Embed Size (px)
Citation preview
Mental Mental Mental Mental RetardationRetardationRetardationRetardation
4/
9/
03
2
:3
6:
58
P
M
2
Introduction
! History’s influence! Dual Diagnosis
! Etiology! Specific Disorders
4/
9/
03
2
:3
6:
58
P
M
3
HistoryHistoryHistoryHistory
! Many hindering elements– Death– Persecution
! Religion! Middle Ages
• Led to general lack of concern

4/
9/
03
2
:3
6:
58
P
M
4
History Cont…History Cont…History Cont…History Cont…
! 1690 John Locke’s “Blank Slate”! 1800s Jean-Marc-Gaspard Itard! 1908 Binet’s IQ test
• Led to better understanding of innate differences
• Gave hope for help
4/
9/
03
2
:3
6:
58
P
M
5
History’s influence on History’s influence on History’s influence on History’s influence on DiagnosisDiagnosisDiagnosisDiagnosis
! 1900s: general knowledge about mental retardation widespread:– “Onset in childhood, significant intellectual or
cognitive limitations and inability to adapt to the demands of everyday life”
! But diagnostic criteria vague
4/
9/
03
2
:3
6:
58
P
M
6
Developing Diagnostic Developing Diagnostic Developing Diagnostic Developing Diagnostic CriteriaCriteriaCriteriaCriteria
! 1910: American Association on Mental Deficiency (AAMR) defined according to functional level– Idiot: 2 year old– Imbecile: 2-7 year old– Moron: 7-12 year old
! Obvious problems

4/
9/
03
2
:3
6:
58
P
M
7
Dev. Diagnostics Cont…Dev. Diagnostics Cont…Dev. Diagnostics Cont…Dev. Diagnostics Cont…
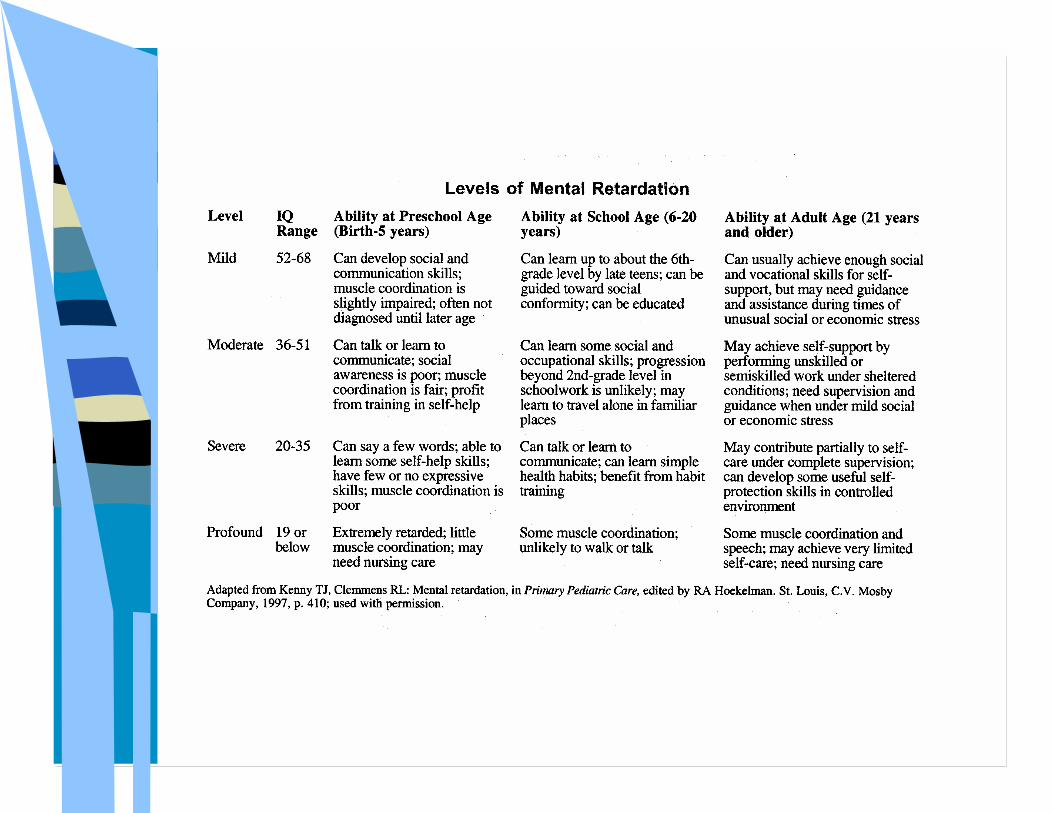
! Revisions based on IQ– Overlaps cause overestimation
! New IQ levels established– Mild:50-70– Moderate:35-50– Severe:20-35– Profound:<20
• STILL too vague

4/
9/
03
2
:3
6:
58
P
M
8
Current Diagnostic CriteriaCurrent Diagnostic CriteriaCurrent Diagnostic CriteriaCurrent Diagnostic Criteria
! Multidimensional approach (DSM-IV, ICD10)– Limits in present functioning– Sub-average IQ– 2 or more:
• Communication, self-care, home living, social skills, community use, self-direction, health and safety, functional academics, leisure, and work
4/
9/
03
2
:3
6:
58
P
M
9

4/
9/
03
2
:3
6:
58
P
M
10
Dual DiagnosisDual DiagnosisDual DiagnosisDual Diagnosis
! Theory that mental retardation exists in conjunction with psychopathologies.– Psychopathologies are not innate
qualities, rather they are developed

4/
9/
03
2
:3
6:
58
P
M
11
! The slow development of diagnostic criteria hindered research for centuries
! New approaches and techniques!!– Etiological approaches– Genetic and biological findings related to
behavior• biopsychosocial

4/
9/
03
2
:3
6:
58
P
M
12
EtiologyEtiologyEtiologyEtiology
! 2 Types:– Idopathic: non-specific: no apparent
cause– Organic: specific
• Pre-natal: chromosome abnormality• Peri-natal: hypoxia, apoxia• Post-natal: brain injury

4/
9/
03
2
:3
6:
58
P
M
13
Etiology Cont…Etiology Cont…Etiology Cont…Etiology Cont…
! Most retardation is mild! Most cases of mild retardation are
combinations of peri- and post-natal causes
! 20-30% of pre-natal causes lead to severe retardation
4/
9/
03
2
:3
6:
58
P
M
14
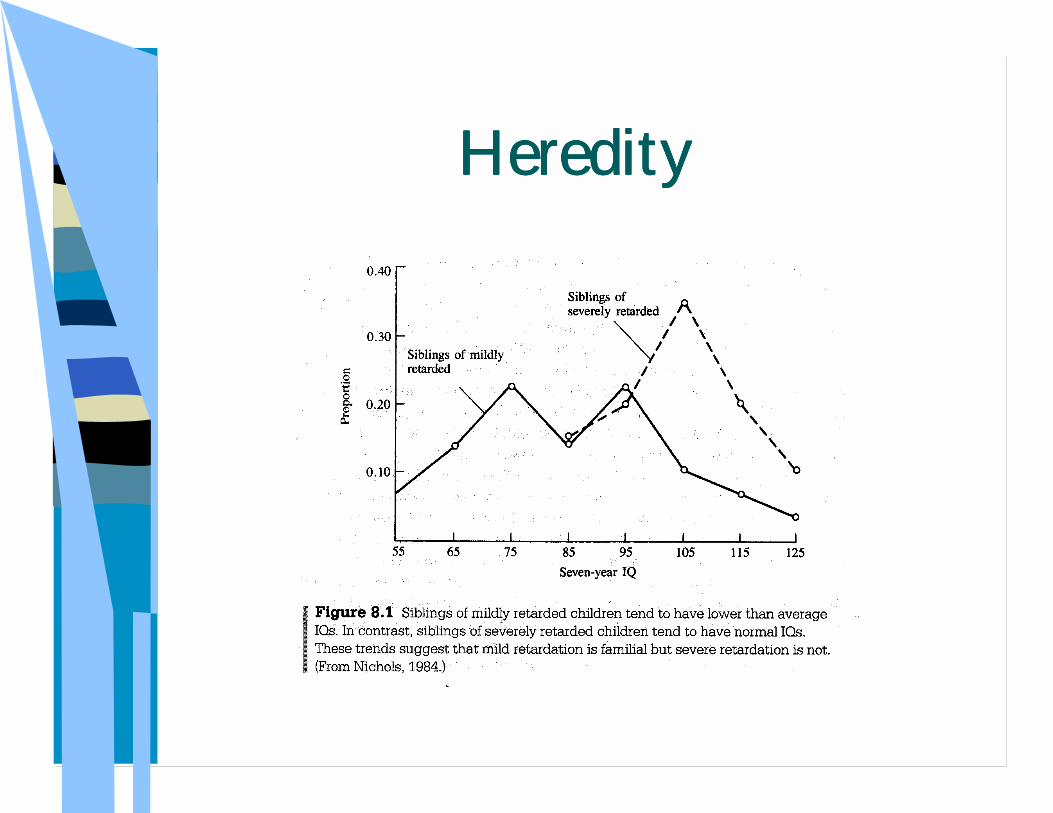
HeredityHeredityHeredityHeredity

4/
9/
03
2
:3
6:
58
P
M
15
PrePrePrePre----Natal RetardationNatal RetardationNatal RetardationNatal Retardation
! Specific genetic effects that cause! Breakthrough research
– Genetics and psychology coupled with biology
4/
9/
03
2
:3
6:
58
P
M
16
WilliWilliWilliWilli----Prader Prader Prader Prader and and and and AngelmanAngelmanAngelmanAngelman
! Both chromosome 15– WP=paternal, affects mRNA processing– AS=maternal, affects ubiquitin ligase
gene that is crucial in development
! Both syndromes from same location! Very different behavioral
characteristics
4/
9/
03
2
:3
6:
58
P
M
17
Cont…characteristicsCont…characteristicsCont…characteristicsCont…characteristics
! Willi-Prader Syndrome– Hyperphagia and impaired satiety
response • Leads to food-stealing and seeking
– OCD (similar to non-retarded)– Behaviors: tantrums, out bursts,
impulsivity, argumentativeness, sadness, withdrawal, and peer problems*• Due to disorder?? Or part of it?

4/
9/
03
2
:3
6:
58
P
M
18
Cont… CharacteristicsCont… CharacteristicsCont… CharacteristicsCont… Characteristics
! Angelman Syndrome– Moderate retardation, abnormal gait,
speech impairment, seizures, and inappropriate happy demeanor*
– Needs further study

4/
9/
03
2
:3
6:
58
P
M
19
ImplicationsImplicationsImplicationsImplications
! Good Willi’s biological start! Some good psychological correlations! Research needed to find biological
abnormalities related to behaviors! And also specifying differences in
maternal and paternal etiology
4/
9/
03
2
:3
6:
58
P
M
20
William’s SyndromeWilliam’s SyndromeWilliam’s SyndromeWilliam’s Syndrome
! Chromosome 7: next to elastin gene, connective tissue disorder
! Anxiety disorders unrelated to age or gender– Environment? Or genetic?

4/
9/
03
2
:3
6:
58
P
M
21
Cont…characteristicsCont…characteristicsCont…characteristicsCont…characteristics
! Behavior: Inattention, hyperactivity, ADHD, impulsivity, and social dis-inhibition
! Language>visial-spatial, visual-motor, construction tasks, or figure copying
! Strengths: memorizing and recognizing faces, auditory short-term memory, and musical talents

4/
9/
03
2
:3
6:
58
P
M
22
ImplicationsImplicationsImplicationsImplications
! Good advocate for dual diagnosis! Need research on biological aspects
4/
9/
03
2
:3
6:
58
P
M
23
Fragile XFragile XFragile XFragile X
! Expanded triplet repeat– 200+ CGGs
! Inactive FMR1 gene (lack gene product FMR1P)– Essential for pre- and post-natal
development– Regulates proteins for synaptic activity

4/
9/
03
2
:3
6:
58
P
M
24
TransmissionTransmissionTransmissionTransmission
! Repeats increase each generation until the X Chromosome becomes ‘fragile’ at a critical region when examined by scientists.
! Not hereditary, chromosome abnormality
4/
9/
03
2
:3
6:
58
P
M
25
Three TypesThree TypesThree TypesThree Types
! Males with full mutations– Mild to moderate IQ, intact verbal abilities– Struggle with short-term memory, audio,
verbal, and perceptual tasks! Mosaic Males (partial FMR1P)
– Higher IQ, moderate symptoms! Females
– Least symptoms (X-inactivation)
4/
9/
03
2
:3
6:
58
P
M
26
BiologicalBiologicalBiologicalBiological
! Studies have found:– Enlarged caudate nucleus
• Inhibition, motor activity, and environmental responses
– Decreased cerebellar vermis size in males• Inattention, hyperactivity, hypersensivity to
stimuli

4/
9/
03
2
:3
6:
58
P
M
27
ImplicationsImplicationsImplicationsImplications
! Since the discovery in 1991, enormous amounts of research has linked:– FMR gene with FMR1P production– FMR1P effect on symptoms– Biological abnormalities that account for
symptoms! Pioneering research must continue

4/
9/
03
2
:3
6:
58
P
M
28
ConclusionConclusionConclusionConclusion
! Fears:– Eugenics– Prejudice
4/
9/
03
2
:3
6:
58
P
M
29
Conclusions Cont…Conclusions Cont…Conclusions Cont…Conclusions Cont…
! Research techniques incorporate 3 important fields:– Biology– Psychology– Genetics
• Non-invasive way to research

4/
9/
03
2
:3
6:
58
P
M
30
!
Biasini, Fred,Lisa Grupe, Lisa Huffman, Norman Bray.“Mental Retardation: A Symptom and a Syndrome”. (To appear in S.Netherton, D. Holmes, & C. E. Walker, (Eds.), Comprehensive Textbook of Child and Adolescent Disorders. New York: Oxford University Press, in press) (found at http://www.uab.edu/cogdev/mentreta.htm)
! Plomin, Defries, McClearn, and McGuffin. Behavioral Genetics, Fourth Edition. Worth Publishers, NY: 2001.
! MERCK MANUAL http://www.merck.com/mrkshared/mmanual_home/sec23/255.jsp: 3/22/03
! ERIC Digests http://www.ericfacility.net/ericdigests/ed372593.html: 3/22/03
! Elisabeth Dykens and Robert Hodapp. “Research in Mental Retardation: Toward an Etiological Approach,” Journal of ChildPsychol. Psychiat. Vol. 42, No. 1 pp. 49-71. Cambridge University Press: 2001.
4/
9/
03
2
:3
6:
58
P
M
31





























