Embed Size (px)
Citation preview

Mesodermal Tumors Associated with Hypoglycemia: *Review of Literature and Report of a Case
DL.NE W. CROCKER, M.D., FRANK J. VEITH, M.D.
From the Departments of Pathology and of Surgery, Peter Bent Brigham Hospitaland Harvard Medical School, Boston, Mass.
THE ABILITY of certain neoplasms to in-terfere with or alter metabolic processes isone of the more interesting facets of oncol-ogy. Norepinephrine elaboration by thepheochromocytoma and serotonin produc-tion by the carcinoid tumor produce clinicalmanifestations which may provide the firstindication of the existence of the responsibletumor. Functioning islet cell adenomas andcarcinomas constitute the majority of tu-mors associated with clinical hypoglycemia.An expanding literature on non-pancreatictumors associated with hypoglycemia exists.Lowbeer's comprehensive review 20 of 48reported cases of hypoglycemia associatedwith non-pancreatic tumors included 23carcinomas and 25 tumors of mesodermalorigin. Most of the carcinomas were of livercell origin. A smaller number arose in theadrenal cortex. Rare instances of carcinomaof the lung43 and of the cecum44 withhypoglycemia have been reported recently.The purpose of this communication is to
report the second case of a rare type offunctioning mesodermal tumor, an heman-giopericytoma. This case illustrates sev-eral important clinical features: 1) hypo-glycemia occurs only when the tumorattains a large size, 2) partial surgical re-duction in tumor mass can provide symp-tomatic relief of hypoglycemia when total
* Submitted for publication April 21, 1964.This study was supported in part by Grants
HE-5274 and HE-06370 from the National HeartInstitute, National Institutes of Health.
excision is impossible, 3) multiple subtotalexcisions of recurrences can relieve recur-rent hypoglycemia and 4) radiotherapy canbe effective in alleviating hypoglycemicsymptoms. In addition, the cases of meso-dermal tumors associated with hypogly-cemia reported since Lowbeer's review willbe tabulated and discussed.
Case ReportA 51-year-old husky white man was admitted
to the Peter Bent Brigham Hospital in a coma onApril 13, 1962 with a recurrent mass in the rightgroin.
The tumor was detected 10 years previouslyby routine rectal examination. The fasting bloodsugar at that time was 73 mg./100 ml. and thepatient had no symptoms of hypoglycemia. Aperineal biopsy of this 10-cm. smooth, firm, non-tender mass in the region of the right seminalvesicle and bladder base was obtained. On July 3,1952 total cystectomy, prostatectomy and bilateralureterosigmoidostomies were performed by Dr. J.Hartwell Harrison.
In November, 1958 the patient noted an en-larged mass in the right groin and swelling of theright leg. Fasting blood sugar was 84 mg./100 ml.and there were no hypoglycemic symptoms. OnJune 24, 1959 the right retroperitoneal area wasexplored via a groin incision. A mass 8 cm. indiameter was found along the right pelvic walladjacent to the rectum and prostatic bed. Afterexcision of the main bulk of tumor together with asegment of extrinsically occluded external iliacvein, residual tumor could be felt along the pubicbone and in the area of the prostatic bed andrectum. The patient felt well and was able towork full time as a millhand.
In March, 1962 the patient first experienceddizziness on awakening in the morning. Fasting
418

Volume 161 MESODERMAL TUMO]Number 3
blood sugar was 50 mg./100 ml. (Normal lowerlimit is 75 mg./100 ml. by the autoanalyzer methodon serum or plasma. Whole blood is not used forthis determination in our laboratory). He had sev-eral episodes of bizarre and aggressive behaviorlasting up to an hour; one of these episodesterminated in coma with right hemiparesis andon admission his blood sugar was 32 mg./100 ml.Neurologic condition improved slowly with intra-venous glucose and subsequent administration ofkaro syrup between meals.
Physical examination confirmed the presenceof a 9 x 5 cm. right groin mass and a 7 x 4 cm.mass anterolateral to the rectum on the right.Barium enema x-rays revealed displacement andfixation of the rectum by an extraluminal mass.Fasting consistently resulted in hypoglycemia withblood glucose levels as low as 31 mg./100 ml.Glucose tolerance test and response to glucagonwere normal. The administration of growth hor-mone, 5 mg./day intramuscularly, was effective indecreasing hypoglycemic symptoms by raising theblood glucose concentration.22
Hypoglycemic episodes began to occur even onstrict in-hospital dietary management with glucosesupplements. Accordingly, on May 31, 1962, alaparotomy was performed through a long para-median incision. Careful exploration of the pan-creas revealed no abnormalities. The pelvis con-tained a large amount of irregular, nodular tumorestimated to weigh 1,200 Gm. The tumor wassolidly attached to the side walls of the pelvis andinfiltrated all the pelvic viscera. There was noevidence of extrapelvic spread. Approximately 75per cent of the gross tumor was removed by in-cising into the tumor nodules and bluntly morcel-
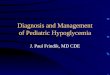
FIG. 1. Closely-packedelongated tumor cellscluster about collapsedcapillaries which are linedby normal endothelialcells. Hematoxylin and
RS AND HYPOGLYCEMIA 419
lating the tumor into removable fragments. Severebleeding necessitated intraoperative transfusion of3,000 cc. of whole blood. The patient had an un-eventful postoperative course. He could tolerate a20-hour fast without developing hypoglycemicsymptoms. During the fast his blood sugar rangedbetween 68 and 132 mg./100 ml. He returned towork and was free of hypoglycemic symptoms for8 months when he noted a few episodes of faint-ness which were relieved by eating, and prior toadmission he had two syncopal attacks. On Febru-ary 22, 1963, about 9 months after his subtotaltumor re-excision, he was readmitted to the hos-pital with findings characteristic of small intestinalobstruction. Blood sugar was 34 mg./100 ml.Following administration of intravenous fluids andglucose a laparotomy was performed. The mid-ileum was surrounded by tumor which obstructedthe lumen by compression. The involved segmentof ileum and the tumor mass which weighed 310Gm. were excised, and end-to-end anastomosiswas performed.
Postoperatively the blood sugar, even after 12-hour fasts, never fell below 87 mg./100 ml. Thepatient felt well for the subsequent 9 months, re-turned to work and had no symptoms of hypo-glycemia although his fasting blood sugar 9 monthsafter ileal resection was 65 mg./100 ml. In viewof this latter finding and the presence of extensiverecurrent tumor in the right groin with deep ex-tension into the abdomen, a course of radiotherapywas considered warranted. A tumor dose of 4,000rads using the 6 MEV machine was delivered tothe right groin and pelvis over a 3-week periodwith resulting objective decrease in size of theperirectal and right inguinal masses. He has had
.;, ,- ik" -A n 40.ml.. ! . 45p . ..:, .1
.ft "! t .'' A

CROCKER AND VEITH Annals of SurgeryMarch 1965
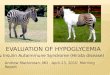
FIG. 2. Hemangioperi-cytoma is a highly vascu-lar tumor as illustratedby this low-power photo-micrograph of recurrenthemangiopericytoma im-pregnated with Wilder'ssilver stain for demon-stration of reticulin. Noteinnumerable capillaries.Tumor cells are locatedoutside reticulin sheath(x 100).
a slow but definite weight gain. Fasting bloodsugar was 92 mg./100 ml.
Pathology. The gross appearance of the tumormasses removed at each surgical procedure in1952, 1959, 1962 and 1963 were identical. Thetumors were unencapsulated, nodular, soft, friable,tan, fleshy and highly vascular. The histologic pat-tern (Fig. 1) was uniformly highly cellular. Thecells were round to elongate with plump ovoidhyperchromatic nuclei. Mitotic figures were pres-ent with an average of 15 mitoses per 50 highpower fields. The whorling of cells about capil-laries was demonstrated by Wilder's reticulin stain.Tumor cells remained outside the reticulin sheathof capillaries, a pattern characteristic of hemangio-pericytomas 40; hence the tumor was designateda malignant hemangiopericytoma with recurrences.
The small amount of insulin-like activity iden-tified * using the epididymal fat pad method inthe tumors removed from our patient in 1962 andin 1963 was considered to represent contaminationof the tumor by circulating blood containing in-sulin. Likewise, studies of the patient's serumfailed to show an abnormal amount of insulin ac-tivity.
Discussion of Pathology. The histologicidentification of an hemangiopericytomarests on the demonstration of the character-istic reticulin pattern (Fig. 2, 3). Reticulinstaining brings out an abundance of capil-
laries lined by normal endothelial cells sur-rounded by concentric rings of tumor cells.These cells, which we consider to be neo-plastic pericytes, remain outside the reticu-lin sheath of the capillaries. This tumor typeis sometimes difficult to distinguish fromvascular undifferentiated carcinomas andsarcoma. The earlier terminology appliedto this type of vascular tumor was "peri-thelioma." Stout 40 established the histo-logic criteria for identifying hemangioperi-cytomas with heavy reliance on the reticu-lin pattern and, by tissue culture methods,demonstrated the similarity of the cellsfrom hemangiopericytomas to the pericytesof Zimmermann.4" Of our case, Dr. Stoutcommented: "This tumor must be a heman-giopericytoma because the vascular patternis perfect." 42Hemangiopericytomas give no histologic
clue regarding malignant potential althoughexcessive mitotic activity would be sug-gestive of malignancy. Even the benignform is unencapsulated and infiltrates lo-cally but aggressive local invasion wouldindicate a malignant tendency. Of course,metastases constitute definitive proof ofmalignancy. The tumor from our patientshows recent evidence of rapid growth with
420
* Assay performed by Dr. Steinke, New Eng-land Deaconess Hospital, Pilgrim Road, Boston,Mass.

Volume 161Number 3
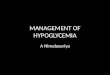
FIG. 3. High-powerphotoniicrograph of anhemangiopericytoma dem-onstrates the dilated cap-illaries surrounded by tu-mor cells. Wilder's retic-ulin stain (X 390).
MESODERMAL TUMORS AND HYPOGLYCEMIA
invasion. The small bowel mass is con-sidered to represent a metastasis.Hemangiopericytoma has been previously
recorded only once in association with hy-poglycemia.17 That patient, a 17-year-oldgirl with hypoglycemic attacks and mas-culinization had permanent relief of hypo-glycemia and masculinization after excisionof a 14 x 14 x 16 cm. retroperitoneal pelvicmass. Local recurrences of tumor, not asbulky as the original, were a problem untilthe time of her death with hepatic metas-tases 10 years after the first excision. Theprolonged clinical course, tendancy to localrecurrence, hypoglycemia and pelvic originprovide a striking parallel to our patient.
Discussion
Lowbeer,20 in 1961, reviewed the reportedcases of extrapancreatic neoplasms associ-ated with hypoglycemia. He collected 48cases from the literature. Of these, 23 werecarcinomas and 25 were of mesodermalorigin. Ten of the mesodermal tumors weresituated in the retroperitoneal region. Sevenwere intrathoracic and eight were intra-abdominal. The majority were fibrosar-comas. The common denominator in all ofthese tumors was their large size, with
421
weights ranging from 770 to 9,000 Gm. Thebest evidence of functional activity con-sisted of relief of hypoglycemic symptomsby excision of the tumor. Almost all re-ported cases including ours fulfill Whipple'striad: low blood glucose, central and au-tonomic nervous system disturbances andrelief of systemic symptoms by the ad-ministration of glucose.Twenty-nine mesodermal tumors associ-
ated with hypoglycemia have been reportedsubsequent to Lowbeer's review (Table 1).Only well documented cases are included.Peritoneal psuedomyxomas and carcinomasincluding hepatomas were excluded. Of the29 patients included in Table 1, 17 weremale and 12 female. The thorax was thesite of origin in 17 cases. Most thoracictumors arose in the mediastinum or frompleura. The abdomen and retroperitonealregion accounted for six and seven cases,respectively. The pelvis was a slightly lesscommon primary site with only four cases.The interval between the initial diagnosis
of tumor and the onset of hypoglycemicsymptoms varied considerably. In those pa-tients whose tumor was noted before theonset of hypoglycemia, the normoglycemicinterval was quite variable, ranging from

CROCKER AND VEITH
0 ~~~~~~~~~~~C)
0. 0
o *-
>oC) r C)C->(,, 4 E
- ~~~ ~ ~~~~~~~~bECS0d
Cd . 0C
000
!CS COCS 5 C CS
0 C) .. 0 0S 0 En0 b
4 ) ) CS9 Z c/) ;
Annals of SurgeryMarch 1965
En 0 C4~~0.0
-4
> bO 0d
aC. *e)C d C
CSe00 4- L C'
~~~~~~6>~~~ - 00E bo~~
~~~~~~~~c
CS C)4
U4 I)0
cSc66 6~~>4. .-i C) t- CN
OCr L ~ c~i'0Ir0O 000qev -4 o~-1 a. C)C) 0
oX ~ XXo b- X Ln -O~LIIoCS ux VQ C.- a)00
0 0 > Ec04 000 0 -~~C C 00 -
o ~ 0 0 C) 0 0 CC 00 0 d0 E
E. ~OCS
-Q 0 -C
1 C)0.. - C
C)CSO-
Cd~~~C
-0 C) ~~~ 0~~~C) ~a..-.- $.. $-H ~~~ ~ -4- 0 c H4 0
I ~~~~ C C
C.,0n Cr) Cr) Cr) %0 V0% 0%) 0% o c 0CCr\ of ol ON 0% oC
W
0
07%o_4 -4 - 4
'IC \0 %~0 V1 \0(0 0O 0O 0% 0%os4 Ch. I" oI
U0CS
S
e ~c a 0 (Y 0C) 0 a % o
00~~~~~~9) 0 CS~~~~( 0e $C)
-(N e') ~~~~~~~ CI) V C'~~~~- 00 0
422
C1)
00
C)._
0
a
0
._
bECd
C.4
C)1
*tz
-q4)
c
x)
C)
x
H
0._:0cSwC)
0
0
._--
¢8
C) x
CS.C)
C0Lfn0%
cn
._;o
0
z
X,
O .0CS 0
O -
a. 0C)
5:-. 1-4

MESODERMAL TUMORS AND HYPOGLYCEMIA
-6-~~~~~~~~~~~
_d 0C0
.0 50 -400
O~O
O 0...>0 -.=$0 0 . - o
-c 0) E311-140PH
E E E E0 0 0
o -° S.
0
0 .-. 0 0s-. I..
=
-C C
. ,C
>- 8n ,,
_ C' os
0. -: ~oEn. tn
v) ci. > x xm 4 4 L;
Cd Cd CB£ E E
d0 0 .0U U -
.0 .0 0)
0t- baLo
0)
0 0
C)C0-0
11
. ~i
6
0o
-o
b)
-._
3. -oCO
W-~ClQ: =zes>s ; = >
E)~0-=E*@E
U) o E
0_ ._
;L
0)
0M
-I.
0 (L ->0to)C
-Lr~ ::s .--cx0 _^ Z
0.20ux
00U)
r.x
0)0.0
z'
>-. 0
)0 5-.0
U0u:.
L.oo)
(OX v)o- +
Lf)is-sOx
-4
=*0 c>.
a A, X~~
x u
N4 0c
so) Li)sCl
C CCl
-0 0
0z 0 00
cl) -d-
,-- Cl4 enCl4 Cl4 Cl Cl4
Volume 161Number 3 423
6
0
~obo
0S.
0
._
u
U)
0
0o._
--~0 _
0)- CIt4 N
ho
0
0)
0.5
1-
4
z
c_
U
5L)
ox
Cl400
0 .0 .0
.n . cn .7C.) U) U
X4 X X
0-0
U
0
.0
-.
0
z
LO O
g - g
d) 0 0)
0 0
e Cd
0) 0)t
0 -
0 n
00)
._0
0.)
2 C.0 o-C;
)
-I 00
\0 \0C01-o
5- '
0o
0)
0 .X
0) -0
) %
ON cq
.- Cl~o
0o \00% ON
0 -WU-)
00 C%
N
0).2
Cvl
0.0

424 CROCKER AND VEITH Annals ofSM
6 C;~~6°~ ~ ~>> ° t- -} Q >E .
0o
0>~~~~~~~~~~*.~~~~~~04
S .c. v) . tn ( . ) . e.0. . 0
4~~~~~~~~~~~~~~~~~-- .-: 4]E *E4 Ef:L.
Cd C4(1d
E >1~ ~ ~ =>b0 05_x
O o 0; SS0
CSCS aSO0 0 UCh O * *t; cs d C.) C.
-0 M C) E .
bc0 ) C0 0 0
ho
E~o00bO 00
0~~~~~~~~~~~~~~~~~~~~~~(14 0%
~~ ~ ~ ~~0.00 0 .0
0C
cl S.
E.
0 = .z~~~~~~~~~~~~~~~~~~~
4-i~~ ~ ~ ~ ~ ~ ~
cn 00~~~~~~~~~~~~~~~~~~s0-
C.)~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~bO C
a-~~~~~~~~~~~~~~~~~
6; c 00
r-qcCa
urgery1965

MESODERMAL TUMORS AND HYPOGLYCEMIA
2 months to 47 years. That a benign tumorcan precede the onset of hypoglycemia byan unusually long interval was illustratedby two cases. A mass in the left hemithoraxwas known to be present for 20 years (Case23) and 47 years (Case 22) prior to theonset of hypoglycemia. In almost half thepatients the presenting complaint was
symptoms subsequently ascribed to hypo-
glycemia. Unfortunately the bizarre be-havior exhibited at times by these patientshas sometimes led to committal for psy-
chiatric evaluation. With increasing severityof the attacks, hypoglycemic shock was
common. Blood sugar determinations dur-ing the attacks established the diagnosis inthe more obscure cases. Recognition of a
tumor did not always resolve the confusion.Despite the presence of a large mass in thethorax, several patients had an abdominalexploration and sometimes subtotal pan-
createctomy before a thoracotomy was per-
formed.23, 30 After a pancreatic source ofhyperinsulinism has been ruled out, there isno doubt that total or partial surgical ex-
cision of the extrapancreatic tumor can bebeneficial and should be done before per-
forming an empirical distal pancreatectomy.Surgical excision of tumor was carried
out in 18 of the 29 patients. Postoperativeremissions of hypoglycemia have beenachieved in all 18 patients who had excisionof tumor and remissions have lasted as
long as 5 years (Case 17). In eight in-stances follow-up examinations 4 to 31months after excision revealed that the pa-tients were living and well with continuousrelief of hypoglycemia. Two patients hadrecurrence of hypoglycemia 4 years (Case29) and 5 years (Case 17) after excision.Of the five patients who had explorationwith biopsy only three died, one was
benefitted by postoperative irradiation andno follow up was recorded for the fifthpatient. All four patients who underwentexploration only and the two patients who
had no operation died. Nine of 11 patientsin whom the tumor was not excised had a
rapid downhill course with a fatal outcome,due primarily to hypoglycemia.When an accessible tumor severely alters
metabolic processes, operation is indicatedeven if the tumor is not completely resecta-ble, since it has been shown that excisionof a large bulk of the tumor will relievethe hypoglycemia. The remission timewhich has been as long as 2 15 to 7 years,2
more than justifies subtotal excision. Thealternative, severe intractible hypoglycemia,is a more common cause of death in thisgroup of patients than are the other growtheffects of the tumor. This fact is well il-lustrated by the rapid demise of those pa-
tients who did not have a resection.Recurrence of tumor and associated hy-
poglycemia is encountered with these mas-
sive tumors.2 15 32 9 When recurrence is as-
sociated with hypoglycemia, re-excisionshould be performed if feasible. The bene-ficial result is illustrated by our case andby Cases 17 and 29. In Case 17, hypo-glycemia was relieved for 5 years by ex-
cision of a large retroperitoneal fibrosar-coma. Excision of a large recurrence pro-
duced another remission of hypoglycemiadespite the existence of pulmonary metas-tases. In Case 29, hypoglycemia recurred 4years after the first excision. Excision oflarge recurrent tumor nodules resulted ina second remission.There is some evidence that radiotherapy
is effective in reducing tumor size andthereby relieving hypoglycemic symp-toms.21' 29 37 Even when radiotherapy doesnot produce visible regression of tumor,the blood sugar level may be raised.37 Com-bined surgical enucleation and radiationproduced a good result for 16 months inMacNaughton's case.21 Unfortunately themajority of mesodermal tumors associatedwith hypoglycemia are probably insuffi-ciently radiosensitive to be influenced bythis mode of treatment so that operationremains the treatment of choice.The mechanism responsible for hypo-
glycemia is not clear and many explanations
Volume 161Number 3 425

426 CROCKER AND VEITH Annals of Surgery426 March ~~~~~~~~~~~~~~~~~~~~~~~~~~1965have been proposed. The three most popu-lar theories are 1) secretion of insulin oran insulin-like substance by the tumor, 2)excessive carbohydrate utilization by thetumor and 3) insufficient hepatic glycogenstorage. The finding of increased insulin-like activity in the tumor extracts of fivepatients 3, 5, 26, 45, 47 and in the serum of onepatient46 tend to support the first theory.The positive radio-immunoassay for insulinin extracts of both tumor and serum inOleesky's case 29 further strengthens thisview. Although negative results could al-ways be due to faulty methodology, somemechanism other than the production of asubstance with, or simulating, insulin-likeactivity must be considered in our case andthe nine others with negative insulin assays.Whatever the mode of action it would ap-pear that the functional ability of certaintumors becomes evident clinically onlywhen the tumor attains a huge size.
Summary and Conclusions
The recent literature on non-epithelialtumors associated with hypoglycemic symp-toms is reviewed and a case of recurrentlocally invasive hemangiopericytoma asso-ciated with hypoglycemia is reported. Thefunctional ability of this tumor became ap-parent only when recurrent tumor attaineda large size 10 years after the first excision.Hypoglycemic symptoms were relieved bysubtotal excisions of the tumor.
This review illustrates the importance ofseeking out functioning tumors and theeffectiveness of reduction of tumor mass inalleviating hypoglycemic symptoms. Theimportance of a vigorous surgical attack onthese tumors is emphasized. This can be alife-saving measure since it is not uncom-mon for these patients to die in hypo-glycemic shock rather than as a result ofmetastases which, in fact, are uncommon.
References
1. Andreew, V. von, I. Goranow and G. Krasti-now: Hypoglykamie bei einen intrathorakalgelagerten Fibrom. Endokrinologie, 38:167,1959.
2. Arkless, H. A.: Coincidence of Rhabdomyo-fibroma of the Diaphragm, Idiopathic Hypo-glycemia and Retroperitoneal Sarcoma. Med.Bull. Vet. Admin., 19:225, 1942.
3. August, J. T. and H. H. Hiatt: Severe Hypo-glycemia Secondary to a NonpancreaticFibrosarcoma with Insulin Activity. N. Engl.J. Med., 258:17, 1958.
4. Barjon, P. and R. La Bange: HypoglycemicMesenchymal Tumors. Presse Med., 69:2635,1961.
5. Boshell, B. R., J. J. Kirschenfeld and P. S.Soteres: Extrapancreatic Insulin-SecretingTumor. N. Engl. J. Med., 270:338, 1964.
6. Bousvaros, G. A.: Hypoglycemia in MetastaticFibrosarcoma of Liver. Brit. Med. J., 1:836,1960.
7. DeCoster, A., M. Payfa, R. Bellens, V. Conradand P. A. Bastenie: Intrathoracie Tumor andHypoglycemia. J. Franc. Med. Chir. Thor.,16:191, 1962.
8. Duncan, G. G. and G. I. Schless: MassiveRetroperitoneal Fibrosarcoma, SpontaneousHypoglycemia and Generalized Splanch-nomegaly: Report of a Case. Metabolism,10:200, 1961.
9. Fast, B. B.: Hypoglycemia Associated withMassive Intraabdominal Mesenchymal Tu-mor. Winnipeg Clin. Quart., 15:104, 1962.
10. Fikenscher, T. F. and P. S. Blom: Hypo-glycemia and Fibrosarcoma. Ned. T. Geneesk,107:1076, 1963.
11. Garfield, C. R., H. V. Belcher and J. S.Shuttleworth: Fibrous Mesothelioma withHypoglycemic Psychosis and Coma. J.A.M.A., 181:380, 1962.
12. Gold, G. L. and B. I. Shnider: Some UnusualSyndromes Associated with Neoplastic Dis-ease. Ann. Int. Med., 51:890, 1959.
13. Hayes, D. M., C. L. Spurr, J. H. Felts andE. C. Miller, Jr.: Von Recklinghausen's Dis-ease with Massive Intraabdominal Tumorand Spontaneous Hypoglycemia: MetabolicStudies Before and After Perfusion of Ab-dominal Cavity with Nitrogen Mustard.Metabolism, 10:183, 1961.
14. Heiskala, H. and M. Gylling: HypoglycemiaAssociated with Carcoma. Duodecim, 79:543, 1963.
15. Hines, R. E.: Hypoglycemia Apparently Dueto Retroperitoneal Sarcoma. Med. Bull. Vet.Admin., 20:102, 1943.
16. Holton, C.: Hypoglycemia-Inducing TumorsResembling Spindle Cell Sarcoma. Acta Med.Scand., 157:97, 1957.
17. Howard, J. W. and P. L. Davis: Retroperi-toneal Hemangiopericytoma Associated withHypoglycemia. Delaware State Med. J., 31:29, 1959.
18. Kuijjer, P. J.: A Tumor of the Lung with Dis-turbances in the Sugar MIetabolism. Arch.Chir. Neerl.. 13:81. 1961.

Volume 161 MESODERMAL TUMORS AND HYPOGLYCEMIA 427Number 3
19. Leger, L., C. Sors, C. Dubost, M. Megdelaine,J. Lejeune, E. Roseau and G. LeMaigre:The Hypoglycemia of Extrapancreatic Mes-enchymal Tumors. Presse Med., 71:219,1963.
20. Lowbeer, L.: Hypoglycemia Producing Extra-pancreatic Neoplasms. Amer. J. Clin. Path.,35:233, 1961.
21. MacNaughton, M. C. and E. A. Priest: Hypo-glycemia Associated with RetroperitonealLeiomyosarcoma. Lancet, 1:204, 1960.
22. Mahon, W. A., M. L. Mitchell, J. Steinke andM. S. Raben: Effect of Human GrowthHormone on Hypoglycemic States. N. Engl.J. Med., 267:1179, 1962.
23. Maier, H. C. and D. Barr: Intrathoracic Tu-mors Associated with Hypoglycemia. J.Thor. Cardiov. Surg., 44:321, 1962.
24. McLeod, C. E.: Report of an Additional Caseof Extrapancreatic Tumor Associated withHypoglycemia. Conn. Med., 24:458, 1960.
25. Meyer-Hofmann, von G., H. Schwarzkopf andH. Hartmann: Spontaneous Hypoglycemiawith Extrapancreatic Tumors. Deutsch. Med.Wschr., 85:2106, 1960.
26. Miller, D. R., R. E. Bolinger, D. Janigan, J.E. Crockett and S. R. Friesen: HypoglycemiaDue to Nonpancreatic Mesodermal Tumors:Report of Two Cases. Ann. Surg., 150:684,1959.
27. Murphy, R.: Hypoglycemia Associated with anExtrapancreatic Neoplasm. Med. Clin. N.Amer., 47:391, 1963.
28. Nevius, D. B. and N. B. Friedman: Meso-theliomas and Extraovarian Thecomas withHypoglycemic and Nephrotic Syndromes.Cancer, 12:1263, 1959.
29. Oleesky, S., I. Bailey, E. Samols and D. Bilkus:Fibrosarcoma with Hypoglycemia and aHigh Serum Insulin Level. Lancet, 2:378,1962.
30. Paulson, G. S., J. J. Feehan and R. S. Westaby,Jr.: Severe Hypoglycemia Due to Meso-thelioma Arising in Pleural Cavity. S. DakotaJ. Med. Pharm., 14:5, 1961.
31. Pederson, J., F. Lund and J. Ringsted: Hypo-glycemia in Presence of Massive Fibrosar-coma. Acta Endocr., 34:148, 1960.
32. Porter, M. R. and V. K. Franz: Tumors As-sociated with Hypoglycemia-Pancreatic andExtrapancreatic. Amer. J. Med., 21:944,1956.
33. Rogers, J. G. and J. M. Houseworth: LargeFibrogenic Tumors and Hypoglycemia.J.A.M.A., 178:1132, 1961.
34. Rossman, E. M.: Mediastinal Neurofibrosar-coma Causing Hypoglycemia. Arch. Int.Med., 104:640, 1959.
35. Sachsse, V. B. and H. Blank: FunktionelleHypoglykamie und organischer Hyperin-sulinismus. Deutsch. Med. Wschr., 84:1679,1959.
36. Schmidt, H. W. and K. Schuerholz: Hypo-glycemic Attacks Due to Intrathoracic Tu-mors. Deutsch. Med. Wschr., 86:2231, 1961.
37. Scholz, D. A., L. B. Woolner and J. T. Priest-ley: Spontaneous Hypoglycemia Associatedwith Fibrogenic Tumor. Ann. Int. Med.,46:796, 1957.
38. Sors, C., L. Leger, C. Dubost and G. Thom-eret: Hypoglycemic Thoracic Mesotheliomas.Rev. Tuberc. (Paris), 26:1268, 1962.
39. Stauffer, J. M., G. E. Granville and S. W.Law: Recurrent Hypoglycemia and Retro-peritoneal Fibrosarcoma. N. Engl. J. Med.,265:979, 1961.
40. Stout, A. P.: Hemangiopericytoma. Cancer,2:1027, 1949.
41. Stout, A. P. and M. R. Murray: Hemangio-pericytoma: A Vascular Tumor FeaturingZimmermann's Pericytes. Ann. Surg., 116:26,1942.
42. Stout, A. P.: Personal communication.43. Thome, G.: C.P.C. N. Engl. J. Med., 268:
1129, 1963.44. Tranquada, R. E., A. B. Bender and P. M.
Beigelman: Hypoglycemia Associated withCarcinoma of the Cecum and Syndrome ofTesticular Feminization. N. Engl. J. Med.,266:1302, 1962.
45. Volk, B. W., M. G. Goldner and B. Wainfield:Spontaneous Hypoglycemia with AbdominalSpindle Cells Sarcoma. Geriatrics, 15:473,1960.
46. Whitney, J. E. and C. G. Massey: ApparentInsulin Activity in a Fibrosarcoma Associatedwith Spontaneous Hypoglycemia. J. Clin.Endocr., 21:5, 1961.
47. Whitney, J. E. and B. I. Heller: Increased In-sulin-Like Activity of Serum in Patient withSpontaneous Hypoglycemia Associated withRetroperitoneal fibrosarcoma. Amer. J. Med.,30:633, 1961.