Embed Size (px)
Citation preview

Kgothatso (KD) Meno
BSc (Hons)
Department of Medical Virology
Supervisor: Co-Supervisor:
Dr J Mans Prof MB Taylor
Noroviruses are a major cause of gastroenteritis
worldwide in humans and animals
It affects people of all ages
Children, elderly and immunocompromised
patients are at risk of severe disease
Norovirus is a highly contagious virus, 18 viral
particles can initiate an infection

Transmission by means of faecal-oral route
The symptoms shown by an individual who is infected by NoVs include nausea, vomiting, non-bloody watery diarrhoea and fever
Virus shedding for 3 weeks after infection
Prolonged in immunocompromised individuals
200 000 deaths of children younger than five years old has been estimated in the developing world annually
Norovirus (NoV) - A member of Caliciviridae family
Small (30 to 35 nm), non-enveloped, icosahedral
Linear, positive sense, single-stranded RNA genome
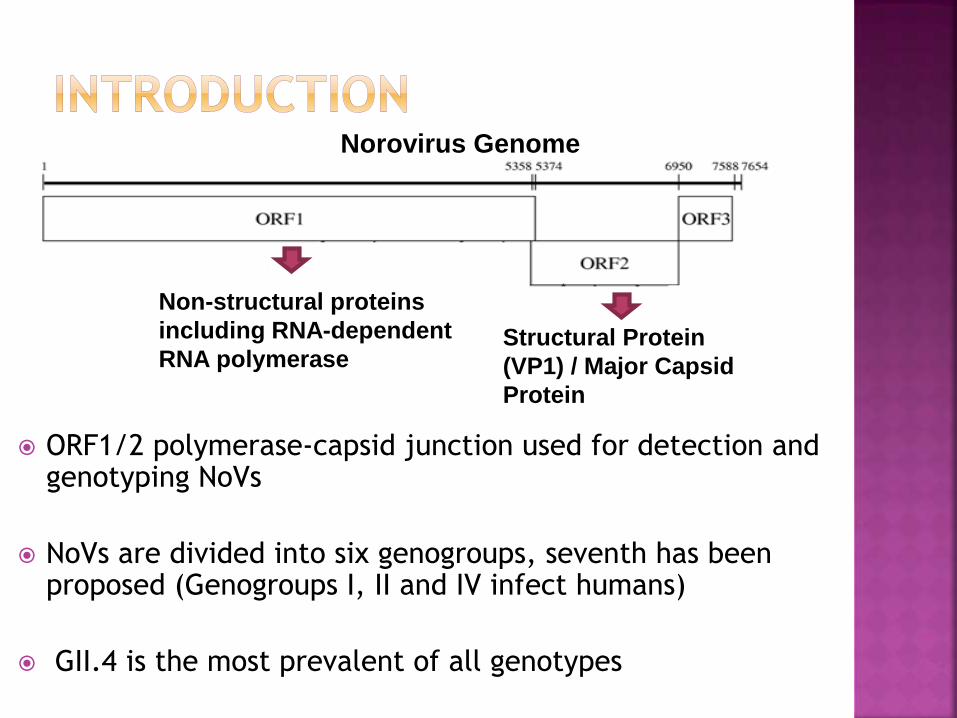
Norovirus Genome
ORF1/2 polymerase-capsid junction used for detection and genotyping NoVs
NoVs are divided into six genogroups, seventh has been proposed (Genogroups I, II and IV infect humans)
GII.4 is the most prevalent of all genotypes
Structural Protein
(VP1) / Major Capsid
Protein
Non-structural proteins
including RNA-dependent
RNA polymerase
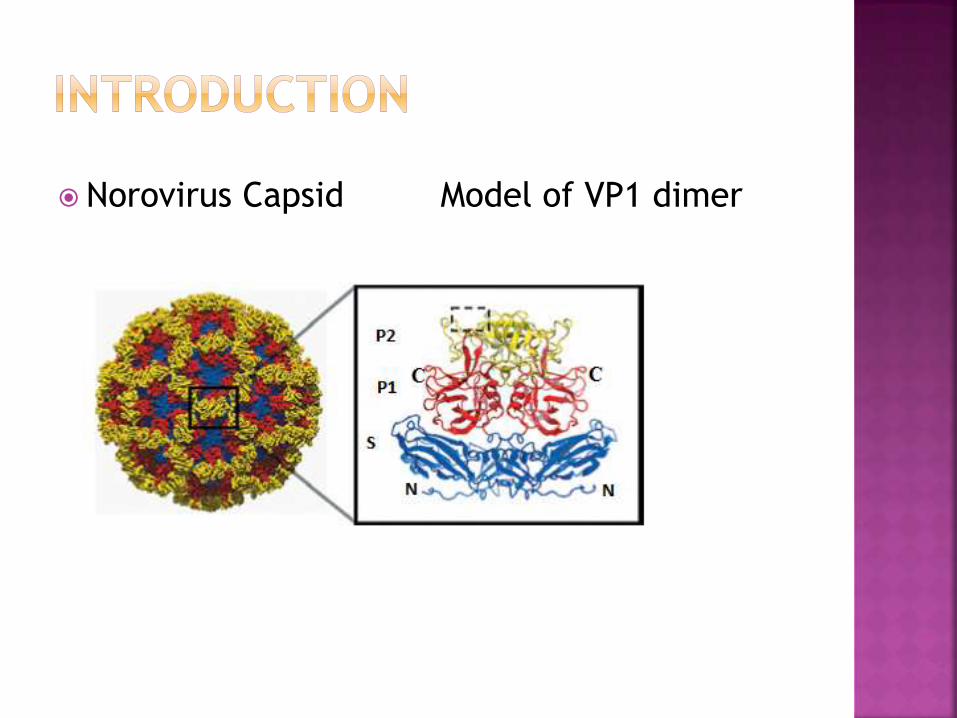
Norovirus Capsid Model of VP1 dimer
To date no commercial NoV vaccine exists
Virus like particles (VLP) vaccines are in clinical
trials (Atmar et al., NEJM, 2011)
Vaccine has been shown to prevent disease but
not infection
Studies are ongoing to evaluate combinations of
genogroups and other aspects of the vaccine

No specific treatment or antiviral therapy for
NoV infection
Treatment: intravenous or oral hydration
At least 40 genotypes within the 6 genogroups

GI
GII
A large number of gastroenteric infections and
outbreaks caused by NoVs are reported but many
suspected cases are not laboratory confirmed
The degree of genetic variability in NoVs makes
it difficult to design sensitive and specific
molecular diagnostic assays
This increases the need and impact of primer
design that is optimised for molecular detection
and typing
Real-time reverse transcriptase-polymerase
chain reaction (real-time RT-PCR) is considered
the “gold standard” for detection of NoVs
Laboratory confirmation of NoV is important in
public health remediation and prevention as well
as enhancing the understanding of NoV
prevalence in the population
Genogroup distribution in South Africa (2009-
2015)
GI (17.7%)
GII (78.5%)
GI+GII (3.8%)
Sizable proportion caused by GI
GI detected but not possible to genotype,
there is diversity primers are not picking up
Since GII is studied more globally, there is
lack of information on GI because research is
skewed to GII
The number of complete genome sequences
of GI Vs. GII
GI is circulating a lot in SA but complete
genomes are missing
In HIV positive children, more severe disease
is associated with GI (Prof NA Page)
GI might be a more relevant genogroup in SA
To optimise NoV GI genotyping primers and to
apply the newly developed genotyping assay to
study NoV GI diversity in clinical specimens and
the environment

To genotype NoV GI detected from sewage samples (April 2015- March 2016) using standard GI primers targeting the polymerase and capsid regions
To construct and analyse multiple alignments of available GI sequences from GenBank
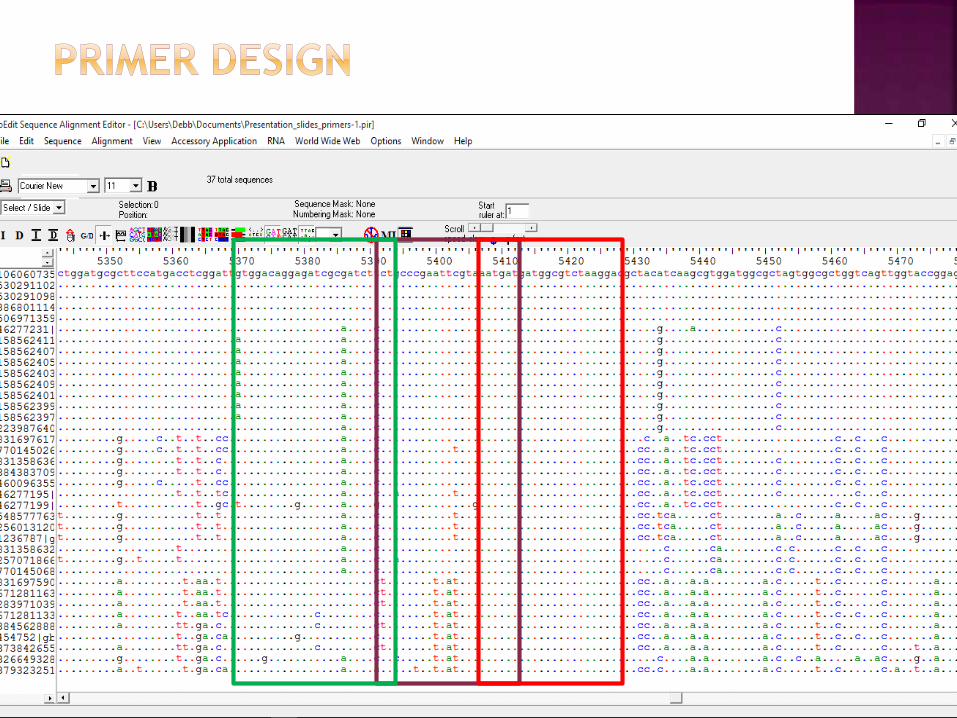
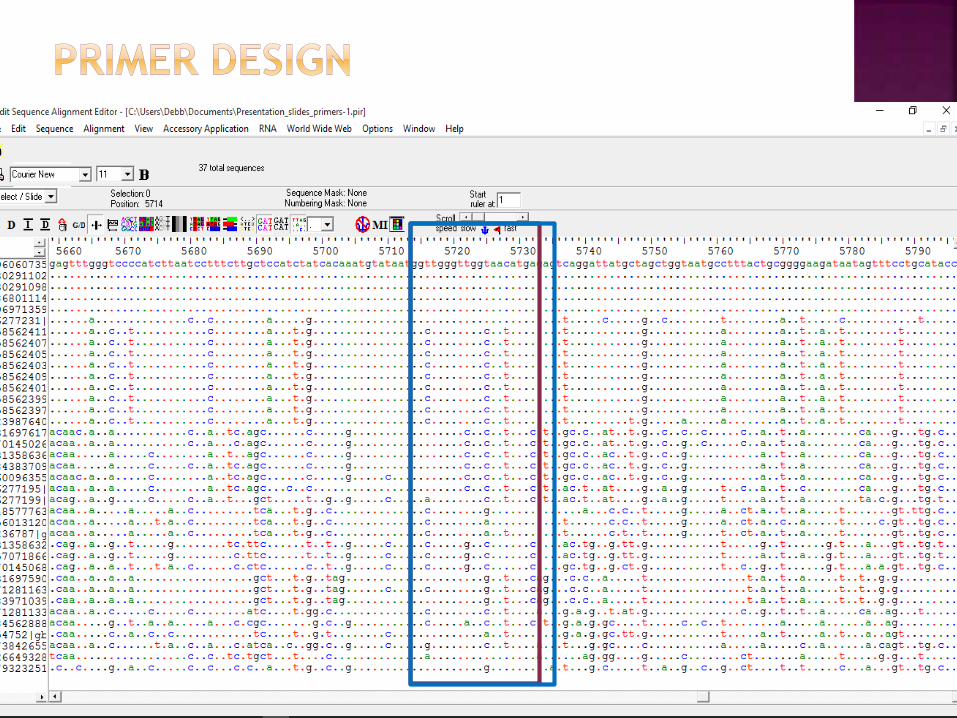
To design primers to optimise conventional RT-PCR
To apply optimised methods to genotype NoV GI strains from the Rotavirus Surveillance Sentinel Programme that could not be typed previously (2011- 2013) and new strains from 2015
To amplify complete capsid gene from selected GI strains for characterisation and phylogenetic analysis
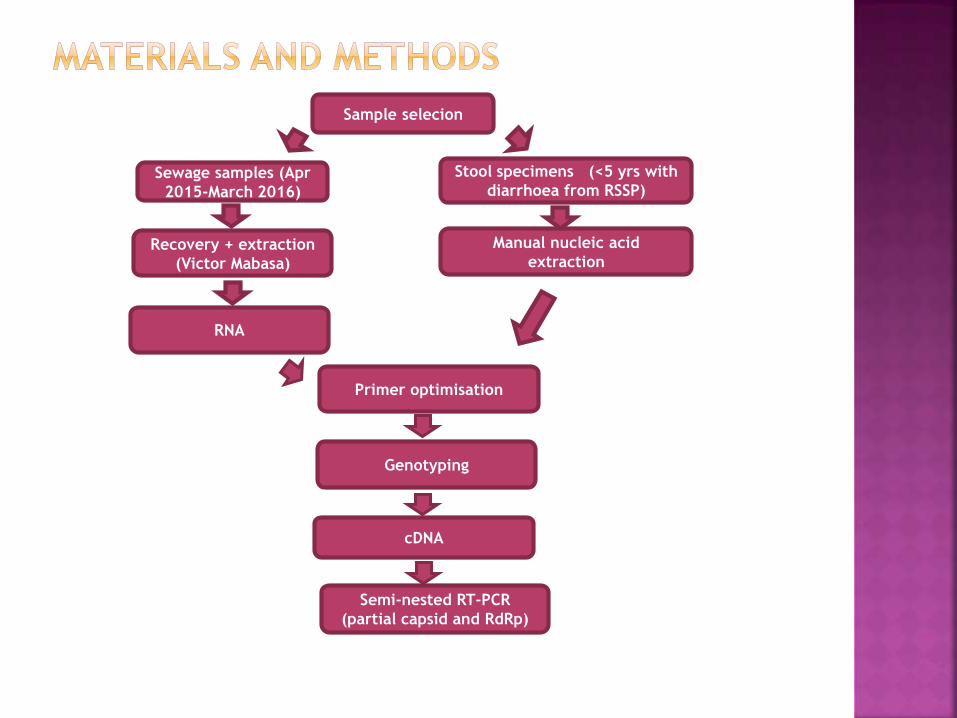
Sample selecion
Sewage samples (Apr
2015-March 2016)
Stool specimens (<5 yrs with
diarrhoea from RSSP)
Recovery + extraction
(Victor Mabasa)
Manual nucleic acid
extraction
RNA
Primer optimisation
Genotyping
cDNA
Semi-nested RT-PCR
(partial capsid and RdRp)
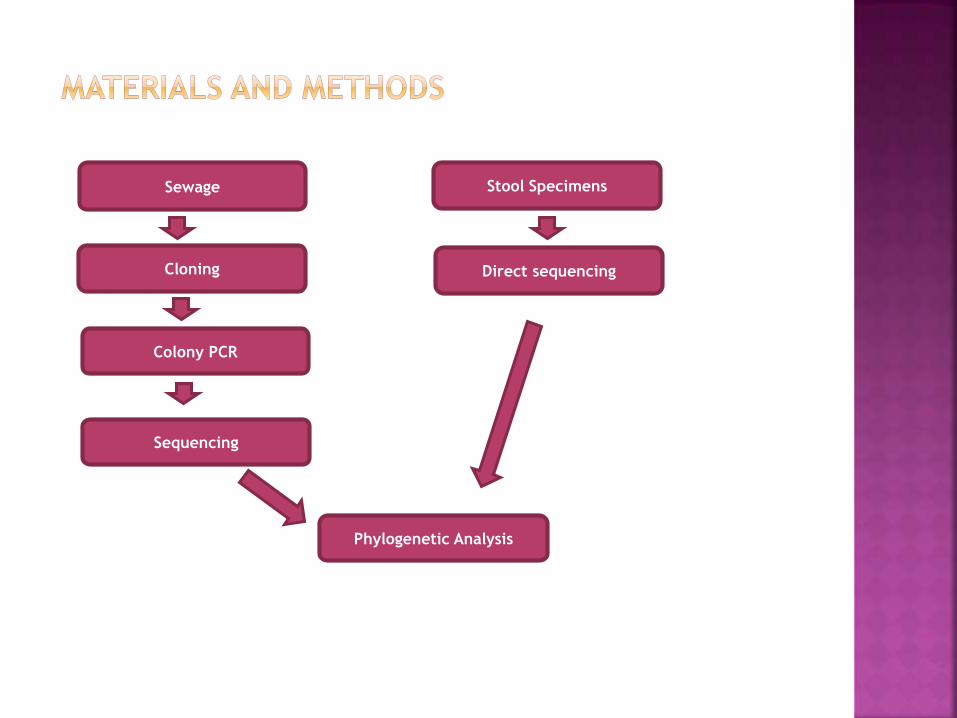
Sewage
Cloning
Colony PCR
Stool Specimens
Direct sequencing
Sequencing
Phylogenetic Analysis
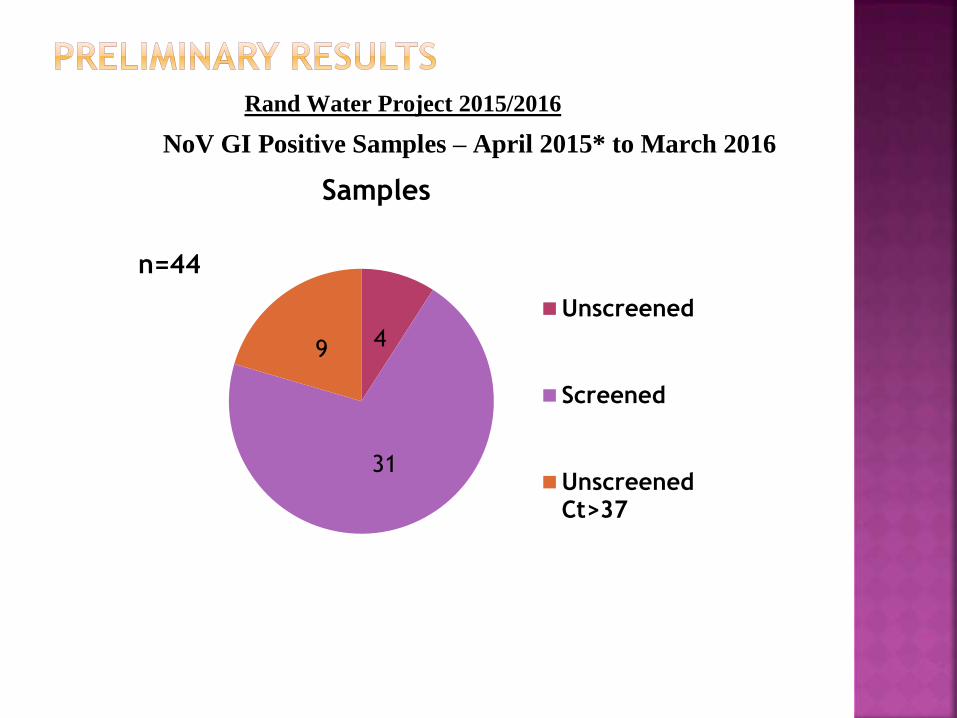
Rand Water Project 2015/2016
NoV GI Positive Samples – April 2015* to March 2016
4
31
9
Samples
Unscreened
Screened
UnscreenedCt>37
n=44

0
1
2
3
4
5
6
7
8
GI p
osi
tive
s
Months
Representation of number of norovirus GI positive samples detected by real-time RT-qPCR and typed by Semi-nested
conventional PCR
Real-time detection
nested PCR typing
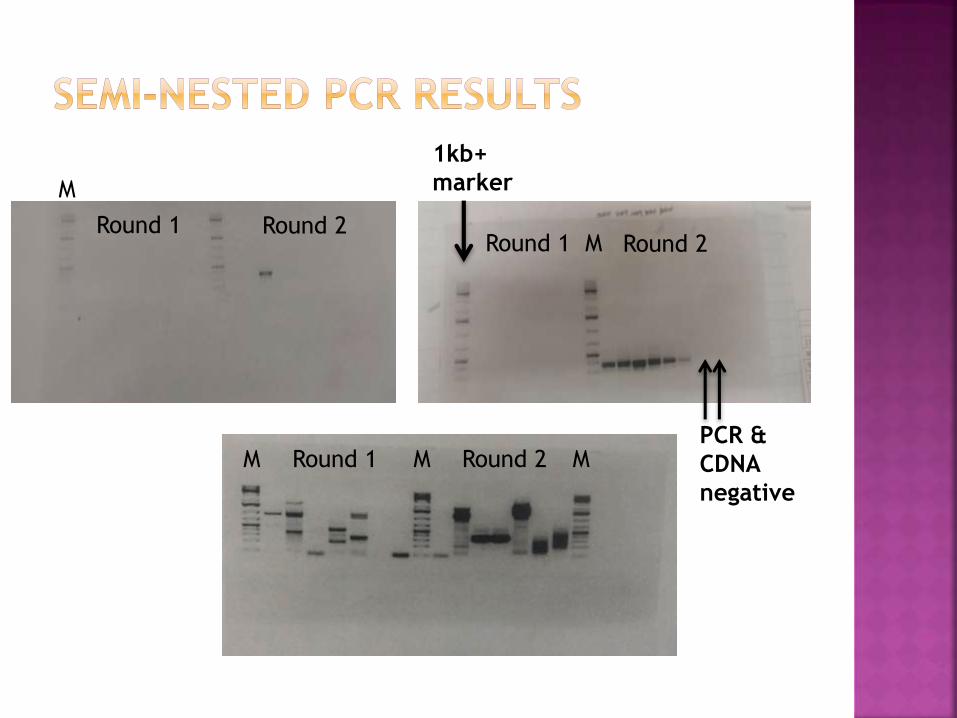
Round 1 Round 2
1kb+
marker
PCR &
CDNA
negative
Round 1 Round 2
Round 2Round 1
M
M
M M M

1kb+
marker
M
M
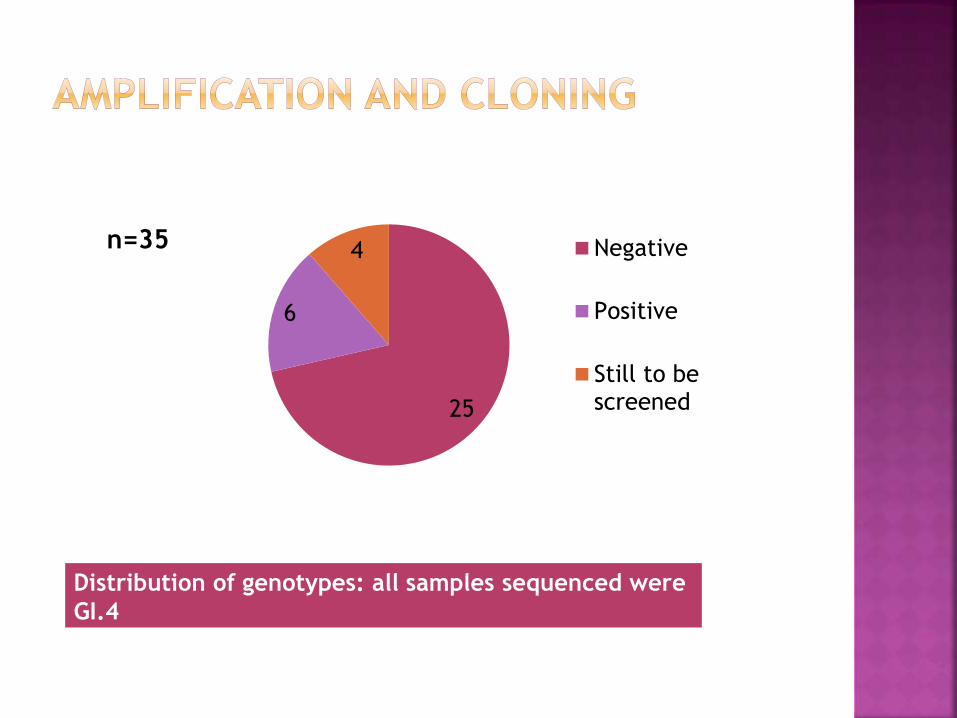
Distribution of genotypes: all samples sequenced were
GI.4
25
6
4 Negative
Positive
Still to bescreened
n=35

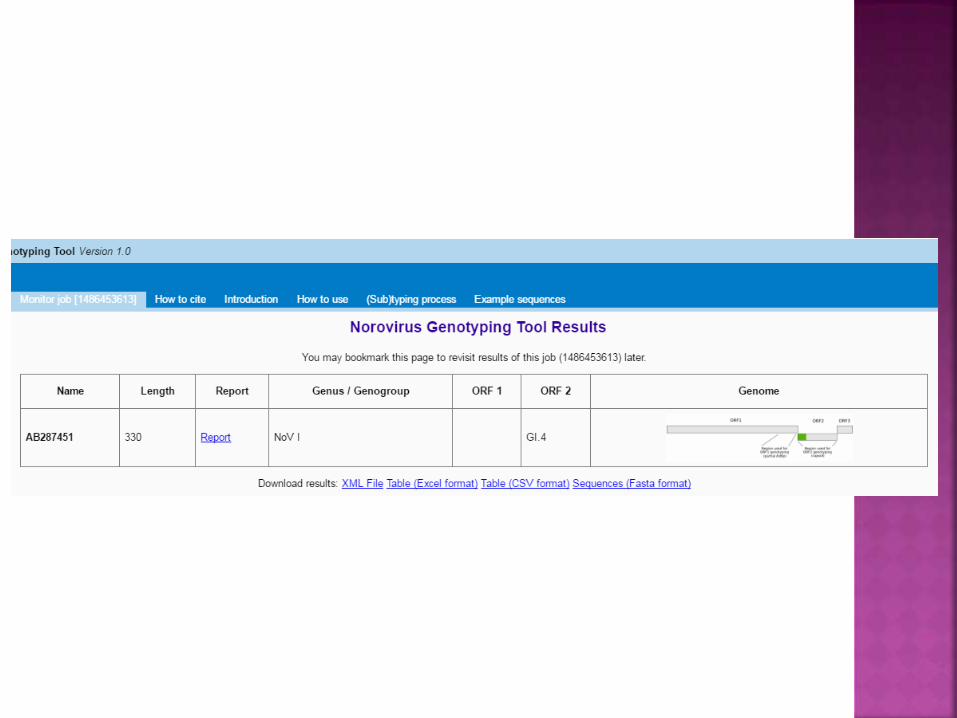
Collected all the complete genomes (33)
Typed them using the norovirus genotyping
tool and aligned them using MAFFT software
in FASTA format
Distribution of genotypes GI.1 22
GI.2 3
GI.3 2
G1.4 1
GI.6 3
GI.8 2
GI Forward primer 1
TGG ACA GGA GAT CGC RAT CT
Tm:66°C
GI Forward primer 2
ATG ATG ATG GCG TCT AAG GA
Tm:61°C
GI Reverse primer
CCI ACC CAI CCA TTR TAC AT
Tm:61°C

Problems encountered:
Encountered problems with the Hot Start
DNA polymerase enzyme, a lot of sewage
samples were screened but there was no
amplification
Although the enzyme worked on clinical
specimens
The standard primer binding region not
completely conserved
The denaturation time (30 sec) too short
Alternative ways attempted:
A different enzyme (Emerald) was used,
there was amplification
High number of none specific amplification
Emerald PCR products: Gel clean up
Use my designed primers on the stool specimens
Go back and screen some of the sewage samples with the new optimised primers and the Hot start DNA polymerase
Go back and screen the previously negative sewage samples with Emerald enzyme
Optimise the Emerald PCR
Design genotype specific primer for capsid 3’ end
Amplify and sequence the complete capsid gene of selected strains


Part of a larger (ethically approved) project (Rotavirus
Sentinel Surveillance Programme), additional ethical
approval has been granted (127/2016)
Total: R71 850
Prof NA Page together with the Rota network
Randwater
NRF
Any Questions?





























![Page Walk on the... · Day 4 Sky Beds* Khwai Private Reserve FI 1 Night ... [BBK] Day 7 Meno A Kwena Maun Airport - Meno A Kwena Day 9 Meno A Kwena Meno A Kwena - Maun Airport . Date](https://img.pdfslide.us/doc/110x75/60559cb33d4d7b2908737830/walk-on-the-day-4-sky-beds-khwai-private-reserve-fi-1-night-bbk-day.jpg)