Embed Size (px)
Citation preview
Anne Kjersti Myhrene Steffenak
DISSERTATION | Karlstad University Studies | 2014:2
Nursing Science
Faculty of Health, Science and Technology
Mental Distress and Psychotropic Drug Use among Young People, and Public Health Nurses` Conceptions of Their Roles
DISSERTATION | Karlstad University Studies | 2014:2
Mental Distress and Psychotropic Drug Use among Young People, and Public Health Nurses` Conceptions of Their Roles
Anne Kjersti Myhrene Steffenak
urn:nbn:se:kau:diva-30600
Distribution:Karlstad University Faculty of Health, Science and TechnologyDepartment of Health SciencesSE-651 88 Karlstad, Sweden+46 54 700 10 00
© The author
ISBN 978-91-7063-531-1
Print: Universitetstryckeriet, Karlstad 2013
ISSN 1403-8099
Karlstad University Studies | 2014:2
DISSERTATION
Anne Kjersti Myhrene Steffenak
Mental Distress and Psychotropic Drug Use among Young People, and Public Health Nurses` Conceptions of Their Roles
WWW.KAU.SE

3
Abstract
Mental Distress, and Psychotropic Drug Use among Young People, and Public Health Nurses’ Conceptions of Their Roles
Aim: The overall aim of this thesis was to study mental distress, health and lifestyle habits, social factors and psychotropic drug use by young people, and how PHNs conceive their roles in relation to this.
Methods: Quantitative and qualitative methods were used. Study I included data from the Norwegian Youth Health Study (NYHS, 11 947 participants, aged 15-16 years) (2000–2003) linked to the Norwegian Prescription Database (NorPD) (2004–2009). Study II included prescription data on psychotropic drugs among 15-16 year olds from the NorPD (2006–2010). Eight young people were interviewed and qualitative content analysis was used to analyse the data (III). Study IV included interviews with 20 Public Health Nurses (PHN), and was analysed using a phenomenographic approach.
Main results: Mental distress was reported among 15.5% of the adolescents non-users of psychotropic drugs, 75% of whom were girls. In both genders reporting mental distress, incident psychotropic use was higher one to nine years, up to 27.7% among girls, as compared with the rest of the participants. In addition, health, lifestyle habits and social factors were associated with incident use (I). Psychotropic drug use increased during 2006–2010, hypnotics and melatonin accounted for most of the increase. In total, 16.4% of all incident psychotropic drug users in 2007 were still having prescriptions dispensed in 2010 (II). Young people experience both beneficial and undesired effects from psychotropic drugs. Access to professional support and follow-up was experienced as insufficient. Life with family, friends, school and work was influenced by psychotropic drug use, and they were afraid of being lonely and stigmatized (III). The PHNs conceived their roles in relation to young people as; the discovering PHNs who became aware of psychotropic drug use in the health dialogues and chose either to act or not to act in relation to this. Those PHNs who took action continued to be the cooperating PHNs who cooperated with the young people, their families, schools, and others. If cooperation was established, the supporting PHNs teach and support the young people in relation to psychotropic drug use (IV).
Conclusions: Attention must be paid to poor mental health and increasing psychotropic drug use by young people. Advances in knowledge, treatment and follow-up is needed. The prevalence of mental distress among young people, with differences between the genders, as well as between socioeconomic groups, should have consequences for health promotion strategies. PHNs in Norway, working in health centres and schools, have responsibility and opportunity to identify and follow-up young people with mental health problems.
Key Words: Adolescents, young people, mental distress, mental health problems, psychotropic drug use, public health nurse

4
Sammendrag
Psykiske lidelser og psykofarmakabruk blant ungdom og helsesøstres oppfatning av sine roller knyttet til dette
Hensikt. Avhandlingens overordnede hensikt var å studere psykiske lidelser, helse- og livsstilsvaner, sosiale faktorer og psykofarmakabruk blant ungdom og helsesøstres oppfatning av egne roller.
Metode. Kvantitative og kvalitative metoder ble brukt. Studie I inkluderte data fra Ungdomsundersøkelsen (11 947 deltakere, 15-16 år) (2000–2003) som ble koblet til Norsk reseptbasert legemiddelregister (2004–2009). Studie II inkluderte foreskrivningsdata på psykofarmaka blant 15-16 åringer fra Norsk reseptbasert legemiddelregister (2006–2010). I studie III ble åtte ungdommer intervjuet, og materialet ble analysert ved hjelp av en kvalitativ innholdsanalyse. Studie IV inkluderte intervju med tyve helsesøstre, og ble analysert ved bruk av en fenomenografisk tilnærming.
Hovedresultater: Blant ungdom som ikke brukte psykofarmaka ved baseline, ble psykisk lidelse rapportert av 15.5 % av ungdommene, 75 % av disse var jenter. For begge kjønn var insident bruk av psykofarmaka ett til ni år senere signifikant høyere blant dem som rapporterte psykisk lidelse ved baseline sammenlignet med resten av deltakerne. Høyest insident psykofarmakabruk ble observert blant jenter med psykisk lidelse ved baseline, 27. 7 %. I tillegg var helse, livsstilsvaner og sosiale faktorer assosiert til insident bruk (I). Samlet bruk av psykofarmaka økte både blant gutter og jenter i løpet av perioden 2006-2010, som tilskrives økt bruk av sovemidler generelt og melatonin spesielt. Totalt hentet 16,4 % av alle insidente brukere av psykofarmaka i 2007 fremdeles ut psykofarmaka i 2010 (II). Ungdom erfarer både fordelaktige og uønskede effekter av psykofarmaka. De erfarte manglende tilgang til profesjonell støtte og oppfølging. Livet med familien, venner, skole og arbeid ble påvirket av psykofarmakabruk, og de var engstelige for å bli stigmatisert (III). Helsesøstrene oppfattet tre deskriptive kategorier relatert til egne roller vedrørende ungdoms psykofarmakabruk: En oppdagende helsesøster som ble klar over psykofarmakabruk i helsesamtalen med ungdommen, og som da valgte enten å handle eller ikke å handle med hensyn til denne bruken. Deretter en samarbeidende helsesøster som handler og fortsetter samarbeidet med ungdommene, deres familier, skolen og andre. Til slutt en støttende helsesøster som samarbeider med de unge, underviser og støtter dem i bruken av psykofarmaka (IV).
Konklusjon: Mer oppmerksomhet bør bli viet dårlig psykisk helse og økende psykofarmakabruk blant ungdom. Kunnskap, behandling og oppfølging bør økes. Forekomsten av psykisk lidelse blant ungdom, med forskjeller mellom kjønn og sosioøkonomiske grupper, må også få konsekvenser for helsefremmende strategier overfor ungdom. Helsesøstre i Norge som arbeider på helsestasjoner og skoler har mulighet til og ansvar for å identifisere og følge opp unge menneskers mentale helseproblemer.
Nøkkelord: Ungdom, psykisk lidelse, psykiske helseproblemer, psykofarmakabruk, helsesøster
5
Table of content
Abstract ................................................................................................................. 3
Sammendrag ......................................................................................................... 4
Abbreviations ........................................................................................................ 7
Original papers ..................................................................................................... 8
Introduction .......................................................................................................... 9
Background .......................................................................................................... 10 Young people ........................................................................................................................... 10 Mental health problems .......................................................................................................... 11
Prevalence of mental distress among young people ....................................................... 12 Health, lifestyle habits and social factors ......................................................................... 14
Psychotropic drug use among young people ....................................................................... 15 Psychotropic drugs .............................................................................................................. 16
The public health nurse .......................................................................................................... 18
Rationale for the thesis ....................................................................................... 22
General and specific aims ................................................................................... 23
Methods .............................................................................................................. 24 The quantitative studies .......................................................................................................... 24
Data sources and collection (I, II) .................................................................................... 24 Participants (I, II) ................................................................................................................ 28 Data analysis (I, II) .............................................................................................................. 29
The qualitative studies ............................................................................................................. 30 Data sources and collection (III, IV) ................................................................................ 30 Participants (III, IV) ............................................................................................................ 30 Data analysis (III, IV) ......................................................................................................... 32
Ethical approval and considerations (I–IV) ......................................................................... 33
Main results ........................................................................................................ 36 Mental distress, health, lifestyle habits and social factors (I) ............................................. 36 Psychotropic drug use (I, II) .................................................................................................. 36 Experience of psychotropic drug use among young people with mental health problems (III) .................................................................................................. 40 The public health nurses’ roles in relation to psychotropic drug use among adolescents (IV) .......................................................................................................... 41
Summary of the results ....................................................................................... 44
Discussion of main results .................................................................................. 46 Young people under mental distress (2000–2003).............................................................. 46 Psychotropic drug use by young people ............................................................................... 49 The public health nurses’ role in relation to psychotropic drug use by young people ....................................................................................................................... 52
6
Methodological considerations .......................................................................... 56 The quantitative studies .......................................................................................................... 56 The qualitative studies ............................................................................................................. 59
Conclusions, implications and future research .................................................. 62 Conclusions .............................................................................................................................. 62 Implications .............................................................................................................................. 62 Future research ......................................................................................................................... 63
Acknowledgements ............................................................................................. 64
References ........................................................................................................... 66
Paper I - IV ......................................................................................................... 79
7
Abbreviations
ATC Anatomical Therapeutic Chemical classification system DDD Defined Daily Dose DSM-IV Diagnostic and Statistical Manual of Mental Disorders, 4th
edition ECTS European Credit Transfer and Accumulation System HSCL-10 Hopkins Symptom Checklist -10 HSCL-25 Hopkins Symptom Checklist -25 ICD-10 International Classification of Diseases, 10th revision, used in
hospitals 10 ICPC International Classification of Diseases, used in the primary
health care MYH Mental Health Young People NIPH Norwegian Institute of Public Health NorPD Norwegian Prescription Database NSD Norwegian Social Science Data Services AS NYHS Norwegian Youth Health Study PHN Public Health Nurse
8
Original papers
This thesis is based on the following papers, which will be referred to by their Roman numerals:
I. Steffenak, A. K. M., Nordström, G., Wilde-Larsson, B., Skurtveit, S., Furu, K. & Hartz, I. (2012). Mental Distress and Subsequent Use of Psychotropic Drugs among Adolescents - A Prospective Register Linkage Study. Journal of Adolescent Health, 50: 578–587.
II. Steffenak, A. K. M., Wilde-Larsson, B., Nordström, G., Skurtveit, S. & Hartz, I. (2012). Increase in psychotropic drug use between 2006 and 2010 among adolescents in Norway: a nationwide prescription database study. Clinical Epidemiology, 4(1): 225-231.
III. Steffenak, A.K.M., Wilde-Larsson, B., Hartz, I. & Nordström, G. Experience of psychotropic drug use among young people with mental health problems. Submitted. 2013.
IV. Steffenak, A.K.M., Nordström, G., Hartz, I. & Wilde-Larsson, B. Public health nurses‘ conception of their roles in relation to psychotropic drug use among adolescents. Re-Submitted to Public Health Nursing. 2013.
Reprints were made with permission from the publishers.
9
Introduction
International studies indicate an increase in mental distress among young people (Patel et al., 2007). Some young people under mental distress may need psychotropic drugs for a short or a longer time (Kessler et al., 2007). There has been an increase in psychotropic drug use among young people (Fegert et al, 2006; Zito et al., 2008b; Zoëga et al., 2009) which could reflect an increase in the number of young people under mental distress. In different countries various patterns of psychotropic drug use are seen (Zito et al., 2008b). The psychotropic drugs used are the same as those that have been approved for use by adults, in this case based on beneficial risk assessments from clinical trial data for adults (Zito et al., 2008a).
In Norway a substantial number of young people with mental health problems are followed up in their municipalities’ health services. Their health problems are often identified at school. Public health nurses (PHNs) in these school health services are some of the health professionals who can identify young people’s mental health needs and provide them with resources for their care (Chisolm et al., 2009).
During the 1990s I worked as a PHN at high school and public health centres for young people in a municipality in Norway. Since then the issues for which young people visited PHNs for have changed. From common subjects with which PHNs usually worked such as birth control, repetitive strain injuries, health examination and immunizations, the subjects have changed to eating disorders, self-injury, anxiety, depression and problems of a more social nature. This experience is my motivation for the subject of this thesis: young people’s mental health, their use of psychotropic drugs and the PHN’s role in relation to this.

10
Background
Young people
Young people move from childhood through adolescence into adulthood facing challenges including mental, emotional, physical and social transformations associated with maturation (Currie et al., 2012). This is a period in life that varies and there are no universally accepted definitions of adolescents and young people. The United Nations understands adolescents to include people aged 10–19 years and young people as those aged 15–24 years for statistical purposes, without prejudice to other definitions by member states (United Nations Population Fund, 2013). In this thesis both adolescents and young people have been used and refer to people aged between 10 and 24 years.
Frønes (2007) described the period of adolescents and young people as a moratorium – a phase in which seeking the meaning of life is essential. As an existential phase, it forms the basis of riots, renewal and innovation. A new life is lived more often than imagined, and the riot and renewal of young people are more like manners and a way of life than an ideology. This phase can be complex, and one in which adolescents and young people take on new responsibilities and experience independence. They search for identity, learn to apply values acquired in early childhood, and develop skills that will help them become caring and responsible adults (United Nations Children’s Fund, 2002). How formative it is depends on the historical context, social system, local conditions, structure of individual lifespans and perceived health (Frønes, 2007). This period is one of the most complex transitions in life. It is a time to explore the concepts of right and wrong, develop the capacity to reason in an abstract way, create hypotheses and think about the future (Piaget, 1932).
Areas of the brain associated with functions such as integrating the sights, smells and language that we experience develop during this period. The prefrontal cortex (located behind the forehead) develops important new functions and does not fully mature until later in the phase. The brain’s ‘commander in chief’ is responsible for planning, organization, judgement, problem-solving and emotional control. The brain reorganizes itself; patterns are formed based on which connections are reinforced by mental or physical activity. Girls and boys learn to marshal their thoughts, measure their impulses

11
and think abstractly – important neural foundations are formed that will last a lifetime (Plessen & Kabicheva, 2010).
A physical maturation is seen, and puberty is considered by many to be a significant biological marker for the onset of this phase, although no clear biological markers are available to indicate its end (Patel et al., 2007).
Mental health problems
The World Health Organization (WHO) recognizes that mental health among young people is one of the most important areas and will in general be one of the most serious global health problems in 2020 (WHO, 2004a). Good mental health among young people leads to the development of and capability for managing thoughts, feelings, behaviour and the demands of various aspects of everyday life. It is fundamental to a good life, but not necessarily synonymous with an absence of mental health problems and stress. Good mental health has implications for self-esteem, behaviour, attendance at school, educational achievement, social cohesion, and future health and life chances (WHO, 2012). Confident young people with good mental health are those most likely to grow into confident adults with good mental health. This is an asset that may help people rebound from any of the setbacks that can occur and will in general help in the continuity of a meaningful life (Walsh, 2006).
There is confusion around the different terminology used when it comes to mental health problems, e.g. mental distress and mental disorders. These terms are often used interchangeably and are derived from different philosophical, theoretical and ideological perspectives. Critical social scientific or user-centred literature tends to use the terms ‘mental health problem’ and ‘mental distress’ to confirm the intention of reflecting a psychosocial paradigm. Mental distress as used in mental health nursing refers to a wide range of mental conditions, from relatively mild pain to milder mental disorders: a disturbing unpleasant mental or emotional state, such as fear, confusion, mood swings, anxiety and depression (Nasjonalt Folkehelseinstitutt, 2011). The medical paradigm, which nursing has tried to move away from, uses the term ‘mental disorder’ (Coppock & Dunn, 2010). The concepts of mental health problems and mental distress are taken as synonymous in this thesis.

12
The most common mental disorders among young people include depression, anxiety disorders, attention deficit hyperactivity disorder (ADHD) and disorders of substance abuse (Costello, 2003; Merikangas, 2005). There is a high rate of self-harm, and suicide is a leading cause of death among adolescents with mental health problems (Patel et al., 2007). After puberty, anxiety and depression are diagnosed the more, 10–15% and 3–8%, respectively. There is a strong correlation between anxiety and depression during adolescence and about 40% of those with depression also have an anxiety disorder (Merikangas, 2005).
Depression among young people is characterized by low mood, sadness, and feelings of hopelessness and helplessness. It is common to have no motivation or interest in things and other people. Self-esteem decreases and the way of thinking changes. A number of young people avoid contact with their friends and take part in fewer social activities (Helland & Mathiesen, 2009). Sleeping problems among young people are common and epidemiological studies indicate that insomnia is linked to behavioural and emotional problems, such as anxiety and depression (Xu et al., 2012).
A review (Siegel & Dickstein, 2011) reported anxiety as the most prevalent mental health problem among young people. Anxiety disorders, at their most basic level, share common features, including excessive fear, avoidance of whatever is feared, and anticipation and worry. Adults report retrospectively that anxiety generally had its onset in childhood or adolescence (Merikangas & Pine, 2002).
Young people are thought to have good health. They live during a period in which the disease burden is low. Increasing mental health problems seems to carry a substantial burden of illness and disability, which could lead to poor personal, social and economic outcomes. Mental health problems are the main cause of disability among young people, 45% of which are caused by mental distress (Gore et al., 2011). Adolescence is the stage at which mental health problems, often detected for the first time, start (Patel et al., 2007).
Prevalence of mental distress among young people
Evidence is mixed as to whether rates of mental distress among young people have increased over the past few decades (Collishaw et al., 2004; Patel et al.,

13
2007). These rates are reported to range from 8% to 57% in different international studies (Patel et al., 2007).
Most mental health problems start after puberty, from the age of 12–14 years, when an increase in prevalence of self-reported anxiety, depression and eating disorders is observed. Mental health problems often continue into adulthood, with half of lifetime cases start by age 14 years, and in total 75% by age 24 (Kessler et al., 2007; WHO, 2011).
After the age of 13 several studies indicate a distinct gender pattern between girls and boys. Generally, girls report more mental health problems and lower quality of life than boys in several countries (Cavallo et al., 2006; Torsheim et al., 2006; Mykletun et al., 2009). In Norway, girls constitute two out of three adolescents aged 13 and over with a mental disorder (Mathiesen et al., 2007; Helland & Mathiesen, 2009).
Hagquist (2009) reported a significant increase in mental distress from 1985 to 2005 among Swedish adolescents, particularly girls. The proportions of girls aged between 16 and 19 years who reported anxiety, worry and anguish increased from 8% to 29%. For boys the corresponding figures were 2% to 7%. A 2011 survey showed that most young people reported good mental health. The level of mental distress increased from grade sixth to grade ninth and girls continue to report mental distress more frequently than boys (Statens Folkhälsoinstitut, 2011).
In Norway, information about the prevalence of mental distress among young people is insufficient (Mykletun et al., 2009). However, a Norwegian study some years ago indicated that 15–20% of young people had a lot of depressive symptoms, and the point prevalence for depressive disorders was 5% (Sund, 2004). There was an estimate that 70 000 children and young people under mental distress needed treatment (Roy et al., 2006; Helland & Mathiesen, 2009; Mykletun et al., 2009).
Recently a national survey reported young people in Norway as having a good life. They got on well with their family and friends, felt comfortable at school and looked forward to a promising future. At the same time, several worries and struggles with mental health problems, sleeping problems, hopelessness and bad self-image were identified, and 10 % struggled with symptoms of

14
depression. The girls are afflicted more than the boys and seek help more frequently (Ungdata 2010–1012, 2013).
Health, lifestyle habits and social factors
The health and lifestyle habits adopted by young people, as well as social factors such as education plans and perception of family economics, might affect their health not only during the adolescence period, but also later in life (Patel et al., 2007; Patton et al., 2009). Based on a holistic health concept and orientation towards individual resources, mental health was thought essentially to be health promotion work (Morgan & Ziglio (2007). A health asset approach involves preventive activities and focuses on protective factors. Factors that build resilience to inhibit high-risk behaviours such as violence, dropping out school and substance abuse, all have a negative effect on mental health (Morgan & Ziglio, 2007). These factors may also have an impact on adolescents’ mental ability to achieve and sustain good mental health; factors include those that operate at different levels, e.g. at the individual level such as self-perceived health, cigarette smoking, alcohol use and physical activity, together with those at a family level, e.g. family economy, and a at school level such as plans for education.
Self-perceived health problems are found to associate with depression and anxiety (Moksnes et al., 2011; Wiklund et al., 2012). Those people with more frequent recurrent health problems were more likely to have higher levels of drug use (Gobina et al., 2011).
Studies indicate an association between mental health problems and lifestyle habits such as smoking, alcohol use and physical activity. Smoking seems to be related to symptoms of subsequent mental health problems (Steuber & Danner, 2006; Lien et al., 2009) and there are associations between alcohol use and sleep problems among young people (Popovici & French, 2013). Furthermore, a cross-sectional study showed that physically active adolescents had reduced odds of developing depressive symptoms (Wiles et al., 2012).
Those whose families had good economy were most comfortable at school (Ungdata 2010–1012, 2013) and previous studies also indicate an association between young people’s socioeconomic inequalities and mental health problems such as depression, anxiety and stress (Levin et al., 2011).
15
Psychotropic drug use among young people
The appropriateness of psychotropic drug use by young people is controversial. As early as 1995, Simeon et al., (1995) described the slow development of knowledge about psychotropic drug use in this group because of a lack of research, ethical issues, regulations and opposition to their use by young people. In spite of these reflections and objections, there is increasing use of psychotropic drugs among young people (Dean et al., 2007; Ilomäki et al., 2011; Hartz et al., 2012).
Unfortunately, evidence for the safety and efficacy of psychotropic drug use in young people is scarce, especially with regard to long-term effects (Bonati & Clavenna, 2005). Psychotropic drugs may stimulate or sedate, alter the emotional experience of anxiety or panic, and influence mood and concentration. They have side effects, some mild, some inconvenient, and others more serious, producing physiological and neurological disturbances (Safer, 2011). A number of psychotropic drugs used by young people are used off-label or off-licence. This term is used for drugs for an unapproved indication, age group, dosage or form of administration. Most of the psychotropic drugs are not tested on or licensed for young people (Kalikstad & Westergren, 2006; Wohlfarth et al., 2009).
Over the past few decades, psychotropic drug use by young people has increased two- to threefold in the USA. The prevalence of psychotropic drug use in the USA is reported to be three times higher than among young people in several European countries. The annual prevalence of any psychotropic medication was significantly greater in the USA (6.7 %) than in the Netherlands (2.9 %) or Germany (2.0 %) (Zito et al., 2008b). A proportional growth has been reported in girls receiving stimulants and boys receiving antidepressants, particularly for the 10–14 year olds (Zito et al., 2003).
Different patterns of psychotropic drug use by young people have been shown between the USA and European countries, but also between European countries. This may reflect cultural beliefs, different regulations, diagnostic classification systems and study design. However, studies from the United Kingdom (UK) indicate a changing prescribing practice that is more along the lines of that in the USA. A fivefold increase in the number of prescriptions and a tenfold increase in the number of adolescents prescribed psychotropic drugs

16
are seen in the UK. The use of antidepressants, hypnotics/anxiolytics and anticonvulsants increased with increasing age. Antidepressants increased 1.6-fold and hypnotics/anxiolytics 1.3-fold (Sivaprasad et al., 2005; Hsia & Maclennan, 2009). Beyond that, a study in Germany described the use of psychotropic medications as moderate but prevalence varied across the different classes of drugs – hypnotics, antipsychotics, antidepressants and anxiolytics (Koelch et al., 2009).
Holstein et al. (2009) reported an increase in drug use for mental distress among young people in Denmark. In Finland psychotropic drug use was rather uncommon until late adolescence; 15% of a cohort born in 1981 had used a psychotropic drug before the age of 25 years (Gyllenberg & Sourander, 2012). In Norway the level of psychotropic drug use by young people has been reported to be relatively low, less than 4%, and the same for boys and girls (Skurtveit et al., 2005). However, between 2004 and 2011, there was a trend towards increasing hypnotic drug use by Norwegians aged between 0 and 17 years (Hartz et al., 2012). Although the use of psychotropic drugs in Norway seems to have increased it still remains rather low (Skurtveit et al., 2005, 2008). The same is also true for the other Nordic countries with the exception of Iceland which has extensive psychotropic drug use in the young population aged between 0 and 17 years (Zoëga et al., 2009).
Psychotropic drugs
Similar to all medications, psychotropic drugs are classified according to the Anatomical Therapeutic Chemical (ATC) classification system (WHO, 2013). This system divides active substances into different groups according to both the organ and system on which they act, and their therapeutic, pharmacological and chemical properties. The drugs are classified into groups at five different levels, then divided into fourteen main groups (first level), with pharmacological/therapeutic subgroups (second level). The third and fourth levels are chemical/pharmacological/therapeutic subgroups and the fifth level is the chemical substance. The second, third and fourth levels are often used to identify pharmacological subgroups (Lingjærde, 2006). As a complete classification melatonin illustrates the structure of the ATC classification system in Table 1.
17
Table 1. The Anatomical Therapeutic Chemical (ATC) classification system illustrated by the classification of melatonin
N Nervous (first level, anatomical main group) N05 Psycholeptics system (second level, therapeutic subgroup) N05C Hypnotics and sedatives (third level, pharmacological subgroup) N05CH Melatonin receptor agonists (fourth level, chemical subgroup) N05CH01 Melatonin (fifth level, chemical substance) – Cicadin, Neurim depot
A defined daily dose (DDD) is assigned only to those drugs that already have an ATC code and is defined as the assumed average maintenance dose per day for a drug used for its main indication in adults. It should be emphasized that the DDD is a unit of measurement and does not necessarily reflect the recommended or prescribed daily dose. Doses for individual patients and patient groups will often differ from the DDD and of necessity have to be based on individual characteristics (e.g. age and weight) and pharmacokinetic considerations (WHO, 2013).
The psychotropic drugs investigated in this thesis are antidepressants (N05A), anxiolytics (N05B), hypnotics (N05C) and systemic antihistamines (R06AD). Indications for psychotropic drug use are different for mental health problems such as anxiety, depression and sleep disturbance (Lingjærde, 2006).
Antidepressants (N05A) are used for depression and mainly consist of two subgroups such as tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs). The SSRIs are recommended used first-line for depression as well as for anxiety in adults because they do not cause as many side effects as the older antidepressants (Lingjærde, 2006; Vaaler & Fasmer, 2013).
Anxiolytics (N05B) are used to treat symptoms of acute anxiety. The benzodiazepines constitute the largest subgroup, which can be habit forming and are recommended prescribed for short-term use (Lingjærde, 2006).
Hypnotics (N05C) are usually used to treat sleep disturbances. Benzodiazepines and the benzodiazepine-like Z-hypnotics (zopiclone, zolpidem and zaleplon) have the same mode of action and many of the same effects. The use of Z-hypnotics has had a large steady increase since their introduction in Norway. The relatively short half-lives of these drugs may cause fewer hangover effects,

18
but Z-hypnotics are no more effective or safer than benzodiazepines (Mellingsæter et al., 2006; Berg et al., 2011).
Systemic antihistamines (R06AD) (phenothiazines) have been used for childhood insomnia in Norway for a long time, and constitute the second most commonly prescribed hypnotic drug among 0–17 year olds in Norway in 2011 (Hartz et al., 2012).
Side-effects of psychotropic drugs differ from one person to another, some get side effects other do not. Different factors affect how the psychotropic drug influence the individual, such as; kind of mental distress, age, sex, body size, physical illnesses, alcohol and nicotine use, liver and kidney function, other medications (interactions), diet, genetics and whether the drug are taken as prescribed. Psychotropic drugs have different side effect profiles, but generally, frequent side-effects are described to be: headache, sedation, gastro-intestinal disturbances, dry mouth, urinary retention, blurred vision, dizziness and weight gain (Lingjærde, 2006).
The public health nurse
It is difficult to define PHNs in a global perspective. In the past and in different parts of the world, PHNs have been known as health visitors, community health nurses and district nurses. There is no shared terminology to clarify the role and titles; however, there are similarities in different countries – PHNs located in community settings with a focus on promoting health and preventing poor health. Knowledge of nursing, social and public health sciences is the basis of community health nursing practices.
In the USA, the community health nurse works in a variety of settings, including state and local health departments. They work, for example, at schools, migrant health clinics, health centres, senior centres and home care programmes (Meadows, 2009). Ellefsen (2001) described health visitors in Scotland who held a central position in the national strategy for health and illness prevention in the twentieth century. In later years their work expanded into a much wider range of services for clients from the cradle to the grave and they specialized in certain areas.
In Sweden district nurses work within primary health care, home nursing care, infant- and preschool child care and they also run nursing care units

19
(Distriktssköterskeföreningen i Sverige, 2013). Clancy (2010) stated the following regarding public health nursing: ‘Historical development of the services has followed the same patterns in all the Nordic countries despite differences in their titles, tasks and claims’ (p. 9).
Usually, the PHNs in Norway have their work located to the municipality, at public health centres, school health services and health clinics for adolescents. In 2009 3510 PHNs worked in these services. They held a central position within the health services and municipality school health services and met most of the children, young people and their families. The work of the PHNs is regulated by Norwegian laws and regulations (Act of Public Health 2012; Act of Health & Care, 2011). These are new laws and a so-called ‘professional neutral act’ which requires physicians and midwifes only in the community. PHNs are not talked about any longer, but there is demand for the qualifications for the job. The duties of the PHNs are described in the Regulation to the Child Health Clinics and the School Health Services (The Norwegian Directorate of Health, 2003a). The aim of this service is to follow, maintain and recover students’ physical and mental health.
Norwegian PHNs are primarily educated as registered nurses with postgraduate qualifications (60 ECTS) in health promotion, working especially for the target group of young people aged 0 and 20 and their families (The Ministry of education & research, 2005). They have a general competence in health promotion, able to work at a universal level and offer help to all young people as well as their families. Health promotion is seen as ‘the process of enabling people to increase control over, and to improve, their health and further to increase the options available to people to exercise more control over their health, environments, and to make choices conductive to health’ (p.1-4) (WHO, 2009b). This is also in accordance with Florence Nightingale’s health-promoting work which was vitally important to her. In the middle of the nineteenth century she saw the importance of cooperation with nature to build and strengthen health, and at the same time to fight against illness and pay attention to what had brought about the illness. She warned of ‘spending too much time in understanding a disease as it presents itself, rather than focusing on cultivating the holistic resource of intelligence to mitigate disease effects’ (Nightingale, 1853, p. 194-195). She thought that many disease causes were to

20
be found in the environment such as scarcity of fresh air, light, heat, calm and cleanliness, or the right food (Alvsvåg, 2012).
In Norway today PHNs play an important role in discovering early inappropriate development of health problems among young people. Furthermore they have to take the initiative and potentially refer to other authorities (Act of Public Health 2012). They also have a role to play in health information and mapping of environments that damage health physically, psychologically and socially for young people in the community. Such roles assert that PHNs must be clear and visible, and active participants in the community. Clancy and Svensson (2009) describe community decision-makers recognizing the contribution of PHNs to public health, but have insufficient knowledge of the content of their service. The PHNs themselves feel like an overlooked service (Clancy, 2007a). To make PHNs more visible Clancy (2010) emphasized the importance of enabling users and collaborators’ access to PHNs but also made policy-makers aware of the public health challenges that PHNs face.
In Norway every municipality is obliged to have a school health service that shall take care of the health of school-aged children and young people (Act of Public Health 2012). The school health service is a low-threshold supply that is easily available and PHNs who work within it have a contact area for all adolescents and young people. The school health service and health clinics are used by approximately 1.2 million users each year. Where school health services are available, 50% of the pupils use them (The Norwegian Directorate of Health, 2010). As a substantial number of young people visit the school health service, PHNs could be the professional who can identify adolescents’ mental health needs and provide them with resources for their care (Chisolm et al., 2009). Adolescents and young people visit PHNs at their school to discuss and safeguard their own health. PHNs provide confidential drop-in sessions at which the students can share worries and concerns, and they offer health counselling and education. Positive effects of health dialogues have been reported, and Borup and Holstein (2002, 2004) underline the fact that the PHN may be not only an additional adult to approach, but also a reliable alternative when neither parents nor teachers are appropriate.
School health services are possibly an under-investigated issue in public health, but they are important because they may be the tool for health promotion

21
among young people (Borup & Holstein, 2007). Studies indicate that adapted health dialogues within school health services are based on an open atmosphere, reflecting openness, trustworthiness, knowledge and supportive attitude (Borup, 2002); this could be an entry point to contact with young people who need help. In this connection health promotion in nursing may support good health choices and help to secure appropriate help for prevention at an early stage. The goals and traditions of public health and health promotion can be applied just as usefully in the field of mental health as they have been in heart health, infectious diseases and tobacco control (WHO, 2004b).
PHNs who work within the school health service are in a position to prevent mental distress and identify psychotropic drug use (Borup & Holstein, 2004, 2010; Herrman et al., 2005). Borup (2011) report that PHNs (school nurse) may reduce students’ proneness to drug use when they experience complaints. In the Norwegian municipalities, health professionals are responsible for intercepting the signals from young people with mental health problems and referring them for examination and further treatment within specialist health care (The Norwegian Directorate of Health, 2008). Young people have the right to health care as stated in the Act of Patients’ Rights (1999). Support for young people with mental health problems is an area that falls naturally into the remit of PHNs. They often see adolescents and young people who struggle at school (Borup & Holstein, 2006; Pirskanen et al., 2007; Arnesdotter et al., 2008). It is therefore essential to acquire knowledge about the different ways in which PHNs become aware of mental health problems and psychotropic drug use by young people and for them to consider their role in relation to this.

22
Rationale for the thesis
Mental distress among young people and its association to health, lifestyle habits and social factors are reported. This is also the case with regard to psychotropic drug use among young people. A gender difference is seen as well. Studies among young people reporting on mental distress and its association to later initiation of psychotropic drug use, as well as psychotropic drug use pattern over time are scarce. Nor do we know much about how young people experience psychotropic drug use as users.
PHNs who meet young people within school health services have an important role to play in health promotion and prevention of illness. Studies describing the role of PHNs in relation to young people with mental health problems who are psychotropic drug users have not been found. Thus there is a need for a study of the role of PHNs in relation to this.
23
General and specific aims
The overall aim was to study mental distress, health and lifestyle habits, social factors and subsequent psychotropic drug use by young people, and how PHNs conceive their roles in relation to this.
The specific aims were as follows:
I. To investigate the association between mental stress, other factors, and subsequent psychotropic drugs in adolescents aged 15–16 years.
II. To investigate the one-year prevalence of psychotropic (hypnotic, antidepressant, anxiolytic) drug use among adolescents aged 15–16 years during 2006–2010 related to gender and subcategories of psychotropic medication, and to study use of psychotropic drugs in the period 2007–2010 among incident psychotropic drug users in 2007.
III. To explore the experience of psychotropic drug use among young people with mental health problems
IV. To describe PHNs’ conceptions of their roles in relation to psychotropic drug use among adolescents.
24
Methods
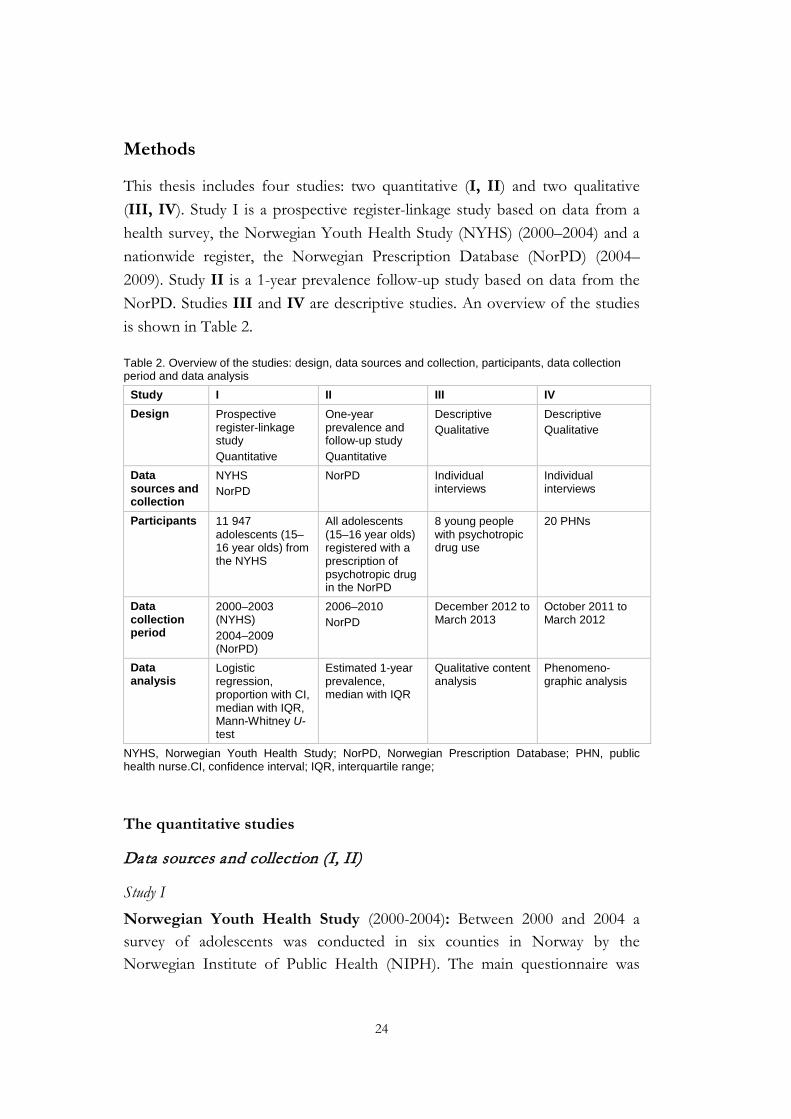
This thesis includes four studies: two quantitative (I, II) and two qualitative (III, IV). Study I is a prospective register-linkage study based on data from a health survey, the Norwegian Youth Health Study (NYHS) (2000–2004) and a nationwide register, the Norwegian Prescription Database (NorPD) (2004–2009). Study II is a 1-year prevalence follow-up study based on data from the NorPD. Studies III and IV are descriptive studies. An overview of the studies is shown in Table 2.
Table 2. Overview of the studies: design, data sources and collection, participants, data collection period and data analysis
Study I II III IV Design Prospective
register-linkage study Quantitative
One-year prevalence and follow-up study Quantitative
Descriptive Qualitative
Descriptive Qualitative
Data sources and collection
NYHS NorPD
NorPD Individual interviews
Individual interviews
Participants 11 947 adolescents (15–16 year olds) from the NYHS
All adolescents (15–16 year olds) registered with a prescription of psychotropic drug in the NorPD
8 young people with psychotropic drug use
20 PHNs
Data collection period
2000–2003 (NYHS) 2004–2009 (NorPD)
2006–2010 NorPD
December 2012 to March 2013
October 2011 to March 2012
Data analysis
Logistic regression, proportion with CI, median with IQR, Mann-Whitney U- test
Estimated 1-year prevalence, median with IQR
Qualitative content analysis
Phenomeno-graphic analysis
NYHS, Norwegian Youth Health Study; NorPD, Norwegian Prescription Database; PHN, public health nurse.CI, confidence interval; IQR, interquartile range;
The quantitative studies
Data sources and collection (I, II)
Study I
Norwegian Youth Health Study (2000-2004): Between 2000 and 2004 a survey of adolescents was conducted in six counties in Norway by the Norwegian Institute of Public Health (NIPH). The main questionnaire was
25
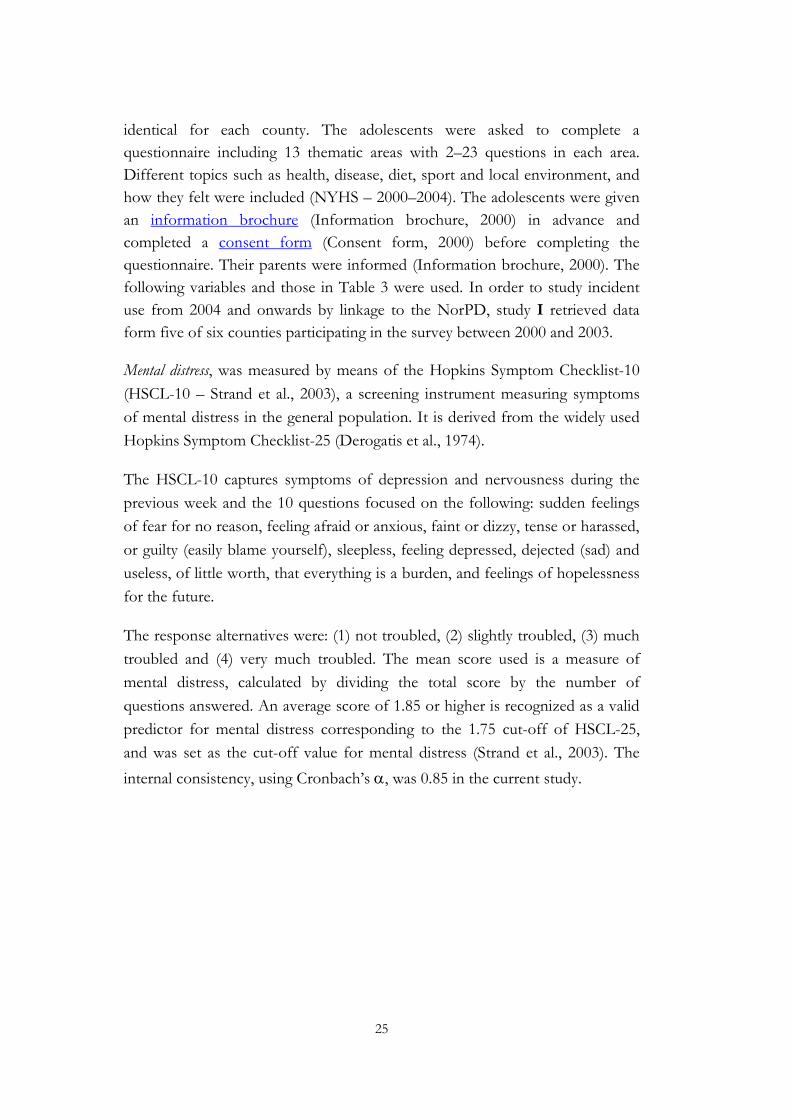
identical for each county. The adolescents were asked to complete a questionnaire including 13 thematic areas with 2–23 questions in each area. Different topics such as health, disease, diet, sport and local environment, and how they felt were included (NYHS – 2000–2004). The adolescents were given an information brochure (Information brochure, 2000) in advance and completed a consent form (Consent form, 2000) before completing the questionnaire. Their parents were informed (Information brochure, 2000). The following variables and those in Table 3 were used. In order to study incident use from 2004 and onwards by linkage to the NorPD, study I retrieved data form five of six counties participating in the survey between 2000 and 2003.
Mental distress, was measured by means of the Hopkins Symptom Checklist-10 (HSCL-10 – Strand et al., 2003), a screening instrument measuring symptoms of mental distress in the general population. It is derived from the widely used Hopkins Symptom Checklist-25 (Derogatis et al., 1974).
The HSCL-10 captures symptoms of depression and nervousness during the previous week and the 10 questions focused on the following: sudden feelings of fear for no reason, feeling afraid or anxious, faint or dizzy, tense or harassed, or guilty (easily blame yourself), sleepless, feeling depressed, dejected (sad) and useless, of little worth, that everything is a burden, and feelings of hopelessness for the future.
The response alternatives were: (1) not troubled, (2) slightly troubled, (3) much troubled and (4) very much troubled. The mean score used is a measure of mental distress, calculated by dividing the total score by the number of questions answered. An average score of 1.85 or higher is recognized as a valid predictor for mental distress corresponding to the 1.75 cut-off of HSCL-25, and was set as the cut-off value for mental distress (Strand et al., 2003). The internal consistency, using Cronbach’s α, was 0.85 in the current study.
26
Table 3. Health and lifestyle habits and social factors such as; education plans and family economy. Variable definitions and response alternatives from the NYHS is shown
Variables Variable definitions (response alternatives)
Self-perceived health Poor (poor and not so good) Good (good and very good)
Experience of physical pain sites during the last 12 months
No sites, 1–2 sites, 3+ sites
Smoking Non-smokers (no and never) Light smokers (I have stopped but smoke occasionally) Daily smokers (daily)
Alcohol use None (no and never) Light (once and 2–3 times) Moderate consumer (4–10 or >10 times)
Physical activity Reported by number of times per week Education plans Reported by means of one of the following alternatives:
university/college, upper secondary school, vocational education, not decided or other
Family economics in relation to other families in Norway
Poor (poor) Moderate (moderate) Good (good and very good)
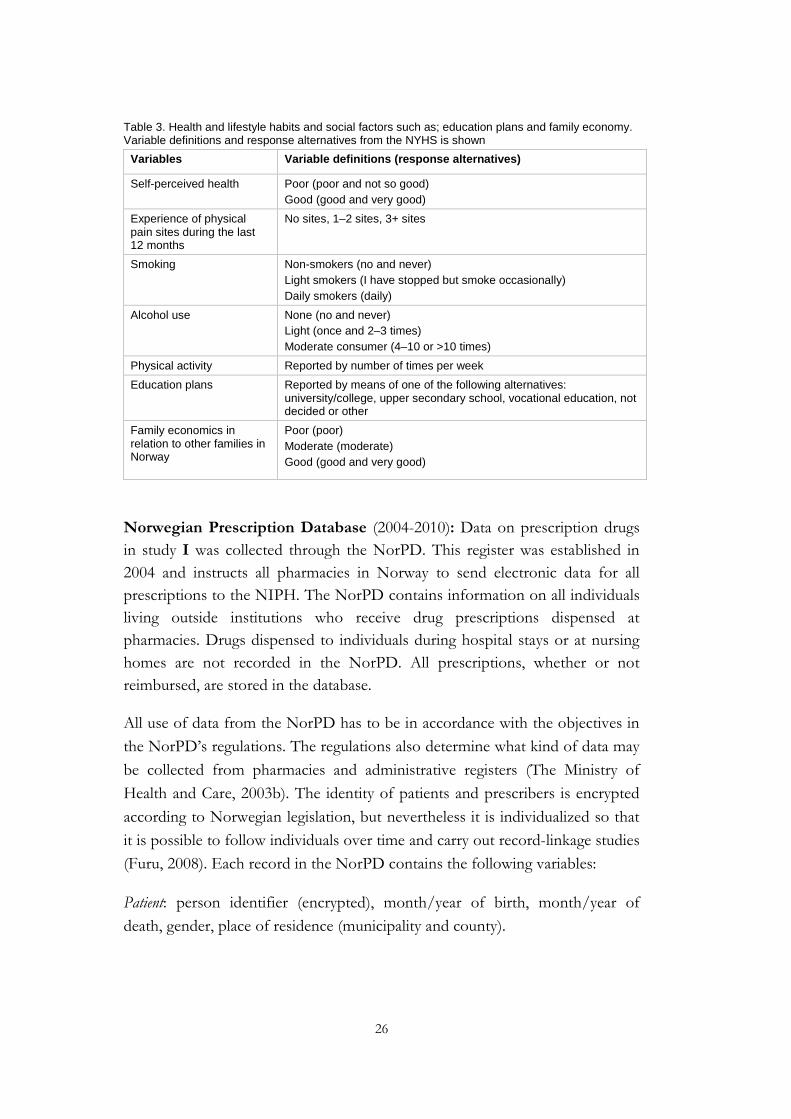
Norwegian Prescription Database (2004-2010): Data on prescription drugs in study I was collected through the NorPD. This register was established in 2004 and instructs all pharmacies in Norway to send electronic data for all prescriptions to the NIPH. The NorPD contains information on all individuals living outside institutions who receive drug prescriptions dispensed at pharmacies. Drugs dispensed to individuals during hospital stays or at nursing homes are not recorded in the NorPD. All prescriptions, whether or not reimbursed, are stored in the database.
All use of data from the NorPD has to be in accordance with the objectives in the NorPD’s regulations. The regulations also determine what kind of data may be collected from pharmacies and administrative registers (The Ministry of Health and Care, 2003b). The identity of patients and prescribers is encrypted according to Norwegian legislation, but nevertheless it is individualized so that it is possible to follow individuals over time and carry out record-linkage studies (Furu, 2008). Each record in the NorPD contains the following variables:
Patient: person identifier (encrypted), month/year of birth, month/year of death, gender, place of residence (municipality and county).
27
Prescriber: person identifier (encrypted), month/year of birth, gender, profession, specialty.
Drug: Nordic article number (brand name, strength, package size), number of packages, ATC code, DDD, category of prescription, code for reimbursement (from March 2008: ICD-10 or ICPC codes) (WHO, 2010; ICPC, 2008), area of application and prescribed dose (free-text), dispensing date, price (pharmacy retail price).
Pharmacy: Name, licence number, municipality and county.
In study I the prescription data on psychotropic drugs retrieved from the NorPD was the patient unique identifying number, gender and age and date of dispensing. The following ATC codes were included as psychotropic drugs – antidepressants (N05A), anxiolytics (N05B), hypnotics (N05C) and phenothiazine derivatives (R06AD. The data was retrieved in the period 1 January 2004 to 31 December 2010. The outcome measure, incident psychotropic drug use was defined as retrieval of at least one prescription from the above drugs during the period 2004-2009.
Record register linkage: To study incident use of psychotropic drugs between 2004 and 2009, record register linkage was carried out between the NYHS (2000–2003) and the NorPD (2004–2009).
According to Furu (2008) such linkage was possible in accordance with Norwegian law, and the approval was received from the Data Inspectorate. The data has to be encrypted by the NIPH and sent to a trusted third part centre – Statistics Norway. Statistics Norway encrypts the data further using an anonymous process, and thereafter the data is linked to files from another register (Furu, 2008).
Study II
Data for this study was collected from the NorPD between 2006 and 2010 and included patient unique identifying number, gender, age, date of dispensing and drug information: ATC code and DDD.
The psychotropic subcategories included antidepressants (N05A), anxiolytics (N05B), hypnotics and phenothiazine derivatives (N05C+R06AD). The phenothiazine derivatives were included together with the hypnotics (N05C)
28
and referred to as hypnotics. Phenothiazine derivatives have been used for childhood insomnia in Norway and constitute the second most prescribed hypnotic drug for 0–17 year olds (Hartz et al., 2012). In addition melatonin (N05CH) was specified. The Z-hypnotics are a group of non-benzodiazepines with effects similar to those of benzodiazepines. They are used to treat sleeping problems.
The 1-year prevalence (per 1000 inhabitants) was investigated during 2006–2010 in relation to gender and subcategories of psychotropic drugs. Recurrent use of psychotropic drugs in the period 2007 to 2010 the use of psychotropic drugs was studied among incident users in 2007. And least, annual amounts of psychotropic drugs were presented as DDDs.
Participants (I, II)
Study I
Altogether 11 947 adolescents aged 15–16 years in grade 10, at secondary schools in five Norwegian counties participated in the NYHS. As the purpose of this study was to investigate incident use of psychotropic drugs, those who were psychotropic drug users at the baseline were excluded from the study population. Thus participants, including those who reported a proprietary name of their psychotropic drug or did not answer ‘Have never used this drug’ for a specific psychotropic drug question, were excluded from the study (n = 1085). As a second step, by use of reimbursement codes, those whose drugs were for treatment of epilepsy (n = 149) or cancer (n = 7) were removed. Finally 123 individuals were removed as a result of missing information on the HSCL-10 score. In total, the study population included 10 583 adolescents, a participation rate of 87%.
Study II
All adolescents aged 15–16 years in 2006 (n = 127 571), 2008 (n = 136 282), and 2010 (n = 128 012), who had filled at least one prescription for the psychotropic drugs antidepressants (N05A), anxiolytics (N05B) and hypnotics (N05C+ R06AD), were included (Table 4).
29
Table 4. The Norwegian Prescription Database: the number of adolescents aged 15–16 years who used a psychotropic drug in 2006, 2008 and 2010
2006 2008 2010 n n n
Hypnotics (ATC code N05C+ R06AD) 1338 1819 2221
Antidepressants (ATC code N06A) 769 825 903
Anxiolytics (ATC code N05B) 384 375 360
ATC, Anatomical Therapeutic Chemical classification system.
Data analysis (I, II)
Study I
The study population was stratified according to mental distress and gender. Baseline characteristics were presented as proportions with a 95% confidence interval (CI) in each stratum, and compared across the strata. No overlap of the CIs was considered significant at the 5% level.
The number of sessions of physical activity per week was presented as median with the interquartile range (IQR) and Mann–Whitney U-test was used for comparison.
Overall and gender-specific associations were estimated between mental distress (HSCL score), lifestyle habits, social factors and incident use of psychotropic drugs using logistic regression analysis; they were presented as crude and adjusted odds ratios (ORs, bi- and multivariate ORs) with 95% CIs (Hair et al., 2010).
Study II
The 1-year prevalence of prescribed psychotropic drugs was estimated by the identification of the number of individuals who had filled at least one prescription in the year for every 1000 inhabitants. The annual amounts of psychotropic drugs used, in terms of DDDs, are presented as median with and interquartile ranges. The proportion of recurrent use was calculated among incident users in 2007 and recurrent use was defined as filling at least one prescription each year over the period 2007–2010. All analyses were done using SPSS 17.0 for Windows, version 17 Inc. (Chicago IL, USA) (George & Mallery, 1999).
30
The qualitative studies
Data sources and collection (III, IV)
Study III
This study included eight interviews. Two were by telephone, and six according to the participants’ wishes, at cafeterias or restaurants, were audio-taped and lasted between 45 minutes and 2.5 hours (mean = 68.62, standard deviation = 38.96 minutes). All the interviews were conducted by the first author. Experiences relating to psychotropic drug use were evoked by asking: ‘Please, tell me about your experiences of psychotropic drug use? Individually adapted follow-up questions were asked such as: Can you give me an example? Can you tell me more about that? Can you explain that a little more?
Study IV
Interviews were at either the PHN’s workplace (n = 19) or their home (n = 1). They used a conversational style, were audio-taped and lasted from 15 minutes to 45 (mean = 28, SD = 8.31) minutes. The interviews included two main questions for the PHNs:
1. What is your conception of your role in relation to psychotropic drug use byadolescents?
2. How do you conception your role in relation to psychotropic drug use byadolescents?
Individually adapted follow-up questions were also asked such as: Can you give me an example? Can you tell me more about that? Can you explain that a little more?
Participants (III, IV) Study III
All the participants were recruited from an association for young people with mental health problems, the Mental Health Youth (MHY). This is an interest group for young people aged up to 30. The organization operates through its members. Their aims are to work for openness about mental health problems, prevention of mental distress and a better health service (Mental Helse Ungdom, 2012a).
31
Information about the study was made available on MHY websites. In addition the leaders of the MHY sent information about the study in one of their regular letters to all the members (Mental Helse Ungdom, 2012b). Young people aged between 16 and 24 years with experience of psychotropic drug use were invited to participate. One reminder was sent out via the website. Ten adolescents contacted the researcher by mail or SMS. One was too old and one did not respond again despite two reminders. After two reminders eight young people wanted to participate, altogether six girls and two boys participated. All participants had experience of psychotropic drug use. They were aged 17–24 years (mean = 20.87, SD = 2.99 years). Three were high school students, two worked, two were university students and one received disability benefit. They came from seven counties in Norway. The data collection took place between December 2012 and March 2013.
Study IV
Recruitment was accomplished by contacting leaders of the PHNs in different municipalities in three counties and two county authorities in the eastern part of Norway. The leaders were asked to identify PHNs working with adolescents and an information letter about the study was sent to the participants. Thereafter the researcher phoned potential PHNs to confirm participation in the study and make an appointment for an interview. Twenty-two PHNs were asked to take part in the study; two declined. The participants were strategically selected and had different background characteristics. So, 20 PHNs working with adolescents in various primary health services were included, and they worked in lower secondary schools (n = 3), upper secondary schools (n = 12), high schools (n = 12), public health for adolescents (n = 6), websites for adolescents (n = 1), follow-up services for adolescents who have dropped out of school (n = 1) and a ‘family team’ (n = 2).
All participants were women aged between 35 and 63 years (mean = 51.5, SD = 7.78 years). They had experience as registered nurses of 14–33 years and as PHNs of 3–27 years (mean = 14, SD = 7.16 years). All had additional education as PHNs and all but one had other additional qualifications. The data collection was performed between October 2011 and March 2012.
32
Data analysis (III, IV)
Study III Qualitative content analysis of Graneheim and Lundman was used (Graneheim & Lundman, 2004; Lundman & Graneheim, 2012). The audio-taped interviews were transcribed verbatim. The interviews were read through several times to get a sense of the whole. The manifest content analysis was made by the first author. Then the whole text about the participants’ experience of psychotropic drug use was divided into meaning units, which were subsequently condensed. The condensed units were abstracted and encoded. Thereafter the various codes were compared based on differences and similarities, and sorted into seven subcategories and three categories; these constitute the manifest content. The tentative categories were discussed by the four researchers and revised. A process of reflection and discussion resulted in agreement about how to sort the codes. Quotes were chosen to illustrate the category in question.
Study IV
A phenomenographic analysis, following that of Alexandersson (1994), was used to describe how the PHNs conceived their role in relation to psychotropic drug use among adolescents.
Phenomenographic ontological assumptions are subjective. ‘At the root of phenomenography lies an interest in describing the phenomena in the world as others see them, and revealing and describing the variation therein’ (Marton & Booth, 1997). The world exists, and different people construe it in different ways using a non-dualist viewpoint: there is only one world, one that is ours and one that people experience in many different ways. What do the participants conceive and how do they describe the phenomenon (Marton & Booth, 1997).
The result of a phenomenographic study is a set of categories describing the qualitative variations in empirical material. These categories are related to each other because they include different conceptions of the phenomenon. This is a whole expressing the outcome space (Alexandersson, 1994).
The methodological procedure is described below and follows Alexanderssons (1994) four steps.
33
Step 1. The audio-taped interviews were listened to, to familiarize ourselves with the data and gain an overall impression. The transcribed interviews were read several times to identify statements related to the questions mentioned earlier. All the statements were identified, e.g. in the way that the situations were described, emphasized or described throughout the interview.
Step 2. Afterwards more systematic work was begun to try to identify patterns of similarities and differences in statements described by the PHNs, and to contrast them. When all the statements had been analysed, the intention was to understand the PHNs’ conceptions, and bring attention to the different parts of the whole and how they relate to each other.
Step 3. The identified conceptions were collected into categories with similar interpreted content. In this way an overall view of the different descriptions was collected and the links between them considered. The preliminary descriptive categories of conceptions were determined.
Step 4. The transcripts were investigated to see whether the descriptive categories agreed with the PHNs’ conceptions and attention was paid to the relationship between the descriptive categories and the whole of each transcript. This particular outcome space captures the role of the PHNs. Three descriptive categories, which have a logical association with each other, were found and revealed distinctive ways in which PHNs conceived their role in relation to psychotropic drug use among adolescents.
Ethical approval and considerations (I–IV)
Each study was conducted according to the Ethical Guidelines for Nursing Research (Northern Nurses`Federation, 2003) and the, Code of Ethics for Nurses (International Council of Nurses, 2012).
Studies I and II
This study is part of the project ‘The epidemiology of prescription drug use. A record-linkage study in Norway’, led by senior researcher Aage Tverdal at the NIPH, which was endorsed by the Regional Committee for Medical Research Ethics. The record linkage was approved by the Norwegian Data Inspectorate, according to current Norwegian law (Act of Personal Health Data Filing System 2002).

34
The identification numbers used in this study are encrypted. The researchers have, at no point, had access to information that might expose the identity of individuals, for example the exact birth date. The pharmacy records of dispensed drugs are electronically and automatically transferred through Statistics Norway before arriving at the NIPH and being included in the NorPD. Statistics Norway acts as a so-called trusted third party centre and is party to data protection to ensure confidentiality of personal information (Furu, 2008). This means that the identity of patients and prescribers has been encrypted according to Norwegian legislation (Act of Personal Health Data Filing System 2002), but nevertheless individualized so that it is possible to follow individuals over time and carry out record-linkage studies. Data linkage is based on the unique identification number system that is available in all the Nordic countries.
Study II
The data is anonymous and there is no requirement for appraisal from a regional ethical committee or the NSD. Data in this study is retrieved from the NorPD. Data used is owned by the NIPH. Access to the data is partially possible on the website www.norpd.no.
Study III
Approval for this study was received from the NSD (No. 26817). The principle of autonomy was followed by the principles of voluntariness, informed consent and confidentiality. The participants received written and verbal information about the voluntary nature of participation and the right to withdraw at any time, with no need to explain (Northern Nurses’ Federation, 2003). The phone number and address of the first author were given to all the participants in the event of any questions.
If the young people had any problems after the interview they were told to contact the health service, and had also the opportunity to call the first author. None of the young people has contacted her. There are considerations to make before involving young people in research. In this study two of the participants were aged <18 years. A principal rule when young people aged <18 years participate in research projects is to obtain parental consent. In this study, the NSD considered that the management of the young people’s personal data could be done by them (Act of the Protection of Personal Information, 2000):
35
the management of personal data is necessary for the study’s goal and the questions relate to the adolescents’ own mental distress and psychotropic drug use. Furthermore, this is justified by the Act of Patients’ Rights (1999) and the Act of Medical and Health Research (2008) which state that people aged >16 years are competent to consent.
Talk of mental distress and psychotropic drug use may put a strain on those adolescents under mental distress. On the other hand, adolescents’ mental distress, psychotropic drug use and treatment need to be mapped out with descriptions from those involved.
The participants chose the place for the interviews. Particularly when interviewing the adolescents and young people, the first author become aware of the participants’ reactions and whether they felt comfortable in the situation.
Study IV
The NSD gave its permission for this study (No. 26817). All the PHNs in this study were competent to consent and ensure their own autonomy. They were given written and verbal information about the voluntary nature of participation and the right to withdraw at any time, with no need to explain (Northern Nurses’ Federation, 2003). The phone number and address of the first author were given to all the participants in the event of any questions.
36
Main results
The results are presented in four sections with subgroups, followed by a summary. The first section is about mental distress, health and lifestyle habits and social factors among young people, in the total population, and according to gender (I). The second section is about psychotropic drug use, in the total population and according to gender (I, II). Thereafter, young people’s experience of psychotropic drug use is presented (III). Finally, the role of PHNs in relation to psychotropic drug use by young people is described (IV). A summary of the results is given at the end of the chapter.
Mental distress, health, lifestyle habits and social factors (I)
Total population
In the total study population of 15-16 years old non-users of psychotropic drugs, 15.5% reported mental distress. In total, unfavourable lifestyle habits were more frequently reported among adolescents reporting mental distress compared with those not reporting mental distress. A larger number of the former group experienced poorer general health and higher numbers of pain sites than the latter group. Furthermore, the prevalence of unfavourable lifestyle habits, such as moderate consumption of alcohol, smoking daily and a lower level of physical activity, was also more frequently reported among the adolescents reporting mental distress.
Gender differences
Girls reported mental distress more frequently than boys, 22.8% and 7.4%, respectively. In total, the girls, both those with and those without mental distress, reported poorer general health and lifestyle habits than the boys. Physical activity was reported to be lower among the girls, and they also reported a higher number of sites of pain than the boys.
Psychotropic drug use (I, II)
Total population
Mental distress was independently associated to incident psychotropic drug use 1–9 years after the adolescents participated in the NYHS. Other factors associated with psychotropic drug use were smoking, poor general health, increasing number of pain sites (experienced over the previous year), lower
41
services, and feeling like a ‘guinea-pig’ when physicians are not sure what psychotropic drug to use.
It’s a pity they do not know more about the effect of the psychotropic drugs. The patients become ‘guinea-pigs’. I have to have the psychotropic drugs, so of two evils…
The young people had to find out information about their drug on their own. Neither the school health service nor other health services were easily accessible to them. They could not locate the school health service and, when they did, and visited the PHN, they felt that the PHN’s focus was on diet and sleeping. A lack of coherent services was also experienced across different levels of the health services. Other young people were satisfied with their treatment and follow-up.
The young people’s social lives were influenced by the psychotropic drug use which they tried to hide from family and friends. They experienced that their families were ashamed of them as psychotropic drug users.
My parents? No, they do not understand the mental health problems and drug use. They tell me to find a job because that will make me better.
The young people did not tell others about their psychotropic drug use because of the reactions and opinions of these others. They felt lonely and stigmatized at school and work.
The public health nurses’ roles in relation to psychotropic drug use among adolescents (IV)
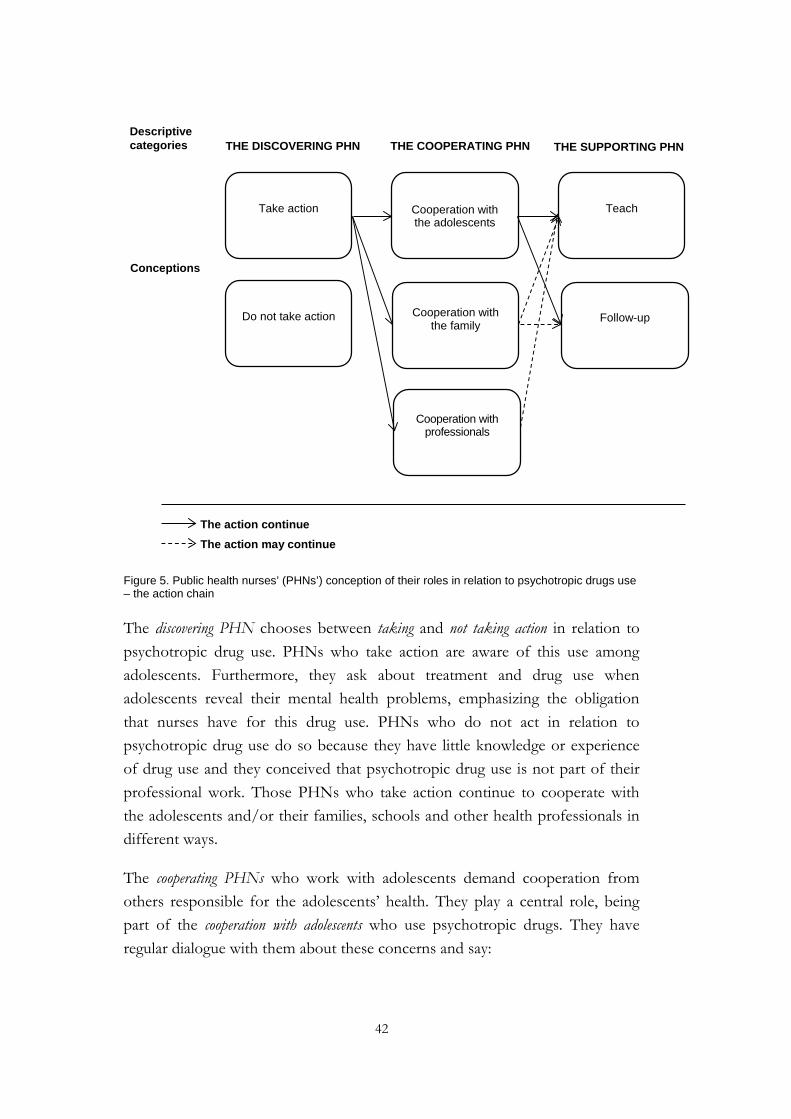
The PHNs’ conception of their roles in relation to psychotropic drug use indicates three roles: the discovering, the cooperating and the supporting PHNs (Figure 5).
42
The action continue The action may continue
Figure 5. Public health nurses’ (PHNs’) conception of their roles in relation to psychotropic drugs use – the action chain
The discovering PHN chooses between taking and not taking action in relation to psychotropic drug use. PHNs who take action are aware of this use among adolescents. Furthermore, they ask about treatment and drug use when adolescents reveal their mental health problems, emphasizing the obligation that nurses have for this drug use. PHNs who do not act in relation to psychotropic drug use do so because they have little knowledge or experience of drug use and they conceived that psychotropic drug use is not part of their professional work. Those PHNs who take action continue to cooperate with the adolescents and/or their families, schools and other health professionals in different ways.
The cooperating PHNs who work with adolescents demand cooperation from others responsible for the adolescents’ health. They play a central role, being part of the cooperation with adolescents who use psychotropic drugs. They have regular dialogue with them about these concerns and say:
Descriptive categories
Conceptions
Cooperation with professionals
Cooperation with the family
Cooperation with the adolescents
Follow-up
Teach Take action
Do not take action
THE DISCOVERING PHN THE COOPERATING PHN THE SUPPORTING PHN
43
The majority of these adolescents remain my responsibility.
PHNs cooperate with adolescents for long periods and place them in a position of cooperating with professionals, such as specialist health care.
Family cooperation is seen as important:
When an adolescent has a hard time, is suffering, we have a close relationship with the family, too.
But the older the adolescent is the more rarely the family is involved. When cooperating with teachers, PHNs help adolescents to plan a parallel course – attending school while receiving treatment.
PHNs make contact with other authorities and describe routines for referral to specialist health care. However, neither specialist health care nor family doctors have the duty to ask for a PHN’s cooperation.
If cooperation could be established, the supporting PHN could teach and follow-up the adolescent in their psychotropic drug use. Supportive PHNs support adolescents in managing their mental health problems and psychotropic drug use through teaching and follow-up. They have personal interactions that vary from providing a space for reflection to learning to direct active teaching.
As distinct from hypnotic drug use, antidepressants were more often the responsibility of the physician:
The physicians prescribe the antidepressants and have the responsibility to follow it up.
Adolescents with depressive or anxiety afflictions were described as belonging to specialist health care. PHNs conceived that these adolescents needed tighter follow-up than they could give, and also that the PHNs were not themselves professionally qualified to follow them up.
44
Summary of the results
The overall aim of this thesis was to study mental distress, health and life style habits, social factors and subsequent use of psychotropic drug use by young people, and how PHNs conceive their roles in relation to this. When summarizing the results as a whole:
• 15.5% of 15-16 year old non-users of psychotropic drugs reported mental distress in 2000-2003, of whom three out of four were girls. The adolescents with mental distress were characterized by poor self-perceived health and unfavourable life style habits. As regards social factors, a greater proportion had plans for vocational education and lower family income (I).
• There was an association between young people who reported mental distress at 15-16 years, and incident use of psychotropic drugs one to nine years later. Other factors associated with psychotropic drug use one to nine years later were smoking, poor general health, increasing number of pain sites (experienced over the previous year), having plans for vocational education and lower family income (I).
• 25.4% of all 15-16 year olds reporting mental distress became new users of psychotropic drugs one to nine years later. In total, 18.3% of the boys and 27.7% of the girls (I).
• The use of psychotropic drugs among 15-16 year olds increased during the period 2006–2010. Hypnotic drugs and melatonin in particular, accounts for most of the increase (II).
• The annual amount of dispensed melatonin among 15-16 year old users is high and corresponds to a more regular use throughout the year. Other subgroups of hypnotics are dispensed to users in annual amounts corresponding to sporadic or short-term use (II).
• In total, one of six incident psychotropic drug users aged 15-16 years in 2007 still has a psychotropic drug prescription dispensed in 2010 (II).
45
• Young people experience psychotropic drugs as beneficial, but have also undesired effects. They expected more professional support and follow-up (III).
• Young people experience that their social lives with the families and friends, school and work were negatively influenced by the psychotropic drug use (III).
• The PHN who becomes aware of psychotropic drug use chooses either to act or not to act in relation to psychotropic drug use. The PHNs who take action continue to cooperate with the adolescents and/or their families, schools, and other professionals. If cooperation was established between the PHN and the adolescent, the supporting PHN teaches and supports the adolescent in relation to psychotropic drug use (IV).
46
Discussion of main results
Young people with mental distress will be discussed below followed by a discussion about psychotropic drug use by young people, and the PHNs’ conceptions of their roles in relation to psychotropic drug use.
Young people under mental distress (2000–2003)
In this thesis the prevalence of mental distress reported among 15–16 year old none-users of psychotropic drugs during 2000–2003 was 15.5% (I). Corresponding figures are reported in other studies (Mykletun et al., 2009; The Ministry of Health & Care, 2013; Torsheim et al., 2006). Anxiety and depression are reported to be the most frequent mental health problem among young people (Costello et al., 2003; Merikangas, 2005). The prevalence of mental health problems varies between countries, but different studies estimate that 20% will experience anxiety while growing up. Half of these will experience disability in relation to their mental health problems (Costello et al., 2003; Mathiesen et al., 2007). It is difficult to summarize data on the prevalence of mental distress among young people and international studies have shown rates of mental distress from 8% to 57% (Patel, 2007). Patel (2007) states, that one of four to five young people will be under mental distress in any given year if these studies are taken together.
However, a recent study of 40 000 young people aged 13–16 years in Norway reported that young people experienced good general health, although at the same time several struggle with mental health problems (Ungdata 2010–1012, 2013). Three of four young people report that they believe in the future and think that they will have a good and happy life (Ungdata 2010-1012, 2013). Nevertheless, too many still struggles with mental health problems, including sleep problems, a feeling of hopelessness and a low self-image; 10% struggle with a high level of mental distress. Approximately half of all Norwegians will be affected by mental health problems during their lives (Larsen, 2010) and mental health problems among young people seem to be a challenge to public health. Although, the general level of health is god, socioeconomic distribution of mental health problems still poses a challenge (The Ministry of Health & Care, 2013).

47
A gender difference in mental distress was observed among 15–16 year olds in our study; one of five girls reported mental distress in 2000–2003, which was three times higher than among the boys (I). This gender difference corresponds well with the work of Hagquist (2007) who also described an increase in mental health problems with increasing age, particularly among girls in Sweden, and especially 15-year-old girls. The differences between the genders may have several explanations. Both girls and boys describe themselves as feeling pressed to act within the ‘guidelines’ and ‘rules’ of their peers if they want to be accepted (Maclean et al., 2010). Perhaps, these commanding ‘rules’ make boys more reluctant to seek help for illness in general, and for mental health problems in particular. Girls tend to feel worse and show more depressive symptoms. Boys are more likely to act out and consider their strengths and good health as part of their growing masculinity (Cavallo et al., 2006). Before the onset of adolescence, an equal proportion of girls and boys reported mental health problems. However, by age 13, a shift took place, and more than twice as many girls as boys reported that they were depressed at age 15, a gender difference that continues into adulthood (Storvoll & Wichstrøm, 2003). Thus, one explanation to the observed gender difference in mental distress in this thesis (I) may be that the HSCL instrument captures symptoms of mental distress more prevalent in girls, and not those in boys.
In our study, and in both genders, those with mental distress reported considerably poorer general health and higher numbers of pain sites compared with the rest of the study population (I). Among the girls with mental distress, 94% reported pain at one or more sites. Furthermore, poor self-reported health and increasing number of pain sites in those aged 15–16 years were both independently associated with later initiation of psychotropic drugs, irrespective of self-reported mental distress status at baseline. The association between pain and mental distress is well known from the literature. Ando et al., (2013) reported, in a study of 18 000 young people, that a large number of pain sites is associated with mental health problems. Physical pain seems to be a possible marker of mental health problems among young people, especially girls. When young people talk about somatic pain, professionals should ask what other pains have been experienced and consider mental health problems, especially when young people report a number of pain sites.

48
The existence of social inequalities in health, including mental health, is well known from the literature, and has been seen in this thesis as well. Mentally distressed individuals had a higher prevalence of markers of a lower socioeconomic position, in terms of poorer self-reported family economy, and a larger proportion with future plans for vocational education, compared with those not reporting mental distress (I). They were also together with a lower perceived family income, independently associated with drug use 1–9 years later. Relevant to this, family economy is a well-known predictor of young people’s health (Chen, 2006). Cost may restrict families’ opportunities to encourage healthy behaviors such as participating in physical activities, access to health resources and helping with psychosocial stress (Currie et al., 2012). Health, including mental health, is possibly a socially created condition, depending on varying circumstances, opportunities and health-related behaviour. In Norway there are concerns about growing variations in patterns of social inequalities in health. The variations in health may be equalized through the alteration of social factors such as family economy and education (The Norwegian Directorate of Health, 2010).
The young people in this thesis (III) report that the prescribed psychotropic drugs gave undesirable effects leading to health complaints and the circumstances around their mental health problems made challenges to their social life. They had problems with school attendance and work, and struggle in relation to their family and friends. This is in line with the study by Breslau et al., (2008), who reported that mental health problems occurring early in life are associated with adverse health during the school years. Mental health problems can also lead to lifelong decrements in economy and social functioning. The young people (III) experienced a life of mental health problems. They avoided telling other people, including their closest family, about these problems because they were anxious about reactions and the fear of being stigmatized. They were aware of the problem with not telling anyone – no one had the possibility to help either (III). Eisenberg et al., (2009) found that help seeking increased if the young people reduced personally held stigmatizing attitudes rather than others’ perceptions. So, the fear of letting others know may reduce the possibility of adjusting school and work life to their needs, and result in missed opportunities for a better life. Worldwide, mental health problems are one of three main causes of years lost by those aged between 10 and 24 years (Gore et al., 2011).
49
The prevalence of mental health problems among young people, with differences between the genders, as well as between socioeconomic groups (Currie, 2012) may have consequences for health promotion strategies among young people, and should emphasize the differences between socioeconomic groups as well as between boys and girls. Young people with mental health problems may need support and follow-up from the health services and some of them struggling with mental health problems may need psychotropic drugs for a short or longer period. The years of growing up seem to be a vulnerable period with physical and emotional transformations. On the basis that this period may be formative for health-related behaviour for the rest of their lives (WHO, 2009a), it is important to map young people’s mental health, lifestyle and social and other factors that influence this.
Psychotropic drug use by young people
In both genders, incident use of psychotropic drugs before the age of 25 was doubled among those who reported mental distress at age 15–16 years, compared with the rest of the study population (I). Mental distress had an independent effect on incident psychotropic drug use. Thus, the initiation of psychotropic drugs was primarily driven by mental distress, which is to be expected because mental distress is an indicator for use in the first place. Still, as many as a quarter of all females with mental distress at age 15–16 years, but not yet using psychotropic drugs, had retrieved at least one prescription of psychotropic drug therapy 1–9 years later to manage it (I).
In this thesis a nation-wide prescription database study showed increasing psychotropic drug use by 15–16 year olds between 2006 and 2010 (II). In parallel, psychotropic drug use has been reported to increase among young people, especially in western countries. Zito et al. (2008a) describe the increase in prevalence among young people in the UK, Germany, Italy, Denmark, the Netherlands and the USA over the last decades.
In study II hypnotic drugs constituted 75% of all psychotropic drugs dispensed to 15–16 year olds, and hypnotic drugs increased by 40 % during 2006 and 2010. Hartz et al. (2012) have reported that there has been an increase in hypnotic drug use among children and young people in general in Norway, not just among 15–16 year olds. The most striking observation in study II was the increase in use of melatonin over the period, which accounted for most of the
50
increase in hypnotic drug use. In addition, the annual amount of melatonin dispensed between 2007 and 2010 among users indicated more than sporadic use of this hypnotic. For example in 2008 fifty per cent of the male melatonin users had an annual amount dispensed corresponding to use of one defined daily dose (1 DDD) every second day or more throughout the year, and 25% filled melatonin prescriptions corresponding to use of more than 1 DDD every day over a year. The annual amount of dispensed melatonin to 15-16 year old users is high and corresponds to more regular use throughout the year, compared with the use of other subgroups of hypnotics, which are dispensed in annual amounts corresponding to sporadic or short-term use (II).
Obviously, melatonin has acquired a major role in the treatment of adolescent sleep problems in Norway, in parallel with observations in an earlier study (Hartz et al., 2012). In Norway, and EU, melatonin is indicated as monotherapy for short-term treatment of primary insomnia, characterized by poor quality of sleep among patients aged 55 years and older (European Medicines Agency, 2013). Melatonin is not approved for use in children and adolescents below age 18 because of insufficient data on safety and efficacy. Melatonin is a hormone with diverse physiological functions, related to the regulation of circadian rhythms and seasonal behaviour, sexual development, retinal physiology, tumour inhibition, and antioxidant, immunomodulatory and anti-ageing properties (Hardeland, 2011, 2012). There has been concern that high melatonin levels from external sources may postpone puberty onset (Srinivasan et al., 2009; Lampiano et al., 2013). However, most studies on melatonin are short term, typically up to four weeks. One observational study evaluated the use of melatonin over three years and its effect on pubertal development, and concluded that melatonin is safe (Geijlswijk et al., 2011). However, the study was small and had other limitations, such as drop-out from reporting pubertal development. Thus, in view of the increasing and regular off-label use in adolescents, more long-term studies seem to be warranted.
Use of anxiolytics and antidepressants by 15–16 year olds were stable throughout the period 2006–2010 (II). Antidepressants were, however, the most common psychotropic drug used long term by adolescents. After four years, almost a quarter of new users in 2007 still filled a prescription for antidepressants in 2010. This may be expected because treatment with antidepressants is recommended for some time after it has been started
51
compared with, for example, hypnotics that are recommended for short-time use only. Girls were more often prescribed antidepressants than boys, possibly due to the fact that they are more likely to present with mental health problems (I) and to ask their physicians for help (Hansen et al., 2009).
Young people interviewed in this thesis experienced both beneficial and undesirable effects of the psychotropic drug prescribed (III). Beneficial effects allowed them to be part of society: feeling good, having more energy, maintaining a level of health, and being with friends. On the other hand, they experienced side effects and adverse events, which included emotional and physical complaints, making them unsure about the medication. Sometimes this resulted in a decision to stop therapy (III). Only a few psychotropic drugs have been approved for use by people aged less than 18 years, and 50% or more of psychotropic drugs used by young people have never actually been studied in this population (European Medicines Agency, 2007). Most psychotropic drugs used by young people are licensed for adults and have not been fully tested on young people. This off-label use of drugs is widespread due to lack of studies on their use (Hsia & Maclennan, 2009).
Adverse drug reactions such as restlessness, subdued emotions, sedation, depression, irritability, hallucinations and dissociation, and somatic symptoms such as losing consciousness, weight gain, fatigue, trembling and cessation of periods, were described by the young people in this thesis (III). Similar effects have also been reported in other studies among young people. Effects such as fatigue and feelings of losing conscious have been reported by other young people taking antidepressants (Safer & Zito, 2006). A review reported adverse effects from psychotropic drugs such as: affect labiality, sedation, increased body weight, hallucinations and physical symptoms such as weight gain, fatigue, trembling and cessation of periods (Safer, 2011). Professionals have to monitor young people who are taking psychotropic drugs closely, and maintain vigilance over those who use drugs for an extended period (Corell et al. 2006).
The young people in this thesis was uncertain in relation to professional’s knowledge because the lack of adequate information about the psychotropic drug from their physicians. After trying out different drugs they resigned themselves to finding one that had the best effect and described that they felt like a ‘guinea-pig’ (III).
52
Physicians and other professionals involved in the support and follow-up of young people prescribed psychotropic drugs must pay special attention to the potentially adverse effects. The young people must have close follow-up, especially because of the scarcity of evidence on the safety and efficacy of use the drugs in this population. In the present study the young people missed out on access to professional support and follow-up, and described the service as occasional and dependent on the individual health professional (III). Corell et al. (2006) stated that physicians and caregivers need to be aware of the different adverse effects of psychotropic drugs and to make more careful selection of choice of drugs. They need to search for drugs with the risk of as few adverse events as possible. Healthy lifestyle counselling and close health monitoring are needed to maximize the effectiveness and safety of these drugs.
Nevertheless, although psychotropic drugs may be effective in reducing mental health problems, they raise questions about increasing use, side effects, long-term treatment and off-label use by young people; this, in turn, may warrant tight follow-up once therapy has been started.
The public health nurses’ role in relation to psychotropic drug use by young people
In this thesis 20 PHNs working with young people in various primary health services were interviewed about their conceptions of psychotropic drug use and their role in relation to this (I). Three categories of PHNs conceptions emerged from the analysis: the discovering, the cooperative and the supportive PHN.
The discovering PHN (IV) chooses between taking and not taking action in relation to young people using psychotropic drugs. PHNs who took action had knowledge of psychotropic drugs and emphasized the obligation that nurses have in relation to this. The young people missed access to the school health service and experienced lacking knowledge of mental health problems and psychotropic drugs from health professionals (III). The regulations for the school health service say that the target group must have access to the service and that staff have the necessary competence and resources (The Norwegian Directorate of Health, 2003a). It must be a service that is easy to visit and a place where the young people are taken seriously, whether their health challenges are minor or major. It must emphasis groups with special problems such as those with mental health problems. The regulation says that

53
professionals in the school health service may give advice and counselling in relation to handling of medication and contribute to necessary education. Young people who visit a PHN have the right to the best possible treatment and assistance in rehabilitation (Act of Patients’ Rights 1999; UN Convention on the Rights of the Child, 1989).
In addition to the formal demands, the PHNs have other demands in relation to the young people whom they meet. Clancy and Svensson (2007b) was concerned with aspects of responsibility among Norwegian PHNs and asked about the essence of ethical responsibility, which can be seen in connection with the discovering PHNs and their choice in taking or not taking action in relation to young peoples´ drug use. The philosopher Levinas says that the responsibility for the ‘Other’ cannot be avoided, ignored or transferred (Levinas, 2008). Clancy and Svensson (2007b) stated, with reference to Levinas, that a PHN’s responsibility is personal and infinite. She found, in her study, that the PHNs felt much more personally responsible than hospital nurses, because their work was mainly in isolation. In this thesis (IV) some of the PHNs felt responsible for the young people using psychotropic drugs and acted in relation to psychotropic drug use; others did not. Those PHNs who chose not to act explained that this was because they had little knowledge of or experience in drug use among young people. This can also be seen in connection with the young people who worried about professionals’ knowledge (III). The PHNs (IV) were uncertain and perhaps a bit worried about what being a PHN meant. They referred to their health-promoting role. This limited understanding of their role should be challenged. Ethics can help nurses to understand that their work involves fear, worry and uncertainty, not just work within their predictable ‘comfort zone’ (Clancy & Svensson, 2007b).
As a PHN, a health problem concerning young people is not a problem that you can avoid because you don’t have the knowledge. The regulations state that existing knowledge must be taken into account (The Norwegian Directorate of Health, 2003a). If you have no knowledge or competence then you, as a professional, must seek to gain the knowledge and competence necessary to meet the needs of young people. Though different barriers may hinder the PHNs possibility to develop their knowledge, health care professionals are obliged to work evidenced based (Griffiths et al., 2001).
54
Often the PHNs in Norway work with young people with no involvement of other. Still, they are dependent on cooperation with others, and this cooperation is also with the young people and other individuals/services, such as the families, schools, family doctors, and primary and specialist health care. PHNs see themselves as central to the cooperation, the ones who are the first to meet the needs of the young people, take the initiative and demand cooperation from those responsible for the young people’s health (IV).
Cooperation and coherent services were analysed some years ago; it was found that there was a lack of cooperation and coordination within the Norwegian health services at all levels (The Ministry of Health and Care, 2005). This was followed up by the Coordination Reform (The Ministry of Health and Care, 2012) and became an important tool for the central authorities to make improvements. According to the regulations, the school health service has to contribute towards good psychosocial and physical environments at the schools and participate in promoting a healthy lifestyle (The Norwegian Directorate of Health, 2003a,b). PHNs tend to conceive their role within the school health services as solitary work, and this conception may give little room for cooperation. PHNs work within their own networks and thus reduce chances of cooperation with other professionals (Clancy & Svensson, 2009). The PHNs in this thesis (IV) conceive limited opportunities to cooperate with the physicians. Some years ago physicians in the municipality were one of the professionals with whom PHNs had a close ‘natural’ cooperation and Clancy (2010) reported that the physicians were an important cooperative partner for PHNs before the family doctor system was introduced in Norway in 2001. Afterwards there has been a discussion about the family doctors connection and participation to the school health service. The opinion to several family doctors were that their work in the school health service could be completed from their offices, which do not fulfil the intention about the school health service as a holistic, interdisciplinary and easy accessible service to the young people (The Norwegian Directorate of Health 2003b). Sufficient access to the health services is experienced by the young people
The PHNs refer young people to other health professionals, but the cooperation is conceived as problematic (IV). A lack of agreement and routines make cooperation difficult. The individual municipality is responsible for putting in place the exact guidelines for cooperation (The Norwegian Directorate of Health, 2003a).
55
In the supporting role, the PHNs teach and support young people about psychotropic drug use (IV). The dialogues with young people can be seen as health dialogues, as described by Borup (2002), and are different stages in the creation of communication, which provide healthy reflections and changes. Golsäter et al., (2010) described an outcome of the health dialogues as giving young people the opportunity to gain knowledge about, and insight into, individual health problems and to be given advice. This gives young people the opportunity to discuss their health individually and openly (Borup & Holstein, 2007), and to receive information about the drug used in a supportive way.
PHNs are engaged in their public health work, health promotion and illness prevention. Some felt that their task was not to act in relation to young people struggling with mental health problems and psychotropic drug use (IV). Individual patient work may take time and resources from the health-promoting work within the municipality. Povlsen and Borup reported (2011) the individual patient perspective to be demanding of resources and results in less chance to see large groups of patients such as those with chronic diseases. Some of the PHNs (IV) conceived the follow-up of young people as demanding and to require resources to which they did not have access.
On the other hand, by supporting and following up young people, PHNs were engaged in helping them to make use of their own individual resources. Those PHNs working with individuals saw this as health promotion: they could help and support young people in realizing their own strengths and possibilities (IV). Pryjmachuck et al., (2012) concluded that PHNs (school nurses) can be engaged in mental health work in their role as public health specialists, by focusing on health promotion and early intervention. PHNs have to articulate and develop their role according to the challenges within the community and society in general.
56
Methodological considerations
The two quantitative studies (I, II) served well to describe mental health problems, health and lifestyle habits, social factors and subsequent psychotropic drug use, together with prevalence and recurrent use of psychotropic drugs by adolescents and young people. This provided a way into the qualitative studies (III, IV) which provide a deeper insight via individual interviews with young people and the PHNs. Nursing research embraces both quantitative and qualitative research methods in order to investigate the whole of nursing and the two methodologies complement each other. Quantitative research is needed to control the phenomena and predict interventions and qualitative research is needed to identify the characteristics of the phenomena (Polit & Beck, 2008).
The quantitative studies
Epidemiology is about exposure, everything that people can be influenced by and illness. It is interesting to what extent there is a relationship between the exposure (other factors) and the illness (Field, 2009; Rothman & Greenland, 1998). Important aspects to assess the quality in quantitative research are validity and reliability. In order to achieve high validity, high reliability is necessary, but high reliability does not call for high validity. Validity is to what degree, the questions really measure what it intends to measure and the reliability; if it produces similar results under consistent conditions (Field, 2009; Polit & Beck, 2008).
Survey data were captured from the NYHS (I) and register data from the NorPD (I, II). An overall goal in epidemiological studies is to measure the value of parameters, such as health and lifestyle habits and social factors as accurately as possible (I). Thus, when interpreting the results, it is essential to consider how much the observed association between mental distress, health and lifestyle habits, social factors such as education plans, family economics and their association to psychotropic drug use may have been affected by errors in the design, data collection and analysis of the study (I) (Field, 2009; Rothman & Greenland, 1998).
The internal validity refers to whether or not the results of a study are valid for the individuals being studied and nor the result of chance (Rothman & Greenland, 1998). Two main types of error may occur: systematic and random.

57
Usually, the amount of random error will decrease, and the confidence interval around the point estimate will be narrower, with increasing sample size. Hence, the first way to increase precision in epidemiological studies is to enlarge the study population. The data used from the NorPD cover the entire population and the NYHS used, had a large sample; data from 11 947 adolescents in five of the counties, so problems with random error were considered to be small (I). However, division of the population into many strata such as according to age, gender and mental distress may result in less precise estimates in each stratum as reflected broader CI.
The main types of systematic error are selection and information bias. Selection bias is a skewedness of the measurement of an estimate. Polit and Beck (2008) reported that ‘bias seldom can be avoided totally because the potential for its occurrence is so pervasive’ (p. 197). Samples of participants included in a study may not be representative of the population in whom the conclusions have been interpreted. The main source of selection bias in survey studies is non-response, either non-attendance or a missed response to a single-item questionnaire (Rothman & Greenland, 1998). Together they had an attendance rate of 84%, which probably made selection bias a minor problem in this study (Winter et al., 2005). The participants completed the survey at school with a project assistant present to help with possible misunderstanding. This could also have ensured the quality of the data, e.g. a missing response to items in the HSCL score was n = 123, out of 10 706; this made the missing response to this item, which constituted our main independent variable, a minor problem. Thus, the more severe mentally distressed young people may have been excluded from the study, because they were not present at school that day or did not want to fill in the questionnaire.
Information bias is related to the accuracy of information collected on different variables, such as mental distress and the other variables. The quality of self-reported data depends on perception and interpretation of survey questions. Most of the variables used in study I are based on self-reported data, so errors could occur due to inaccurate recollection or misinterpretation of questions. What kind of question is asked affects how the participant answers it (Polit & Beck, 2008). Probably, questions about physical exercise may be answered more positively than questions about cigarette smoking.
58
Mental distress was measured by the HSCL-10, which has proved to have satisfactory validity and reliability (Strand et al., 2003). In this thesis the internal consistency, using Cronbach’s α, was 0.85 which is considered to be good (Polit & Beck, 2008). The HSCL-10 captures self-reported symptoms of depression and nervousness over the previous week. An inherent limitation is that information from a week ago can be inaccurately recalled and reported. HSCL-10 captures symptoms of depression and nervousness, not externalizing behaviours. Adolescent boys are more likely to exhibit these behaviours, which may lead to an underestimation of the prevalence of mental distress among boys in our study (Maclean et al., 2010). Study I is prospective, using a nationwide register as an end-point, which implies minimal risk of selection or information bias. The complete national prescription register and the use of the unique 11-digit personal identity number assigned to all Norwegian citizens ensure valid data linkage at an individual level between the questionnaire and the register. The study could not assess whether these findings were valid for other age groups.
In study II data from the NorPD was used. An important advantage of using register-based information is that it circumvents the common problem of underreporting psychotropic drug use (Nielsen et al., 2008; Skurtveit et al., 2008). Errors in measurement such as selection bias are eliminated through the use of a comprehensive national prescription register of psychotropic drug use; this removes inadequate recall by respondents. Information- and recall bias is eliminated due to detailed information on the prescription. The person does not have to recall any information about the prescription.
However, lack of information on adherence is always an issue when reporting prescription data for drug use. We do not know how many of the drugs purchased were actually taken. In some countries, misuse has become a problem among adolescents and young people. Furthermore, sharing prescription drugs, and getting prescription drugs from a relative or friend, seems to be a trend (Apa-Hall et al., 2008). This may have led to under- or overestimation of drug use in this study. Furthermore, adolescents in hospitals and institutions are not registered in the Norwegian Prescription Database, and were not taken account of. Another limitation is that we do not have any information on the indications for use of the study drugs.
59
The qualitative studies
Qualitative content analysis was chosen to analyse the transcribed interviews with the young people (III). The qualitative content analysis deals with what the text says e.g. the content aspect and describes the visible, obvious components, referred to as the manifest content (Graneheim & Lundman, 2004; Lundman & Graneheim, 2012; Polit & Beck, 2008).
A phenomenographic approach (Alexandersson, 1994) was used analysing the PHNs conceptions (IV). The phenomenographic approach allows PHNs to discern and describe the different ways in which they conceived the phenomenon – their role in relation to psychotropic drug use. The approach explores how people describe their experiences of something or how something appears to them.
To develop trustworthiness the criteria; credibility, dependability, confirmability and transferability were used through the research process (Lincoln & Guba, 1985; Graneheim & Lundman, 2004; Lundman & Graneheim, 2012; Polit & Beck, 2008).
Credibility involves evaluation of two aspects: how the investigation was carried out and how credibility was demonstrated. Credibility measures how vivid and faithful the description of the data is and whether the participants will recognize the described experiences and conceptions as their own (Lincoln & Guba, 1985; Polit & Beck, 2008).
Eight young people who used psychotropic drugs were interviewed. They represented different backgrounds and had various experiences of psychotropic drug use (III). This could increase the possibility of shedding light on different aspects of psychotropic drug use. A strategic sample was used according to the phenomenographic approach (Alexandersson, 1994) (IV). PHNs in different municipalities and counties, of different ages and doing different kinds of work, were encouraged to add various and relevant perceptions about their role.
During the analysis process, there is always a risk of losing the meaning of the text, which may produce units that are too broad or too narrow. In these studies the development of subcategories and categories (III), conceptions and descriptive categories (IV), respectively are illustrated, and representative quotes from the transcribed text are presented. During analysis (III, IV) the text from
60
the interviews was compared against the interpretations. All four authors read the interviews and repeatedly considered and reconsidered emerging categories.
Dependability refers to evidence that is consistent and stable (Lincoln & Guba, 1985; Polit & Beck, 2008) – data that is stable over time. Data collection was extended over a period of barely four months (III) and five months (IV). Open-ended introductory questions were asked in both studies, followed by individually adapted follow-up questions (III, IV). All the interviews were done by the first author, which may ensure that the same questions and follow-up questions are asked (Polit & Beck, 2008). According to Graneheim and Lundeman (2004) interviewing is an evolving process that gives new insights into the phenomenon and may influence the follow-up questions.
Confirmability is to the degree to which the results are derived from data from the participants, and the context of the study, rather than from researcher bias (Lincoln & Guba, 1985; Polit & Beck, 2008).
In both studies (III, IV) one of the researchers had worked for several years as a PHN and psychiatric nurse with young people. It may be argued that it is impossible for a researcher who has spent time within the professional fold to have an unbiased opinion. It is risky not to acknowledge the preconceived ideas brought to the investigation by the researcher. This must be balanced by the analysis work and quotes that were used to strengthen the data. This risk to go native was also balanced by the three members of the research group.
Transferability refers to the generalizability of the data, can the results be transferred to or have applicability in other settings or groups (Polit & Beck, 2008). The descriptions of context, selection and characteristics of participants, data collection and process of analysis make it possible for the reader to assess transferability to other groups and contexts (Lincoln & Guba, 1985).
Descriptions of the data collection and the steps in the analytical process were followed and reported according to Graneheim and Lundman (2004) (III) and Alexandersson (1994) (IV). The three co-authors read the interviews and participated in the analysis. Each step was discussed by the authors in line with their own opinions. Members of an organization for young people with mental health problems participated (III). There is a question of how well they represented, or differed from other young people with experience of psychotropic drug use. Neither we do not claim to have captured all the

61
variations in PHNs’ conceptions of psychotropic drug use among young people (IV). Transferability is enhanced by comprehensive presentation of the subcategories and categories, conceptions and descriptive categories, respectively, and results and representative quotes from the transcribed text.
62
Conclusions, implications and future research
Conclusions
Young people with mental distress are characterized by poor self-perceivedhealth, unfavourable life style habits and regarding social factors a greaterproportion have plans for vocational education and lower family income.
Gender differences are seen among girls and boys reporting mental distressand psychotropic drug use.
Psychotropic drug use increase among young people is mainly attributableto increasing use of hypnotics and off-label use of melatonin in particular.Melatonin is used more regular throughout a year, as compared to otherhypnotics.
Young people experience beneficial as well as undesired effects ofpsychotropic drugs.
Young people experience lacking access to professional support and follow-up.
Young people experience a problematic social life linked to negativereactions on psychotropic drug use by their families, friends, school andwork.
PHNs who discover psychotropic drug use among young people chose toact or not to. This may have consequences for the cooperation with theyoung people, family, school, work and the professionals. If cooperationwas established the PHN support young people in relation to psychotropicdrug use.
Implications
The prevalence of mental distress, with a high frequency of initiation ofpsychotropic drug use among young people should have consequences forhealth promotion in the school health service. PHNs need more knowledgeof young people’s mental health, psychotropic drugs and its use.
63
Concerning mental distress among young people, there is a genderdifference, as well as differences between socioeconomic groups. Thisshould affect the PHNs approach.
Some young people experience lack of access to professional support andfollow-up. There is a need for an easier access to the health services foryoung people suffering from mental distress.
Psychotropic drugs are used off-label among young people. Physiciansprescribing psychotropic drugs for young people must pay special attentionto the potentially adverse effects and must give the young people a closefollow-up.
PHNs need to gain more knowledge on psychotropic drugs, in line with theprevalence of mental health problems and increased psychotropic drug useamong young people.
PHNs, working in health centres and schools, have a responsibility topromote health and prevent health problems. They have the responsibilityand opportunity to identify young people struggling with mental healthproblems and psychotropic drug use as well as teach and support significantothers.
Future research
Further studies are needed on off-label use psychotropic drugs amongyoung people is needed.
Further studies are needed to investigate young people’s experiences ofpsychotropic drug use.
Further studies are required regarding female gender and psychotropic druguse.
Further studies are needed on why individuals and society do not acceptmental health problems among young people.
Intervention studies are needed with regard to health promotionprogrammes aimed at fortifying young people’s mental health. Theprograms have to emphasize the differences between genders as well associoeconomic groups.
64
Acknowledgements
I would like to express my gratitude to those who have helped and supported me in my work presented in this thesis.
First of all, I render my gratitude to the young people and the Public Health Nurses. Their participation and their sharing of thoughts and experience made the task possible.
Professor Gun Nordström, my principal supervisor and my two supervisors, Professor Bodil Wilde-Larsson and Professor Ingeborg Hartz, thank you for sharing your wide experience and knowledge with me. Your feedback and criticism has been of great value to me. Thank you for your time and care.
Thank you to the University of Karlstad and Professor Gun Nordström for accepting me as a doctoral student.
I also would like to give my thanks to the personal at the library at Hedmark University College, and Anne Mill Åkrann Brækhus for helping me. Jane Sugarman in London, England has done an excellent job in language vetting this thesis. Thank you.
Professor Kari Furu and Professor Svetlana Skurtveit at the Norwegian Institute of Public Health, thank you for your help and expertise in epidemiology and statistics.
All the other doctoral students at the University of Karlstad – I am very grateful for valuable discussions and comments at seminars. Bente Weimand, for sharing wine and thoughts, I missed you the last year. To all the other doctoral students, my mentor Anna Josse Eklund, the group from Gjøvik; Randi Ballangrud, Randi Tosterud, Sigrid Wangensten, Øyfrid Larsen Moen and Hege Kletthagen, the ladies from Østfold; Ann Karin Helgesen and Vigdis Abrahamsen Grøndahl. Thank you. Thanks to all the Swedish students during this year’s Anna Nordin, Cecilia Olsson, Ingrid From, Kaisa Bjuresäter, Anna Abelsson, Anna Willman, Karin Ängeby, Ann-Catrin Blomberg, Lena German-Millberg.
Øyfrid Larsen Moen, Mona Perzenius, Jan Nilsson and Hanne Søberg Finnbråten, I thank you for reading and comment my manuscripts.

65
The day Tuva Sandsdalen Mytting started her doctoral work the tours between Elverum and Karlstad become much, much better. No more lonely trips between Elverum and Karlstad for me, but coffee, discussions and sharing of thoughts, worries and joy. I am particularly grateful to you.
Thanks to the other PhD students at Hedmark University College for sharing common destiny; Liv, Randi, Berit, Anne, Inger Helen, Anne Marit, Per, Bjørn, Stein Egil, Annette, and Hanne.
A particular thanks to the Hedmark University College; Dean Sven Inge Sunde and the Head of Department of Nursing and Mental Health, Marianne Stensvehagen and Ulf Stigsson for giving me the opportunity to do my PhD. Bente Giset, I am grateful for your knowledge about – how to put every table, figure and character at the right place on paper. Thanks to all my colleges at the University College for your interest and support.
Finally, to my favourite young persons in life, Ingeborg, Kristine, Håvard, Helene and Falk who give my life value and meaning. To my husband Einar, I have been lucky in having your encouragement, support and the sharing of your knowledge in language, history and society to the best for me and my PhD.

66
References
A record-linkage study in Norway (2006–2010). Available at: www.forskningsradet.no/servlet/Satellite?c=Prosjekt&cid=1193731616637&pagename=ForskningsradetNorsk/Hovedsidemal&p=1181730334233. Accessed November 18, 2013.
Act of Health and Care (2011). Ministry of Health and Care Services (MHCS).Oslo. Available at: http://lovdata.no/dokument/NL/lov/2011-06-24-30 Accessed November 18, 2013.
Act of Medical and Health Research (2008). Ministry of Health and Care Services (MHCS). Oslo. Available at: http://www.ub.uio.no/ujur/ulovdata/lov-20080620-044-eng.pdf Accessed November 18, 2013.
Act of Patients’ Rights (1999). Ministry of Health and Care Services (MHCS). Oslo. Available at: http://www.ub.uio.no/ujur/ulovdata/lov-19990702-063-eng.pdf Accessed November 18, 2013
Act of Personal Health Data Filing System (2002). Ministry of Health and Care Services (MHCS). Oslo. Available at: http://www.regjeringen.no/en/dep/hod/Subjects/the-department-of-public-health/Act-of-18-May-2001-No-24-on-Personal-Health-Data-Filing-Systems-and-the-Processing-of-Personal-Health-Data-Personal-Health-Data-Filing-System-Act-.html?id=224129 Accessed November 18, 2013.
Act of Protection of Personal Information (2000). Justis- og beredskapsdepartementet. Oslo. Available at: http://lovdata.no/dokument/NL/lov/2000-04-14-31 Accessed November 18, 2013.
Act of Public Health (2012). Ministry of Health and Care Services (MHCS). Oslo. Available at: http://www.regjeringen.no/upload/HOD/Hoeringer%20FHA_FOS/123.pdf Accessed November 18, 2013.
Alexandersson, M. (1994). Den fenomenografiska forskningsansatsens fokus. In: Starrin B., Svensson P. G. (eds), Kvalitativ metod och vetenskapsteori. Lund, Sweden: Studentlitteratur, pp. 111–136.
Alvsvåg, H. (2012). Helsefremming og sykdomsforbygging – et historisk og sykepleiefaglig perspektiv. In: Gammersvik Å., Larsen T. (eds), Helsefremmende sykepleie – i teori og praksis. Bergen, Norge: Fagbokforlaget, pp. 79-97.
Ando, S., Yamasaki, S., Shimodera, S., Sasaki, T., Oshima, N., Furukawa, T., . . . Nishida, A. (2013). A greater number of somatic pain sites is associated with poor mental health in adolescents: a cross-sectional study. BMC Psychiatry, 13(1): 1-8. doi: 10.1186/1471-244X-13-30
67
Apa-Hall, P., Scwartz-Bloom, R. D., McConnell, E. S. (2008). The current state of teenage drug abuse: trend toward prescription drugs. Journal of School Nursing, 15(suppl).
Arnesdotter, Å., Olander, Å., Ragneskog, H. (2008). Hälsosamtalet – en utmaning för skolsköterskan. Vård i Norden, 28(57): 9.
Berg, C., Sakshaug, S., Handal, M., Skurtveit, S. (2011). Z-hypnotika – sovemidlene som dominerer markedet i Norge. Norsk Farmaceutisk Tidsskrift, 4: 14-7.
Bonati, M., Clavenna, A. (2005). The epidemiology of psychotropic drug use in children and adolescents. International Review of Psychiatry, 17(3): 181–188.
Borup, I. (2002). The school health nurse’s assessment of a successful health dialogue. Health & Social Care in the Community, 10(1): 10–19.
Borup, I., Holstein, B. (2004). Social class variations in schoolchildren’s self-reported outcome of the health dialogue with the school health nurse. Scandinavian Journal of Caring Sciences, 18: 343–350.
Borup, I., Holstein, B. (2006). Does poor school satisfaction inhibit positive outcome of health promotion at school? A cross-sectional study of schoolchildren’s response to health dialogues with school health nurses. Journal of Adolescent Health, 38: 758–760.
Borup, I., Holstein, B. (2007). Schoolchildren who are victims of bullying report benefit from health dialogues with the school health nurse. Health Education Journal, 66(1): 58–67.
Borup, I. (2011). Re-visit to the school nurse and adolescents’medicine use. Health Education Journal, 70: 274–284.
Breslau, J., Lane, M., Sampson, N., & Kessler, R. C. (2008). Mental disorders and subsequent educational attainment in a US national sample. Journal of Psychiatric Research, 42(9):708-716. doi: 10.1016/j.jpsychires.2008.01.016
Cavallo, F., Zambon, A., Borraccino, A., Raven-Sieberer, U., Torsheim, T., Lemma, P. (2006). Girls growing through adolescence have a higher risk of poor health. Quality of Life Research, 15: 1577–1585.
Chen E, Martin AD, Matthews KA. (2006). Socioeconomic status and health: Do gradients differ within childhood and adolescence? Social Science & Medicine, 62: 2161–70.
Chisolm, D., Klima, J., Gardner, W., Kelleher, K. (2009). Adolescent behavioral risk screening and use of health services. Administration & Policy in Mental Health & Mental Health Services Research, 36: 374–380.
68
Clancy, A. (2007a). A profession under threat? An exploratory case study of changes in Norwegian public health nursing. International Nursing Review, 54: 197–203.
Clancy, A., & Svensson, T. (2007b). ‘Faced’ with responsebility: Levinasian ethics and the challenges of responsibillity in Norwegian public health nursing. Nursing Philosophy, 8: 155-166.
Clancy, A., Svensson, T. (2009). Perceptions of public health nursing practice by municipal health officials in Norway. Public Health Nursing, 26: 412–420.
Clancy, A. (2010). Perceptions of public health nursing practice. On borders and boundaries, visibility and voice. Doctoral thesis, Nordic School of Public Health, Gothenburg, Sweden.
Collishaw, S., Maughan, B., Goodman, R., Pickles, A. (2004). Time trends in adolescent mental health. Journal of Child Psychology & Psychiatry, 45: 1350–1362.
Consentform. (2000). Available at: http://www.fhi.no/dokumenter/75b88ff5ef.pdf Accessed December 2, 2013.
Coppock, V., Dunn, R.W. (2010). Understanding Social Work Practice in Mental Health. Oxford: Oxford University Press.
Corell, C. U., & Carlson, H. E. (2006). Endocrine and metabolic adverse effects of psychotropic medications in children and adolescents. Journal of the American Academy of Child & Adolescent Psychiatry, 45(7): 771-791.
Costello, E. J., Mustillo, S., Erkanli, A., Keeler, G., & Angold, A. (2003). Prevalence and Development of Psychiatric Disorders in Childhood and Adolescence. Archives of General Psychiatry, 60(8): 837-844.
Currie, C., Zanotti, C., Morgan, A. J., Currie, D., de Looze, M., Roberts, C., . . . Barnekow, V. (2012). Social determinants of health and well-being among young people. København: World Health Oganization.
Dean, A.J., Hendy, A., McGuire, T. (2007). Antidepressants in children and adolescents – Changes in utilisation after safety warnings. Pharmacoepidemiology and Drug Safety, 16: 1048–1053.
Derogatis, L.R., Lipman, R.S., Rickels, K., Uhlenhuth, E.H., Covi, L. (1974). The Hopkins Symptom Checklist (HSCL): a self-report symptom inventory. Behavioural Science, 19(1): 1–15.
Distriktssköterskeföreningen i Sverige(DSF) (2013). Kompetencbeskrivning för legitemerad sjuksjöterska med specialistsjuksjöterskeeksamen, Distriktsskjöterska. Available at: www.distriktsskoterska.se Accessed November 30, 2013.
Eisenberg, D., Downs, M. F., Golberstein, E., & Zivin, K. (2009). Stigma and help seeking for mental health among college students. Medical Care Research & Review, 66(5): 522-541. doi: 10.1177/1077558709335173
69
Ellefsen, B. (2001). Changes in health visitors’work. Journal of Advanced Nursing, 34: 346–355.
European Medicines Agency (2013). Summary of products characteristics Melatonin. Available at: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/000695/human_med_000701.jsp&mid=WC0b01ac058001d124 Accessed November 25, 2013.
European Medicines Agency (2007). The European paediatric initiative: History of the Paediatric Regulation. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/Other/2009/09/WC500003693.pdf Accessed November 25, 2013.
Fegert, J., Kölch, M., Zito, J., Glaeske, G., Janhsen, K. (2006). Antidepressant use in children and adolescents in Germany. Journal of Child & Adolescent Psychopharmacology, 16(1–2): 197–206.
Field, A. (2009). Discovering Statistics using SPSS, 3rd edn. Newbury Park, CA: Sage Publications.
Frønes, I. (2007). Moderne barndom, 2nd edn. Oslo: Cappelen Akademisk Forlag.
Furu, K. (2008). Establishment of the nationwide Norwegian Prescription Database (NorPD) – new opportunities for research in pharmacoepidemiology in Norway. Norsk epidemiologi, 18: (2).
Geijlswijk, I., Mol, R., Egberts, T. G., & Smits, M. (2011). Evaluation of sleep, puberty and mental health in children with long-term melatonin treatment for chronic idiopathic childhood sleep onset insomnia. Psychopharmacology, 216(1): 111-120. doi: 10.1007/s00213-011-2202-y
George, D., Mallery, P. (1999). SPSS for Windows, step by step – a simple guide and reference. A Viacom Company, MA, USA.
Gobina, I., Välimaa, R., Tynjälä, J., et al. (2011). The medicine use and corresponding subjective health complaints among adolescents, a cross-national survey. Pharmacoepidemiology & Drug Safety, 20: 424–431.
Golsäter, M., Sidenvall, B., Lindfors, H., & Enskär, K. (2010). Pupils`perspectives on preventive health dialogues. British Journal of School Nursing, 5:(1).
Gore, F.M., Bloem, P.J.N., Patton, G.C., et al. (2011). Global burden of disease in young people aged 10-24 years: a systematic analysis. The Lancet, 377: 2093–2102.
70
Graneheim, U.H., Lundman, B. (2004). Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Education Today, 24: 105–112.
Griffiths, J.M., Closs, S.J., Bryar, R.M., Hostick, T., Kelly, S., Cooke, J. (2001). Barriers to research implementation by community nurses. British Journal of Community Nurses. 6(10):501–10.
Gyllenberg, D., Sourander, A. (2012). Psychotropic drug and polypharmacy use among adolescents and young adults: Findings from the Finnish 1981 Nationwide Birth Cohort Study. Nordic Journal of Psychiatry, 66: 336–342.
ICPC (2008). International Classification of Primary Care. Available at: http://www.legemiddelsiden.no/default.aspx?PageID=706&ReportID=56&field=ICPC_Code&Value=F Accessed Decenmber 3, 2013.
International Council for Nurses. (2012). Code of Ethics for Nurses. Available at: www.icn.ch/images/stories/documents/about/icncode_english.pdf. Accessed November 18, 2013.
Ilomäki, R., Ilomäki, E., Hakko, H., Räsänen, P. (2011). Psychotropic medication history of inpatient adolescents – Is there a rationale for benzodiazepine prescription? Addictive Behaviors, 36:(1–2), 161–165.
Information brochure (2000). Available at: http://www.fhi.no/dokumenter/d4cee6e283.pdf Accessed November 18, 2013.
Hagquist, C. E. I. (2007). Health inequalities among adolescents--the impact of academic orientation and parents' education. European Journal of Public Health, 17(1): 21-26. doi: 10.1093/eurpub/ckl087
Hair, J.F., Black, W.C., Babin, B.J., Anderson, R.E. (2010). Multivariate Data Analysis A Global Perspective, 7th edn. New York: Pearson.
Hansen, D. L., Hansen, E. H., & Holstein, B. E. (2009). Young women's use of medicines: autonomy and positioning in relation to family and peer norms. Health : An Interdisciplinary Journal for the Social Study of Health, Illness and Medicine , 13:(4): 467-485. doi: 13/4/467 [pii]
Hardeland, R., Cardinali, D. P., Srinivasan, V., Spence, D. W., Brown, G. M. and Pandi-Perumal, S. R. (2011). Melatonin--a pleiotropic, orchestrating regulator molecule. Progress in Neurobiology. 93: 350-84.
Hardeland, R. (2012). Melatonin in aging and disease -multiple consequences of reduced secretion, options and limits of treatment. Aging & Disease. 3: 194-225.
Hartz, I., Furu, K., Bratlid, T., Handal, M., Skurtveit, S. (2012). Hypnotic drug use among 0–17 year olds during 2004–2011: A nationwide prescription database study. Scandinavian Journal of Public Health, 40: 704–711.
71
Helland, M. J., Mathiesen, K. (2009). 13–15 åringer fra vanlige familier i Norge - hverdagsliv og psykisk helse . Rapport 2009: 1 Nasjonalt folkehelseinstitutt. www.fhi.no: Nasjonalt folkehelseinstitutt.
Herrman, H., Saxena, S., Moodie, R. (2005). Promoting Mental Health. World Health Organization, Department of Mental Health and Substance Abuse in collaboration with the Victorian Health Promotion Foundation and The University of Melbourne. Available at: www.who.int/mental_health/evidence/MH_Promotion_Book.pdf. Accessed November 18, 2013.
Holstein, B., Andersen, A., Due, P., Hansen, E. H. (2009). Børns og unges brug af lægemidler mot smerter og psykiske problemer. Udviklingen fra 1988 til 2006. Videnskab & Praksis. Ugeskrift Læger, 171(1): 24–28.
Hsia, Y., Maclennan, K. (2009). Rise in psychotropic drug prescribing in children and adolescents during 1992–2001: a population-based study in the UK. European Journal of Epidemiology 24: 211–216.
Kalikstad, B., Westergren, T. (2006). Medisiner til barn – når nødløsninger blir rutine. Tidsskrift for den Norske Lægeforening, 7(126): 930–932.
Kessler, R., Angermeyer, M., Anthony, J., et al. (2007). Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry, 6(3): 168–176.
Koelch, M., Prestel, A., Singer, S., et al. (2009). Psychotropic medication in children and adolescents in germany: prevalence, indications, and psychopathological patterns. Journal of Child & Adolescent Psychopharmacology, 19: 765–770.
Lampiano, F., Du Plessis, S.S. (2013). New developments of melatonin on reproduction. World Journal of Obstetrics & Gynecology, 2: 15-22.
Larsen, B. I. (2010). Health Promotiom - achieving good health for all. Director of Division, Knut Inge Klepp (Ed.). Oslo: Norwegian Directorate of Health.
Levin, K.A., Torsheim, T., Vollebergh, W., et al. (2011). National income and income inequality, family affluence and life satisfaction among 13 year old boys and girls: a multilevel study in 35 countries. Social Indicators Research, 104: 179–194.
Levinas, E. (2008). Den annen humanisme. Bokklubbens kulturbibliotek. Oslo.
Lien, L., Sagatun, Å., Heyerdahl, S., Søgaard, A. J., Bjertness, E. (2009). Is the relationship between smoking and mental health influenced by other unhealthy lifestyle factors? results from a 3-year follow-up study among adolescents in Oslo, Norway. Journal of Adolescent Health, 45: 609–617.
Lincoln, Y. S., Guba, E.G. (1985). Naturalistic Inqury. Newbury Park, CA: Sage Publications.
72
Lingjærde, O. (2006). Psykofarmaka Medikamentell behandling av psykiske lidelser (5. utgave ed.). Kristiansand: Høyskoleforlaget Norwegian Academic Press.
Lundman, B., Graneheim, U. H. (2012). Kvalitativ Innhållsanalys. In: Granskär M., Höglund-Nielsen B. (eds), Tillämpad kvalitativ forskning innom hälsa och sjukvård. Studentlitteratur ( pp. 249).
Maclean, A., Sweeting, H., Hunt, K. (2010). ‘Rules’ for boys, ‘guidelines’ for girls: Gender differences in symptom reporting during childhood and adolescence. Social Science & Medicine, 70: 597–604.
Marton, F., Booth, S. (1997). Learning and Awareness. Mahwah, NJ: Lawrence Erlbaum Associates.
Mathiesen, K., Kjeldsen, A., Skipstein, A., Karevold, E., Torgersen, L., Helgeland, H. (2007). Trivsel og oppvekst- barndom og ungdomstid. Nasjonalt folkehelseinstitutt. Available at: www.fhi.no/dokumenter/90be49af81.pdf. Accessed November 18, 2013.
Meadows, P. (2009). Community Health Nursing. American Journal of Nursing, 109: 19.
Mellingsæter, T. C., Bramness, J. G., Slørdal, L. (2006). Er z-hypnotika bedre og tryggere sovemedisiner enn benzodiazepiner? Tidsskrift for den Norske Lægeforening, 126: 2954–2956.
Mental Helse Ungdom (2012a). Available at: www.mentalhelseungdom.no/ Accessed November 18, 2013.
Mental Helse Ungdom (2012b). Available at: http://www.mentalhelseungdom.no/arkiv/oensker-du-aa-delta-i-forskningsprosjektet-ungdoms-psykiske-helse-med-spesielt-fokus-paa-bruk-av-psykofarmaka Accessed November 27, 2013.
Merikangas, K. R. (2005). Vulnerability factors for anxiety disorders in children and adolescents. Child & Adolescent Psychiatric Clinics of North America, 14: 649–679.
Merikangas, K. R., Pine, D. (2002). Genetic and other vurlnerability factors for anxiety and stress disorders In: Davis K.L., Charney D., Coyle J.T., Nemeroff C. (eds), Neuropsychopharmacology: 868 The Fifth Generation of Progress. Bethesda, MD: National Institute of Mental Health.
Moksnes, U. K., Rannestad, T., Espnes, G. A., Byrne, D. G. (2011). The associations between stress, sence of coherence and subjectie health complaints in adolescents: Sense of coherence as apotential moderator. Stress & Health. 27(3):157-165.
Morgan, A., Ziglio, E. (2007). Revitalising the evidence base for public health: an assets model. Promotion & Education, 14(2 suppl): 17–22.
73
Mykletun, A., Knudsen, A. K.,: Mathiesen, K. S. (2009). Psykiske lidelser i Norge: Et folkehelseperspektiv 2009:8. Available at: http://www.fhi.no/dav/d39d557a77.pdf Accessed Descember 1, 2013.
Nasjonalt Folkehelseinstitutt (2011). Available at: www.fhi.no/eway/default.aspx?pid=239&trg=List_6212&Main_6157=6263:0:25,6336&MainContent_6263=6464:0:25,8303&List_6212=6218:0:25,8359:1:0:0:::0:0 Accessed November 18, 2013.
Nielsen, M. W., Søndergaard, B., Kjøller, M., Hansen, E. H. (2008). Agreement between self-reported data on medicine use and prescription records vary according to method of analysis and therapeutic group. Journal of Clinical Epidemiology, 61: 919–924.
Nightingale, F. (1853). ‘Sick-nursing and Health Nursing’. In I. Hampton (ed.), Nursing of the sick-1893 (pp. 24-37). New York: McGraw-Hill. (Original work published 1893).
Northern Nurses´ Federation. (2003). Ethical guidelines for nursing research in the Nordic countries. Available at: www.sykepleien.no/ikbViewer/Content/337889/SSNs%20etiske%20retningslinjer.pdf. Accessed November 18, 2013.
Norwegian Prescription Database (2004–2010). National Institute of Public Health. Available at: www.fhi.no/eway/default.aspx?pid=233&trg=MainArea_5661&MainArea_5661=5565:0:15,3791:1:0:0:::0:0&MainLeft_5565=5544:50553::1:5569:10. Accessed November 18, 2013.
Norwegian Youth Health Study (2000–2004). Available at: www.fhi.no/eway/default.aspx?pid=240&trg=MainContent_6898&Main_6664=6898:0:25,7898:1:0:0:::0:0&MainContent_6898=6706:0:25,8471:1:0:0:::0:0. Accessed November 18, 2013.
Patel, V., Flisher, A. J., Hetrick, S., Mc Gorry, P. (2007). Mental health of young people: a global public-health challenge. The Lancet, 369: 1302–1313.
Patton, G. ., Coffey, C., Sawyer, S. M., et al. (2009). Global patterns of mortality in young people: a systematic analysis of population health data. The Lancet, 374: 881–892.
Piaget, J. (1932). The language and thought of a child. New York: Harcourt, Brace & Co.
Pirskanen, M., Laukkanen, E., Pietilä, A. M. (2007). A formative evaluation to develop a school health nursing early intervention model for adolescent substance use. Public Health Nursing, 24: 256–264.
74
Plessen, K. J., Kabicheva, G. (2010). Hjernen og følelser – fra barn til voksen. Tidsskriftet for den Norske Lægeforening, 9(139): 932-5.
Polit, D. F., Beck, C. T. (2008). Nursing Research, Generating and Assessing Evidence for Nursing Practice, 8th edn. Philadelphia, PA: Lippingcott Williams & Wilkins, p. 19.
Popovici, I., French, M. T. (2013). Binge drinking and sleep problems among young adults. Drug & Alcohol Dependence, 132(1–2): 207–215.
Povlsen, L., Borup, I. K. (2011). Holism in nursing and health promotion: distinct or related perspectives? – a literature review. Scandinavian Journal of Caring Sciences, 25: 798–805.
Pryjmachuk, S., Graham, T., Haddad, M., & Tylee, A. (2012). School nurses' perspectives on managing mental health problems in children and young people. Journal of Clinical Nursing, 21 (5/6): 850-859. doi: 10.1111/j.1365-2702.2011.03838.x
Rothman, K., & Greenland, S. (1998). Precision and validity in epidemiological studies. In: Rothman, K., & Greenland, S. (eds), Philadelphia, PA. Modern Epidemiology (115 – 134). Lippincott Williams & Wilkins. Philadelphia, PA.
Roy, B., Grøholt, B., Heyerdahl, S., Clench-Aas, J. (2006). Self-reported strengths and difficulties in a large Norwegian population 10–19 years. European Child & Adolescent Psychiatry, 15:189–198.
Safer, D. (2011). Age-grouped differences in adverse drug events from psychotropic medication. Journal of Child &Adolescent Psychopharmacology. 21(4): 299-309.
Safer, D., Zito, J. (2006) Treatment-emergent adverse events from selective serotonin reuptake inhibitors by age group: children versus adolescents. Journal of Child & Adolescent Psychopharmacology . 16(1-2): 159-69.
Siegel, R. S., Dickstein, D. P. (2011). Anxiety in adolescents: Update on its diagnosis and treatment for primary care providers. Review. Adolescent Health, Medicine & Therapeutics, 1:(16).
Simeon, J., Wiggins, D., Williams, E. (1995). Worldwide use of psychotropic drugs in child and adolescent psychiatric disorders. Progress In Neuro-Psychopharmacology & Biological Psychiatry, 19: 455–465.
Sivaprasad, L., Kolind, A., Berg, B. (2005). Use of psychotropic medication in an outpatient CAMHS over a 5-year period. Child & Adolescent Mental Health, 10: 179–182.
Skurtveit, S., Rosvold, E. O., & Furu, K. (2005). Use of psychotropic drugs in an urban adolescent population: the impact of health-related variables, lifestyle and sociodemographic factors – The Oslo Health Study 2000–2001. Pharmacoepidemiology & Drug Safety, 14: 277–283.
75
Skurtveit, S., Selmer, R., Tverdal, A., Furu, K. (2008). The validity of self-reported prescription medication use among adolescents varied by therapeutic class. Journal of Clinical Epidemiology, 61: 714–717.
Srinivasan, V., Spence, W. D., Pandi-Perumal, S. R., Zakharia, R., Bhatnagar, K. P., & Brzezinski, A. (2009). Melatonin and human reproduction: Shedding light on the darkness hormone. Gynecological Endocrinology, 25(12): 779-785. doi: doi:10.3109/09513590903159649
Statens Folkhälsoinstitut (2011). Kartläggning av psykisk hälsa bland barn och unga. Resultat från den nationella totalundersökningen i årskurs 6 och 9 hösten 2009.
Steuber, T. L., Danner, F. (2006). Adolescent smoking and depression: Which comes first? Addictive Behaviors, 31(1): 133–136.
Storvoll, E. E., & Wichstrøm, L. (2003). Gender differences in changes in and stability of conduct problems from early adolescence to early adulthood. Journal of Adolescence, 26(4): 413-429.
Strand, B .H., Dalgard, O. S., Tambs, K., Rognerud, M. (2003). Measuring the mental health status of the Norwegian population: a comparison of the instruments SCL-25, SCL-10, SCL-5 and MHI-5 (SF-36). Nordic Journal of Psychiatry, 57(2): 113–118.
Sund, A. M. (2004). Development of Depressive Symptoms in Early Adolescence. Doctoral thesis, Norwegian University of Science and Technology, Trondheim, Norway.
The Ministry of Education and Research (2005). Forskrift til rammeplan for helsesøster. Oslo. Available at: www.lovdata.no/cgi-wift/ldles?doc=/sf/sf/sf-20051201–1381.html. Accessed November 18, 2013.
The Ministry of Health and Care. (2003a). Regulations of the maternal and child health centre- and the school health service Oslo. Available at: http://www.lovdata.no/for/sf/ho/ho-20030403-0450.html Accessed November 18, 2013.
The Ministry of Health and Care (2003b). Social Indicators Research Norwegian Prescription Register . Regulations for the managment of data in the Norwegian Prescription Register. Oslo. Available at: http://lovdata.no/dokument/SF/forskrift/2003-10-17-1246. Accessed November 18, 2013.
The Ministry of Health and Care (2005). Fra stykkevis til helt, En sammenhengende helsetjeneste, NOU 2005: 3. Oslo. Available at: http://www.regjeringen.no/nb/dep/hod/dok/nouer/2005/nou-2005-03.html?id=152579Accessed December 3, 2013.
76
The Ministry of Health and Care (2012).The Coordination Reform. Report No. 47 (2008-2009) to the Storting. Oslo. Available at: http://www.regjeringen.no/upload/HOD/Dokumenter%20INFO/Samhandling%20engelsk_PDFS.pdf Accessed November 25, 2013.
The Ministry of Health and Care (2013). Folkehelsemeldingen. (2013). Folkehelsemeldingen. God helse - felles ansvar. Meld.ST. 34 (2012-2013). Oslo. Available at: http://www.regjeringen.no/pages/38307106/PDFS/STM201220130034000DDDPDFS.pdf. Accessed November 18, 2013.
The Norwegian Directorate of Health (2003 b).Veileder for kommunenes helsefremmende og forebyggende arbeid i helstasjons- og skolehelsetjenesten. Available at: www.helsedirektoratet.no/publikasjoner/veileder-til-forskrift-om-kommunens-helsefremmende-og-forebyggende-arbeid-i-helsestasjons--og-skolehelsetjenesten-/Publikasjoner/veileder-til-forskrift-kommunens-helsefremmende-og-forebyggende-arbeid-i-helsestasjons--og-skolehelsetj-.pdf. Oslo. Accessed November 18, 2013.
The Norwegian Directorate of Health (2008). Veileder for poliklinikker i psykisk helsevern for barn og unge. Oslo. Available at: www.helsedirektoratet.no/publikasjoner/psykisk-helsevern-for-barn-og-unge-veileder-for-poliklinikker/Publikasjoner/psykisk-helsevern-for-barn-og-unge-veileder-for-poliklinikker.pdf. Accessed November 18, 2013.
The Norwegian Directorate of Health (2010). Health Promotion – achieving good health for all. Oslo. Available at: http://www.helsedirektoratet.no/english/publications/health-promotion--achieving-good-health-for-all-/Sider/default.aspx Accessed November 25, 2013.
Torsheim, T., Ravens-Sieberer, U., Hetland, J., Välimaa, R., Danielson, M., Overpeck, M. (2006). Cross-national variation of gender differences in adolescent subjective health in Europe and North America. Social Science & Medicine, 62: 815–827.
Ungdata 2010–1012. (2013). NOVA report 10/13: Norwegian Social Research (Norsk institutt for forskning om oppvekst, velferd og aldring. Accessed November 18, 2013.
United Nations Childrens’s Fund (2002). Adolescence. A time that matters, Vols 1–44. New York. Available at: http://www.unicef.org/publications/index_4266.html Accessed December, 03 2013.
United Nations Convention on the Rights of the Child. (1989). The Rights of the Child,. Available at: http://www.childrensrights.ie/sites/default/files/submissions_reports/files/UNCRCEnglish_0.pdf. Accessed November 25, 2013.
77
United Nations Population Fund (2013). Adolescents and Youth Demographics: A Brief Overview. Available at: http://www.unfpa.org/webdav/site/global/shared/factsheets/One%20pager%20on%20youth%20demographics%20GF.pdf Accessed December 02, 2013.
Vaaler, A. E., Fasmer, O.B. (2013). Antidepressive legemidler – klinisk praksis må endres. Tidsskrift for den Norske Legeforening, 133: 428 – 430.
Walsh, F. (2006). Strengthening Family Resilience. The Guilford Press. New York.
WHO (2004 a). Atlas. Child and Adolescent Mental health Resources Global Concerns: Implications for the future Word psychiatric. Geneva: World Health Organization. Available at: http://www.who.int/mental_health/resources/Child_ado_atlas.pdf Accessed November 18, 2013.
WHO (2004 b). Promoting mental health : concepts, emerging evidence, practice : summary report. Melbourne: Retrieved from http://www.who.int/mental_health/evidence/en/promoting_mhh.pdf. Accessed November 25, 2013.
WHO (2009a). Global Health Risks, Mortality and burden of disease attributable to selected major risks: World Health Organization 2009. Available at: http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf Accessed November 25, 2013.
WHO (2009b). Milestones in Health Promotion Statements from Global Conferences. Aavailable at: http://www.who.int/healthpromotion/Milestones_Health_Promotion_05022010.pdf Accessed November 25, 2013.
WHO (2010). ICD-10. Available at: http://apps.who.int/classifications/icd10/browse/2010/en Accessed November 18, 2013.
WHO (2011). Young people: health risks and solutions. Fact sheet no. 345. Available at: www.who.int/mediacentre/factsheets/fs345/en/ Accessed November 18, 2013.
WHO (2012). Adolescent Mental Health. Mapping actions of nongovernmental organizations and other international development organizations. Geneva: WHO. Available at: whqlibdoc.who.int/publications/2012/9789241503648_eng.pdf. Accessed November 18, 2013.
WHO (2013). WHO Collaborating Centre for Drug Statistics Methodology. mailto:[email protected]: Norwegian Institute of Public Health. Available at: www.whocc.no. Accessed November 18, 2013.
78
Wiklund, M., Malmgren-Olsson, E. B., Ohman, A., Bergstrom, E., Fjellman-Wiklund, A. (2012). Subjective health complaints in older adolescents are related to perceived stress, anxiety and gender – a cross-sectional school study in Northern Sweden. BMC Public Health, 12(1): 993.
Wiles, N., Haase, A., Lawlor, D., Ness, A., Lewi, G. (2012). Physical activity and depression in adolescents: cross-sectional findings from the ALSPAC cohort. Social Psychiatry & Psychiatric Epidemiology, 47: 1023–1033.
Winter, A. F. d., Oldehinkel, A.J., Veenstra, R., Brunnekreeft, A., Verhulst, F .C., Ormel, J. (2005). Evaluation of non-response bias in mental health determinants and outcomes in a large sample of pre-adolescents. European Journal of Epidemiology, 20(2):173-181.
Wohlfarth, T., Kalverdijk, L., Rademaker, C., Schothorst, P., Minderaa, R., Gispen-de Wied, C. (2009). Psychopharmacology for children: From off label use to registration. European Neuropsychopharmacology, 19: 603–608.
Xu, Z., Su, H., Zou, Y., Chen, J., Wu, J., Chang, W. (2012). Sleep quality of Chinese adolescents: Distribution and its associated factors. Journal of Paediatrics & Child Health, 48: 138–145.
Zito, J. M., Derivan, A. T., Kratochvil, C. J., Safer, D. J., Fegert, J. M., Greenhill, L. L. (2008a). Off-label psychopharmacologic prescribing for children: History supports close clinical monitoring. Child and Adolescent Psychiatry & Mental Health, 2: 24.
Zito, J. M., Safer, D. J., Berg, L., et al. (2008b). A three-country comparison of psychotropic medication prevalence in youth. Child & Adolescent Psychiatry & Mental Health, 2(1): 26.
Zito, J. M., Safer, D. J., DosReis, S., et al. (2003). Psychotropic practice patterns for youth: a 10-year perspective. Archives of Pediatric Adolescent Medicine, 157(1): 17–25.
Zoëga, H., Baldursson, G., Hrafnkelsson, B., Almarsdóttir, A. B., Valdimarsdóttir, U., Halldórsson, M. (2009). Psychotropic drug use among Icelandic children: A nationwide population-based study. Journal of Child & Adolescent Psychopharmacology, 19: 757–764.
urn:nbn:se:kau:diva-30600
Mental Distress and Psychotropic Drug Use among Young People, and Public Health Nurses` Conceptions of Their Roles
International studies indicate an increase in mental distress and psychotropic drug use among young people. In this thesis mental distress is reported among 15.5 % of the young people. Of those reporting mental distress 75 % were girls. One quarter of the girls reporting mental distress at 15-16 years of age was incident users of psychotropic drugs one to nine years later. Psychotropic drug use, increase among young people, particularly hypnotic drugs. The young people experience beneficial and undesired effects of the psychotropic drugs. They miss out on professional availability and follow-up, and experience negative reactions related to their psychotropic drug use by their significant others. The public health nurse who discovers psychotropic drug use among young people chooses either to act or not to act in relation to this. Those who choose to act continue to cooperate with the young people and others. An established cooperation was followed by a public health nurse who supports and teaches the young people. The prevalence of mental distress, with a high frequency of initiation of psychotropic drug use among young people should have consequences for health promotion in the school health service. Public health nurses, working in health centers and schools, have a responsibility to promote health and prevent health problems. They have the responsibility and opportunity to identify young people struggling with mental health problems and psychotropic drug use as well as teach and support significant others.
DISSERTATION | Karlstad University Studies | 2014:2
ISSN 1403-8099
ISBN 978-91-7063-531-1













![MENTAL DISTRESS DAMAGES FOR B CONTRACT D W McLauchlan "Mental Distress Damages for Breach of ... (1875) LR 10 QB 111, 122, Blackburn J. 14 Hadley v ... 16 Jarvis v Swan Tours Ltd [1973]](https://img.pdfslide.us/doc/110x75/5ae70d147f8b9a9e5d8e8bf3/mental-distress-damages-for-b-contract-d-w-mclauchlan-mental-distress-damages-for.jpg)