinitions, is approximately 67%
for all-causemortality and 1217% for CVD. A report fromthe
Framingham Heart Offspring Study [74]recently showed that the PAR
for the metabolicsyndrome as a predictor of CVD and coronaryheart
disease was 34% and 29%, respectively, inmen and 16% and 8%,
respectively, in women.The metabolic syndrome components that
con-
tributed most to the cardiovascular outcomeswere elevated blood
pressure and low HDL cho-lesterol, with PAR estimates of 33% and
25%,respectively.The metabolic syndrome varies in its predic-
tive capacity for CVD by ethnicity, gender andthe presence or
absence of hyperglycemia [75,76]. In the Framingham Offspring
database, themetabolic syndrome accounted for approxi-mately
one-fourth of cardiovascular morbidity[74]. In the Botnia study,
subjects with themetabolic syndrome had a threefold increasedrisk
of coronary heart disease and stroke, a five-to sixfold increased
risk of CVD death, andincreased all-cause mortality [77]. In
Finnishmen, insulin resistance and the metabolic syn-drome
predicted coronary heart disease eventsand both CVD and all-cause
mortality [78].Therisk of death from all causes and CVD
increasedwith growing numbers of abnormalities [79].The presence of
the metabolic syndrome iden-
tifies those with relatively high long-term risk ofCVD and thus
calls for intensified lifestyletherapy. It needs to be stressed
that the meta-bolic syndrome itself is a relatively poor
indicatorof absolute short-term risk [80], because it doesnot
contain key determinants of short-term risksuch as age, serum
cholesterol, gender andsmoking status. A more accurate predictor
ofshort-term risk is Framingham scoring, whichincludes all of the
major risk factors.
Metabolic syndrome and diabetesdevelopment
The metabolic syndrome not only accompaniesbut also precedes and
predicts type 2 diabetes[81, 82].The San Antonio Heart Study
investi-gators compared OGTT results against theNCEP andWHO
criteria for the metabolic syn-drome in predicting diabetes. Of the
three,impaired glucose tolerance on the OGTT wasthe best with a
predictive value of 43% vs. 31%by the NCEP criteria and 30% by the
modifiedWHO criteria [83]. Furthermore, even in sub-jects with
impaired glucose tolerance, the pres-ence of the metabolic syndrome
increased therisk of progression of type 2 diabetes,
althoughfurther studies are needed to confirm this obser-vation.
Interestingly, in a study among non-diabetic American Indians, the
homeostasismodel assessment for insulin resistance and themetabolic
syndrome at baseline were associatedwith an increased risk of type
2 diabetes, butCVD was not predicted independently of
othercardiovascular risk factors [84].
5International Diabetes MonitorVolume 18, Number 5, 2006
Review articles
-
In a recent review of prospective studies usingthe NCEP andWHO
definitions of the meta-bolic syndrome, Ford [73] found that the
PARfor type 2 diabetes was between 30% and 52%.
The primary goal of clinical managementin patients with the
metabolic syndromeis to reduce their long-term risk of CVD
In the Framingham cohort, the presence of themetabolic syndrome
at baseline was also foundto be a powerful predictor of new-onset
diabetes.Using the revised NCEP definition for the meta-bolic
syndrome, the PAR for type 2 diabetes was62% in men and 47% in
women [74]. Asexpected, elevated blood glucose (100 mg/dl)was
associated with the highest PAR of 62%for type 2 diabetes, while
the combination ofelevated blood glucose, abdominal obesity andlow
HDL cholesterol was associated with a large12-fold increased risk
of incident type 2diabetes. However, trait combinations that didnot
include elevated blood glucose also impartedan approximately
fivefold increased risk of inci-dent type 2 diabetes.This is
consistent with theconcept that the metabolic syndrome trait
com-bination reflects an underlying insulin
resistancepathophysiology.
Management of the metabolic syndrome
The primary goal of clinical management inpatients with the
metabolic syndrome is toreduce their long-term risk of CVD.The
primaryemphasis should be on the modification ofunderlying risk
factors (obesity, physical inactiv-ity and atherogenic diet)
through lifestylechanges. Not only do these interventionsimprove
individual metabolic syndrome compo-nents, but they have been shown
to amelioratethe underlying pathophysiologic determinants ofthe
syndrome, such as obesity, insulin resistanceand inflammation [13,
85]. No studies haveexamined the value of tailoring the
treatmentalgorithm to the particular combination of crite-ria that
resulted in the diagnosis of the metabolicsyndrome [72], nor
whether the presence of themetabolic syndrome justifies earlier
applicationof pharmacologic interventions for
preclinicalabnormalities in syndrome components, e.g.
pre-hypertension, prediabetes or suboptimal lipidlevels. Specific
pharmacologic interventions maybe indicated for the management of
clinicallysignificant components of the syndrome, e.g.
hypertension, dyslipidemia, glucose intoleranceor the
procoagulant state. It is unknown whetherinsulin sensitizers, as an
approach to the treat-ment of insulin resistance itself, or the use
ofagents that lower C-reactive protein levels such asstatins,
fibrates, nicotinic acid and thiazolidine-diones would be of value
in preventing CVD inall or a subset of patients with the metabolic
syn-drome outside their current clinical indications.
Acknowledgments
Dr Florezs work is supported by grants from theDepartment
ofVeterans Affairs MiamiGRECCand CSP#465, Pan American Health
Organiza-tion RC/RG-T/VEN/3201, and UMHumanaHealth Service
Research. Dr Goldbergs work issupported by grants from the National
Institutesof Health NIDDK DK01 0500 and2RO1HL36588-16.
References
1.OrchardTJ, Becker DJ, Bates M et al. Plasma insulinand
lipoprotein concentrations: an atherogenic associa-tion? Am J
Epidemiol 1983; 118(3): 32637.
2.Haffner SM, Fong D, Hazuda HP et al. Hyperinsulin-emia, upper
body adiposity, and cardiovascular risk fac-tors in
non-diabetics.Metabolism 1988; 37(4): 33845.
3. Reaven GM. Role of insulin resistance in human dis-ease.
Diabetes 1988; 37(12): 1595607.
4. Bjrntorp P.The associations between obesity, adiposetissue
distribution and disease. Acta Med Scand Suppl1988; 723: 12134.
5. Juhan-Vague I,Vague P. Interrelations between carbo-hydrates,
lipids, and the hemostatic system in relation tothe risk of
thrombotic and cardiovascular disease. Am JObstet Gynecol 1990; 163
(1 part 2): 31315.
6. Avogaro P, Crepaldi G, Enzi G,Tiengo A. Associazionedi
iperlidemia, diabete mellito e obesita di medio grado.Acta Diabetol
Lat 1967; 4: 3641.
7.Haller H. Epidemiology and associated risk factors
ofhyperlipoproteinemia. Z Gesamte Inn Med 1977; 32(8):1248.
8. Singer P. Diagnosis of primary hyperlipoproteinemias.
ZGesamte Inn Med 1977; 32(8): 12933.
9. Stern MP, Haffner SM. Body fat distribution
andhyperinsulinemia as risk factors for diabetes and
cardio-vascular disease. Arteriosclerosis 1986; 6(2): 12330.
10.World Health Organization. Definition, diagnosis,
andclassification of diabetes mellitus and its complications:
reportof aWHO consultation. Geneva:WHO, 1999.
11. Expert Panel on Detection, Evaluation, andTreatmentof High
Blood Cholesterol in Adults. Executive sum-mary of the third report
of the National CholesterolEducation Program (NCEP) Expert Panel on
Detec-tion, Evaluation, andTreatment of High Blood Choles-terol in
Adults (AdultTreatment Panel III). J Am MedAssoc 2001; 85:
248697.
12.Nesto RW.The relation of insulin resistance syndromesto risk
of cardiovascular disease. Rev Cardiovasc Med2003; 4 (suppl 6):
S1118.
13.Grundy SM, Cleeman JI, Daniels SR et al., for theAmerican
Heart Association and National Heart, Lung,
6 International Diabetes Monitor Volume 18, Number 5, 2006
Review articles
-
and Blood Institute. Diagnosis and management of themetabolic
syndrome: an American HeartAssociation/National Heart, Lung, and
Blood InstituteScientific Statement. Circulation 2005;
112(17):273552.
14. Alberti KG, Zimmet P, Shaw J, for the IDF Epidemiol-ogyTask
Force Consensus Group.The metabolic syn-drome a new worldwide
definition. Lancet 2005;366(9491): 105962.
15.Hunt KJ, Resendez RG,Williams K et al., for the SanAntonio
Heart Study. National Cholesterol EducationProgram versusWorld
Health Organization metabolicsyndrome in relation to all-cause and
cardiovascularmortality in the San Antonio Heart Study.
Circulation2004; 110(10): 12517.
16. Ford ES, GilesWH, DietzWH. Prevalence of the meta-bolic
syndrome among US adults: findings from theThird National Health
and Nutrition Examination Sur-vey. J Am Med Assoc 2002; 287(3):
3569.
17.Onat A, Ceyhan K, Basar O et al. Metabolic syndrome:major
impact on coronary risk in a population with lowcholesterol levels
a prospective and cross-sectionalevaluation. Atherosclerosis 2002;
165(2): 28592.
18.Gupta A, Gupta R, Sarna M et al. Prevalence of dia-betes,
impaired fasting glucose and insulin resistancesyndrome in an urban
Indian population. Diabetes ResClin Pract 2003; 61(1): 6976.
19. Azizi F, Salehi P, Etemadi A, Zahedi-Asl S. Prevalenceof
metabolic syndrome in an urban population:TehranLipid and Glucose
Study. Diabetes Res Clin Pract 2003;61(1): 2937.
20. Al-Lawati JA, Mohammed AJ, Al-Hinai HQ, JousilahtiP.
Prevalence of the metabolic syndrome among Omaniadults. Diabetes
Care 2003; 26(6): 17815.
21. Balkau B,Vernay M, Mhamdi L et al., for theD.E.S.I.R. Study
Group.The incidence and persistenceof the NCEP (National
Cholesterol Education Pro-gram) metabolic syndrome.The French
D.E.S.I.R.study. Diabetes Metab 2003; 29(5): 52632.
22. Cameron AJ, Shaw JE, Zimmet PZ.The metabolic syn-drome:
prevalence in worldwide populations. EndocrinolMetab Clin North Am
2004; 33(2): 35175.
23. Santos AC, Lopes C, Barros H. Prevalence of
metabolicsyndrome in the city of Porto. Rev Port Cardiol
2004;23(1): 4552.
24. Park HS, Oh SW, Cho SI et al.The metabolic syndromeand
associated lifestyle factors among South Koreanadults. Int J
Epidemiol 2004; 33: 32836.
25. Ford ES. Prevalence of the metabolic syndrome definedby the
International Diabetes Federation among adultsin the U.S. Diabetes
Care 2005; 28(11): 27459.
26. Lorenzo C,Williams K, Gonzalez-Villalpando C,Haffner SM.The
prevalence of the metabolic syndromedid not increase in Mexico City
between 19901992and 19971999 despite more central obesity.
DiabetesCare 2005; 28(10): 24805.
27.Miccoli R, Bianchi C, Odoguardi L et al. Prevalence ofthe
metabolic syndrome among Italian adults accordingto ATP III
definition.Nutr Metab Cardiovasc Dis 2005;15(4): 2504.
28.Martinez-Larrad MT, Fernandez-Perez C, Gonzalez-Sanchez JL et
al., for the Grupo de Estudio de AtencionPrimaria de Segovia.
Prevalence of the metabolic syn-drome (ATP-III criteria).
Population-based study ofrural and urban areas in the Spanish
province ofSegovia.Med Clin (Barc) 2005; 125(13): 4816.
29. AthyrosVG, BouloukosVI, Pehlivanidis AN et al., forthe
MetS-Greece Collaborative Group.The prevalenceof the metabolic
syndrome in Greece: the MetS-GreeceMulticentre Study. Diabetes Obes
Metab 2005; 7(4):397405.
30. Al-Nozha M, Al-Khadra A, Arafah MR et al. Metabolic
syndrome in Saudi Arabia. Saudi Med J 2005; 26(12):191825.
31. Florez H, Silva E, FernandezV et al. Prevalence andrisk
factors associated with the metabolic syndrome anddyslipidemia in
white, black, Amerindian and mixedHispanics in Zulia
State,Venezuela. Diabetes Res ClinPract 2005; 69(1): 6377.
32. Einhorn D, Reaven GM, Cobin RH et al. AmericanCollege of
Endocrinology position statement on theinsulin resistance syndrome.
Endocr Pract 2003; 9(3):23752.
33. Balkau B, Charles MA. Comment on the provisionalreport from
theWHO consultation. European Groupfor the Study of Insulin
Resistance (EGIR). DiabeticMed 1999; 16(5): 4423.
34. Tan CE, Ma S,Wai D et al. Can we apply the
NationalCholesterol Education Program AdultTreatment
Paneldefinition of the metabolic syndrome to Asians? DiabetesCare
2004; 27(5): 11826.
35. Ferrannini E, Haffner SM, Mitchell BD, Stern
MP.Hyperinsulinaemia: the key feature of a cardiovascularand
metabolic syndrome. Diabetologia 1991; 34:41622.
36.Haffner SM,Valdez RA, Hazuda HP et al. Prospectiveanalysis of
the insulin-resistance syndrome (syndromeX). Diabetes 1992; 41:
71522.
37. Lemieux I, Pascot A, Couillard C et al.
Hypertriglycerid-emic waist: a marker of the atherogenic metabolic
triad(hyperinsulinemia; hyperapolipoprotein B; small, denseLDL) in
men? Circulation 2000; 102: 17984.
38. ParkYW, Zhu S, Palaniappan L et al.The metabolicsyndrome:
prevalence and associated risk factor findingsin the US population
from theThird National Healthand Nutrition Examination Survey
19881994. ArchIntern Med 2003; 163: 42736.
39. Carr DB, Utzschneider KM, Hull RL et al. Intra-abdominal fat
is a major determinant of the NationalCholesterol Education Program
AdultTreatment PanelIII criteria for the metabolic syndrome.
Diabetes 2004;53: 208794.
40. Festa A, DAgostino R Jr, Howard G et al. Chronic
sub-clinical inflammation as part of the insulin
resistancesyndrome: the Insulin Resistance Atherosclerosis
Study(IRAS). Circulation 2000; 102(1): 427.
41.Miranda PJ, DeFronzo RA, Califf RM, Guyton JR.Metabolic
syndrome: definition, pathophysiology, andmechanisms. Am Heart J
2005; 149(1): 3345.
42. Le Roith D, ZickY. Recent advances in our understand-ing of
insulin action and insulin resistance. Diabetes Care2001; 24(3):
58897.
43. Cusi K, Maezono K, Osman A et al. Insulin
resistancedifferentially affects the PI 3-kinase and MAP
kinase-mediated signaling in human muscle. J Clin Invest
2000;105(3): 31120.
44. Ruan H, Lodish HF. Regulation of insulin sensitivity
byadipose tissue-derived hormones and inflammatorycytokines. Curr
Opin Lipidol 2004; 15: 297302.
45. Palaniappan L, Carnethon MR,WangY et al. Predictorsof the
incident metabolic syndrome in adults: theInsulin Resistance
Atherosclerosis Study. Diabetes Care2004; 27(3): 78893.
46.HanTS,Williams K, Sattar N et al. Analysis of obesityand
hyperinsulinemia in the development of metabolicsyndrome: San
Antonio Heart Study. Obes Res 2002;10(9): 92331.
47. Ruderman N, Chisholm D, Pi-Sunyer X, Schneider S.The
metabolically obese, normal-weight individualrevisited. Diabetes
1998; 47(5): 699713.
48. Perseghin G, Ghosh S, Gerow K, Shulman GI. Meta-bolic
defects in lean nondiabetic offspring of NIDDMparents: a
cross-sectional study. Diabetes 1997; 46(6):10019.
7International Diabetes MonitorVolume 18, Number 5, 2006
Review articles
-
49. Jensen MD, Haymond MW, Rizza RA et al. Influence ofbody fat
distribution on free fatty acid metabolism inobesity. J Clin Invest
1989; 83(4): 116873.
50. Abate N, Chandalia M, Snell PG, Grundy SM. Adiposetissue
metabolites and insulin resistance in nondiabeticAsian Indian men.
J Clin Endocrinol Metab 2004; 89(6):27505.
51. Petersen KF, Shulman GI. Pathogenesis of skeletalmuscle
insulin resistance in type 2 diabetes mellitus. AmJ Cardiol 2002;
90(5A): 1118G.
52. Browning LM, Jebb SA, Mishra GD et al. Elevatedsialic acid,
but not CRP, predicts features of the meta-bolic syndrome
independently of BMI in women. Int JObes Relat Metab Disord 2004;
28(8): 100410.
53.Weisberg SP, McCann D, Desai M et al. Obesity isassociated
with macrophage accumulation in adiposetissue. J Clin Invest 2003;
112(12): 1796808.
54. YouT,Yang R, Lyles MF et al. Abdominal adipose tis-sue
cytokine gene expression: relationship to obesityand metabolic risk
factors. Am J Physiol EndocrinolMetab 2005; 288(4): E7417.
55. Juhan-Vague I, Alessi MC, Mavri A, Morange PE. Plas-minogen
activator inhibitor-1, inflammation, obesity,insulin resistance and
vascular risk. JThromb Haemost2003; 1(7): 15759.
56.Kern PA, Di Gregorio GB, LuT et al. Adiponectinexpression
from human adipose tissue: relation to obe-sity, insulin
resistance, and tumor necrosis factor-alphaexpression. Diabetes
2003; 52(7): 177985.
57. Ross R. Atherosclerosis an inflammatory disease.NEngl J Med
1999; 340: 11526.
58.Hansson GK. Immune mechanisms in atherosclerosis.Arterioscler
ThrombVasc Biol 2001; 21(12): 187690.
59. Libby P. Inflammation in atherosclerosis.Nature
2002;420(6917): 86874.
60. PearsonTA, Mensah GA, Alexander RW et al. Markersof
inflammation and cardiovascular disease. Applicationto clinical and
public health practice. A statement forhealthcare professionals
from the Centers for DiseaseControl and Prevention and the American
Heart Asso-ciation. Circulation 2003; 107: 499511.
61. Fichtlscherer S, Heeschen C, Zeiher AM. Inflammatorymarkers
and coronary artery disease. Curr Opin Phar-macol 2004; 4:
12431.
62.Hurt-Camejo E, Camejo G, Peilot H et al. Phospholi-pase A2 in
vascular disease. Circ Res 2001; 89: 298304.
63.KhovidhunkitW, Memon RA, Reinglod KR, GrunfeldC. Infection
and inflammation-induced proatherogenicchanges of lipoproteins. J
Infect Dis 2000; 181 (suppl 3):S46272.
64. Frohlich M, Imhof A, Berg G et al. Association
betweenC-reactive protein and features of the metabolic syn-drome:
a population-based study. Diabetes Care 2000;23: 18359.
65. Pickup JC, Mattock MB, Chusney GD, Burt D.NIDDM as a disease
of the innate immune system:association of acute-phase reactants
and interleukin-6with metabolic syndrome X. Diabetologia 1997;
40:128692.
66.Mendall MA, Patel P, Ballam L et al. C-reactive proteinand
its relation to cardiovascular risk factors: a popula-tion based
cross sectional study. Br Med J 1996;321(7038): 10615.
67. Tracy RP, Lemaitre RN, Psaty BM et al. Relationship
ofC-reactive protein to risk of cardiovascular disease inthe
elderly: results from the Cardiovascular HealthStudy and the Rural
Health Promotion Project.Arterioscler ThrombVasc Biol 1997; 17(6):
11217.
68. Pradhan AD, Manson JE, Rifai N et al. C-reactive pro-
tein, interleukin-6, and risk of developing type 2 dia-betes
mellitus. J Am Med Assoc 2001; 286(3): 32734.
69. Yudkin JS, Stehouwer CD, Emeis JJ, Coppack SW. C-reactive
protein in healthy subjects: associations withobesity, insulin
resistance, and endothelial dysfunction.Arterioscler ThrombVasc
Biol 1999; 19(4): 9728.
70. Ridker PM, Buring JE, Cook NR, Rifai N. C-reactiveprotein,
the metabolic syndrome, and risk of incidentcardiovascular events.
An 8-year follow-up of 14719 ini-tially healthy American women.
Circulation 2003;107(3): 3917.
71. Ford ES. Insulin resistance syndrome: the public
healthchallenge. Endocr Pract 2003; 9 (suppl 2): 235.
72.Kahn R, Buse J, Ferrannini E, Stern M.The metabolicsyndrome:
time for a critical appraisal. Joint statementfrom the American
Diabetes Association and the Euro-pean Association for the Study of
Diabetes. Diabetologia2005; 48(9): 168499.
73. Ford ES. Risks for all-cause mortality,
cardiovasculardisease, and diabetes associated with the metabolic
syn-drome: a summary of the evidence. Diabetes Care 2005;28(7):
176978.
74.Wilson PW, DAgostino RB, Parise H et al. Metabolicsyndrome as
a precursor of cardiovascular disease andtype 2 diabetes mellitus.
Circulation 2005; 112(20):306672.
75. Brown SA, Hutchinson R, Morriset J et al. Plasma
lipid,lipoprotein cholesterol, and apoprotein distribution
inselected US communities.The Atherosclerosis Risk inCommunities
(ARIC) study. Arterioscler Thromb 1993;13: 113958.
76. Laws A, Hoen HM, Selby JV et al. Differences ininsulin
suppression of free fatty acid levels by genderand glucose
tolerance status. Relation to plasma triglyc-eride and
apolipoprotein B concentrations. InsulinResistance Atherosclerosis
Study (IRAS) Investigators.Arterioscler ThrombVasc Biol 1997; 17:
6471.
77. Isomaa B, Almgren P,TuomiT et al. Cardiovascularmorbidity
and mortality associated with the metabolicsyndrome. Diabetes Care
2001; 4: 6839.
78. Lakka HM, Laaksonen DE, LakkaTA et al.The meta-bolic
syndrome and total and cardiovascular diseasemortality in
middle-aged men. J Am Med Assoc 2002;288: 270916.
79. Trevisan M, Liu J, Bahsas FB, Menotti A. Syndrome Xand
mortality: a population-based study. Risk Factorand Life Expectancy
Research Group. Am J Epidemiol1998; 148: 95866.
80.Grundy SM. Point: the metabolic syndrome still lives.Clin
Chem 2005; 51: 13524.
81.Keklinen P, Sarlund H, Pyrl K, Laakso M. Hyper-insulinemia
cluster predicts the development of type 2diabetes independently of
family history of diabetes.Diabetes Care 1999; 22: 8692.
82.Hanson RL, Imperatore G, Bennett PH, KnowlerWC.Components of
the metabolic syndrome and incidenceof type 2 diabetes. Diabetes
2002; 51: 31207.
83. Lorenzo C, Okoloise M,Williams K et al.The metabolicsyndrome
as predictor of type 2 diabetes: the San Anto-nio Heart Study.
Diabetes Care 2003; 26: 31539.
84. Resnick HE, Jones K, Ruotolo G et al. Insulin resis-tance,
the metabolic syndrome, and risk of incident car-diovascular
disease in nondiabetic American Indians:the Strong Heart Study.
Diabetes Care 2003; 26: 8617.
85. OrchardTJ,Temprosa M, Goldberg R et al., for the Dia-betes
Prevention Program Research Group.The effect ofmetformin and
intensive lifestyle intervention on themetabolic syndrome: the
Diabetes Prevention Programrandomized trial.Ann Intern Med 2005;
142: 6119.
8 International Diabetes Monitor Volume 18, Number 5, 2006
Review articles







![Metabolic Syndrome[1]](https://img.pdfslide.us/doc/110x75/577cd7141a28ab9e789dffc3/metabolic-syndrome1.jpg)