Embed Size (px)
Citation preview

Mental Il lness & Suicide in the Media
A Mindframe Resource for the Cour ts

c) Commonwealth of Australia
ISBN: 1-74186-539-5
Online ISBN: 1-74186-540-9
This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced by any process
without written permission from the Commonwealth. Requests and inquiries concerning reproduction rights should be directed to the
Commonwealth Copyright Administration, Attorney Generals Department, Robert Garran Offices, National Circuit, Canberra, ACT 2600
or posted at http://www.ag.gov.au/cca
The opinions expressed in this document are those of the authors and are not necessarily those of the Commonwealth.
Content developed by the Hunter Institute of Mental Health in consultation with an Advisory Group of experts, for the Mental Health
and Suicide Prevention Programs Branch, of the Australian Government Department of Health and Ageing.
Designed by Advocart Pty Ltd
Publications approval number: P3-3362
The project website at www.mindframe-media.info contains the most up to date information and advice on how to obtain additional
copies of the resource.

Foreword
In Australia, one in five people will directly experience a mental illness in their lifetime and recent data suggests about 1800 people take their own life each year. The media has an important role to play in influencing community attitudes towards and perceptions of both mental illness and suicide.
The courts are an important news source for most media organisations. Information is accessible, timely, and viewed as having high human or dramatic interest. Often, court stories involve themes of fear, horror or shock, and much information can be deeply personal and intimate. Through court and inquest proceedings journalists are privy to details about a person’s mental health status, specific details about a suicide death, and claims made by witnesses, victims and experts called to give testimony.
Australian research1 has indicated that the most problematic type of news coverage of mental illness and suicide results from information collected at courts and coroners courts, or from the police. While magistrates, coroners and other court officials may not talk directly to the media or seek out media coverage on a regular basis, their general dealings with journalists may have an impact on the way a story is developed.
Mental Illness & Suicide in the Media: A Mindframe Resource for Courts has been produced as part of the Australian Government’s Mindframe National Media Initiative. This Initiative aims to encourage responsible, accurate and sensitive coverage of suicide and mental illness through a range of complimentary projects working with the media in Australia.
This resource provides practical advice and information for judges, magistrates, coroners, media liaison officers and other court staff to support their work with the media. This may be through indirect means, such as statements and remarks made in court, or directly through comments or information provided to the media.
As representatives of peak media bodies, suicide prevention and mental health organisations
and the Australian Government, we commend this resource to you.
National Media and Mental Health Group, April 2008
This resource contains practical information for courts to support their direct and indirect
interactions with the media. It contains suggestions for providing or managing information
about mental illness or suicide that are consistent with best practice guidelines for reporting.
‘I don’t want to be told what to say and do, but I do want to be informed about what I say and do’.
This resource has been developed as part of the Mindframe for Police and Courts Project.
It was developed by the Hunter Institute of Mental Health in consultation with an Advisory
Group of experts, with funding from the Australian Government Department of Health and
Ageing as part of the Mindframe National Media Initiative.
The development of this resource has been informed by consultations with a variety of
stakeholders across Australia, including:
n Media liaison officers in departments of justice;
n Individual judges, magistrates and coroners;
n Administrators of courts;
n Media professionals;
n Mental health and suicide prevention experts;
n Members of the National Media and Mental Health Group.
This resource is also available in electronic form at www.mindframe-media.info
About th i s resource

Contents
1. Introduction 1
2. Mental Illness in the Media 5
n Evidence of Impact ......................................................................................................... 6n Key Issues to Consider – Judicial Officers ................................................................. 8n Key Issues to Consider – Other Officers of the Court ............................................. 11n Mindframe Considerations for Media Professionals .............................................. 14
3. Suicide in the Media 15
n Evidence of Impact ....................................................................................................... 16n Key Issues to Consider – Judicial Officers ............................................................... 18n Key Issues to Consider – Other Officers of the Court ............................................. 21n Mindframe Considerations for Media Professionals .............................................. 24
4. About Mental Illness 25
n Specific Mental Illnesses ............................................................................................ 26n Mental Illness in Australia ........................................................................................... 31n Common Myths about Mental Illness ........................................................................ 33
5. About Suicide 35
n An Overview of Suicide in Australia .......................................................................... 36n Common Misconceptions about Suicide .................................................................. 44
6. Media and the Courts 45
7. Further Information 51
n Helplines & Contacts .................................................................................................... 53n References ..................................................................................................................... 58

Ac knowledgements
This resource was developed by the Hunter Institute of Mental Health, in partnership with an Advisory Group
of experts, for the Mental Health and Suicide Prevention Programs Branch of the Australian Government
Department of Health and Ageing.
People involved in the development of this resource include:
Jaelea Skehan, Martin O’Connor, Michael Romeo, Amy Visser & Trevor Hazell (Hunter Institute of Mental
Health); Jane Johnston (Griffith University); Terry Anderson (South Australia Courts); Elizabeth Gaynor (Victoria
County Court); John Arms (NSW Coroner’s Courts); Sue Hunt, Annabel Dobson & Kirrily Cornwell (Department
of Health and Ageing).
The project team also acknowledges the involvement of the following people in the consultation and review
process for these resources:
Michael Johnson & Hugh Jorgenson (ACT Magistrates Court), John Merrick (NSW State Coroners Office),
Magistrate Wayne Evans & Magistrate Jeff Linden (Magistrates Courts NSW), Chief Magistrate Brian Martin
(NT), Dr Celia Kemp (NT Coroners Court), Lorelei Fong Lim (NT Justice), Dianne Pendergast & Louise Logan
(Queensland Adult Guardian), Paul Rutledge (Queensland Department Public Prosecutors), Susan Gardiner
(Queensland Guardianship and Administration Tribunal), Wendy Grenfell (Queensland Health), Marcus Richard
(Queensland Office of Public Advocate), Mark Johns (SA State Coroner), Magistrate Bill Ackland (SA),
Jim Connolly (Tasmania Courts Administration), Arnold Schott (Tasmania State Coroner), Graeme Johnstone
(Victoria State Coroner), Louise Glanville (Victoria Attorney General’s office), Maria Lusby (Victoria Judicial
College), Chief Judge Michael Rozenes (Victoria County Court), Sue James (WA Department of Justice),
and Cathy Heycock (SANE Australia).
The project team recognises the advice and support from the National Media and Mental Health Group that
provides guidance to all projects funded under the Mindframe National Media Initiative:
Ms Heather Forbes & Ms Rhianna Patrick (Australian Broadcasting Corporation), Dr Matthew Dobson
(Australian Communications and Media Authority), Ms Alina Lieurance (FreeTV Australia), Commercial Radio
Australia, Mr Warwick Costin & Mr Rex Jory (Australian Press Council), Mr Michael Winter (Australian
Writers’ Guild), Ms Georgina McClean (SBS), Mr Clive Skene (Flinders Medical Centre), Ms Barbara Hocking
(SANE Australia), Ms Julie Foster (beyondblue), Ms Janet Meagher (Australian Mental Health Consumer
Network), and Mr Simon Tatz (Mental Health Council of Australia).

1
The media has an important role to play in influencing community attitudes towards and
perceptions of both mental illness and suicide. Research2 about the way the Australian media
portrays suicide and mental illness indicated that the most problematic type of news coverage
about these issues resulted from information collected by journalists at courts and coroners
courts, or from the police.
While magistrates, coroners and other members of the court rarely talk directly to the media,
courts remain a major source of information for journalists. Along with police stations, the
courts are routine sites for gathering news, and media organisations invest considerable
resources in this type of journalism3. Court proceedings are scheduled, so they become part
of the regular news diary. Courts and court information is easily accessed by editors and
journalists, it can be planned for and predicted, and is efficiently and effectively monitored.
Courts are a valuable source of information for the media about incidents and cases where
mental illness or suicide may be raised. In fact, having mental illness raised in court may make
a particular case more ‘newsworthy’. Similarly, suicide deaths that result in a coronial inquiry
may be of more interest to journalists, due to speculation about the cause of death or possible
breaches in duty of care.
Often crime and court stories involve themes of fear,
horror or shock, and much information can be deeply
personal and intimate. Australian research found
that these framing devices are not only identified
in major Australian newspapers and broadcast
media, but also appear in regional news4. In addition,
sensational or inappropriate language in the
headline or broadcast leads in these types of stories
is common.
‘Schizo’ teen jailed 10 years.
A schizophrenic teenager who battered his friend to death with a lump of timber has been jailed for 10 years by a Sydney court.
Northern Territory News (2007, 11 August, p.15)
Introduction

2
Courts and coroners courts often give journalists access to quite shocking and graphic or bizarre details, such as the manner of a death or the circumstances leading up to an incident. Sometimes shocking detail may be justified by the need to draw attention to the seriousness of a particular case. However, it is possible that vulnerable groups could interpret this information in a different way.
This resource provides practical advice and information for judges, magistrates, coroners, media liaison officers and other court staff to support their work with the Australian media. This may be through indirect means, such as statements and remarks
made in court, or directly through comments or information provided to the media.
The key sections of this resource are those that specifically outline the Issues to Consider when working with the media about mental illness or suicide. The ‘orange’ tabbed sections at the front of the resource summarise key points related to Mental Illness in the Media and Suicide in the Media.
In response to needs identified in consultations about the development of this resource some additional sections have been added. The ‘green’ tabbed sections provide some general facts, statistics and information About Mental Illness and About Suicide. The final ‘yellow’ tabbed sections contain basic information about Media and the Courts, along with Further Information about the Mindframe website and some other useful websites and contacts for further information.
The resource has been developed following consultation with a range of court representatives in each state and territory. The information is supported by a more comprehensive website at www.mindframe-media.info
‘I always find it
interesting… reading
about or watching
programs about people
who suicide. In a way I
look up to people who kill
themselves. I think, well,
so many other people do
it, maybe I’ll do it as well.’

3
The Mindframe National Media Initiative (Mindframe Initiative) is funded by the Australian Government Department of Health and Ageing and guided by the National Media and Mental Health Group. The Initiative aims to influence media coverage of issues related to mental illness and suicide by encouraging responsible, accurate and sensitive portrayals. The strategy includes a number of complementary projects and resources, working with a variety of sectors in Australia, as outlined in Figure 1.
Projects and resources funded under the Mindframe Initiative include:
n The Media Monitoring Project 2001, 2007 – providing critical reviews of the international literature and investigating the extent and nature of reporting in Australia through a 12-month baseline study in 2001 and a 6-year follow-up study in 2007;
n The Mindframe Media and Mental Health Project – developing and promoting resources and professional development opportunities for media professionals to encourage accurate and sensitive reporting of suicide and mental illness;
n The Response Ability Project – developing and disseminating curriculum resources for the university training of journalism students and support for Australian universities implementing the materials;
n SANE Australia’s Media Centre – supporting both media and the mental health sector in the development of stories about suicide and mental illness, including the community action site, StigmaWatch;
n Mindframe for the Mental Health Sector – developing and promoting resources and professional development opportunities for the mental health and suicide prevention sectors;
n Mindframe Stage and Screen – developing and promoting resources for scriptwriters and other people involved in the development of Australian film, television and theatre;
n Mindframe for Police and Courts – developing and disseminating resources and professional development opportunities for police and the courts.
More information on all projects and resources funded under the Mindframe Initiative are available from www.mindframe-media.info
The Mind f rame Nat iona l Media In i t i at ive

4
Figure 1: Resources and projects under the Mindframe Initiative
Mindframe for Police- Resources for police officers
Mindframe Media and Mental Health Project- Resources for media
professionals
Mindframe for Courts - Resources for
judicial and other officers of the courts
The Media Monitoring
Study, 2001, 2007
SANE Australia’s Media Centre &
StigmaWatch program
National Media and Mental Health Group
Including representatives from the Australian Government Department of Health and Ageing,
peak media bodies and mental health and suicide preventation organisations.
Response Ability for Journalism Education
- Resources for university training of journalism students
Mindframe Stage and Screen
- Resources for Australian film,
television and theatre
Mindframe for the Mental Health Sector
- Resources for the mental health and
suicide prevention sector

5
Research has indicated that for many people the media is their primary source of information about mental illness5. According to national and international research, mental illness tends to be portrayed negatively in the mass media. While Australian research6 has demonstrated that media reporting of mental illness may be improving, examples of inappropriate reporting can still be seen.
Negative reporting of mental illness appears to influence community attitudes, which in turn may lead to stigma and discrimination7. Instances of negative reporting impact significantly on people experiencing mental illness and may reduce appropriate help-seeking behaviour, resulting in untreated illness and possibly contributing to suicidal thinking and behaviour8.
We’re a long way off people accepting that mental illness is just another illness. There is still a stereotypical stigma attached to it that is negatively reinforced
every time there is bad reporting.9
Australian research has shown that coverage of mental illness that results from information collected at courts or from the police is the most problematic type of news coverage10. Many news stories from the courts about mental illness focus on violence. These stories relate to specific and relatively rare circumstances, but audiences are likely to draw generalised inferences about people diagnosed with a mental illness as a result.
As is the case in the general community, members of the media may hold misconceptions about mental illness that may influence the frame they use for a particular story. It is important, therefore, that people involved in the judiciary understand the potential impact of reporting mental illness in certain ways and are aware of the principles of best practice reporting promoted through the Mindframe Initiative.
What follows in this section is: a summary of research evidence regarding the impact of media reporting; issues to consider for judicial officers about indirect communication with the media; issues to consider for other officers of the court about direct communication with the media; and an outline of the issues media professionals are asked to consider when reporting mental illness.
Media Reporting of Mental Illness

6
Research has demonstrated that the media has an important role to play in informing and
influencing community attitudes towards mental illness and people affected by mental illness.
A summary of findings from a critical review of the national and international literature11 is
provided below.
The media is an important source of information for many people about mental health and mental illness.
n A German study found that the media is the most important source of information for many
people on mental health and illness and that negative media reports were more commonly
recalled than positive ones12.
n A number of American studies also found that the media is an important source of
information about mental health issues13, 14.
Mental illness tends to be portrayed negatively in news media, with coverage promoting negative images and stereotypes.
n An Australian study found that electronic and print media coverage often reflects and
perpetuates the myths and misunderstandings associated with mental illness15.
n A study of newspaper items on mental illness in a New Zealand newspaper in 1997 found
that mental illness was portrayed negatively and that people with a mental illness were
portrayed as a danger and a threat to the community16.
Courts are an important source of information for media stories involving mental illness.
Australian research has shown that the most problematic type of news coverage about mental illness results from information collected at court or from the police17.
Many of these stories focus on violence and relate to specific and relatively rare circumstances. Audiences, however, are likely to make generalisations about people
with a mental illness as a result.
Evidence of Impact: Media Repor ting of Mental Illness

7
Negative reporting of mental illness has a direct effect on attitudes.
n Individuals citing the media as the most important source of their information had more
negative attitudes towards mental illness18.
n Media accounts of mental illness that instil fear have a greater influence on public opinion
than direct contact with people who have a mental illness19.
n A number of studies demonstrated that exposure to negative stories, both fictional and non-
fictional, had a direct effect on attitudes which was not altered by subsequent exposure to
positive stories 20, 21.
n A German study found that students who read negative articles about mental illness
expressed more negative attitudes toward people with a mental illness22.
Negative portrayals impact directly on people living with a mental illness.
n Three quarters of consumers of mental health services in a UK study felt that media
coverage was ‘unfair, unbalanced or very negative’, while 50% believed media portrayal
of mental health issues had ‘a negative effect on their mental health’ 23.
n A survey by SANE Australia found that 95% of consumers believed that negative portrayals
of mental illness had an effect on them and 80% reported that the effect was negative.
Consumers described direct effects including distress, perceptions of stigma and
self-stigma24.
A more comprehensive summary of the research evidence is available from
www.mindframe-media.info

8
Courts are a valuable source of information for the media about incidents and cases where mental illness may be raised. In fact, having mental illness raised in court may make a particular case more ‘newsworthy’. Through court proceedings journalists are privy to details about a person’s mental health status, past mental ill health and claims made by witnesses and experts called to give testimony. While magistrates and other court officials may not talk directly to the media or seek out media coverage on a regular basis, their general dealings with journalists may have an impact on the way a story is developed.
This section is broken into two parts:
n PART 1 summarises some key issues to consider for judicial officers to guide their indirect contact with the media around mental illness.
n PART 2 summarises some key issues to consider for other officers of the court to guide their direct interactions with the media around mental illness.
These issues to consider support the guidelines provided to Australian journalists about the
reporting of mental illness (see page 14).
Issues to Consider: Judicial Officersn Consider the potential impact of the story and whether to make official comment. n Consider whether journalists will be able to understand and correctly interpret the
impact of mental illness on the proceedings and the judgement.n Check that your language is appropriate and that it does not stigmatise mental illness.n Be mindful not to reinforce common myths and stereotypes about mental illness.
Issues to Consider: Other Officers of the Courtsn Consider the potential impact of the story and whether to make official comment. n Where appropriate, provide information about treatment and support options for people
living with mental illness.n Check that your language is appropriate and that it does not stigmatise mental illness. n Be mindful not to reinforce common myths and stereotypes about mental illness.n Refer journalists to Mindframe.
Key I s sues to Cons ider

9
Par t 1 : For Jud ic i a l Of f i cer s
Consider the potential impact of a particular story and whether to make official media comment.
n Consider if you are able to provide comment or advice to media professionals. Do you need
advice or support from the Media Unit?
n Does the story have the potential to contribute to better understanding of mental health and
mental illness in the wider community? There may be the potential to include information
that will assist in understanding how mental illness is dealt with in the courts.
n If the story is more generally about mental illness, you may want to refer the journalist to the
‘expert comment’ section of the Mindframe website at www.mindframe-media.info
Consider whether journalists will be able to understand and correctly interpret the impact of mental illness on the proceedings and the judgement.
n When issuing judgements, consider whether it is possible to place statements relating
to mental illness in a context that minimises misinterpretation by members of the court,
including journalists.
n Journalists are asked to question whether mental illness actually contributes to a news
story in a significant way. Ensure that you provide enough information through remarks and
statements to assist them in making this judgement call.
n Is there any capacity for you to remind journalists present in court about their responsibilities
when reporting mental health and illness? This may prompt some journalists to do further
research before compiling the story.

10
In sentencing and remarks from the bench, check that your language is appropriate and that it does not stigmatise mental illness.
n A key part of court reporting involves quoting remarks made from the Bench. The language used when reporting on mental illness can contribute to stereotypes, myths and stigma. Journalists are unlikely to edit ‘direct quotes’ from sentencing remarks and judgements even when they recognise that the language may not be helpful.
n It is important that the language used is consistent with suggestions provided to the media. Your comments potentially reach many members of the community.
• Avoid negative language, e.g. ‘mental patient’, lunatic’, ‘schizo’, ‘psycho’ etc.
• Avoid labelling a person by their mental illness – e.g. a person is not ‘a schizophrenic’, they are ‘currently experiencing’, ‘being treated for’ or ‘have a diagnosis of’ schizophrenia.
• Be careful not to imply that all mental illnesses are the same and ensure that correct terminology is used in relation to specific diagnoses.
• Do not use diagnostic terms unless the diagnosis has been confirmed by a medical professional.
• Be aware of the language you use when referring to someone leaving hospital – e.g. a person is ‘discharged’ from hospital not ‘released’ and they ‘leave’ or ‘go missing’, they do not ‘escape’.
Be mindful not to reinforce common myths and stereotypes about mental illness.
n While news stories that emanate from court proceedings relate to specific and relatively rare circumstances, audiences are likely to draw from them general inferences about people living with a mental illness and the risk they may pose to the public.
n The type of information presented in court, and subsequent media reports, may reinforce stereotypes such as those that link mental illness with violence or suggest people with mental illness are unable to work, parent or lead fulfilling lives.
n Ensure not to make generalisations about mental illness broadly or specific mental illnesses.

11
Par t 2 : For Other Of f i cer s o f the Cour t
Consider the potential impact of a particular story and whether to make official media comment.
n Find out what the journalists needs, including the angle for the story. Is the issue about a judgement in a particular case, or more generally about the interface between mental illness and the courts?
n Consider whether the story has the potential to contribute to better understanding of mental health and mental illness in the wider community. There may be an opportunity to include information that will assist in understanding how mental illness is dealt with in the courts.
n While you always have the option of saying ‘no’ you may also want to consider the impact of not participating in a story. That is, the story may still be run without expert comment and advice. This may sometimes be worse than participating.
n If the story is more generally about mental illness, you may want to refer the journalist to the
‘expert comment’ section of the Mindframe website at www.mindframe-media.info
Where appropriate, provide information about treatment and support options for people living with mental illness.
n Stories that involve mental illness may prompt someone who is concerned about themselves or someone they know to seek help. Media stories sourced to the courts rarely have information about where to seek help or where to access further information for people who may be directly or indirectly affected by mental illness.
n Where possible provide media professionals with helpline numbers and suggest that the information is included in the report.
It is important to provide support information relevant to the audience of each story. For most reports it will be appropriate to cite a national helpline such as the one provided
by SANE Australia on 1800 18 SANE (7263). However, you may also want to consider contact details for particular population groups provided on page 53.

12
In interviews or any other interactions, check that your language is appropriate and that it does not stigmatise mental illness.
n The language used when reporting on mental illness can contribute to stereotypes, myths
and stigma. Journalists may be unlikely to edit ‘direct quotes’ from interviews, press
releases or transcripts.
n It is important that the language used is consistent with suggestions provided to media
professionals. Remember that your comments potentially reach many members of
the community.
• Avoid negative language, e.g. ‘mental patient’, lunatic’, ‘schizo’, ‘psycho’ etc.
• Avoid labelling a person by their mental illness – e.g. a person is not ‘a schizophrenic’,
they are ‘currently experiencing’, ‘being treated for’ or ‘have a diagnosis of
schizophrenia’.
• Be careful not to imply that all mental illnesses are the same and ensure that correct
terminology is used when a diagnosis is referred to.
• Do not use diagnostic terms unless the diagnosis has been confirmed by a
medical professional.
• Be aware of the language you use when referring to someone leaving hospital – e.g. a
person is ‘discharged’ from hospital not ‘released’ and they ‘leave’ or ‘go missing’,’ they
don’t ‘escape’.
Victim impact statements are very powerful and often used by journalists to add emotion and human interest to a story. These statements may include comments about
the mental health of either the accused or the victim themselves.
These statements may provide an opportunity to highlight the impact of traumatic events on someone’s mental health, where the victim details how the event has
affected them and their family. These statements, however, may also perpetuate fear and misunderstanding about mental illness, especially where an offender is described
using derogatory language that implies the existence of a mental illness.

13
Be mindful not to reinforce common myths and stereotypes about mental illness.
n The type of information presented in court, and subsequent media reports, may reinforce
stereotypes such as those that link mental illness with violence or suggest people with
mental illness are unable to work, parent or lead fulfilling lives.
n Consider whether it is appropriate to provide some context surrounding an incident.
For example, where violence occurs it is often in the context of drug use, distressing
hallucinations or treatment that has been ceased or ineffective.
Some stories gain additional prominence and national attention because of a seemingly extraordinary frame, usually taken from court testimony or comments from a judge.
A mentally ill man who believed he was an alien due to be picked up by a spaceship killed his father and his faithful dog by repeatedly stabbing them, a judge said yesterday.
(Kalgoorlie Miner, 29 June 2000)
Refer journalists to Mindframe.
n Are the journalists covering the courts or conducting an interview aware of the Mindframe
guidelines for reporting mental illness available from www.mindframe-media.info?
n Is there an opportunity to recommend that journalists access the site for appropriate helpline
numbers that they can add and contact details for mental health organisations that may be
able to assist with the story?
n It is recommended that the Mindframe website be added to the bottom of all correspondence
with media professionals that may involve mental illness.
n You may want to designate at least one person who can discuss ‘ways of reporting mental
illness’ with media professionals who approach your jurisdiction and ensure they are
aware of the Mindframe resources for media professionals. This may be a public affairs
unit or an identified media liaison representative.

14
Reporting Suicide and Mental Illness: A Mindframe resource for media professionals makes
a number of suggestions for editors and journalists to consider when reporting mental illness.
These ‘issues to consider’ are informed by research evidence related to the impact of media
portrayal of mental illness, and are summarised below.
n Consider whether the person’s mental illness is relevant to the story and whether it needs to
be included. In particular, whether it needs to be referred to in the headline or lead.
n Ensure any references made to mental illness are accurate and in context.
n Be mindful of language used in relation to mental illness:
• Avoid negative language such as ‘psycho’, ‘schizo’, ‘mental patient’ or ‘lunatic asylum’.
• Avoid referring to someone as ‘a victim’, ‘suffering from’ or ‘afflicted’ with mental illness.
• Avoid language that labels a person or suggests mental illness is a life sentence.
• Ensure that medical terminology is not used out of context, e.g. ‘schizophrenic policy’.
n Be mindful of stereotypes such as those that link mental illness with violence or suggest
people who have mental illness are unable to work, parent or lead fulfilling lives.
n Be careful not to imply that all mental illnesses are the same. The term mental illness covers
a wide range of symptoms, conditions and effects.
n Ensure that informed consent has been gained before interviewing people affected by
mental illness.
n Include helpline numbers and information about options for those seeking help.
n Seek advice from recommended health experts.
A complete outline of ‘issues to consider’ for media professionals can be accessed from the
Mindframe website at www.mindframe-media.info
Mind f rame Cons iderat ions for Media Profes s iona l s

15
The media has an important role to play in influencing social attitudes to suicide and potentially the actions of vulnerable people. Australian and international research shows that reporting of suicide can have an impact on vulnerable people25.
People in despair may be influenced by media reports of suicide, particularly where they identify with the person in the report, or where suicide is romanticised, glamorised or otherwise portrayed as an ‘acceptable’ course of action.
I think it’s how you [report suicide], because I think that the offset against things like copycats is the information that you give [people] so that they
are better informed 26.
Media codes of practice state that, in general, suicides will not be reported. However, there will be times when a death will be reported if it is considered to be ‘in the public interest’. This might include the death of a prominent person, a death in a public place, or a death that is in some way related to other political or social issues, such as a death in custody. While media generally take a responsible approach to reporting suicide, examples of inappropriate reporting can still be seen.
A significant number of news items about suicide result from information gathered at coroners’ inquests and other courts27. Often, specific details of method or location of death are included in the proceedings of an inquest, and can then find their way into media reports.
Coroners, magistrates, court administrators and media liaison officers need to have an understanding of the potential impact of reporting suicide in certain ways. This may inform the way in which they relate to journalists in both formal (e.g. media statements) and informal (e.g. court proceedings) ways.
What follows in this section is: a summary of research evidence regarding the impact of media reporting; issues to consider for judicial officers about indirect communication with the media; issues to consider for other officers of the court about direct communication with the media; and an outline of the issues media professionals are asked to consider when reporting suicide.
Media Reporting of Suicide

16
Research has demonstrated that while increased rates of actual suicide have been associated with some reporting, examples of decreased rates of actual suicide following reports have also been found. A summary of findings from a critical review of the national and international literature28 is provided below.
A number of characteristics have been associated with increased rates of suicide.
Reporting of celebrity suicide.
n A series of American studies found increased rates of suicide in months in which front page newspaper articles of celebrity suicide appeared29, 30.
n A Canadian study found an increase in suicide rates in the month following the reported death of a prominent person in Quebec.31
High profile reporting of suicide.
n A number of studies have found increased rates of suicide in the months that front-page reports of non-celebrity suicides appeared32, 33, 34.
Description of method and location.
n Higher rates of suicide by a particular method have been found to follow the appearance of newspaper stories on a suicide by these methods 35, 36, 37, 38.
n An Austrian study conducted after the suicide death of a celebrity found a correlation in suicide method in those areas with high newspaper distribution post suicide39.
Where vulnerable people identify with the person who is the subject of the story.
n A US study found an increase in the rate of death by suicide among older people following reporting of suicide in this population group40 .
n An Australian study found an increase in the number of males who died by suicide following newspaper reports of suicides with the peak being three days after reporting 41.
n A US study found that suicide stories to which a local audience has the greatest exposure are likely to produce contagion and that, in particular, local television news is a potent influence 42.
Ev idence o f Impact : Media Repor t ing o f Su ic ide

17
Prolonged or repetitive reporting of a suicide.
n An Australian study found evidence for a ‘dose response effect’, where the greater the
coverage of a particular suicide the greater the risk of an increase in subsequent suicides43.
Courts are important sources of information for media stories about suicide
Many newspaper and broadcast news stories about suicide result from information
collected by journalists at courts or coroner’s courts or from the police 44. These stories
are the most problematic in terms of following media guidelines for reporting of suicide,
due to the use and placement of the word ‘suicide’ in headlines and broadcast leads,
details of the method of suicide, and the prominence given to the story.
Other characteristics of reporting have been associated with decreased rates of suicide.
Portrayal that positions suicide as a tragic waste and an avoidable loss and focuses on the devastating effects on others.
n An Australian study of reporting following Kurt Cobain’s suicide found rates among young
Australians aged 15-24 were significantly lower in the month following the reporting of his
death than for corresponding months in previous years. Significantly, the media were highly
critical of Cobain’s decision to end his life 45.
n A US study showed rates of completed and attempted suicide by young people fell following
the broadcast of telemovies showing the impact of suicide46.
Reporting that does not describe method or location of death.
n Austrian studies found that the number of completed and attempted suicides in the Vienna
subway dropped after the introduction of media guidelines led to less frequent reporting of
suicides by that method and in that location 47, 48, 49.
A more comprehensive summary of the research evidence is available from
www.mindframe-media.info

18
Courts are a valuable source of information for the media about incidents of suicide that they may deem to be ‘newsworthy’. Through court proceedings and inquests journalists are privy to details about the circumstances surrounding a death. As such, courts may be called upon by the media to make comment about particular cases or issues from time to time. While coroners and other court officials may not talk directly to the media or seek out media coverage, their general dealings with journalists in the courtroom may have an impact on the way a story is developed.
This section is broken into two parts:
n PART 1 summarises some key issues to consider for judicial officers to guide their indirect contact with the media around suicide.
n PART 2 summarises some key issues to consider for other officers of the court to guide their direct interactions with the media around suicide.
These issues to consider support the guidelines provided to Australian journalists about the
reporting of suicide (see page 24).
Key I s sues to Cons ider
Issues to Consider: Judicial Officersn Consider the potential impact of the story and whether to make official comment. n Avoid specific description of the method and location of suicide and consider how
to manage this information in the courtroom.n Check your language does not glamorise or normalise suicide.
Issues to Consider: Other Officers of the Courtsn Consider the potential impact of the story and whether to make official comment. n Avoid specific description of the method and location of suicide.n Consider how to include information that may improve community understanding.n Check your language does not glamorise or normalise suicide.n Include information that promotes help-seeking behaviour.n Refer journalists to Mindframe.
19
Par t 1 : For Jud ic i a l Of f i cer s
Consider the potential impact of the story and whether to make official media comment.
n Consider if you are able to provide comment or advice to media professionals. Do you need advice or support from your media liaison unit?
n Think about whether the story is likely to have benefits for the community. That is, does it provide an opportunity to increase community understanding, highlight groups at risk or promote help-seeking behaviour in some way? If this is the case, consider in what ways you may be able to have input.
n If the story is generally about suicide or suicide prevention, you may want to refer the journalist to the ‘expert comment’ section of the Mindframe website.
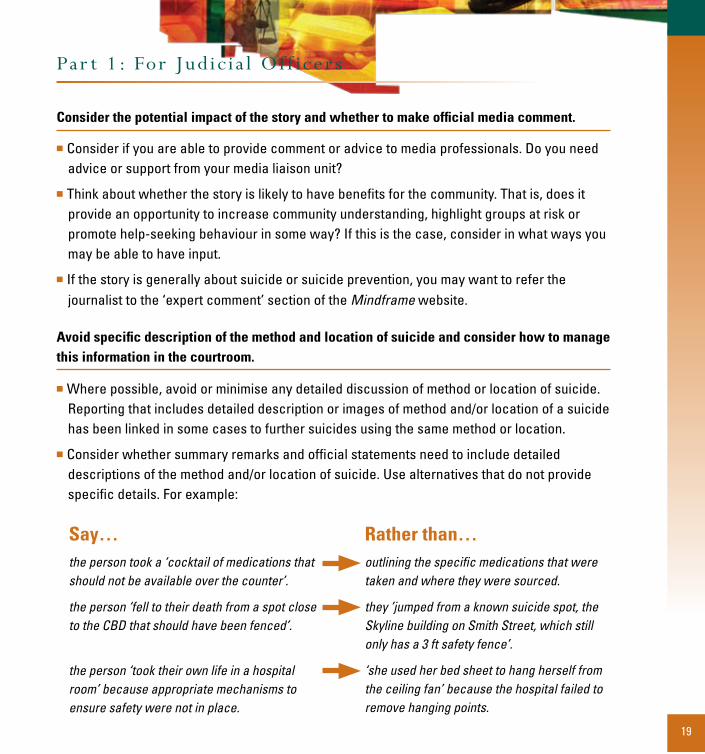
Avoid specific description of the method and location of suicide and consider how to manage this information in the courtroom.
n Where possible, avoid or minimise any detailed discussion of method or location of suicide. Reporting that includes detailed description or images of method and/or location of a suicide has been linked in some cases to further suicides using the same method or location.
n Consider whether summary remarks and official statements need to include detailed descriptions of the method and/or location of suicide. Use alternatives that do not provide specific details. For example:
Say…the person took a ‘cocktail of medications that should not be available over the counter’.
the person ‘fell to their death from a spot close to the CBD that should have been fenced’.
the person ‘took their own life in a hospital room’ because appropriate mechanisms to ensure safety were not in place.
Rather than…outlining the specific medications that were taken and where they were sourced.
they ’jumped from a known suicide spot, the Skyline building on Smith Street, which still only has a 3 ft safety fence’.
‘she used her bed sheet to hang herself from the ceiling fan’ because the hospital failed to remove hanging points.

20
n Consider how to manage details of the method or location that are raised as part of the
proceedings. Is there an opportunity to remind journalists about their codes of practice that
discourage any detailed description of method or location of a suicide death?
n When making recommendations about duty of care that may involve suicide methods,
or highlighting the need for preventative measures at ‘suicide spots’, consider whether
providing details may do more harm than good. For example, media stories highlighting the
need for further fencing at a particular location may in fact increase rates of suicide from
that location.
n Be mindful that for many Aboriginal and Torres Strait Islander communities there are cultural
protocols around naming and showing pictures or video of a person who has passed away.
Consider how to manage this information in the courtroom.
Check your language does not glamorise suicide or present it as normal or an option for dealing with problems.
n Have you considered the impact of verbal and written language you use about suicide? The
language used in media reports can contribute to suicide being presented as glamorous,
normal or as an option for dealing with problems.
n Consider how you might manage inappropriate language raised in the courtroom. Always
use appropriate language when talking about suicide from the bench. For example:
Use…‘non fatal’ or ‘attempt on his/her life’
‘took their own life’ or ‘died by suicide’
statements such as ‘increasing rates’ or ‘cluster of deaths’
n Avoid simplistic explanations that suggest suicide might be the result of a single factor or
event. This may be difficult when discussing a specific case, but ensure comments do not
generalise one case to all cases.
Rather than…‘unsuccessful suicide’
‘successful suicide’ or ‘committed suicide’
‘suicide epidemic’ which is sensationalist and inaccurate

21
Par t 2 : For Other Of f i cer s o f the Cour t
Consider the potential impact of the story and whether to make official media comment.
n Find out what the journalist needs. Is the issue about an inquest or case or more generally about suicide or suicide prevention? Consider if you are the most appropriate person to be commenting on the issue under question.
n Avoid engaging in repetitive, prominent or excessive reporting of suicide, which may normalise suicide. This has been linked to increased rates of actual suicide. This does not, however, mean that all suicide reports should be avoided.
n Think about whether the story is likely to have benefits for the community. That is, does it provide an opportunity to increase community understanding, highlight groups at risk or promote help-seeking behaviour in some way? If this is the case, consider in what ways you may be able to have input.
n While you always have the option of saying ‘no’ you may want to consider the impact of not participating in a story. That is, the story may still be run without expert comment and advice.
n If the story is generally about suicide or suicide prevention, you may want to refer the journalist to the ‘expert comment’ section of the Mindframe website at www.mindframe-media.info
n You may want to designate at least one person who can discuss ‘ways of reporting suicide’ with media professionals who approach your jurisdiction and ensure they are aware of the Mindframe resources for media professionals. This may be a public affairs unit or an identified media liaison representative.
When deciding whether to participate in a story you may want to consider what type of media is making the approach and whether you are best placed to provide them with information. Do they require general information or information related to a specific
case before the courts or coroner?

22
Avoid specific description of the method and location of suicide and instruct media to be cautious with this information.
n Details regarding the method and location of a suicide may be an important part of a coronial inquest, and included in documents and statements relating to the proceedings. Take any opportunity to remind journalists about their codes of practice that discourage any detailed description of method or location of a suicide death.
n Consider alternative suggestions for ways to talk about the method and location that do not provide specific details (see page 19 for some examples).
n For suicide deaths involving an Aboriginal or Torres Strait Islander person, be mindful of releasing their name or details to the media. Where the information is made public, request that media professionals respect appropriate cultural protocols.
Consider how to include information that will improve community understanding.
n Placing stories about suicide in the context of risk factors can assist in breaking down myths about suicide, and promote a better understanding of it as a wider community issue. This may be done directly through your work with the media, or in partnership with mental health and suicide prevention experts.
n Avoid simplistic explanations that suggest suicide might be the result of a single factor or event. This may be difficult when discussing a specific case, but ensure comments do not generalise one case to all cases.
n Provide suicide prevention information such as risk factors and warning signs and encourage its inclusion in the story (see pages 41-43).
n Provide information in simple terms and without jargon.
Consider the impact of a media story on people bereaved by suicide. If the media wish to interview those who have been bereaved by suicide, be aware
that these people may be quite vulnerable. People bereaved by suicide may be at risk of experiencing mental health problems and possibly taking their own lives. They may
be particularly vulnerable in the first year following the death and on anniversaries after that time. Sometimes, the media may seek to access the bereaved at court or inquest locations. In these cases, they may need particular support from grief
counselling services to deal with the distress of these interviews.

23
Include information that promotes help-seeking behaviour.
n Vulnerable people may be distressed by reports of suicide and in some cases may be prompted to harm themselves. As such, it is important that helpline numbers are included with all reports about suicide.
n Where possible provide media professionals with helpline numbers and information and suggest that the information is included in the report. Some numbers and services are provided on page 53. Alternatively refer the journalist to the Mindframe website.
n Preparing a list of contacts that you or your jurisdiction could use in stories will assist when deciding which details to give to media professionals. This may be particularly useful when information is required within a short deadline.
Refer journalists to Mindframe.
n Are journalists covering the inquest or conducting an interview aware of the Mindframe guidelines for reporting suicide available from www.mindframe-media.info?
n Is there an opportunity to recommend they access the site for appropriate helpline numbers they can add and contact details for mental health and suicide prevention organisations that may be able to assist with the story?
n It is recommended that the Mindframe website be added to the bottom of all correspondence with media professionals that may involve suicide.
For most reports, a helpline such as Lifeline on 13 11 14 will be appropriate. It is important, however, to provide support information relevant to the audience for each story.
n Aboriginal and Torres Strait Islander people may prefer to see a health worker at their local Aboriginal Medical Service. See the VIBE website at www.vibe.com.au
n For Australians from culturally and linguistically diverse backgrounds it would be useful to include contact details for the relevant state transcultural mental health services as well as the national Telephone Interpreter Service (13 14 50). Information is available from Multicultural Mental Health Australia on 02 9840 3333 or www.mmha.org.au
n For young Australians it would be more useful to provide the Kids Helpline on 1800 55 1800, or websites such as www.reachout.com.au
24
Reporting Suicide and Mental Illness: A Mindframe resource for media professionals makes a number of suggestions for editors and journalists to consider when reporting suicide. These are based on research evidence into the impact of media portrayal of suicide, are consistent with industry codes of practice and are summarised below.
n Consider whether the story needs to be run and how many stories relating to suicide there have been in the last month, so as to avoid a succession of stories or a high volume.
n Refrain from using language that may glamorise or sensationalise suicide.
• Avoid using the word suicide in a headline or lead, using phrases such as ‘took their own life’ as an alternative.
• Refrain from using terms such as ‘unsuccessful suicide’, ‘successful suicide’ or ‘committed suicide’.
• Avoid sensational statements like ‘suicide epidemic’. Statements such as ‘increasing rates’ or a ‘cluster of suicides’ are more accurate.
n Avoid detailed descriptions or visuals of the method and location of a suicide, and make comment on the wastefulness of the act.
n Take extra care when reporting celebrity suicide. This coverage has the potential to glamorise and normalise suicide and may prompt copycat behaviour.
n To reduce prominence, locate stories about suicide in the inside pages of a paper and further down the order of reports in TV or radio news.
n Follow media codes of practice around privacy, grief and trauma when reporting personal tragedy.
n Seek advice from recommended health experts and place the story in context by providing information about underlying causes and risk factors.
n Include helpline numbers and information about options for those seeking help.
A complete outline of ‘issues to consider’ for media professionals can be accessed from the Mindframe website at www.mindframe-media.info
Mind f rame Cons iderat ions for Media Profes s iona l s

25
This section includes some facts and statistics about mental illness as well as short
descriptions of the more common illnesses. Comprehensive facts and statistics are available
from the Mindframe website at www.mindframe-media.info
Clinical Definitions
Mental health is a positive term referring to a state of emotional and social wellbeing in which
the individual realises his or her own abilities, can cope with the normal stresses of life, can
work productively or fruitfully, and is able to make a contribution to his or her community 50.
A mental illness (or mental disorder) is a diagnosable illness that significantly interferes
with an individual’s cognitive, emotional or social abilities. There are different types of mental
illnesses and each of these will occur with a different degree of severity.
A mental health problem also interferes with a person’s cognitive, emotional or social abilities,
but may not meet the criteria of an illness. Mental health problems often occur as a result
of life stressors, and are usually less severe and of shorter duration than mental disorders,
although they may develop into mental disorders.
Legal Definitions
Mental illness – The legal definition of mental illness is more restricted. Mental Health Acts
across Australia consider that a person’s clinical diagnosis of mental illness can result in
involuntary treatment if, owing to their illness, there are reasonable grounds for believing that
care, treatment or control of the person is necessary, for their own protection from serious
harm, or for the protection of others from serious harm.
Mentally disordered – A person may be mentally disordered, even in the absence of a
diagnosed mental illness, if their behaviour for the time being is so irrational as to justify a
conclusion on reasonable grounds that temporary care, treatment or control of the person is
necessary for their own, or others’ protection.
About Mental Illness

26
Depression
Mood disorders are those where a person’s mood is distorted or inappropriate to their circumstances. The most commonly experienced mood disorder is depression. Clinical depression is more than just temporary unhappiness or feeling down. It is an illness that may be felt as a sadness that does not go away and/or an ongoing loss of pleasure and enjoyment in most activities.
Major depression will be experienced by one in five adults at some point in their lives and accounts for more days lost to illness than almost any other disorder, physical or mental51. Up to two fifths of Australia’s young people experience depressed moods in any six-month period.
Some of the symptoms that often occur with major depression include: sleep disturbance, loss of energy and concentration, feelings of worthlessness, hopelessness and guilt, inability to cope with decisions, weight loss or gain, and thoughts of death.
Sometimes depression develops after a major event, such as a loss of a loved one or a separation. Depression may also occur after repeated stress or ongoing abuse. However, it can also occur without apparent cause and in people who have coped well with life previously. Sometimes depression will lift after only a few weeks. In other cases, the depression will continue for months or years, perhaps requiring hospitalisation, and affecting the person’s life and relationships.
There are a number of treatments for depression, including professional counselling, psychotherapy and antidepressant medication. The vast majority of people experiencing a major depression will recover fully, sometimes without treatment. However, effective treatment can greatly assist people to recover much faster and can lessen the pain and the
cost that may be associated with the illness.
Bipolar disorder
Bipolar disorder, previously known as manic depression, is characterised by recurrent episodes of extreme mood variation from major depression to very elevated mood (mania). The extent of mood range varies between people. Some experience both mania and depressed
Spec i f i c Menta l I l lnes ses

27
mood, others only the ‘highs’ without depression. Episodes of both depression and mania can range from mild to severe. A person may also experience symptoms of psychosis (see page 29).
The symptoms of mania include: feeling very high and happy, increased energy and reduced need for sleep, rapid speech and thought, reduced inhibitions, grandiose plans and beliefs, and a lack of insight that these behaviours or beliefs are unusual.
These symptoms can be damaging to people’s lives and relationships. People with bipolar disorder can have to contend with large debt, broken relationships and damaged reputations as a result of out-of-character behaviour during a manic episode.
Bipolar disorder is likely to be caused by several factors, including biochemistry, genetic inheritance, stress and sometimes seasonal effects 52. Between episodes of low or high mood, people experience normal mood variation and are able to live full and productive lives. For some people, extreme mood swings occur regularly. For others, the highs or lows may be occasional with years of stable moods between.
Treatment for bipolar illness includes medication, psychological therapies and lifestyle changes.
Anxiety Disorders
Anxiety is a persistent sense of stress, fear or worry in the absence of a rational reason for these feelings. A person is said to be experiencing an anxiety disorder when they have an intense and paralysing sense of fear or a more sustained pattern of worrying, to the extent that it interferes with their everyday life. Some people experience physical sensations of fear, such as shortness of breath, a tight chest, racing heart or even dizziness. Approximately 20% of people will develop an anxiety disorder at some point in their lives53. This can occur at almost
any age.
Many factors influence the development of an anxiety disorder, including genetic makeup, life experiences, developmental stage, family history, and factors such as stress and physical health. In some cases anxiety may be the result of a highly traumatic experience, such as torture or abuse. Many people with anxiety disorders also experience depression.
There are several different types of anxiety disorders. These share common symptoms, although the contexts in which the symptoms are experienced vary. The more common forms of anxiety disorders include: generalised anxiety disorder, panic disorder, phobic disorders, post-traumatic stress disorder and obsessive-compulsive disorder.

28
Anxiety symptoms can be treated using Cognitive Behavioural Therapy (CBT) or other psychological therapies. CBT works by focussing on changing the way a person thinks in order to modify how they respond to anxiety-provoking situations. Medication, such as anti-
depressants, can also be useful for people experiencing severe anxiety.
Psychotic Disorders
Several mental illnesses are grouped under the term Psychotic disorders, which are
characterised by some form of psychosis. Psychosis involves a loss of contact with, or
distortion of, reality, which may include hallucinations or delusions, disorganisation of thought
and lack of insight. These symptoms may cause difficulties in social situations and inability to
cope with day-to-day living requirements.
Examples of psychotic disorders include: Schizophrenia, Schizoaffective disorder,
Schizophreniform disorder, Brief psychotic disorder, Delusional disorder, Shared psychotic
disorder, Substance induced psychosis, and Psychosis due to a general medical condition.
The most common psychotic disorder is Schizophrenia. It is a serious mental illness which
affects almost one person in 10054. The term covers several related disorders, all with
overlapping symptoms. Each individual can have a unique combination of signs and symptoms
and, therefore, a unique experience of the disorder.
The first onset of schizophrenia is typically in adolescence or early adulthood for males and
a little later in females55. The onset may be rapid, developing over several weeks, or it may
be slow, over months or years. Some people experience only one or more brief episodes and
recover fully. Others may have to deal with the illness throughout their lives.
The symptoms of schizophrenia are grouped into two categories56. The term positive symptoms
refers to an excess or distortion of everyday thought processes or perception (the process of
acquiring, interpreting, selecting, and organising information gathered from the five senses).
Negative symptoms refers to the onset of a loss or absence of everyday abilities.
Mental health clinicians use the umbrella term psychosis to describe the mental state of a
person experiencing acute symptoms of schizophrenia. A psychotic episode is a term that
describes a period of time whereby the positive or psychotic symptoms are highly active.

29
The positive symptoms of a psychotic episode include:
• Thought disorder – Thought disorder is a term that describes a persistent underlying disturbance of conscious thought and is classified largely by its effects on speech and writing57. Affected persons may: speak incessantly, invent words, use speech that reflects ideas switching from one train of thought to another or respond to questions with ‘longwinded’, unfocused or irrelevant answers.
• Delusions – A delusion is a fixed, false personal belief held with absolute conviction despite all evidence to the contrary. The belief is often pathological in nature, is outside the person’s normal cultural practices and dominates their thoughts and behaviours58. Delusions are categorised according to their content. For example, delusions of persecution where there is a belief that another person or force is in some way interfering with the individual’s life.
• Hallucinations – Hallucinations are false perceptions in the absence of a real external stimulus, affecting any of the five senses. The most common are auditory hallucinations which take the form of voices 59. This occurs in 60–70% of people diagnosed with schizophrenia. Voices usually occur in the third person and provide a running commentary, arguing with the person or repeating the person’s thoughts. Visual hallucinations occur in about 10% of people with schizophrenia, but are more indicative of an organic disorder.
Psychosis usually occurs in three stages:
1. The Prodromal Phase. A period of early symptoms and signs of schizophrenia that precede an acute fully developed psychotic episode. During this period (varying from weeks to years) a person experiences changes in their thoughts, feelings, behaviours and perception.
2. The Acute Phase. A period when positive symptoms of schizophrenia emerge. Most people come to the attention of mental health services and begin treatment at this stage.
3. The Recovery Phase. A period (6-8 months following acute treatment) when positive symptoms of the acute phase begin to dissipate, and negative symptoms become more prominent.
No cure is known for schizophrenia, but great advances have been made in early management and long term control of the illness. Early detection of the initial symptoms (early psychosis) and their management with medication, psychotherapy, social support and family programs can help to return the person to optimal functioning.

30
Personality Disorders
Personality Disorders are diagnostic categories used to describe specific types of personality
problems. Clinicians use this term to describe patterns of thinking and behaviour that are
extreme, inflexible and maladaptive60. Personality disorders may cause major disruption to a
person’s life and are usually associated with significant distress to the self or others. A person
with a personality disorder has longstanding and persistent difficulties resulting from the way
they feel about and view themselves, others and the world in general61. They often experience
themselves as unworthy or different, experience others as uncaring or even hostile and may
view the world as a dangerous place devoid of any real meaning or sense of purpose62.
As a result of these ways of viewing themselves and the world, relationships – whether
intimate or in work or social settings – are often fraught with difficulty. These difficulties
are often so great that education, work and day-to-day living are disrupted to the point that
significant social disadvantage may occur.
People with personality disorders experience an inner fragility and lack the resilience to cope
with many of life’s difficulties. Not only can stressful or adverse life events have a devastating
impact on their wellbeing, but so too can the responses of others towards them.
Responses or actions of others which seem to confirm their sense of unworthiness or their
expectation that others will treat them badly, for example, may lead to emotional responses
of depression, anxiety, or even rage. These painful emotional experiences frequently lead
to self-harm or suicide attempts. Substance abuse, compulsive behaviour or idiosyncratic
preoccupations are other ways that people with personality disorders attempt to deal with
their internal distress.
Treatment of personality disorders has generally been viewed as more difficult compared to
other disorders. There is now, however, strong evidence for the benefit of certain types of
therapies63. These are generally long-term and involve the development of a relationship with
a therapist in which difficulties and their origins can be explored and understood, or in which
new strategies, coping skills and alternative behaviours can be learnt.

31
In 1997 the Australian Bureau of Statistics (ABS) conducted the National Survey of Mental Health and Wellbeing 64. Findings of the adult survey are summarised below.
n Almost one in five Australians (17.7%) had experienced a mental illness at some time during the 12 months before the survey.
n Men and women experienced similar rates of mental illness. The incidence of mental illness was higher for men and women living alone than those living with other people. Similarly, rates of mental illness were higher among people who were separated or divorced (24% for men and 27% for women).
n Women were more likely than men to experience anxiety disorders (12% compared with 7.1%) and mood disorders (7.4% compared with 4.2%). Men were more than twice as likely as women to have substance abuse disorders (11% compared with 4.5%).
n People unemployed or not in the paid workforce had the highest rates of mental illness, a prevalence rate of 26.9% for unemployed men and 26% for unemployed women, compared with prevalence rates of 15.1% for men and 14.7% for women in full-time paid employment.
n Anxiety disorders were most common, and affected one in ten adults, followed by mood disorders 5.8% (of which depression is 5.1%), and substance use disorders – 7.7% (of which 6.5% is alcohol related).
n Women were more likely than men to use services for mental health problems.
Mental Illness and the Law
Research has found that, due to a range of reasons, people living with a mental illness may have particular barriers preventing them from participating in the legal system65. These barriers can be problematic for people appearing as witnesses or victims of a crime, as well as for those who may be accused.
The research indicated that people experiencing a mental illness often face difficulties in their day-to-day life. They are more likely to receive a low income, leading to problems with housing and homelessness. Additionally, the symptoms of some types of mental illnesses may manifest
Menta l I l lnes s in Austra l i a

32
as unusual behaviour, which may bring people displaying such symptoms to the attention of police. In extreme cases, such behaviour might result in charges such as offensive language and conduct, resisting arrest and assaulting police. This type of behaviour may be especially common in those with a coexisting substance abuse problem.
The particular barriers faced by people living with a mental illness are many and varied. Some of the key issues highlighted by research include:
n People with a mental illness may find the legal process particularly stressful, especially courtroom situations. They may already experience significant stress in their lives, arising from family, financial and housing problems and may find the extra stress involved in the legal process overwhelming.
n Some mental illnesses are characterised by cognitive impairment, including memory loss and problems with planning and concentrating. This can lead to problems with keeping appointments and understanding legal proceedings and documents.
n People with a mental illness are often viewed as less credible by those in the legal sector. They may also be viewed as less credible by police when making statements relating to being the victims of crime, which may be taken less seriously as a result.
Disability caused by mental illness
Mental illness can be more disabling for some people than many chronic physical illnesses. ‘Disability’ refers to the degree to which an illness interferes with a person’s ability to work, take care of themselves or carry on relationships. International research66 looked at the amount of disability caused by a number of physical and mental health problems. From that research, some illustrative examples can be made:n The disability caused by moderate depression is similar to the disability from
relapsing multiple sclerosis, severe asthma, chronic hepatitis B or deafness;n The disability from severe post-traumatic stress disorder is comparable to the
disability from paraplegia;n The disability from severe schizophrenia is comparable to the disability from
quadriplegia.
In the Australian context, mental illnesses rank as the third biggest health concern after heart disease and cancer.

33
Myth: People who are mentally ill are violent.
n Research indicates that people receiving treatment for a mental illness are no more violent
or dangerous than the general population67.
n People living with a mental illness are more likely to be victims of violence, especially
self-harm. It has been calculated that the lifetime risk of someone with an illness such as
schizophrenia seriously harming or killing another person is just .005%, while the risk of that
person killing themselves is nearly 10%68.
n There appears to be a weak statistical association between mental illness and violence
in certain subgroups, for example – people not receiving treatment who have a history of
violence, and those who abuse drugs or alcohol.
n The correlation between episodes of violence in people experiencing mental illness is
comparatively weaker than violent behaviour in the context of alcohol abuse and violent
behaviour in young males between the ages of 15 and 2569.
Myth: Mental illness is a life sentence.
n Depending on the age of onset and the severity of the mental illness, generally speaking,
most people will experience complete recovery, especially if they receive help early.
Some people may require ongoing treatment to manage their illness.
n Some people have only one episode of mental illness and recover fully. For others, episodes
of mental illness occur occasionally with years of wellness between episodes. For a minority
of those with a more severe illness, periods of acute illness will occur regularly and, without
medication and effective management, leave little room for recovery.
n Though some people experience significant disability as a result of a mental illness, many go
on to live full and productive lives while receiving ongoing treatment.
Common Myths about Menta l I l lnes s

34
Myth: Mental illnesses are all the same.
n There are many types of mental illnesses and many kinds of symptoms or effects.
n Though a particular mental illness will tend to show a certain range of symptoms, not
everyone will experience the same symptoms – for example many people with schizophrenia
may hear voices, while others may not.
n Simply knowing a person has a mental illness will not tell you how well or ill they are,
what symptoms they are experiencing, or whether they may recover or manage the
illness effectively.
n Mental illnesses are not purely ‘psychological’ and can have many physical features. While
a mental illness may affect a person’s thinking and emotions, it can also have strong physical
effects such as insomnia, speech impediment, weight gain or loss, increase or loss of
energy, chest pain and nausea.
Myth: Some cultural groups are more likely than others to experience mental illness.
n Anyone can develop a mental illness and no one is immune to mental health problems.
n People born in Australia have slightly higher rates of mental illness than those born outside
Australia in either English-speaking or non English-speaking countries.
n Many people from culturally and linguistically diverse and refugee backgrounds have
experienced torture, trauma and enormous loss before coming to Australia. These
experiences can cause significant psychological distress and vulnerability to mental illness.
n Cultural background affects how people experience mental illness and how they understand
and interpret the symptoms of mental illness.

35
Suicide is a prominent health concern in Australia. A suicide death can have devastating
impacts on family, friends, colleagues, and potentially the whole community.
This section contains information about suicide, suicide risk and a brief overview of Australian
facts and statistics. Comprehensive facts and statistics can be found on the Mindframe
website at www.mindframe-media.info
For more information about suicide prevention in Australia, download the Living Is For
Everyone (LIFE) Framework at the LIFE website www.livingisforeveryone.com.au
About Suicide
Definition of Terms
Terms that are commonly used when discussing suicide include:
Suicide death – a death is classified as a suicide when a coroner determines that it has occurred as a result of self-inflicted harm where the intention was to die.
Attempted suicide – self-inflicted harm where death does not occur but the intention of the person was to die. There are three types of attempted suicide: without injury, with injury, and with a fatal outcome (suicide).
Self-harm – any behaviour that involves deliberate injury to oneself. Self-harm may be an attempt at suicide although it is not necessarily so. It is usually a response to distress.
Suicidal behaviour – acts such as suicide and attempted suicide. This also includes suicide related communications such as verbal or nonverbal statements expressing suicidal intent.
Suicidal ideation/thoughts – thoughts about, or plans for, taking one’s own life that may or may not lead to a suicide attempt.
Suicide intent - implies a conscious desire or wish to die or escape from life. Suicide intent does not necessarily denote that an individual has undertaken an analysis or has knowledge of the medical lethality of different methods or means.

36
Despite some concerns about its accuracy, the main source of Australian data on suicides is
the Australian Bureau of Statistics (ABS). They release new data on an annual basis. Unless
otherwise stated, the statistics provided in this document are from ABS publications70.
How many people die by suicide in Australia?
n Suicide is a prominent public health concern in Australia. For the past decade, more than
2000 people have taken their life each year (with numbers dropping below 2000 in 2006 with
1799 deaths recorded). These figures may be an underestimation.
n For the past decade suicide represented 1-2% of all deaths registered in Australia.
n Although suicide attempts are more common in women than men, generally men take their
own lives at a rate four times that of women.
Is the problem getting worse?
n Suicide rates for both males and females have generally decreased since the mid-90s, with
the overall suicide rate decreasing by 34% between 1997 and 2006.
n Despite the common belief that there is a “youth suicide epidemic”, suicide rates among
young males have fallen considerably over recent years (by about 50% since 1997), and
suicide in children under the age of 15 is a rare event in Australia.
n Despite these decreases, suicide remains a major external cause of death, accounting for
more deaths than transport accidents between 1995 and 2006.
n Although accurate suicide statistics are difficult to obtain for Aboriginal and Torres Strait
Islander people, figures reveal that the percentage of all deaths attributable to suicide is
generally much higher for these populations and may be increasing.
An Over v iew of Su ic ide in Austra l i a

37
Do rates vary between states and territories?
n Combining suicide data over a 5-year period provides a more reliable picture of differences
across the states and territories due to the relatively small number of suicides in some states
and territories in any one year.
n In recent years (2002-2006) Tasmania and the Northern Territory had the highest rate of
suicide, followed by South Australia. In contrast, New South Wales and Victoria had the
lowest rates of suicide and the ACT and Queensland had fluctuating rates.
Are the rates different for males and females?
n Suicide rates for males are higher than those for females and have been higher since at
least the 1920s. More women than men, however, attempt suicide71.
n The ratio of male to female suicides rose from 2:1 in the 1960s to over 4:1 in the mid 1990s.
In recent years, the suicide rate for males has reduced slightly to almost 4 times that of
females, and is consistent across most age groups.
n Between 1997 and 2006, the suicide rate fell by 34%, with this rate of change similar for
males (35%) and females (31%).
Do rates vary across age groups?
n From 1990 until 1997, 20 to 24 year old men were consistently the most likely of all age groups
to die by suicide, with rates reaching 42.8 per 100,000 in 1997. However, between 1998 and
2005 the highest rates have been observed for males aged in the 25-45 year age groups.
In 2006 the highest rate was observed in men aged over 85 (although the rates are inflated
by the small population) followed by the 35 to 54 year age groups.
n From 1990 onwards, there has not been any one age group of females that has consistently
had a higher rate of suicide than other age groups.
n The largest drop in suicide rates between 1997 and 2006 was observed for 15 to 24 year olds,
with a fall of 56% in suicide rates for this group.

38
Figure 2. Suicide Rates, All Ages, 1980-2006, by Sex 72.
Are the patterns the same for Aboriginal and Torres Strait Islander people?
n Accurate suicide statistics and population estimates are difficult to obtain for Aboriginal and
Torres Strait Islander people. Due to both the relatively small numbers and low coverage
in some areas of Australia, the ABS only publishes data for NSW, QLD, SA and NT. Thus
data on suicide rates are likely to be, at best, minimum figures and the information must be
interpreted cautiously.
n The percentage of deaths attributable to suicide is much higher among Aboriginal and Torres
Strait Islander people (about 4%) than other Australians (about 1.5%).
n Suicide is more concentrated in the earlier adult years for Aboriginal and Torres Strait
Islander people than for the general Australian population, with recent data indicating the
highest rates for both males and females in the 15-24 year age group.
45.0
40.0
35.0
30.0
25.0
20.0
15.0
10.0
5.0
0.0
Rate
per
100
,000
Males
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
Females

39
Do rates vary among people from culturally and linguistically diverse backgrounds?
n One quarter of suicides in Australia occur among people who have migrated to Australia,
with 60% of these being from non-English speaking countries. However, rates vary according
to country of origin, gender and age73.
n First generation migrants in Australia show similar suicide rates to those in their country
of origin.
n Rates are generally higher among people born in English-speaking countries, and those from
western, northern and eastern Europe, and lower among people from southern Europe, the
Middle East and Asia74.
n Overall, males born outside of Australia have a lower suicide rate than Australian-born
males, while the rate is higher for females born overseas than for Australian-born females.
The rate is also higher for people of both genders aged over 65 75.
Do rates vary between urban and rural areas?
n There is some evidence that suicide rates in rural and remote areas are significantly
greater than in urban populations. This may be especially true among young men in
remote regions 76.
n Possible factors contributing to higher rates in these areas include isolation, rural poverty,
increased risk-taking behaviour and access to lethal means (eg firearms). It has also been
suggested that a culture of self-reliance, that does not encourage help-seeking behaviour,
may be one of the most important contributing factors to youth suicide in rural areas77.
What are the most common methods of suicide?
n Since the late 90s, more than 40% of suicide deaths have been from hanging, making this the
most common method.
n Males who die by suicide are more likely to do so via hanging than females, with
approximately 50% of male suicide deaths due this method since 2001, compared with 40%
of female suicide deaths.

40
n Females who take their own lives do so via drug poisoning in more than a quarter of cases, whereas for males, this method constitutes less than 10% of suicide deaths.
n Suicides by firearms were far more common among males in the mid 1990s, but the numbers per year are now less than half. This is most likely due to restrictions on firearm ownership
in place since 1997.
Are people in custody more at risk?
n People in any form of custody have suicide rates more than three times higher than the general population.
n The Royal Commission into Aboriginal Deaths in Custody found that Aboriginal and Torres Strait Islander people were not more likely to die in custody than non-Indigenous people78. High numbers of Aboriginal and Torres Strait Islander deaths in custody were related to the
high rates of incarceration in this population group.
What are some of the impacts of suicide?
n A death by suicide can have devastating impacts on family, friends, colleagues, health professionals, emergency services, and potentially the whole community. People who have been directly affected by suicide may themselves experience mental health problems, and are at increased risk of taking their own lives.
n People who identify with the person who has taken their own life (as someone in a similar life stage or circumstance to themselves) may be adversely affected by their death and
consider suicide themselves as a result.
What is the relationship between self-harm and suicide?
n The relationship between self-harm and suicide is complex. Most commonly the motivation for self-harming behaviour is to cope with, or to gain a sense of relief from painful emotions and distressing personal experiences, not to result in death 79.
n Any action that is deliberately intended to cause death is best regarded as a suicide attempt 80. Any deliberate attempt on one’s life that results in death is best understood to
be a suicide.

41
n According to published research, more than half of individuals who self-harm do not have
suicidal thoughts at the time of self-harm and self-harm has been described as a way to
avoid suicide 81.
n This being said, acts of self-harm need to be taken seriously. Individuals who self-harm may
be considered at higher risk of further, more severe self-harm and later suicide82. Self-harm
and suicide attempts can be performed by the same individual – and in some cases the
intent may not be completely clear.
What are some risk factors for suicide?
There is no single cause for suicidal behaviour and each person’s situation is unique. Suicide
is a complex phenomenon and rarely occurs as the result of a single event. However, research
has revealed a number of common risk factors, which may increase the likelihood of someone
taking their own life:
n Individual factors – such as being male, experiencing physical health problems and
stressful life events such as bereavement or relationship breakdown. Young gay, lesbian or
transgender people may also have an increased risk of suicide;
n Mental illness – such as depression, substance abuse, psychotic disorders and a history of
previous suicide attempts;
n Family-related factors – such as family breakdown, family conflict, child custody issues,
abuse or family history of suicide;
n Social factors – such as socio-economic disadvantage, unemployment, being Aboriginal or
Torres Strait Islander, school disengagement, incarceration, and social and geographical
isolation (especially remote communities);
n Environmental factors – such as access to methods of suicide and exposure to suicide
methods via the media or peers. Suicide sometimes occurs in ‘clusters’ within a local area,
when people identify with the distress of someone who has taken their own life.

42
People who are more at risk of suicide include:
n people who have previously attempted suicide;n people with mental disorders;n people with alcohol or drug abuse problems;n males (particularly those aged 25-45 years);n young Aboriginal or Torres Strait Islander males;n people who are in any form of custody;n people in remote communities;n people bereaved by suicide.
Are there protective factors for suicide?
Similar to risk factors, there are no clear universal protective factors that may decrease the
likelihood of a person taking their life. Some known factors include:
n being connected or belonging to a family, school or other community, such as a sporting or
recreation group;
n having at least one significant person to relate to and bond with (whether that is a family
member, a friend or other person);
n having personal coping skills and resilience to deal with difficult situations;
n a sense of meaning, spiritual faith or belief that suicide is wrong;
n economic security, particularly in older people;
n good physical as well as mental health;
n early detection and treatment for mental illness and emotional problems;
n restricted access to means, such as firearms, prescription medications and certain
geographical locations.

43
Risk and protective factors are often at opposite ends of the same continuum.
For example, social isolation (risk factor) and social connectedness (protective factor)
are both extremes of social support.
Risk and protective factors may be modifiable (things that are changeable) or
non-modifiable (things that are unchangeable). For example, in some areas of Australia
isolated older men may be more likely, according to statistics, to take their own life.
Nothing can be done about their age or gender (non-modifiable factors), but it is
possible to change their social isolation (modifiable factor).
Figure 3. Examples of typical triggers or precipitating events to suicide.*
n Mental health problems
n Male
n Family discord, violence or abuse
n Family history of suicide
n Alcohol or other substance abuse
n Social or geographical isolation
n Financial stress
n Bereavements
n Hopelessnessn Feeling trapped –
like there’s no way out
n Increasing alcohol or drug use
n Withdrawing from friends, family or society
n No reason for living, no sense of purpose in life
n Prior suicide attemptn Uncharacteristic or
impaired judgement or behaviour
n Relationship endingn Loss of status
or respectn Debilitating physical
illness or accidentn Death or suicide of
relative or friendn Suicide of someone
famous or member of peer group
n Argument at homen Being abused
or bulliedn Media report on
suicide or suicide methods
n Expressed intent to die
n Has plan in mind
n Has access to lethal means
n Impulsive, aggressive or anti-social behaviour
Risk factors
Warning signs
Tipping point
Imminent Link
* Adapted with permission from the LIFE Framework, 2008 83.

44
Myth: Most suicides occur without warning.
n Although there may be some cases where suicide occurs without warning, many people that
attempt or die by suicide give verbal or non-verbal clues before the incident.
n Often there has been a history of personal problems, mental health issues, suicide threats or
prior attempts.
n Many people thinking about suicide will tell someone and some will seek professional help.
Myth: People who attempt suicide are just selfish or weak.
n People who attempt suicide are often experiencing extreme negative feelings (depression,
guilt, fear, anxiety) and may believe there is no other solution.
n People in this situation need professional and personal support, not judgement.
Myth: People who talk about taking their own life are just seeking attention.
n Any suggestion of suicidal thoughts or threats of suicide should always be taken seriously.
n A person who threatens or attempts to take their life is in need of support, whether or not
they are serious about ending their life at that particular time.
n Addressing the underlying problems may reduce the risk of future attempts.
Myth: Talking about suicide with someone at risk will give them the idea and increase the chance they will take their own life.
n Many troubled people may be relieved if the issue is raised in a caring and non-judgemental
way, allowing them to talk one-on-one about their feelings and to seek help.
n However, specifically raising the issue of suicide in a group setting (eg a school classroom),
or in the media without providing an opportunity to talk about the issue one-on-one is
not recommended.
Common Misconceptions about Suicide

Media and the Courts
The courts and the media are very different. They have different cultural expectations,
deadlines, commercial imperatives, historical development, language and protocols.
This section provides a basic overview of the media and the courts, including why the
courts are such a staple news source for journalists.
Why the media interest in courts?
News stories may be broadly categorised as routine, staged and spontaneous events.
Court reporting is generally routine news, as it occurs on a predictable basis, with regular
timing, sources, and venue. The courts have been described as “a feast of stories” among
other things84.
We try to find on a daily basis a sort of representative smattering of very different matters that are being handled from the Supreme Court,
to the local, to all the many tribunals.
…a forum for human issues where ordinary people are seen in extraordinary circumstances.
Courts are extremely cost effective, protected, you’re unlikely to be sued … [they’re] cheap, quick and dirty. Courts turn out some really good stories 85.
There are several reasons why court reporting is a staple for most media organisations86.
n Unlike other rounds, where the reporter has to seek out opposing points of view, courts
provide these in their adversarial context. Generally speaking, reporters will get their stories
from within the court-room.
45

46
n The relative safe reporting environment afforded by the privilege of courts means reporters can report and write stories relatively simply, as long as they are fair and balanced in their reportage and avoid legislative prohibitions.
n Often crime and court stories involve themes of fear, horror or shock, and much information can be deeply personal and intimate, therefore ‘newsworthy’.
n High profile and interesting stories can often be planned for through examination of the court lists and knowledge of police charges.
What makes news?
Much of what goes on in court is not newsworthy. It is mundane and will not be of interest to the media. In addition, because news space varies, what makes news one day, may not make it the next.
Two key elements of court cases that make them particularly newsworthy are conflict and deviant behaviours, which often occur in abundance. Court cases will often incorporate these news values or themes if they are to become news stories. Other news values include:
n Prominence, high impact, controversy, protest, key decisions, violence, scandal, moral disorder, proximity, human interest and timeliness;
n They may also include immediacy, dramatization, personalisation, simplification, titillation, non-conventionalism and novelty.
Paranoid schizophrenic attacker wants more freedom.A paranoid schizophrenic who avoided jail after two frenzied stabbings
has asked the Supreme Court for more freedom.Advertiser (2006, 19 December, p.23)
War veteran’s accused killer a schizophrenic.The man accused of killing a World War II veteran in an alleged unprovoked attack
has been suffering from schizophrenia for 21 years, a court heard yesterday. Daily Telegraph (2006, 4 October, p.4)

47
Any of these news values, themes or elements may be obviously located in a story, even
before the court case begins. Other times, these elements will emerge as the court case
develops and the journalist witnesses a development or shift in the case. Sometimes a news
angle will only emerge half way through a court case, when a comment, witness, finding or
piece of evidence is brought in.
The following table, adapted from the Australian Press Council report into newspapers in 2005,
breaks down what makes news in a range of papers. It may come as no surprise that crime is
the highest category of all categories of news, in all of the pages under analysis.
What is a court round?
A journalist’s ‘round’ is the particular field they work in and report on. The round is intended to
help the journalist develop a specialisation within the field, including greater knowledge and a
range of key sources from which to draw.
Courts are part of this rounds system. If the round system worked ideally, these reporters
would all know the laws and restrictions pertaining to the courts. This is, however, not always
the case.
Content analysis of Australian metropolitan & regional newspapers 2005
Content% of All (2448)
% of Page 1 (299)
% of Metro (1573)
% Regional (442)
% Sundays (435)
Crime 14.50 15.7 13.90 16.1 15.20
Federal politics 12.10 11.70 14.60 4.75 10.10
Entertainment 12.10 7.36 10.80 13.10 15.90
Accident/Emergency 10.70 10.70 9.35 15.80 10.60
State politics 8.05 7.36 10.20 4.07 4.14
Other 49.91 46.77 40.69 45.49 42.53
(Source, Australian Press Council) 87.

48
Who covers the court round?
The courts round is sometimes a training ground for young reporters. They bring to it what
they have learned at university, in their cadetship training and their general knowledge. That
is not to say that all court reporters are legal novices – some have law degrees or extended
legal knowledge. Nevertheless, the range of expertise amongst court reporters can be
huge, especially in cases where the ‘usual’ court reporter is absent, and a less experienced
colleague may cover courts in their stead.
This wide range of expertise, coupled with journalists’ often limited knowledge of complex
issues such as mental health and suicide, can result in a severely restricted pool of knowledge
to accurately cover coroners’ findings, committal proceedings, bail applications, pleas and so
on in court cases which deal with these issues.
Do journalists work together?
Court reporting tends to be somewhat different to other journalistic rounds in that reporters
often cooperate with each other, even when they represent different media outlets. The
regular contact between journalists at the courtroom means that they will often rely on each
other to fill in missed material, or for tips as to a good story.
Nevertheless, competition amongst journalists exists in all rounds and courts are no different.
Reporters will use a wide range of sources to find out what’s going on in courts, confirm
information and investigate.
What types of media are more interested in the courts?
Print media have a long history of covering courts, sharing the courts’ media rooms and
dedicating one reporter to the round. Radio and television on the other hand tend to send
reporters on a more ad-hoc basis, when a ‘good’ story is expected in court. Knowing what’s in
a day’s court line-up will usually come from police stories (earlier arrests) and police tip-offs
as well as other sources like lawyers.
Print journalists often therefore have a great ‘ownership’ of the round that they nurture and
cover systematically which allows them to develop sources within the courts and often form
positive working relationships.

49
How is the news story developed?
Changes in technology have led to greater multiple-platform reporting, using online as well as
traditional media. This means that one story can have several versions for a range of media
which will be built up from earlier stories. It also means that the speed with which stories can
be developed and released is greatly increased.
In one recent example, a reporter was able to send notification of a verdict in a case
by text message from the courtroom, meaning that a story ‘brief’ was available on a
newspaper’s website within minutes of the verdict, beating radio. That story was later
expanded as the journalist wrote the details of what had happened in the proceedings,
but shows how quickly news media can reach an audience.
The development of a news story will usually follow a set path where, once written and filed
by the journalist, it is subedited for the print version of the paper (and/or the online version).
At this point, the journalist usually has no control over the editing of their story. This can
prove problematic in covering court stories because the story in its entirety can often provide
context and important background which may, due to space, have to be reduced or removed.
Figure 4. Flowchart of the court/news process (in a newspaper).
Court list holds potential stories & the journalist beginsresearch
Story written by journalist based on court proceedings and interviews and filed to newspaper
Story selection at newspaper (depends on multiple factors)
Story to subeditor –edited to fit space and headlined Story appears
in newspaper – (may not appear in all editions)

50
What about headlines?
Headlines are also written by the sub-editor, beyond the control of the court reporter.
While they should reflect the story’s key point, these can sometimes be skewed toward a
catchy phrase or word choice that is more sensational than the body of the story. It is worth
remembering that journalists do not control this element of newspaper production despite
being the public face of the story.
Who are key sources of information?
Reporters rely heavily on sources, as well as first hand observation, in court reporting. The most common sources are:
n Lawyers – prosecutors and defence counsel; n Police Media Unit, police stories;n Court staff – sheriffs, bailiffs, clerk of the court, judge’s associates; n Court lists from daily newspapers or internet; n Informants or tip/offs; andn Other journalists in court and other media.
Since the early 1990s an additional common source in many jurisdictions has been the Court Information Officer. Those jurisdictions without these officers have been noted to be at a disadvantage when it comes to court-media relations.
The issue of access to information and meeting deadlines is crucial to getting a story right. In most cases, not providing information, or making transcript costs prohibitive, will not result in a story being abandoned. More likely, it will result in a story that is incomplete or inaccurate. Assisting the media to access accurate information is, therefore, key.
The July 2000 judgement of a young woman found to have killed her son provides an example of different headlines:
Stabbed toddler’s mother freed: judge cites life of pain (Age, 7 July 2000)
Judge lets killer mum walk free (Herald Sun, 7 July 2000)
No jail for mother who killed in a state of crisis (Sydney Morning Herald, 7 July 2000)

51
www.mindframe-media.info
The Mindframe Website
Mindframe Resources for Courts can be
found at www.mindframe-media.info
by clicking on the “Courts” tab.
The website also provides information
about other projects that form part of
the Mindframe Initiative.
The section for courts contains
information about the impact of news
reporting as well as further facts,
statistics, descriptions of specific
disorders, useful contacts, and a glossary
of terms. It also provides examples
and further clarification of “issues to
consider” for judicial officers and other
officers of the court.

52
Australian Indigenous Health Infonet – www.healthinfonet.ecu.edu.auAccess to information, research and resources related to social and emotional wellbeing for Aboriginal and Torres Strait Islander people.
Australian Network for Promotion, Prevention and Early Intervention for Mental Health (Auseinet) – www.auseinet.com A comprehensive website and clearinghouse for research, resources and link relevant to promotion, prevention and early intervention for mental health in Australia.
beyondblue: The National Depression Initiative – www.beyondblue.orgAccess to accurate and easy to read information about depression, anxiety and related disorders.
headspace: Youth Mental Health Foundation – www.headspace.org.auYouth friendly site with information about mental health issues and local services for young people.
Living is for Everyone (LIFE) Framework and website – www.livingisforeveryone.com.au Updated information, and links for health professionals and the wider community to enhance the understanding and prevention of suicide and self-harm in Australia.
The Media Monitoring Project I & II – www.mindframe-media.infoStudies assessing the extent and nature of reporting about suicide and mental illness in the Australian media over two 12-month periods, 2000-2001 & 2006-2007.
Mental Health in Australia – www.mentalhealth.gov.auInformation on the Australian Government’s role and contributions to mental health reform activities in Australia and the agencies responsible for implementation.
On the edge of justice: the legal needs of people with a mental illness in NSW – http://www.lawfoundation.net.au/report/mental This study, published by the Law and Justice Foundation of NSW in 2006, examines the legal and access to justice issues experienced by people with a mental illness.
SANE Australia – www.sane.org General information about mental illness, including access to fact sheets, resources, Helpline
Online, SANE’s youth website, and the StigmaWatch program.
Other Use fu l Webs i tes

53
Nat iona l Counse l l ing and Refer ra l L ines
Lifeline – 13 11 14
A 24-hour telephone counselling
and referral service across Australia.
www.lifeline.org.au
Just Ask – 1300 13 11 14
Mental health information line for
rural communities.
Kids Helpline – 1800 55 1800
A 24-hour free counselling service for
young people aged between 5 and 25.
www.kidshelponline.com.au
Mensline Australia – 1300 78 99 78
A 24-hour counselling service for men.
www.menslineaus.org.au
Mental Illness Fellowship – 1800 98 59 44
Mental health information and referral.
www.mifellowship.org.au
SANE Helpline – 1800 18 SANE (7263)
Mental illness information, support
and referral throughout Australia.
www.sane.org
Vietnam Veterans Counselling Service – 1800 011 046A 24-hour emergency counselling service for veterans and their families.www.vvaa.org.au/vvcs.htm
Salvo Care Line –1300 651 251 A crisis counselling service available throughout Australia. www.salvos.org.au
Suicide Helpline (VIC) – 1300 651 251A 24-hour telephone counselling and referral service for Victoria only. www.suicidehelpline.org.au
Crisis Care – 1800 18 45 27Information and links to counselling services for gay and lesbian people in Australia.www.glccs.org.au
ReachOut! – www.reachout.com.auInteractive website to help young people through tough times.
Vibe Australia Healthy Vibe – www.vibe.com.au For details of Aboriginal Medical Services in Australia.

54
Australian Institute for Suicide Research and PreventionSuicide and self-harm research, suicide prevention, training.(07) 5552 9089 or 0408 727 706www.griffith.edu.au/aisrap/
beyondblue – The National Depression InitiativeDepression and suicide, anxiety, bipolar disorder & postnatal depression.(03) 9810 6100 or 0408 810 242www.beyondblue.org.au www.ybblue.com.au (youth)
Black Dog InstituteDepression, bipolar disorder, stigma and discrimination.(02) 9382 4368www.blackdoginstitute.org.au
depressioNetDepression and online support, mental illness, suicide and self-harm, stigma.(02) 9331 7222www.depressionet.com.au
LifelineMental health and wellbeing, help seeking,suicide and self-harm, stigma.(02) 6215 9416 or 0417 440 078www.lifeline.org.au
Mental Health Council of AustraliaDelivery and funding of mental health services, mental health policy, & stigma.(02) 6285 3100 or 0417 289 111www.mhca.org.au
Multicultural Mental Health Australia Mental health information and service delivery for people from culturally and linguistically diverse backgrounds. (02) 9840 3333www.mmha.org.au
Office for Aboriginal and Torres Strait Islander Health Information on services & wellbeing for Aboriginal and Torres Strait Islander people.(02) 6289 5027 www.health.gov.au
ORYGEN Youth HealthYouth mental illness (mood, anxiety, eating, substances), suicide, self-harm. (03) 9342 2800www.orygen.org.au
SANE AustraliaMental illness, suicide and self-harm, stigma and discrimination, media reporting.(03) 9682 5933 or 0414 427 291www.sane.org & www.itsallright.org
Exper t Comment

55
State Hea l th Depar tments
Mental Health Media Unit
ACT - www.health.act.gov.au (02) 6205 0896 (02) 6205 0896
NSW - www.health.nsw.gov.au (02) 9391 9000 (02) 9391 9121
NT - www.health.nt.gov.au (08) 8999 2553 (08) 8999 2886
Queensland - www.health.qld.gov.au (07) 3234 0111 (07) 3234 1316
SA - www.health.sa.gov.au (08) 8226 6000 (08) 8226 6488
Tasmania - www.dhhs.tas.gov.au (03) 6230 7549 (03) 6233 4890
Victoria - www.dhs.vic.gov.au (03) 9606 8592 (03) 9096 7296
WA - www.health.wa.gov.au (08) 9222 4099 (08) 9489 2888
Name Website Phone
Australian Communications and Media Authority (ACMA) www.acma.gov.au 1300 850 115
Special Broadcasting Service (SBS) www.sbs.com.au 1800 500 727
Australian Broadcasting Corporation (ABC) www.abc.net.au (02) 8333 1500
Australian Press Council www.presscouncil.org.au 1800 025 712
Commercial Radio Australia www.commercialradio.com.au (02) 9281 6577
Free TV Australia www.freetvaust.com.au (02) 8968 7100
Australian Subscription Television
and Radio Association (ASTRA) www.astra.org.au (02) 9776 2684
Contact s in the Austra l i an Media

56
Add your local or other useful contacts here:
Usefu l Contact s

Add your local or other useful contacts here:
57
Usefu l Contact s

58
1 Francis, C., Pirkis, J., Dunt, D., & Blood, R. W. (2001). Mental health and illness in the media: A review of the literature. Canberra: Commonwealth Department of Health and Ageing.
2 Francis, C., Pirkis, J., Dunt, D., & Blood, R. W. (2001). Op Cit.
3 Dare A., Pirkis J., Blood R.W., Rankin B., Williamson S., Burgess P. & Jolley D. (In Press). The Media Monitoring Project: Changes in Media Reporting of Suicide and Mental Health and Illness in Australia, 2000/01-2006/07. Melbourne: Centre for Health Policy, Programs and Economics, The University of Melbourne.
4 Dare A., Pirkis J., Blood R.W., Rankin B., Williamson S., Burgess P. & Jolley D. (In Press). Op cit.
5 Benkert, O., Graf-Morgenstern, M., Hillert, A., Sandman, J., Ehmig, S.C., Weissbecker, H., et. al. (1997). Public opinion on psychotropic drugs: An analysis of the factors influencing acceptance or rejection. Journal of Nervous and Mental Disease, 185, 151-158.
6 Francis, C., Pirkis, J., Dunt, D. & Blood, R.W. (2001) Op Cit.
7 Ibid
8 Ferriman, A. (2000). The stigma of schizophrenia. British Medical Journal, 320, 522.
9 Hunter Institute of Mental Health (2007). Mindframe for Law Enforcement: Final Scoping Study Report. Available from www.mindframe-media.info
10 Dare A., Pirkis J., Blood R.W., Rankin B., Williamson S., Burgess P. & Jolley D. (In Press). Op cit.
11 Francis, C., Pirkis, J., Dunt, D., & Blood, R. W. (2001). Op Cit.
12 Benkert, O., Graf-Morgenstern, M., Hillert, A., Sandman, J., Ehmig, S.C., Weissbecker, H., et. al. (1997). Op Cit.
13 Granello, D., Pauley, P., & Carmichael, A. (1999). Relationship of the media to attitudes towards people with mental illness. Journal of Humanistic Counselling Education and Development, 38, 98-103.
14 Lopez, L. R. (1991). Adolescent’s attitudes toward mental illness and perceived sources of their attitudes: An examination of pilot data. Archives of Psychiatric Nursing, 5, 271-80.
15 Hyler, S. E., Gabbard, G. O., & Schneider, I. (1991). Homicidal maniacs and narcissistic parasites: Stigmatisation of mentally ill persons in the movies. Hospital and Community Psychiatry, 42, 1044-1048.
16 Allan, R., & Nairn, R. G., (1997). Media depiction of mental illness: An analysis of the use of dangerousness. Australian and New Zealand Journal of Psychiatry, 31, 375-381.
17 Dare A., Pirkis J., Blood R.W., Rankin B., Williamson S., Burgess P. & Jolley D. (In Press). Op cit.
18 Granello, D., Pauley, P., & Carmichael, A. (1999). Op cit.
References

59
19 Rosen, A., Walter, G., Politis, T., & Shortland, M. (1997). From shunned to shining: Doctors, madness and psychiatry in Australian and New Zealand cinema. Medical Journal of Australia, 167, 640-644.
20 Domino, G. (1983). Impact of the film ‘One Flew over the Cuckoo’s Nest’, on attitudes towards mental illness. Psychological Reports, 53, 170-182.
21 Wahl, O. F., & Lefkowits, J. Y. (1989). Impact of a television film on attitudes towards mental illness. American Journal of Community Psychology, 1794, 521-528.
22 Dietrich, S., Heider, D., Matschinger, H., & Angermeyer, M. C. (2006). Influence of newspaper reporting on adolescents’ attitudes toward people with mental illness. Social Psychology and Psychiatric Epidemiology, 41, 318-322
23 Ferriman, A. (2000). Op Cit.
24 SANE Australia. (2005). Make it real! A report on consumer impressions of and responses to film and television portrayals of mental illness and suicide. A consultation project conducted by SANE Australia for the National Media and Mental Health Working Group.
25 Pirkis, J. & Blood, R.W. (2001) Suicide and the Media: A Critical Review. Canberra: Commonwealth Department of Health and Ageing.
26 Hunter Institute of Mental Health (2007) Op Cit.
27 Dare A., Pirkis J., Blood R.W., Rankin, B., Williamson S., Burgess P. & Jolley D. (In Press). Op cit.
28 Pirkis, J., & Blood, R. W. (2001). Op cit.
29 Wasserman, I.M. (1984). Imitation and suicide: A re-examination of the Werther effect. American Sociological Review, 49, 427-436.
30 Stack, S. (1987). Celebrities and suicide: A taxonomy and analysis, 1948-1983. American Sociological Review, 52, 401-412.
31 Tousignant, M., Mishara, B.L., Caillaud, A., Fortin, V., & St-Laurent, D. (2005). The impact of media coverage of the suicide of a well-known Quebec reporter: the case of Gaëtan Girouard. Social Science & Medicine, 60, 1919-1926.
32 Phillips, D. P. (1974). The influence of suggestion on suicide: Substantive and theoretical implications of the Werther effect. American Sociological Review, 39, 340-354.
33 Stack, S. (1990). Audience receptiveness, the media and aged suicide, 1968-1980. Journal of Aging Studies, 4, 195-209.
34 Wasserman, I. M. (1992). The impact of epidemic, war, prohibition and media on suicide: United States 1910-1920. Suicide and Life Threatening Behaviour, 22, 240-254.
35 Ashton, J. R., & Donnan, S. (1979). Suicide by burning: A current epidemic. British Medical Journal, 2, 769-770.
36 Ashton, J. R., & Donnan, S. (1981). Suicide by burning as an epidemic phenomenon: An analysis of 82 deaths and inquests in England and Wales in 1978-79. Psychological Medicine, 11, 735-739.

60
37 Versey, M. J., Kamanyire, R., & Volans, G. N. (1999). Antifreeze poisonings give more insight into copycat behaviour (letter). British Medical Journal, 319, 1131.
38 Chan, K.P.M., Yip, P.S.F., Au, J. & Lee, D.T.S. (2005). Charcoal-burning suicide in post-transition Hong Kong. British Journal of Psychiatry, 186, 67-73.
39 Etzersdorfer, E., Voracek, M., & Sonneck, G., (2004). A dose-response relationship between imitational suicides and newspaper distribution. Archives of Suicide Research, 8, 137-145.
40 Stack, S. (1990). Op cit.
41 Hassan, R. (1995). Effects of newspaper stories on the incidence of suicide in Australia: A research note. Australian and New Zealand Journal of Psychiatry, 29, 480-483.
42 Romer, D, Jamiewson, P.E. & Jamieson, KH. (2006). Are news reports of suicide contagious? A stringent test in six U.S. cities. In Journal of Communication, 56, 253-270.
43 Pirkis J. E., Burgess, P.M., Francis, R., Blood, W. & Jolley, D.J. (2006). The relationship between media reporting of suicide and actual suicide in Australia. Social Science & Medicine, 62, 2874-2886.
44 Dare A., Pirkis J., Blood R.W., Rankin B., Williamson, S., Burgess, P. & Jolley, D. (In Press). Op cit.
45 Martin, G., & Koo, L. (1997). Celebrity Suicide: Did the death of Kurt Cobain affect suicides in Australia? Archives of Suicide Research, 3, 187-198.
46 Gould, M.S., & Shaffer, D. (1986). The impact of suicide in television movies. New England Journal of Medicine, 315, 690-694.
47 Etzersdorfer, E., & Sonneck, G. (1988). Preventing suicide by influencing mass media reporting: The Viennese experience 1980 – 1996. Archives of Suicide Research, 4, 67-74.
48 Etzersdorfer, E., Sonneck, G., & Nagel Kuess, S. (1992). Newspaper reports and suicide (letter). New England Journal of Medicine, 327, 502-503.
49 Sonneck, G., Etzersdorfer., E & Nagel Kuess, S. (1994). Imitative suicide on the Viennese subway. Social Science and Medicine, 38, 453-457.
50 The World Health Report. (2001). Mental Health: New understanding, new hope. Geneva: World Health Organisation. Retrieved February 5, 2006 from: http://www.who.int/whr/2001/en/.
51 World Health Organisation. Retrieved 03 April, 2008 from http://www.who.int/mental_health/management/depression/definition/en/
52 Maj, M., Akiskal, H.S., Lopez-Ibor, J., & Sartorius, N. (2002). Bipolar Disorder - WPA Series Evidence and Experience in Psychiatry. London: Wiley.
53 Griez. E, Faravelli, C., Nutt, D. & Zohar, J. (2001). Anxiety Disorders- An Introduction to Clinical Management and Research. London: Wiley.
54 Millon, T. (2004). Personality disorders in modern life, 2nd ed. New Jersey: Wiley.
55 Magnavita, J. J (2004). Op Cit.
56 Magnavita, J. J. (2004). Handbook of Personality Disorders -Theory and Practice. London: Wiley.

61
57 Maj, M., Akiskal. H.S., Mezzich, J.E. & Okasha, A. (2005). Personality Disorders - WPA Series Evidence and Experience in Psychiatry. London: Wiley.
58 Ibid
59 Ibid 60 American Psychiatric Association (2004).
Practice Guideline for the Treatment of Patients with Schizophrenia, 2nd Edition. APA Press
61 Ibid62 Stefan, M., Travis, M. & Murray, R.M. (2002). An
Atlas of Schizophrenia. London: Partheon.
63 Ibid64 Australian Bureau of Statistics. (1997). National
survey of mental health and wellbeing. Canberra, ACT: Australian Bureau of Statistics
65 Karras, M., McCarron, E., Gray, A. & Ardasinski, S. (2006) On the edge of justice: the legal needs of people with a mental illness in NSW. Sydney: Law and Justice Foundation of NSW.
66 Stouthard M.E.A., Essink-Bot M.L., Bonsel G.J., Barendregt J.J., Kramer P.G., vande Water H.P.A., Gunning-Schepers L.J., & van der Maas P.J. (1997). Disability Weights for Diseases in the Netherlands. Rotterdam: Erasmus University.
67 New South Wales Mental Health Sentinel Review Committee. (2003). Tracking Tragedy: A systemic look at suicides and homicides amongst mental health inpatients. NSW: Centre for Mental Health, Department of Health.
68 SANE Australia (2003). Factsheet 5. Violence and mental illness. Retrieved from: www.sane.org
69 Brennan, P. A., Mednick, S. A., & Hodgins, S.
(2000). Major mental disorders and criminal
violence in a Danish birth cohort. Archives of
General Psychiatry, 57, 494-500
70 Australian Bureau of Statistics. (2008). Causes
of Death, Australia, 2006. ABS catalogue
number 3303.0.
71 de Looper, M. & Bhatia, K. (2001). Australian
Health Trends, 2001 (AIHW Cat. No. PHE 24).
Canberra, ACT: AIHW.
72 Australian Bureau of Statistics. (2008). Op Cit.
73 Cantor, C. & Neulinger, K. (2000) The
epidemiology of suicide and attempted suicide
among young Australians. Australian and New
Zealand Journal of Psychiatry, 34, 370–387
74 Steel, Z., & McDonald, B. (2000). Suicide in
Immigrants Born in Non-English Speaking
Countries: The latest research. Retrieved
February 15, 2006 from: http://www.mmha.org.
au/MMHAPublications/Synergy/Winter2000/
McDonaldSuicide/view
75 McDonald, B., & Steel, Z. (1997). Immigrants and
Mental Health: An epidemiological analysis.
Sydney: Transcultural Mental Health Centre.
76 Australian Bureau of Statistics. (2000). Suicides
Australia 1921-1998. ABS Catalogue no. 3309.
77 Patterson, I., & Pegg, S. (1999). Nothing to do:
The relationship between ‘leisure boredom’ and
alcohol and drug addiction. Is there a link to
youth suicide in rural Australia? Youth Studies
Australia, 18, 24-29.

62
78 Final Report Of The Royal Commission Into Aboriginal Deaths In Custody Summary. Retrieved February 1, 2008 from http://www.austlii.edu.au/au/special/rsjproject/rsjlibrary/rciadic/rciadic_summary/rcsumk01.html
79 RANZCP (2005). Self-harm. Australian Treatment Guide for Consumers and Carers. Melbourne: The Royal Australian and New Zealand College of Psychiatrists.
80 Ibid
81 Stanley, B., Gameroff, M., Michalsen, V & Mann, J. (2001). Are suicide attempters who self-mutilate a unique population? American Journal of Psychiatry, 158, 427-432.
82 Owens, D., Horrocks, J. & House, A. (2002). Fatal and non-fatal repetition of self-harm. British Journal of Psychiatry, 181, 193-199.
83 Commonwealth of Australia (2008). LiFE: A Framework for Prevention of Suicide in Australia. Canberra: Australian Government.
84 Johnston, J. (2004) Communicating courts: an analysis of the changing interface between the courts and the media, unpublished Ph.D thesis, Griffith University, Gold Coast. pp. 135-136
85 Ibid
86 Ibid
87 Australian Press Council, (2006) The state of the news print media in Australia. Retrieved February 10 http://www.prescouncil.org.au/












![the media monitoring project - Amazon S3...and mental health/illness during the life of Reporting Suicide and Mental Illness[3]. The Media Monitoring Project collected media items](https://img.pdfslide.us/doc/110x75/5e80d10d991aeb40f21aca6f/the-media-monitoring-project-amazon-s3-and-mental-healthillness-during-the.jpg)



















