Embed Size (px)
Citation preview

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 7 1 , N O . 6 , 2 0 1 8
ª 2 0 1 8 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
THE PRESENT AND FUTURE
STATE-OF-THE-ART REVIEW
Metabolic SurgeryWeight Loss, Diabetes, and Beyond
Manan Pareek, MD, PHD,a,b Philip R. Schauer, MD,c Lee M. Kaplan, MD, PHD,d Lawrence A. Leiter, MD,e
Francesco Rubino, MD,f Deepak L. Bhatt, MD, MPHa
ABSTRACT
ISS
Fro
va
an
Ho
On
Co
As
ha
the
me
Es
ha
ha
Re
Ca
Ca
da
Cli
ed
Ins
mu
ed
Ca
ed
CA
My
Me
Dis
Co
rep
Ma
The alarming rise in the worldwide prevalence of obesity is paralleled by an increasing burden of type 2 diabetes mellitus.
Metabolic surgery is the most effective means of obtaining substantial and durable weight loss in individuals with obesity.
Randomized trials have recently shown the superiority of surgery over medical treatment alone in achieving improved
glycemic control, as well as a reduction in cardiovascular risk factors. The mechanisms seem to extend beyond the
magnitude of weight loss alone and include improvements in incretin profiles, insulin secretion, and insulin sensitivity.
Moreover, observational data suggest that the reduction in cardiovascular risk factors translates to better patient
outcomes. This review describes commonly used metabolic surgical procedures and their current indications and
summarizes the evidence related to weight loss and glycemic outcomes. It further examines their potential effects on
cardiovascular outcomes and mortality and discusses future perspectives. (J Am Coll Cardiol 2018;71:670–87)
© 2018 by the American College of Cardiology Foundation.
N 0735-1097/$36.00 https://doi.org/10.1016/j.jacc.2017.12.014
m the aBrigham and Women’s Hospital Heart & Vascular Center, Harvard Medical School, Boston, Massachusetts; bCardio-
scular and Metabolic Preventive Clinic, Department of Endocrinology, Odense University Hospital, Odense, Denmark; cBariatric
d Metabolic Institute, Cleveland Clinic, Cleveland, Ohio; dObesity, Metabolism and Nutrition Institute, Massachusetts General
spital, Boston, Massachusetts; eLi Ka Shing Knowledge Institute, St. Michael’s Hospital, University of Toronto, Toronto,
tario, Canada; and the fDepartment of Metabolic and Bariatric Surgery, Diabetes and Nutritional Science Division, King’s
llege Hospital, London, United Kingdom. Dr. Pareek has served on the advisory board of and received speaker’s honoraria from
traZeneca. Dr. Schauer has served on the advisory boards of The Medicines Company, GI Dynamics, Neurotronic, and Pacira;
s been a consultant for Ethicon, The Medicines Company, and Novo Nordisk; and has received research support from Ethicon,
National Institutes of Health, Medtronic, and Pacira. Dr. Leiter has received research funding from, has provided continuing
dical education on behalf of, and/or has acted as an adviser to Amgen, AstraZeneca, Boehringer Ingelheim, Eisai, Eli Lilly,
perion, GlaxoSmithKline, Janssen, Merck, Novo Nordisk, Sanofi/Regeneron, Servier, and The Medicines Company. Dr. Rubino
s served on the scientific advisory boards of Fractyl and GI Dynamics; has received consulting fees from Ethicon and Medtronic;
s received speaker’s honoraria from Ethicon and Novo Nordisk; and has received grants from the National Institute for Health
search (UK) and Ethicon. Dr. Bhatt has served on the advisory boards of Cardax, Elsevier Practice Update Cardiology, Medscape
rdiology, and Regado Biosciences; has served on the board of directors of the Boston VA Research Institute and the Society of
rdiovascular Patient Care; has been Chair of the American Heart Association Quality Oversight Committee; has served on the
ta monitoring committees of Cleveland Clinic, Duke Clinical Research Institute, Harvard Clinical Research Institute, Mayo
nic, and Population Health Research Institute; has received honoraria from the American College of Cardiology (senior associate
itor, Clinical Trials and News, ACC.org), Belvoir Publications (Editor-in-Chief, Harvard Heart Letter), Duke Clinical Research
titute (clinical trial steering committees), Harvard Clinical Research Institute (clinical trial steering committee), HMP Com-
nications (Editor-in-Chief, Journal of Invasive Cardiology), Journal of the American College of Cardiology (guest editor; associate
itor), Population Health Research Institute (clinical trial steering committee), Slack Publications (chief medical editor,
rdiology Today’s Intervention), Society of Cardiovascular Patient Care (secretary/treasurer), and WebMD (continuing medical
ucation steering committees), Clinical Cardiology (deputy editor), NCDR-ACTION Registry Steering Committee (chair), and VA
RT Research and Publications Committee (chair); has received research funding from Amarin, Amgen, AstraZeneca, Bristol-
ers Squibb, Chiesi, Eisai, Ethicon, Forest Laboratories, Ironwood, Ischemix, Lilly, Medtronic, Pfizer, Roche, Sanofi, and The
dicines Company; has received royalties from Elsevier (editor, Cardiovascular Intervention: A Companion to Braunwald’s Heart
ease); has been site co-investigator for Biotronik, Boston Scientific, and St. Jude Medical; has been a trustee of the American
llege of Cardiology; and has conducted unfunded research for FlowCo, Merck, PLx Pharma, and Takeda. Dr. Kaplan has
orted that he has no relationships relevant to the contents of this paper to disclose.
nuscript received September 15, 2017; revised manuscript received December 13, 2017, accepted December 15, 2017.

AB BR E V I A T I O N S
AND ACRONYM S
AGB = adjustable gastric
banding
BMI = body mass index
BPD = biliopancreatic diversion
BPDDS = biliopancreatic
diversion with duodenal switch
CI = confidence interval
HbA1c = glycated hemoglobin
HR = hazard ratio
OR = odds ratio
RYGB = Roux-en-Y gastric
bypass
SG = sleeve gastrectomy
T1DM = type 1 diabetes
mellitus
T2DM = type 2 diabetes
mellitus
J A C C V O L . 7 1 , N O . 6 , 2 0 1 8 Pareek et al.F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7 Metabolic Surgery: Weight Loss, Diabetes, and Beyond
671
T he worldwide prevalence of obesity, character-ized by a body mass index (BMI) $30 kg/m2,has more than doubled from approximately
5% in 1975 to 13% in 2014 (1,2). About 4% of personsare severely obese (BMI $35 kg/m2), whereas 1%have morbid obesity (BMI $40 kg/m2). Assumingunaltered trends, as much as one-fifth of the worldpopulation may have obesity by 2025 (1). In the UnitedStates, more than one-third of adults have obesity,with considerable differences in prevalence depend-ing on race and socioeconomic status (3).
Obesity is a well-known risk factor for type 2 dia-betes mellitus (T2DM) (2). Thus, there has been aparallel increase in the prevalence of T2DM, currentlystanding at 9% worldwide and projected to reachw12% by 2025 (4). When the growing population istaken into account, the global burden of diabetes islikely to rise by more than 50% in the next decade(4,5). The metabolic abnormalities associated withobesity increase the risk of cardiovascular disease,including coronary artery disease and heart failure(6). Indeed, most of the w7% of deaths for which aBMI above 25 kg/m2 appears responsible can berelated to cardiovascular disease or T2DM (2). Theunderlying mechanisms have not been fully eluci-dated, but they may include metabolic, hemody-namic, and inflammatory effects of having anincreased adipose tissue mass (6).
Regardless of how achieved, weight loss has thepotential to mitigate the adverse effects of obesity(6). The purpose of this review is to describecontemporary metabolic surgical procedures, theirindications, and the effects of these procedures onweight loss, glycemic outcomes, cardiovascular out-comes, and mortality among adult individuals.
MEDICAL MANAGEMENT OF OBESITY
Although behaviorally based treatments can deliverstatistically significant weight loss, the magnitude isgenerally modest, and the weight loss is often notdurable (7). A 2014 meta-analysis by Dombrowskiet al. (8) showed a significant, but small difference in1-year weight loss of 1.6 kg with diet and physicalactivity compared with a control group. Conversely,the randomized Look AHEAD (Action for Health inDiabetes) trial (9) provided an example of a successfullifestyle intervention program. Among overweight orobese individuals with T2DM, one-half of thoseassigned to intensive lifestyle intervention (caloriegoal of 1,200 to 1,800 kcal daily and $175 min ofmoderate intensity physical activity weekly) had aclinically meaningful weight loss of $ 5% (mean 4.7%)of their initial weight at 8 years as compared with
approximately one-third of patients in thecontrol group (9). Sustained, modest weightloss with lifestyle improvement versus con-trol was also seen at 10 years in the FinnishDiabetes Prevention Study, but not at 10-yearfollow-up in the Diabetes Prevention Program(10,11).
Healthy lifestyle measures should be pro-moted in all individuals as primary, second-ary, and tertiary prevention for overweight orobesity and associated complications (12,13).In patients with obesity, the major compo-nents of lifestyle therapy consist of reducedcalorie intake, physical activity, and behav-ioral interventions. The energy deficit shouldgenerally be w500 to 750 kcal daily (12,13).Moderate aerobic exercise of >150 min perweek, distributed over 3 to 5 days, combinedwith resistance exercise 2 to 3 times perweek, is recommended. Behavioral changes
(e.g., self-monitoring and goal setting) should beincluded as part of the intervention. The weight lossgoal is 10% in subjects with pre-diabetes or themetabolic syndrome and at least 5% to 15% in thosewho have T2DM (13).Combining weight loss drugs with lifestyle inter-vention can produce greater weight loss comparedwith lifestyle intervention alone (13,14). These med-ications may reinforce behavioral or lifestyle changes,increase the potential for physical activity, and havebeneficial effects on related comorbidities. Many an-tiobesity drugs have been marketed over the years,but some were later withdrawn because of unac-ceptable adverse effects (15,16). The 5 antiobesityagents currently approved by the U.S. Food and DrugAdministration are orlistat, lorcaserin, naltrexone-bupropion, phentermine-topiramate, and liraglutide(13,17). A 2016 meta-analysis by Khera et al. (18) foundsignificant 1-year weight loss for these drugs in com-parison with placebo, ranging from 2.6 kg with orli-stat to 8.8 kg with phentermine-topiramate.Contemporary guidelines suggest the addition ofantiobesity medication to lifestyle measures inindividuals with BMI $30 kg/m2 or BMI $27 kg/m2
with at least 1 obesity-associated comorbidity who aremotivated, but have failed to lose weight or maintainweight loss by using high-intensity lifestyle inter-vention alone (Table 1) (13,14,17). Drug therapy mayalso be initiated concomitantly with lifestyle therapyin patients with BMI $27 kg/m2 who have (severe)weight-related complications (13). If $5% of bodyweight has not been lost after 3 months of therapy orthere are issues with tolerability or safety, the drugshould be discontinued. If the weight loss criterion is

TABLE 1 Common Cardiovascular and Metabolic
Obesity-Associated Comorbidities
Type 2 diabetes mellitus
Hypertension
Hyperlipidemia
Coronary, cerebral, and peripheral vascular disease
Heart failure
Atrial fibrillation
Venous stasis disease and thromboembolic disorders
Obstructive sleep apnea
Chronic kidney disease
Data from references 12–14, 59, and 104.
Pareek et al. J A C C V O L . 7 1 , N O . 6 , 2 0 1 8
Metabolic Surgery: Weight Loss, Diabetes, and Beyond F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7
672
met, the drug may be continued. Importantly, there isa risk of weight regain when discontinuing pharma-cotherapy, particularly when behavioral measures arenot used. Given the different efficacy and safetyprofiles, there is no general treatment algorithm, andthe choice of agent should be individualized(13,14,17). So far, only liraglutide has demonstratedclinical cardiovascular benefit (19).
In patients with T2DM and overweight or obesity,the choice of glucose-lowering medications shouldconsider their effects on weight. Antidiabetic agentsassociated with weight loss include biguanides(metformin), a-glucosidase inhibitors, sodium-glucose cotransporter-2 inhibitors, glucagon-likepeptide-1 receptor agonists, and amylin analogues.Sodium-glucose cotransporter-2 inhibitors andglucagon-like peptide-1 receptor agonists appear tobe particularly effective. Dipeptidyl peptidase-4 in-hibitors are considered weight neutral, whereas in-sulin, insulin secretagogues (sulfonylureas,meglitinides), and peroxisome proliferator-activatedreceptor agonists are associated with weight gain.Use of medications for comorbid conditions that areassociated with weight gain (e.g., antipsychotic, an-tidepressant, anticonvulsant and glucocorticoidagents) should be kept to a minimum (13,14,17,20).
METABOLIC SURGERY
Gastrointestinal surgery provides the most substantialand sustainable weight loss in individuals with obesity(21). The procedures are collectively referred to asbariatric (from the Greek words baros [weight] andiatrikos [medicine]) or metabolic (when the intent iscardiometabolic risk reduction) surgery and are amongthe most common gastrointestinal procedures. TheInternational Federation for the Surgery of Obesity andMetabolic Diseases reported that almost 580,000metabolic procedures were performed worldwide in2014 (22). The American Society for Metabolic and
Bariatric Surgery estimated that in the United States179,000 metabolic procedures were done in 2013 and196,000 were performed in 2015 (23). The AmericanHeart Association also acknowledges the growingimportance of these techniques (24).
Weight loss and glycemic effects were traditionallythought to be results of caloric restriction (reducedgastric volume) and/or malabsorption of ingested nu-trients, but more recent studies have demonstratedthat changes in the physiology of energy balance andbody fat mass are the primary mechanisms. Indeed,widespread alterations in the secretion and activity ofhormones and neurotransmitters affecting appetite,satiety, energy expenditure, and glucose metabolismin response to these surgical procedures have beenincreasingly recognized (25–27). All contemporaryprocedures can be done laparoscopically and includeRoux-en-Y gastric bypass (RYGB), sleeve gastrectomy(SG), adjustable gastric banding (AGB), and bil-iopancreatic diversion with duodenal switch (BPDDS)(28,29). The principal anatomic alterations from theseprocedures are shown in Figures 1A to 1D.
RYGB comprises w40% of the metabolic operationscurrently performed and is the most frequent pro-cedure in Latin America, including South America(22,28). In this procedure, a w15- to 30-ml proximalgastric pouch is created, separated from the distalstomach. After transection of the jejunum approxi-mately 50 to 75 cm beyond the ligament of Treitz, thegastric pouch is anastomosed to the distal intestinalsegment, and the proximal intestinal segment isanastomosed to the jejunum, approximately 100 to150 cm more distally (Figure 1C). After this procedure,ingested nutrients flow directly from the gastricpouch into the midjejunum and pass through the 100-to 150-cm Roux (alimentary) limb, thereby bypassingthe duodenum and proximal jejunum (29). Theseanatomic changes lead to alterations in the signalingbetween luminal factors and the intestinal mucosa,thus generating neurohumoral effects that furtherlead to alterations in hunger, satiety, energy balance,modest fat malabsorption, and weight loss (27,30–32).
SG has recently replaced RYGB as the mostcommonly performed weight loss procedure world-wide (28). In this procedure, most of the greater cur-vature of the stomach is resected, resulting in atubular stomach that includes the lesser curvaturethat is resistant to stretching. The pylorus is pre-served (Figure 1B) (29). Resection of the greater cur-vature removes most of the oxyntic (endocrine)mucosa of the stomach and leads to alterations inneurohumoral signaling that are strikingly similar tothose observed after RYGB. Surprisingly, thesechanges also lead to accelerated gastric emptying and

FIGURE 1 Contemporary Procedures for Metabolic Surgery
The 4 contemporarymetabolic surgical procedures: (A) adjustable gastric banding; (B) sleeve gastrectomy; (C)Roux-en-Y gastric bypass; and (D)
biliopancreatic diversionwith duodenal switch. Reprintedwith permission from Piche et al (128). Copyright 2015 Canadian Journal of Cardiology.
J A C C V O L . 7 1 , N O . 6 , 2 0 1 8 Pareek et al.F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7 Metabolic Surgery: Weight Loss, Diabetes, and Beyond
673
early exposure of ingested nutrients to the small in-testinal mucosa (27,30,31).
During AGB, a locking silicone ring (band) is placedaround the upper stomach, 1 to 2 cm below thegastroesophageal junction, and connected to a
subcutaneous infusion port through which the banddiameter can be adjusted by injecting or removingsaline. This creates a 30-ml upper gastric pouch(Figure 1A). With AGB, designed to be a less invasive,more purely restrictive operation than RYGB or SG,

TABLE 2 Randomized Controlled Trials of Metabolic Surgery Versus Medical Therapy for Patients With Type 2 Diabetes Mellitus
First Author(Ref. #) Intervention Control
Key InclusionCriteria
SampleSize
PrimaryFollow-UpDuration
Weight Reduction(Intervention vs. Control)
Diabetes Remission(Intervention vs. Control)
Dixon et al. (40) Conventional therapyplus laparoscopicAGB
Conventionaltherapy
Age 20–60 yrsBMI 30–40 kg/m2
T2DM <2 yrs
60 2 yrs 21.1 kg vs. 1.5 kg,p < 0.001
Fasting plasma glucose<126 mg/dl andHbA1c <6.2% withoutantidiabetic drugs:
73% vs. 13%, p < 0.001
Schauer et al.* (41) Intensive medicaltherapy pluseither RYGB orSG (bothlaparoscopic)
Intensivemedicaltherapy
Age 20-60 yrsBMI 27–43 kg/m2
T2DM with HbA1c
>7.0%
150 1 yr RYGB 29.4 kg vs. SG25.1 kg vs. medical5.4 kg
RYGB vs. medical,p < 0.001
SG vs. medical,p < 0.001
RYGB vs. SG, p ¼ 0.02
HbA1c #6.0%:RYGB 42% vs. SG 27% vs.
medical 12%RYGB vs. medical, p ¼ 0.002SG vs. medical, p ¼ 0.008RYGB vs. SG, p ¼ 0.59
Mingrone et al.* (42) Medical therapy pluseitherlaparoscopicRYGB or openBPD
Medical therapy Age 30–60 yrsBMI $35 kg/m2
T2DM $5 yrs withHbA1c $7.0%
60 2 yrs RYGB 33.3% vs. BPD33.8% vs. medical4.7%
RYGB vs. medical,p < 0.001
BPD vs. medical,p < 0.001
Fasting plasma glucose<100 mg/dl andHbA1c <6.5% for at least 1 yrwithout antidiabetic drugs:
RYGB 75% vs. BPD 95% vs.medical 0%
RYGB vs. medical, p < 0.001BPD vs. medical, p < 0.001
Ikramuddin et al.(43)
Intensive medicalmanagement pluslaparoscopicRYGB
Intensivemedicalmanagement
Age 30–67 yrsBMI 30–39.9 kg/m2
T2DM $6 monthswith HbA1c
$8.0% and serumC-peptide>1.0 ng/ml
120 1 yr 26.1% vs. 7.9%,p < 0.001
HbA1c <7.0%, LDL-cholesterol <100 mg/dl,and systolic bloodpressure <130 mm Hg:
49% vs. 19%, p < 0.001
Liang et al. (44) Laparoscopic RYGB Usual care withor withoutexenatide
Age 30–60 yrsBMI >28 kg/m2
T2DM treated withantidiabetic drugsfor >12 months,HbA1c >7.0%,serum C-peptide>0.3 mg/l, andhypertension
108 1 yr Changes in BMI werenot directlyreported
RYGB vs. usual,p < 0.01
RYGB vs. exenatide,p < 0.05
Usual vs. exenatide,p $ 0.05
RYGB 90% vs. usual 0% vs.exenatide 0%
Wentworth et al.(45)
Multidisciplinarydiabetes care pluslaparoscopic AGB
Multidisciplinarydiabetes care
Age 18–65 yrsBMI 25–30 kg/m2
T2DM <5 yrs
51 2 yrs 11.5 kg vs. 1.6 kg,p ¼ 0.002
Fasting plasma glucose<126 mg/dl and 2-h oralglucose tolerancetest <200 mg/dl withoutantidiabetic drugs:
52% vs. 8%, p ¼ 0.001
Courcoulas et al.(46)
RYGB or laparoscopicAGB
Intensivelifestyleweight lossintervention
Age 25–55 yrsBMI 30–40 kg/m2
T2DM with fastingplasma glucose> 126 mg/dl or onantidiabetic drugs
69 1 yr RYGB 26.8 kg vs. AGB17.4 kg vs. lifestyle10.3 kg
RYGB vs. lifestyle,p < 0.001
AGB vs. lifestyle,p ¼ 0.02
RYGB vs. AGB,p ¼ 0.001
HbA1c <5.7%, fasting plasmaglucose #100 mg/dlwithout antidiabetic drugs:
RYGB 17% vs. AGB 23% vs.lifestyle 0%
RYGB vs. lifestyle, p ¼ 0.11AGB vs. lifestyle, p ¼ 0.02RYGB vs. AGB, p ¼ 0.72
Halperin et al. (47) RYGB Intensivemedicaldiabetes andweightmanagementprogram
Age 21–65 yrsBMI 30–42 kg/m2
T2DM >1 yr withHbA1c $6.5% onantidiabetic drugs
38 1 yr Changes in BMI werenot directlyreported
p < 0.001 in favor ofRYGB
HbA1c <6.5% and fastingplasma glucose <126 mg/dl:
58% vs. 16%, p ¼ 0.03
Continued on the next page
Pareek et al. J A C C V O L . 7 1 , N O . 6 , 2 0 1 8
Metabolic Surgery: Weight Loss, Diabetes, and Beyond F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7
674
the original anatomy can be restored by removing theband (29). In general, weight loss after AGB is sub-stantially less than that seen after RYGB or SG, and asmany as 75% of AGB devices require removal for lackof weight loss, substantial weight gain, or esoph-agogastric complications (33). As a result, the use of
AGB has declined substantially over the past decade,and it now accounts for only 5% to 10% of bariatricprocedures in the United States (28).
BPDDS accounts for only about 2% of metabolicprocedure now performed (28). In the originalbiliopancreatic diversion (BPD) procedure, the

TABLE 2 Continued
First Author(Ref. #) Intervention Control
Key InclusionCriteria
SampleSize
PrimaryFollow-UpDuration
Weight Reduction(Intervention vs. Control)
Diabetes Remission(Intervention vs. Control)
Parikh et al. (48) RYGB, SG, or AGB (alllaparoscopic), onthe basis ofpatient’spreference
Intensivemedicalweightmanagement
Age NSBMI 30–35 kg/m2
T2DM
57 6 months 17.3 kg vs. 1.8 kg,p < 0.001
Fasting plasma glucose<126 mg/dl, 2-h oralglucose tolerancetest <200 mg/dl, andHbA1c <6.5% withoutantidiabetic drugs:
65% vs. 0%, p < 0.001
Ding et al. (49) Laparoscopic AGB Intensivemedicaldiabetes andweightmanagementprogram
Age 21–65 yrsBMI 30–42 kg/m2
T2DM >1 yr withHbA1c $6.5% onantidiabetic drugs
45 1 yr Changes in BMI werenot directlyreported
p ¼ 0.03 in favor ofAGB
HbA1c <6.5% and fastingplasma glucose <126 mg/dl:
33% vs. 23%, p ¼ 0.46
Cummings et al. (50) Laparoscopic RYGB Intensivelifestyle andmedicalintervention
Age 25–64 yrsBMI 30–45 kg/m2
T2DM on antidiabeticdrugs
43 1 yr 25.8% vs. 6.4%, p <
0.001HbA1c <6.0% without
antidiabetic drugs:60% vs. 6%, p ¼ 0.002
*Please see Figure 2 for results at 5 years.
AGB ¼ adjustable gastric banding; BMI ¼ body mass index; BPD ¼ biliopancreatic diversion; HbA1c ¼ glycated hemoglobin; LDL ¼ low-density lipoprotein; NS ¼ not specified; RYGB ¼ Roux-en-Y gastricbypass; SG ¼ sleeve gastrectomy; T2DM ¼ type 2 diabetes mellitus.
J A C C V O L . 7 1 , N O . 6 , 2 0 1 8 Pareek et al.F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7 Metabolic Surgery: Weight Loss, Diabetes, and Beyond
675
duodenum is divided from the pylorus, which isremoved, and the ileum is divided as well. The distalileum is subsequently attached to the stomach andthe proximal ileum, thereby delivering enzymes fromthe pancreas and bile from the liver, and the duo-denum is anastomosed to the terminal ileum. Themore commonly performed BPDDS involves apylorus-preserving SG and a proximal duodenojeju-nostomy that causes ingested nutrients to bypass upto 4 m of the duodenum and jejunum (Figure 1D)(29,34). As with RYGB and SG, the primary mecha-nisms of BPDDS appear to be widespread changes inmetabolic physiology that lead to altered appetite andfood preference, decreased nutrient ingestion, fatand protein malabsorption, and profound weight loss.The extent of reduced fat and protein absorption isgreater than that observed with RYGB because of themore extensive intestinal bypass. Pathologicalmacronutrient malabsorption in the form of proteincalorie malnutrition (5%) can occur, but this is pri-marily an adverse effect of the operation correctableby oral protein augmentation (80 to 100 g/day) orshortening the bypassed portion of the small bowel(27,30,35).
WEIGHT LOSS
Gastrointestinal surgery has been demonstrated tohave substantially greater efficacy than lifestyle orbehavioral and pharmacological treatments forobesity (21,36–38). A 2004 meta-analysis of 136studies, 5 of which were randomized, with a totalof 22,094 patients undergoing metabolic surgery
reported a mean 40-kg weight loss (36). Weightreductions for individual procedure types were 43 kgfor RYGB, 29 kg for AGB, and 46 kg for BPDDS; how-ever, there was no information on follow-up dura-tion. Weight loss with SG, the newest technique,appears to range between that of RYGB and AGB (39).
In a more recent meta-analysis of 11 randomizedcontrolled trials with 796 obese patients, metabolicsurgery resulted in a 26-kg greater weight reductionthan nonsurgical treatment (p< 0.001) (21). Controlledtrials that have directly compared surgery with medi-cal treatment in patients with overweight or obesityand T2DM corroborate these findings (Table 2) (40–50).
However, both meta-analyses and individual trialsshould be interpreted in light of their short-term(usually #2 years) duration (51). Studies that havereported long-term (>5 years) outcomes include theprospective, matched SOS (Swedish Obese Subjects)study, in which mean weight loss at 15 years was 27%for gastric bypass and 13% for gastric bandingcompared with 1% for controls (52–54). Similar find-ings were seen at 20 years. Peak weight loss aftersurgery was achieved at 1 year and was 38% and 21%for RYGB and AGB, respectively. Of note, because theSOS study was begun more than 25 years ago, mostsurgical patients in this study underwent vertical-banded gastroplasty, a procedure that is now rarelyperformed. Another observational study showed a21% greater weight loss at 10 years after RYGBcompared with a matched control cohort that did notundergo surgery (55). Finally, 2 randomized trialshave recently reported 5-year outcomes, demon-strating durable weight reduction after RYGB, SG, and

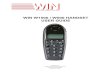
FIGURE 2 The 5-Year Changes in Body Weight, Rates of Diabetes Remission, and Changes in Glycated Hemoglobin, in Randomized Controlled Trials of Patients
With Obesity and Type 2 Diabetes Mellitus
Abso
lute
Red
uctio
n (k
g)
0
P = 0.17
–37.0±13.8
–44.7±22.4
Mingrone et al.
–10.0±12.2
Changes in Body Weight at 5 Years
P < 0.001
P < 0.001
P = 0.01
–23.2±9.6
–18.6±7.5
Schauer et al.
P = 0.003
P = 0.003
–50
–40
–30
–20
–10
–70
–60
–80
A
31
23
P = 0.003
P = 0.002
P = 0.43
0
Perc
enta
ge R
emitt
ed (%
)
80
37
63
P < 0.001
Mingrone et al.0
Diabetes Remission at 5 Years
Schauer et al.
30
40
50
60
70
10
20
0
B
RYGB BPD SG Medical Therapy
Abso
lute
Red
uctio
n (%
)
0.0
P = 0.59
–2.0±1.5
–2.5±1.8
Mingrone et al.
–1.6±1.0
Changes in Glycated Hemoglobin at 5 Years
P = 0.25P = 0.59
P = 0.67
–2.1±1.8
–2.1±2.3
Schauer et al.
P = 0.003P = 0.003
–3.5–4.0
–2.5–3.0
–2.0
–1.0–1.5
–0.5
–5.0–4.5
–6.0–5.5
C
–5.3±10.8
–0.3±2.0
(A) The absolute reductions in body weight (kg) according to study arm in the 2 randomized controlled trials of patients with obesity and type 2 diabetes mellitus that
have reported 5-year outcomes (56,57). The bars denote mean weight reduction, whereas the lines represent the standard deviation. (B) The percentage of patients
who achieved diabetes remission (bars) according to study arm. Definitions of diabetes remission: Mingrone et al. (56): fasting plasma glucose#100 mg/dl and glycated
hemoglobin #6.5% without drug therapy; Schauer et al. (57): glycated hemoglobin #6.5% without drug therapy. The p value in the study by Mingrone et al. (56) was
based on a chi-square test across all 3 groups. The p values in the study by Schauer et al. (57) were adjusted for multiple comparisons. (C) The absolute reductions in
glycated hemoglobin (%) according to study arm. The bars denote mean glycated hemoglobin reduction, whereas the lines represent the standard deviation.
BPD ¼ biliopancreatic diversion; RYGB ¼ Roux-en-Y gastric bypass; SG ¼ sleeve gastrectomy. Data from Mingrone et al. (56) and Schauer et al. (57).
Pareek et al. J A C C V O L . 7 1 , N O . 6 , 2 0 1 8
Metabolic Surgery: Weight Loss, Diabetes, and Beyond F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7
676
BPD (Figure 2A) (56,57). Interestingly, the change inbody weight was more pronounced with RYGB ascompared with SG (57).
DIABETES AND GLYCEMIC CONTROL
A considerable amount of high-quality evidence hasalso accumulated supporting metabolic surgery asan effective means of treating T2DM (21,36–38).These procedures improve glucometabolic profiles
as seen by reductions in glycated hemoglobin(HbA1c) and concomitant increases in circulatingincretin concentrations, insulin sensitivity, and b-cellfunction (58). Many patients with T2DM who undergothese procedures experience complete remission ofthe diabetes, formally defined as having normal HbA1c
or fasting plasma glucose without needing antidia-betic drugs for duration of at least 1 year (59).
Observational evidence for long-term durability ofsurgically achieved glycemic control is mainly

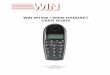
FIGURE 3 Simplified Model of Potential Effects of Metabolic Surgery on
Glucose Metabolism
Type 2 Diabetes Mellitus
Metabolic Surgery
↓Calories ↑Ileal Nutrient Delivery ↑Bile Acids ΔGut Microbiota
↓Weight ↑Incretins ↓Insulin Resistance ↑Insulin Secretion
↓Cardiovascular Events ↓Mortality
Diabetes Remission/Improvement
Several factors appear to drive the metabolic benefits of surgery, including caloric
restriction, increased nutrient delivery to the distal small intestine, increased bile acid
concentrations, and changes in the gut microbiome. These alterations result in weight loss
and favorable hormonal changes. The improvements in glucose metabolism may reduce
cardiovascular events and mortality. [ ¼ increase; Y ¼ decrease; D ¼ change.
J A C C V O L . 7 1 , N O . 6 , 2 0 1 8 Pareek et al.F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7 Metabolic Surgery: Weight Loss, Diabetes, and Beyond
677
derived from the large SOS study (60). In patientswho underwent surgery versus those who did not, the2-year diabetes remission rates, defined as bloodglucose levels lower than 110 mg/dl and no diabetesmedications, were 72% and 16% (p < 0.001), respec-tively, whereas the corresponding rates at 15 yearswere 30% and 7% (p ¼ 0.001) respectively. These in-vestigators also explored the preventive effect ofmetabolic surgery and found a significantly lower15-year risk of T2DM among individuals who under-went surgery compared with a control group(adjusted hazard ratio [HR]: 0.17; 95% confidenceinterval [CI]: 0.13 to 0.21; p < 0.001) (61). Results fromthe SOS study were included in a meta-analysis of 21cohort studies (6,373 individuals) with at least 2 yearsof follow-up that showed an overall 65% chance ofdiabetes remission in patients who underwentsurgery, with the highest remission rate for BPDDS(99%), followed by RYGB (74%), SG (61%), and AGB(33%) (38). Importantly, the included studies useddifferent criteria for diabetes remission.
The meta-analysis of randomized controlledtrials by Gloy et al. (21) also reported a significantlygreater chance of achieving diabetes remission inpatients treated with metabolic surgery than innonsurgically treated controls (relative risk: 22.1;95% CI: 2.3 to 154.3; p ¼ 0.002). Additionally, arecent pooled analysis of randomized controlledtrials including patients with T2DM demonstrated amean 1.14% greater drop in HbA1c after surgical versusmedical treatment (p < 0.001) (62). Results from ran-domized trials of metabolic surgery among patientswith T2DM are summarized in Table 2. Despiteconsiderable variations in study design, includingvaried inclusion criteria and procedures used, resultshave consistently and strongly favored metabolicsurgery (40–50).
The STAMPEDE (Surgical Treatment and Medica-tions Potentially Eradicate Diabetes Efficiently) trialwas a randomized controlled study that examined therole of metabolic surgery in the diabetic population(41). A total of 150 patients with T2DM and BMI of 27to 43 kg/m2 were randomized to RYGB, SG, or inten-sive medical therapy alone. At 1 year, 12% of patientsin the medical therapy group had achieved diabetestreatment targets (HbA1c #6.0%) compared with 42%in the RYGB group (p ¼ 0.002) and 37% in the SGgroup (p ¼ 0.008). The effects of metabolic surgerywere durable, with a substantially greater effect at 5years than medical treatment (Figure 2B) (57,63).
The study by Mingrone et al. (42), in which medicaltherapy was compared with RYGB and BPD in 60patients with T2DM and BMI $35 kg/m2, also showedfavorable outcomes with metabolic surgery. Rates of
diabetes remission (fasting plasma glucose <100 mg/dland HbA1c <6.5% without drug treatment) 2 yearsafter RYGB, BPD, and medical therapy were 75%, 95%,and 0%, respectively (p < 0.001 for both comparisonswith surgery vs. medical therapy). At 5 years, the HbA1c
level was significantly lower in the combinedsurgical group than in the medical group (p ¼ 0.04)(Figure 2C) (56).
Outcomes of metabolic surgery in patients withtype 1 diabetes mellitus (T1DM) are much less studiedcompared with those for T2DM. A 2016 review of 17retrospective case studies including just 107 patientswith T1DM and moderate to severe obesity(BMI >35 kg/m2) demonstrated significant weight loss(BMI decrease w10 kg/m2), reduced insulin re-quirements, and improved HbA1c (reduction of 0.5%)(64). However, there was a concerning incidence ofpost-operative diabetic ketoacidosis as high as 20% to25%, as well as significant hypoglycemia, thatsuggested the need for diligent post-operativeglucose monitoring and management. Furthermore,gastrointestinal dysmotility conditions includingpost-operative ileus, intractable nausea and

Pareek et al. J A C C V O L . 7 1 , N O . 6 , 2 0 1 8
Metabolic Surgery: Weight Loss, Diabetes, and Beyond F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7
678
vomiting, and acute gastric remnant dilation havebeen reported at higher rates compared with thoseseen in patients with T2DM. Given that many patientswith T1DM have underlying autonomic neuropathyand gastroparesis, such occurrences should be antic-ipated and managed accordingly. Because of thecurrent paucity of outcome data, a clear role ofmetabolic surgery for T1DM in severely obese patientsis yet to be determined.
MECHANISMS OF ACTION
After metabolic surgery, diabetes starts to improvewithin days to weeks, whereas weight loss occursmuch more slowly (65). This suggests that themechanisms of metabolic benefit extend beyond themagnitude of weight loss alone, a concept that hasbeen demonstrated in animal models even at long-term follow-up (66). The pathophysiological alter-ations involved are not completely understood, butthe major paradigm revolves around the pivotalphysiological role of the gastrointestinal tract inglucose homeostasis (Figure 3) (30,67,68).
Caloric restriction with or without metabolic sur-gery can lead to depletion of liver fat within a week,followed by improved hepatic insulin sensitivity andclearance (69,70). In fact, short term improvementsin insulin sensitivity and b-cell function are similarfor very low-calorie diets and RYGB (69). After sur-gery, post-load insulin secretion is also enhanced,possibly secondary to increased glucagon-like pep-tide-1 secretion observed after RYGB, SG, and BPDDS(71,72). The accelerated food entry into the distalportion of the small intestine with a resultantincreased delivery of undigested nutrients may beinvolved in the alteration of hormonal responses(30,73). Glucagon-like peptide-1 stimulates post-prandial secretion of insulin and inhibits that ofglucagon (67). It also slows gastric emptying andenhances satiety, thus leading to weight loss, and theanorexigenic effects may be augmented by aconcomitantly increased secretion of peptide YY(26,72,74). The rapid distention of the small intestinemay further diminish appetite (75). Increasedglucagon-like peptide-1 secretion and insulin secre-tion may possibly be seen after a very low-caloriediet, but studies have reported inconsistent findings(69,70,76).
Changes in inflammatory and adipokine profilesmay also affect glucose metabolism, although theirroles after metabolic surgery appear to be lessimportant (77). Both C-reactive protein andinterleukin-6 levels decrease considerably, in
parallel with the increased insulin sensitivity (78).Concentrations of the satiety-inducing hormone lep-tin decrease because of its close correlation with totalbody fat mass (79–81). Persons with obesity havedramatically increased leptin levels, but they alsohave leptin resistance, which counterbalances theotherwise catabolic effects of leptin. Interestingly,even though weight loss through calorie restrictionincreases leptin sensitivity, metabolic surgery doesnot seem to have such an effect (82). Concentrationsof ghrelin, an appetite-stimulating hormone, initiallydecrease, but they subsequently increase andapproach pre-operative levels (72,81). Anotherpotentially important concept is the deposition ofectopic, including visceral, fat, which is associatedwith many metabolic abnormalities in individualswith obesity. Patients whose T2DM, hypertension,and other conditions resolve after metabolic surgeryappear to have greater ectopic fat mobilization thando patients whose same disorders do not resolve, aneffect that is independent of the degree ofweight loss (83,84).
Finally, other factors may include increased bileacid concentrations and altered gut microbiota(30,68). Serum concentrations of bile acids increaseafter RYGB and are positively associated with peaksecretion of glucagon-like peptide-1. Therefore, it hasbeen suggested that bile acids directly stimulateglucagon-like peptide-1 secretion (30). Patients withobesity have an increased Firmicutes to Bacteroidesbacteria ratio compared with lean control subjects,and this difference disappears after weight loss. Othergut changes associated with metabolic surgery mayfurther alter the microbiome. Because its compositionplays an important role in energy extraction, the gutmicrobiota could potentially be involved in thedevelopment of obesity and associated metaboliccomplications (30).
Most of the pathophysiological evidence comesfrom subjects who have undergone RYGB. Indeed,time to diabetes remission is longer, and the corre-lation between weight loss and improved glycemiccontrol is seemingly stronger, among patients un-dergoing AGB, findings suggesting that unlike theother metabolic procedures, AGB does not inducesignificant weight loss independent effects onglucose homeostasis (40,42). AGB also does not affectglucagon-like peptide-1 concentrations, and its ef-fects on inflammation and adipokines are far lesspronounced than after the other procedures (80,85).It has been suggested that the effects of AGB are notthe result of mechanical restriction, but rather reflectenhanced satiety (86).

TABLE 3 Potential Complications Associated With Specific Types
of Metabolic Surgery
Complications RYGB SG AGB BPDDS
Stricture or stenosis � � �Band erosion, leakage, or slippage �Gallstone � � � �Gastrogastric fistula �Gastric remnant dilation �Marginal ulcer � �Nutritional deficiencies � � (�) �Small bowel obstruction � �Reflux � � �
Parentheses indicate that the risk is not zero but is lower than the other procedureswith an � sign. Data from Hanipah and Schauer (29) and Schauer et al. (62).
BPDDS ¼ biliopancreatic diversion with duodenal switch; � ¼ potentialcomplication; other abbreviations as in Table 2.
FIGURE 4 General Complications of Metabolic Surgery
0 2 4 6
0.1-5.6
1.0-4.0
0.3-1.3
0.1-0.3
Approximate Frequency (%)
Bleeding
Cardiopulmonary
Death
Sepsis
Important general complications of metabolic surgery. The bars denote the full range of
the estimated frequencies. Data from Hanipah and Schauer (29) and Schauer et al. (62).
J A C C V O L . 7 1 , N O . 6 , 2 0 1 8 Pareek et al.F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7 Metabolic Surgery: Weight Loss, Diabetes, and Beyond
679
CARDIOVASCULAR RISK AND MORTALITY
There has been a growing interest in exploring theinfluence of metabolic surgery on cardiovascularoutcomes (24). Randomized trials have now shownpromising long-term changes in the burden of car-diovascular risk factors (56,57), whereas informationon subclinical damage and, in particular, cardiovas-cular events and mortality is mainly derived fromobservational studies (65,87–89).
Vest et al. (87) conducted a systematic review of 73cardiovascular risk factor studies (3 randomized) witha total of 19,543 individuals who underwent metabolicsurgery. These investigators found significant re-ductions in traditional cardiovascular risk factors, asseen by resolution or improvement of diabetes in 73%,hypertension in 63%, and hyperlipidemia in 65%,during an average 4.8-year follow-up period.A minority of the included studies reported C-reactiveprotein levels, which decreased by 73% post-operatively. Finally, imaging studies showed im-provements in left ventricular structure and diastolicfunction, independent of improvements in bloodpressure, benefits that may extend to systolic functionand coronary artery calcium (87,90,91).
There is increasing evidence that the reduced car-diovascular risk factor burden after metabolic surgerytranslates to better patient outcomes because obser-vational studies have consistently shown reductions incardiovascular events and mortality (77). For instance,a recent meta-analysis of 4 observational studies withcontrol groups found that patients with a BMI$30 kg/m2 who were undergoing metabolic surgeryhad significantly lower risks of all-cause mortality(odds ratio [OR]: 0.55; 95%CI: 0.46 to 0.65),myocardialinfarction (OR: 0.71; 95% CI: 0.54-0.94), stroke(OR: 0.66; 95% CI: 0.49 to 0.89), and the composite of
myocardial infarction or stroke (OR: 0.67; 95% CI: 0.54to 0.83) as compared with controls (88).
At a median of 14.7 years, the observational SOSstudy had the longest follow-up duration of theincluded studies (53). Sjöström et al. (92) reportedsignificantly reduced risks of cardiovascular mortality(adjusted HR: 0.47; 95% CI: 0.29 to 0.76; p¼0.002) andof composite cardiovascular events (fatal or nonfatalmyocardial infarction or stroke) (adjusted HR: 0.67;95%CI: 0.54 to 0.83; p<0.001) withmetabolic surgery.These investigators also demonstrated a reduction inall-cause mortality during an average of 10.9 years(adjusted HR: 0.71; 95% CI: 0.54 to 0.92; p ¼ 0.01) (92).Finally, surgery lowered the risk of macrovascularoutcomes (coronary artery disease, cerebrovasculardisease, or peripheral artery disease) among patientswith T2DM at baseline (adjusted HR: 0.68; 95% CI: 0.54to 0.85; p ¼ 0.001) (60).
Favorable outcomes for other types of cardiovas-cular events that are associated with obesity anddiabetes have been reported as well. The SOS in-vestigators recently reported a significantly lowerlong-term risk of atrial fibrillation in surgically versusmedically treated patients (HR: 0.71; 95% CI: 0.60 to0.83; p < 0.001) (93). A second large Scandinaviancohort study further showed a decreased risk of heartfailure in patients with obesity who were treatedsurgically versus those who were not (HR: 0.54; 95%CI: 0.36 to 0.82), and similar findings were noted in alarge U.S. case-control study (p ¼ 0.008) (89,94).
COMPLICATIONS
The health benefits of metabolic surgery must becarefully weighed against the possible complications

TABLE 4 Vitamin and Mineral Supplementation After
Metabolic Surgery
Vitamin B1: $12 mg (preferably 50 mg) daily
Vitamin B12: oral/sublingual 350–500 mg daily, subcutaneous/intramuscular 1,000 mg monthly, or nasal, targeted tonormal levels
Folate: 400–800 mg (800–1,000 mg in women of childbearingage) daily
Iron: $18 mg (45–60 mg after RYGB, SG, or BPDDS or in menstruatingfemale patients) daily
Calcium citrate: 1,200–1,500 mg (1,800–2,400 mg after BPDDS) daily
Vitamin D: 3,000 IU daily, titrate serum 25-hydroxyvitamin D levelsto >30 ng/ml
Vitamin A: 5,000 IU (5,000-10,000 IU after RYGB or SG, 10,000 IUafter BPDDS) daily
Vitamin E: 15 mg daily
Vitamin K: 90–120 mg (300 mg after BPDDS) daily
Zinc: 8–11 mg (8–22 mg after RYGB, 16–22 mg after BPDDS) daily
Copper: 1 mg (2 mg after RYGB or BPDDS) daily
Data from Mechanick et al. (104) and Parrott et al. (105).
Abbreviations as in Tables 2 and 3.
Pareek et al. J A C C V O L . 7 1 , N O . 6 , 2 0 1 8
Metabolic Surgery: Weight Loss, Diabetes, and Beyond F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7
680
(Table 3, Figure 4) (29,37,62,95,96). Potential risk fac-tors for such complications includemale sex, smoking,older age, greater BMI, increasing number of comor-bidities, procedure type, and prolonged operative time(95,97–99). Fortunately, over the past 2 decades, theoverall risk of these procedures has declined as a resultof increased surgical experience and training, use oflaparoscopic approaches, improved perioperative andpost-operative care, and mandatory quality re-quirements and reporting (100,101).
A 2007 meta-analysis reported a total 30-day mor-tality rate of 0.28% and amortality rate from 30 days to2 years of 0.35% for metabolic surgery (102). The riskwas higher with BPDDS than with RYGB, SG, and AGB.It was also higher for open versus laparoscopic surgery.Subsequently published observational studies,including the LABS (Longitudinal Assessment of Bar-iatric Surgery) study, have confirmed these findings(95,96,98). In addition, data from the U.S. NationwideInpatient Sample database have shown a stable 0.1%risk of in-hospital death (103). Themost common causeof death is venous thromboembolism, followed byother cardiopulmonary events and complications ofgastrointestinal leaks (95,98).
The LABS consortium reported a 30-day morbidityrate of w4%, whereas the Nationwide InpatientSample data showed an in-hospital morbidity rate ofw9% (95,103). These nonfatal complications includecardiovascular and pulmonary events, anastomoticleakage, bowel obstruction, internal hernia,infection, hemorrhage, and nutritional deficiency(37,95,97,98,103).
Nutritional deficiencies resulting from inade-quate intake, malabsorption, or both comprise themost common long-term complications after meta-bolic surgery and more often occur after BPDDS orRYGB than after SG or AGB (104,105). Manymicronutrient deficiencies, especially of vitamin D,calcium, and iron, are prevalent pre-operatively inpatients with obesity and are likely to persist orworsen post-operatively. Anemia has been reportedin up to three-fourths of all cases and is mainlycaused by deficiencies of iron and vitamin B12, aswell as inflammation (106,107). Post-operative de-ficiencies of folate, selenium, zinc, copper, and vi-tamins A, B1, B2, B6, C, D, E, and K can also occur,although there is wide variation in reported oc-currences (104,105). Low vitamin D and calciummay lead to a significant reduction in bone mineraldensity (108). Correction of these micronutrientdeficiencies is generally possible with appropriatevitamin, iron, and calcium supplementation, butregular lifelong follow-up is required to ensureoptimal nutritional status (104,105). Guideline rec-ommendations for post-operative supplementationare summarized in Table 4. Besides calcium,vitamin D, and vitamin B12, the deficiencies canoften be corrected with 1 (AGB) or 2 (other pro-cedures) multivitamin tablets.
Severe hypoglycemia is another important long-term complication. A Swedish cohort study foundthat the risk of this condition more than doubled afterRYGB, although the absolute risk remained low at0.2% (109). Interestingly, AGB did not increase therisk of hypoglycemia. The underlying mechanismsare unclear (110).
CURRENT GUIDELINES AND
CHOICE OF PROCEDURE
Recent clinical guidelines have stated that metabolicsurgery should be recommended in patients with aBMI $40 kg/m2 without concomitant medical prob-lems and in patients with a BMI $35 kg/m2 who haveat least 1 severe obesity-associated comorbidity,(e.g., poorly controlled T2DM) (Table 1)(12,13,17,59,104). Comorbidity prevalence in patientswith a BMI of 35 to 39.9 kg/m2 is high, approximately50%, 10%, and 20% for hypertension, diabetes, anddyslipidemia, respectively (111). Metabolic surgeryshould also be considered in patients with a BMI of30 to 34.9 kg/m2 and poorly controlled T2DM(17,59,104). Because of the differences in the re-lationships among BMI, visceral fat, and cardiovas-cular and metabolic risk in patients of Asian descent,

FIGURE 5 Algorithm for the Treatment of Type 2 Diabetes Mellitus, as Suggested by the International Diabetes Organizations
Patients withType 2 Diabetes
ObeseBMI ≥30 kg/m2
or ≥27.5 for Asians
Class III ObeseBMI ≥40 kg/m2
or ≥37.5 for Asians
Expedited Assessmentfor Metabolic Surgery Optimal Lifestyle and Medical Rx Optimal Lifestyle and Medical Rx
(including injectable meds and insulin)
Class II ObeseBMI 35.0-39.9 kg/m2
or 32.5-37.4 for Asians
Class II Obesewith Poor
Glycemic Control
RecommendMetabolic Surgery
ConsiderMetabolic Surgery
NonsurgicalTreatment
Class II Obesewith Adequate
Glycemic Control
Class I Obesewith Poor
Glycemic Control
Class I Obesewith Adequate
Glycemic Control
Class I ObeseBMI 30.0-34.9 kg/m2
or 27.5-32.4 for Asians
NonobeseBMI <30 kg/m2
or <27.5 for Asians
Flowchart depicting an algorithm for treatment of type 2 diabetes mellitus, according to obesity class and degree of glycemic control, as suggested by international
diabetes organizations. The indications are intended for patients who are considered appropriate candidates for elective surgery. Reprinted with permission from
Rubino et al. (59). Copyright 2016 by Diabetes Care. BMI ¼ body mass index; Meds ¼ medications; Rx ¼ treatment.
J A C C V O L . 7 1 , N O . 6 , 2 0 1 8 Pareek et al.F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7 Metabolic Surgery: Weight Loss, Diabetes, and Beyond
681
it has been suggested that BMI cutoffs be lowered by2.5 kg/m2 in this population (17,59). Figure 5 sum-marizes the role of metabolic surgery in treatingT2DM, as recently proposed by the internationaldiabetes organizations (59).
Candidates for metabolic surgery should be care-fully selected using a multidisciplinary teamapproach. Patients must have an acceptable operativerisk, be motivated to lose weight, and have respondedinadequately to behaviorally based treatment. How-ever, optimization of glycemic control should beattempted. Metabolic surgery is contraindicated inpatients with current alcohol or substance abuse,uncontrolled psychiatric disorder, poor understand-ing of the risks and benefits, and lack of commitmentto nutritional supplementation and long-term post-operative follow-up (17,59,104).
There is insufficient evidence to recommend aspecific metabolic procedure clearly over another forindividual patients (59,104). For now, the choice de-pends on the patient’s preference and characteristics,local expertise, and treatment goals, including care-fully balancing the risk of long-term nutritional andgastrointestinal sequelae with that of achievingsatisfactory glycemic control and cardiovascular riskreduction. Scoring tools, such as the IndividualizedMetabolic Surgery Score, may assist in clinical deci-sion making (112). Furthermore, cost issues and ac-cess to surgery may play important roles. Although SGis now the most commonly performed metabolicprocedure, presumably because of its simpler tech-nique as compared with RYGB, the use of thesesurgical procedures is still much more prevalent inhigh-income countries. For example, the United

CENTRAL ILLUSTRATION Potential Approach to Patients With Varying Degrees of Obesity and Type 2Diabetes Mellitus
Patient with Obesity and/orType 2 Diabetes Mellitus
Lifestyle ModificationConsider Antidiabetic DrugsConsider Weight Loss Drugs
Assess Severity
Class I Obesity andAdequate Glycemic Control
Lifestyle and MedicalTreatment
Consider SG, RYGB, orAGB*
Recommend SG, RYGB, orAGB*
Recommend SG, RYGB,AGB*, or BPDDS
Class I Obesity andPoor Glycemic Control
Class II Obesity withSignificant Comorbidity or
Poor Glycemic ControlClass III Obesity
Pareek, M. et al. J Am Coll Cardiol. 2018;71(6):670–87.
Flowchart depicting a potential algorithm for treatment of patients with obesity and/or type 2 diabetes mellitus. Lifestyle modification is indicated for all patients,
whereas drug treatment may be considered. Metabolic surgery and its degree of invasiveness are based on the degree of obesity and glycemic control. *AGB is steadily
declining in popularity because of high revision rates and suboptimal long-term weight loss. AGB ¼ adjustable gastric banding; BPDDS ¼ biliopancreatic diversion with
duodenal switch; RYGB ¼ Roux-en-Y gastric bypass; SG ¼ sleeve gastrectomy.
Pareek et al. J A C C V O L . 7 1 , N O . 6 , 2 0 1 8
Metabolic Surgery: Weight Loss, Diabetes, and Beyond F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7
682
States accounts for approximately one-third of suchprocedures performed worldwide (22). In terms ofbariatric-metabolic efficacy, BPDDS is the mosteffective, followed by RYGB, SG, and AGB, respec-tively (41,42,46,48,56,57,59,63). As alluded to in theprevious section, a reverse gradient is seen for safety.Revision rates for RYGB and SG are similar, but SG iseasier to perform and slightly safer because it doesnot involve multiple anastomoses. AGB is associatedwith low perioperative complication rates but highrevision rates, and it is the least effective for weightloss. BPDDS should be reserved for those patientswith extreme obesity (e.g., BMI >60 kg/m2) becauseof the substantial risk of nutritional deficits; in pa-tients with the most severe obesity, this procedure isoften performed in 2 steps, with an initial SG, fol-lowed after a period of weight loss by addition of theduodenojejunal bypass component (29,59,65,104).
Patients who undergo metabolic surgery need long-term monitoring. This is best managed by a
multidisciplinary team approach similar to that usedpre-operatively. The frequency of follow-up dependson the procedure and the burden of comorbidities. Theminimum recommended surgical and nutritionalfollow-up frequency is every 6 months during the first2 years and annually thereafter, whereas glycemiccontrol should generally be monitored with the sameintervals as for medically treated patients. Insulin andsulfonylurea dosages should be progressively reducedto avoid hypoglycemia, and cessation of antidiabeticmedication may be considered if a normal HbA1c levelhas been observed for at least 6 months. The healthylifestyle measures described should be maintainedafter surgery. Patients who fail to lose weight or whoregain it should be evaluated for their compliance withlifestyle or behavioral measures, including maladap-tive eating patterns, use of medications that mayadversely affectweight, psychological complaints, andmedical conditions or surgical complications associ-ated with weight gain (17,59,104).

J A C C V O L . 7 1 , N O . 6 , 2 0 1 8 Pareek et al.F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7 Metabolic Surgery: Weight Loss, Diabetes, and Beyond
683
CONCLUSIONS AND PERSPECTIVES
Metabolic surgery is highly effective in obtaining sig-nificant and durable weight loss at a low perioperativerisk when appropriate patient selection and long-termfollow-up are ensured. High-quality evidence fromrandomized controlled trials shows the superiority ofsurgical over medically based treatment for enhancingglycemic control and achieving diabetes remission.Observational data suggest that these benefits lead toless adverse cardiovascular risk profiles with a conse-quent reduction in macrovascular events and mortal-ity. Additional benefits may include improved qualityof life and a reduced risk for other obesity-related anddiabetes-related disorders, including microvasculardisease, sleep apnea, fatty liver disease, andmalignantdiseases (60,113–115).
Comparable glycemic benefits of surgery havebeen observed in patients with lower initial BMIs<35 kg/m2. In the STAMPEDE trial, the antidiabeticeffects of surgery were the same in patients withbaseline BMIs higher and lower than 35 kg/m2
(41,57,63). Shah et al. (116) demonstrated a substantialbenefit of RYGB in Indian patients with an initialBMI <35 kg/m2, and similar BMI-independent benefitsof surgery have been established in meta-analyses(117,118). As a result, current guidelines support theuse of metabolic surgery in individuals with mildobesity and poorly controlled T2DM (12,59,104).Although the antidiabetic effects of AGB appear lesspowerful than those of other metabolic operations, 1study nonetheless demonstrated the ability of AGB toinduce remission of T2DM, defined as fastingglucose <126 mg/dl and post-load glucose during a2-h oral glucose tolerance test <200 mg/dl, at least2 days after cessation of antidiabetic medication,among overweight (BMI 25 to 30 kg/m2) individuals(45). The utility of metabolic surgery in specific dis-ease populations, such as those with congestive heartfailure, and defining the benefit-to-risk profile of eachprocedure for treating diabetes in different pop-ulations, need further investigation. Conclusive dataregarding end-organ damage, particularly renal out-comes (e.g., urinary albumin excretion), are also notavailable, but the role of metabolic surgery for suchendpoints is currently being investigated (119–121).Similarly, although surgery appears to have beneficialeffects on blood pressure and lipid levels, some pa-tients do not experience a reduction in risk factorburden, and durability is uncertain (122). Reportedpredictors of nonresolution of hypertension includeolder age, concomitant diabetes, less weight loss, andAfrican-American race (123). With respect to lipid
levels, matters may be complicated by alterations insome, but not all, cholesterol subtypes, as well as theeffect of dietary patterns (124,125). Finally, althoughthese procedures appear to be beneficial with respectto weight loss and cardiometabolic risk reduction inadolescents with obesity, more studies of long-termefficacy and safety in this setting are needed (126).
In some patients, the bariatric and metabolic ef-fects of gastrointestinal surgery may diminish overtime, with relapse of T2DM in patients who hadinitially achieved full remission. Even in these pa-tients, however, the recurrent diabetes is generallyfar less severe, requires less intensive medicationregimens, and is more easily controlled than beforethe metabolic surgery. Patients who are older, useinsulin, regain weight, or have greater baseline waistcircumference, longer diabetes duration, or poor pre-operative glycemic control appear to be at highest riskfor late post-operative diabetes recurrence(65,117,127). Even in the setting of diabetes relapse,however, a legacy effect may exist. Finally, the effectof post-operative antidiabetic medications in patientswhose diabetes failed to remit or recurred late aftersurgery is currently being examined (Canagliflozin vs.Placebo for Post Bariatric Patients With PersistentType 2 Diabetes [CARAT]; NCT02912455). Many of theunanswered questions about metabolic surgery andlong-term risk will be clarified through long-termcardiovascular outcomes data from randomized tri-als (Surgical Versus Medical Treatment of Insulin-Dependent Type 2 Diabetes Mellitus in Patients Witha Body Mass Index Between 26 and 35 kg/m2 [Diasurg 2];DRKS00004550). In addition, a more thorough un-derstanding of the mechanistic alterations associatedwith metabolic surgery could help enhance its effec-tiveness and durability and help define which oper-ations are most appropriate in specific patients.
The traditional concept of reserving metabolicsurgery for persons exceeding a certain BMI thresholdis rapidly evolving. Safer procedures and expandedtreatment indications have added to the complexitiesof choosing the right procedure for the right patient.Potentially, the future approach for patients withvarying degrees of obesity and T2DM will be lifestylemodification for all, pharmacological treatment ofobesity and T2DM for many, and metabolic surgeryfor the growing number of patients whose metabolicdisease is severe or refractory to less invasive ap-proaches. Thus, much as coronary artery disease istreated with medical therapy, percutaneous coronaryintervention, and coronary artery bypass grafting onthe basis of the severity of disease, comorbidities, andresponse to noninvasive measures, a similar approach

Pareek et al. J A C C V O L . 7 1 , N O . 6 , 2 0 1 8
Metabolic Surgery: Weight Loss, Diabetes, and Beyond F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7
684
is evolving for the treatment of obesity and T2DM(Central Illustration). Because both the prevalence andthe severity of these disorders are still increasing, andas the global burden rises, metabolic surgery is likelyto play an increasingly important role in improvingcardiovascular health.
ADDRESS FOR CORRESPONDENCE: Dr. Deepak L.Bhatt, Brigham and Women’s Hospital Heart &Vascular Center, Harvard Medical School, 75 FrancisStreet, Boston, Massachusetts 02115. E-mail:[email protected].
RE F E RENCE S
1. NCD Risk Factor Collaboration (NCD-RisC).Trends in adult body-mass index in 200 coun-tries from 1975 to 2014: a pooled analysis of1698 population-based measurement studieswith 19.2 million participants. Lancet 2016;387:1377–96.
2. GBD 2015 Obesity Collaborators, Afshin A,Forouzanfar MH, et al. Health effects of over-weight and obesity in 195 countries over 25 years.N Engl J Med 2017;377:13–27.
3. Ogden CL, Carroll MD, Kit BK, Flegal KM.Prevalence of childhood and adult obesity in theUnited States, 2011-2012. JAMA 2014;311:806–14.
4. NCD Risk Factor Collaboration (NCD-RisC).Worldwide trends in diabetes since 1980: a pooledanalysis of 751 population-based studies with 4.4million participants. Lancet 2016;387:1513–30.
5. International Diabetes Federation. DiabetesAtlas, 8th edition. 2017. Available at: www.diabetesatlas.org/. Accessed December 22, 2017.
6. Poirier P, Giles TD, Bray GA, et al. Obesity andcardiovascular disease: pathophysiology, evalua-tion, and effect of weight loss: an update of the1997 American Heart Association scientific state-ment on obesity and heart disease from theObesity Committee of the Council on Nutrition,Physical Activity, and Metabolism. Circulation2006;113:898–918.
7. Tuah NA, Amiel C, Qureshi S, Car J, Kaur B,Majeed A. Transtheoretical model for dietary andphysical exercise modification in weight lossmanagement for overweight and obese adults.Cochrane Database Syst Rev 2011;(10)CD008066.
8. Dombrowski SU, Knittle K, Avenell A, Araujo-Soares V, Sniehotta FF. Long term maintenance ofweight loss with non-surgical interventions inobese adults: systematic review and meta-analyses of randomised controlled trials. BMJ2014;348:g2646.
9. Look AHEAD Research Group. Eight-yearweight losses with an intensive lifestyle inter-vention: the Look AHEAD study. Obesity (SilverSpring) 2014;22:5–13.
10. Diabetes Prevention Program Research Group,Knowler WC, Fowler SE, et al. 10-year follow-upof diabetes incidence and weight loss in the Dia-betes Prevention Program outcomes study. Lancet2009;374:1677–86.
11. Lindstrom J, Peltonen M, Eriksson JG, et al.Improved lifestyle and decreased diabetes riskover 13 years: long-term follow-up of the rando-mised Finnish Diabetes Prevention Study (DPS).Diabetologia 2013;56:284–93.
12. Jensen MD, Ryan DH, Apovian CM, et al. 2013AHA/ACC/TOS guideline for the management of
overweight and obesity in adults: a report of theAmerican College of Cardiology/American HeartAssociation Task Force on Practice Guidelines andThe Obesity Society. J Am Coll Cardiol 2014;63:2985–3023.
13. Garvey WT, Mechanick JI, Brett EM, et al.American Association of Clinical Endocrinologistsand American College of Endocrinology compre-hensive clinical practice guidelines for medicalcare of patients with obesity. Endocr Pract 2016;22 Suppl 3:1–203.
14. Apovian CM, Aronne LJ, Bessesen DH, et al.Pharmacological management of obesity: anEndocrine Society clinical practice guideline. J ClinEndocrinol Metab 2015;100:342–62.
15. European Medicines Agency. The EuropeanMedicines Agency recommends Suspension of theMarketing Authorisation of Acomplia. 2008.Available at: http://www.ema.europa.eu/ema/index.jsp?curl¼pages/news_and_events/news/2009/11/news_detail_000244.jsp&mid¼WC0b01ac058004d5c1. Accessed December 22, 2017.
16. U.S. Food and Drug Administration. FDA DrugSafety Communication: FDA Recommends Againstthe Continued Use of Meridia (Sibutramine). 2010.Available at: https://www.fda.gov/Drugs/DrugSafety/ucm228746.htm. Accessed December22, 2017.
17. American Diabetes Association. Obesity man-agement for the treatment of type 2 diabetes.Diabetes Care 2017;40 Suppl 1:S57–63.
18. Khera R, Murad MH, Chandar AK, et al. Asso-ciation of pharmacological treatments for obesitywith weight loss and adverse events: a systematicreview and meta-analysis. JAMA 2016;315:2424–34.
19. Marso SP, Daniels GH, Brown-Frandsen K,et al. Liraglutide and cardiovascular outcomes intype 2 diabetes. N Engl J Med 2016;375:311–22.
20. American Diabetes Association. Pharmacologicapproaches to glycemic treatment. Diabetes Care2017;40 Suppl 1:S64–74.
21. Gloy VL, Briel M, Bhatt DL, et al. Bariatricsurgery versus non-surgical treatment for obesity:a systematic review and meta-analysis of rando-mised controlled trials. BMJ 2013;347:f5934.
22. Angrisani L, Santonicola A, Iovino P, et al.Bariatric surgery and endoluminal procedures:IFSO worldwide survey 2014. Obes Surg 2017;27:2279–89.
23. American Society for Metabolic and BariatricSurgery. Estimate of Bariatric Surgery Numbers,2011-2015. 2016. Available at: https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers.Accessed December 22, 2017.
24. Poirier P, Cornier MA, Mazzone T, et al.Bariatric surgery and cardiovascular risk factors: ascientific statement from the American HeartAssociation. Circulation 2011;123:1683–701.
25. Heneghan HM, Nissen S, Schauer PR. Gastro-intestinal surgery for obesity and diabetes: weightloss and control of hyperglycemia. Curr Athe-roscler Rep 2012;14:579–87.
26. le Roux CW, Aylwin SJ, Batterham RL, et al.Gut hormone profiles following bariatric surgeryfavor an anorectic state, facilitate weight loss, andimprove metabolic parameters. Ann Surg 2006;243:108–14.
27. Miras AD, le Roux CW. Mechanisms underlyingweight loss after bariatric surgery. Nat Rev Gas-troenterol Hepatol 2013;10:575–84.
28. Khorgami Z, Shoar S, Andalib A, Aminian A,Brethauer SA, Schauer PR. Trends in utilizationof bariatric surgery, 2010-2014: sleeve gas-trectomy dominates. Surg Obes Relat Dis 2017;13:774–8.
29. Hanipah ZN, Schauer PR. Surgical treatment ofobesity and diabetes. Gastrointest Endosc ClinN Am 2017;27:191–211.
30. Madsbad S, Dirksen C, Holst JJ. Mechanisms ofchanges in glucose metabolism and bodyweightafter bariatric surgery. Lancet Diabetes Endocrinol2014;2:152–64.
31. Arble DM, Sandoval DA, Seeley RJ. Mecha-nisms underlying weight loss and metabolicimprovements in rodent models of bariatricsurgery. Diabetologia 2015;58:211–20.
32. Mahawar KK, Sharples AJ. Contribution ofmalabsorption to weight loss after Roux-en-Ygastric bypass: a systematic review. Obes Surg2017;27:2194–206.
33. Aarts EO, Dogan K, Koehestanie P,Aufenacker TJ, Janssen IM, Berends FJ. Long-termresults after laparoscopic adjustable gastricbanding: a mean fourteen year follow-up study.Surg Obes Relat Dis 2014;10:633–40.
34. Marceau P, Hould FS, Simard S, et al. Bil-iopancreatic diversion with duodenal switch.World J Surg 1998;22:947–54.
35. Ionut V, Burch M, Youdim A, Bergman RN.Gastrointestinal hormones and bariatric surgery-induced weight loss. Obesity (Silver Spring)2013;21:1093–103.
36. Buchwald H, Avidor Y, Braunwald E, et al.Bariatric surgery: a systematic review and meta-analysis. JAMA 2004;292:1724–37.
37. Chang SH, Stoll CR, Song J, Varela JE,Eagon CJ, Colditz GA. The effectiveness and risksof bariatric surgery: an updated systematic review

J A C C V O L . 7 1 , N O . 6 , 2 0 1 8 Pareek et al.F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7 Metabolic Surgery: Weight Loss, Diabetes, and Beyond
685
and meta-analysis, 2003-2012. JAMA Surg 2014;149:275–87.
38. Yu J, Zhou X, Li L, et al. The long-term effectsof bariatric surgery for type 2 diabetes: systematicreview and meta-analysis of randomized and non-randomized evidence. Obes Surg 2015;25:143–58.
39. Hutter MM, Schirmer BD, Jones DB, et al. Firstreport from the American College of SurgeonsBariatric Surgery Center Network: laparoscopicsleeve gastrectomy has morbidity and effective-ness positioned between the band and the bypass.Ann Surg 2011;254:410–20; discussion 420–2.
40. Dixon JB, O’Brien PE, Playfair J, et al.Adjustable gastric banding and conventionaltherapy for type 2 diabetes: a randomizedcontrolled trial. JAMA 2008;299:316–23.
41. Schauer PR, Kashyap SR, Wolski K, et al. Bar-iatric surgery versus intensive medical therapy inobese patients with diabetes. N Engl J Med 2012;366:1567–76.
42. Mingrone G, Panunzi S, De Gaetano A, et al.Bariatric surgery versus conventional medicaltherapy for type 2 diabetes. N Engl J Med 2012;366:1577–85.
43. Ikramuddin S, Korner J, Lee WJ, et al.Roux-en-Y gastric bypass vs intensive medicalmanagement for the control of type 2 diabetes,hypertension, and hyperlipidemia: the DiabetesSurgery Study randomized clinical trial. JAMA2013;309:2240–9.
44. Liang Z, Wu Q, Chen B, Yu P, Zhao H,Ouyang X. Effect of laparoscopic Roux-en-Ygastric bypass surgery on type 2 diabetes melli-tus with hypertension: a randomized controlledtrial. Diabetes Res Clin Pract 2013;101:50–6.
45. Wentworth JM, Playfair J, Laurie C, et al.Multidisciplinary diabetes care with and withoutbariatric surgery in overweight people: a rando-mised controlled trial. Lancet Diabetes Endocrinol2014;2:545–52.
46. Courcoulas AP, Goodpaster BH, Eagleton JK,et al. Surgical vs medical treatments for type 2diabetes mellitus: a randomized clinical trial.JAMA Surg 2014;149:707–15.
47. Halperin F, Ding SA, Simonson DC, et al. Roux-en-Y gastric bypass surgery or lifestyle withintensive medical management in patients withtype 2 diabetes: feasibility and 1-year results of arandomized clinical trial. JAMA Surg 2014;149:716–26.
48. Parikh M, Chung M, Sheth S, et al. Ran-domized pilot trial of bariatric surgery versusintensive medical weight management on dia-betes remission in type 2 diabetic patients whodo NOT meet NIH criteria for surgery and therole of soluble RAGE as a novel biomarker ofsuccess. Ann Surg 2014;260:617–22; discussion622–4.
49. Ding SA, Simonson DC, Wewalka M, et al.Adjustable gastric band surgery or medical man-agement in patients with type 2 diabetes: a ran-domized clinical trial. J Clin Endocrinol Metab2015;100:2546–56.
50. Cummings DE, Arterburn DE, Westbrook EO,et al. Gastric bypass surgery vs intensive lifestyleand medical intervention for type 2 diabetes: the
CROSSROADS randomised controlled trial. Dia-betologia 2016;59:945–53.
51. Puzziferri N, Roshek TB 3rd, Mayo HG,Gallagher R, Belle SH, Livingston EH. Long-termfollow-up after bariatric surgery: a systematic re-view. JAMA 2014;312:934–42.
52. Sjöström L, Lindroos AK, Peltonen M, et al.Lifestyle, diabetes, and cardiovascular risk factors10 years after bariatric surgery. N Engl J Med2004;351:2683–93.
53. Sjöström L, Peltonen M, Jacobson P, et al.Bariatric surgery and long-term cardiovascularevents. JAMA 2012;307:56–65.
54. Sjöström L. Review of the key results from theSwedish Obese Subjects (SOS) trial: a prospectivecontrolled intervention study of bariatric surgery.J Intern Med 2013;273:219–34.
55. Maciejewski ML, Arterburn DE, Van Scoyoc L,et al. Bariatric surgery and long-term durability ofweight loss. JAMA Surg 2016;151:1046–55.
56. Mingrone G, Panunzi S, De Gaetano A, et al.Bariatric-metabolic surgery versus conventionalmedical treatment in obese patients with type 2diabetes: 5 year follow-up of an open-label, sin-gle-centre, randomised controlled trial. Lancet2015;386:964–73.
57. Schauer PR, Bhatt DL, Kirwan JP, et al. Bar-iatric surgery versus intensive medical therapy fordiabetes: 5-year outcomes. N Engl J Med 2017;376:641–51.
58. Kashyap SR, Bhatt DL, Wolski K, et al. Meta-bolic effects of bariatric surgery in patients withmoderate obesity and type 2 diabetes: analysis ofa randomized control trial comparing surgery withintensive medical treatment. Diabetes Care 2013;36:2175–82.
59. Rubino F, Nathan DM, Eckel RH, et al. Meta-bolic surgery in the treatment algorithm for type 2diabetes: a joint statement by international dia-betes organizations. Diabetes Care 2016;39:861–77.
60. Sjöström L, Peltonen M, Jacobson P, et al.Association of bariatric surgery with long-termremission of type 2 diabetes and with microvas-cular and macrovascular complications. JAMA2014;311:2297–304.
61. Carlsson LM, Peltonen M, Ahlin S, et al. Bar-iatric surgery and prevention of type 2 diabetes inSwedish obese subjects. N Engl J Med 2012;367:695–704.
62. Schauer PR, Mingrone G, Ikramuddin S,Wolfe B. Clinical outcomes of metabolic surgery:efficacy of glycemic control, weight loss, andremission of diabetes. Diabetes Care 2016;39:902–11.
63. Schauer PR, Bhatt DL, Kirwan JP, et al. Bar-iatric surgery versus intensive medical therapy fordiabetes: 3-year outcomes. N Engl J Med 2014;370:2002–13.
64. Kirwan JP, Aminian A, Kashyap SR,Burguera B, Brethauer SA, Schauer PR. Bariatricsurgery in obese patients with type 1 diabetes.Diabetes Care 2016;39:941–8.
65. Adams TD, Arterburn DE, Nathan DM,Eckel RH. Clinical outcomes of metabolic surgery:
microvascular and macrovascular complications.Diabetes Care 2016;39:912–23.
66. Rubino F, Marescaux J. Effect of duodenal-jejunal exclusion in a non-obese animal model oftype 2 diabetes: a new perspective for an olddisease. Ann Surg 2004;239:1–11.
67. Drucker DJ. The role of gut hormones inglucose homeostasis. J Clin Invest 2007;117:24–32.
68. Kaplan LM. What bariatric surgery can teachus about endoluminal treatment of obesity andmetabolic disorders. Gastrointest Endosc ClinN Am 2017;27:213–31.
69. Jackness C, Karmally W, Febres G, et al. Verylow-calorie diet mimics the early beneficial effectof Roux-en-Y gastric bypass on insulin sensitivityand beta-cell function in type 2 diabetic patients.Diabetes 2013;62:3027–32.
70. Lingvay I, Guth E, Islam A, Livingston E. Rapidimprovement in diabetes after gastric bypasssurgery: is it the diet or surgery? Diabetes Care2013;36:2741–7.
71. Bojsen-Moller KN, Dirksen C, Jorgensen NB,et al. Early enhancements of hepatic and later ofperipheral insulin sensitivity combined withincreased postprandial insulin secretion contributeto improved glycemic control after Roux-en-Ygastric bypass. Diabetes 2014;63:1725–37.
72. Peterli R, Steinert RE, Woelnerhanssen B, et al.Metabolic and hormonal changes after laparo-scopic Roux-en-Y gastric bypass and sleeve gas-trectomy: a randomized, prospective trial. ObesSurg 2012;22:740–8.
73. Dirksen C, Damgaard M, Bojsen-Moller KN,et al. Fast pouch emptying, delayed small intes-tinal transit, and exaggerated gut hormone re-sponses after Roux-en-Y gastric bypass.Neurogastroenterol Motil 2013;25:346–e255.
74. Rubino F, Gagner M, Gentileschi P, et al. Theearly effect of the Roux-en-Y gastric bypass onhormones involved in body weight regulation andglucose metabolism. Ann Surg 2004;240:236–42.
75. Bjorklund P, Laurenius A, Een E, Olbers T,Lonroth H, Fandriks L. Is the Roux limb a deter-minant for meal size after gastric bypass surgery?Obes Surg 2010;20:1408–14.
76. Pournaras DJ, Osborne A, Hawkins SC, et al.Remission of type 2 diabetes after gastric bypassand banding: mechanisms and 2 year outcomes.Ann Surg 2010;252:966–71.
77. Vest AR, Heneghan HM, Schauer PR, Young JB.Surgical management of obesity and the rela-tionship to cardiovascular disease. Circulation2013;127:945–59.
78. Kopp HP, Kopp CW, Festa A, et al. Impact ofweight loss on inflammatory proteins and theirassociation with the insulin resistance syndrome inmorbidly obese patients. Arterioscler Thromb VascBiol 2003;23:1042–7.
79. Shimizu H, Shimomura Y, Hayashi R, et al.Serum leptin concentration is associated with totalbody fat mass, but not abdominal fat distribution.Int J Obes Relat Metab Disord 1997;21:536–41.
80. Trakhtenbroit MA, Leichman JG, Algahim MF,et al. Body weight, insulin resistance, and serum

Pareek et al. J A C C V O L . 7 1 , N O . 6 , 2 0 1 8
Metabolic Surgery: Weight Loss, Diabetes, and Beyond F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7
686
adipokine levels 2 years after 2 types of bariatricsurgery. Am J Med 2009;122:435–42.
81. Falken Y, Hellstrom PM, Holst JJ, Naslund E.Changes in glucose homeostasis after Roux-en-Ygastric bypass surgery for obesity at day three,two months, and one year after surgery: role ofgut peptides. J Clin Endocrinol Metab 2011;96:2227–35.
82. Munzberg H, Laque A, Yu S, Rezai-Zadeh K,Berthoud HR. Appetite and body weight regula-tion after bariatric surgery. Obes Rev 2015;16Suppl 1:77–90.
83. Auclair A, Martin J, Bastien M, et al. Is therea role for visceral adiposity in inducing type 2diabetes remission in severely obese patientsfollowing biliopancreatic diversion with duodenalswitch surgery? Obes Surg 2016;26:1717–27.
84. Auclair A, Biertho L, Marceau S, et al. Bariatricsurgery-induced resolution of hypertension andobstructive sleep apnea: impact of modulation ofbody fat, ectopic fat, autonomic nervous activity,inflammatory and adipokine profiles. Obes Surg2017;27:3156–64.
85. Korner J, Inabnet W, Febres G, et al. Pro-spective study of gut hormone and metabolicchanges after adjustable gastric banding andRoux-en-Y gastric bypass. Int J Obes (Lond) 2009;33:786–95.
86. Burton PR, Brown WA. The mechanism ofweight loss with laparoscopic adjustable gastricbanding: induction of satiety not restriction. Int JObes (Lond) 2011;35 Suppl 3:S26–30.
87. Vest AR, Heneghan HM, Agarwal S,Schauer PR, Young JB. Bariatric surgery and car-diovascular outcomes: a systematic review. Heart2012;98:1763–77.
88. Zhou X, Yu J, Li L, et al. Effects of bariatricsurgery on mortality, cardiovascular events, andcancer outcomes in obese patients: systematicreview and meta-analysis. Obes Surg 2016;26:2590–601.
89. Benotti PN, Wood GC, Carey DJ, et al. Gastricbypass surgery produces a durable reduction incardiovascular disease risk factors and reduces thelong-term risks of congestive heart failure. J AmHeart Assoc 2017;6:e005126.
90. Priester T, Ault TG, Davidson L, et al. Coronarycalcium scores 6 years after bariatric surgery. ObesSurg 2015;25:90–6.
91. Vest AR, Patel P, Schauer PR, et al. Clinical andechocardiographic outcomes after bariatric sur-gery in obese patients with left ventricular systolicdysfunction. Circ Heart Fail 2016;9:e002260.
92. Sjöström L, Narbro K, Sjöström CD, et al.Effects of bariatric surgery on mortality in Swedishobese subjects. N Engl J Med 2007;357:741–52.
93. Jamaly S, Carlsson L, Peltonen M, Jacobson P,Sjöström L, Karason K. Bariatric surgery and therisk of new-onset atrial fibrillation in Swedishobese subjects. J Am Coll Cardiol 2016;68:2497–504.
94. Sundstrom J, Bruze G, Ottosson J, Marcus C,Naslund I, Neovius M. Weight loss and heart fail-ure: a nationwide study of gastric bypass surgeryversus intensive lifestyle treatment. Circulation2017;135:1577–85.
95. Longitudinal Assessment of Bariatric Surgery(LABS) Consortium, Flum DR, Belle SH, et al. Peri-operative safety in the longitudinal assessment ofbariatric surgery. N Engl J Med 2009;361:445–54.
96. Aminian A, Brethauer SA, Kirwan JP,Kashyap SR, Burguera B, Schauer PR. How safe ismetabolic/diabetes surgery? Diabetes Obes Metab2015;17:198–201.
97. Poulose BK, Griffin MR, Zhu Y, et al. Nationalanalysis of adverse patient safety for events inbariatric surgery. Am Surg 2005;71:406–13.
98. Morino M, Toppino M, Forestieri P,Angrisani L, Allaix ME, Scopinaro N. Mortality afterbariatric surgery: analysis of 13,871 morbidlyobese patients from a national registry. Ann Surg2007;246:1002–7; discussion 1007–9.
99. Fridman A, Moon R, Cozacov Y, et al. Pro-cedure-related morbidity in bariatric surgery: aretrospective short- and mid-term follow-up of asingle institution of the American College of Sur-geons Bariatric Surgery Centers of Excellence.J Am Coll Surg 2013;217:614–20.
100. Sekhar N, Torquati A, Youssef Y, Wright JK,Richards WO. A comparison of 399 open and 568laparoscopic gastric bypasses performed during a4-year period. Surg Endosc 2007;21:665–8.
101. Azagury D, Morton JM. Bariatric surgeryoutcomes in US accredited vs non-accreditedcenters: a systematic review. J Am Coll Surg2016;223:469–77.
102. Buchwald H, Estok R, Fahrbach K, Banel D,Sledge I. Trends in mortality in bariatric surgery: asystematic review and meta-analysis. Surgery2007;142:621–32; discussion 632–5.
103. Khan S, Rock K, Baskara A, Qu W, Nazzal M,Ortiz J. Trends in bariatric surgery from 2008 to2012. Am J Surg 2016;211:1041–6.
104. Mechanick JI, Youdim A, Jones DB, et al.Clinical practice guidelines for the perioperativenutritional, metabolic, and nonsurgical support ofthe bariatric surgery patient–2013 update:Cosponsored by American Association of ClinicalEndocrinologists, The Obesity Society, and Amer-ican Society for Metabolic & Bariatric Surgery.Obesity (Silver Spring) 2013;21 Suppl 1:S1–27.
105. Parrott J, Frank L, Rabena R, Craggs-Dino L,Isom KA, Greiman L. American Society for Meta-bolic and Bariatric Surgery integrated healthnutritional guidelines for the surgical weight losspatient 2016 update: micronutrients. Surg ObesRelat Dis 2017;13:727–41.
106. Vargas-Ruiz AG, Hernandez-Rivera G,Herrera MF. Prevalence of iron, folate, and vitaminB12 deficiency anemia after laparoscopic Roux-en-Ygastric bypass. Obes Surg 2008;18:288–93.
107. von Drygalski A, Andris DA. Anemia afterbariatric surgery: more than just iron deficiency.Nutr Clin Pract 2009;24:217–26.
108. Liu C, Wu D, Zhang JF, et al. Changes in bonemetabolism in morbidly obese patients after bar-iatric surgery: a meta-analysis. Obes Surg 2016;26:91–7.
109. Marsk R, Jonas E, Rasmussen F, Naslund E.Nationwide cohort study of post-gastric bypasshypoglycaemia including 5,040 patients
undergoing surgery for obesity in 1986-2006 inSweden. Diabetologia 2010;53:2307–11.
110. McLaughlin T, Peck M, Holst J, Deacon C.Reversible hyperinsulinemic hypoglycemia aftergastric bypass: a consequence of altered nutrientdelivery. J Clin Endocrinol Metab 2010;95:1851–5.
111. Nguyen NT, Magno CP, Lane KT, Hinojosa MW,Lane JS. Association of hypertension, diabetes,dyslipidemia, and metabolic syndrome withobesity: findings from the National Health andNutrition Examination Survey, 1999 to 2004. J AmColl Surg 2008;207:928–34.
112. Aminian A, Brethauer SA, Andalib A, et al.Individualized metabolic surgery score: procedureselection based on diabetes severity. Ann Surg2017;266:650–7.
113. Sjöström L, Gummesson A, Sjöström CD, et al.Effects of bariatric surgery on cancer incidence inobese patients in Sweden (Swedish Obese Subjectsstudy): a prospective, controlled intervention trial.Lancet Oncol 2009;10:653–62.
114. Sarkhosh K, Switzer NJ, El-Hadi M, Birch DW,Shi X, Karmali S. The impact of bariatric surgery onobstructive sleep apnea: a systematic review. ObesSurg 2013;23:414–23.
115. Bower G, Toma T, Harling L, et al. Bariatricsurgery and non-alcoholic fatty liver disease: asystematic review of liver biochemistry and his-tology. Obes Surg 2015;25:2280–9.
116. Shah SS, Todkar JS, Shah PS, Cummings DE.Diabetes remission and reduced cardiovascular riskafter gastric bypass in Asian Indianswith bodymassindex 35 kg/m(2). Surg Obes Relat Dis 2010;6:332–8.
117. Panunzi S, De Gaetano A, Carnicelli A,Mingrone G. Predictors of remission of diabetesmellitus in severely obese individuals undergoingbariatric surgery: do BMI or procedure choice mat-ter? A meta-analysis. Ann Surg 2015;261:459–67.
118. Cummings DE, Cohen RV. Bariatric/metabolicsurgery to treat type 2 diabetes in patients with aBMI 35 kg/m2. Diabetes Care 2016;39:924–33.
119. Miras AD, le Roux CW. Metabolic surgery:shifting the focus from glycaemia and weight toend-organ health. Lancet Diabetes Endocrinol2014;2:141–51.
120. Zhou X, Li L, Kwong JS, Yu J, Li Y, Sun X.Impact of bariatric surgery on renal functions inpatients with type 2 diabetes: systematic review ofrandomized trials and observational studies. SurgObes Relat Dis 2016;12:1873–82.
121. Cohen RV, Pereira TV, Aboud CM, et al. Micro-vascular outcomes after metabolic surgery (MOMS)in patients with type 2 diabetes mellitus and class Iobesity: rationale and design for a randomisedcontrolled trial. BMJ Open 2017;7:e013574.
122. Schiavon CA, Bersch-Ferreira AC, Santucci EV,et al. Effects of bariatric surgery in obese patientswith hypertension: the GATEWAY randomized trial(Gastric Bypass To Treat Obese Patients WithSteady Hypertension). Circulation 2017 Nov 13[E-pub ahead of print].
123. Adams ST, Salhab M, Hussain ZI, Miller GV,Leveson SH. Obesity-related hypertension and itsremission following gastric bypass surgery: a

J A C C V O L . 7 1 , N O . 6 , 2 0 1 8 Pareek et al.F E B R U A R Y 1 3 , 2 0 1 8 : 6 7 0 – 8 7 Metabolic Surgery: Weight Loss, Diabetes, and Beyond
687
review of the mechanisms and predictive factors.Blood Press 2013;22:131–7.
124. Bays HE, Jones PH, Jacobson TA, et al. Lipidsand bariatric procedures part 1 of 2: scientificstatement from the National Lipid Association,American Society for Metabolic and Bariatric Sur-gery, and Obesity Medicine Association: fullreport. J Clin Lipidol 2016;10:33–57.
125. Bays H, Kothari SN, Azagury DE, et al. Lipidsand bariatric procedures part 2 of 2: scientific
statement from the American Society for Metabolicand Bariatric Surgery (ASMBS), the National LipidAssociation (NLA), and Obesity Medicine Associa-tion (OMA). Surg Obes Relat Dis 2016;12:468–95.
126. Inge TH, Courcoulas AP, Jenkins TM, et al.Weight loss and health status 3 years after bar-iatric surgery in adolescents. N Engl J Med 2016;374:113–23.
127. Arterburn DE, Bogart A, Sherwood NE,et al. A multisite study of long-term remission
and relapse of type 2 diabetes mellitusfollowing gastric bypass. Obes Surg 2013;23:93–102.
128. Piche ME, Auclair A, Harvey J, Marceau S,Poirier P. How to choose and use bariatric surgeryin 2015. Can J Cardiol 2015;31:153–66.
KEY WORDS bariatric, cardiovascular risk,diabetes, metabolic, obesity

![Emotion-Aware Human Attention Predictionopenaccess.thecvf.com/.../Cordel_Emotion-Aware_Human...CVPR_2019_paper.p… · tor known to influence human attention [12, 35]. Behav-ioral](https://img.pdfslide.us/doc/110x75/5e1726b523240b1b284699a2/emotion-aware-human-attention-tor-known-to-iniuence-human-attention-12-35.jpg)