Embed Size (px)
Citation preview
MENTAL HEALTH COUNSELOR’S PROFESSIONAL LIABILITY POLICY
EXPLANATION OF PREMIUM RATES
INDIVIDUAL POLICY
(a) Under GROUPS 1, 2 & 3, coverage is provided to employed professionals individual coverageONLY as a W2 form employee. Practice outside the employment setting would not be covered.
(b) Under GROUPS 4, 5 & 7, coverage is provided to professionals who are self-employed only orwho are employed and doing outside practice. Individual coverage is provided for all youremployees as well as providing protection for you. Every professional and/or paraprofessionalemployee must be listed in Question 4(b) of the application and a premium must be paid foreach. The “Insured” rate would be charged for you. Employees with a Masters or higher in themental health field would pay the “Professional Employee” rate and any other employee exceptclerical would pay the “Paraprofessional Employee” rate. A premium charge is also made for anyIndependent Contractor or Consultant for whom you file a 1099 form whose services are in themental health field. This charge is made for the additional exposure you have in using suchservices. The Independent Contractor or Consultant listed is not covered.
PARTNERSHIP AND CORPORATE POLICY (Group 4, 5, & 7)
PARTNERSHIP – All partners must be listed under Question 4 (b) and a premium charge made foreach one. Every professional and paraprofessional employee must also be listed under Question 4(b)and a premium charge made for each one. You will find the premium charge for each Partner as wellas each Professional Employee (anyone with a Masters or higher in the mental health field) underthe “Partners and Professional Employee” rate. Any other employee except clerical will be chargedthe “Paraprofessional Employee” rate. A premium charge is also made for any IndependentContractor or Consultant for whom you file a 1099 form whose services are in the mental healthfield. This charge is made for the additional exposure you have in using such services. TheIndependent Contractor or Consultant listed is not covered.
GENERAL BUSINESS CORPORATIONS – The corporation pays the “Corporation” rate for theentity. Each owner and any employee with a Masters or higher in the mental health field pays the“Professional Employee” rate. Any other employee except clerical will be charged the“Paraprofessional Employee” rate. A premium charge is also made for any Independent Contractoror Consultant for whom you file a 1099 form whose services are in the mental health field. Thischarge is made for the additional exposure you have in using such services. The IndependentContractor or Consultant listed is not covered.
PROFESSIONAL CORPORATION (P.C.) OR PROFESSIONAL ASSOCIATION (P.A.) with noemployees other than the owner qualifies for the Individual rate.
PROFESSIONAL CORPORATION (P.C.) OR PROFESSIONAL ASSOCIATION (P.A.) withemployees would be rated the same as a general business corporation.
RATE SCHED
ULES A
ND
EXPLA
NATIO
N O
F PREMIU
M RA
TES
MH-DAR RATE
PREMIUM DISCOUNTS
Part-time discount: You are entitled to a 35% discount provided your activities as a professional do notexceed 20 hours a week. This discount is not available if you have employees, if you are in a partnership orif you own a corporation. This discount should be rounded off to the nearest dollar. It should be computedbefore taking any other discounts. If you are taking the part-time discount, make sure you enclose theadditional part-time worksheet. If you do not take the discount, we assume you do not want the part-timecoverage. You will find this rate has been computed for you and is indicated on the appropriate rateschedule for the group you qualify under.
Risk Management Discount: This discount applies only to the individual insured who meets ourunderwriting criteria for the Risk Management Discount. A 5% discount will be given for the completion of3 CE credits. Please forward proof (certificate of completion) and the syllabus and outline in order to beconsidered for the discount. We will refund the 5% if you qualify.
ADDITIONAL INSUREDS
If you need to list an additional insured on your policy, you must complete the Request for AdditionalInsured form included. The premium charges are as follows: Landlord - $15 First additional insured - $30Each additional insured thereafter - $15
DEFENSE REIMBURSEMENT COVERAGE
$5,000 for legal defense reimbursement for costs relating to proceedings (a hearing or disciplinary actionbefore a state licensing board or governmental regulatory body involving allegations of unprofessionalconduct, or a civil proceeding in which you are not a defendant but have been ordered to offer depositiontestimony regarding treatment rendered to a patient, or a civil proceeding in which you are not a party but havereceived a subpoena for record production) is provided in the policy at no additional cost to you. You canchoose a higher limit of $25,000, $50,000 or $75,000 for an additional premium which you will find on therate schedule for the group you qualify under.
Application must be signed, dated, fully completed and accompanied by the premium to be considered.
Please make checks payable to: American Professional Agency, Inc.
Program Administrator:AMERICAN PROFESSIONAL AGENCY, INC.
95 Broadway, Amityville, NY 11701(631) 691-6400 – (800) 421-6694www.americanprofessional.com
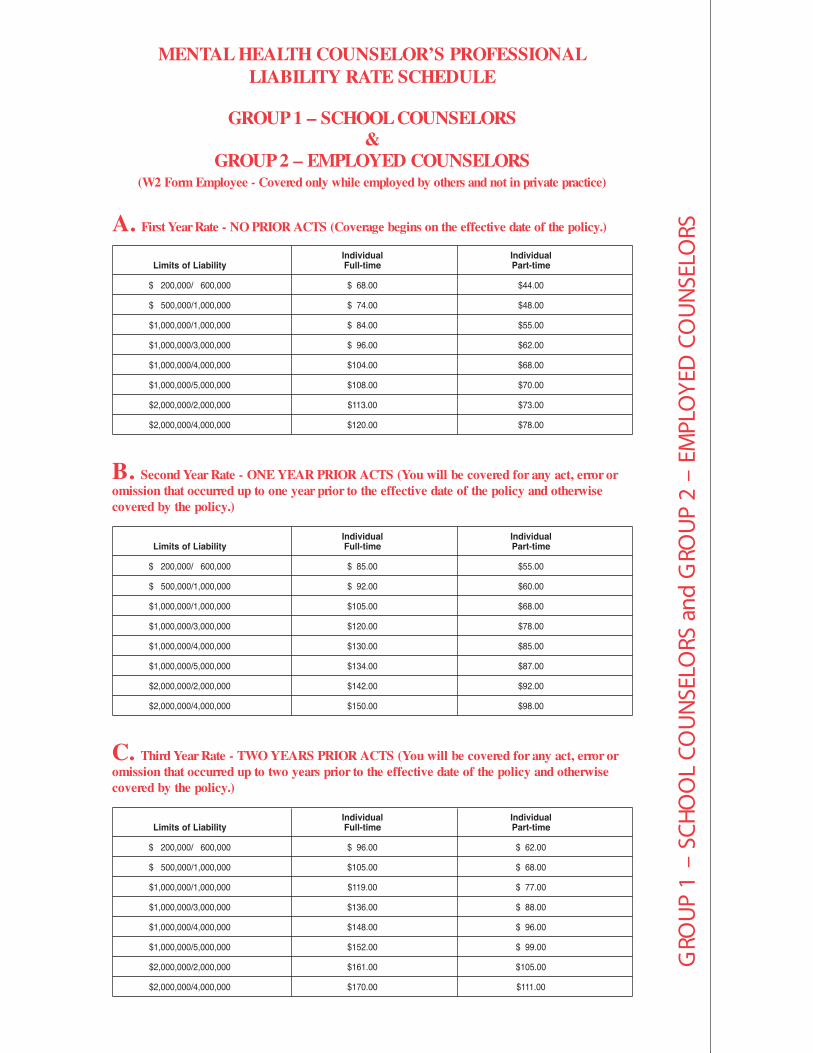
A. First Year Rate - NO PRIOR ACTS (Coverage begins on the effective date of the policy.)
laudividnIlaudividnIemit-traPemit-lluFytilibaiL fo stimiL
00.44$00.86 $000,006 /000,002 $
00.84$00.47 $000,000,1/000,005 $
00.55$00.48 $000,000,1/000,000,1$
00.26$00.69 $000,000,3/000,000,1$
00.86$00.401$000,000,4/000,000,1$
00.07$00.801$000,000,5/000,000,1$
00.37$00.311$000,000,2/000,000,2$
00.87$00.021$000,000,4/000,000,2$
B. Second Year Rate - ONE YEAR PRIOR ACTS (You will be covered for any act, error oromission that occurred up to one year prior to the effective date of the policy and otherwisecovered by the policy.)
laudividnIlaudividnIemit-traPemit-lluFytilibaiL fo stimiL
00.55$00.58 $000,006 /000,002 $
00.06$00.29 $000,000,1/000,005 $
00.86$00.501$000,000,1/000,000,1$
00.87$00.021$000,000,3/000,000,1$
00.58$00.031$000,000,4/000,000,1$
00.78$00.431$000,000,5/000,000,1$
00.29$00.241$000,000,2/000,000,2$
00.89$00.051$000,000,4/000,000,2$
C. Third Year Rate - TWO YEARS PRIOR ACTS (You will be covered for any act, error oromission that occurred up to two years prior to the effective date of the policy and otherwisecovered by the policy.)
laudividnIlaudividnIemit-traPemit-lluFytilibaiL fo stimiL
00.26 $00.69 $000,006 /000,002 $
00.86 $00.501$000,000,1/000,005 $
00.77 $00.911$000,000,1/000,000,1$
00.88 $00.631$000,000,3/000,000,1$
00.69 $00.841$000,000,4/000,000,1$
00.99 $00.251$000,000,5/000,000,1$
00.501$00.161$000,000,2/000,000,2$
00.111$00.071$000,000,4/000,000,2$
MENTAL HEALTH COUNSELOR’S PROFESSIONALLIABILITY RATE SCHEDULE
GROUP 1 – SCHOOL COUNSELORS&
GROUP 2 – EMPLOYED COUNSELORS(W2 Form Employee - Covered only while employed by others and not in private practice)
GRO
UP
1 –
SCH
OO
L CO
UN
SELO
RS a
nd G
ROU
P 2
– EM
PLO
YED
CO
UN
SELO
RS

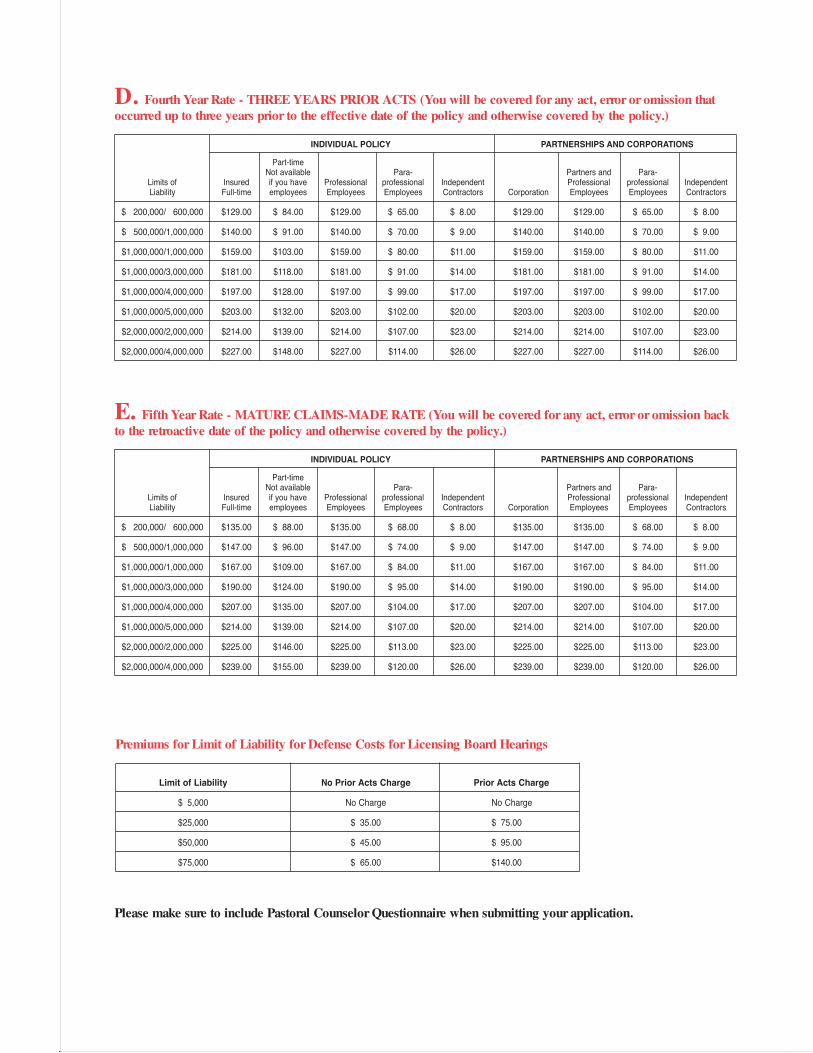
D. Fourth Year Rate - THREE YEARS PRIOR ACTS (You will be covered for any act, error oromission that occurred up to three years prior to the effective date of the policy and otherwise coveredby the policy.)
laudividnIlaudividnIemit-traPemit-lluFytilibaiL fo stimiL
00.07 $00.801$000,006 /000,002 $
00.67 $00.711$000,000,1/000,005 $
00.68 $00.331$000,000,1/000,000,1$
00.99 $00.251$000,000,3/000,000,1$
00.701$00.561$000,000,4/000,000,1$
00.111$00.071$000,000,5/000,000,1$
00.711$00.081$000,000,2/000,000,2$
00.421$00.091$000,000,4/000,000,2$
E. Fifth Year Rate - MATURE CLAIMS-MADE RATE (You will be covered for any act, error oromission back to the retroactive date of the policy and otherwise covered by the policy.)
laudividnIlaudividnIemit-traPemit-lluFytilibaiL fo stimiL
00.37 $00.311$000,006 /000,002 $
00.08 $00.321$000,000,1/000,005 $
00.19 $00.041$000,000,1/000,000,1$
00.401$00.061$000,000,3/000,000,1$
00.311$00.471$000,000,4/000,000,1$
00.611$00.971$000,000,5/000,000,1$
00.321$00.981$000,000,2/000,000,2$
00.031$00.002$000,000,4/000,000,2$
Premiums for Limit of Liability for Defense Costs for Licensing Board Hearings
Limit of Liability No Prior Acts Charge Prior Acts Charge
egrahC oNegrahC oN000,5 $
00.57 $00.53 $000,52$
00.59 $00.54 $000,05$
00.041$00.56$000,57$

GRO
UP
3 –
BACH
ELO
RS IN
MEN
TAL
HEA
LTH
A. First Year Rate - NO PRIOR ACTS (Coverage begins on the effective date of the policy.)
laudividnIlaudividnIemit-traPemit-lluFytilibaiL fo stimiL
00.24$00.46 $000,006 /000,002 $
00.64$00.07 $000,000,1/000,005 $
00.15$00.97 $000,000,1/000,000,1$
00.95$00.09 $000,000,3/000,000,1$
00.46$00.89 $000,000,4/000,000,1$
00.66$00.101$000,000,5/000,000,1$
00.07$00.701$000,000,2/000,000,2$
00.37$00.311$000,000,4/000,000,2$
B. Second Year Rate - ONE YEAR PRIOR ACTS (You will be covered for any act, error oromission that occurred up to one year prior to the effective date of the policy and otherwisecovered by the policy.)
laudividnIlaudividnIemit-traPemit-lluFytilibaiL fo stimiL
00.25$00.08 $000,006 /000,002 $
00.75$00.78 $000,000,1/000,005 $
00.46$00.99 $000,000,1/000,000,1$
00.37$00.311$000,000,3/000,000,1$
00.08$00.321$000,000,4/000,000,1$
00.38$00.721$000,000,5/000,000,1$
00.78$00.431$000,000,2/000,000,2$
00.29$00.241$000,000,4/000,000,2$
C. Third Year Rate - TWO YEARS PRIOR ACTS (You will be covered for any act, error oromission that occurred up to two years prior to the effective date of the policy and otherwisecovered by the policy.)
laudividnIlaudividnIemit-traPemit-lluFytilibaiL fo stimiL
00.95 $00.19 $000,006 /000,002 $
00.46 $00.99 $000,000,1/000,005 $
00.37 $00.211$000,000,1/000,000,1$
00.38 $00.821$000,000,3/000,000,1$
00.09 $00.931$000,000,4/000,000,1$
00.49 $00.441$000,000,5/000,000,1$
00.89 $00.151$000,000,2/000,000,2$
00.401$00.061$000,000,4/000,000,2$
MENTAL HEALTH COUNSELOR’S PROFESSIONALLIABILITY RATE SCHEDULE
GROUP 3 – BACHELORS IN MENTAL HEALTH(Covered only while employed by others and not in private practice)

D. Fourth Year Rate - THREE YEARS PRIOR ACTS (You will be covered for any act, error oromission that occurred up to three years prior to the effective date of the policy and otherwise coveredby the policy.)
laudividnIlaudividnIemit-traPemit-lluFytilibaiL fo stimiL
00.66 $00.201$000,006 /000,002 $
00.27 $00.011$000,000,1/000,005 $
00.18 $00.521$000,000,1/000,000,1$
00.39 $00.341$000,000,3/000,000,1$
00.101$00.551$000,000,4/000,000,1$
00.501$00.161$000,000,5/000,000,1$
00.011$00.961$000,000,2/000,000,2$
00.611$00.971$000,000,4/000,000,2$
E. Fifth Year Rate - MATURE CLAIMS -MADE RATE (You will be covered for any act, error oromission back to the retroactive date of the policy and otherwise covered by the policy.)
laudividnIlaudividnIemit-traPemit-lluFytilibaiL fo stimiL
00.07 $00.701$000,006 /000,002 $
00.57 $00.611$000,000,1/000,005 $
00.68 $00.231$000,000,1/000,000,1$
00.89 $00.051$000,000,3/000,000,1$
00.701$00.461$000,000,4/000,000,1$
00.011$00.961$000,000,5/000,000,1$
00.611$00.871$000,000,2/000,000,2$
00.321$00.981$000,000,4/000,000,2$
Premiums for Limit of Liability for Defense Costs for Licensing Board Hearings
Limit of Liability No Prior Acts Charge Prior Acts Charge
egrahC oNegrahC oN000,5 $
00.57 $00.53 $000,52$
00.59 $00.54 $000,05$
00.041$00.56$000,57$

GRO
UP
4 –
CLER
GY
AN
D P
AST
ORA
L CO
UN
SELO
RS
A. First Year Rate - NO PRIOR ACTS (Coverage begins on the effective date of the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
Limits of Insured if you have Professional professional Independent Professional professional IndependentLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $ 81.00 $53.00 $ 81.00 $41.00 $ 8.00 $ 81.00 $41.00 $ 8.00
$ 500,000/1,000,000 $ 88.00 $57.00 $ 88.00 $44.00 $ 9.00 $ 88.00 $ 88.00 $44.00 $ 9.00
$1,000,000/1,000,000 $100.00 $65.00 $100.00 $50.00 $11.00 $100.00 $100.00 $50.00 $11.00
$1,000,000/3,000,000 $114.00 $74.00 $114.00 $57.00 $14.00 $114.00 $114.00 $57.00 $14.00
$1,000,000/4,000,000 $124.00 $81.00 $124.00 $62.00 $17.00 $124.00 $124.00 $62.00 $17.00
$1,000,000/5,000,000 $128.00 $83.00 $128.00 $64.00 $20.00 $128.00 $128.00 $64.00 $20.00
$2,000,000/2,000,000 $135.00 $88.00 $135.00 $68.00 $23.00 $135.00 $135.00 $68.00 $23.00
$2,000,000/4,000,000 $143.00 $93.00 $143.00 $72.00 $26.00 $143.00 $143.00 $72.00 $26.00
MENTAL HEALTH COUNSELOR’S PROFESSIONAL LIABILITYRATE SCHEDULE
GROUP 4 – CLERGY AND PASTORAL COUNSELORS
B. Second Year Rate - ONE YEAR PRIOR ACTS (You will be covered for any act, error or omission thatoccurred up to one year prior to the effective date of the policy and otherwise covered by the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
Limits of Insured if you have Professional professional Independent Professional professional IndependentLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $101.00 $ 66.00 $101.00 $51.00 $ 8.00 $101.00 $101.00 $51.00 $ 8.00
$ 500,000/1,000,000 $110.00 $ 72.00 $110.00 $55.00 $ 9.00 $110.00 $110.00 $55.00 $ 9.00
$1,000,000/1,000,000 $125.00 $ 81.00 $125.00 $63.00 $11.00 $125.00 $125.00 $63.00 $11.00
$1,000,000/3,000,000 $143.00 $ 93.00 $143.00 $72.00 $14.00 $143.00 $143.00 $72.00 $14.00
$1,000,000/4,000,000 $155.00 $101.00 $155.00 $78.00 $17.00 $155.00 $155.00 $78.00 $17.00
$1,000,000/5,000,000 $160.00 $104.00 $160.00 $80.00 $20.00 $160.00 $160.00 $80.00 $20.00
$2,000,000/2,000,000 $169.00 $110.00 $169.00 $85.00 $23.00 $169.00 $169.00 $85.00 $23.00
$2,000,000/4,000,000 $179.00 $116.00 $179.00 $90.00 $26.00 $179.00 $179.00 $90.00 $26.00
C. Third Year Rate - TWO YEARS PRIOR ACTS (You will be covered for any act, error or omission thatoccurred up to two years prior to the effective date of the policy and otherwise covered by the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
Limits of Insured if you have Professional professional Independent Professional professional IndependentLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $115.00 $ 75.00 $115.00 $ 58.00 $ 8.00 $115.00 $115.00 $ 58.00 $ 8.00
$ 500,000/1,000,000 $125.00 $ 81.00 $125.00 $ 63.00 $ 9.00 $125.00 $125.00 $ 63.00 $ 9.00
$1,000,000/1,000,000 $142.00 $ 92.00 $142.00 $ 71.00 $11.00 $142.00 $142.00 $ 71.00 $11.00
$1,000,000/3,000,000 $162.00 $105.00 $162.00 $ 81.00 $14.00 $162.00 $162.00 $ 81.00 $14.00
$1,000,000/4,000,000 $176.00 $114.00 $176.00 $ 88.00 $17.00 $176.00 $176.00 $ 88.00 $17.00
$1,000,000/5,000,000 $182.00 $118.00 $182.00 $ 91.00 $20.00 $182.00 $182.00 $ 91.00 $20.00
$2,000,000/2,000,000 $192.00 $125.00 $192.00 $ 96.00 $23.00 $192.00 $192.00 $ 96.00 $23.00
$2,000,000/4,000,000 $203.00 $132.00 $203.00 $102.00 $26.00 $203.00 $203.00 $102.00 $26.00
$ 81.00
D. Fourth Year Rate - THREE YEARS PRIOR ACTS (You will be covered for any act, error or omission thatoccurred up to three years prior to the effective date of the policy and otherwise covered by the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
tnednepednIlanoisseforplanoisseforPtnednepednIlanoisseforplanoisseforPevah uoy fiderusnIfo stimiLLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $129.00 $ 84.00 $129.00 $ 65.00 $ 8.00 $129.00 $129.00 $ 65.00 $ 8.00
$ 500,000/1,000,000 $140.00 $ 91.00 $140.00 $ 70.00 $ 9.00 $140.00 $140.00 $ 70.00 $ 9.00
$1,000,000/1,000,000 $159.00 $103.00 $159.00 $ 80.00 $11.00 $159.00 $159.00 $ 80.00 $11.00
$1,000,000/3,000,000 $181.00 $118.00 $181.00 $ 91.00 $14.00 $181.00 $181.00 $ 91.00 $14.00
$1,000,000/4,000,000 $197.00 $128.00 $197.00 $ 99.00 $17.00 $197.00 $197.00 $ 99.00 $17.00
$1,000,000/5,000,000 $203.00 $132.00 $203.00 $102.00 $20.00 $203.00 $203.00 $102.00 $20.00
$2,000,000/2,000,000 $214.00 $139.00 $214.00 $107.00 $23.00 $214.00 $214.00 $107.00 $23.00
$2,000,000/4,000,000 $227.00 $148.00 $227.00 $114.00 $26.00 $227.00 $227.00 $114.00 $26.00
E. Fifth Year Rate - MATURE CLAIMS-MADE RATE (You will be covered for any act, error or omission backto the retroactive date of the policy and otherwise covered by the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
tnednepednIlanoisseforplanoisseforPtnednepednIlanoisseforplanoisseforPevah uoy fiderusnIfo stimiLLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $135.00 $ 88.00 $135.00 $ 68.00 $ 8.00 $135.00 $135.00 $ 68.00 $ 8.00
$ 500,000/1,000,000 $147.00 $ 96.00 $147.00 $ 74.00 $ 9.00 $147.00 $147.00 $ 74.00 $ 9.00
$1,000,000/1,000,000 $167.00 $109.00 $167.00 $ 84.00 $11.00 $167.00 $167.00 $ 84.00 $11.00
$1,000,000/3,000,000 $190.00 $124.00 $190.00 $ 95.00 $14.00 $190.00 $190.00 $ 95.00 $14.00
$1,000,000/4,000,000 $207.00 $135.00 $207.00 $104.00 $17.00 $207.00 $207.00 $104.00 $17.00
$1,000,000/5,000,000 $214.00 $139.00 $214.00 $107.00 $20.00 $214.00 $214.00 $107.00 $20.00
$2,000,000/2,000,000 $225.00 $146.00 $225.00 $113.00 $23.00 $225.00 $225.00 $113.00 $23.00
$2,000,000/4,000,000 $239.00 $155.00 $239.00 $120.00 $26.00 $239.00 $239.00 $120.00 $26.00
Please make sure to include Pastoral Counselor Questionnaire when submitting your application.
Premiums for Limit of Liability for Defense Costs for Licensing Board Hearings
Limit of Liability No Prior Acts Charge Prior Acts Charge
egrahC oNegrahC oN000,5 $
00.57 $00.53 $000,52$
00.59 $00.54 $000,05$
00.041$00.56$000,57$
GRO
UP
5 –
SELF
-EM
PLO
YED
CO
UN
SELO
RS O
R CE
RTIF
IED
HYP
NO
TIST
S
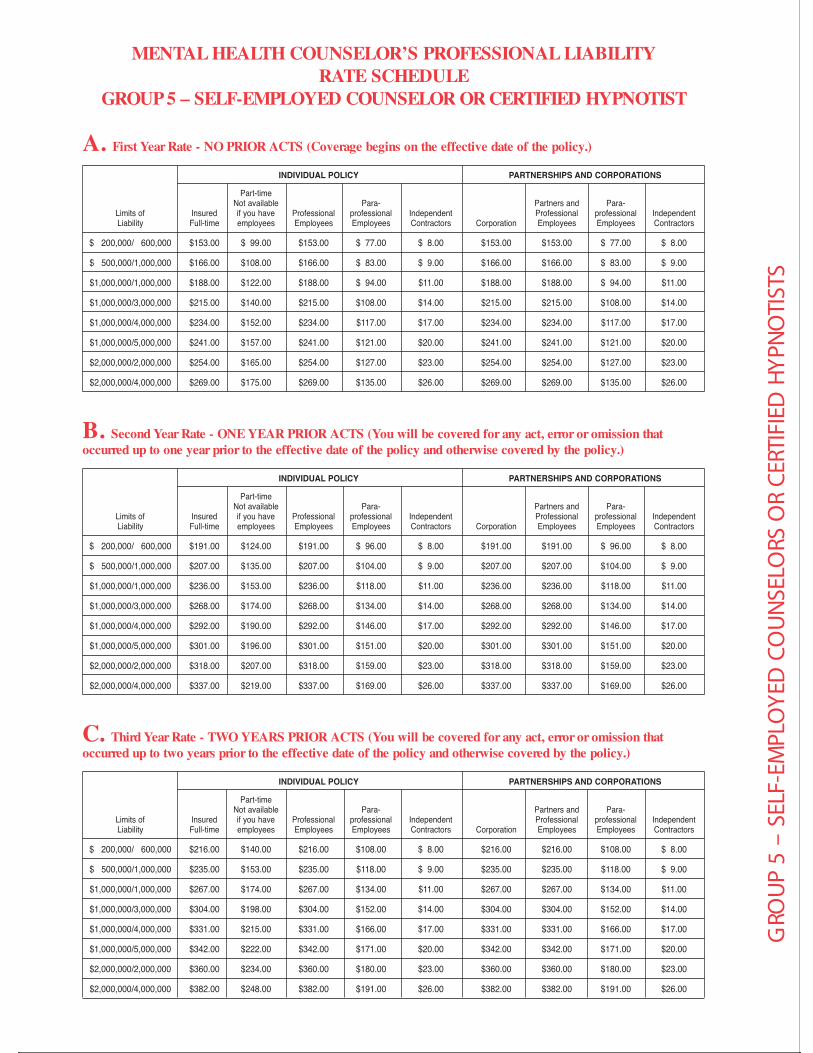
A. First Year Rate - NO PRIOR ACTS (Coverage begins on the effective date of the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
tnednepednIlanoisseforplanoisseforPtnednepednIlanoisseforplanoisseforPevah uoy fiderusnIfo stimiLLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $153.00 $ 99.00 $153.00 $ 77.00 $ 8.00 $153.00 $153.00 $ 77.00 $ 8.00
$ 500,000/1,000,000 $166.00 $108.00 $166.00 $ 83.00 $ 9.00 $166.00 $166.00 $ 83.00 $ 9.00
$1,000,000/1,000,000 $188.00 $122.00 $188.00 $ 94.00 $11.00 $188.00 $188.00 $ 94.00 $11.00
$1,000,000/3,000,000 $215.00 $140.00 $215.00 $108.00 $14.00 $215.00 $215.00 $108.00 $14.00
$1,000,000/4,000,000 $234.00 $152.00 $234.00 $117.00 $17.00 $234.00 $234.00 $117.00 $17.00
$1,000,000/5,000,000 $241.00 $157.00 $241.00 $121.00 $20.00 $241.00 $241.00 $121.00 $20.00
$2,000,000/2,000,000 $254.00 $165.00 $254.00 $127.00 $23.00 $254.00 $254.00 $127.00 $23.00
$2,000,000/4,000,000 $269.00 $175.00 $269.00 $135.00 $26.00 $269.00 $269.00 $135.00 $26.00
MENTAL HEALTH COUNSELOR’S PROFESSIONAL LIABILITYRATE SCHEDULE
GROUP 5 – SELF-EMPLOYED COUNSELOR OR CERTIFIED HYPNOTIST
B. Second Year Rate - ONE YEAR PRIOR ACTS (You will be covered for any act, error or omission thatoccurred up to one year prior to the effective date of the policy and otherwise covered by the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
tnednepednIlanoisseforplanoisseforPtnednepednIlanoisseforplanoisseforPevah uoy fiderusnIfo stimiLLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $191.00 $124.00 $191.00 $ 96.00 $ 8.00 $191.00 $191.00 $ 96.00 $ 8.00
$ 500,000/1,000,000 $207.00 $135.00 $207.00 $104.00 $ 9.00 $207.00 $207.00 $104.00 $ 9.00
$1,000,000/1,000,000 $236.00 $153.00 $236.00 $118.00 $11.00 $236.00 $236.00 $118.00 $11.00
$1,000,000/3,000,000 $268.00 $174.00 $268.00 $134.00 $14.00 $268.00 $268.00 $134.00 $14.00
$1,000,000/4,000,000 $292.00 $190.00 $292.00 $146.00 $17.00 $292.00 $292.00 $146.00 $17.00
$1,000,000/5,000,000 $301.00 $196.00 $301.00 $151.00 $20.00 $301.00 $301.00 $151.00 $20.00
$2,000,000/2,000,000 $318.00 $207.00 $318.00 $159.00 $23.00 $318.00 $318.00 $159.00 $23.00
$2,000,000/4,000,000 $337.00 $219.00 $337.00 $169.00 $26.00 $337.00 $337.00 $169.00 $26.00
C. Third Year Rate - TWO YEARS PRIOR ACTS (You will be covered for any act, error or omission thatoccurred up to two years prior to the effective date of the policy and otherwise covered by the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
tnednepednIlanoisseforplanoisseforPtnednepednIlanoisseforplanoisseforPevah uoy fiderusnIfo stimiLLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $216.00 $140.00 $216.00 $108.00 $ 8.00 $216.00 $216.00 $108.00 $ 8.00
$ 500,000/1,000,000 $235.00 $153.00 $235.00 $118.00 $ 9.00 $235.00 $235.00 $118.00 $ 9.00
$1,000,000/1,000,000 $267.00 $174.00 $267.00 $134.00 $11.00 $267.00 $267.00 $134.00 $11.00
$1,000,000/3,000,000 $304.00 $198.00 $304.00 $152.00 $14.00 $304.00 $304.00 $152.00 $14.00
$1,000,000/4,000,000 $331.00 $215.00 $331.00 $166.00 $17.00 $331.00 $331.00 $166.00 $17.00
$1,000,000/5,000,000 $342.00 $222.00 $342.00 $171.00 $20.00 $342.00 $342.00 $171.00 $20.00
$2,000,000/2,000,000 $360.00 $234.00 $360.00 $180.00 $23.00 $360.00 $360.00 $180.00 $23.00
$2,000,000/4,000,000 $382.00 $248.00 $382.00 $191.00 $26.00 $382.00 $382.00 $191.00 $26.00

D. Fourth Year Rate - THREE YEARS PRIOR ACTS (You will be covered for any act, error or omission thatoccurred up to three years prior to the effective date of the policy and otherwise covered by the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
tnednepednIlanoisseforplanoisseforPtnednepednIlanoisseforplanoisseforPevah uoy fiderusnIfo stimiLLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $242.00 $157.00 $242.00 $121.00 $ 8.00 $242.00 $242.00 $121.00 $ 8.00
$ 500,000/1,000,000 $263.00 $171.00 $263.00 $132.00 $ 9.00 $263.00 $263.00 $132.00 $ 9.00
$1,000,000/1,000,000 $298.00 $194.00 $298.00 $149.00 $11.00 $298.00 $298.00 $149.00 $11.00
$1,000,000/3,000,000 $340.00 $221.00 $340.00 $170.00 $14.00 $340.00 $340.00 $170.00 $14.00
$1,000,000/4,000,000 $370.00 $241.00 $370.00 $185.00 $17.00 $370.00 $370.00 $185.00 $17.00
$1,000,000/5,000,000 $382.00 $248.00 $382.00 $191.00 $20.00 $382.00 $382.00 $191.00 $20.00
$2,000,000/2,000,000 $403.00 $262.00 $403.00 $202.00 $23.00 $403.00 $403.00 $202.00 $23.00
$2,000,000/4,000,000 $427.00 $278.00 $427.00 $214.00 $26.00 $427.00 $427.00 $214.00 $26.00
E. Fifth Year Rate - MATURE CLAIMS-MADE RATE (You will be covered for any act, error or omission backto the retroactive date of the policy and otherwise covered by the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
tnednepednIlanoisseforplanoisseforPtnednepednIlanoisseforplanoisseforPevah uoy fiderusnIfo stimiLLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $254.00 $165.00 $254.00 $127.00 $ 8.00 $254.00 $254.00 $127.00 $ 8.00
$ 500,000/1,000,000 $276.00 $179.00 $276.00 $138.00 $ 9.00 $276.00 $276.00 $138.00 $ 9.00
$1,000,000/1,000,000 $314.00 $204.00 $314.00 $157.00 $11.00 $314.00 $314.00 $157.00 $11.00
$1,000,000/3,000,000 $358.00 $233.00 $358.00 $179.00 $14.00 $358.00 $358.00 $179.00 $14.00
$1,000,000/4,000,000 $389.00 $253.00 $389.00 $195.00 $17.00 $389.00 $389.00 $195.00 $17.00
$1,000,000/5,000,000 $402.00 $261.00 $402.00 $201.00 $20.00 $402.00 $402.00 $201.00 $20.00
$2,000,000/2,000,000 $424.00 $276.00 $424.00 $212.00 $23.00 $424.00 $424.00 $212.00 $23.00
$2,000,000/4,000,000 $449.00 $292.00 $449.00 $225.00 $26.00 $449.00 $449.00 $225.00 $26.00
Premiums for Limit of Liability for Defense Costs for Licensing Board Hearings
Limit of Liability No Prior Acts Charge Prior Acts Charge
egrahC oNegrahC oN000,5 $
00.57 $00.53 $000,52$
00.59 $00.54 $000,05$
00.041$00.56$000,57$
Please make sure to include the Hypnotist Questionnaire if you are applying as a certified Hypnotist.
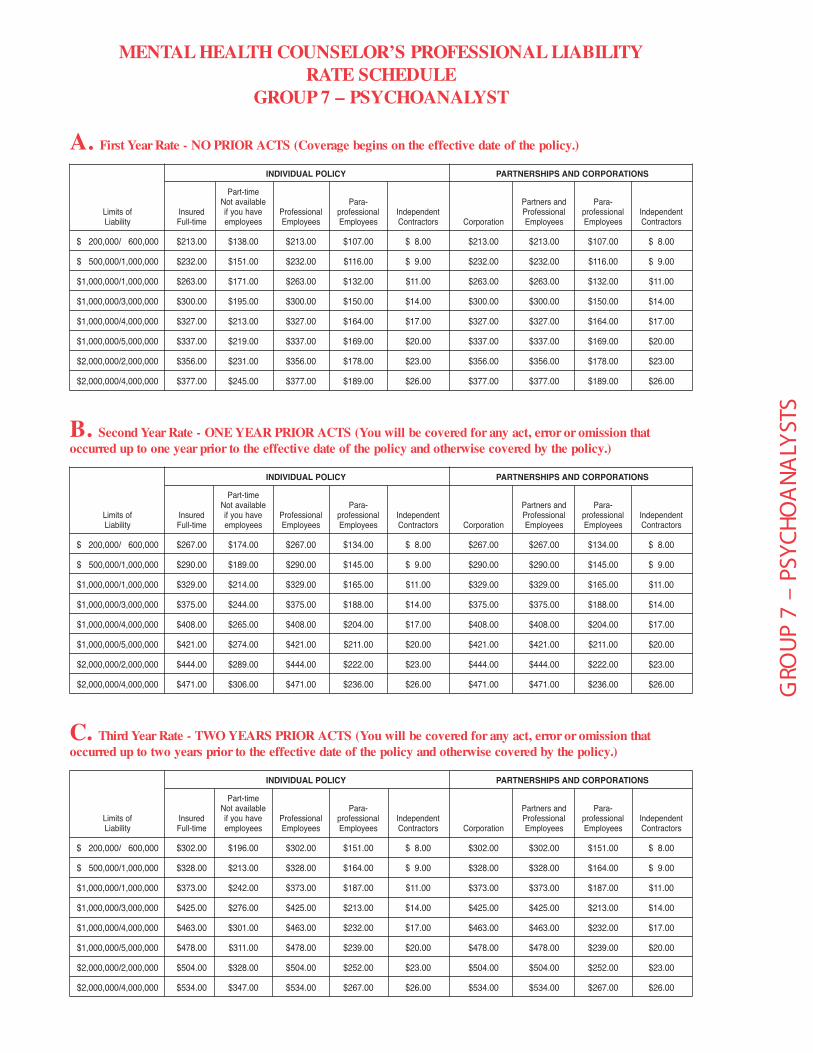
A. First Year Rate - NO PRIOR ACTS (Coverage begins on the effective date of the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
tnednepednIlanoisseforplanoisseforPtnednepednIlanoisseforplanoisseforPevah uoy fiderusnIfo stimiLLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $213.00 $138.00 $213.00 $107.00 $ 8.00 $213.00 $213.00 $107.00 $ 8.00
$ 500,000/1,000,000 $232.00 $151.00 $232.00 $116.00 $ 9.00 $232.00 $232.00 $116.00 $ 9.00
$1,000,000/1,000,000 $263.00 $171.00 $263.00 $132.00 $11.00 $263.00 $263.00 $132.00 $11.00
$1,000,000/3,000,000 $300.00 $195.00 $300.00 $150.00 $14.00 $300.00 $300.00 $150.00 $14.00
$1,000,000/4,000,000 $327.00 $213.00 $327.00 $164.00 $17.00 $327.00 $327.00 $164.00 $17.00
$1,000,000/5,000,000 $337.00 $219.00 $337.00 $169.00 $20.00 $337.00 $337.00 $169.00 $20.00
$2,000,000/2,000,000 $356.00 $231.00 $356.00 $178.00 $23.00 $356.00 $356.00 $178.00 $23.00
$2,000,000/4,000,000 $377.00 $245.00 $377.00 $189.00 $26.00 $377.00 $377.00 $189.00 $26.00
MENTAL HEALTH COUNSELOR’S PROFESSIONAL LIABILITYRATE SCHEDULE
GROUP 7 – PSYCHOANALYST
GRO
UP
7 –
PSYC
HOA
NALY
STS
B. Second Year Rate - ONE YEAR PRIOR ACTS (You will be covered for any act, error or omission thatoccurred up to one year prior to the effective date of the policy and otherwise covered by the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
tnednepednIlanoisseforplanoisseforPtnednepednIlanoisseforplanoisseforPevah uoy fiderusnIfo stimiLLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $267.00 $174.00 $267.00 $134.00 $ 8.00 $267.00 $267.00 $134.00 $ 8.00
$ 500,000/1,000,000 $290.00 $189.00 $290.00 $145.00 $ 9.00 $290.00 $290.00 $145.00 $ 9.00
$1,000,000/1,000,000 $329.00 $214.00 $329.00 $165.00 $11.00 $329.00 $329.00 $165.00 $11.00
$1,000,000/3,000,000 $375.00 $244.00 $375.00 $188.00 $14.00 $375.00 $375.00 $188.00 $14.00
$1,000,000/4,000,000 $408.00 $265.00 $408.00 $204.00 $17.00 $408.00 $408.00 $204.00 $17.00
$1,000,000/5,000,000 $421.00 $274.00 $421.00 $211.00 $20.00 $421.00 $421.00 $211.00 $20.00
$2,000,000/2,000,000 $444.00 $289.00 $444.00 $222.00 $23.00 $444.00 $444.00 $222.00 $23.00
$2,000,000/4,000,000 $471.00 $306.00 $471.00 $236.00 $26.00 $471.00 $471.00 $236.00 $26.00
C. Third Year Rate - TWO YEARS PRIOR ACTS (You will be covered for any act, error or omission thatoccurred up to two years prior to the effective date of the policy and otherwise covered by the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
tnednepednIlanoisseforplanoisseforPtnednepednIlanoisseforplanoisseforPevah uoy fiderusnIfo stimiLLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $302.00 $196.00 $302.00 $151.00 $ 8.00 $302.00 $302.00 $151.00 $ 8.00
$ 500,000/1,000,000 $328.00 $213.00 $328.00 $164.00 $ 9.00 $328.00 $328.00 $164.00 $ 9.00
$1,000,000/1,000,000 $373.00 $242.00 $373.00 $187.00 $11.00 $373.00 $373.00 $187.00 $11.00
$1,000,000/3,000,000 $425.00 $276.00 $425.00 $213.00 $14.00 $425.00 $425.00 $213.00 $14.00
$1,000,000/4,000,000 $463.00 $301.00 $463.00 $232.00 $17.00 $463.00 $463.00 $232.00 $17.00
$1,000,000/5,000,000 $478.00 $311.00 $478.00 $239.00 $20.00 $478.00 $478.00 $239.00 $20.00
$2,000,000/2,000,000 $504.00 $328.00 $504.00 $252.00 $23.00 $504.00 $504.00 $252.00 $23.00
$2,000,000/4,000,000 $534.00 $347.00 $534.00 $267.00 $26.00 $534.00 $534.00 $267.00 $26.00

D. Fourth Year Rate - THREE YEARS PRIOR ACTS (You will be covered for any act, error or omission thatoccurred up to three years prior to the effective date of the policy and otherwise covered by the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
tnednepednIlanoisseforplanoisseforPtnednepednIlanoisseforplanoisseforPevah uoy fiderusnIfo stimiLLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $338.00 $220.00 $338.00 $169.00 $ 8.00 $338.00 $338.00 $169.00 $ 8.00
$ 500,000/1,000,000 $367.00 $239.00 $367.00 $184.00 $ 9.00 $367.00 $367.00 $184.00 $ 9.00
$1,000,000/1,000,000 $417.00 $271.00 $417.00 $209.00 $11.00 $417.00 $417.00 $209.00 $11.00
$1,000,000/3,000,000 $475.00 $309.00 $475.00 $238.00 $14.00 $475.00 $475.00 $238.00 $14.00
$1,000,000/4,000,000 $517.00 $336.00 $517.00 $259.00 $17.00 $517.00 $517.00 $259.00 $17.00
$1,000,000/5,000,000 $534.00 $347.00 $534.00 $267.00 $20.00 $534.00 $534.00 $267.00 $20.00
$2,000,000/2,000,000 $563.00 $366.00 $563.00 $282.00 $23.00 $563.00 $563.00 $282.00 $23.00
$2,000,000/4,000,000 $596.00 $387.00 $596.00 $298.00 $26.00 $596.00 $596.00 $298.00 $26.00
E. Fifth Year Rate - MATURE CLAIMS-MADE RATE (You will be covered for any act, error or omission backto the retroactive date of the policy and otherwise covered by the policy.)
SNOITAROPROC DNA SPIHSRENTRAPYCILOP LAUDIVIDNI
Part-time-araPdna srentraP-araPelbaliava toN
tnednepednIlanoisseforplanoisseforPtnednepednIlanoisseforplanoisseforPevah uoy fiderusnIfo stimiLLiability Full-time employees Employees Employees Contractors Corporation Employees Employees Contractors
$ 200,000/ 600,000 $356.00 $231.00 $356.00 $178.00 $ 8.00 $356.00 $356.00 $178.00 $ 8.00
$ 500,000/1,000,000 $386.00 $251.00 $386.00 $193.00 $ 9.00 $386.00 $386.00 $193.00 $ 9.00
$1,000,000/1,000,000 $439.00 $285.00 $439.00 $220.00 $11.00 $439.00 $439.00 $220.00 $11.00
$1,000,000/3,000,000 $500.00 $325.00 $500.00 $250.00 $14.00 $500.00 $500.00 $250.00 $14.00
$1,000,000/4,000,000 $544.00 $354.00 $544.00 $272.00 $17.00 $544.00 $544.00 $272.00 $17.00
$1,000,000/5,000,000 $562.00 $365.00 $562.00 $281.00 $20.00 $562.00 $562.00 $281.00 $20.00
$2,000,000/2,000,000 $593.00 $385.00 $593.00 $297.00 $23.00 $593.00 $593.00 $297.00 $23.00
$2,000,000/4,000,000 $628.00 $408.00 $628.00 $314.00 $26.00 $628.00 $628.00 $314.00 $26.00
Premiums for Limit of Liability for Defense Costs for Licensing Board Hearings
Limit of Liability No Prior Acts Charge Prior Acts Charge
egrahC oNegrahC oN000,5 $
00.57 $00.53 $000,52$
00.59 $00.54 $000,05$
00.041$00.56$000,57$
IMPORTANT SURCHARGE INFORMATIONUnderwritten by: Darwin National Assurance Company
NOTICE TO KENTUCKY RESIDENTS:
Kentucky law requires insurance companies to charge all policies written for its residents a surcharge of 1.8%. We are also required to assess your policy with a municipality tax which is based on the location of your residence. In order for us to compute this additional tax, we need to have you contact our office for the appropriate premium. Please call 1-800-421-6694.
NOTICE TO NEW JERSEY RESIDENTS:
The New Jersey Property and Liability Insurance Guaranty Association requires insurance companies to charge all policies written for its residents a surcharge of .09%. Please include this additional amount when remitting your premium.
NOTICE TO WEST VIRGINIA RESIDENTS:
West Virginia law requires insurance companies to charge all policies written for its residents a surcharge of .55%. Please include this additional amount when remitting your premium.
DAR- Surcharge(Psychology, Mental Health and Marriage and Family Therapists)Rev. 2/13
IMPORTANT INFORMATIONPURCHASING GROUP FEE NOTICE
A $5.00 annual Purchasing Group fee needs to be added to your premium to help defer the administrative costs for maintaining the Professional Counselors Purchasing Group.
Insured Full-time
Part-time Not available if
you have employees
Professional Employees
Para-professional Employees
Independent Contractors Corporation
Partners and Professional Employees
Para-professional Employees
Independent Contractors
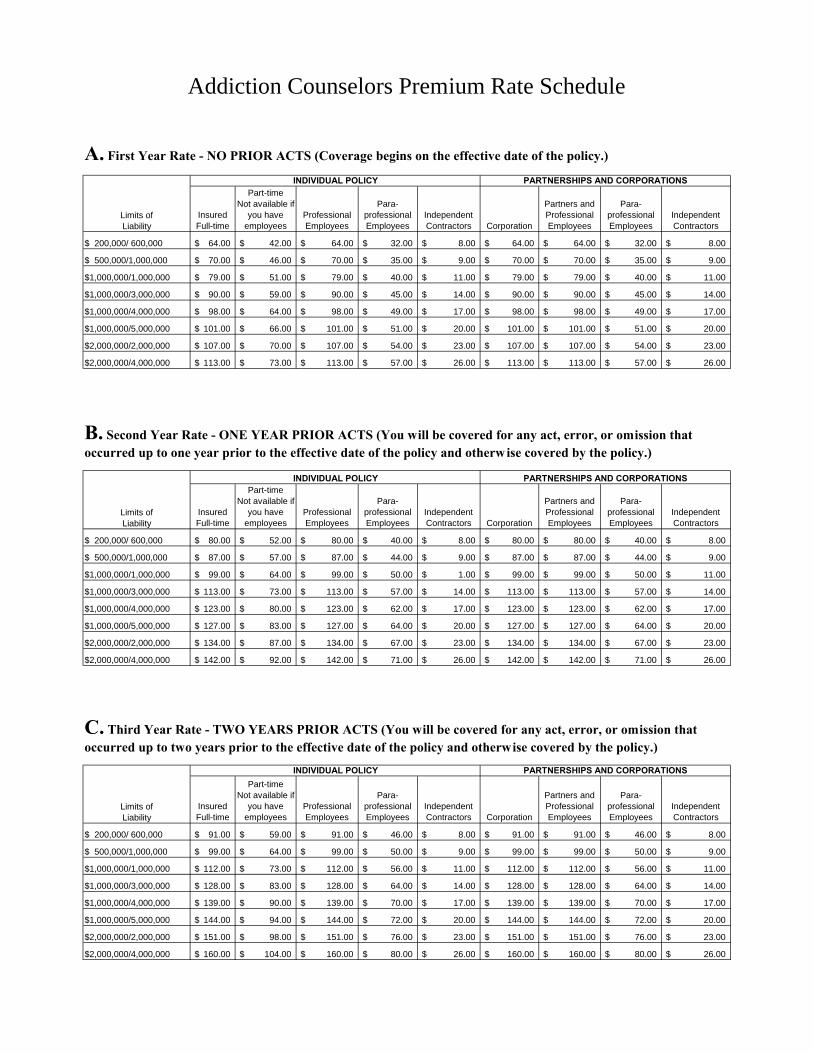
$ 200,000/ 600,000 64.00$ 42.00$ 64.00$ 32.00$ 8.00$ 64.00$ 64.00$ 32.00$ 8.00$
$ 500,000/1,000,000 70.00$ 46.00$ 70.00$ 35.00$ 9.00$ 70.00$ 70.00$ 35.00$ 9.00$
$1,000,000/1,000,000 79.00$ 51.00$ 79.00$ 40.00$ 11.00$ 79.00$ 79.00$ 40.00$ 11.00$
$1,000,000/3,000,000 90.00$ 59.00$ 90.00$ 45.00$ 14.00$ 90.00$ 90.00$ 45.00$ 14.00$
$1,000,000/4,000,000 98.00$ 64.00$ 98.00$ 49.00$ 17.00$ 98.00$ 98.00$ 49.00$ 17.00$
$1,000,000/5,000,000 101.00$ 66.00$ 101.00$ 51.00$ 20.00$ 101.00$ 101.00$ 51.00$ 20.00$
$2,000,000/2,000,000 107.00$ 70.00$ 107.00$ 54.00$ 23.00$ 107.00$ 107.00$ 54.00$ 23.00$
$2,000,000/4,000,000 113.00$ 73.00$ 113.00$ 57.00$ 26.00$ 113.00$ 113.00$ 57.00$ 26.00$
Insured Full-time
Part-time Not available if
you have employees
Professional Employees
Para-professional Employees
Independent Contractors Corporation
Partners and Professional Employees
Para-professional Employees
Independent Contractors
$ 200,000/ 600,000 80.00$ 52.00$ 80.00$ 40.00$ 8.00$ 80.00$ 80.00$ 40.00$ 8.00$
$ 500,000/1,000,000 87.00$ 57.00$ 87.00$ 44.00$ 9.00$ 87.00$ 87.00$ 44.00$ 9.00$
$1,000,000/1,000,000 99.00$ 64.00$ 99.00$ 50.00$ 1.00$ 99.00$ 99.00$ 50.00$ 11.00$
$1,000,000/3,000,000 113.00$ 73.00$ 113.00$ 57.00$ 14.00$ 113.00$ 113.00$ 57.00$ 14.00$
$1,000,000/4,000,000 123.00$ 80.00$ 123.00$ 62.00$ 17.00$ 123.00$ 123.00$ 62.00$ 17.00$
$1,000,000/5,000,000 127.00$ 83.00$ 127.00$ 64.00$ 20.00$ 127.00$ 127.00$ 64.00$ 20.00$
$2,000,000/2,000,000 134.00$ 87.00$ 134.00$ 67.00$ 23.00$ 134.00$ 134.00$ 67.00$ 23.00$
$2,000,000/4,000,000 142.00$ 92.00$ 142.00$ 71.00$ 26.00$ 142.00$ 142.00$ 71.00$ 26.00$
Insured Full-time
Part-time Not available if
you have employees
Professional Employees
Para-professional Employees
Independent Contractors Corporation
Partners and Professional Employees
Para-professional Employees
Independent Contractors
$ 200,000/ 600,000 91.00$ 59.00$ 91.00$ 46.00$ 8.00$ 91.00$ 91.00$ 46.00$ 8.00$
$ 500,000/1,000,000 99.00$ 64.00$ 99.00$ 50.00$ 9.00$ 99.00$ 99.00$ 50.00$ 9.00$
$1,000,000/1,000,000 112.00$ 73.00$ 112.00$ 56.00$ 11.00$ 112.00$ 112.00$ 56.00$ 11.00$
$1,000,000/3,000,000 128.00$ 83.00$ 128.00$ 64.00$ 14.00$ 128.00$ 128.00$ 64.00$ 14.00$
$1,000,000/4,000,000 139.00$ 90.00$ 139.00$ 70.00$ 17.00$ 139.00$ 139.00$ 70.00$ 17.00$
$1,000,000/5,000,000 144.00$ 94.00$ 144.00$ 72.00$ 20.00$ 144.00$ 144.00$ 72.00$ 20.00$
$2,000,000/2,000,000 151.00$ 98.00$ 151.00$ 76.00$ 23.00$ 151.00$ 151.00$ 76.00$ 23.00$
$2,000,000/4,000,000 160.00$ 104.00$ 160.00$ 80.00$ 26.00$ 160.00$ 160.00$ 80.00$ 26.00$
Limits of Liability
INDIVIDUAL POLICY PARTNERSHIPS AND CORPORATIONS
Addiction Counselors Premium Rate Schedule
INDIVIDUAL POLICY PARTNERSHIPS AND CORPORATIONS
Limits of Liability
A. First Year Rate - NO PRIOR ACTS (Coverage begins on the effective date of the policy.)
B. Second Year Rate - ONE YEAR PRIOR ACTS (You will be covered for any act, error, or omission that occurred up to one year prior to the effective date of the policy and otherwise covered by the policy.)
Limits of Liability
INDIVIDUAL POLICY PARTNERSHIPS AND CORPORATIONS
C. Third Year Rate - TWO YEARS PRIOR ACTS (You will be covered for any act, error, or omission that occurred up to two years prior to the effective date of the policy and otherwise covered by the policy.)

Insured Full-time
Part-time Not available if
you have employees
Professional Employees
Para-professional Employees
Independent Contractors Corporation
Partners and Professional Employees
Para-professional Employees
Independent Contractors
$ 200,000/ 600,000 102.00$ 66.00$ 102.00$ 51.00$ 8.00$ 102.00$ 102.00$ 51.00$ 8.00$
$ 500,000/1,000,000 110.00$ 72.00$ 110.00$ 55.00$ 9.00$ 110.00$ 110.00$ 55.00$ 9.00$
$1,000,000/1,000,000 125.00$ 81.00$ 125.00$ 63.00$ 11.00$ 125.00$ 125.00$ 63.00$ 11.00$
$1,000,000/3,000,000 143.00$ 93.00$ 143.00$ 72.00$ 14.00$ 143.00$ 143.00$ 72.00$ 14.00$
$1,000,000/4,000,000 155.00$ 101.00$ 155.00$ 78.00$ 17.00$ 155.00$ 155.00$ 78.00$ 17.00$
$1,000,000/5,000,000 161.00$ 105.00$ 161.00$ 81.00$ 20.00$ 161.00$ 161.00$ 81.00$ 20.00$
$2,000,000/2,000,000 169.00$ 110.00$ 169.00$ 85.00$ 23.00$ 169.00$ 169.00$ 85.00$ 23.00$
$2,000,000/4,000,000 179.00$ 116.00$ 179.00$ 90.00$ 26.00$ 179.00$ 179.00$ 90.00$ 26.00$
Insured Full-time
Part-time Not available if
you have employees
Professional Employees
Para-professional Employees
Independent Contractors Corporation
Partners and Professional Employees
Para-professional Employees
Independent Contractors
$ 200,000/ 600,000 107.00$ 70.00$ 107.00$ 54.00$ 8.00$ 107.00$ 107.00$ 54.00$ 8.00$
$ 500,000/1,000,000 116.00$ 75.00$ 116.00$ 58.00$ 9.00$ 116.00$ 116.00$ 58.00$ 9.00$
$1,000,000/1,000,000 132.00$ 86.00$ 132.00$ 66.00$ 11.00$ 132.00$ 132.00$ 66.00$ 11.00$
$1,000,000/3,000,000 150.00$ 98.00$ 150.00$ 75.00$ 14.00$ 150.00$ 150.00$ 75.00$ 14.00$
$1,000,000/4,000,000 164.00$ 107.00$ 164.00$ 82.00$ 17.00$ 164.00$ 164.00$ 82.00$ 17.00$
$1,000,000/5,000,000 169.00$ 110.00$ 169.00$ 85.00$ 20.00$ 169.00$ 169.00$ 85.00$ 20.00$
$2,000,000/2,000,000 178.00$ 116.00$ 178.00$ 89.00$ 23.00$ 178.00$ 178.00$ 89.00$ 23.00$
$2,000,000/4,000,000 189.00$ 123.00$ 189.00$ 95.00$ 26.00$ 189.00$ 189.00$ 95.00$ 26.00$
Premiums for Limit of Liability for Defense Costs for Licensing Board Hearings
D. Fourth Year Rate - THREE YEARS PRIOR ACTS (You will be covered for any act, error, or omission that occurred up to three years prior to the effective date of the policy and otherwise covered by the policy.)
Limits of Liability
INDIVIDUAL POLICY PARTNERSHIPS AND CORPORATIONS
E. Fifth Year Rate - MATURE CLAIMS-MADE RATE (You will be covered for any act, error, or omission back to the retroactive date of the policy and otherwise covered by the policy.)
Limits of Liability
INDIVIDUAL POLICY PARTNERSHIPS AND CORPORATIONS
Limit of Liability
$5,000
$25,000
$50,000
$75,000
$45.00
$65.00
Prior Acts Charge
No Charge
$75.00
$95.00
$140.00
No Prior Acts Charge
No Charge
$35.00
IMPORTANT SURCHARGE INFORMATION Underwritten by: Darwin National Assurance Company
NOTICE TO KENTUCKY RESIDENTS:
Kentucky law requires insurance companies to charge all policies written for its residents a surcharge of 1.8%. We are also required to assess your policy with a municipality tax which is based on the location of your residence. In order for us to compute this additional tax, we need to have you contact our office for the appropriate premium. Please call 1-800-421-6694.
NOTICE TO NEW JERSEY RESIDENTS:
The New Jersey Property and Liability Insurance Guaranty Association requires insurance companies to charge all policies written for its residents a surcharge of .09%. Please include this additional amount when remitting your premium.
NOTICE TO WEST VIRGINIA RESIDENTS:
West Virginia law requires insurance companies to charge all policies written for its residents a surcharge of .55%. Please include this additional amount when remitting your premium.
IMPORTANT INFORMATION PURCHASING GROUP FEE NOTICE
A $25.00 annual Purchasing Group fee needs to be added to your premium to help defer the administrative costs for maintaining the Professional Counselors Purchasing Group.
DAR- Surcharge (Addiction Counselors) Rev. 6/15/15
Addiction Counselors Only





























