Embed Size (px)
Citation preview

Mental distress in the Danish generalpopulation
Olsen LR, Mortensen EL, Bech P. Mental distress in the Danish generalpopulation.
Objective: To present data on mental distress in the Danish generalpopulation using recently validated Hopkins symptom checklist(SCL) subscales and compare with data from other countries. Toevaluate associations between mental distress and biopsychosocialfactors.Method: Questionnaires were sent to a gender- and age-stratifiedrandom sample comprising 2040 Danes. Mean SCL subscale scoreswere calculated. Cases were defined in accordance with the traditionalcriteria, and Danish and US raw score cut-offs were compared. Amultiple regression model was developed to describe associationsbetween biopsychosocial factors and SCL scores.Results: The response rate was 58%. The Danish mean scores weresignificantly higher than reported for a US non-patient sample, andDanish raw score cut-offs for caseness were higher. The Danish scoreswere closer to Nordic mean scores. Age, gender, social status, somaticdisorder and traumatic life events in the past year in work life as well aspersonal life were significantly associated with the level of mentaldistress. SCL scores were compared with scores on the MajorDepression Inventory.Conclusion: The SCL mean scores of the Danish general populationwere relatively high, but similar to data from the Nordic countries.Consequently, interpretation of the Danish SCL requires Danishnorms and Danish cut-off scores for caseness.
L. R. Olsen1, E. L. Mortensen2,P. Bech11Psychiatric Research Unit, Frederiksborg GeneralHospital, Hilleroed and 2Department of HealthPsychology, Institute of Public Health, University ofCopenhagen, Copenhagen, Denmark
Key words: epidemiology; questionnaire; stress,psychological
Lis Raabaek Olsen, Roersangervej 16, DK-2600 Glostrup,Denmark.E-mail: [email protected]
Accepted for publication November 30, 2005
Significant outcomes
• Normative data on mental distress in the Danish general population now exist.• Biological, psychological and social factors all have an impact on Hopkins symptom checklist (SCL)
mean scores.• The SCL can be used as a screening instrument for major depression.
Limitations
• These normative data only represents the Danish general population.• The analysis of biopsychosocial factors is cross-sectional.• The SCL score should not be used as a psychiatric diagnostic instrument on its own.
Introduction
Mental distress is frequently used as an outcomemeasure in medical and psychological research. Itmay be defined as an individual’s level of mental
complaints and symptoms. Self-report question-naires are widely used to assess mental distressbecause they directly reflect the experience andsymptoms of the individual. The most extensivelyused self-report questionnaire measuring mental
Acta Psychiatr Scand 2006: 113: 477–484All rights reservedDOI: 10.1111/j.1600-0447.2005.00743.x
Copyright � 2006 The AuthorsJournal Compilation � 2006 Blackwell Munksgaard
ACTA PSYCHIATRICASCANDINAVICA
477

distress seems to be the Hopkins Symptom Check-list (SCL-90) (1). It has been used during the past50 years as an outcome measure in studies evalu-ating the effects of medical, psychopharmacologi-cal and psychotherapeutic treatment.The SCL-90 differs from most other question-
naires in this field by measuring both distressexpressed inwards (depression, somatization andanxiety) and distress expressed outwards (aggres-sion, impulsivity and psychoticism), while mostother scales focus only on distress expressedinwards. In contrast to the General Health Ques-tionnaire (2) which only covers one single dimen-sion, the SCL-90 is claimed to cover nine differentdimensions of mental distress: somatization, inter-personal sensitivity, depression, anxiety, phobicanxiety, obsession–compulsion, hostility, paranoidideation and psychoticism. It is not a diagnosticinstrument or a personality inventory, but aninstrument from which both a symptom profileand a general distress score can be derived.Psychiatric disorder and personality characteristicswill, however, influence the SCL-90 symptomprofile and general distress level.The SCL-90 algorithm for the definition of cases
is based on the Global Severity Index (GSI) andcomparison with national norms (3). This is incontrast to DSM-IV (4) or ICD-10 (5) diagnosticclassification that is based on diagnostic symptomcriteria and not on comparison of quantitativemeasures of general distress and symptom severitywith population norms. Thus, the purpose of theSCL-90 cut-off for caseness is to indicate thedemarcation between normal distress and clinicalcases (e.g. clinical anxiety or depression). Asdiscussed by van Praag et al. (6) it is importantwhen measuring stress-related biological factorsand hormones to refer to quantitative mentaldistress dimensions covering the zone betweennormal stress-reaction and pathological levels ofdepressive illness. In the present study, the SCL iscompared with an indicator of depression, theMajor Depression Inventory (MDI).When a questionnaire is used in different coun-
tries, both translation problems and culturaldifferences may affect score distributions (7), andconsequently normative data are needed for eachculture and language. However, in many SCLstudies results have been compared with the USnormative data collected at least 30 years ago (4) –even though SCL scores have been demonstratedto be influenced by e.g. cultural setting (8). Animportant goal of the present study was to presentnormative SCL data for the Danish general pop-ulation and to analyse how SCL scores are affectedby a broad spectrum of biological, psychological
and social factors. A previous population studypresented Danish normative data for the SF-36 (9),but no studies in the Danish general populationhave focused on degree of mental distress anddetailed description of mental symptoms.
Aims of the study
To present Danish normative data on mentaldistress, as evaluated by SCL, and to comparelevel of symptoms and raw score cut-offs forcaseness between various countries. To evaluatethe associations between degree of mental distressand biological, psychological and social factors,and to evaluate the relationship between SCLscores and major depression (as defined by theMDI).
Material and methods
Sample
The age- and gender-stratified sample included2040 Danish citizens drawn randomly from TheCivil Registration System in Denmark. The samplecomprised 17 men and 17 women born in eachyear in the period 1920–1979 (i.e. aged 20–79 years). The data were collected in April 2000using a mailed questionnaire booklet. Participationwas anonymous, as there was no name or otheridentification code on the booklet. A number onthe return envelope made it possible to identifyresponders and non-responders. The latter receiveda reminder twice, and after the second reminder allnames and addresses were destroyed. Booklets andenvelopes were separated immediately after receipt.The local Ethical Committee method accepted thismethod of ensuring anonymity.Data from this sample on other variables inclu-
ded in the mailed questionnaire booklet have beenreported elsewhere (10).
SCL-92
The most commonly used version of the question-naire comprises 90 items, but two competingversions exist, as Derogatis replaced two itemsfrom the original SCL-90 anxiety subscale with twonew items and called the revised version SCL-90-R(3). The SCL-92 version used in this study is acombination of the SCL-90 and SCL-90-R com-prising all 92 items from the two versions. Byinterchanging the two anxiety items from theanxiety subscale, this version may either bescored corresponding to the SCL-90 or to theSCL-90-R. The merged version of SCL-92 used in
Olsen et al.
478

the present study has been translated into Danishin accordance with international rules (1). Thevalidity of the SCL-92 has previously been dem-onstrated by Mokken–Loevinger analysis andRasch analysis (1).The items on the scale are rated on a five-point
Likert scale ranging from 0 (not at all) to 4(extremely). The time frame is the past week.Besides the nine subscales, the global total score
(3) covering all 92 items constitutes a GSI. Itemresponse analyses have demonstrated that the GSIdoes not reflect one single dimension, but that thisis the case for 63 non-psychotic items, i.e. soma-tization, obsession–compulsion, interpersonal sen-sitivity, depression, anxiety and phobic anxiety (1).In this paper, data will be presented for both thetraditional index (GSI-92) and the unidimensionalGSI-63 index.In the present study, cases were defined accord-
ing to Derogatis criteria (4), i.e. either a GSI score,or two or more subscale scores at or above aT-score of 63: cases ¼ TGSI > T63 or T2DIM >T63. This was recently shown to be the best cut-offscore for cases, giving 90% correct classification(11).
Potential determinants of distress
Sociodemographic factors Sociodemographic varia-bles (gender, age, school education, professionaleducation, yearly personal income and yearlyhousehold income) were registered. An index forsocial status was calculated based on schooleducation, profession and yearly householdincome. Each variable was coded from 1 to 5,and the average of these three re-coded variableswas used as index for social status.
Health status Somatic diseases were registered by achecklist including 24 of the most common somaticdiseases; each participant had to indicate whetherhe/she currently suffered from the disease, wascurrently treated by a medical doctor for thedisease or had ever been hospitalized for thedisease. Diseases were dichotomized as absent orpresent (having at least one somatic disease).
Life events Questions about traumatic life eventsover the past year included five work relatedquestions (unemployment, not being promoted,conflicts with colleagues, superiors or subordinates)and seven questions related to events in the family(children severely ill, severe educational problemsfor children, severe conflicts with grown-upchildren, severe problems in marriage, own severeillness, severe illness or death among relatives, severe
economical problems). These questions were modi-fied from the questions used in the CopenhagenCity Heart Study (12). Traumatic events in the pastyear with regard to personal life and traumaticevents in the past year with regard to work weredichotomized as present or absent, being presentwhen at least one traumatic event with regard topersonal or work life, respectively, had occurred.
Major Depression Inventory
TheMDI scale contains the symptoms of depressioncovered by the ICD-10 as well as the DSM-IVdiagnostic systems. On a six-point Likert scale, theindividual items measure how much of the time thesymptoms have been present during the past14 days. This is indicated on a scale from 0 (thesymptom has not been present at all) to 5 (thesymptom has been present all of the time). TheMDIis scored according to the guidelines describedelsewhere (13). A diagnosis of major depression(DSM-IV), or mild, moderate or severe depression(ICD-10), can be extracted from the scores.The MDI can also be scored as a scale measuring
severity of depressive states. In this case, the totalscore of the 10 items is calculated, and conse-quently the theoretical score range is from 0 (nodepression) to 50 (extreme depression) (14).In previous studies, we successfully tested the
MDI scale for applicability and external validity bymeans of sensitivity (true positive rate) and specif-icity (true negative rate) when using SCAN (TheSchedules for Clinical Assessment in Neuropsychi-atry) as the gold standard; a sensitivity of 0.86 anda specificity of 0.86 was found (13). In addition,correspondence with the Hamilton DepressionScale was investigated (14). A Hamilton score of13 corresponded to 20.9 (95% CI 19.4–22.3) on theMDI, a Hamilton score of 18 corresponded to 27.1(95% CI 25.8–28.5) on the MDI, and a Hamiltonscore of 25 corresponded to 35.9 (95% CI 34.0–37.8) on the MDI.Moreover, we have tested the internal consis-
tency by use of Cronbach’s coefficient alpha, anddimensionality and homogeneity by use of Raschanalyses and Mokkens analysis (13, 14).In clinical research, it was shown that the MDI is
useful as a diagnostic tool and as an outcomemeasure for antidepressant treatment (15, 16).
Statistical analysis
The sample was divided into four age groups (19–34, 35–49, 50–64 and 65–79 years). Mean scoresfor the individual subscales of the SCL-92, the GSIand the GSI-63 (the GSI based on the 63-item
Mental distress in Danish population
479

non-psychotic scale) were calculated for genderand age sub-groups and analysed by 2 · 4 anova
(gender and four age groups).Mean scores were compared with data from
other studies by anova/t-test. Furthermore, effectsizes by means of Cohens d (17) were calculated,using SD for the Danish sample as standard.Unlike significance tests, these indices are inde-pendent of sample size.Following the US manual (3), normalized and
standardized T-scores with a mean of 50 and astandard deviation of 10 were derived. In addition,raw score cut-offs for caseness were defined as theraw score corresponding to a T-score of 63. Thenumber of cases based on Danish cut-offs wascompared with the number of cases based on theUS cut-offs [raw scores corresponding to T-scoreof 63 in the US standardization sample describedby Derogatis (3)]. Tests of differences betweencorrelated proportions for each of the four agegroups within each gender were used to test thedifferences in the number of cases based on Danishand US cut-offs.Age, gender, social status, personal life events,
work life events and somatic disease were analysedas potential determinants of distress and mentalsymptoms. First, bivariate associations betweenthe SCL scales and the potential determinants wereanalysed and then all six variables were included inmultiple linear regression model predicting eachSCL scale.Pearson correlations were calculated to estimate
correlations among the anxiety scales and GSIindex of the SCL-92, SCL-90 and the SCL-90-R.The Pearson correlation was also calculated
between the GSI and the MDI total score. Inaddition, optimal cut-off scores for depression wereestimated for SCL-92, SCL-63 and the depressionsubscale by using the diagnosis of major depressionaccording to the MDI as reference. The ReceiverOperating Characteristic curve was used for esti-
mating the optimal cut-off score giving the highestsensitivity and specificity.
Results
Of the 2040 individuals in the sample, 39 partic-ipants were lost because of incorrect address,hospitalization or institutionalization. The SCL-92 was completed by 1152 participants, i.e. aresponse rate of 58%. The final sample had analmost equal representation of men and women(54% women). As the original sample consisted ofequal-sized age strata, the age distribution is not,and was not expected to be, comparable with thatof the total Danish population (see Table 1).However, because of slightly different responserates for gender and age subgroups, the gender andage distribution of the final sample was moresimilar to the year 2000 Danish population thanmight be expected from the sampling criteria (18).Thus, females and younger age groups comprised alarger proportion of the sample as they do in theDanish population.Table 1 shows the raw mean scores for the
different subscales, the GSI-63, and the GSI-92 forthe total sample and separately for each gender aswell as for the four age subgroups. The femalemean scores were statistically significantly higherthan the male mean scores for somatization,interpersonal sensitivity, depression and anxietysubscales, GSI-63 and GSI-92. When controllingfor gender, somatization was positively associatedwith age while interpersonal sensitivity, hostilityand paranoid ideation were negatively associatedwith age. Neither the GSI-63 nor the GSI-92 meanscores were significantly associated with age. anovarevealed no significant interactions between genderand age for any SCL scale.The Danish mean scores were compared with
international data from the US (3), Norway (19)and Finland (20). The Danish mean scores for GSI
Table 1. Mean (SD) scores of mental distress in the Danish general population
Age group (years) SOM OC IS DEP ANX HOS PHOB PAR PSY 63-item GSI
Females (n ¼ 620)19–34 (n ¼ 165) 0.47 (0.52) 0.67 (0.63) 0.76 (0.66) 0.73 (0.70) 0.49 (0.57) 0.45 (0.53) 0.15 (0.38) 0.53 (0.67) 0.28 (0.39) 0.55 (0.50) 0.53 (0.48)35–49 (n ¼ 184) 0.56 (0.62) 0.63 (0.62) 0.59 (0.54) 0.70 (0.70) 0.52 (0.52) 0.40 (0.41) 0.11 (0.30) 0.49 (0.61) 0.21 (0.32) 0.52 (0.48) 0.50 (0.46)50–64 (n ¼ 150) 0.56 (0.57) 0.66 (0.64) 0.56 (0.62) 0.63 (0.66) 0.46 (0.55) 0.30 (0.37) 0.15 (0.38) 0.43 (0.59) 0.21 (0.32) 0.50 (0.51) 0.47 (0.47)65–80 (n ¼ 121) 0.69 (0.58) 0.69 (0.66) 0.44 (0.49) 0.58 (0.58) 0.42 (0.51) 0.24 (0.29) 0.20 (0.36) 0.33 (0.43) 0.19 (0.29) 0.50 (0.46) 0.47 (0.42)
Males (n ¼ 532)19–34 (n ¼ 121) 0.33 (0.36) 0.59 (0.54) 0.53 (0.53) 0.52 (0.62) 0.39 (0.38) 0.34 (0.41) 0.01 (0.24) 0.55 (0.61) 0.21 (0.28) 0.41 (0.38) 0,40 (0.37)35–49 (n ¼ 133) 0.43 (0.48) 0.55 (0.55) 0.48 (0.53) 0.51 (0.61) 0.45 (0.50) 0.36 (0.45) 0.01 (0.22) 0.49 (0.57) 0.21 (0.32) 0.42 (0.42) 0.42 (0.41)50–64 (n ¼ 135) 0.42 (0.44) 0.55 (0.58) 0.45 (0.48) 0.46 (0.53) 0.37 (0.47) 0.24 (0.30) 0.12 (0.29) 0.46 (0.57) 0.19 (0.29) 0.39 (0.41) 0.38 (0.38)65–80 (n ¼ 143) 0.48 (0.53) 0.69 (0.63) 0.45 (0.54) 0.53 (0.56) 0.36 (0.50) 0.31 (0.37) 0.16 (0.44) 0.39 (0.55) 0.21 (0.30) 0.45 (0.47) 0.42 (0.43)
Total (n ¼ 1152) 0.49 (0.53) 0.63 (0.61) 0.54 (0.56) 0.59 (0.63) 0.44 (0.51) 0.34 (0.41) 0.13 (0.34) 0.46 (0.59) 0.22 (0.32) 0.47 (0.46) 0.45 (0.43)
SOM, somatization; OC, obsession/compulsion; IS, interpersonal sensitivity; DEP, depression; ANX, anxiety; HOS, hostility; PHOB, phobic anxiety; PAR, paranoid ideation; PSY,psychoticism; 63-item, total score for the non-psychotic subscales; GSI, Global Severity Index.
Olsen et al.
480

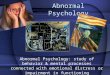
were higher than the US (anova, P < 0.0001), thedifference was statistically significant for all of thesubscales as well (P < 0.05) except for the subscaleof phobic anxiety. The Danish mean scores for GSIwere closer to but still higher than the Norwegiandata (P < 0.01); the difference was statisticallysignificant for the subscales (P < 0.05) exceptphobic anxiety and hostility. The Danish GSImean scores were lower than the Finnish scores,anova (P < 0.0001), and the difference was alsostatistically significant for all subscales (P < 0.05)except paranoid ideation. Effect sizes by means ofCohens d were for the US sample in the range0.20–0.45, for the Finnish sample in the range0.18–0.59. This should be interpreted as small tomoderate effect sizes (17).For visual comparison, Danish SCL-90-R data
vs. US, Norwegian and Finnish normative data areshown as a graph (Fig. 1).T-scores were calculated and raw score cut-offs
derived to estimate the number of cases. In total,17.5% of the Danish sample was classified as cases.Comparison of raw score cut-offs from the presentstudy with the raw score cut-offs set by Derogatis(3) based on T-scores from a sample of US maleand female non-patients is shown in Table 2. Thepercentage of cases in the Danish sample ispresented in Table 3 for gender and age subgroups.
Bivariate analyses showed that age and genderwere significantly associated with a number of SCLscales while social status was associated with allscales except hostility. Traumatic life events inpersonal and work life and somatic disease weresignificantly associated with all SCL scales.Table 4 presents the results for a multiple linear
regression model that included all six variables.The table shows that between 7% and 17% of thevariance of each SCL scale is explained by themodel. The table also shows partial correlationsbetween each SCL scale and the six predictorvariables. For life events, significant partial corre-lations were observed for all scales, while socialstatus and somatic disease were significantly asso-ciated with most SCL scales. Age was significantly
SCL-90-R DK versus US. N and SF
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
SOM O - S
I - S
DEPANX
HOS
PHOBPAR
PSYGSI
SCL-90-R
Mea
n s
core
Denmark DK America US Norway N Finland SF
DK
SF
N
US
Fig. 1. SCL-90-R data from the Danish general population(n ¼ 1.153) vs. US normative data (n ¼ 974) (1), Norwegiannormative data (n ¼ 973) (17) and Finnish normative data(n ¼ 337) (18).
Table 2. Raw score cut-offs for caseness (based on T-score ¼ 63) on the indi-vidual subscales (dimensions) and global score (GSI) based on data from thepresent study (Danish) versus data from Derogatis� non-patient population (1) (US)
Danish US
FemalesSOM 1.29 1.07OC 1.53 1.05IS 1.39 0.93DEP 1.60 1.13ANX 1.15 0.91HOS 0.85 0.83PHOB 0.34 0.58PAR 1.18 0.93PSY 0.66 0.44GSI 1.08 0.80
MalesSOM 0.97 0.70OC 1.36 0.93IS 1.11 0.68DEP 1.29 0.72ANX 0.94 0.54HOS 0.76 0.76PHOB 0.20 0.30PAR 1.25 0.91PSY 0.55 0.44GSI 0.87 0.58
SOM, somatization; OC, obsession/compulsion; IS, interpersonal sensitivity; DEP,depression; ANX, anxiety; HOS, hostility; PHOB, phobic anxiety; PAR, paranoidideation; PSY, psychoticism; GSI, Global Severity Index.
Table 3. Number of cases in the various age and gender groups based on the rawscore cut-offs for caseness from Table 2, case definition: TGSI > T63 orT2DIM > T63 (1)
Age group (years)
Females (n ¼ 605) Males (n ¼ 531)
Danish US Danish US
19–34 21.2 35.2* 18.2 35.5*35–49 16.9 27.9* 19.5 35.3*50–64 17.8 26.7* 14.9 33.6*65–79 14.4 26.1* 16.1 32.9*Total 17.9 29.3* 17.1 34.4*
All values are in percentage.*P < 0.0001 (tests of differences between correlated proportions).
Mental distress in Danish population
481

associated with a number of subscales and the twoGSI scores while only the depression subscale wasstrongly associated with gender, indicating higherscores in women than in men.When focusing on caseness as the dependent
variable, a logistic regression model consisting ofsomatic disorder, traumatic life events in the familyand traumatic life events in work life showed to besignificant. Odds ratios for caseness were forsomatic disorder 1.5 (95% CI 1.1; 2.2), for trau-matic disorder in the past year, personal life, 1.8(95% CI 1.3; 2.5), and for traumatic events in thepast year, work life, 2.1 (95% CI 1.5; 3.1).The correlation between the MDI total score
and GSI was 0.83, P < 0.0001.Cut-off scores for major depression are presen-
ted in Table 5.The correlation between the anxiety scale of the
SCL-92 and the anxiety scale of both the SCL-90and the SCL-90-R was 0.99 while the correlationbetween the anxiety scales of the SCL-90 and theSCL-90-R was 0.98. The intercorrelations of theGSI index were 1.00 among all three SCL versions,and all three GSI index correlated 0.99 with theSCL-63 GSI index.
Discussion
This study has made Danish normative data for theSCL available. As this is the first Danish SCL-90
study of the general population, no comparabledata exist. However, compared with US data, thescores are somewhat higher, indicating the import-ance of national normative data. The possibilitythat symptom and distress levels are actuallyhigher in Denmark than that in the USA whenthe US SCL data were collected cannot be com-pletely disregarded, but we believe that severalother factors may explain the difference betweenthe SCL data from the two countries: the selectionof the US non-patient sample is not described indetail and few sociodemographic data are availableand the sample was not selected from the wholecountry but was a stratified random sample from alarge Eastern state (3). Thus, the higher DanishSCL scores may reflect sample differences, trans-lation factors, cultural differences or differenceswith respect to epoch, and the relatively highDanish scores are not strong evidence of highdistress level in the Danish general population. TheDanish scores are only slightly higher than com-parable Norwegian scores. The Finnish scores areeven higher than the Danish, presumably becausethe timeframe used is a year and not a week (20).The Finnish sample had an over-representation offemales while the US non-patient sample includedmore males than the Danish sample. Althoughmales consistently obtain lower scores than females(20), the relatively small difference in sex ratio(50% vs. 46%) cannot alone explain the differencesbetween Danish and US non-patient scores (thelargest effect sizes were approaching half a SD).Assuming that symptom and distress levels are
similar in the Danish and US non-patient samplesthis study demonstrates the importance of usingrelevant SCL data for defining cases. Thus, theprevalence of cases was up to twice as high whenapplying US raw score cut-offs to the Danishsample, indicating that the use of inappropriatenormative data may lead to incorrect conclusions
Table 4. Partial correlations and explained variancefor each SCL scale in a linear regression model withsix predictorsAge Gender
Socialstatus
Work relatedlife events
Family relatedlife events Somatic disorder
Explainedvariance (R2)
SOM )0.02 )0.12*** )0.18*** 0.11*** 0.18*** 0.22*** 0.16OC )0.04 )0.04 )0.15*** 0.07* 0.17*** 0.10** 0.08IS )0.17*** )0.09** )0.16*** 0.13*** 0.12*** 0.07* 0.09DEP )0.09** )0.12*** )0.13*** 0.12*** 0.19*** 0.09* 0.10ANX )0.08** )0.07* )0.11*** 0.13*** 0.16*** 0.10*** 0.08HOS )0.15*** )0.04 )0.10*** 0.13*** 0.13*** 0.07* 0.07PHOB )0.00 )0.04 )0.14*** 0.12*** 0.08* 0.04 0.05PAR )0.14*** )0.03 )0.17*** 0.23*** 0.13*** 0.09** 0.12PSY )0.12*** )0.01 )0.16*** 0.09** 0.14*** 0.08** 0.07GSI SCL-92 )0.09** )0.09** )0.17*** 0.14*** 0.18*** 0.12*** 0.12GSI SCL-63 )0.08** )0.09** )0.17*** 0.13*** 0.18*** 0.12*** 0.11
SOM, somatization; OC, obsession/compulsion; IS, interpersonal sensitivity; DEP, depression; ANX, anxiety; HOS,hostility; PHOB, phobic anxiety; PAR, paranoid ideation; PSY, psychoticism; 63-item, total score for the non-psychoticsubscales; GSI, Global Severity Index; SCL, Hopkins symptom checklist. *P < 0.05, **P < 0.01, ***P < 0.001. For allSCL scales the explained variance (R2) is significant at P < 0.0001.
Table 5. Raw score cut-offs for major depression (in accordance with MDI, DSM-IV diagnosis) on the SCL-scales, and corresponding sensitivity and specificity
Cut-off score Sensitivity Specificity
SCL-92 0.90 0.85 0.90SCL-63 1.00 0.82 0.91SCL DEP-scale 1.77 0.79 0.96
MDI, Major Depression Inventory; SCL, Hopkins symptom checklist; DEP, depres-sion.
Olsen et al.
482

about the level of mental distress. Clearly, the rawscore cut-offs as stated in Table 3 should be usedwhen the SCL-92 is used as a screening instrumentin Denmark.The intercorrelations among the anxiety scales
and GSI index of the three SCL-versions indicatethat the choice of SCL version will rarely – if ever –make a significant difference and that this also isthe case with respect to the choice between theGSI-63 and the traditional GSI index based on allavailable items. Thus, findings from studies usingone SCL version can be compared with studiesusing one of the two other versions.Age, gender, and social status were observed to
be significant predictors of the GSI-63 and theGSI-92. Age was a significant, but relatively weakpredictor of the overall distress level, but signifi-cant and stronger negative associations wereobserved for several subscales. Although theassociation with somatization was only significantwhen age was categorized into four groups andonly when adjusted for gender, it seems reasonableto expect more somatic complaints in older people.Older people may also be expected to be less hostileand in particular less sensitive in interpersonalrelations (21). Females obtained higher meanscores than males on a number of subscales, inparticular on the depression subscale, and thesegender differences on subscales are the backgroundfor the overall higher distress scores in females(GSI-63 and GSI-92). Significant inverse associa-tions with social status were observed for all SCLscores except the anxiety scale, demonstrating asocial gradient with respect to distress and mentalsymptoms in the Danish population.Traumatic life events in personal and work life
were strong predictors of all SCL scores, andsomatic disorder was also significantly associatedwith most SCL scores (except phobic anxiety).When focusing on caseness, the same predictorswere seen. The traumatic life events included inthis study cover common life events and notcatastrophic events typically associated with adiagnosis of post-traumatic stress disorder(PTSD). Most studies have either focused on theimpact of PTSD (22) or the impact of lifetimeevents (23) on distress level. Our study has focusedon traumatic events in the past year, including worklife as well as personal life. Events from both areaswere associated with the observed level of symp-toms and distress, and this demonstrates that theSCL scales are sensitive to the effects of negative lifeevents that have affected the individual relativelyrecently. The fact that social status, life eventsduring the past year and somatic disease wereassociated with scores on most SCL scales is not
unexpected because of the previously reported highintercorrelations among the scales (1).Mean scores on the MDI was found to be highly
correlated to scores on the SCL, and Table 5demonstrates relatively high sensitivity and specif-icity for empirically derived SCL cut-off scores.Although the SCL is not a diagnostic tool, thefigures suggest that it may be used as a screeninginstrument for depression.In conclusion, we have presented data from the
Danish general population on the level of mentaldistress and mental symptoms as measured by theSCL-92. These data are important for futureclinical research serving as normative data andcan be used for comparisons with studies in othercultural settings. The outcome of various treatmentstrategies can be evaluated not only by analysingchanges from baseline to follow-up, but also by thepercentages of patients moving from above tobelow the SCL cut-off values for caseness (24). Theusefulness of the SCL as a screening instrument formajor depression was demonstrated.
References
1. Olsen LR, Mortensen EL, Bech P. The SCL-90 and SCL-90R versions validated by item response models in aDanish community sample. Acta Psychiatr Scand2004;110:225–229.
2. Goldberg DP, Hillier VF. A scaled version of the GeneralHealth Questionnaire. Psychol Med 1979;9:139–145.
3. Derogatis LR. SCL-90-R: Symptom Checklist-90-R.Administration, scoring and procedures manual, 3rd edn.Minneapolis, Minnesota: National computer systems,1994.
4. American Psychiatric Association. Diagnosis and statisti-cal manual of mental disorders (DSM-IV), 4th edn.Washington, District of Columbia: American PsychiatricAssociation, 1994.
5. World Health Organization. The ICD-10 classification ofmental and behavioural disorders. Diagnostic criteria forresearch. Geneva: WHO, 1983.
6. van Praag HM, de Kloet R, van Os J. Stress, the brain anddepression. Cambridge: Cambridge University Press, 2004.
7. Simonsen E, Mortensen EL. Difficulties in translation ofpersonality scales. J Personal Disord 1990;4:290–296.
8. Barker-Collo SL. Culture and validity of the SymptomChecklist-90-Revised and profile of mood states in a NewZealand student sample. Cultur Divers Ethnic MinorPsychol 2003;9:185–196.
9. Bjorner JB, Damsgaard MT, Watt T, Groenvold M. Tests ofdata quality, scaling assumptions, and reliability of theDanish SF-36. J Clin Epidemiol 1998;51:1001–1011.
10. Olsen LR, Mortensen EL, Bech P. Prevalence of majordepression and stress indicators in the Danish generalpopulation. Acta Psychiatr Scand 2004;109:96–103.
11. Pedersen G, Karterud S. Is SCL-90R helpful for the clini-cian in assessing DSM-IV symptom disorders? Acta Psy-chiatr Scand 2004;110:215–224.
12. SethiAA,NordestgaardBG,Agerholm-LarsenB,FrandsenE,Jensen G, Tybjerg-Hansen A. Angiotensinogen polymor-phisms and elevated blood pressure in the general
Mental distress in Danish population
483

population: the Copenhagen City Heart Study. Hyperten-sion 2001;37:875–881.
13. Bech P, Rasmussen N-A, Raabæk Olsen L, Noerholm V,Abildgaard W. The sensitivity and specificity of the MajorDepression Inventory using the present state examinationas the index of diagnostic validity. J Affect Disord2001;66:159–164.
14. Olsen LR, Jensen DV, Noerholm V, Martiny K, Bech P. Theinternal and external validity of the Major DepressionInventory in measuring severity of depression. PsycholMed 2003;33:351–356.
15. Sorensen C, Brandes A, Hendricks O et al. Psychosocialpredictors of depression in patients with acute coronarysyndrome. Acta Psychiatr Scand 2005;111:116–124.
16. Martiny K, Lunde M, Unden M, Dam H, Bech P. Adjunctivebright light in non-seasonal major depression: results frompatient-reported symptom and well-being scales. ActaPsychiatr Scand 2005;111:453–459.
17. Cohen J. Statistical power analysis for the behavioral sci-ences, 2nd edn. Hillsdale, New Jersey: Lawrence EarlbaumAssociates, 1988.
18. Statistics Denmark StatBank Denmark. Population andelections. BEFIA (WWW document). Available at: http://www.statistikbanken.dk/BEF1A/
19. Vassendt O, Lian L, Andersen HT. Norwegian versions ofthe NEO-Personality Inventory, Symptom Checklist 90Revised, and Giessen Subjective Complaints List. Part 1.Tidsskrift for Norsk Psykologforening 1992;29:1150–1160.
20. Holi MM, Sammallathi PR, Aalberg VA. A Finnish valid-ation study of the SCL-90. Acta Psychiatr Scand1998;97:42–46.
21. Lavie CJ, Milani RV. Impact of aging on hostility in cor-onary patients and effects of cardiac rehabilitation andexercise training in elderly persons. Am J Geriatr Cardiol2004;3:125–130.
22. Ursano RJ, Fullerton CS, Vance K, Kao TC. Posttraumaticstress disorder and identification in disaster workers. Am JPsychiatry 1999;156:353–359.
23. Amir M, Lev-Wiesel R. Time does not heal all wounds:quality of life and psychological distress of people whosurvived the holocaust as children 55 years later. J TraumaStress 2003;16:295–299.
24. Rasmussen N-A, Schroeder P, Olsen LR, Broedsgaard M,Unden M, Bech P. Modafinil augmentation in depressedpatients with partial response to antidepressants: a pilotstudy on self-reported symptoms covered by the MajorDepression Inventory (MDI) and the Symptom Checklist(SCL-92). Nordic J Psychiatry 2005;59:173–178.
Olsen et al.
484














![MENTAL DISTRESS DAMAGES FOR B CONTRACT D W McLauchlan "Mental Distress Damages for Breach of ... (1875) LR 10 QB 111, 122, Blackburn J. 14 Hadley v ... 16 Jarvis v Swan Tours Ltd [1973]](https://img.pdfslide.us/doc/110x75/5ae70d147f8b9a9e5d8e8bf3/mental-distress-damages-for-b-contract-d-w-mclauchlan-mental-distress-damages-for.jpg)