Embed Size (px)
Citation preview

Chapter 4
Mental Disorders and the Brain

CONTENTSPage
METHODS USED TO STUDY MENTAL DISORDERS. . . . . . . . . . . . . . . . . . . . . . . . . . . .Biochemistry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Anatomy and Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
SCHIZOPHRENIA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Biochemistry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Anatomy and Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Synthesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
MOOD DISORDERS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Biochemistry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Anatomy and Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Synthesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ANXIETY DISORDERS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Obsessive-Compulsive Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Panic Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Synthesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
IMPLICATIONS FOR TREATMENT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .SUMMARY AND CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .CHAPTER 4 REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7172747777798182828285868888889092929394
BoxesBox Page4-A. Cloning Dopamine Receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 754-B. Serotonin and Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
FiguresFigure Page4-1. Neurons . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 724-2. The Synapse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 734-3. Brain Structures Involved in Mental Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 764-4. MRI Scan of an Individual With Schizophrenia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 794-5. PET Scan of an Individual With Schizophrenia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 804-6. PET Scans of an Individual With Bipolar Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 864-7. PET Scan of an Individual With Obsessive-Compulsive Disorder . . . . . . . . . . . . . . . . 894-8. PET Scan of an Individual With Panic Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92
TablesTable Page4-1. Techniques for Imaging the Brain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 774-2. Drugs in Development for Mental Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93

Chapter 4
Mental Disorders and the Brain
Studying the factors that play a role in mentaldisorders is like putting together a jigsaw puzzle.The pieces of the puzzle are bits of information aboutthe workings of the human brain. This chapterconsiders the chemistry, structure, and function ofthe human brain in mental disorders. Another keypiece in the puzzle is the heritability of thesedisorders, which is discussed in chapter 5.
The nature and amount of information availableabout the biology of mental disorders reflects thecourse of neuroscience research over the years.During the 1960s and 1970s there were advances inthe methods used to study the chemistry of the brainand a resulting increase in knowledge about brainpharmacology and biochemistry. Many scientiststherefore focused their work on the roles of naturalchemicals and pharmaceuticals in mental disorders.The following decade, the 1980s, saw advances inmolecular biology and imaging technologies, whichin turn led to study of brain anatomy and activity andthe molecules involved. The pace and extent ofresearch into the biological components of mentaldisorders mirror these developments, with the bodyof knowledge concerning the chemistry of the brainbeing much larger than the growing database aboutother factors. Currently, some of the most activeresearch involves techniques that enable investiga-tors to study the activity of the brain in livingsubjects. These advances and the expectation offuture discoveries have infused researchers in thearea of mental disorders with optimism that furtherstudies will pay off in a greater knowledge of thebrain, a better understanding of disorders, and thedevelopment of new treatments for them.
Scientists examine the activity of the brain todetermine its normal functioning and to see whetherbiological factors are associated with a given mentaldisorder. When a factor is identified, an importantdistinction must be made as to whether it iscorrelated with the disorder or in fact causes it. Acorrelated factor is one that is linked to the disorderand may result in some of its symptoms. Forexample, a perturbation of the chemical functioningof an area of the brain may be correlated withsymptoms characteristic of a disorder. Understand-ing the perturbation can explain how the symptomsoccur-that is, what the biological underpinnings
are-but it does not explain what caused thechemical disturbance. Thus, a correlated factor—inthis case the chemical perturbation-is secondary tothe underlying cause of the disorder. The consistentassociation of either a causative or correlative factorwith a disorder can provide a biological marker toaid in the diagnosis of the disorder, which in turn canbe critical to research and treatment. The identifica-tion of factors that are associated with a disorder canalso provide an understanding of the mechanismsunderlying symptoms; this is crucial to the develop-ment of rational therapeutic interventions. Mostbasic of all is the identification of specific causes ofmental disorders. To date, research into the biologyof the mental disorders considered here has identi-fied several factors that are associated with theirsymptoms; there is much less evidence regarding thecauses of these disorders.
To solve the puzzle of what causes and contrib-utes to mental disorders, all of the pieces have to bestudied and fit together. It is important to note thatnot all of them will necessarily be biological.Although beyond the scope of this report, psycho-logical and social factors also contribute. Thus,when a biological factor is identified, research mustpoint out how it interacts with psychological andsocial factors that may produce, modify, or deter-mine how mental disorders are expressed. Forexample, it may be that biological factors create apredisposition to certain disorders. The psychologi-cal and social experiences of an individual, such asexposure to stress or a negative life event, may thenshape the likelihood that that factor will manifestitself as the clinical condition.
METHODS USED TO STUDYMENTAL DISORDERS
To understand the involvement of biologicalfactors in mental disorders, researchers conductexperiments in animals, analyze biological samplesfrom patients, and study patients’ biochemistry,brain anatomy, behavior, and mental activities. Ingeneral, basic mechanisms of the brain’s physiol-ogy, chemistry, and anatomy are studied in eitheranimal models that approximate aspects of a disor-der or in tissue samples from living persons andbrain samples from deceased ones. Patient popula-
–71-

72 ● The Biology of Mental Disorders
tions are examined to learn more about symptomsand characteristics associated with disorders. Under-standing mental disorders depends on connectinginformation from these diverse observations. Ulti-mately, the most comprehensive information isderived from studies and techniques that permitdirect measurements in humans, both those with andthose without mental disorders. Although it is verydifficult to study the working brain in humans, newtechniques enable investigators to observe somephysiological processes in living subjects. Refine-ment of these techniques, and the development ofadditional ones, will most likely enhance the under-standing of mental disorders.
It is often difficult to put disparate biologicalpieces together into a unified hypothesis about thebiological underpinnings of a mental disorder. Manytimes, results from studies contradict each other orare inconsistent, which further complicates thisprocess. A number of factors contribute to thesecontradictions and inconsistencies. A better under-standing of the workings of the healthy brain isessential to understanding what might go wrong inmental disorders. As a result, there is still much to belearned. Also, some older research techniques pro-vide only crude measures of brain activity, produc-ing less precise findings. Finally, the difficulty ofdistinguishing specific mental disorders may resultin a heterogeneous research population, which canthen produce difficult-to-interpret results. To some
extent, the explosion in neuroscience research inrecent years and the development of new, sophisti-cated techniques and methodologies for more pre-cise, complex analysis have reduced, and willcontinue to alleviate, many of these problems.
Biochemistry
Study of the biochemistry of the brain involvesexamining the many chemicals involved in commun-ication and processing of information in the brain.Neurotransmitters are chemicals released by nervecells, or neurons, to communicate with each other.Neurons are the cells that process information in thebrain. A neuron consists of a cell body with longextensions, much like the branches of a tree, calleddendrites (figure 4-l). Also projecting out of the cellbody is a single fiber called the axon, which canextend a great distance (figure 4-l). When a neuronis activated, it releases a neurotransmitter into thesynapse, the gap between two neurons (figure 4-2).The molecules of the neurotransmitter move acrossthe synapse and attach themselves, or bind, toproteins, called receptors, in the outer wall of anadjacent cell (figure 4-2). Usually, the axon terminalis the part of the cell that releases neurotransmittersinto the synapse, and the dendrites and cell body arethe areas of the neuron which contain receptors thatform synapses with the axons of other neurons.
Once the neurotransmitter has activated a recep-tor, it unbinds from the receptor. It then has to be
Figure 4-l—Neurons
Synapse
Two neurons in synaptic contact.SOURCE: R. Brain (New York, NY: Bantam Books, 1984).

Chapter Mental Disorders and the Brain ● 73
Figure 4-2—The Synapse
Nerve impulse
Auto-breakdown
receptor
Neurotransmitters ReceptorsReceiving cell
The synapse and associated structures.SOURCE: Office of Technology Assessment, 1992.
removed from the synapse so the synapse will beavailable for a new message. This is done either bythe neurotransmitter’s being taken backup into theneuron that released it (a process called reuptake) orby it being broken down chemically into compoundscalled-metabolizes (figure 4-2).
For each neurotransmitter in the brain, there arespecific receptors to which it can attach. Binding bythe neurotransmitter activates the receptor, whichcan have different effects, depending on the recep-tor. Receptors can be linked to a variety of biochem-ical and cellular mechanisms that are turned on or offby the activation of the receptor. A neuron can havethousands of receptors for many different neuro-transmitters. Some neurotransmitters activate neu-rons (excitatory neurotransmitters), while othersdecrease the activity of neurons (inhibitory neuro-transmitters).
When a neuron is activated, changes occur in itsmembrane, resulting in a shift in the balance of ions(electrically charged molecules) between the insideand outside of the neuron. This change in ionicbalance triggers an electrical impulse inside theneuron. The electrical impulse travels from the cellbody, down the axon, to the axon terminal. At the
axon terminal, the impulse causes the release ofneurotransmitter from the neuron into the synapse.
Sometimes a receptor for one neurotransmittercan affect a receptor for another neurotransmitter. Insuch cases, the receptors are biochemically coupled:The activation of one modulates the functioning ofthe other, either increasing or decreasing its activity.A neuron can also have receptors for the neurotrans-mitter it releases; these are usually located near thesite where the neurotransmitter is released into thesynapse (figure 4-2). Such receptors are acted on bythe neuron’s own neurotransmitter to regulate therelease of the neurotransmitter. Thus, these autorecep-tors, as they are called, act as a feedback mechanismto regulate a neuron’s activity. The activity of aneuron will be determined by the cumulative activityof all its various receptors.
While receptors are specific for a neurotransmit-ter, there may be a variety of receptor subtypes,linked to different cellular mechanisms, that allrespond to the same neurotransmitter. In this way,one neurotransmitter can have diverse effects invarious areas of the brain. Also, the number ofreceptors in the brain is not static. In response toincreased production of a neurotransmitter, thenumber of receptors for that neurotransmitter willdecrease; conversely, depletion of a neurotransmit-ter will result in an increase in the number ofreceptors for that neurotransmitter. This mechanismallows the brain to compensate for changes inneurotransmitter levels. Such receptor changes areimportant in therapeutics; some drugs mimic neuro-transmitters by stimulating increases or decreases inreceptor numbers. In some cases, these changes maybe directly related to the drug’s therapeutic effect.
Many chemicals have been identified as neuro-transmitters, among them acetylcholine, the cat-echolamines (norepinephrine, epinephrine, dopam-ine), serotonin, various amino acids, and peptides,including certain hormones. Various chemicals inthe brain other than neurotransmitters and theirreceptors are necessary for brain function. They maybe associated with the biochemical mechanismsactivated by neurotransmitter-receptor interactions,involved with the production and breakdown ofneurotransmitters, or responsible for carrying outmetabolic activity.
Abnormalities in any of these chemicals, theirreceptors, or the cellular mechanisms that are turnedon or off by the receptors could contribute to mental

74 . The Biology of Mental Disorders
disorders. For example, there may be too much ortoo little of a neurotransmitter, or the receptors for aneurotransmitter may not function properly. Mecha-nisms activated by receptors maybe defective, or thesystems responsible for deactivating neurotransmit-ters maybe faulty. Also, breakdowns in the chemicalsystems responsible for the normal functioning ofcells in the nervous system may play a role in mentaldisorders. Such alterations in neurotransmitter sys-tems have been implicated in the symptoms ofcertain mental disorders (see later discussions).
Scientists use a variety of tools and methods tostudy these factors. Biochemical assays are availableto measure receptor number and activity, concentra-tions of neurotransmitters, and many other biochem-ical parameters of brain function. The majority ofthese assays are used with tissue from animals orfrom patients (i.e., postmortem brain samples ortissue samples from living patients). For example,information about concentrations of neurotransmittersis derived from measuring these compounds or theirmetabolizes in samples of blood or cerebrospinalfluid (i.e., fluid inside and surrounding the brain andspinal cord). Nevertheless, such samples provideonly an indirect measure of what is occurring in thebrain. The inability to observe and measure thechemical activity of the brain directly has hamperedinvestigators’ understanding of how these processesmay go awry in mental disorders. One new tech-nique that enables scientists to study biochemistry inthe living brain is positron emission tomography(PET) (see later discussion). In particular, it can beused to assay some biochemical measures, such asdistribution and number of receptors, in livinghuman subjects.
The last decade has also seen the application ofmolecular biological techniques to study the brain.Genetic information about the brain and its compo-nents is studied and manipulated to understand thecellular and molecular workings of the brain. Whilethese new techniques are just beginning to have animpact on the study of mental disorders, they havealready provided valuable information about recep-tor subtypes (box 4-A) and other aspects of thebiochemistry of the brain.
Information about underlying biochemical abnor-malities is also often derived from studying theactions of therapeutically effective drugs (i.e., psy-chopharmacology). In fact, many initial advances inunderstanding the biochemistry of mental disorders
came from studies of drug actions in the brain. If adrug is found to be effective in treating a disorder,examination of that drug’s chemical action in thebrain may lead to the discovery of an intrinsicpathology. For example, the finding that effectiveantidepressant drugs act on catecholamines led tothe study of these neurotransmitters in depression(see later discussion). Conversely, drug develop-ment may be guided by previously acquired knowl-edge about a disorder, which directs research effortsto create compounds that will act on an alreadyidentified pathology. If a specific neurotransmittersystem is identified as being aberrant in a disorder,drugs can be designed to interact with some aspectof that system, such as the receptors, to try to reversethe abnormality.
Anatomy and Activity
Abnormalities in the structure of the brain or in itsactivity in specific locations can contribute to mentaldisorders. In the brain, neurons that share the sameanatomical region, and to varying degrees the samefunction, are assembled into groups called nuclei.The brain is made up of hundreds of nuclei. Someconsist of neurons that produce many differentneurotransmitters, while others are predominantly ofone type. Axons extending from nuclei conveyinformation between and among them. Thus, thebrain comprises many nuclei, which are connectedby pathways of axons that contain various neuro-transmitters. Information is conveyed and processedvia networks made up of interconnected nuclei.
Some networks of nuclei are particularly relevantto mental disorders (figure 4-3). In general, these arenetworks that control cognitive (i.e., perception,recognition, reasoning, judgment, imagination), be-havioral, and emotional functions. Disruptions ofthese areas are likely to be involved in the thinkingand mood disturbances characteristic of severemental disorders. The cerebral cortex (the portion ofthe brain that is critical in decisionmaking) isimportant in this regard, especially the frontal lobes,which are considered to be the seat of higher-order. .thinkmg and which enables humans to reasonabstractly. The limbic system, a network of struc-tures (e.g., hippocampus, amygdala, parts of thetemporal lobe of the cortex) located in the upper partof the brain (figure 4-3) and involved in control ofemotional behavior, is also important in mentaldisorders. Additional areas of the brain implicated inmental disorders are the basal ganglia, a group of

Chapter 4--Mental Disorders and the Brain ● 75
Box 4-A-Cloning Dopamine Receptors
Advances in the ability to manipulate and express genetic information provide an important new means ofstudying the brain. One area in which the tools of the molecular biologist have contributed significantly is theidentification of receptor subtypes for neurotransmitters, These techniques have permitted the cloning of genes forspecific receptors and have provided a detailed characterization of the receptor’s three-dimensional structure. Notonly is this information important for understanding better how the brain works, but it also aids the developmentof drugs specifically designed to act only on certain receptors. This specificity can increase the efficacy of a drugwhile decreasing the side effects it causes. The recent identification of several receptor subtypes for the neuro-transmitter dopamine is an example of the contribution molecular biology is making to understanding the brain.
Previous to the use of molecular biological techniques, two dopamine receptors had been characterized, basedon the ability of various drugs to bind to them. For example, drugs that are effective in treating schizophrenia (calledtypical antipsychotic drugs) ail bind to the same dopamine receptor--the D2 receptor. In addition, another receptorthat binds dopamine, but not typical antipsychotic drugs, was identified and called the D 1 receptor. Other evidence,derived using pharmacological techniques, suggested that there might be additional dopamine receptors, but it wasnot until the gene for each of the dopamine receptor subtypes was identified that their existence was confirmed.
Currently, six dopamine receptor subtypes have been identified and cloned using molecular biologicaltechniques. Although all of these receptors are acted on by dopamine, they all have slightly different molecularstructures. In addition, there are some differences in their location in the brain, the cellular mechanisms that theyturn on when they are activated, and their ability to bind typical antipsychotic drugs. Both the Dl and D5 receptorsare linked to the same cellular mechanism, are located in the hippocampus and cortex, and do not readily bind typicalantipsychotic drugs. They differ in their ability to bind dopamine and dopamine-like drugs. There are two types ofD2 receptors: Both bind typical antipsychotic drugs, and both are found in parts of the limbic system, basal ganglia,and cortex. They differ in that each is linked to a different cellular mechanism, and one is a dopamineautoreceptor— a receptor that lies on the dopamine neuron itself, regulating the cell’s activity (see text). The D3 andD4 receptors are found predominantly in the limbic system. While it is unclear what cellular mechanisms areactivated by these receptors, the D3 receptor is thought to be an autoreceptor. Neither binds typical antipsychoticdrugs as effectively as D2 receptors, and the D4 receptor readily binds a new atypical antipsychotic drug, clozapine(see text).
The identification of these dopamine receptor subtypes has provided new insights into how more efficaciousantipsychotic medications can be designed. Since clozapine is a highly effective antipsychotic drug but producesfewer side effects than typical antipsychotics, it is thought that its mixture of strong binding to D4 receptors and weakbinding to D2 receptors accounts for its action. Currently there is great interest in understanding the variousdopamine receptor subtypes to determine their role in schizophrenia and how drugs can be designed to target them.
The complexity of the dopamine receptor system indicates the many ways that a single neurotransmitter canhave myriad effects in the brain. Molecular biological techniques provide an important tool for clarifying these basicbrain mechanisms, providing new information about how they maybe disturbed in mental disorders and leadingthe way for the development of more efficacious medications.
SOURCES: E. Kandel, J. Schwartz and T. Jessell (eds.), Principles of Neuroscience (New York NY: Elsevier Science publishing, 1991); P.Sokoloff, B. Giros, M. Martres, et al., ‘‘Molecular Cloning and Characterization of a Novel Dopamin e Receptor (D3) as a Targetfor Neuroleptics,” Nature 347: 146-151, 1990; R Sunahara, H. Guarn, B. O’Dowd, et al., ‘‘Cloning of the Gene for a HumanDopamine D5 Receptor With Higher Affinity for Dop amine Than Dl,’ Nature 350:614-619, 1991; H. van Tol, J. Bunzow, H. Guan,et al., “Cloning of the Gene for a Human Dopamine D4 Receptor With High Affinity for the Antipsychotic Clozapine, ’ Nature350:610-614, 1991.
nuclei just below the cerebral cortex, some of which flight response); and the raphe nuclei, also found incoordinate movement and others of which are part of the brainstem (figure 4-3), made up of serotoninthe limbic system; the hypothalamus, a collection of neurons that regulate sleep, are involved withnuclei at the base of the brain (figure 4-3) that behavior and mood, and are connected to the limbicregulate hormones and behaviors such as eating, system. It must be kept in mind, however, that if any. .drinking, and sex; the locus ceruleus, a nucleus in the of these, or other brain structures, are impaired in abrainstem (figure 4-3) made up of norepinephrine mental disorder, it is unlikely that only the functionneurons that are intimately involved in the body’s of that structure will be affected. Since the brain isresponse to stressful situations (i.e., the fight-or- organized as networks of nuclei, any structural or

Chapter Mental Disorders and the Brain ● 73
Figure 4-2—The Synapse
Nerve impulse
Auto-breakdown
receptor
Neurotransmitters ReceptorsReceiving cell
The synapse and associated structures.SOURCE: Office of Technology Assessment, 1992.
removed from the synapse so the synapse will beavailable for a new message. This is done either bythe neurotransmitter’s being taken backup into theneuron that released it (a process called reuptake) orby it being broken down chemically into compoundscalled-metabolizes (figure 4-2).
For each neurotransmitter in the brain, there arespecific receptors to which it can attach. Binding bythe neurotransmitter activates the receptor, whichcan have different effects, depending on the recep-tor. Receptors can be linked to a variety of biochem-ical and cellular mechanisms that are turned on or offby the activation of the receptor. A neuron can havethousands of receptors for many different neuro-transmitters. Some neurotransmitters activate neu-rons (excitatory neurotransmitters), while othersdecrease the activity of neurons (inhibitory neuro-transmitters).
When a neuron is activated, changes occur in itsmembrane, resulting in a shift in the balance of ions(electrically charged molecules) between the insideand outside of the neuron. This change in ionicbalance triggers an electrical impulse inside theneuron. The electrical impulse travels from the cellbody, down the axon, to the axon terminal. At the
axon terminal, the impulse causes the release ofneurotransmitter from the neuron into the synapse.
Sometimes a receptor for one neurotransmittercan affect a receptor for another neurotransmitter. Insuch cases, the receptors are biochemically coupled:The activation of one modulates the functioning ofthe other, either increasing or decreasing its activity.A neuron can also have receptors for the neurotrans-mitter it releases; these are usually located near thesite where the neurotransmitter is released into thesynapse (figure 4-2). Such receptors are acted on bythe neuron’s own neurotransmitter to regulate therelease of the neurotransmitter. Thus, these autorecep-tors, as they are called, act as a feedback mechanismto regulate a neuron’s activity. The activity of aneuron will be determined by the cumulative activityof all its various receptors.
While receptors are specific for a neurotransmit-ter, there may be a variety of receptor subtypes,linked to different cellular mechanisms, that allrespond to the same neurotransmitter. In this way,one neurotransmitter can have diverse effects invarious areas of the brain. Also, the number ofreceptors in the brain is not static. In response toincreased production of a neurotransmitter, thenumber of receptors for that neurotransmitter willdecrease; conversely, depletion of a neurotransmit-ter will result in an increase in the number ofreceptors for that neurotransmitter. This mechanismallows the brain to compensate for changes inneurotransmitter levels. Such receptor changes areimportant in therapeutics; some drugs mimic neuro-transmitters by stimulating increases or decreases inreceptor numbers. In some cases, these changes maybe directly related to the drug’s therapeutic effect.
Many chemicals have been identified as neuro-transmitters, among them acetylcholine, the cat-echolamines (norepinephrine, epinephrine, dopam-ine), serotonin, various amino acids, and peptides,including certain hormones. Various chemicals inthe brain other than neurotransmitters and theirreceptors are necessary for brain function. They maybe associated with the biochemical mechanismsactivated by neurotransmitter-receptor interactions,involved with the production and breakdown ofneurotransmitters, or responsible for carrying outmetabolic activity.
Abnormalities in any of these chemicals, theirreceptors, or the cellular mechanisms that are turnedon or off by the receptors could contribute to mental

76 ● The Biology of Mental Disorders
Figure 4-3—Brain Structures Involved inMental Disorders
Frontal cortex Hypothalamus
\ I
a,
Hippocampus Raphe nuolei
Temporal cortex
Three-dimensional drawing of the human brain.SOURCE: Adapted from Lewis E. Calver, University of Texas, Southwest-
ern Medical Center, Dallas, TX, 1992.
functional impairment in part of a network can createa disturbance throughout the network.
Structural changes associated with mental disor-ders can include anatomical abnormalities in thestructure of the brain or irregularities in the individ-ual cells within a region of the brain. The classicaltechniques for gathering information about brainstructure-the macroscopic and microscopic post-mortem examination of normal brains and brainsfrom individuals who have had mental disorders—have been augmented with a number of newertechniques and machines that make possible thestudy of the structure of the brain in living persons(table 4-l). Computerized axial tomography (CAT),which uses computers to combine a series of x-rays,provides clearer pictures of the brain than x-raysalone. Remarkably clear and detailed images ofbrain structure are obtained using magnetic reso-nance imaging (MRI) scans, which detect molecular
changes in the brain that occur when an individual isexposed to a strong magnetic field. Abnormalitiesthat can be detected by either CAT or MRI scansinclude structural brain abnormalities, changes inthe volume of brain tissue, and enlargement of thecerebral ventricles.1 Decreases in the volume ofbrain tissue and enlargement of the cerebral ventri-cles indicate either atrophy or underdevelopment ofa brain region.
The activity of the brain can also be studied todetermine damage or malfunctioning in a region ofthe brain. Neuropsychologica1 testing seeks to deter-mine brain damage by measuring deficits in aperson’s performance on various tasks. For example,deficits on tests that measure language performanceimply damage to the regions of the brain thatsubserve language skills, while poor performance oncertain types of puzzles indicates abnormalities inregions devoted to various kinds of cognitive andsensory information processing. While neuropsy-chologica1 testing is helpful in identifying areas ofbrain pathology, the measures used are indirect, andexact locations of involved regions can only beinferred. However, when combined with more directmethods of looking at the brain, they provide apowerful tool for studying brain function andanatomy.
Measurement of electrical activity in the brainusing the electroencephalograph (EEG) provides amore direct indication of brain function, and com-bining the EEG with computer analysis provides aneven more detailed measure. Electrical activity canbe measured while subjects are resting or engagingin some sort of sensory or cognitive task. Byexamining the electrical patterns of the brain,investigators can observe changes in normal brainresponses and where they occur. A shortcoming ofthese measures is that they reflect the cumulativeactivity of broad areas of the brain, usually near thesurface. This makes it more difficult to locate areasof possible pathology.
PET scanning and single-photon-emission com-puted tomography (SPECT) are imaging techniquesthat reveal brain activity. They do so by creatingcomputerized images of the distribution of radioac-tively labeled materials in the brain. Researchersadminister labeled materials to a subject either byinjection or inhalation. Subsequent distribution of
The cerebral ventricles are spaces in the brain that are filled with fluid.

Chapter 4-Mental Disorders and the Brain ● 77
Table 4-l—Techniques for Imaging the Brain
Technique How it works What it images
Computerized axial Computer construction of x-raytomography (CAT) images
Magnetic resonance Images molecular changes inimaging (MRI) brain cells when exposed to a
strong magnetic field
Computer analysis of Creates maps of brain electricalelectroencephalogram activity by computer analysis of(EEG) EEG
Single-photon-emission Creates images of the distribu-computed tomography tion of radioactively labeled sub-(SPECT) stances in the brain following
either injection into the blood orinhalation
Positron emission Creates images of the distribu-tomography (PET) tion of radioactively labeled sub-
stances following injection intothe blood
Structure
Structure and activity (when used inconjunction with a magnetically activesubstance)
Activity
Activity (regional cerebral blood flow)
Activity (regional cerebral blood flow,glucose utilization) and neurochemicalactivity (receptor number and distri-bution)
SOURCE: Office of Technology Assessment, 1992.
these materials reflects the activity of the brain.Recently, MRI scanning has also been adapted forthis function. PET, SPECT, and MRI enable research-ers to measure the utilization of glucose or theamount of blood flowing in a region of the brain (i.e.,regional cerebral blood flow). Both glucose utiliza-tion and regional cerebral blood flow are indicatorsof brain activity: The more active a region is, themore blood will flow through it and the moreglucose it will use. Abnormal activity levels inspecific brain regions, in the whole brain, or in thenormal asymmetry of activity between the two sidesof the brain can be discerned with these techniques.Also, as previously mentioned, PET scanning can bedone following the injection of labeled drugs thatattach to specific receptors, making it possible tovisualize the number and distribution of receptorpopulations. As with EEG measures, these scanningtechniques can be done either while the subject is atrest or doing a task. While the imaging techniquesnow being used to study mental disorders willundoubtedly be refined, they provide for the firsttime a window through which to view the humanbrain at work.
SCHIZOPHRENIAThe symptoms of schizophrenia reflect a broad
range of cognitive and emotional dysfunctions thatare commonly categorized as either positive ornegative symptoms (see ch. 3). Positive symptomsinclude hallucinations and delusions, paranoid psy-chosis, as well as bizarre behaviors and thought
disorder. Negative symptoms include emotionalflattening (i.e., flat affect), loss of motivation,general loss of interest, and social withdrawal. Insome cases, specific alterations in the biochemistryor anatomy of the brain have been associated witheither positive or negative symptoms. As with othersevere mental disorders, there are many cluesavailable regarding schizophrenia, and a number ofhypotheses have been put forward in an attempt tounify this information into an explanation of theunderlying pathology.
BiochemistryDopamine
The most prominent and enduring theory regard-ing the biochemistry of schizophrenia concerns therole of the neurotransmitter dopamine. This theoryis based on two sets of observations about drugaction. First, drugs that increase dopamine activity,such as amphetamine, L-dopa, cocaine, and meth-ylphenidate, sometimes induce a paranoid psychosisin normal individuals that is similar to some aspectsof schizophrenia. The same drugs, when adminis-tered to patients with schizophrenia, sometimesinduce a transitory worsening of symptoms, particu-larly increasing psychosis and disturbance ofthought. Second, and in contrast, drugs that blockcertain dopamine receptors often ease the symp-toms, in particular the positive symptoms, of schizo-phrenia. In general, there is a close correlationbetween how well these drugs block dopaminereceptors and their antipsychotic effect. The thera-

78 ● The Biology of Mental Disorders
peutic effectiveness of dopamine-blocking drugsand the ability of dopamine-enhancing drugs toworsen the symptoms of schizophrenia provideevidence for the role of excessive concentrations ortransmission of dopamine in at least some aspects ofthe disorder. Nevertheless, studies that have tried tomeasure dopamine activity in schizophrenia are lessconclusive (81).
The concentrations of certain chemicals (e.g.,homovanillic acid, a metabolize of dopamine) can bemeasured by scientists to provide information aboutdopamine activity. A number of investigators havemeasured these chemicals in the tissue and fluids ofpersons with and without schizophrenia. If higherconcentrations of dopamine are associated withschizophrenia, then higher concentrations of thesechemicals would be expected in persons withschizophrenia. The results are inconclusive. A re-view of this research (12) shows that in some studieshigher dopamine concentrations were found inpersons with schizophrenia; in others no suchassociation was found. Conflicting results have alsobeen found in studies of dopamine receptors, al-though one subtype of dopamine receptor (the D2
receptor) may be increased in schizophrenia (12).
Thus, regardless of the index of dopamine activityexamined in studies, results are variable. Datasupporting the dopamine-excess hypothesis are usu-ally contradicted by data that fail to find differencesbetween persons with schizophrenia and controls.Part of this variability is undoubtedly due to theimprecision of some of the measures used. The useof newer, more sophisticated techniques may re-solve some of these contradictions. For example, aspreviously described, there are a number of dopa-mine receptor subtypes (see box 4-A). As the abilityto study these receptor subtypes improves, altera-tions in a specific receptor population may becomeevident. Part of the variability in results may also bedue to differences in the characteristics of thepatients with schizophrenia studied. Factors such ashow long an individual has had the disorder and hisor her age when it first appeared can affect findings.
There also is some evidence that dopamineactivity may be associated with specific symptomsof schizophrenia. For example, when changes reflect-ing increased dopamine function are observed, theyoften occur in patients with prominent positivesymptoms, particularly psychosis (12). Other stud-ies support the proposition that dopamine deficiency
is associated with the negative symptoms of schizo-phrenia. For example, a correlation between lowlevels of dopamine chemicals in cerebrospinal fluidand negative symptoms has been reported (59). Inaddition, dopamine-blocking drugs used to treat thepositive symptoms of schizophrenia produce behav-iors suggestive of the negative symptoms in animalsand humans free of mental disorders (81,88). Thus,the contradictions between dopamine excess anddopamine deficiency as explanations for schizophre-nia can be reconciled by proposing that each isassociated with different symptoms of the disease—that is, positive and negative symptoms, respectively(12,60,88)-and that each involves different neuralnetworks (see later discussion). However, thesehypotheses are controversial and it is possible thatone or both are incorrect. Nonetheless, most scien-tists agree that dopamine plays some role in schizo-phrenia.
Other Neurotransmitters
Alterations in the amount or function of otherneurotransmitters in persons with schizophreniahave also been examined by researchers. Bothincreased and decreased levels of serotonin havebeen postulated as being associated with schizophre-nia. The decreased-level hypothesis was based onthe effects of LSD (lysergic acid diethylamide),which blocks serotonin activity in the brain andcauses effects that are similar to some of the positivesymptoms (e.g., hallucinations) seen inpatients withschizophrenia (21). These observations were notsupported by other data; in particular, they werecontradicted by evidence that some drugs effectiveagainst schizophrenia reduce serotonin activity.Also, as with the dopamine hypothesis, measures ofserotonin in the blood, cerebrospinal fluid, andpostmortem brain tissue do not provide clear an-swers. Both increased and decreased measures ofserotonin and its metabolizes in blood and cerebro-spinal fluid have been observed, and results frommeasures in postmortem brain tissue have beeninconclusive (53). Thus, while there is some indica-tion that serotonin activity may be altered inschizophrenia, the exact nature of its involvement isunclear.
Both an excess and a deficiency in the activity ofthe neurotransmitter norepinephrine have been asso-ciated with schizophrenia, although data indicatethat an excess of norepinephrine is more likely toproduce symptoms (80,90). Increased norepineph-

Chapter Mental Disorders and the Brain . 79
rine has been observed in the cerebrospinal fluid andblood of patients with schizophrenia (21,82). Sincedopamine and norepinephrine have complex interac-tions, namely, that disturbances in one affect theother, it is unclear whether any observed increase innorepinephrine is primary to schizophrenia or sec-ondary to changes in the dopamine system (53).
These neurotransmitters interact with and modu-late the activity of many other neurotransmitter andneuropeptide systems; awareness of this fact has ledto the study of these chemicals in schizophrenia. Theopiate peptides are thought to affect dopamineneurons, and naloxone, a drug that blocks opiatereceptors, may have antipsychotic properties (53). Inaddition, there have been findings relating otherpeptides to schizophrenia (53). Since alterations insuch neuropeptides could facilitate, inhibit, or other-wise alter the pattern of activity of other nerve cells,further study of the status of peptides in schizophre-nia is warranted.
Finally, a more specific neurotransmitter hypoth-esis involves the action of the drug phencyclidine(PCP) (31). PCP can produce symptoms that resem-ble both the positive and the negative symptoms ofschizophrenia and can exacerbate these symptoms inpeople with the disorder. It is thought that PCPproduces these dual effects by acting at differentsites in the brain (21). PCP inhibits the activity of theexcitatory neurotransmitter glutamate by interferingwith the receptor for glutamate. From that observa-tion, it has been speculated that inhibition of theglutamate receptor in the hippocampus results in thenegative symptoms associated with schizophrenia(21). PCP also weakly blocks the reuptake ofdopamine, and in other areas of the limbic systemthere is some evidence that PCP inhibition ofglutamate secondarily causes an increase in dopa-mine activity. These effects on dopamine couldresult in the positive symptoms of schizophrenia. Inboth instances, there is implicit involvement ofglutamate in the onset of symptoms of schizophre-nia. While there is currently little experimentalevidence to support this hypothesis, it represents anew avenue of investigation in schizophrenia re-search.
Thus, while it is likely that dopamine plays somerole in schizophrenia, the involvement of otherneurotransmitters is unclear. Since brain neurotrans-mitter systems interact with each other, it is oftendifficult to isolate a cause-effect relationship. The
modulatory action that neurotransmitters exert sug-gests that there may be complex interactions inschizophrenia between dopamine systems and theseother brain chemicals.
Anatomy and Activity
Alterations in a number of brain structures,notably the frontal cortex and limbic system, havebeen implicated in schizophrenia. In particular,ventricular enlargement and evidence of changes inthe size of various brain regions have been observedin imaging studies and postmortem examinations(figure 4-4). Limbic structures, such as the hip-pocampus and parts of the temporal lobes, are mostaffected. However, the specificity of these findingsfor schizophrenia has been questioned becausethey also occur in normal aging and in a variety ofother neurological and psychiatric conditions (10,21).
Attempts to replicate these findings have yieldedcontradictory results. In some cases, evidence ofchanges in the volume of the frontal cortex andtemporal lobes has been observed, but the data arenot conclusive and additional studies are needed toconfirm the results (10). Some PET studies haveexamined brain metabolism in schizophrenia andhave observed decreased activity in the frontalcortex and limbic structures, as well as increased
Figure 4-4—MRI Scan of an IndividualWith Schizophrenia
Brain structure shown of individual who does not have schizophre-nia (top) and a person who does (bottom). The ventricles areenlarged in schizophrenia (black areas).SOURCE: W. Carpenter, Maryland Psychiatric Research Center, and H.
I_Oats Associates, Inc.

80 ● The Biology of Mental Disorders
Figure 4-5-PET Scan of an IndividualWith Schizophrenia
Brain activity in an individual who does not have schizophre-nia (right) and a person who does (left). The frontal showsmore activity in schizophrenia (white areas).SOURGE: W. Carpenter, Maryland Psychiatric Research Center, and H.
Associates, Inc.
activity in the basal ganglia (10,21) (figure 4-5). Ingeneral, these studies indicate that decreased frontalcortex activity is associated with the negativesymptoms of schizophrenia. This coincides withdata from animal studies, which indicate that dam-age to the frontal lobes produces behaviors similar tothe negative symptoms.
EEG studies that show a higher incidence ofabnormal electrical activity in the brain of patientswith schizophrenia than in normal subjects providefurther evidence of the involvement of the frontalcortex. These abnormalities often appear in thetemporal lobe as well. Impairments on neuropsy-chological tests, such as problem-solving and atten-tion deficits, also indicate that these structures areaffected in schizophrenia (34,39). For example, 65percent of patients with schizophrenia often havedifficulty visually following a moving object, com-pared to 8 percent of subjects who do not haveschizophrenia (21) (see ch. 5). It is thought thatdefects in maintaining attention, as a result of adysfunction in the frontal lobes and limbic system,contribute to these visual task defects.
These data have led to a number of hypothesesthat attempt to unify the information regarding brainstructures implicated in schizophrenia. In particular,these theories assign important functions to thelimbic system and frontal cortex. The limbic system
is integral to motivation, gratification, memory, andmany other emotions and thought-processes whosedisturbance is associated with psychosis and theother positive symptoms of schizophrenia. Thefrontal cortex has been implicated in the negativesymptoms of schizophrenia. The proposed theoriesdiffer as to whether the two sets of dysfunctionsshould be viewed as dependent or independent andin the specific structures presumed to be involved.
One theory postulates that they are dependent andthat an insult during the development of the brainthat affected the functioning of the frontal cortex(see later discussion) can lead to negative symptoms(84). Since the frontal cortex and limbic system areinterconnected, with the frontal cortex inhibitingactivity in the limbic system, this theory posits thatthe dysfunction of the frontal cortex reduces theinhibition on the Iimbic system, leading to thepositive symptoms.
Another theory suggests that positive and nega-tive symptoms are mediated by two different net-works within the frontal cortex and limbic systemand that dysfunction in one of these networks isseparate from dysfunction in the other (9). Thiscoincides with data from PET studies which showthat negative symptoms are only correlated withdecreased activity in the frontal cortex.
A third theory implicates a disruption in theactivity of the basal ganglia and its interaction withother brain structures (16,17). This theory is basedon three experimental findings: First, there isincreased metabolic activity in the basal ganglia ofpatients with schizophrenia; second, patients withschizophrenia have difficulty performing visualattention tasks, which are mediated by areas of thecortex; and third, animals with lesions in dopamine-containing areas of the brain that project to the basalganglia display some of the behavioral impairmentsseen in schizophrenia. This evidence has led to thehypothesis that schizophrenia is related to impairedactivity in a network composed of the basal ganglia,certain cortical areas, and other brain structures andthat the impairment is secondary to decreaseddopamine activity.
These hypotheses attempt to find a basis for thedisturbed behaviors observed in schizophrenia; theyare overlapping and not always mutually exclusive.The available data point to networks involvingcertain limbic structures in psychosis and networksinvolving the frontal cortex in negative symptoms.

Chapter 4-Mental Disorders and the Brain ● 81
The precise interaction between these networks andthe possible involvement of other brain structuresand areas still need to be clarified. Based on thesetheories, predictions (which can themselves betested with additional studies) can be made about theinvolvement of various areas of the brain in schizop-hrenia.
Other Factors
Immune and Viral Factors
Viral theories for the cause of schizophrenia arederived from reports that a number of viral andimmune indices, such as the number and function ofimmune system cells, are deviant inpatients with thedisorder (13,32,83). Also, there is some epidemio-logical evidence to support a viral hypothesis.Schizophrenia may have a north-to-south prevalencegradient, may be endemic in a few areas (e.g.,northern Sweden), and occurs somewhat more oftenin persons born in the winter. It has also beenobserved that fetuses in the second trimester ofgestation during an influenza epidemic have anincreased risk of developing schizophrenia as adults.However, it has been difficult to conduct definitivestudies, since any potential marker of an immune orviral process associated with schizophrenia is appli-cable in only some cases and is subject to interpreta-tion as secondary to conditions associated with thedisease (e.g., crowding of hospitalized patients,exposure of individuals living in low socioeconomiccircumstances, and poor health habits).
Developmental Factors
The observed changes in brain volume of personswith schizophrenia, and the cellular alterations thataccompany these changes, are thought to be irrevers-ible but not progressive (54). Current informationsuggests that the magnitude and nature of anatomi-cal and morphological changes in schizophrenia arepresent at the onset of the disorder and do not varyover the lifetime of an individual. A possibility isthat these abnormalities reflect changes that oc-curred very early in life or in utero, either as theresult of some specific damage or a pathologicalalteration in the normal development of the brain.
Evidence that developmental factors may play arole derives from the observation that infants bornafter a complicated pregnancy or labor are atincreased risk for developing schizophrenia asadults (41,42). One mechanism by which gestational
or birth complications may alter brain developmentis diminished oxygen supply (i.e., hypoxia). Thistheory is attractive for two reasons. First, manypregnancy and birth complications are associatedwith temporary hypoxia. Second, limbic structures,especially the hippocampus, are among the mostsensitive areas in the developing brain to the adverseconsequences of hypoxia. Also, subtle deviations inneurological and psychological functioning havebeen observed from infancy in children who are athigh risk of developing schizophrenia (11). Al-though far from established, it is possible that early,adverse gestational influences on the developingbrain create a risk of both birth complications and,later, schizophrenia. A corollary to this propositionis that a pathological influence operating early ingestation alters the development of the brain tocreate subsequent vulnerability to schizophrenia. Anintriguing possible instance of this proposition is therelationship, discussed earlier, between pregnancyduring influenza epidemics and the development ofschizophrenia.
What specific alterations in the brain may resultfrom such insults is unknown; however, it is clearthat subtle deviations in the development of the braincould create dysfunctions associated with specificbehaviors. Furthermore, it is possible that suchsubtle brain abnormalities are not manifest untilmuch later in life, when new demands are placed onthe brain systems during adolescence and adulthood.Postmortem findings of abnormalities in the numberand organization of some nerve cells (1,37) suggestthat the developmental process of cell migration, bywhich the cells in the brain become organized intothe normal pattern of neuronal networks, may havegone awry in schizophrenia. Altered cell migrationcould be a genetic result, might be caused bygestational insults, or might involve an interaction ofboth. Another process that might be involved is thepruning of nerve cells that occurs as the braindevelops (18). During early development, the brainhas more neurons than it needs; the fine-tuningnecessary for efficient functioning involves elimi-nating certain nerve cells and many of the synapsesconnecting cells. Failure to prune nerve cells andsynapses adequately, or an error in selecting whichones to prune, could underlie dysfunctions that leadto the manifestation of the symptoms of schizophre-nia. Whatever developmental processes play a rolein schizophrenia is still an open question.

82 ● The Biology of Mental Disorders
Synthesis
Although various alterations in the biochemistry,anatomy, and activity of the brain have beenobserved in schizophrenia, there are several impor-tant points regarding these data (21). The highvariability among patients on any one of thebiological factors and the lack of agreement amongstudies about many of them suggest that schizophre-nia is a heterogeneous disorder, with patientsexhibiting different clusters of symptoms. Thisvariability could also reflect the effects of otherfactors, such as psychosocial variables, on thebiological components. The fact that some of thebiological abnormalities observed in schizophreniaare also seen in other conditions calls into questiontheir specificity to, and their role in, schizophrenia.
Despite the equivocal nature of the researchfindings, conclusions can still be drawn from them.Dopamine plays a role in at least some of thesymptoms of schizophrenia; however, the character-istics of that involvement are unclear, and dopa-mine’s precise relationship to the positive andnegative symptoms of schizophrenia remains to beelucidated. The role of other neurotransmitters inschizophrenia, and if and how they interact withdopamine systems, needs to be clarified. Given thecognitive and emotional functions governed by thefrontal cortex and limbic system, it is not surprisingthat alterations in these regions have been implicatedin schizophrenia. Abnormal functioning of thefrontal lobes has been one of the most consistentfindings in schizophrenia, and, while less welldocumented, there does seem to be a relationshipbetween decreased frontal cortex activity and nega-tive symptoms. Positive symptoms appear to beassociated with increased metabolic activity in thelimbic system.
While completed studies furnish valuable infor-mation regarding what might be wrong in the brainof a person with schizophrenia, the question of whyschizophrenia occurs remains unanswered. The roleof abnormal brain development or an injury to thebrain, either during development or early in life, isan important avenue of investigation. As with otherfactors associated with schizophrenia, the precisemechanisms that may be involved are subject tospeculation. The interaction of such a precipitatingevent with genetic factors (see ch. 5) is anotherplausible cause.
MOOD DISORDERSMood disorders include major depression and
bipolar disorder. As the name indicates, majordepression is marked by a deep depression that canbe unremitting. Bipolar disorders are characterizedby periods of depression alternating with manicepisodes. Sadness is a normal human emotion inresponse to various life events, but depression thathas no known cause or unremitting depression thatinterferes with normal activity is pathological.Available data regarding the role of biologicalfactors in major depression and bipolar disorderoften overlap. This reflects the fact that thesedisorders may be closely linked. The depressed statemay be mediated by the same brain regions in bothconditions. However, different brain mechanismsmay be involved in the manic state and the swingfrom depression to mania that is characteristic ofbipolar disorder.
Biochemistry
Neurotransmitter Systems
Prominent hypotheses concerning depression havefocused on altered function of the group of neuro-transmitters called monoamine (i.e., norepineph-rine, epinephrine, serotonin, dopamine), particularlynorepinephrine (NE) and serotonin (25,51,70). Evi-dence that monoamines are involved comes from theknowledge of the mechanism of action of the twoclasses of clinically effective antidepressant medica-tions—tricyclic antidepressants and monoamine ox-idase inhibitors (MAOIS). Tricyclic antidepressantsblock the reuptake of neurotransmitters, and MAOIsblock the action of monoamine oxidase, the enzymeinvolved in the chemical breakdown of the monoa-mine transmitters once they are released into thesynapse. The net effect of both of these types ofdrugs is to prolong the activity of these neurotrans-mitters in the synapse.
In the 1960s, the clinical observation that patientswho were taking a norepinephrine-blocking drug forhigh blood pressure developed depression led to thehypothesis that depression was the result of lowconcentrations of monoamine, in particular NE(25). Some experiments have shown that patientswith bipolar disorder have decreased NE metabolizesduring depression and increased amounts duringmania, which supports the NE imbalance hypothe-sis; other studies, however, have shown that patients

Chapter 4--Mental Disorders and the Brain ● 83
Box 4-B—Serotonin and Suicide
More than 30,000 Americans commit suicide each year, making it the eighth leading cause of death in theNation. It is the second leading cause of death among adolescents. Changes in a number of indices of serotoninactivity are correlated with suicide attempts and suicide completions. Suicidal behavior is associated with decreasedconcentrations of serotonin and its metabolizes in cerebrospinal fluid and the brain. Among successful suicides,decreased concentrations are usually found in the brainstem, where the raphe nuclei, the major serotonin-containingnuclei in the brain, are located. Also, increased numbers of serotonin receptors have been observed in the brains ofsuicide victims, usually in the frontal cortex. Since certain frontal cortex neurons receive connections from thoseof the raphe nuclei, it is possible that the receptor increase is a compensatory response to decreased serotonin activityin the raphe neurons. A decrease in the number of serotonin autoreceptors in suicide victims has been reported insome studies. Finally, suicide attempters, as compared to nonattempters, show decreased release of the hormoneprolactin following administration of a serotonin-stimulating drug. This blunted prolactin response is indicative ofa low level of serotonin activity. These data indicate that a net decrease in serotonin activity in the brain is associatedwith suicidal behavior.
These data do not mean that decreased serotonin causes a person to commit suicide. First of all, not everysuicide victim exhibits decreased serotonin. For example, serotonin metabolize concentrations are not reduced inindividuals with bipolar disorder who attempt suicide, compared to individuals with bipolar disorder who do notattempt suicide. Also, there is some evidence that among suicide attempters, measures of decreased serotoninactivity correlate with the lethality of the method us@ that is, the more violent the attempted suicide method (e.g.,cutting arteries v. drug overdose), the more depressed the serotonin activity. In addition, some of these samemeasures of serotonin activity, such as low levels of serotonin metabolizes in the cerebrospinal fluid and bluntedresponse to prolactin, can be observed in individuals who exhibit impulsive and aggressive behavior. This suggeststhat, rather than causing suicide, decreased serotonin activity is correlated with a behavioral predisposition that canlead to suicide. If individuals who are burdened with feelings of despondency also have depressed serotonin activity,the propensity for aggression may be directed internally, tragically resulting in a successful suicide attempt.
SOURCES: E.F. Coccaro and J.L. AstiIl, ‘‘Central Serotonergic Function in Parasuicide,’ Progress in Neuro-Psychop harmacology &Biological Psychiatry 14:663-674, 1990; K.Y. Little and D.L. Sparks, “Brain Markers and Suicide: Can a Relationship Be Found?”Journal of Forensic Sciences 35:1393-1403, 1990; J.J. Mann, V. Arango, M.D. Underwood, et al., “Neurochemical correlates ofsuicidal Behavior Involv ement of Serotonergic and Non-Serotonergic Systems,” Pharmacology and Toxicology 3:37-60, 1990;J.J. Mann, V. Arango, and M.D. Underwood, ‘ ‘Serotonin and Behavior, ‘‘Annals of the New York Academy of Sciences 60&476-484,1990; L.C. Ricci and M.M. Wellman, ‘‘Monoamines: Biochemical Markers of Suicide?” Journal of Clinical Psychology46:106-116, 1990.
with major depression exhibit increased concentra- addition, decreased dopamine metabolizes have beentions of NE metabolizes (51,70).
As more information has been gathered, it hasbecome clear that the chemistry of depression ismore complex and that other neurotransmitters,especially serotonin, maybe involved. For example,fluoxetine, a highly effective antidepressant drugthat is widely prescribed, acts exclusively on sero-tonin.
Although the results from studies of serotoninmetabolizes are not conclusive, there is some indica-tion that concentrations of serotonin are decreased inmood disorders (25). Also, low concentrations ofserotonin metabolizes have been observed in peoplewho commit suicide (box 4-B). As a result of thesefindings, it has been hypothesized that decreasedserotonin plays a role in mood disorders (25,46). In
observed in some, but not all, studies of depression.
One fact that argues against the monoamineimbalance hypothesis is the time lag betweenadministration of antidepressant medications andtheir clinical effect. These medications increaseneurotransmitter levels almost immediately uponadministration, but their therapeutic effects often donot appear until 2 or 3 weeks after initiation of drugtherapy. This time lag has led to the suggestion thatthe receptors for monoamines may be involved—specifically, that the clinical effects of these drugsare due to reductions in the number of receptors tocompensate for the drug-induced increased levels ofmonoamine neurotransmitters. It would take weeksfor such compensatory changes to come about.
One hypothesis related to drug-induced changesin receptors involves a receptor for NE (25). There

84 ● The Biology of Mental Disorders
are a number of NE receptor subtypes. One is anautoreceptor that decreases the release of NE into thesynapse when it is activated. It has been hypothe-sized that these NE autoreceptors are overly activein depression. The therapeutic effects of antidepres-sant drugs are the result of exposing the autorecep-tors to higher concentrations of neurotransmitter,which decreases their number, ultimately increasingthe activity of the NE-containing neurons. While thishypothesis would explain the delayed appearance ofclinical effects of antidepressant dregs, studies of theNE autoreceptor in depression have found nospecific evidence of an abnormality to date.
Currently, no clear evidence links abnormalserotonin receptor activity in the brain to depression(51). Increased receptors for serotonin have beenobserved in the brains of suicide victims (box 4-B),but there are conflicting results from studies thathave examined serotonin receptors in depressedpersons (25). Changes in serotonin receptor activityhave been measured indirectly in mood disorders,notably bipolar disorder, using blood platelets (atype of cell found in the blood) which also containserotonin and are used to investigate mechanismsrelated to serotonin and its receptors (46). Bothincreased numbers of a subtype of serotonin receptorand decreased sites for the reuptake of serotonin intothe platelets have been seen in the platelets ofpersons with depression (46). However, it is unclearhow these changes relate to serotonin activity in thebrain of persons with major depression and bipolardisorder.
While there is sufficient evidence to support thenotion that abnormalities in monoamine systems arean important component of depression, the datacurrently available do not provide consistent evi-dence either for altered neurotransmitter levels or fordisruption of normal receptor activity. This has ledto a dysregulation hypothesis, which states that thereis a more general perturbation in the mechanismsthat regulate the activity of the monoamine neuro-transmitters and that clinically effective drugs re-store efficient regulation (70). Linked to this hypoth-esis is the fact that the monoamine systems interactwith each other-the activity of one affects andmodulates the activity of another. Based on availabledata, it has been proposed that decreased activitywithin the NE-serotonin component of the system isassociated with depression, while increased activityof the NE-dopamine component tends to promotemania (25).
Complicating the picture is the fact that otherneurotransmitters have been implicated in bipolardisorder. Based on evidence that agents whichactivate acetylcholine systems can induce depres-sion and that agents which block such activity havesome ability to alleviate depression (51), it has beenpostulated that increased acetylcholine activity in-duces depression and decreased activity inducesmania (15,25,30,70). Furthermore, a number ofinvestigators have proposed that the salient mecha-nism may be the balance between NE and ace-tylcholine systems, with a predominance of ace-tylcholine activity associated with depression and apredominance of NE activity associated with mania(25,28,51,70). A role for the inhibitory neurotrans-mitter gamma-aminobutyric acid (GABA) has alsobeen put forth, based on the paradoxical finding thatincreased GABA activity has both an antidepressantand an antimanic effect (25,40,51). Given thatGABA is a ubiquitous inhibitory neurotransmitter, itis possible that increasing its activity can result inthe modulation of a number of other neurotransmit-ter systems, which could explain its broad range ofeffects. Finally, there is evidence that some neu-ropeptides may also be involved in mood disorders(6,23,25). In particular, decreased levels of somato-statin and increased levels of corticotropin-releasingfactor are associated with depression.
Thus, a number of neurotransmitters have beenimplicated in mood disorders, with NE and serotoninbeing the most prominent. Lithium is the mosteffective drug for the treatment of mania and forcontrolling the mood swings between depressionand mania that characterize bipolar disorder. It is notknown how lithium affects the activity of neurons,but like many other chemicals that are important tonormal brain functioning, lithium is an ion—that is,a molecule that has an electrical charge. It is thoughtthat, whatever its action on neurons, lithium hasmany different effects in the brain (8). It increasesserotonin activity, decreases acetylcholine activity,affects the activity of both norepinephrine anddopamine, and inhibits some of the intracellularmechanisms that are initiated by activation ofreceptors. Since lithium has such a broad range ofactions that can affect the neurotransmitter systemsimplicated in mood disorders, its therapeutic effectmay be due to its capacity to correct the neurotrans-mitter abnormalities associated with mania anddepression, and to prevent the changes in neuro-

Chapter 4-Mental Disorders and the Brain ● 85
chemical balance that are thought to be responsiblefor the mood swings of bipolar disorder.
Neuroendocrine Systems
Abnormalities in hormone regulation are commonin depression (7,25,70,71), perhaps because regula-tion of hormones and the glands that secrete them isunder the control of the same neurotransmitters inthe brain that are thought to be dysfunctional indepression. In particular, the activities of the pitui-tary, adrenal, and pineal glands are affected. Manyof the symptoms associated with depression (e.g.,changes in appetite, sleep, and sex drive) may berelated to these hormonal changes, which means thatthe hormonal abnormalities may be secondary to theneurotransmitter alterations of the disorder (7).Nonetheless, there is great interest in studying thesechanges in hopes of discovering a biological markerand developing diagnostic tests for depression.
A number of hormones have been studied todetermine if depressed persons consistently exhibitabnormal concentrations of them or show an abnor-mal release of them in response to some sort ofpharmacological challenge. Current information in-dicates that while some of these hormones arealtered in depression, variability in baselines andpharmacological response, as well as the possibilityof changes due to other causes, makes them unrelia-ble markers for depression (7,70,71).
Depressed persons often have elevated concentra-tions of the hormone cortisol (7,25,70,71), whichresults from increased concentrations of corticotropin-releasing factor. In healthy individuals, administra-tion of the drug dexamethasone suppresses theconcentration of cortisol in the blood. The dexametha-sone-suppression test (DST), developed as a test ofhormone functioning, has been studied as a possiblediagnostic tool in depression. Approximately 40 to50 percent of persons diagnosed with major depres-sion have an abnormal DST in that they do notsuppress cortisol in response to dexamethasone (70).In very severe cases, particularly psychoticallydepressed patients, the percentage ranges from 60 to80. It is not known why only some patients show anabnormal DST. Whether this reflects variability inresponse to DST or a subpopulation of depressedpatients has yet to be resolved. Therefore, there areseveral problems with using the DST as a diagnostictool (7,25,70,71). Aside from the fact that not alldepressed patients show an abnormal DST, a num-ber of other clinical (e.g., Alzheimer’s disease,
anorexia nervosa) and nonclinical conditions (e.g.,fasting, ingestion of caffeine) can result in abnormalDSTs. Although its effectiveness as a diagnostic toolis limited, the test maybe useful in predicting whichpatients are likely to relapse following cessation ofdrug therapy: If DST results remain abnormal duringtherapy, the patient is more likely to relapse once theantidepressant is withdrawn (7).
Another aspect of endocrine function related todepression is the association between depressionand reproduction-related events in women (2).Hormonal alterations related to menstruation, preg-nancy, childbirth, and menopause can affect neuro-transmitters that regulate mood and behavior. Theevidence regarding the relationship between thesehormonal fluctuations and the occurrence of depres-sion is mixed. Nevertheless, the clear association ofmood alterations with these reproductive events insome women suggests an area for additional investi-gation. Understanding these biochemical interac-tions could provide new insights into the pathologyof depression.
Anatomy and Activity
It is unclear which areas of the brain may beinvolved in mood disorders. The data regardinganatomical defects and activity in the brain ofpersons with mood disorders are equivocal. Giventhat few studies have been conducted and that theirresults have varied, it is impossible to come to anyconclusions regarding relationships between thedata and the cause and symptoms of mood disorders.Overall, the data suggest an association betweenmood disorders and abnormalities of large regions ofthe brain, especially the frontal and temporal lobes;they also imply an abnormal difference between theleft and right sides of the brain. Normally, the leftand right sides of the brain are involved in different,although overlapping, functions. For example, theleft is usually more specialized for language andlogical “thinking, while the right is more involvedwith spatial processing. As a result of these differentfunctions, the two halves of the brain often exhibitdifferent levels of activity. In mood disorders, someof the normal differences in activity level betweenthe right and left sides of the brain appear to bealtered.
Few postmortem studies have investigated ana-tomical alterations in the brains of persons withmood disorders, although a number of studies have

&5 ● The Biology of Mental Disorders
examined depression and mania that are secondaryto other insults to the brain (e.g., tumors, stroke,wounds) (25). Often, the trauma-induced alterationin mood occurs as a single episode of eitherdepression or mania; there are only a few reports ofbipolar disorder occurring as a result of braindamage. Although the secondary nature of thedisorders severely limits the usefulness of thesestudies, some anatomical patterns can be discerned.In general, depression and mania are associated withdamage to the frontal and temporal lobes of thebrain, while bipolar disorders are associated withdiverse areas of the brain. Depression tends to beassociated with damage to the left side of the brainand mania with damage to the right (25).
Additional information has been derived fromstudies using CAT and MRI scans (25). While notconclusive, data from CAT scans indicate thatpatients with mood disorders, especially bipolardisorder, have decreased cortical volume. The clini-cal features most frequently correlated with de-creased cortical volume are psychotic symptoms andpoor response to treatment. The few MRI studies ofpersons with bipolar disorder indicate that there maybe some structural abnormalities present, especiallyin the frontal and temporal lobes (25).
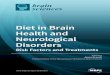
Studies measuring cerebral blood flow and glu-cose utilization have also produced some evidenceof abnormal activity in mood disorders (25,85)(figure 4-6). The available data suggest that personswith bipolar disorder, as well as persons with majordepression, show decreased activity in a specificportion of the frontal lobes called the prefrontalcortex; persons with bipolar disorder also show amore general decrease in activity involving thewhole cortex and the left frontal lobes (25). Thus,these studies implicate the left side of the brain.However, results of studies using neuropsychologi-cal testing and observations of electrical activity inthe brain caused by performing a task implicate adeficit in the right side (25,74,86). Neuropsycholog-ical testing consistently finds deficits in tasks relatedto right-hemisphere functioning, such as spatiallearning and memory, among persons with mooddisorders (25). The imaging data, which are consist-ent with the postmortem studies, are from studies ofthe brain in its resting state, whereas the neuropsy-chological testing and electrophysiological studiesmeasured the active functioning of the brain inresponse to a task. It is unclear whether thedivergence in observations represents discrete ab-
Figure 4-&PET Scans of an IndividualWith Bipolar Disorder
Brain activity in a person when depressed (top and bottom rows)and when in the manic state (middle row).SOURCE: L. Baxter, M. J. et al., “Cerebral Metabolic
Rates for Glucose in Mood Disorders: Studies With PositronEmission Tomography and F1 8,” Archivesof Genera/ Psychiatry 1985 (copyright 1985 American Medical Association).
normalities that are detected selectively by thedifferent methods. Additional data need to becollected, using imaging techniques in conjunctionwith performance tasks, to clarify this issue and todetermine the significance of these differences inactivity on the two sides of the brain.
Other Factors
Sleep and Biological Rhythms
Sleep disturbances are common in persons withmajor depression (25,38,68,70) and, like the altera-tions in endocrine function discussed earlier, arelikely to be secondary to a primary pathology. Sleepconsists of rapid eye movement (REM) sleep (thetime during which dreaming takes place) andnon-REM sleep. Both REM and non-REM sleep canbe monitored with the EEG. In the course of a night,REM and non-REM sleep cycle approximatelyevery 90 minutes. In depression, the first REMperiod occurs earlier than normal after sleep begins,the time spent in REM sleep is increased, and thelength of non-REM sleep decreases. In 80 to 85percent of depressed persons, sleep is broken byfrequent awakenings, while the remaining percent-age show features of hypersomnia. It has beensuggested that depressed persons can be differenti-ated from other individuals on the basis of the

Chapter Mental Disorders and the Brain ● 8 7
abnormalities in REM sleep (70). The early occur-rence of REM sleep has been repeatedly demon-strated in depression. Based on these observations,it has been suggested that shortened REM latency,and possibly other REM sleep measures, can be usedto diagnose depression (70); others question thespecificity of these changes to depression (25).
The sleep of persons with bipolar disorder is oftendisturbed and varies with clinical state, severity, andstage of the disorder (25). When depressed, bipolarpatients may sleep excessively, and when manic,may sleep little or not at all. Sleep can also influencethe switch from one phase to another. Sleep lossoften precedes, and may trigger, a manic episode.Also, one or two nights of sleep deprivation can havea short-term antidepressant effect (25,79). Thisevidence indicates that in some cases mania can beprevented and depression treated by appropriatemanipulation of the sleep-wake cycle (25).
The sleep cycles previously described are anexample of a biological rhythm. The precedingreport in the Office of Technology Assessment’sneuroscience series (79) describes and discussesbiological rhythms-the changes in various physio-logical and behavioral functions that repeat atregular intervals and provide a framework of tempo-ral organization for those functions-and theireffects. and consequences. While sleep stages aremeasured in minutes, many biological rhythms (e.g.,body temperature, secretion of hormones, sleep-wake cycle, alertness, memory) have a 24-hour cycleand are called circadian rhythms. For example, bodytemperature fluctuates over 24 hours, with peakbody temperature occurring during the day andlowest body temperature occurring at night.
The cyclic pattern of bipolar disorder and the factthat people with depression exhibit daily and sea-sonal fluctuations in mood suggest a link betweenmood disorders and biological rhythms. Whetherthat link is causative or correlative is unknown (79).Changes in biological rhythms have been observedin some persons with mood disorders (25,72). Thefact that animal studies have indicated that someantidepressant medications have an effect on theorganization of circadian rhythms provides a furtherlink between mood disorders and biologicalrhythms. Finally, a seasonal variation in the occur-rence of depression has been observed. A specificsyndrome of winter depression, which remits during
the summer, has been identified and named seasonalaffective disorder (SAD). Although it is not clearwhether SAD is associated with altered biologicalrhythms, it is related to changes in the length ofdaylight across the seasons. Exposure to additionallight during the winter is an effective treatment forSAD.
Kindling and Sensitization
Recurrences of mania and depression in bipolardisorder tend to increase in frequency overtime. Theneurobiological phenomena of electrical kindlingand behavioral sensitization observed in animalsmay provide clues to the physiological mechanismsunderlying this pattern of cycling (25). Repeatedadministration of low-level electrical stimulation toan area of the brain results in kindling, or increasedresponsiveness to electrical stimulus that leads to thedevelopment of seizures. If the stimulation isrepeated frequently enough, the area becomes sosensitive that seizures will occur spontaneously.Similarly, behavioral sensitization refers to theincreasing behavioral response that results fromrepeated administration of the same dose of astimulant drug.
While these phenomena are not directly analo-gous to the mood disturbances of bipolar disorder,they do share certain characteristics (62). Forexample, in each, early episodes require a precipitat-ing event, while later ones can occur spontaneously.Also, repeated exposure to precipitating events leadsto more frequent occurrence of episodes. Thesecharacteristics coincide with the concept that earlyepisodes of mania or depression result from somesort of psychosocial stress but later episodes canoccur in the absence of such a stimulus, and with theobservation that episodes tend to occur with ashorter and shorter cycle.
Thus, the same or similar brain mechanismscontrolling kindling and sensitization could play arole in the cycling of bipolar disorder. Someevidence for this is seen in the fact that serotonin,norepinephrine, and GABA, neurotransmitters im-plicated in mood disorders, all inhibit the kindlingphenomenon (25). Also, lithium, which is effica-cious in treating bipolar disorder, blocks behavioralsensitization, while carbamazepine, an antiseizuremedication that is also effective in bipolar disorder,blocks kindling.

88 ● The Biology of Mental Disorders
Immune and Viral Factors
Results from some studies have raised the possi-bility that mood disorders may be associated withabnormalities in the body’s immune system or withviral infection (25). For example, some studiesindicate that persons with major depression mayhave a compromised immune system, as indicatedby their diminished response to infectious chal-lenges. Also, some studies have found increasedantibodies to certain viruses that infect the nervoussystem (i.e., cytomegalovirus, herpes, and Bornadisease virus) in some persons with mood disorders.Thus, there is limited evidence that immune systemdysfunction or viral infection may be associatedwith mood disorders in some persons, although theavailable data are far from conclusive. If suchassociations exist, it is unclear what relationshipthey may have to the onset and symptoms of thedisorder.
Synthesis
There are many disparate pieces to the puzzle ofmood disorders, and fitting the available onestogether is difficult. Early theories that depressionand bipolar disorder are the result of a simpleimbalance in norepinephrine or that a specificanatomical locus could be identified are now recog-nized as simplistic. Clinically effective drugs haveshown that adjusting the activity in monoamine-containing regions of the brain has an antidepressanteffect. Whether this indicates there is a primarydysfunction in these regions in depression has yet tobe proved. The implications of the other factorsdescribed in this section are also unclear.
An approach that encompasses the diversity ofexperimental data and is at the same time harmoni-ous with the clinical profile of the disorders isneeded in order to construct a meaningful hypothe-sis. As discussed in chapter 3, it is unclear whetherdepression is a single disorder or a collection ofdisorders. This possible heterogeneity complicatesattempts to delineate biological factors that might beinvolved. It is likely that the same regions of thebrain mediate depression in both major depressionand bipolar disorder. If separate subtypes of depres-sion exist, this same network of structures is likelyto be involved; what differentiates the disorders maybe the factors that disrupt the network. This ideacoincides with information suggesting that mooddisorders occur because integrated control systems
in the brain are disrupted, rather than because ofdefects in specific regions. The explanations thatthere is an overall dysregulation in the balancebetween the different monoamine neurotransmittersystems and that the brain mechanisms whichcontrol biological rhythms may be involved in mooddisorders are examples of hypotheses involvingdisruptions of integrated control systems. As moreinformation is gathered about these and othersystems, researchers will gain a clearer understand-ing of how they maybe disrupted in mood disorders.
ANXIETY DISORDERSAnxiety is a normal human emotion that can help
people cope with certain situations. It is only whenanxiety or its manifestations become excessive andinterfere with normal performance or health thatthey are considered pathological and termed adisorder (see ch. 3). Anxiety disorders includegeneralized anxiety disorder, panic disorder, obsessive-compulsive disorder (OCD), social and simplephobias, and posttraumatic stress disorder (PTSD).This discussion will be limited to the disorders inwhich biological factors have been most extensivelystudied, namely, OCD and panic disorder.
Obsessive-Compulsive Disorder
Idiosyncratic daily rituals and odd personal habitsare ubiquitous. It is only when obsessions orcompulsions, or both, cause marked distress, occupymore than 1 hour a day, and cause significant socialor occupational dysfunction that the diagnosis ofOCD is made (63) (see ch. 3). OCD is commonlyaccompanied by depression. Symptoms includerecurrent obsessions with fears of contamination,harming others, and worries that doors are notlocked or lights have not been turned off. Compul-sions such as washing, checking, counting, andrearranging are common. Though most patientsknow that these thoughts and behaviors are irra-tional, they cannot put them out of their mind. Theinvoluntary, repetitive nature of the cognitive ormotor behaviors associated with OCD, coupled withrecent experimental findings, suggests a role forbiological factors in OCD.
Biochemistry
Drugs that are effective in treating OCD act byblocking the reuptake of serotonin into the neuronfrom which it was released (49,50,87). Not allpersons with OCD respond to these drugs (91),

Chapter Mental Disorders and the Brain ● 89
however, and it is unclear whether these personsrepresent a subgroup of patients with OCD (91). Thepotency of drugs that block serotonin reuptakesuggests that persons who do respond may haveabnormal serotonin functioning, but supportingevidence is meager. Like other neurotransmittersystems, the serotonin system is complex. Serotoninis found in a number of specific areas of the brain,and several receptor subtypes have been identified.While a few studies have shown that drugs that blockserotonin receptors can exacerbate OCD symptoms,no abnormalities in the synthesis, release, reuptake,metabolism, or receptors of serotonin in patientswith OCD have been identified in other studies (87).Also, while the reuptake-blocking effects of drugsoccur immediately, the therapeutic response usuallydoes not develop until after several weeks oftreatment (24,87). This delay suggests that theclinical effect could be the result of adaptive changesin the serotonin or other neurotransmitter systems inresponse to the changes in serotonin levels inducedby the drugs (87). Thus, it is not certain whetherthese drugs act directly on a primary defect of thedisorder or whether they act indirectly, via theserotonin system, to counteract the effects of aprimary defect.
It has also been proposed that dopamine systemsplay a role in OCD (24). Symptoms of OCDsometimes result from damage to the basal ganglia,which have high concentrations of dopamine. Tour-ette’s syndrome, a disorder characterized by motorand vocal tics, and often symptoms of OCD as well,is thought to result from a dysfunction of thedopamine system in the basal ganglia. Based onobservations that serotonin can inhibit the activity ofdopamine systems and that the basal ganglia receiveinput from serotonin-containing neurons, a hypothe-sis has been put forward that an alteration in thenormal interaction of these neurotransmitter systemsin the basal ganglia may be involved in OCD (24).There are some preliminary findings that drugs thatact on dopamine may have an effect on OCD (24),and data from anatomical studies also indicate a rolefor the basal ganglia in OCD. This hypothesis isconsidered in greater detail in the next section,which describes the basal ganglia and some of theiranatomical connections.
Anatomy and Activity
Persons with OCD exhibit a variety of abnormali-ties on neuropsychological tests (91). In general,
329=309 O - 92 - 4 : QL3
Figure 4-7—PET Scan of an IndividualWith Obsessive-Compulsive Disorder
Brain activity in the brain of a person with OCD (right) and the brainof a person without OCD (left). In OCD, there is increased activityin the frontal cortex.SOURCE: L. Baxter, UCLA Center for Health Sciences, Los Angeles, CA.
these tests point to dysfunctions in the frontal lobes,basal ganglia, and hippocampus. For example,persons with OCD often perform poorly on tests thatmeasure memory and attention. PET studies ofglucose utilization have shown greater than normalactivity in parts of the basal ganglia and an area ofthe frontal cortex, the orbital cortex, in OCD (4,5,91)(figure 4-7). Data from the few CAT studies thathave been ‘done indicate that the only differencebetween the brains of OCD patients and controls isa decrease in the size of various regions in the basalganglia (64,91). These data, coupled with thosepreviously discussed, lead to the hypothesis thatOCD is the result of an abnormal interactionbetween the basal ganglia and other areas of thebrain, principally the orbital cortex (4,5,35,64,91).These areas work together to coordinate movementin response to thought. If the basal ganglia aredamaged, involuntary movements such as tics occur.
The thoughts and impulses that often make upobsessions (e.g., those related to aggression, hy-giene, sex, and danger) are thought to be generatedin the frontal cortex. In normal individuals, the basalganglia-orbital system filters these impulses, puttingthem aside so that they are not acted upon. Accord-ing to this theory of OCD, the filtering effect thatkeeps an individual from acting on thoughts orimpulses does not work properly. As a result, athought occurs and the person takes action. Again,the association with Tourette’s syndrome is striking.Individuals with this disorder exhibit not only motor

90 ● The Biology of Mental Disorders
tics, but involuntary vocalizations, often of anobscene or socially unacceptable nature (such asracial epithets). The basal ganglia-orbital cortexhypothesis posits a dysfunction in the normal controlof thoughts (obsessions), which can lead to reactivemotor activity (compulsions).
Panic Disorder
Panic disorder is marked by recurrent periods ofintense fear that last for several minutes. The attacksare not triggered by anxiety-provoking situations,and patients often report that they occur ‘‘out of theblue. ’ Many persons with panic disorder experiencevarying degrees of anxiety between attacks inanticipation of the next panic attack (57). This ‘‘fearof fear’ often results in patients with panic disorderdeveloping agoraphobia, the fear of being in publicplaces.
Several theories have been postulated to explainpanic disorder (57). One views panic as the result ofhyperactivity of the physiological mechanisms thatare normally activated in stressful situations (i.e., thesympathetic nervous system). Another posits thatindividuals have an increased psychological sensi-tivity to normal fluctuations in physiological re-sponses. This theory suggests that patients maymisinterpret normal physiological changes as dan-gerous, inducing more anxiety and precipitating apanic attack. Another theory suggests that there is aprimary defect in brain mechanisms related to theneurotransmitter norepinephrine, which is associ-ated with the sympathetic response. A role forsensitivity to the chemicals lactate and carbondioxide, for hyperventilation, and for dysfunction inthe temporal lobe of the brain have also beenproposed. There is experimental evidence to sup-port, or in some cases refute, these various theories.Thus, while there are a lot of puzzle pieces, there iscurrently no unified theory of panic disorder.
Biochemistry
Information about the pharmacology associatedwith panic disorder can be derived both from drugsthat are effective in treating the disorder and fromagents that induce a panic attack when given to apatient. The most effective drugs for treating anxietyare the benzodiazepines. In high doses, these drugsare also effective in controlling panic disorder.Benzodiazepines exert their antianxiety effects indi-rectly, by increasing the action of the inhibitory
neurotransmitter GABA. The discovery that thereare specific receptors in the brain for benzodiaze-pines indicates that there must be a chemicalproduced by the brain that would normally attach tothese receptors (although such a chemical has yet tobe discovered). Benzodiazepine receptors are cou-pled to GABA receptors, and activation of theformer accentuates the effects of GABA, whichturns off overly active brain cells (14,76).
Unlike GABA and its receptors, which are foundthroughout the brain, benzodiazepine receptors arelocated in only a few brain structures. Thus, not allGABA receptors are coupled with benzodiazepinereceptors. The GABA receptors that are coupled tobenzodiazepine receptors and that respond to thedrug are known as GABAA receptors. The areas ofthe brain that contain both benzodiazepine andGABAA receptors include the hippocampus and theamygdala, both limbic system structures (76). Asdescribed previously, the Limbic system plays a rolein controlling emotional behavior. Thus, it is thoughtthat the antianxiety effect of benzodiazepines resultsfrom their action on GABAA receptors in thehippocampus and amygdala.
Another compound, buspirone, is effective fortreating general anxiety, but instead of affectingGABA, it acts on other chemical systems in thebrain. Buspirone decreases the activity of the neuro-transmitter serotonin in some areas of the brain andactivates receptors for the neurotransmitter dopa-mine in other areas (76). Buspirone acts on serotoninsystems through a complex interaction with anumber of different subtypes of serotonin receptors.This action, coupled with other experimental find-ings, has led to the speculation that increasedactivity in serotonin-containin g areas, particularlythe raphe nuclei, maybe involved in anxiety (55). Itis thought that the raphe nuclei, via their connectionswith the limbic system, may be involved in mediat-ing anxious behavior and that activation wouldcause anxiety.
The most effective drugs for treating panicdisorder are the drugs used to treat depression,although they exert a therapeutic action in panic thatis different from that in depression (76). The efficacyof these drugs has led to the theory that panic resultsfrom overactivity of the norepinephrine systems inthe brain that mediate the fight-or-flight response,

Chapter Mental Disorders and the Brain ● 91
principally the locus ceruleus (3,43,55,65). It shouldbe kept in mind, however, that the neurons in thelocus ceruleus make connections with neurons in thelimbic system and can affect their activity. Thehypothesis is that a panic attack is the result ofinappropriate activation of the norepinephrine sys-tem in the locus ceruleus. Studies have shown thatpanic attacks can be caused by drugs that increaseeither the activity of cells in the locus ceruleus or therelease of norepinephrine from them, whereas theantidepressants used to treat panic decrease theactivity of the locus ceruleus (29,55,61,76).
Any number of agents can provoke panic attacksin persons who suffer from panic disorder, includingthe chemical lactate (administered intravenously)and carbon dioxide (inhaled). At a high enoughconcentration, carbon dioxide will also induce panicin controls. The mechanism by which these agentscause panic attacks is unknown (22,27,73,76). Lac-tate has complex actions in the brain, includingeffects on serotonin, norepinephrine, and othertransmitter systems, as well as areas of the brain thatrespond to changes in blood chemistry and regulaterespiration (73). Inhalation of carbon dioxide upsetsthe balance of oxygen in the blood and can affect itsacidity (27). The areas of the brain that monitor andcontrol functions such as respiration and the cardio-vascular system are connected with the locus cerul-eus as part of the fight-or-flight response. One theoryholds-that the norepinephrine system in the locusceruleus is unusually sensitive in persons with panicdisorder. Thus, according to this theory, lactate andcarbon dioxide cause changes in either the body orthe brain that indirectly activate the norepinephrinesystem in the locus ceruleus, precipitating a panicattack (27,55,73,92). Lactate induces a panic attackin about 80 percent of persons with panic disorder(55). This high correlation has led to the suggestionthat lactate response can be considered a diagnosticmarker for the disorder (20), although variability inthe characteristics of the response among patientshas called this into question (55).
While it seems likely that the locus ceruleus isinvolved in panic disorder, other experimentalevidence raises the question as to whether that roleis primary or secondary to the cause of the disorderand whether other brain systems are also involved(76). For example, serotonin has also been impli-cated in the genesis of panic attacks (55,58,76).Serotonin connections to the locus ceruleus inhibit
the activity of locus ceruleus cells, and drugs thatpotentate the action of serotonin suppress panicattacks (76). It has been postulated that a primarydecrease in activity in this serotonin-inhibitingsystem may play a role in inducing panic attacks (58)and that the role of the locus ceruleus is secondaryto this effect. In addition, the action of caffeineindicates that other brain systems besides the locusceruleus may be involved. Caffeine can precipitatea panic attack in persons with panic disorder(55,76,77). As a result, people who suffer from panicattacks often learn, on their own, to avoid caffeine-laden products such as coffee and chocolate. Caf-feine’s principal action in the brain is to block thereceptors for the inhibitory neurotransmitter ade-nosine. However, caffeine also has some effect onnorepinephrine, dopamine, and benzodiazepine sys-tems. It is not known whether caffeine producespanic by inhibiting adenosine activity, some otheraction, or a combination of these (77). It is alsounclear how or whether caffeine’s panic-inducingaction relates to the occurrence of panic disorder.
Anatomy and Activity
The few CAT and MRI studies that have exami-ned the brain structure of persons with panicdisorder provide evidence of brain atrophy orunderdevelopment, particularly in the frontal andtemporal lobes (33). However, given the limitednumber of studies that have been done, the signif-cance of these results is unclear and must beconsidered preliminary (33).
Abnormal activity has also been observed in thebrains of persons with panic disorder (26,44,45,67).At rest, panic disorder patients who are sensitive tolactate exhibited increased cerebral blood flow to theparahippocampal gyrus (PHG), an area of thecerebral cortex that is associated with the limbicsystem (figure 4-8). Normal controls or lactate-insensitive panic patients did not show these changes.Based on these results, it was proposed that a PHGabnormality was involved in a predisposition topanic, and it was further hypothesized that activationof a norepinephrine pathway to the PHG initiates anattack (67). However, this hypothesis is based onlimited data, and conflation will require addi-tional studies. Furthermore, it does not explain whatmechanism might be present in lactate-insensitivepanic disorder patients. Other studies have demon-

92 ● The Biology of Mental Disorders
Figure 4-8-PET Scan of an IndividualWith Panic Disorder
IMPLICATIONS FORTREATMENT
Whole brain activity (left side) and abnormal activity in theparahippocampal gyrus (right side) in the brain of a person withpanic disorder in the nonpanic state.SOURCE: E. Good Samaritan Hospital, Phoenix, AZ.
strated that there is an increase in cerebral blood flowduring lactate-induced panic attacks (67).
Synthesis
There is evidence that a number of differentbiological factors play a role in OCD and panicdisorder. The possible role of the basal ganglia-orbital cortex system in OCD is an intriguing theory,coupling areas of the brain involved in cognitive andmotor activity. Further examination of these brainregions, the role of dopamine mechanisms, and theirinteractions with serotonin systems are importantareas for future research related to OCD. Both limbicstructures and the locus ceruleus are implicated inpanic disorder. Data suggest that the limbic struc-tures mediate generalized feelings of anxiety, influ-enced by the activity of GABA, while the locusceruleus controls an active response to anxiety-provoking stimuli (i.e., panic attacks). The anatomi-cal connections between these two regions of thebrain suggest that there might be some interaction ofthese systems in panic disorder, but additional studyof these systems and their interaction is necessary.
One of the greatest promises of research into thebiology of mental disorders is the development ofmore efficacious treatments-particularly drugs. Atthe same time, effective treatment of a mentaldisorder must take into consideration all aspects ofthe disorder—biological, psychological, and social.Thus, developments related to biological factorsassociated with a disorder contribute to the totaltherapeutic protocol available to treat patients.
The antipsychotic drug chlorpromazine, used totreat persons with schizophrenia, provides an exam-ple of the development of a biological treatment. Thediscovery that chlorpromazine was an antipsychoticdrug was serendipitous (36). The drug was originallydeveloped in the search for an effective antihista-mine; the chance clinical observation that it had anantipsychotic effect led to its use in schizophrenia.Once chlorpromazine’s effect was established, re-search into its mechanism of action led to the findingthat it exerted its effect by blocking the D2 dopaminereceptor subtype (see earlier discussion). This led inturn to the development of additional antipsychoticdrugs, called typical antipsychotics, that also act byblocking D2 dopamine receptors.
The chlorpromazine story also illustrates the pointthat most therapeutic advances in psychophar-macology have occurred by chance. A drug discov-ered to be efficacious was then examined further, toadvance researchers’ understanding of the biologicalmechanisms underlying a disorder (36).
The impetus for developing new drugs comesfrom the fact that current drugs are imperfect (89).Side effects are common, and not all patientsrespond to a given drug. In general, these problemsresult from existing drugs’ inability to act selectivelyon the symptoms of a disorder. For example, whiletypical antipsychotic drugs act by blocking D2
receptors in areas of the brain involved withschizophrenia symptoms, they also block D2 recep-tors in other areas of the brain, which produces themovement side effects characteristic of these drugs.Another example is the side effects associated withantidepressant drugs, which result when the antide-pressants act on other neurotransmitter systemsbesides the monoamine systems thought to beinvolved with depression.

Chapter Mental Disorders and the Brain ● 9 3
Beyond the need for more efficacious drugs withfewer side effects, the financial impact that moreeffective treatments can have is another factordriving the search for new drugs. Improved treat-ments can decrease total treatment costs by reducingthe need for hospitalization; they can decrease otherfinancial effects as well, such as lost wages due todisability. For example, a study conducted in 1980estimated that the introduction of lithium in 1969,for the treatment of bipolar disorder, resulted in anaverage yearly savings in treatment costs of $290million in the United States (66). It was alsoestimated that in the first year following the intro-duction of lithium, $92 million in lost wages wasregained (66).
By attaining a better understanding of whatneurochemical systems are affected in a disorder andhow those systems interact with others, moreeffective drugs can be developed to treat thesymptoms of a disorder while minimizing sideeffects. The recent strides that have been made inbasic neuroscience research, particularly advancesin molecular and cellular neurobiology, will facili-tate this process (75,78). The ability to clonereceptor subtypes and identify precisely the molecu-lar structure of receptors and other biochemicalconstituents of the brain will enable scientists toconstruct drugs that act more precisely. Thus, thedevelopment of drugs for mental disorders is enter-ing a new phase in which both clinical and basicresearch findings will be applied to the design ofmore efficacious medications.
The antipsychotic drug clozapine and the antide-pressant fluoxetine are examples of this new genera-tion of drugs. Clozapine, a so-called atypical anti-psychotic drug, not only blocks D2 receptors but alsoacts on other dopamine receptors (see box 4-A) andon serotonin receptors to create different effects onthese systems in different areas of the brain (47).Clozapine is thought to block sufficient dopamine inappropriate areas of the brain to control psychosis,while acting on other areas of the brain to avert theblanket D2 blockade that produces side effects.Unlike traditional antidepressants, which have abroad effect on catecholamine and other neurotrans-mitter systems, fluoxetine (Prozac) was designedspecifically to block serotonin reuptake (69). As aresult, it has an antidepressant action equivalent tothat of older drugs, but without many of their sideeffects.
Table 4-2—Drugs in Development forMental Disorders
Disorder United States Other countries
Schizophrenia . . . . . . . . . . . . . . . . . . 76 42
Mood disorders . . . . . . . . . . . . . . . . 83 61
Anxiety disorders . . . . . . . . . . . . . . . 91 46
SOURCE: PJB Publications, Pharmaprojecfs (Surrey, England: PJB Publi-cations, 1992).
Both of these drugs are improvements on oldermedications, but neither is totally without problems.Although clozapine does not produce the movementside effects associated with typical antipsychoticdrugs, it is associated with an even more dangerousside effect. About 2 percent of persons takingclozapine develop a potentially deadly blood dis-ease, agranulocytosis. As a result, anyone taking thedrug must be tested regularly; if there is anyindication of the disease, treatment must be stopped.The need for constant monitoring makes administra-tion of clozapine costly, ranging between $6,000 and$9,000 a year (19). While fluoxetine has many fewerside effects than older antidepressants, it is associ-ated with such adverse reactions as nausea, nervous-ness, insomnia, and headache (56).
Despite these problems, the advantages of thesedrugs make them highly popular. For example, inspite of the costs associated with clozapine, resultsfrom a study demonstrated that over a 2-year periodthere was a savings of approximately $16,000 perpatient, per year, as a result of decreased hospitalize-tion among 37 patients who had taken the drug (48).Total U.S. sales of clozapine in 1991 were estimatedto be $60 million (19), while 1990 sales forfluoxetine were put at $500 million (52). Currently,a number of other drugs, which may representfurther improvements on the medications that havebeen used in the past to treat mental disorders, arebeing developed and tested (table 4-2). These newdrugs represent the latest efforts to apply informa-tion derived from the study of the biology of mentaldisorders to treatment of patients.
SUMMARY AND CONCLUSIONS
Evidence exists for the activity of a variety ofbiological factors in each disorder reviewed in thisreport. However, it is difficult to put the strands ofevidence together in a unified hypothesis about therole of biological factors in a given disorder.

94 ● The Biology of Mental Disorders
Most of the biological factors that have beenidentified relate to changes in the brain that arecorrelated with a disorder. These include alterationsin neurotransmitter systems, such as the associationof increased or decreased levels of dopamine withthe various symptoms of schizophrenia and the roleof monoamines in mood disorders. Disruptions inbrain activity are associated with disorders as well,such as the decreased activity found in the frontallobes of persons with schizophrenia and the in-creased activity in the basal ganglia of persons withOCD. These factors, and the others discussed in thischapter, provide insights into the mechanisms un-derlying the symptoms displayed by patients. Abetter understanding of such mechanisms shouldenable scientists to develop more effective treat-ments.
Less is known about the causes of mentaldisorders. The influence of various factors, such asdevelopmental and viral factors, has been hypothe-sized, but as yet there is no definitive explanation forany of these disorders. To understand what leads tothe onset of mental disorders, researchers mustconsider the role of psychological and social factorsand how they may interact with a pathologicalbiological condition. For example, the alterations inthe limbic system and locus ceruleus associated withpanic disorder may represent a biological predispo-sition that is shaped by an individual’s experiencesto determine whether and how the disorder ismanifested, while the kindling-sensitization modelof bipolar disorder suggests that life events canmodify abnormal brain activity.
It is essential to learn how the healthy brain works.Research in the basic neuroscience provides thefoundation for research on the biology of mentaldisorders. Advances in the neuroscience haveresulted in the development of new techniques andimprovements on old ones that greatly increase ourability to study the brain. Combining such tech-niques as neuropsychological testing or biochemicalanalysis with brain imaging techniques extends thatability even further. Current research is increasinglytaking multidimensional approaches to the study ofmental disorders, integrating data concerning differ-ent aspects of brain functioning and behavior intotestable hypotheses. That trend is expected toaccelerate.
Essential to this effort will be strategies forstudying the integrated networks of brain structures
that control behaviors. Some mental disorders maybe collections of disorder subtypes, indicating thatthe normal functioning of a network that mediates abehavior can be disrupted at various points. Theultimate goals of research are to understand howbrain structures work in concert to produce behavior,how this process is disrupted in mental disorders,and what factors cause it to go awry.
CHAPTER 4 REFERENCES1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
Altshuler, L.L., Conrad, A., Kovelman, J.A., et al.,‘‘Hippocampal pyramidal Cell Orientation in Schiz-ophrenia: A Controlled Neurohistologic Study of theYakoviev Collection,’ Archives of General Psychia-try 44:1094-1098, 1987.American Psychological Association, Women andDepression, E. McGrath, G.P. Keita, B.R. Strickland,and N.F. Russo (eds.) (Washington, DC: AmericanPsychological Association, 1990).Ballenger, J. C., “Toward an Integrated Model ofPanic Disorder,’ American Journul of Orthopsychi-atry 59:284-293, 1989.Baxter, L.R., ‘‘Brain Imaging as a Tbol in Establish-ing a Theory of Brain Pathology in ObsessiveCompulsive Disorder,’ Journal of Clinical Psychia-try 51:22-25, 1990.Baxter, L. R., Schwartz, J.M., Guze, B. H., et al.,“PET Imaging in Obsessive Compulsive DisorderWith and Without Depression,” Journal of ClinicalPsychiatry 51:61-69, 1990.Berger, P.A., and Nemeroff, C. B., “Opioid Peptidesin Affective Disorders, ” Psychopharmacology: TheThird Generation of Progress, H.Y Meltzer (cd.)(New York, NY: Raven Press, 1987).Brown, G. M., “Psychoneuroendocrinology of De-pression,” Psychiatric Journal of the University ofOttawa 14:344-348, 1989.Bunney, W.E., and Garland-Bunney, B.L., “Mecha-nisms of Action of Lithium in Affective Illness: Basicand Clinical Implications, ” Psychopharmacology:The Third Generation of Progress, H.Y. Mekzer(cd.) (New York, NY: Raven Press, 1987).Carpenter, W.T., Buchanan, R.W., Kirkpatrick, B., etal., “Negative Symptoms: A Critique of CurrentApproaches,” Proceedings of the Workshop onNegative/Positive Schizophrenia, June 29-30, 1990(Heidelberg: Springer-Verlag, in press).Cleghorn, J. M., Zipursky, R. B., and List, S.J.,“Structural and Functional Brain Imaging in Schizo-phrenia,’ ‘JournulofPsychiatricNeuroscience 16:53-74, 1991.Cornblatt, B., Winters, L., and Erlenmeyer-Kimling,L., ‘Attentional Markers of Schizophrenia: EvidenceFrom the New York High-Risk Study,” Schizophre-nia: Scient$ic Progress, S.C. Schulz and C.A.

Chapter Mental Disorders and the Brain . 95
T’ammin ga (eds.) (New York, NY: Oxford UniversityPress, 1989).
12. Davis, K.L., Kahn, R. S., KO, G., et al., “Dopamine inSchizophrenia: A Review and Reconceptualization,’American Journal of Psychiatry 148:1474-1486,1991.
13. DeLisi, L.E., “Viral and Immune Hypotheses forSchizophrenia,’ Psychopharmacology: The ThirdGeneration of Progress, H.Y Meltzer (cd.) (NewYork, NY: Raven Press, 1987).
14. Dilsaver, S. C., “Generalized Anxiety Disorder,”American Family Physician 39:137-144, 1989.
15. Dilsaver, S. C., and Coffman, J.A., “CholinergicHypothesis of Depression: A Reappraisal,” Journalof Clinical Psychopharmacology 9:173-179, 1989.
16. Early, T. S., Posner, M. I., Rieman, E.M., et al.,“Hyperactivity of the Left Striato-Pallidal Projec-tion. Part I: Lower Level Theory,” PsychiatricDevelopments 2:85-108, 1989.
17. Early, T. S., Posner, M.T., Reiman, E. M., et al., “LeftStriato-Pallidal Hyperactivity in Schizophrenia. PartII: Phenomenology and Thought Disorder,” Psychi-atric Developments 7:109-121, 1989.
18. Feinberg, I., ‘‘Cortical P~ning and the Developmentof Schizophrenia, ’ Schizophrenia Bulletin 15:477-490, 1989.
19. Freudenheim, M., ‘*Seeking Safer Treatments forSchizophrenia,’ New York Times, Jan. 15, 1992, p.47.
20. Fyer, A, J., Liebowitz, M. R., German, J. M., et al.,“Lactate Vulnerability of Remitted Panic Patients,”Psychiatry Research 14:143-148, 1985.
21. Garza-Trevino, E. S,, Volkow, N. D., Cancro, R., etal., “Neurobiology of Schizophrenia Syndromes,”Hospital and Community Psychiatry 41:971-980,1990.
22. Glover, V., and Sandier, M., “Tribulin and Stress:Clinical Studies on a New Neurochemical System,’Frontiers of Clinical Neuroscience, vol. 8, Neurobi-ology of Panic Disorder, J.C. Ballenger (cd.) (NewYork, NY: Alan R. Liss, 1990).
23. Gold, P. W., and Rubinow, D. R., “NeuropeptideFunction in Affective Illness: Corticotropin-Releasing Hormone and Somatostatin as ModelSystems,” Psychopharrnucology: The Third Gener-ation of Progress, H.Y. Meltzer (cd.) (New YorkNY: Raven Press, 1987).
24. Goodman, W. K., McDougle, C.J., Price, L. H., et al.,“Beyond the Serotonin Hypothesis: A Role forDopamine in Some Forms of Obsessive CompulsiveDisorder,” Journal of Clinical Psychiatry 51:36-43,1990.
25. Goodwin, F. K., and Jamison, K. R., Manic-Depressive Illness (New York, NY: Oxford Univer-sity Press, 1990).
26. German, J.M., Liebowitz, M.R., Fyer, A.J., etal., “ANeuroanatomical Hypothesis for Panic Disorder,”American Journal of Psychiatry 146:148-161, 1989.
27. German, J.M., andPapp, L.A., “RespiratoryPhysiol-ogy of Panic,” Frontiers of Clinical Neuroscience,vol. 8, Neurobiology of Panic Disorder, J.C. Bal-lenger (cd.) (New York, NY: Alan R. Liss, 1990).
28. Hasey, G., and Hanin, I., “The Cholinergic-Adrenergic Hypothesis of Depression ReexaminedUsing Clonidine, Metoprolol, and Physostigmine inan Animal Model,” Biological Psychiatry 29;127-138, 1991.
29. Heninger, G.R., and Charney, D. S., “MonoamineReceptor Systems and Anxiety Disorders,” Psychi-atric Clinics of North America 11:309-326, 1988.
30. Janowsky, D. S., and Overstreet, D.H., “CholinergicDysfunction in Depression,” Pharmacology andToxicology 66(suppl. 3):100-111, 1990.
31. Javitt, D. C., and Zukin, S.R., “Recent Advances inthe Phencyclidine Model of Schizophrenia,’ Ameri-can Journal of Psychiatry 148:1301-1308, 1991.
32. Kaufman, C.A., and Ziegler, R.J., “The Viral Hy-pothesis of Schizophrenia,” Receptors and Ligandsin Psychiatry, A.K. Sen and T. Lee (eds.) (Cam-bridge, England: Cambridge University Press, 1987).
33. Kellner, C., and Roy-Byrne, P.P., “Computed To-mography and Magnetic Resonance Imaging in PanicDisorder,” Frontiers of Clinical Neuroscience, vol.8, Neurobiology of Panic Disorder, J.C. Ballenger(cd.) (New York, NY: Alan R. Liss, 1990).
34. Keshavan, M. S., and Ganguli, R., “Biology ofSchizophrenia,’ Progress in Basic Clinical Pharmac-ology, vol. 3, The Biological Basis of PsychiatricTreatment, R. Pohl and S. Gershon (eds.) (Basel:Karger, 1990).
35. Khanna, S., “Obsessive-Compulsive Disorder: IsThere a Frontal Lobe Dysfunction?” BioZogicaZPsychiatry 24:602-613, 1988.
36. Klerman, G., “Future Prospects for Clinical Psy-chopharmacology, “ Psychopharmacology: The ThirdGeneration of Progress, H.Y Meltzer (cd.) (NewYork, NY: Raven Press, 1987).
37. Kovelman, J.A., and Scheibel, A. B., “ANeurohisto-logical Correlate of Schizophrenia,’ BioZogicaZ Psy-chiatry 19:1601-1621, 1984.
38. Kupfer, D.J., Frank, E., Jarrett, D.B., et al., “Interre-lationship of Electroencephalographic Sleep Chrono-biology and Depression,” Biological Rhythms andMentaZ Disorders, D.J. Kupfer, T.H. Mo* and J.D.Barchas (eds.) (New Yorlq NY: Guilford Press,1988).
39. L%n, S., Yurgelun-Todd, D., and Craft, S., “Contri-butions of Clinical Neuropsychology to the Study ofSchizophrenia,’ Journal of Abnormal Psychology98:341-356, 1989.

96 ● The Biology of Mental Disorders
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
Lloyd, K. G., Zivkovic, B., Scatton, B., et al., “TheGABAergic Hypothesis of Depression,” Progress inNeuropsycho-Pharrnacology and Biological Psychi-atry 13:341-351, 1989.Lyon, M., Barr, C. E., Cannon, T.D., et al., “FetalNeural Development and Schizophrenia,” Schizo-phrenia Bulletin 15:149-161, 1989.McNeil, ‘IF., “Perinatal Influences in the Develop-ment of Schizophrenia,’ Biological Perspectives ofSchizophrenia, H. Helmchen and T.A. Henn (eds.)(New York, NY: John Wiley & Sons, 1987).Maser, J.D., and Woods, S.W., “The BiologicalBasis of Panic: Psychological Interactions,’ Psychi-atric Medicine 8:121-147, 1990.Mathew, R.J., and Wilson, W.H., “Cerebral BloodFlow in Anxiety and Panic,” Frontiers of ClinicalNeuroscience, vol. 8, Neurobiology of Panic Disor-der, J.C. Ballenger (cd.) (New York, NY: Alan R.Liss, 1990).Mathew, R.J., and Wilson, W.H., “Anxiety andCerebral Blood Flow,’ American Journal of Psychi-atry 147:838-849, 1990.Meltzer, H., “Serotonergic Dysfunction in Depres-sion, ’ British Journal of Psychiatry 155:25-31,1989.Meltzer, H., “The Mechanism of Action of NovelAntipsychoticDrugs,” Schizophrenia Bulletin 17:263-287, 1991.Meltzer, H., “Dimensions of Outcome With Cloza-pine,” British Journal of Psychiatry 160:46-53,1992.Murphy, D.L., and Pigott, TA., “A ComparativeRole for Serotonin in Obsessive Compulsive Disor-der, Panic Disorder, and Anxiety,” Journal ofClinical Psychiatry 51(suppl.):53-58, 1990.Murphy, D.L., Zohar, J., Benkelfat, C., et al.,“Obsessive-CompulsiveD isorder as a5-HT Subsystem-Related Behavioral Disorder,” British JournaZ ofPsychiatry Supplement 8:15-24, 1989.Nair, N.P., and Sharma, M., “Neurochemical andReceptor Theories of Depression,’ Psychiatric Jour-nal of the University of Ottawa 14:328-341, 1989.Newsweek, ‘The Promise of Prozac,’ Mar. 26,1990,pp. 38-41.Neylan, T. C., and van Kammen, D.P., “BiologicalMechanisms of Schizophrenia: An Update,” Psychi-atric Medicine 8:41-52, 1990.North, C. S., “New Concepts of Schizophrenia,”Comprehensive Therapy 15;8-21, 1989.Nutt, D.J., “The Pharmacology of Human Anxiety,”Pharmacology Therapeutics 47:233-266, 1990.Pary, R., Tobias, C., and Lippmann, S., “Fluoxetine:Prescribing Guidelines for the Newest Antidepres-sant, ” Southern Medical Journal 82:1005-1009,1989.
57.
58.
59.
60.
61<
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
Pasnau, R. O., and Bystrits@, A., “An Overview ofAnxiety Disorders,” Bulletin of the MenningerClinic 54:157-170, 1990.Pecknold, J, C., “Serotonin Abnormalities in PanicDisorder,” Frontiers of Clinical Neuroscience, vol.8, Neurobiology of Panic Disorder, J.C. Ballenger(cd.) (New York, NY: Alan R. Liss, 1990).Pickar, D., Breier, A., Hsiao, J.K., et al., “Cerebro-spinal Fluid and Plasma Monoamine Metabolizes andTheir Relation to Psychosis,” Archives of GeneralPsychiatry 47:641-648, 1990.Pickar, D., Litman, R. E., Konicki, P.E., et al.,‘‘Neurochemical and Neural Mechanisms of Positiveand Negative Symptoms in Schizophrenia,’ ModernProblems in Pharmacopsychiatr-y 24:124-125, 1990.Pohl, R., Yeragani, V., Balon, R., et al., “Isoproterenol-Induced Panic: A Beta Adrenergic Model of PanicAnxiety,” Frontiers of Clinical Neuroscience, vol. 8,Neurobiology of Panic Disorder, J.C. Ballenger (cd.)(New York, NY: Alan R. Liss, 1990).Post, R.M., and Weiss, S.R.B., “Non-HomologousAnimal Models of Affective Illness: Clinical Rele-vance of Sensitization and Kindling,” Animal Mod-eZs of Depression, G. Koob, C. Elders, and D.J.Kupfer (eds.) (Boston, MA: Birkhauser, 1989).Rapoport, J. L., “The Waking Nightmare: An Over-view of Obsessive Compulsive Disorder,” Journalof Clinical Psychiatry 51(suppl.):25-28, 1990.Rapoport, J. L., and Wise, S. P., “Obsessive-Compulsive Disorder: Evidence for Basal GangliaDysfunction,” Psychopharmacology Bulletin 24:380-384, 1988.Redmond, D.E., “Neurochemical Basis for Anxietyand Anxiety Disorders: Evidence From Drugs WhichDecrease Human Fear and Anxiety,” Anxiety and theAnxiety Disorders, A.H. ‘lhma and J.D. Maser (eds.)(Hillsdale, NJ: Lawrence ErlbaumAssociates, 1985).Reifman, A., and Wyatt, R.J., “Lithium: A Brake inthe Rising Cost of Mental Illness,” Archives ofGeneral Psychiatry 37:385-388, 1980.Reiman, E. M., “PET, Panic Disorder, and NormalAnticipatory Anxiety,” Frontiers of Clinical Neuro-science, vol. 8, Neurobiology of Panic Disorder, J.C.Ballenger (cd.) (New York, NY: Alan R. Liss, 1990).Reynolds, C.F., Gillin, J. C., and Kupfer, D.J., ‘Sleepand Affective Disorders, ’ Psychopharmacology:The Third Generation of Progress, H.Y. Meltzer(cd.) (New York, NY: Raven Press, 1987).Rickels, K., and Schweizer, E., “Clinical Overviewof Serotonin Reuptake Inhibitors, ’ Journal of CZini-cal Psychiatry 51:9-12, 1990.Rothschild, A. J., “Biology of Depression,” MedicalClinics of North America 72:765-790, 1988.Rubin, R.T., “Pharmacoendocrinology of MajorDepression,” European Archives of Psychiatry andNeurological Sciences 238:259-267, 1989.

Chapter Mental Disorders and the Brain . 97
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
Sack, D.A., Rosenthal, N.E., Parry, B.L., et al.,“Biological Rhythms in Psychiatry,” Psychophar-macology: The Third Generation of Progress, H.Y.Meltzer (cd.) (New York, NY: Raven Press, 1987).Sandberg, D. P., and Liebowitz, M. R., “PotentialMechanisms for Sodium Lactate’s Induction ofPanic,” Frontiers of Clinical Neuroscience, vol. 8,Neurobiology of Panic Disorder, J.C. Ballenger (cd.)(New York, NY: Alan R. Liss, 1990).Small $ J. G., “Psychiatric Disorders and EEG,”Electroencephalograph: Basic Principles, ClinicalApplications, & Related Fields, 2nd cd., E. Nieder-meyer and F.H. DaSilva (eds.) (Baltimore, MD:Williams & Wilkins, 1987).Snyder, S. H., “Molecular Strategies in Neuropsy-chopharmacology: Old and New,” Psychopharma-cology: The Third Generation of Progress, H.Y.Meltzer (cd.) (New York, NY: Raven Press, 1987).Teicher, M. H., “Biology of Anxiety,” MedicalClinics of North America 72:791-814, 1988.Uhde, T.W., “Caffeine Provocation of Panic: AFocus on Biological Mechanisms,” Frontiers ofClinical Neuroscience, vol. 8, Neurobiology of PanicDisorder, J.C. Ballenger (cd.) (New York NY: AlanR. Liss, 1990).Uhl, G. R., Jayararnan, A., and Nishimori, S., “Neu-ropharmacologic Tahniques in the Molecular Biol-ogy of Schizophrenia, ’ Advances in Neuropsychia -try and Psychopharmacolo~, vol. 1, SchizophreniaResearch, C.A. Tamrninga and S.C. Schultz (eds.)(New York, NY: Raven Press, 1991).U.S. Congress, Office of Technology Assessment,Biological Rhythms: Implications for the Worker,OTA-BA-463 (Washington, DC: U.S. GovernmentPrinting Office, 1991).van Karnmen, D. P., and Gelemter, J. P., “Biochemi-cal Instability in Schizophrenia I: The Norepineph-rine System,’ Psychopharmacology: The Third Gen-eration of Progress, H.Y. Meltzer (cd.) (New YorkNY: Raven Press, 1987).van Karnmen, D. P., and Kelley, M., “Dopamine andNorepinephrine Activity in Schizophrenia: An Inte-
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
grative Perspective,” Schizophrenia Research 4:173-191, 1991.van Karnmen, D. P., Peters, J., Yao, J., et al.,“Norepinephrine in Acute Exacerbations of ChronicSchizophrenia,’ Archives of General Psychiatry47:161-168, 1990.Waltrip, R.W., Carrigan, D.R., and Carpenter, W.T,“Immunopathology and Viral Reactivation,” Jour-nul of Nervous & Mental Disorders 178:729-738,1990.Weinberger, D.R., “Implications of Normal BrainDevelopment for the Pathogenesis of Schizophre-nia,” Archives of General Psychiatry 44:660-669,1987.Wiesel, F.-A., “Positron Emission Tomography inPsychiatry,” Psychiatric Developments 1:19-47,1989.Williamson, P. C., and Kaye, H., “EEG MappingApplications in Psychiatric Disorders,” CanadianJournal of Psychiatry 34:680-686, 1989.Winslow, J.T, and Insel, TR., “Neurobiology ofObsessive Compulsive Disorder: A Possible Role forSerotonin,” Journul of Clinical Psychiatry Sl(suppl.):27-31, 1990.Wise, R. A., ‘ ‘Neuroleptic-Induced Anhedonia ,” Ad-vances in Neuropsychiatry and Psychopharmacol-ogy, vol. 1, C.A. Tamminga and S.C. Schulz (eds.)(New York, NY: Raven Press, 1991).Wyatt, R.J., “Introduction: Side Effects,” Psy-chopharmacology: The Third Generation of Prog-ress, H.Y. Meltzer (cd.) (New York, NY: RavenPress, 1987).Wyatt, R.J., Kirch, D. C., and DeLisi, L.E. “Schizo-phrenia: Biochemical, Endocrine, and Immunologi-cal Studies,” Comprehensive Textbook of Psychia-try, vol. 1, 5th cd., H.I. Kaplan and B.J. Sadock (eds.)(Baltimore, MD: Williams & Wilkins, 1989).Zohar, J., Insel, T., and Rasmussen, S. (eds.), ThePsychobiology of Obsessive-Compulsive Disorder(New York, NY: Springer Publishing, 1991).Zuckerman, M., Psychobiology of Personality (Camb-ridge, England: Cambridge University Press, 1991).