Embed Size (px)
Citation preview

Mental Health Consequences of Bioterrorism - Year 2:
An Advanced Course for Hospital Emergency Department
Clinical Staff

Supported by Grant Number U3RHS04301-01-00 from the Health Resources and Services
Administration (HRSA). Its contents are solely the responsibility of the authors and do not
necessarily represent the official views of HRSA.
Disclaimer

Acknowledgments
Written by Rebecca Smith, MD
Curriculum Development & Review Committee:Grant Brenner, MDKristina Jones, MD
G Luke Larkin, MD, MS, MSPH, FACEPCraig L Katz, MD
Roger Nathaniel, MDCarol North, MD, MPEIlisse Perlmutter, MD

Why another course in psychosocial aspects of
bioterrorism?

OverviewDidactic - 20min Using the SARS epidemic, we’ll illustrate:
• Key psychosocial dimensions of a bioterrorist attack relevant to ED staff
• ED staff are at increased risk for being both victim and vector
• Communication between individuals, institutions and groups about risk appraisal
Cases – 50min• Applications to ED staff• Psychosocial preparedness & mental health issues • Development of risk communication – based
strategies for individuals and groups• Differentiation of acute presentations of severe
distress from diagnosis, Integration of psych first aid into routine care.

Emergency vs. Disaster
• As ED staff, you all handle the extraordinary, QD!• You always have capacity to handle the
extraordinary, right? But...• In disasters, needs exceed capacity, for ALL
systems, even the ED – Normal procedures insufficient.
• What will it be like for YOU to be in a situation where needs exceed capacity?

Core Competencies
1. Identify psychosocial vulnerabilities of ED Health Care Workers as first responders in BT attack & develop a plan for preparedness
2. Understand principles of risk communication & apply to communication with individuals & crowds
3. Differentiate distress v. diagnosis– Common post-disaster mental health myths– PTSD symptoms ≠ PTSD!
4. Integrate Psychological First Aid into care

Psychosocial Vulnerabilities of ED Health Care Workers
• ED Health Care Workers are First Responders for the nation, 24/7
• ED already a combat zone of austerity & overcrowding
• Increased Risk for Infection in EDVictim/Vector
• Big changes in work and home role

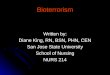
SARS timeline
ABCDEFGHIJKLM
Onset of symptoms Time stayed at Hotel M
February March4 531 624 25 26 227 2820 21 22 2315 16 17 18 19
Hotel MetropoleHong Kong
From Brendan Flannery, PhD, the CDC SARS Investigative Team

Hotel MHong Kong
Guangdong Province,
China A
A
H,J
A
H,J
Hong Kong SAR
95 HCW
>100 close contacts
United States
1 HCW
I, L,M
I,L,M
KIreland
0 HCWK
Singapore
34 HCW
37 close contacts
C,D,E
C,D,E
B
B
Vietnam
37 HCW
21 close contacts
F,G
Canada
18 HCWF,G
11 close contacts
SARS transmission:Health Care Workers & Families

Example: SARS8437 Probable Cases
China: 5327(Beijing: 2521)
(Guangdong: 1511)
H.K.: 1755
Viet Nam: 63
Singapore: 206
Canada: 250(Toronto: 242)
Taiwan: 671
As of July 11, 2003. Source: WHO

Isolation & Quarantine
• Both are methods of “community containment.”• Isolation: the separation of persons who have a
specific infectious illness from those who are healthy, and the restriction of their movement to stop the spread of disease.
• Quarantine: the separation and restriction of movement of persons who, while not yet ill, have been exposed to an infectious agent and therefore may become infectious.
• Both can be either voluntarily or compelled by public health authorities.

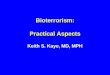
Toronto Outbreak, Spring 2003Paramedics on Quarantine
0
20
40
60
80
100
120
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39
Day of Outbreak
# o
f p
ara
me
dic
s
Total Staffperson-Days on Quarantine = 2035

2003 SARS Outbreak Acute Psychological Responses
• Patient reactions:– Isolation, loneliness, stigma– Anxiety associated with fever spikes– Fear and guilt about well-being of family/friends
– Insomnia
• Staff reactions:– Conflict between work & family responsibilities– Complexity of caring for other HCWs
– Diminished control, freedom, self-esteem
(Maunder et al, 2003)

Personal Preparedness Planning• You have a disaster plan at work. The hospital has one.
– Do you know it?• But do you have a disaster plan for yourself and your family?• What sorts of BT training & support are available for you in
your hospital or on the web?• Bioterrorism Literacy:
– What is ICS? – State and Hospital plans and policies re: Quarantine &
Isolation?• Psychosocial Literacy:
– What are your sources of resilience?– How do you actively cope?

Principles of Risk Communication: Treatment and Prophylaxis
for Anxiety and Panic1. Listen to, acknowledge, and respect the fears, anxieties and uncertainties:
- they want to know that you care before they care what you know.
2. Appear calm and in control, even in the face of public fear, anxiety and uncertainty; provide others with ways to participate, be constructive, channel their energy, and regain control.
3. Offer authentic statements of caring, empathy, compassion and listening; back up those statements with actions.
4. Be honest, ethical, frank, and open, recognizing that there are limits on what needs to be disclosed.
5. Avoid using humor; if humor is needed, plan and test carefully.

Principles of Risk Communication
6. Be hopeful so as to avoid fixation on the negative.- avoid the five N’s: no, not, never, nothing, none
7. When providing info or sharing bad news, be proactive but remember – Need 3 positives to balance 1 negative.
8. Avoid mixed or inconsistent verbal and non-verbal messages
9. Hone verbal & non-verbal media skills. - Avoid major media traps, guarantees, speculating on worst case
scenarios. Covello, 2004

Assessing Patients Psychological Assessment Principles
• What is known about the event, including its known scope, impact, and public health implications?
• Who is the person in front of me, including their personal, social, and psychological history as well as their connection to the disaster?
• When in the time course of the event is their ED visit occurring?
Katz, 2004

Acute Psychological Responses (intense but changeable)
• “Stunned”• “Shocked”• Anger at authority• Feeling abandoned• Uncommon vulnerability• Exaggerated rumors• Intense love / altruism• Heroism / Industry• Desperation
• Bewilderment• Fear• Impasse• Numbness• Apathy• Helplessness• Urgency• Discomfort• Confusion
(Wolfenstein, 1957)(Katz et al, 2002, 2004)

Bioterrorism and Mental Illness
• Acute Stress Disorder (can only diagnose within 30 days of trauma)
• Post Traumatic Stress Disorder (can only diagnose AFTER 30 days post-trauma)
• Major Depressive Episode/Disorder
• Panic Attack/Panic Disorder
• Generalized Anxiety Disorder

Assessing PatientsPsychological First Aid
• provide for basic needs (water, blankets, privacy)
• protect from further exposure – reduce environmental stimulation or agitation
• support the most distressed• keep families together & provide social support
– awareness of impact on entire family• provide information, foster communication and
education– orient to available services– use effective risk communication techniques

Web Resources
• www.cdc.gov “emergency preparedness” • www.bt.cdc.gov “cdc bioterrorism info”• www.nyc.gov/health/nycmed 1-888-NYCMED9• Health Alert Network, gives you emails on alerts”
from the NYS dept of health and mental hygiene Email: [email protected]
• CDC health alerts, learning modules • www.phppo.cdc.gov/han/