Embed Size (px)
Citation preview
MENOPAUSA I ENVELLIMENT: MALALTIA D’ALZHEIMER
Enfoc des del ginecòleg
M. Manubens
Departament de Ginecología, Obstetricia i ReproduccióINSTITUT UNIVERSITARI DEXEUS
Barcelona

ESTRÓGENOS
SNC
Neurotransmisores Modulando la:Neuropéptidos Excitabilidad eléctricaNeuroesteroides Función sináptica
genómico no genómico
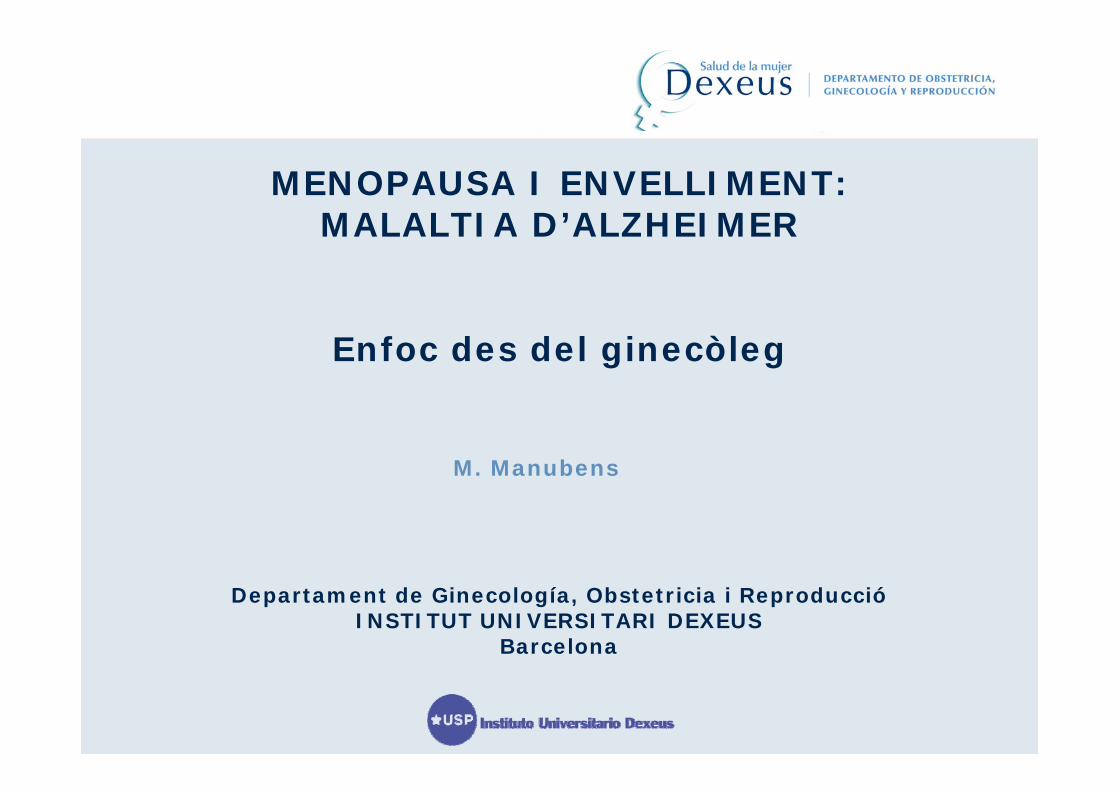
Estrógenos y cerebro
Existen RE en el cerebro en regiones implicadas en la cognición Incluyendo•Cortex cerebral 1•Hipocampo 2•Prosencéfalo 3
la actividad colinérgica 4, serotonérgica 5,6 y dopaminérgica 7en la mujer postmenopáusica
Tienen influencia sobre la función cognitiva
1Shughrue PJ, et al. J Comp Neurol. 1997;388:507-25; 2Weiland NG, et al. J Comp Neurol. 1997;388:603-12; 3Shughrue PJ, et al. Neuroscience. 2000;96:41-9; 4van Amelsvoort T, et al. Psychoneuroendocrinology. 2003;28:101-12; 5Kugaya A, et al. Am J Psychiatry. 2003;160:1522-4; 6van Amelsvoort TA, et al. Psychoneuroendocrinology. 2001;26:493-502; 7Craig MC, et al. Psychoneuroendocrinology. 2004;29:1309-16.
– Estrogen in therapeutic doses alters brain activation– Results suggest that estrogen affects brain areas
involved in working memory
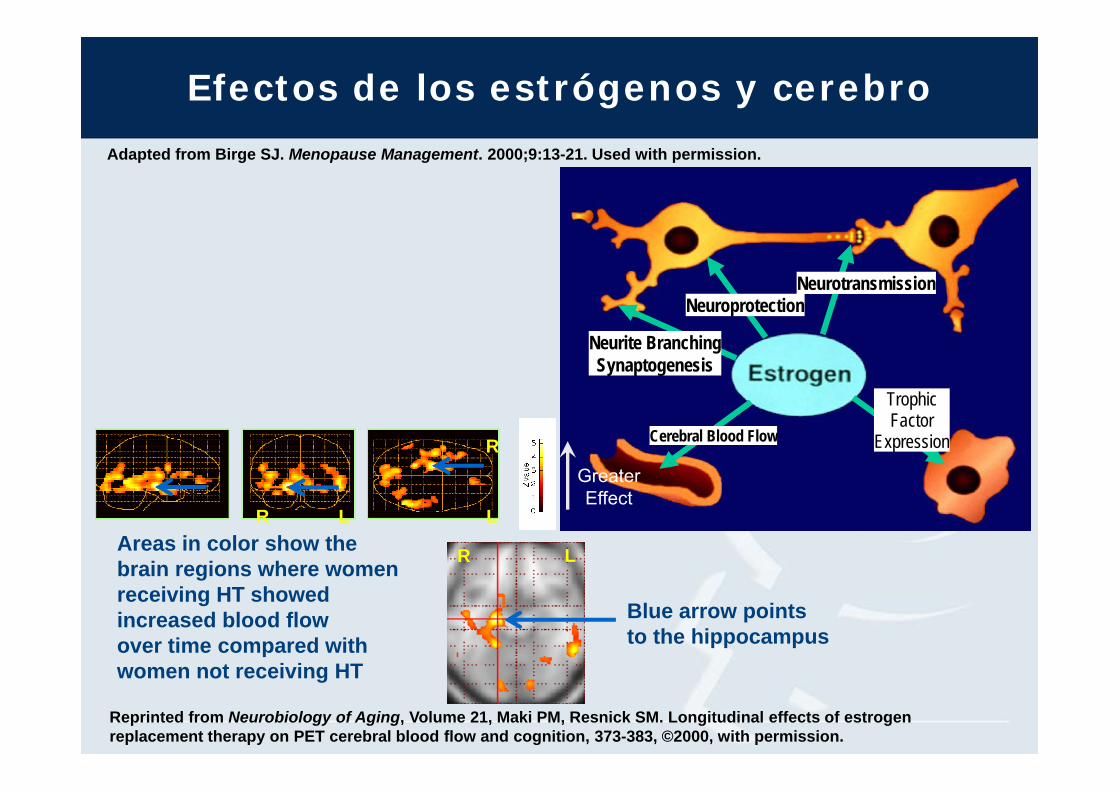
Efectos de los estrógenos y cerebro
NeurotransmissionNeuroprotection
Neurite BranchingSynaptogenesis
Cerebral Blood Flow
Trophic Factor
Expression
Adapted from Birge SJ. Menopause Management. 2000;9:13-21. Used with permission.
GreaterEffect
R
R L L
R L
Blue arrow points to the hippocampus
Areas in color show the brain regions where women receiving HT showed increased blood flow over time compared with women not receiving HT
Reprinted from Neurobiology of Aging, Volume 21, Maki PM, Resnick SM. Longitudinal effects of estrogen replacement therapy on PET cerebral blood flow and cognition, 373-383, ©2000, with permission.
Menopausia y función cognitiva
Las evidencias clínicas demuestran como durante el períodoclimatérico la ausencia de estrógenos en el sistema límbicoinduce modificaciones del carácter, comportamiento y funcióncognitiva, funciones que mejoran tras la administración deestrógenos
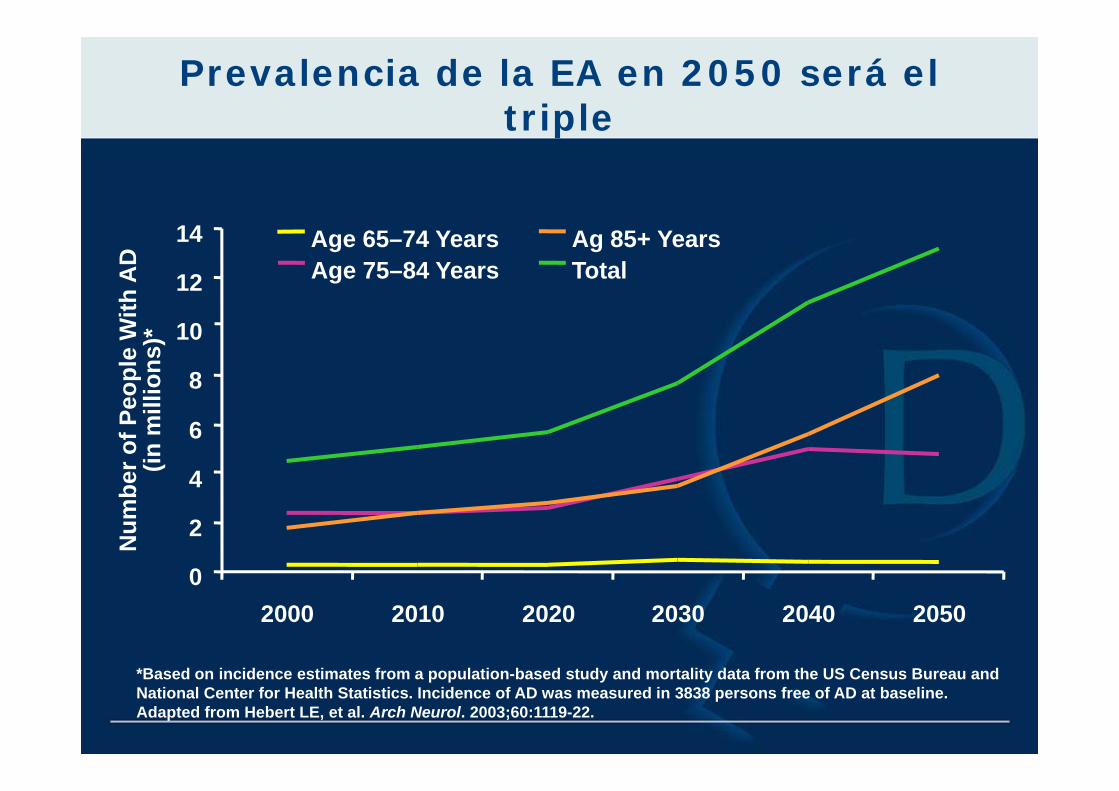
Prevalencia de la EA en 2050 será el triple
Age 65–74 YearsAge 75–84 Years
Ag 85+ YearsTotal
Num
ber o
f Peo
ple
With
AD
(in m
illio
ns)*
0
2
4
6
8
10
12
14
2000 2010 2020 2030 2040 2050
*Based on incidence estimates from a population-based study and mortality data from the US Census Bureau and National Center for Health Statistics. Incidence of AD was measured in 3838 persons free of AD at baseline.Adapted from Hebert LE, et al. Arch Neurol. 2003;60:1119-22.
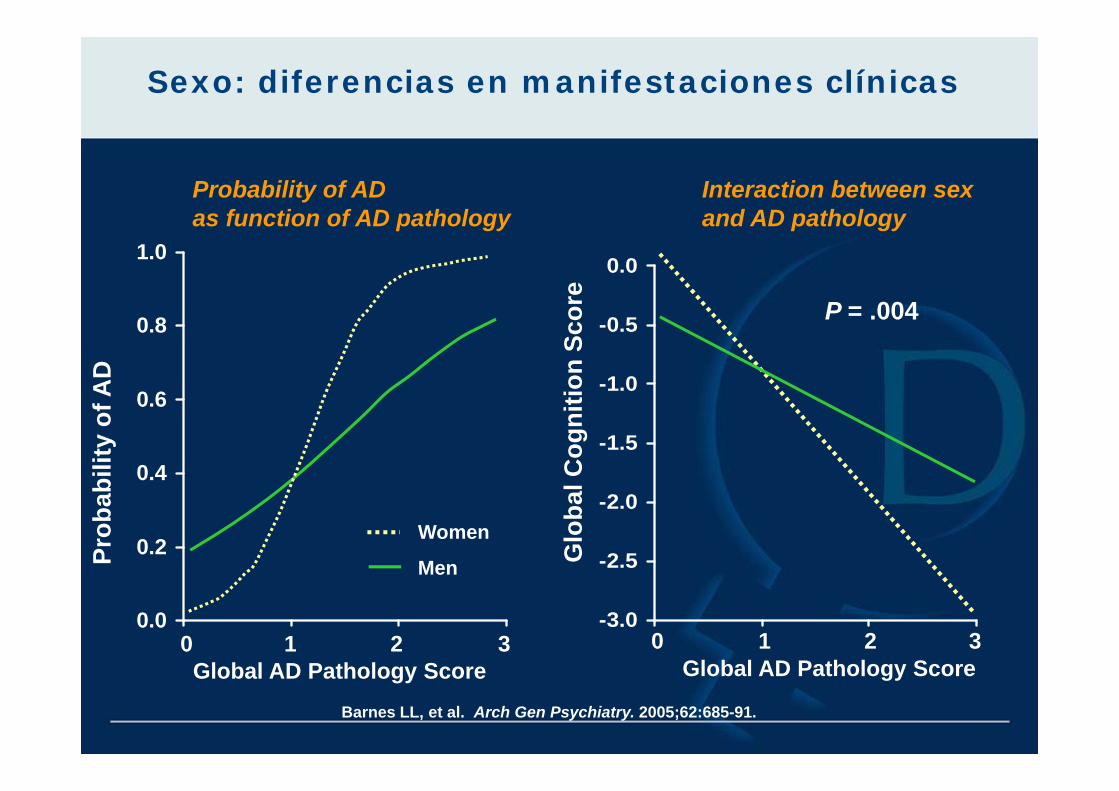
Sexo: diferencias en manifestaciones clínicas
0.0
0.2
0.4
0.6
0.8
1.0
Prob
abili
ty o
f AD
Global AD Pathology Score0 1 32
Men
Women
-3.0
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
Glo
bal C
ogni
tion
Scor
e
0 1 2 3Global AD Pathology Score
Barnes LL, et al. Arch Gen Psychiatry. 2005;62:685-91.
Probability of AD as function of AD pathology
Interaction between sex and AD pathology
P = .004
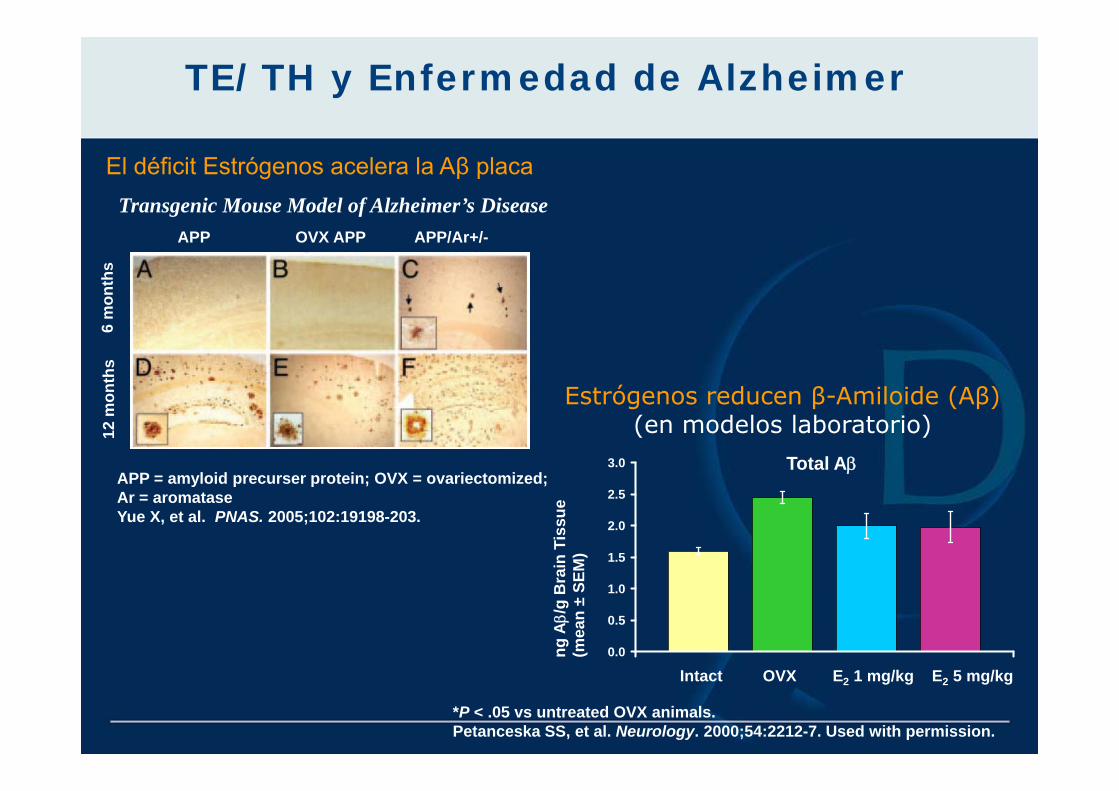
TE/TH y Enfermedad de Alzheimer
0.0
0.5
1.0
1.5
2.0
2.5
3.0 Total Aβ
Estrógenos reducen β-Amiloide (Aβ)(en modelos laboratorio)
ng Aβ/
g B
rain
Tis
sue
(mea
n ±
SEM
)
Intact OVX E2 1 mg/kg E2 5 mg/kg
*P < .05 vs untreated OVX animals.Petanceska SS, et al. Neurology. 2000;54:2212-7. Used with permission.
El déficit Estrógenos acelera la Aβ placa
APP = amyloid precurser protein; OVX = ovariectomized; Ar = aromataseYue X, et al. PNAS. 2005;102:19198-203.
Transgenic Mouse Model of Alzheimer’s DiseaseAPP OVX APP APP/Ar+/-
6 m
onth
s12
mon
ths
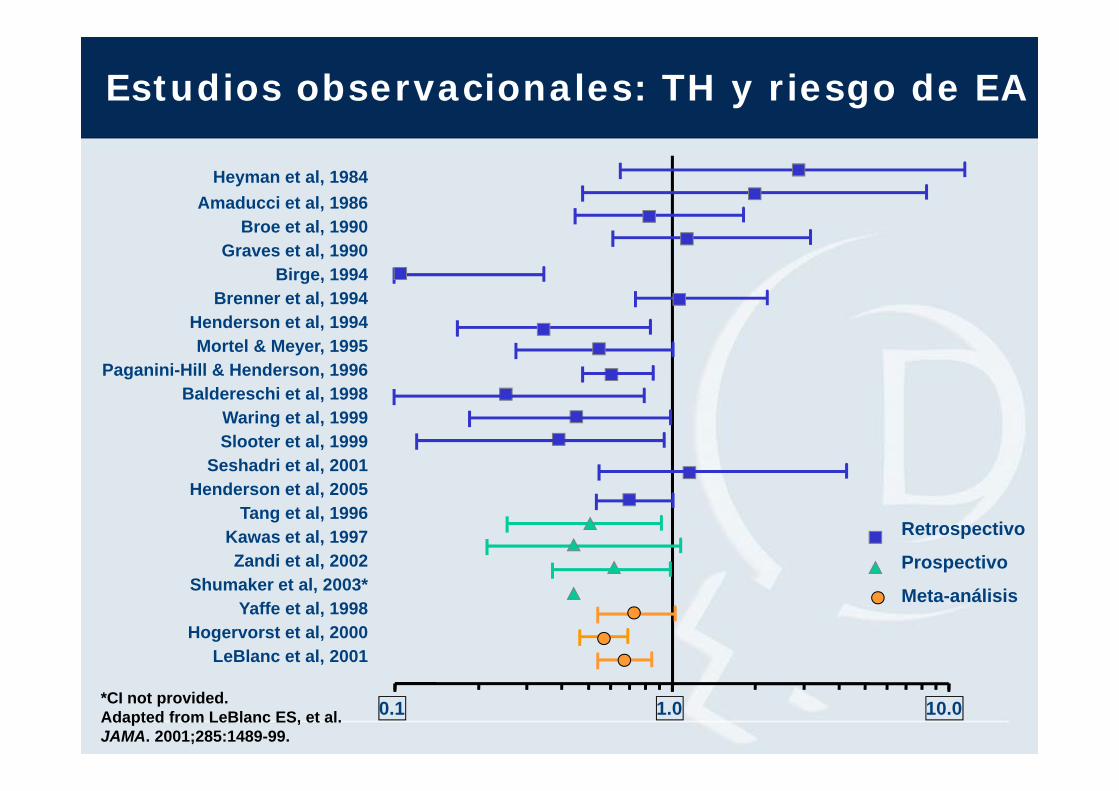
Estudios observacionales: TH y riesgo de EA
0.1 1.0 10.0
Heyman et al, 1984Amaducci et al, 1986
Broe et al, 1990Graves et al, 1990
Birge, 1994Brenner et al, 1994
Henderson et al, 1994Mortel & Meyer, 1995
Paganini-Hill & Henderson, 1996Baldereschi et al, 1998
Waring et al, 1999Slooter et al, 1999
Seshadri et al, 2001Henderson et al, 2005
Tang et al, 1996Kawas et al, 1997Zandi et al, 2002
Shumaker et al, 2003*Yaffe et al, 1998
Hogervorst et al, 2000LeBlanc et al, 2001
Retrospectivo
Prospectivo
Meta-análisis
*CI not provided.Adapted from LeBlanc ES, et al. JAMA. 2001;285:1489-99.
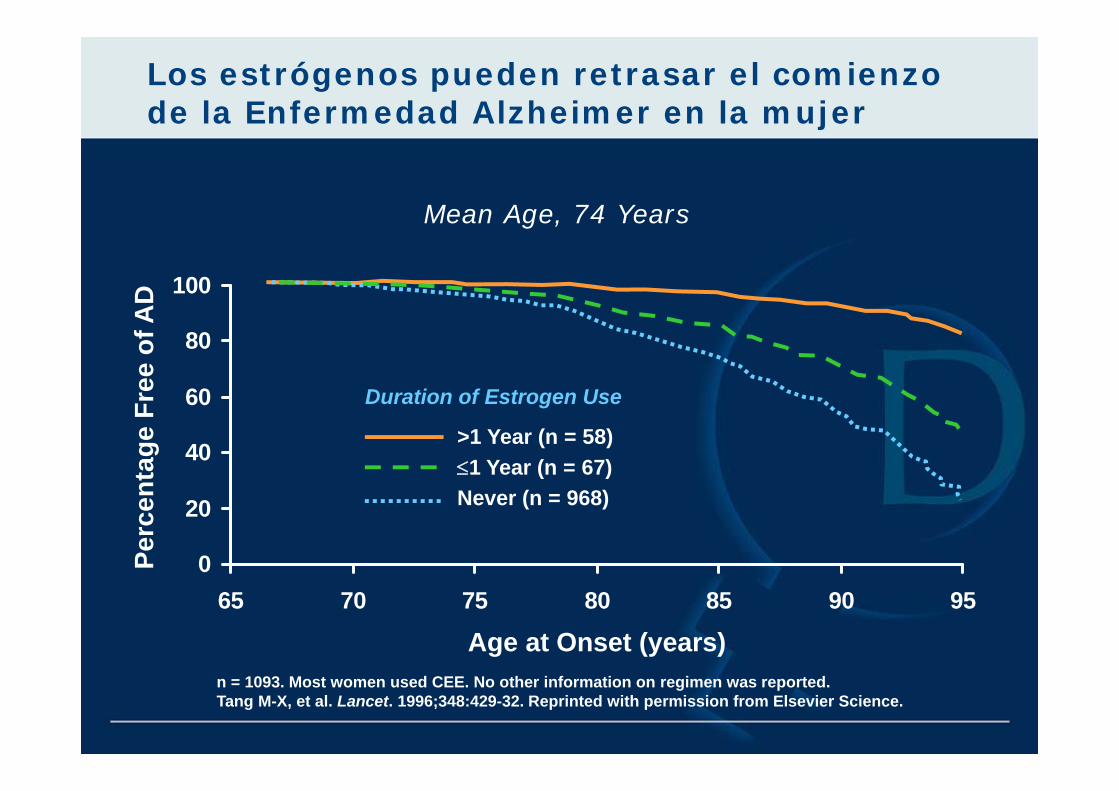
0
20
40
60
80
100
65 70 75 80 85 90 95
Perc
enta
ge F
ree
of A
D
Age at Onset (years)
>1 Year (n = 58)≤1 Year (n = 67)Never (n = 968)
Duration of Estrogen Use
Los estrógenos pueden retrasar el comienzo de la Enfermedad Alzheimer en la mujer
Mean Age, 74 Years
n = 1093. Most women used CEE. No other information on regimen was reported.Tang M-X, et al. Lancet. 1996;348:429-32. Reprinted with permission from Elsevier Science.
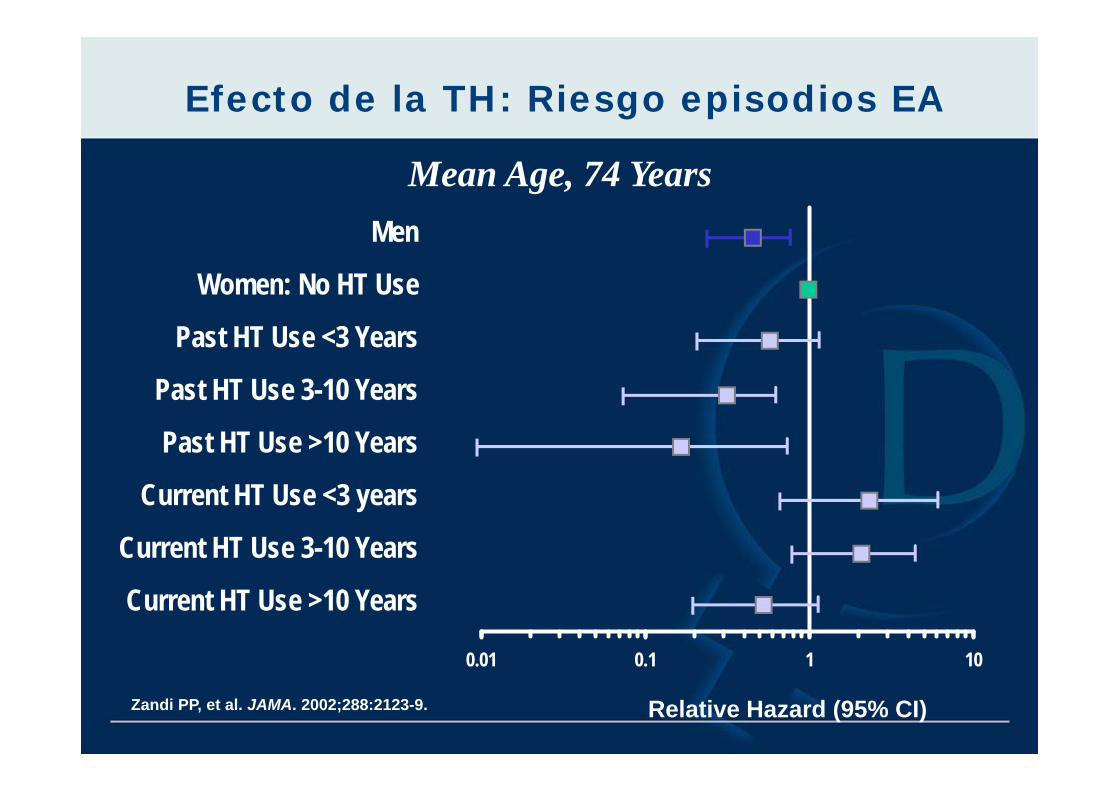
0.01 0.1 1 10
Men
Women: No HT Use
Past HT Use <3 Years
Past HT Use 3-10 Years
Past HT Use >10 Years
Current HT Use <3 years
Current HT Use 3-10 Years
Current HT Use >10 Years
Zandi PP, et al. JAMA. 2002;288:2123-9. Relative Hazard (95% CI)
Mean Age, 74 Years
Efecto de la TH: Riesgo episodios EA
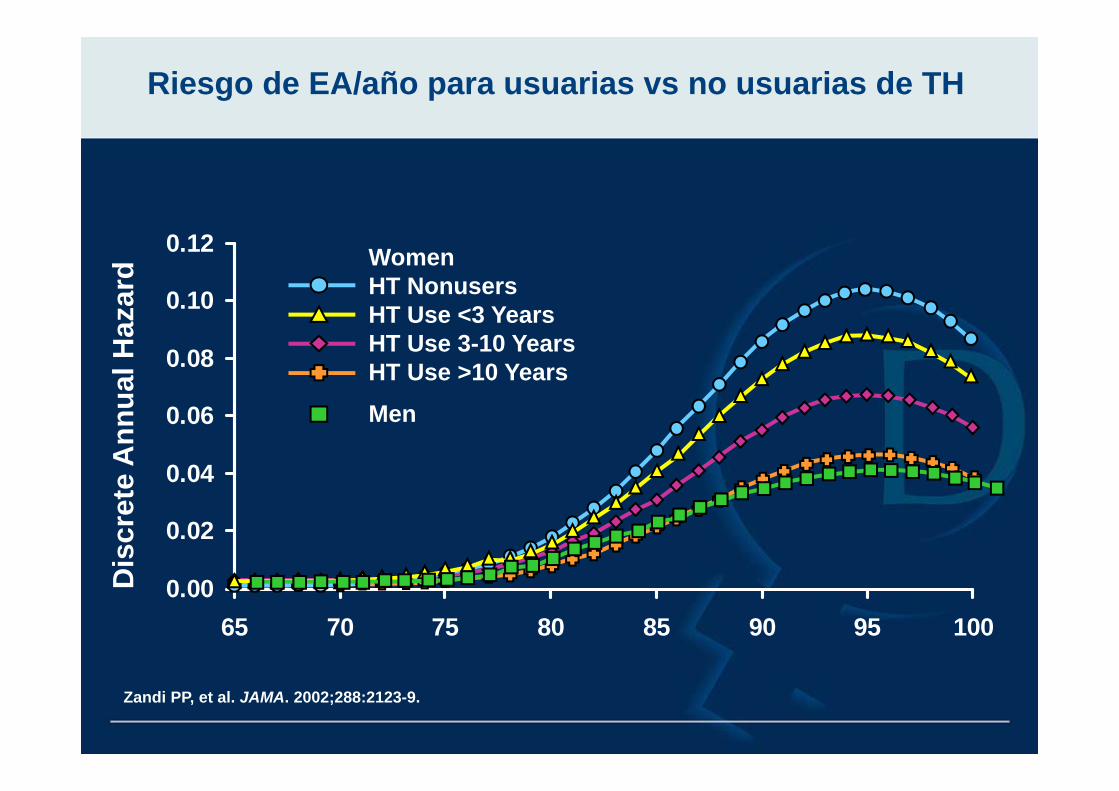
0.00
0.02
0.04
0.06
0.08
0.10
0.12
65 70 75 80 85 90 95 100
WomenHT NonusersHT Use <3 YearsHT Use 3-10 YearsHT Use >10 Years
Men
Riesgo de EA/año para usuarias vs no usuarias de TH
Zandi PP, et al. JAMA. 2002;288:2123-9.
Dis
cret
e A
nnua
l Haz
ard
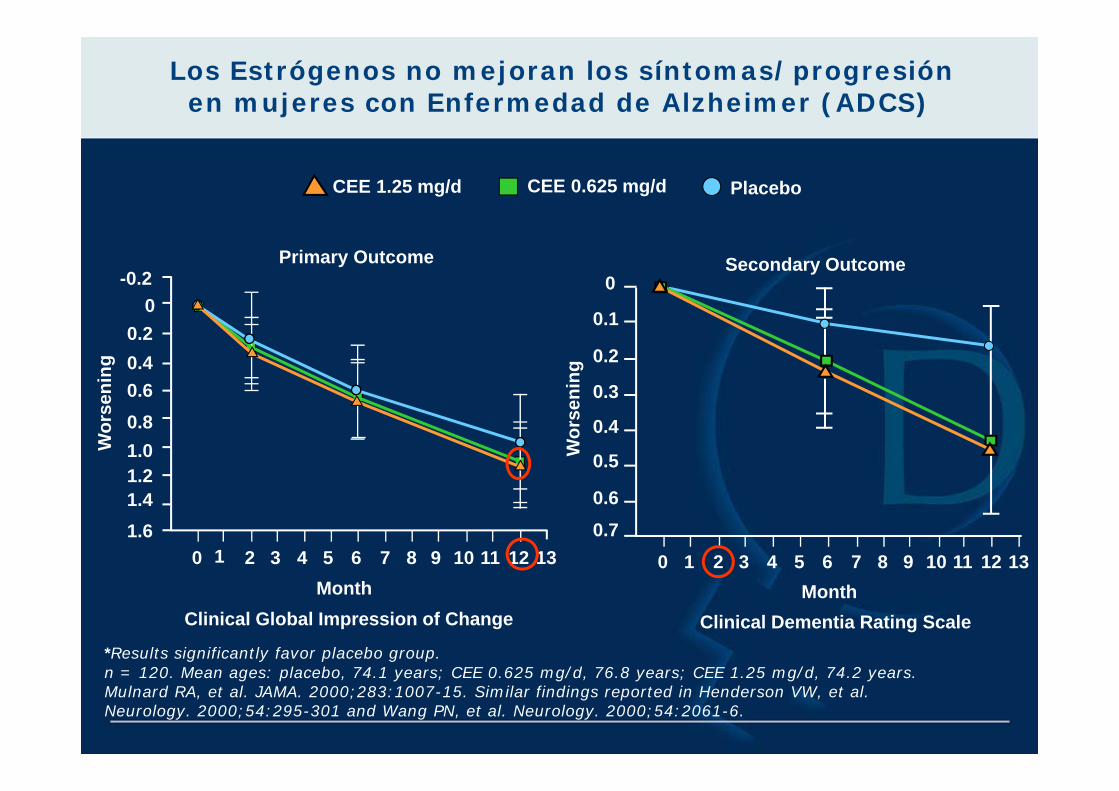
Clinical Global Impression of Change
Primary Outcome
0 1 2 3 4 5 6 7 8 9 10 11 12 13
-0.20
0.20.40.60.81.01.21.41.6
Wor
seni
ng
Month
Clinical Dementia Rating ScaleMonth
Wor
seni
ng
0.70.6
0.5
0.4
0.3
0.2
0.1
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13
Secondary Outcome
Los Estrógenos no mejoran los síntomas/progresión en mujeres con Enfermedad de Alzheimer (ADCS)
PlaceboCEE 0.625 mg/dCEE 1.25 mg/d
*Results significantly favor placebo group.n = 120. Mean ages: placebo, 74.1 years; CEE 0.625 mg/d, 76.8 years; CEE 1.25 mg/d, 74.2 years.Mulnard RA, et al. JAMA. 2000;283:1007-15. Similar findings reported in Henderson VW, et al. Neurology. 2000;54:295-301 and Wang PN, et al. Neurology. 2000;54:2061-6.
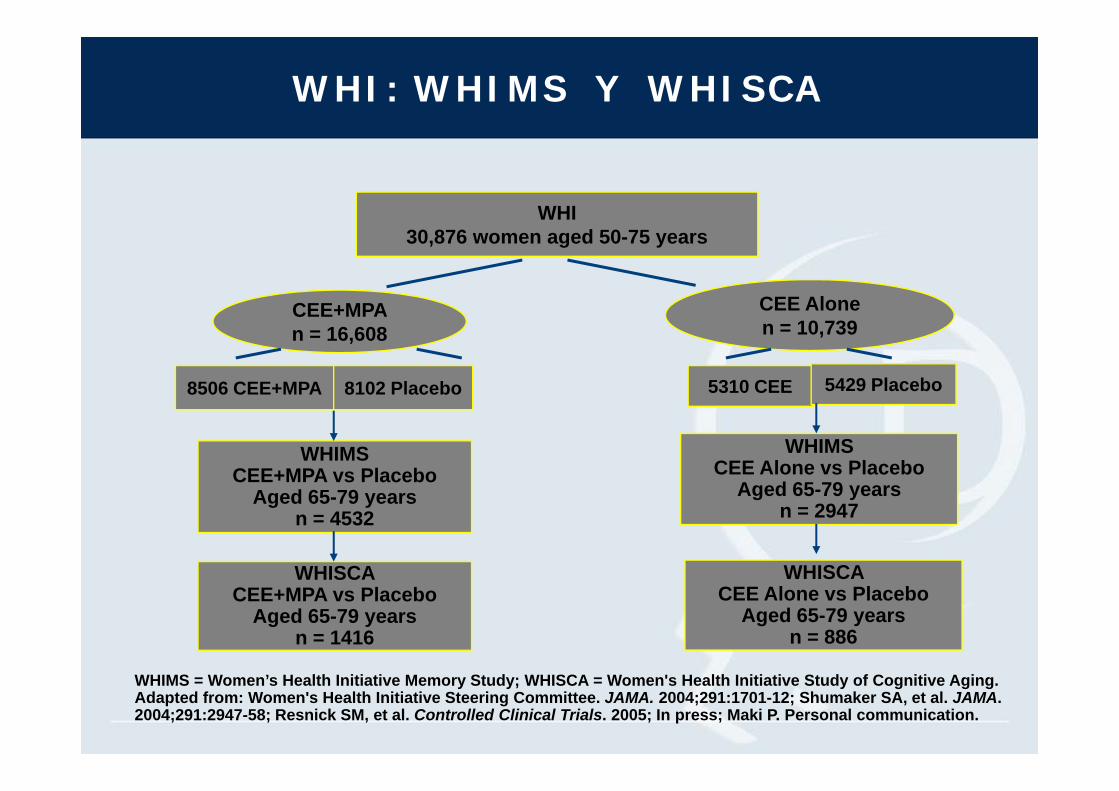
WHI: WHIMS Y WHISCA
CEE+MPA n = 16,608
8506 CEE+MPA 8102 Placebo
WHIMSCEE+MPA vs Placebo
Aged 65-79 years n = 4532
WHISCACEE+MPA vs Placebo
Aged 65-79 yearsn = 1416
CEE Alonen = 10,739
5310 CEE 5429 Placebo
WHIMS CEE Alone vs Placebo
Aged 65-79 yearsn = 2947
WHISCA CEE Alone vs Placebo
Aged 65-79 yearsn = 886
WHI30,876 women aged 50-75 years
WHIMS = Women’s Health Initiative Memory Study; WHISCA = Women's Health Initiative Study of Cognitive Aging.Adapted from: Women's Health Initiative Steering Committee. JAMA. 2004;291:1701-12; Shumaker SA, et al. JAMA. 2004;291:2947-58; Resnick SM, et al. Controlled Clinical Trials. 2005; In press; Maki P. Personal communication.
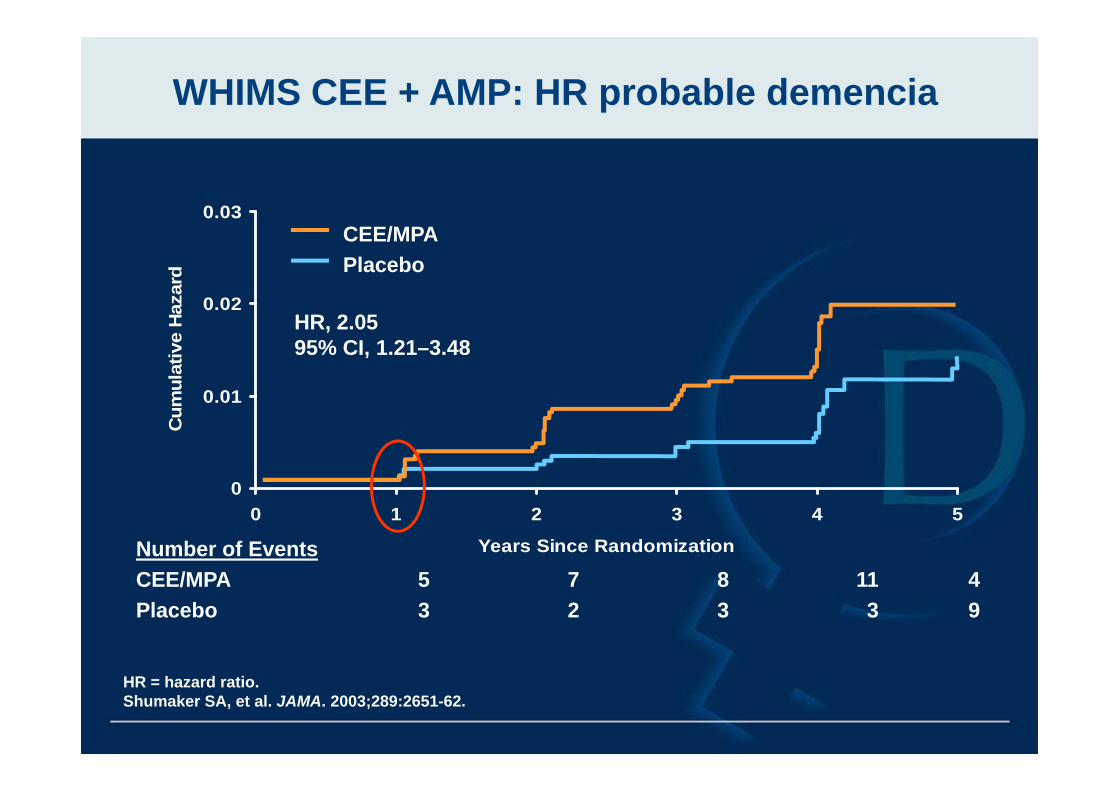
HR = hazard ratio.Shumaker SA, et al. JAMA. 2003;289:2651-62.
WHIMS CEE + AMP: HR probable demencia
0
0.01
0.02
0.03
0 1 2 3 4 5
Years Since Randomization
Cum
ulat
ive
Haz
ard
HR, 2.0595% CI, 1.21–3.48
CEE/MPAPlacebo
Number of EventsCEE/MPA 5 7 8 11 4Placebo 3 2 3 3 9
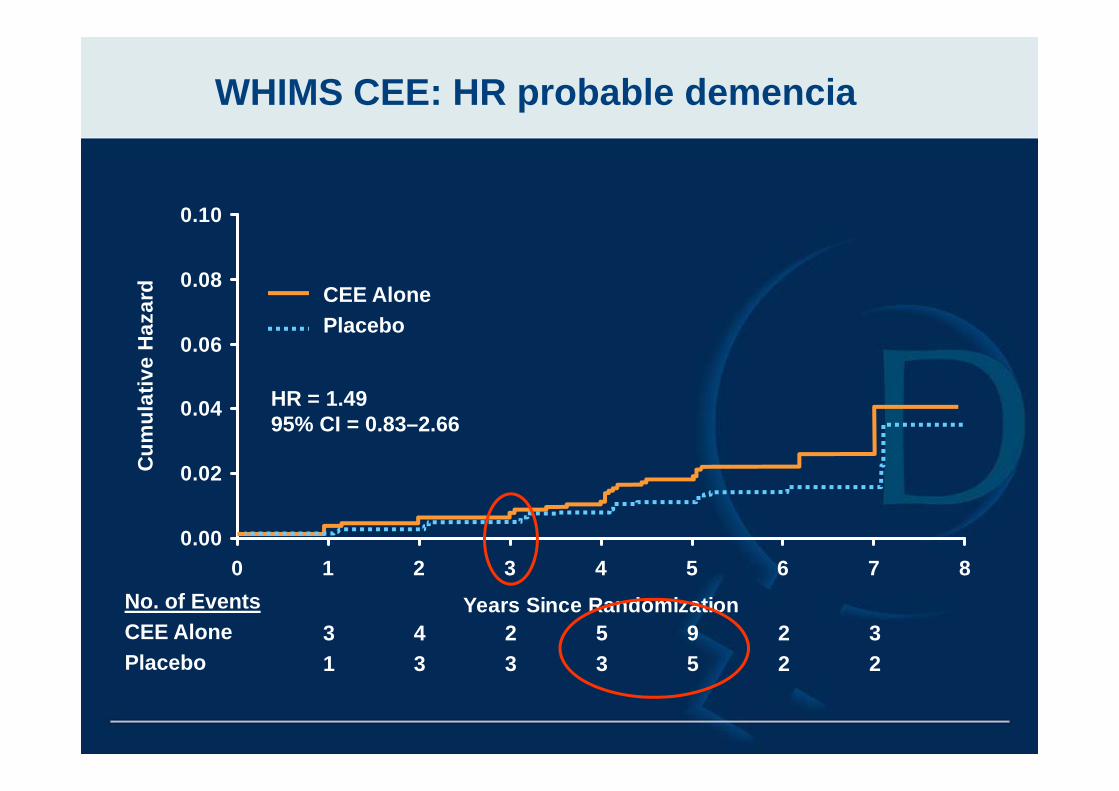
0.00
0.02
0.04
0.06
0.08
0.10
0 1 2 3 4 5 6 7 8
Years Since Randomization
Cum
ulat
ive
Haz
ard
HR = 1.4995% CI = 0.83–2.66
CEE AlonePlacebo
No. of EventsCEE AlonePlacebo
31
43
23
53
95
22
32
WHIMS CEE: HR probable demencia
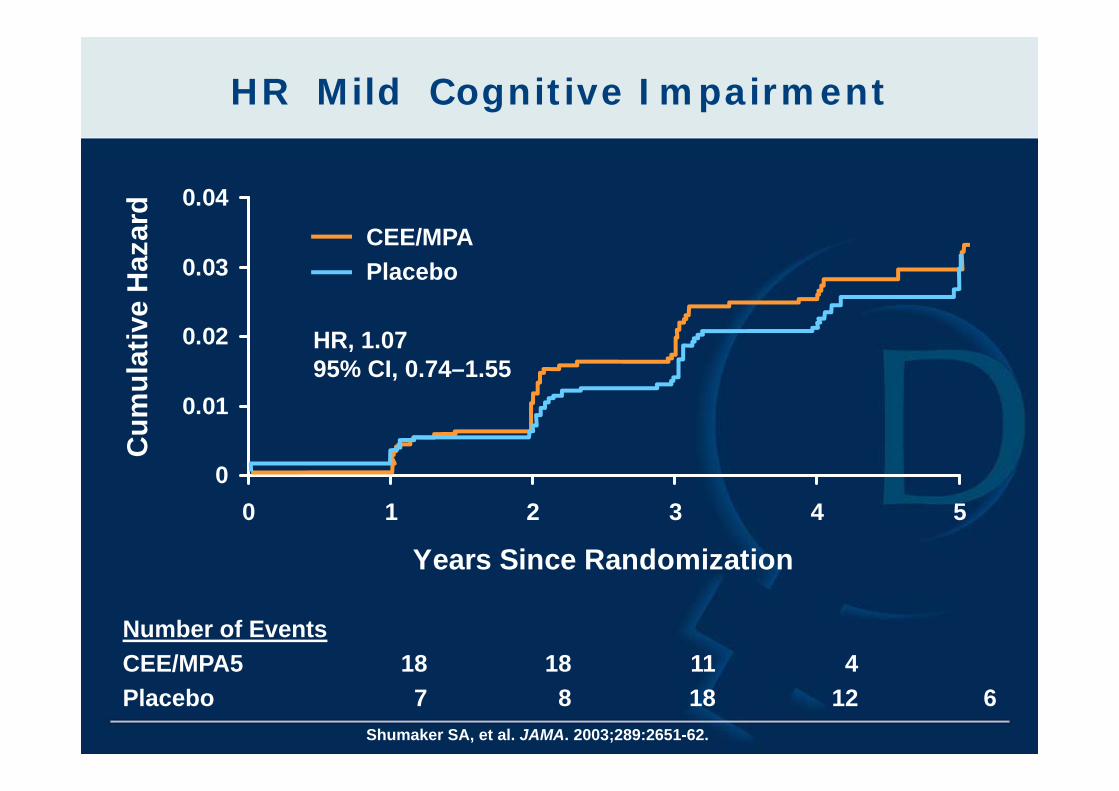
HR Mild Cognitive Impairment
0
0.01
0.02
0.03
0.04
0 1 2 3 4 5
Years Since Randomization
Cum
ulat
ive
Haz
ard
Number of EventsCEE/MPA5 18 18 11 4Placebo 7 8 18 12 6
Shumaker SA, et al. JAMA. 2003;289:2651-62.
HR, 1.0795% CI, 0.74–1.55
CEE/MPAPlacebo
Conclusiones
TH no puede indicarse como prevención para el declive cognitivo y la EA
Estudios observacionales sugieren un papel de los estrógenos retrasando el inicio de la Enfermedad de Alzheimer.
Los estrógenos no enlentecen la progresión o mejoran lossíntomas de la EA
El tiempo de inicio de la TH con respecto a la menopausia ser crítico sobre efecto cognitivo
- La iniciación precoz en el tiempo puede ser beneficiosasobre algunos aspectos cognitivos
- El inicio tardío podría ser neutral o negativo
Estudios randomizados en mujeres >65 años encuentran un incremento del riesgo para todas las demencias con TH