Embed Size (px)
Citation preview

Metabolic Bone Diseases
METAOLC BONE DISEASES
are diseases of bones caused by disturbances in metabolism of bones
& is characterized by a decrease in bone density & bone strength
either by Increasing bone resorption Or: Decreasing bone formation Or: Both

Blood Calcium Homeostasis &
Metabolic Bone Diseases

Biological Roles of Calcium
1- Calcium in Bone :
Calcium is a major & essential component of bone Generally, bone is specialized mineralized connective tissue that contains: 1- Cells: osteoblasts & osteoclasts 2- organic matrix: materials like collagen type I & others proteoglycans 3- mineral: hydroxy apatite (Calcium + Phosphorous)
Role of calcium in bones: 1- Mechanical role (it gives bone its hardness, tolerability, strength etc..) 2- Material of turnover in skeleton (bone resporption & bone formation= remodelling) 5% per year of adult skeleton 3- Reservoir for calcium to help stabilize extracellular calcium ions Ca2+ Calcium gets out from bones to blood & reverse to correct decrease or increase in Ca2+ in blood
2- Calcium located in other extracellular locations: 1- Extracellular calcium ions Ca2+ should be maintained within narrow limits as this is necessary for normal excitability of nerves & muscles . 2- Extracellular Ca2+ is essential for blood clotting mechanisms.
Calcium ions inside cells (cytosolic) is much less than extracellular Ca2+ So, cells have transport systems to maintain this difference. Accordingly: increased intracellular calcium is a signal for some biological activity of cells

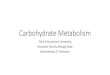
Total CalciumOf the Body
~99 % in bone
ICF
1 %
Blood Clotting
Excitability of Nerve & Muscle
Bone Formation
Reservoir for ECF [Ca2+]
Metabolic Regulation for Action of
Hormones & Enzyme Activation
ECF
Biological Functions of Calcium

Calcium in Blood

Regulation of Calcium Metabolism
Calcium Homeostasis
Calcium in plasma of blood 1- Ionized (Ca2+) 2- Bound with plasma proteins (albumin) 3- Complexed with citrate
Ionized calcium Ca2+ is the physiologically important component So, Ca2+ in blood is regulated mainly by: 1- 1, 25 dihydroxycholecalcefrol (1, 25 DHCC) 2- Parathyroid hormone (PTH) 3- Calcitonin hormone 1 & 2 increase Ca2+ in blood 3 decreases Ca2+ in blood
1, 2 & 3 regulate calcium metabolism through 3 organs 1- Bones2- Intestines3- Kidneys

Calcium Homeostasis
The concentration of calcium, phosphorous &magnesium in the plasma depends on
ORGAN PHYSIOLOGY: Net effect of bone mineral deposition & resorption Intestinal absorption Renal excretion

Organ Calcium Homeostasis

Blood[Ca2+]
is Regulated By:
Parathyroid Hormone (PTH)
Active Vitamin D (Calcitriol) or 1,25 DHCC
Calcitonin Hormone
EndocrinalCalcium Homeostasis

Vitamin D A group of sterols with a hormone-like function.
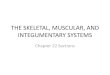
Sources of Vitamin D
1- Skin synthesis (On Exposure to Sun Lights): In the skin, 7 dehydrocholesterol is converted to vitamin D3 by exposure to sunlight 2- Diet: - Animal Source Cholecalciferol (Vitamins D3) - Plant Source: Ergocalciferol (Vitamin D2) Vitamin D2 & D3 are NOT biologically active
– Activation of cholecalciferol (vitamin D3) Cholecalciferol (Vitamin D3) is activated in the body to the biologically active form by two hydroxylations: first in the liver (at position 25) by 25 hydroxylase & then in the kidney at positions 1 by 1 α hydroxylase
Active Vitamin D 1, 25 dihydroxycholecalciferol (Calcitriol or DHCC)

Vitamin D2
plant source
Vitamin D3animal source
fatty fishLiver
egg yolk
7-dehydrocholesterolIn the skin
DIET VITAMINs D
SOURCES OF VITAMIN D
Sun Rays

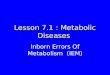
Vitamin D metabolism
Cholecalciferol (Vitamin D3) is derived from 7-dehydrocholesterol in the skin by sunlight or supplied in the diet
In liver: Cholecalciferol is converted to 25-hydroxycholecalciferol (25-HCC) by the enzyme 25 hydroxylase 25-hydroxycholecalciferol is the predominant form of vitamin D in blood 25-hydroxycholecalciferol is the main storage form of vitamin in the body In kidneys: The 1 α hydroxylase enzyme converts 25 hydroxycholecalciferol to 1,25-dihydroxycholecalciferol (1, 25 DHCC or Calcitriol) which is the biologically active form of vitamin D

Function of Vitamin D
The overall function of 1,25 DHCC is to maintain adequate plasma levels of calcium
this function is achieved by
• increasing uptake of calcium by the intestine
• Increase calcium reabsorption by the kidney
• stimulating resorption of bone (when necessary) in EMERGENCY HYPOCALCEMIA

Vitamin D deficiency
calcium of bone is mobilized outside bone with
demineralization of bone
Rickets (in children) Osteomalacia (in adults)

Rickets Continued formation of the collagen matrix
BUTWith incomplete mineralization
Soft Boneswith
Bone Deformity
Osteomalacia Demineralization of preexisting bones
with
Increased Susceptibility to Fractures (due to weakness of bone)

Rickets & Osteomalacia
Rickets & Osteomalacia are metabolic bone diseases occurring due to poor mineralization (calcium content) of bone
Causes of poor calcification of bones:
I. Vitamin D deficiency 1- Deficiency of sources of vitamin D3: Nutrional Vitamin D deficiency (vitamin D3) Poor exposure to sun light
2- Impaired vitamin D metabolism: Renal Rickets: chronic renal failure causes deficiency of 1 hydroxylase of the kidney Hypoparathyroidism: causing decrease in activity of 1 α hydroxylase Genetic defects in vitamin D metabolism (defect in its activation) Genetic defects of vitamin D receptors
II. Calcium Deficiency (nutritional or defect in intestinal absorption)

In Chronic Renal Failure
Low activity of Renal 1 -a Hydroxylase
Decreased ability to form the
active form of vitamin D(1, 25 DHCC will be low)
Treatment: 1,25 DHCC (Calcitriol)
Renal RicketsRenal Osteodystrophy

Laboratory Investigations for the Diagnosis of Rickets & Osteomalacia
Investigations to confirm the diagnosis of rickets: Blood levels of 25-hydroxycholecalciferol (25 HCC) Blood calcium, (hypocalcemia) Blood Alkaline phosphatase (ALP)
Investigations to diagnose the cause of rickets: Kidney function tests (KFT) Blood 1, 25 dihydroxycholecalciferol (1, 25 DHCC) Blood PTH Others i.e. molecular genetics (if indicated)

Parathyroid Hormone (PTH)
• The active hormone is secreted in response to al fall in plasma Ca2+ with a result in Ca2+ increase in plasma.
• On bone: PTH stimulates bone resorption by osteoclasts
• On kidney:
1- PTH increases reabsorption of calcium from kidney tubules. 2- PTH decreases phosphorous reabsorption from kidney tubules. 3- PTH promotes activity of 1 a hydroxylase of the kidney (with more hydroxylation of 25 hydroxycholecalciferol. (25 HCC) to 1,25 DHCC (activation of vitamin D) which increases intestinal absorption of calcium so, action on intestine is indirect (via Vitamin D)

HypoparathyroidismDeficiency or absence of parathyroid hormone (PTH)
Causes:
• Surgically removed by mistake during thyroidectomy • Destruction of the glands by auto-immune process• Pseudohypoparathyroidism: receptors for PTH fail to respond to PTH
Biochemical Effects:
1- Hypocalcemia 2- Hyperphosphatemia 3- Deficiency of blood levels of 1, 25 DHCC : 25 HCC is not hydroxylated to 1, 25 DHCC

Hyperparathyroidism Causes:• Parathyroid adenoma• Diffuse hyperplasia of parathyroid glands
Biochemical Effects:1- Hypercalcemia2- Hypophosphatemia3- Hypercalcuria (increased excretion in urine to reduce blood calcium) 4- Increased markers of bone resorption
Clinical features of hyperparathyroidism Manifestations of hypercalcemia
• Generalized muscular weakness• Neurological symptoms: inability to concentrate, confusion• Anorexia, nausea, vomiting, constipation• Polyuria & polydepsia• Calcium stones in kidney• ECG changes: Shortened Q-T interval & bradycardia

Calcitonin Hormone
Calcitonin hormone is :– Secreted by the parafollicular or “C” cells of the thyroid gland– Released in response to high blood calcium (hypercalcemia)
In cases of hypercalcemia,Calcitonin Hormone blood [Ca2+] by:
– Osteoclast activity (preventing release of calcium to blood)
– Renal reabsorption of calcium Net result of its action blood calcium CALCITONIN IS THE ONLY HYPOCALCEMIC HORMONE

• Most prevalent metabolic bone disease in adults• It means reduction in bone mass per unit volume i.e. bone matrix composition is normal, but it is reduced
• Typically silent (without symptoms) until it leads to fracture at a degree of trauma that would not have caused a fracture in a non-osteoprotic skeleton.
Fractures are called fragility or osteoporotic fractures) Most affected: vertebral compression (may be asymptomatic) & hip fractures (requires surgery in most cases)
• Post-menopausal women lose more bone mass than men (primary osteoporosis)
• Osteoporosis diagnosis is by dual energy x-ray absorpitometry (DXA) scan• Lab diagnosis: not conclusive
Metabolic Diseases of Bone: Osteoporosis

Main Causes of Osteoporosis
1- Increased Bone Resorption
Estrogen deficiency (as in menopause)
Hyperparathyroidism (activation of osteoclasts) Hyperthyroidism (increase proteolysis) Hypogonadism (low testosterone which is an anabolic hormone)
2- Decrease Bone Formation
Liver disease (low protein production)
Age over 50
3- Both
Hypercortisolism (as Cushing’s syndrome)

Risk Factors of Osteoporosis
Advanced age (esp. in females) Certain Drugs Family history of osteoporosis or fractures Immobilization Smoking Excess alcohol intake Cushing’s syndrome Long term glucocorticoids therapy Hyperparathyroidism Hyperthyroidism Vitamin D disorders Certain malignancies
In these cases1-Bone Mass Density (BMD): Dual Energy X-ray Absorptiometry (DXA) is highly recommended to evaluate bone density2- Vitamin D level in blood is checked3- Secondary endocrinal causes of osteoporosis are checked (T3, T4, PTH, Cortisol, Testosterone)4- Biochemical Bone Markers (not of great help)