-
7/30/2019 Menstrual Cycle Lect 2013
1/33
1
Menstrual cycle
Physiology
Dr. Atef Abood
-
7/30/2019 Menstrual Cycle Lect 2013
2/33
2
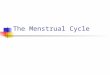
Ovaries
Primordial follicle one layer of squamouslike follicle
cells surrounds the oocyte
Primary follicle two or more layers of cuboidalgranulosa cells
enclose the oocyte
Secondary follicle has a fluid-filled space betweengranulosa
cells that coalesces to form a centralantrum
Graafian follicle secondary follicle at its mostmature stage
that bulges from the surface of theovary
Ovulation ejection of the oocyte from the ripeningfollicle
Corpus luteum ruptured follicle after ovulation
-
7/30/2019 Menstrual Cycle Lect 2013
3/33
3
-
7/30/2019 Menstrual Cycle Lect 2013
4/33
4
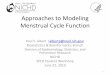
Oogenesis
At puberty, one activated primary oocyte producestwo haploid
cells
The first polar body
The secondary oocyte
The secondary oocyte arrests in metaphase II and isovulated
If penetrated by sperm the second oocyte completes
meiosis II, yielding: One large ovum (the functional gamete)
A tiny second polar body
-
7/30/2019 Menstrual Cycle Lect 2013
5/33
5
-
7/30/2019 Menstrual Cycle Lect 2013
6/33
6
Ovarian Cycle
Monthly series of events associated with the
maturation of an egg
Follicular phase period of follicle growth
(days 114)
Luteal phase period of corpus luteum
activity (days 1428)
Ovulation occurs midcycle
-
7/30/2019 Menstrual Cycle Lect 2013
7/33
7
-
7/30/2019 Menstrual Cycle Lect 2013
8/33
8
Follicular Phase
This phase is under the effect of FSH and to a little extent
LH.
It starts by activation of several; primordial follicles.
At the 6th day only one follicle starts to grow rapidlybecoming
a dominant follicle called the Graffian follicle while
the others regress. The primordial follicle, directed by the
oocyte, becomes a
primary follicle
Primary follicle becomes a secondary follicle The theca
folliculi and granulosa cells cooperate to produce estrogens
The zona pellucida forms around the oocyte The antrum is
formed
-
7/30/2019 Menstrual Cycle Lect 2013
9/33
9
Follicular Phase (Cont.)
The secondary follicle becomes a vesicular
follicle
The antrum expands and isolates the oocyte and
the corona radiata
The full size follicle (vesicular follicle) bulges from
the external surface of the ovary
The primary oocyte completes meiosis I, and thestage is set for
ovulation
-
7/30/2019 Menstrual Cycle Lect 2013
10/33
10
-
7/30/2019 Menstrual Cycle Lect 2013
11/33
11
Ovulation
Ovulation occurs when the ovary wall ruptures
and expels the secondary oocyte
Mittelschmerz a twinge of pain sometimes
felt at ovulation
1-2% of ovulations release more than one
secondary oocyte, which if fertilized, results in
twins
-
7/30/2019 Menstrual Cycle Lect 2013
12/33
12
Luteal Phase
After ovulation, the ruptured follicle collapses,granulosa cells
enlarge, and along with internalthecal cells, form the corpus
luteum
The corpus luteum secretes progesterone and
estrogen If pregnancy does not occur, the corpus luteum
degenerates in 10 days, leaving a scar (corpusalbicans)
If pregnancy does occur, the corpus luteum produceshormones
until the placenta takes over that role (atabout 3 months)
-
7/30/2019 Menstrual Cycle Lect 2013
13/33
13
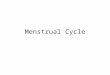
Uterine (Menstrual) Cycle
Series of cyclic changes that the uterineendometrium goes
through each month in responseto ovarian hormones in the blood
: Menstrual phase Days 1-5
uterus sheds all but the deepest part of the endometrium
Days 6-14: Proliferative (preovulatory) phaseendometrium
rebuilds itself
Days 15-28: Secretory (postovulatory) phase
endometrium prepares for implantation of theembryo
-
7/30/2019 Menstrual Cycle Lect 2013
14/33
14
Endometrium
Has numerous uterine glands that change in length
as the endometrial thickness changes
Stratum functionalis:
Undergoes cyclic changes in response to ovarian hormones
Is shed during menstruation
Stratum basalis:
Forms a new functionalis after menstruation ends
Does not respond to ovarian hormones
-
7/30/2019 Menstrual Cycle Lect 2013
15/33
15
Proliferative phase
Duration: 2 weeks
Thickness: 0.5mm 5mm
Under the influence of estrogens from the developing
follicle, the endometrium increases rapidly in thickness
from the fifth to the fourteenth days of the menstrual
cycle.
As the thickness increases, the uterine glands are
drawn out so that they lengthen, but they do notbecome
convoluted or secrete to any degree. These
endometrial changes are also called the preovulatory or
follicular phase of the cycle.
-
7/30/2019 Menstrual Cycle Lect 2013
16/33
16
Secretory phase
Duration: 2 weeks
Thickness: 5-6mm After ovulation, the endometrium becomes
more
highly vascularized and slightly edematous underthe influence of
estrogen and progesterone from
the corpus luteum. The glands become coiled and tortuous, and
they
begin to secrete a clear fluid. Consequently, thisphase of the
cycle is called the secretory or luteal
phase. Late in the luteal phase, the endometrium, like the
anterior pituitary, produces prolactin, but thefunction of this
endometrial prolactin is unknown.
-
7/30/2019 Menstrual Cycle Lect 2013
17/33
17
Menses
If fertilization does not occur, progesterone levels
fall,depriving the endometrium of hormonal support
Spiral arteries kink and go into spasms and endometrialcells
begin to die
The functional layer begins to digest itself
Spiral arteries constrict one final time then suddenlyrelax and
open wide The rush of blood fragments weakened capillary beds
and the functional layer sloughs Nonclotting menstrual blood
mainly comes from artery
(75%) Interval: 24-35 days (28 days). duration: 2-6 days.
the
first day of menstrual bleeding is consideredy by day 1
Shedding: 30-50 ml
-
7/30/2019 Menstrual Cycle Lect 2013
18/33
18
Menstruation
Menstrual blood composition
is predominantly arterial, with only 25% of theblood being of
venous origin. It contains tissuedebris, prostaglandins, and
relatively large amountsof fibrinolysin from endometrial tissue.
Thefibrinolysin lyses clot, so that menstrual blood doesnot
normally contain clots unless the flow isexcessive.
The usual duration: 3-5 days, but flows as short as 1day and as
long as 8 days can occur in normal women.
-
7/30/2019 Menstrual Cycle Lect 2013
19/33
19
Menstruation
The amount of blood lost may range normally
slight spotting to 80 mL; the average amount lost
is 30 mL.
Loss of more than 80 mL is abnormal. Obviously,
The amount of flow can be affected by various
factors, including the thickness of the
endometrium, medication, and diseases that
affect the clotting mechanism. After
menstruation, a new endometfrom rium
regenerates from the stratum basale.
-
7/30/2019 Menstrual Cycle Lect 2013
20/33
20
Menses (Cont.) When the corpus luteum regresses, hormonal
support for the endometrium is withdrawn.
The endometrium becomes thinner, which adds tothe coiling of the
spiral arteries. Foci of necrosis
appear in the endometrium, and these coalesce. There is in
addition spasm and then necrosis of the
walls of the spiral arteries, leading to spottyhemorrhages that
become confluent and produce
the menstrual flow.
-
7/30/2019 Menstrual Cycle Lect 2013
21/33
21
Menses (Cont.)
The vasospasm is probably produced by locally
released prostaglandins. There are large
quantities of prostaglandins in the secretory
endometrium and in menstrual blood, and
infusions of PGF2 produce endometrial necrosisand bleeding.
One theory of the onset of menstruation holds
that in necrotic endometrial cells, lysosomalmembranes break
down, with the release of
enzymes that foster the formation of
prostaglandins from cellular phospholipids.
-
7/30/2019 Menstrual Cycle Lect 2013
22/33
22
Changes of other genital organs
Cervix
During follicular phase estrogen causes mucus to be
thin,clear, watery and the the midcycle a drop can be
stretched into a long, thin thread that may be 8-12cm or more in
length. In addition, it dries in an
arborizing, fern-like pattern
During luteal phase progesterone causes mucus to
be thick, opaque, tenacious and cellular and loss of
ability to form fern like appearance.
-
7/30/2019 Menstrual Cycle Lect 2013
23/33
23
-
7/30/2019 Menstrual Cycle Lect 2013
24/33
24
Changes of other genital organs
Cyclic changes in the vagina
Under the influence of estrogens, the vaginal
epithelium becomes cornified,
Under the influence of progesterone, a thick
mucus is secreted, and the epithelium proliferates
and becomes infiltrated with leukocytes.
-
7/30/2019 Menstrual Cycle Lect 2013
25/33
25
Changes of other genital organs
Cyclic changes in the breast Estrogens cause proliferation of
mammary ducts.
progesterone causes growth of lobules and alveoli.
The breast swelling, tenderness, and painexperienced by many
women during the 10 days
preceding menstruation are probably due to
distention of the ducts, hyperemia, and edema of
the interstitial tissue of the breast. All these changesregress,
along with the symptoms, during
menstruation.
-
7/30/2019 Menstrual Cycle Lect 2013
26/33
26
Establishing the Ovarian Cycle
During childhood, ovaries grow and secrete
small amounts of estrogens that inhibit the
hypothalamic release of GnRH
As puberty nears, GnRH is released; FSH and
LH are released by the pituitary, which act on
the ovaries
These events continue until an adult cyclic
pattern is achieved and menarche occurs
-
7/30/2019 Menstrual Cycle Lect 2013
27/33
27
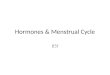
Hormonal Interactions During the Ovarian
Cycle
Day 1 GnRH stimulates the release of FSH and LH
FSH and LH stimulate follicle growth and maturation, and
low-level estrogen release
Rising estrogen levels: Inhibit the release of FSH and LH
Estrogen levels increase and high estrogen levels have apositive
feedback effect on the pituitary, causing a suddensurge of LH
The LH spike stimulates the primary oocyte to completemeiosis I,
and the secondary oocyte continues on tometaphase II
-
7/30/2019 Menstrual Cycle Lect 2013
28/33
28
Hormonal Interactions During the Ovarian
Cycle
Day 14 LH triggers ovulation
LH transforms the ruptured follicle into a corpus
luteum, which produces inhibin, progesterone, and
estrogen These hormones shut off FSH and LH release and
declining LH ends luteal activity
Days 26-28 decline of the ovarian hormones
Ends the blockade of FSH and LH
The cycle starts anew
-
7/30/2019 Menstrual Cycle Lect 2013
29/33
29
-
7/30/2019 Menstrual Cycle Lect 2013
30/33
30
-
7/30/2019 Menstrual Cycle Lect 2013
31/33
31
-
7/30/2019 Menstrual Cycle Lect 2013
32/33
32
Summary of hormonal control of the cycle
In an important sense, regression of the corpus luteum
(luteolysis) starting 3-4 days before menses is the key to
themenstrual cycle. PGF2 appears to be a physiologic
luteolysin,
but this prostaglandin is only active when endothelial cells
producing ET-1 are present. Therefore it appears that at least
in
some species luteolysis is produced by the combined action
ofPGF2
and ET-1. In some domestic animals, oxytocin secreted by
the corpus luteum appears to exert a local luteolytic
effect,
possibly by causing the release of prostaglandins. Once
luteolysis begins, the estrogen and progesterone levels fall
andthe secretion of FSH and LH increases. A new crop of
follicles
develops to start a new cycle
-
7/30/2019 Menstrual Cycle Lect 2013
33/33
33
Menstrual Abnormalities
Anovulatory cycle
Amenorrhea
Primary amenorrhea: period never occurs
Secondary amenorrhea stop of the cycle after normal
periods have occurred. Menorrahgia: excessive bleeding
during
menstruation
Hypomenorrhea: scanty or little bleeding
Metrorrahgia: bleeding between cycles.
Oligomenorrhea: reduced frequency of the periods.