Alcoholic Liver Cirrhosis
I. PERSONAL DATA
Name: Baby D.G.
Address: Umilag, Lamut, Ifugao
Age: 1 yr 9 mos
Birthdate: December 31, 2004
Birthplace: Umilag, Lamut, Ifugao
Religion: Evangelical
Date and Time of Diagnosis: September 25,2006; 4 PMAdmitting
Diagnosis: S/P Untreated Meningitis with Hydrocephalus
, R/O TB Meningitis, 4th degree Malnutrition
Attending Physician: Dr. Benzon
II. HISTORY OF PRESENT ILLNESS
Before the delivery, DGs mother did not have any prenatal
check-up, she is confident enough since her 4 kids were delivered
normal. The mother decided to deliver her baby via (NSD) normal
spontaneous delivery.
Our patient was born on a G5P4 mother in their home and was
assisted by her husband and a neighbor. The baby was normal upon
delivery. The baby was a girl and the cord was primitively cut with
bamboo sticks by her husband with no check-up was done.
It has been a year since birth and DG had not received any
immunizations , which were supposedly given right after delivery,
when in fact their house was just near the Brgy. Health Center. No
vaccination was given due to negligence.
Three months after birth, the baby suffered cough and fever for
five days. With her mothers instinct of experience with her 4
children, she bought over-the-counter drugs (Ambroxol and
Paracetamol) to treat the illness. For almost a year, baby didnt
experience any health problem.
It was March of this year that baby suffered from fever, cough,
vomiting and loose, watery- mucoid stools occurring about 4-5
times/day, for three days. The mother was so worried that she went
to Dr. Balisan for consultation. Medication was given to treat the
diarrhea last March 10, 2006. Above symptoms persisted with
fever.
They then went to Panupdupan Hospital on March 16, 2006 and the
baby was diagnosed with blood infection as claimed by the mother.
She was given Ampicillin, Chloramphenicol, and Cefuroxime during
the entire hospitalization, which lasted for two weeks. The fever
and cough became worst. No improvements were noted hence they opted
to transfer at Ifugao Provincial Hospital and DG was diagnosed with
Meningitis on March 29, 2006. Upon admission patient was febrile
and drowsy. Lumbar tap was done for CSF analysis. She was started
with Ceftriaxone and Mannitol. During babys stay at the hospital,
an NGT was inserted for oral feeding since she had difficulty
sucking her moms breast. Baby also had seizure episodes and muscle
spasms. Diazepam was ordered and administered. To further support
the diagnosis, CSF analysis and total cell count was done. Result
was increased WBC, decreased RBC, decreased sugar and positive
CHON. Head CT scan was also requested but was not done due to
financial problems.
After a day or two, mother noticed that babys lumbar area was
swollen. Mother decided that the baby should be taken home to
consult a manghihilot to treat the swollen back. A HAMA form was
signed by mother to end their 1 month stay in hopital. They went
home with NGT still inserted to baby DG. Milk was introduced via
NGT to sustain the child.
The NGT was only removed by the mother last July 2006 when
mother decided to introduce soft food and baby DG was able to
tolerate it. Baby was fed lugaw as her staple food for three
months.
First week of September, baby again suffered from dysphagia,
cough, vomiting and diarrhea for three weeks. A week after, no
intake of food and not even fluids was noted by her mother. She
went to Dra. Quilang and requested for NGT insertion. The following
day, mother sought consultation at Dra. Padres clinic and pleaded
her to do everything to improve babys status. Dra. Padre diagnosed
the baby with S/P Untreated Meningitis with Hydrocephalus, r/o TB
meningitis, Cerebral Palsy, 4th degree malnutrition and referred
baby DG to Veterans Regional Hospital.
III. ENVIRONMENTAL DATA
Their house is a semi-concrete 20x20m excluding the kitchen.
Their source of water is from a spring and is directly delivered
through rubber tubings. They usually drink directly from it and
sometimes boil the water for the babys formula. They have an open
type toilet. They have a vegetable garden and three hogs to support
the family expenses. It was only during the hospitalization that
almost all resources were depleted. It takes one hour to travel to
Lagawe Poblacion, since the family needed to cross two rivers
before they could reach Lagawe.
IV. SOCIO-ECONOMIC DATA
Due to meager resources the family seldom eat balanced and
nutritious foods. The familys usual diet is usually composed of
instant noodles, sardines, vegetable tops, rice and, sometimes,
coffee serves as their viand. The eldest, age 11, and the second
child, age 9 are both in the fourth grade. The third child is in
the first grade and the fourth child is supposedly in day care but
wasnt well-managed to go to school due to the hospitalization of
the youngest sibling. To augment the financial aspect of the family
the father and the mother works at the relatives rice field.
V. PRE-CLINICAL GROWTH AND DEVELOPMENTALS STATUS:VI. BREIF
DESCRIPTION OF THE ILLNESSA. Cerebral Palsy
Definition
Cerebral palsy (CP) is a group of motor problems and physical
disorders related to a brain injury. CP causes uncontrolled reflex
movements and muscle tightness (spasticity) that may affect a part,
a side, or the entire body, with varying severity. Several
conditions, such as mental retardation, seizures, or vision and
hearing problems, are often also associated with cerebral
palsy.
Types:
1. Athetoid/Dyskinetic Cerebral PalsyThis type of cerebral palsy
is usually characterized by slow uncontrollable movements which
usually affect the muscles in legs, hands, feet, and in some cases
face or throat, which can result in drooling or grimacing. Such
symptoms are most visible during times of emotional stress and are
virtually invisible during sleep. In addition, this type of
cerebral palsy can cause speech disorders. Athetoid or Dyskinetic
cerebral palsy falls in to roughly 10-20 per cent of all cases.
2. Spastic Cerebral Palsy Spastic cerebral palsy is the most
common type of cerebral palsy, accounting for nearl 80 percent of
all cerebral palsy cases. Children with this type of cerebral palsy
have one or more tight muscle groups which limit movement. Children
with spastic cerebral palsy have stiff and jerky movements. They
often have a hard time moving from one position to another. They
may also have a hard time holding and letting go of objects.3.
Ataxic Cerebral PalsyThis form is cerebral palsy usually results in
very shaky or unsteady movements as well as weak sense of balance,
poor coordination, and depth perception in children. Children
affected with ataxic cerebral palsy usually take longer to complete
certain tasks as a result of such shaky movements and poor
coordination. This type of condition occurs in about 5-10 percent
of all cases.
4. Mixed Cerebral PalsyIn some cases, more than one of the above
symptoms are present and most often include but are not limited to
the combination of athetoid movements and spasticity.Causes
Cerebral palsy is caused by a brain injury or problem that
occurs during fetal growth, birth, or within the first 2 to 3 years
of life. CP can result from: Complications related to prematurity
Being deprived of blood, oxygen, or other nutrients before or
during birth. A serious head injury. Developing a serious infection
that can affect the brain, such as meningitis. Some conditions that
are passed from parent to child (genetic conditions) that are
linked to abnormal brain development.
In many cases, the exact cause of the injury is not known.
Symptoms problems with body movement and posture, although the
degree of physical disability varies
slight limp or an uncoordinated walk
have little or no control over their arms and legs or other
parts of their body, such as their mouths and tongues
seizures or mental retardation.
Babies born with severe CP often have an irregular posture;
their bodies may be either very floppy or very stiff. Birth
defects, such as an irregularly shaped spine, small jawbone, or
small head, sometimes occur along with cerebral palsy.
Diagnosis
Cerebral palsy (CP) usually takes several months to several
years to diagnose. However, most children with CP are diagnosed by
about 18 months of age. If a child is born with a severe form of
CP, a health professional may be able to diagnose the condition
within the first few weeks of life. However, parents and caregivers
usually are the first to notice that a baby has developmental
delays that may be early signs of CP.]
Usually a health professional diagnoses cerebral palsy based on
a baby's medical history (including parents' observations of
developmental delays), physical examination, and results of
screening tests.
Additional tests, such as developmental questionnaires, computed
tomography (CT) scan or magnetic resonance image (MRI) of the head,
or an ultrasound of the brain may be done. These tests can help a
health professional determine the cause of CP.
Treatment
There is no cure for cerebral palsy. Treatment is often needed
throughout life to help manage symptoms, prevent complications, and
maximize abilities. Although CP does not get worse over time, new
challenges can develop as the child grows and develops.
Medications, surgery, special equipment and devices, physical
therapy, and individualized training may all be used.
B. Malnutrition (Marasmus)
Marasmus is one component of protein-energy malnutrition (PEM).
It a severe form of malnutrition caused by inadequate intake of
protein and calories, and it usually occurs in the first year of
life, resulting in wasting and growth retardation.The major factors
that cause a deficit of caloric and protein intake
1. the transition from breastfeeding to nutrition-poor foods in
infancy2. acute infections of the gastrointestinal tract, 3. and
chronic infections such as HIV or tuberculosis..
The physiologic response to a negative energy balance is to
reduce energy consumption. Children who suffer from marasmus
display decreased activity, lethargy, behavioral changes, slowed
growth, and weight loss. The subsequent effects on the body are
wasting and a loss of subcutaneous fat and muscle, resulting in
growth retardation. The majority of children who suffer from
marasmus never return to age-appropriate growth standards.
The cornerstone of therapy for marasmus is to supply the body
with the necessary nutritional requirements. The nutritional needs
of children in the rehabilitation stage require at least 150
kilocalories per kilogram per day. Dehydration must be addressed
with oral rehydration therapy, while micronutrient deficiencies,
such as vitamin A deficiency, require supplementation.
Immunizations must be reviewed and given as necessary to reduce the
burden of infectious diseases on children's bodies. Finally, family
education must be ongoing to improve behavioral responses to such
conditions. Some ready-to-use formulas and foods have also been
developed. Such a broad approach must be taken to help reduce the
morbidity and mortality caused by this condition.C.
HYDROCEPHALUS
Hydrocephalus is the most common problem faced by the pediatric
neurosurgeon and may be due to a variety of conditions (congenital,
posthemorrhagic in premature infants, postmeningitic, obstruction
by tumors or cysts, etc.). Hydrocephalus may cause injury to the
brain by raising the intracranial pressure (ICP).
As cerebral blood perfusion is determined by the difference
between mean arterial pressure and ICP, an elevated ICP may result
in widespread ischemia. Additional injury occurs when the enlarged
ventricles associated with hydrocephalus disrupt the axons that
course around them. Finally, hydrocephalus also causes disruption
of the ependymal surface of the ventricles with periventricular
white matter showing axonal degeneration and gliosis.
The clinical consequences of brain injury resulting from
untreated hydrocephalus include widespread neurologic and cognitive
dysfunction, blindness and a massively enlarged head if the process
begins in an infant with open sutures.
The most common causes of acquired hydrocephalus are hemorrhage,
infection (meningitis) and tumors. Hemorrhage and meningitis have
similar mechanisms for causing obstruction: particular matter
occludes the aqueduct or arachnoid granulations or the inflammatory
response causes adhesions in the CSF pathways (usually at the base
of the brain) that obstruct flow. Tumors cause hydrocephalus by
growing into the CSF pathways or by causing brain shifts that
impede CSF flow.Clinical FeaturesInfants
1. Increasing head circumference.
2. Irritability, lethargy, poor feeding, and vomiting.
3. Bulging anterior fontanelle.
4. Widened cranial sutures.
5. McEwen's cracked pot sign with cranial percussion.
6. Scalp vein dilation (increased collateral venous
drainage).
7. Sunset sign (forced downward deviation of the eyes, a
neurologic sign almost unique with hydrocephalus).
8. Epidsodic bradycardia and apnea.
Medical
Four principal modes of medical therapy are used.
1. Remove CSF.
2. Decrease CSF production.
3. Decrease cerebral water content.
4. Increase CSF absorption.D. MeningitisV. Anatomy and
PhysiologyRespiratory SystemHuman Anatomy
Respiratory System, in anatomy and physiology are organs that
deliver oxygen to the circulatory system for transport to all body
cells. Oxygen is essential for cells, which use this vital
substance to liberate the energy needed for cellular activities. In
addition to supplying oxygen, the respiratory system aids in
removing of carbon dioxide, preventing the lethal buildup of this
waste product in body tissues. Day-in and day-out, without the
prompt of conscious thought, the respiratory system carries out its
life-sustaining activities. If the respiratory systems tasks are
interrupted for more than a few minutes, serious, irreversible
damage to tissues occurs, followed by the failure of all body
systems, and ultimately, death.
While the intake of oxygen and removal of carbon dioxide are the
primary functions of the respiratory system, it plays other
important roles in the body. The respiratory system helps regulate
the balance of acid and base in tissues, a process crucial for the
normal functioning of cells. It protects the body against
disease-causing organisms and toxic substances inhaled with air.
The respiratory system also houses the cells that detect smell, and
assists in the production of sounds for speech.
The respiratory and circulatory systems work together to deliver
oxygen to cells and remove carbon dioxide in a two-phase process
called respiration. The first phase of respiration begins with
breathing in, or inhalation. Inhalation brings air from outside the
body into the lungs. Oxygen in the air moves from the lungs through
blood vessels to the heart, which pumps the oxygen-rich blood to
all parts of the body. Oxygen then moves from the bloodstream into
cells, which completes the first phase of respiration. In the
cells, oxygen is used in a separate energy-producing process called
cellular respiration, which produces carbon dioxide as a byproduct.
The second phase of respiration begins with the movement of carbon
dioxide from the cells to the bloodstream. The bloodstream carries
carbon dioxide to the heart, which pumps the carbon dioxide-laden
blood to the lungs. In the lungs, breathing out, or exhalation,
removes carbon dioxide from the body, thus completing the
respiration cycle.
STRUCTURE
The organs of the respiratory system extend from the nose to the
lungs and are divided into the upper and lower respiratory tracts.
The upper respiratory tract consists of the nose and the pharynx,
or throat. The lower respiratory tract includes the larynx, or
voice box; the trachea, or windpipe, which splits into two main
branches called bronchi; tiny branches of the bronchi called
bronchioles; and the lungs, a pair of saclike, spongy organs. The
nose, pharynx, larynx, trachea, bronchi, and bronchioles conduct
air to and from the lungs. The lungs interact with the circulatory
system to deliver oxygen and remove carbon dioxide.
A Nasal Passages Anatomy of the Nose
The uppermost portion of the human respiratory system, the nose
is a hollow air passage that functions in breathing and in the
sense of smell. The nasal cavity moistens and warms incoming air,
while small hairs and mucus filter out harmful particles and
microorganisms
The flow of air from outside of the body to the lungs begins
with the nose, which is divided into the left and right nasal
passages. The nasal passages are lined with a membrane composed
primarily of one layer of flat, closely packed cells called
epithelial cells. Each epithelial cell is densely fringed with
thousands of microscopic cilia, fingerlike extensions of the cells.
Interspersed among the epithelial cells are goblet cells,
specialized cells that produce mucus, a sticky, thick, moist fluid
that coats the epithelial cells and the cilia. Numerous tiny blood
vessels called capillaries lie just under the mucous membrane, near
the surface of the nasal passages. While transporting air to the
pharynx, the nasal passages play two critical roles: they filter
the air to remove potentially disease-causing particles; and they
moisten and warm the air to protect the structures in the
respiratory system.
Filtering prevents airborne bacteria, viruses, other potentially
disease-causing substances from entering the lungs, where they may
cause infection. Filtering also eliminates smog and dust particles,
which may clog the narrow air passages in the smallest bronchioles.
Coarse hairs found just inside the nostrils of the nose trap
airborne particles as they are inhaled. The particles drop down
onto the mucous membrane lining the nasal passages. The cilia
embedded in the mucous membrane wave constantly, creating a current
of mucus that propels the particles out of the nose or downward to
the pharynx. In the pharynx, the mucus is swallowed and passed to
the stomach, where the particles are destroyed by stomach acid. If
more particles are in the nasal passages than the cilia can handle,
the particles build up on the mucus and irritate the membrane
beneath it. This irritation triggers a reflex that produces a
sneeze to get rid of the polluted air.
The nasal passages also moisten and warm air to prevent it from
damaging the delicate membranes of the lung. The mucous membranes
of the nasal passages release water vapor, which moistens the air
as it passes over the membranes. As air moves over the extensive
capillaries in the nasal passages, it is warmed by the blood in the
capillaries. If the nose is blocked or stuffy due to a cold or
allergies, a person is forced to breath through the mouth. This can
be potentially harmful to the respiratory system membranes, since
the mouth does not filter, warm, or moisten air.
In addition to their role in the respiratory system, the nasal
passages house cells called olfactory receptors, which are involved
in the sense of smell. When chemicals enter the nasal passages,
they contact the olfactory receptors. This triggers the receptors
to send a signal to the brain, which creates the perception of
smell.
B Pharynx
Air leaves the nasal passages and flows to the pharynx, a short,
funnel-shaped tube about 13 cm (5 in) long that transports air to
the larynx. Like the nasal passages, the pharynx is lined with a
protective mucous membrane and ciliated cells that remove
impurities from the air. In addition to serving as an air passage,
the pharynx houses the tonsils, lymphatic tissues that contain
white blood cells. The white blood cells attack any disease-causing
organisms that escape the hairs, cilia, and mucus of the nasal
passages and pharynx. The tonsils are strategically located to
prevent these organisms from moving further into the body. One
tonsil, called the adenoids, is found high in the rear wall of the
pharynx. A pair of tonsils, the palatine tonsils, is located at the
back of the pharynx on either side of the tongue. Another pair, the
lingual tonsils, is found deep in the pharynx at the base of the
tongue. In their battles with disease-causing organisms, the
tonsils sometimes become swollen with infection. When the adenoids
are swollen, they block the flow of air from the nasal passages to
the pharynx, and a person must breathe through the mouth.
C Larynx
Air moves from the pharynx to the larynx, a structure about 5 cm
(2 in) long located approximately in the middle of the neck.
Several layers of cartilage, a tough and flexible tissue, comprise
most of the larynx. A protrusion in the cartilage called the Adams
apple sometimes enlarges in males during puberty, creating a
prominent bulge visible on the neck.
While the primary role of the larynx is to transport air to the
trachea, it also serves other functions. It plays a primary role in
producing sound; it prevents food and fluid from entering the air
passage to cause choking; and its mucous membranes and
cilia-bearing cells help filter air. The cilia in the larynx waft
airborne particles up toward the pharynx to be swallowed.
Food and fluids from the pharynx usually are prevented from
entering the larynx by the epiglottis, a thin, leaflike tissue. The
stem of the leaf attaches to the front and top of the larynx. When
a person is breathing, the epiglottis is held in a vertical
position, like an open trap door. When a person swallows, however,
a reflex causes the larynx and the epiglottis to move toward each
other, forming a protective seal, and food and fluids are routed to
the esophagus. If a person is eating or drinking too rapidly, or
laughs while swallowing, the swallowing reflex may not work, and
food or fluid can enter the larynx. Food, fluid, or other
substances in the larynx initiate a cough reflex as the body
attempts to clear the larynx of the obstruction. If the cough
reflex does not work, a person can choke, a life-threatening
situation. The Heimlich maneuver is a technique used to clear a
blocked larynx. A surgical procedure called a tracheotomy is used
to bypass the larynx and get air to the trachea in extreme cases of
choking.
D Trachea, Bronchi, and Bronchioles
Air passes from the larynx into the trachea, a tube about 12 to
15 cm (about 5 to 6 in) long located just below the larynx. The
trachea is formed of 15 to 20 C-shaped rings of cartilage. The
sturdy cartilage rings hold the trachea open, enabling air to pass
freely at all times. The open part of the C-shaped cartilage lies
at the back of the trachea, and the ends of the C are connected by
muscle tissue.
The base of the trachea is located a little below where the neck
meets the trunk of the body. Here the trachea branches into two
tubes, the left and right bronchi, which deliver air to the left
and right lungs, respectively. Within the lungs, the bronchi branch
into smaller tubes called bronchioles. The trachea, bronchi, and
the first few bronchioles contribute to the cleansing function of
the respiratory system, for they, too, are lined with mucous
membranes and ciliated cells that move mucus upward to the
pharynx.
E Alveoli
Human Lungs
Though the right lung has three lobes, the left lung, with a
cleft to accommodate the heart, has only two. The two branches of
the trachea, called bronchi, subdivide within the lobes into
smaller and smaller air vessels. They terminate in alveoli, tiny
air sacs surrounded by capillaries. When the alveoli inflate with
inhaled air, oxygen diffuses into the blood in the capillaries to
be pumped by the heart to the tissues of the body, and carbon
dioxide diffuses out of the blood into the lungs, where it is
exhaled.
The bronchioles divide many more times in the lungs to create an
impressive tree with smaller and smaller branches, some no larger
than 0.5 mm (0.02 in) in diameter. These branches dead-end into
tiny air sacs called alveoli. The alveoli deliver oxygen to the
circulatory system and remove carbon dioxide. Interspersed among
the alveoli are numerous macrophages, large white blood cells that
patrol the alveoli and remove foreign substances that have not been
filtered out earlier. The macrophages are the last line of defense
of the respiratory system; their presence helps ensure that the
alveoli are protected from infection so that they can carry out
their vital role.
The alveoli number about 150 million per lung and comprise most
of the lung tissue. Alveoli resemble tiny, collapsed balloons with
thin elastic walls that expand as air flows into them and collapse
when the air is exhaled. Alveoli are arranged in grapelike
clusters, and each cluster is surrounded by a dense hairnet of
tiny, thin-walled capillaries. The alveoli and capillaries are
arranged in such a way that air in the wall of the alveoli is only
about 0.1 to 0.2 microns from the blood in the capillary. Since the
concentration of oxygen is much higher in the alveoli than in the
capillaries, the oxygen diffuses from the alveoli to the
capillaries. The oxygen flows through the capillaries to larger
vessels, which carry the oxygenated blood to the heart, where it is
pumped to the rest of the body.
Carbon dioxide that has been dumped into the bloodstream as a
waste product from cells throughout the body flows through the
bloodstream to the heart, and then to the alveolar capillaries. The
concentration of carbon dioxide in the capillaries is much higher
than in the alveoli, causing carbon dioxide to diffuse into the
alveoli. Exhalation forces the carbon dioxide back through the
respiratory passages and then to the outside of the body.
III REGULATION
Diaphragm and Respiration As the diaphragm contracts and moves
downward, the pectoralis minor and intercostal muscles pull the rib
cage outward. The chest cavity expands, and air rushes into the
lungs through the trachea to fill the resulting vacuum. When the
diaphragm relaxes to its normal, upwardly curving position, the
lungs contract, and air is forced out.
The flow of air in and out of the lungs is controlled by the
nervous system, which ensures that humans breathe in a regular
pattern and at a regular rate. Breathing is carried out day and
night by an unconscious process. It begins with a cluster of nerve
cells in the brain stem called the respiratory center. These cells
send simultaneous signals to the diaphragm and rib muscles, the
muscles involved in inhalation. The diaphragm is a large,
dome-shaped muscle that lies just under the lungs. When the
diaphragm is stimulated by a nervous impulse, it flattens. The
downward movement of the diaphragm expands the volume of the cavity
that contains the lungs, the thoracic cavity. When the rib muscles
are stimulated, they also contract, pulling the rib cage up and out
like the handle of a pail. This movement also expands the thoracic
cavity. The increased volume of the thoracic cavity causes air to
rush into the lungs. The nervous stimulation is brief, and when it
ceases, the diaphragm and rib muscles relax and exhalation occurs.
Under normal conditions, the respiratory center emits signals 12 to
20 times a minute, causing a person to take 12 to 20 breaths a
minute. Newborns breathe at a faster rate, about 30 to 50 breaths a
minute.
The rhythm set by the respiratory center can be altered by
conscious control. The breathing pattern changes when a person
sings or whistles, for example. A person also can alter the
breathing pattern by holding the breath. The cerebral cortex, the
part of the brain involved in thinking, can send signals to the
diaphragm and rib muscles that temporarily override the signals
from the respiratory center. The ability to hold ones breath has
survival value. If a person encounters noxious fumes, for example,
it is possible to avoid inhaling the fumes.
A person cannot hold the breath indefinitely, however. If
exhalation does not occur, carbon dioxide accumulates in the blood,
which, in turn, causes the blood to become more acidic. Increased
acidity interferes with the action of enzymes, the specialized
proteins that participate in virtually all biochemical reaction in
the body. To prevent the blood from becoming too acidic, the blood
is monitored by special receptors called chemoreceptors, located in
the brainstem and in the blood vessels of the neck. If acid builds
up in the blood, the chemoreceptors send nervous signals to the
respiratory center, which overrides the signals from the cerebral
cortex and causes a person to exhale and then resume breathing.
These exhalations expel the carbon dioxide and bring the blood acid
level back to normal.
A person can exert some degree of control over the amount of air
inhaled, with some limitations. To prevent the lungs from bursting
from overinflation, specialized cells in the lungs called stretch
receptors measure the volume of air in the lungs. When the volume
reaches an unsafe threshold, the stretch receptors send signals to
the respiratory center, which shuts down the muscles of inhalation
and halts the intake of air.
THE DIGESTIVE SYSTEM
The Digestive System is a series of connected organs whose
purpose is to break down, or digest, the food we eat. Food is made
up of large, complex molecules, which the digestive system breaks
down into smaller, simple molecules that can be absorbed into the
bloodstream. The simple molecules travel through the bloodstream to
all of the body's cells, which use them for growth, repair, and
energy.
All animals have a digestive system, a feature that
distinguishes them from plants. Plants produce their own food in a
process called photosynthesis, during which they use sunlight to
convert water and carbon dioxide into simple sugars. But animals,
including humans, must take in food in the form of organic matter,
such as plants or other animals.
Digestion generally involves two phases: a mechanical phase and
a chemical phase. In the mechanical phase, teeth or other
structures physically break down large pieces of food into smaller
pieces. In the chemical phase, digestive chemicals called enzymes
break apart individual molecules of food to yield molecules that
can be absorbed and distributed throughout the body. These enzymes
are secreted (produced and released) by glands in the body.
The digestive system of most animals consists mainly of a long,
continuous tube called the alimentary canal, or digestive tract.
This canal has a mouth at one end, through which food is taken in,
and an anus at the other end, through which digestive wastes are
excreted. Muscles in the walls of the alimentary canal move the
food along. Most digestive organs are part of the alimentary canal.
However, two accessory digestive organs, the liver and pancreas,
are located outside the alimentary canal. These organs contribute
to chemical digestion by releasing digestive juices into the canal
through tubes called ducts.
THE HUMAN DIGESTIVE SYSTEM
The human digestive system consists of a series of organs and
structures that help break down food and absorb nutrients for use
throughout the body. Food enters the digestive system through the
mouth and passes through the esophagus, stomach, small intestine,
large intestine, and rectum. Other organs, such as the liver,
further aid in the breakdown of food, absorption of nutrients, and
elimination of undigestible materials from the body
If a human adults digestive tract were stretched out, it would
be 6 to 9 m (20 to 30 ft) long. In humans, digestion begins in the
mouth, where both mechanical and chemical digestion occur. The
mouth quickly converts food into a soft, moist mass. The muscular
tongue pushes the food against the teeth, which cut, chop, and
grind the food. Glands in the cheek linings secrete mucus, which
lubricates the food, making it easier to chew and swallow. Three
pairs of glands empty saliva into the mouth through ducts to
moisten the food. Saliva contains the enzyme ptyalin, which begins
to hydrolyze (break down) starcha carbohydrate manufactured by
green plants.
Once food has been reduced to a soft mass, it is ready to be
swallowed. The tongue pushes this masscalled a bolusto the back of
the mouth and into the pharynx. This cavity between the mouth and
windpipe serves as a passageway both for food on its way down the
alimentary canal and for air passing into the windpipe. The
epiglottis, a flap of cartilage, covers the trachea (windpipe) when
a person swallows. This action of the epiglottis prevents choking
by directing food from the windpipe and toward the stomach.
A The Esophagus
The presence of food in the pharynx stimulates swallowing, which
squeezes the food into the esophagus. The esophagus, a muscular
tube about 25 cm (10 in) long, passes behind the trachea and heart
and penetrates the diaphragm (muscular wall between the chest and
abdomen) before reaching the stomach. Food advances through the
alimentary canal by means of rhythmic muscle contractions
(tightenings) known as peristalsis. The process begins when
circular muscles in the esophagus wall contract and relax (widen)
one after the other, squeezing food downward toward the stomach.
Food travels the length of the esophagus in two to three
seconds.
A circular muscle called the esophageal sphincter separates the
esophagus and the stomach. As food is swallowed, this muscle
relaxes, forming an opening through which the food can pass into
the stomach. Then the muscle contracts, closing the opening to
prevent food from moving back into the esophagus. The esophageal
sphincter is the first of several such muscles along the alimentary
canal. These muscles act as valves to regulate the passage of food
and keep it from moving backward.
B The Stomach
The stomach, located in the upper abdomen just below the
diaphragm, is a saclike structure with strong, muscular walls. The
stomach can expand significantly to store all the food from a meal
for both mechanical and chemical processing. The stomach contracts
about three times per minute, churning the food and mixing it with
gastric juice. This fluid, secreted by thousands of gastric glands
in the lining of the stomach, consists of water, hydrochloric acid,
an enzyme called pepsin, and mucin (the main component of mucus).
Hydrochloric acid creates the acidic environment that pepsin needs
to begin breaking down proteins. It also kills microorganisms that
may have been ingested in the food. Mucin coats the stomach,
protecting it from the effects of the acid and pepsin. About four
hours or less after a meal, food processed by the stomach, called
chyme, begins passing a little at a time through the pyloric
sphincter into the duodenum, the first portion of the small
intestine.
C The Small Intestine
Most digestion, as well as absorption of digested food, occurs
in the small intestine. This narrow, twisting tube, about 2.5 cm (1
in) in diameter, fills most of the lower abdomen, extending about 6
m (20 ft) in length. Over a period of three to six hours,
peristalsis moves chyme through the duodenum into the next portion
of the small intestine, the jejunum, and finally into the ileum,
the last section of the small intestine. During this time, the
liver secretes bile into the small intestine through the bile duct.
Bile breaks large fat globules into small droplets, which enzymes
in the small intestine can act upon. Pancreatic juice, secreted by
the pancreas, enters the small intestine through the pancreatic
duct. Pancreatic juice contains enzymes that break down sugars and
starches into simple sugars, fats into fatty acids and glycerol,
and proteins into amino acids. Glands in the intestinal walls
secrete additional enzymes that break down starches and complex
sugars into nutrients that the intestine absorbs. Structures called
Brunners glands secrete mucus to protect the intestinal walls from
the acid effects of digestive juices.
The small intestines capacity for absorption is increased by
millions of fingerlike projections called villi, which line the
inner walls of the small intestine. Each villus is about 0.5 to 1.5
mm (0.02 to 0.06 in) long and covered with a single layer of cells.
Even tinier fingerlike projections called microvilli cover the cell
surfaces. This combination of villi and microvilli increases the
surface area of the small intestines lining by about 150 times,
multiplying its capacity for absorption. Beneath the villis single
layer of cells are capillaries (tiny vessels) of the bloodstream
and the lymphatic system. These capillaries allow nutrients
produced by digestion to travel to the cells of the body. Simple
sugars and amino acids pass through the capillaries to enter the
bloodstream. Fatty acids and glycerol pass through to the lymphatic
system.
D The Large Intestine
A watery residue of indigestible food and digestive juices
remains unabsorbed. This residue leaves the ileum of the small
intestine and moves by peristalsis into the large intestine, where
it spends 12 to 24 hours. The large intestine forms an inverted U
over the coils of the small intestine. It starts on the lower
right-hand side of the body and ends on the lower left-hand side.
The large intestine is 1.5 to 1.8 m (5 to 6 ft) long and about 6 cm
(2.5 in) in diameter.
The large intestine serves several important functions. It
absorbs waterabout 6 liters (1.6 gallons) dailyas well as dissolved
salts from the residue passed on by the small intestine. In
addition, bacteria in the large intestine promote the breakdown of
undigested materials and make several vitamins, notably vitamin K,
which the body needs for blood clotting. The large intestine moves
its remaining contents toward the rectum, which makes up the final
15 to 20 cm (6 to 8 in) of the alimentary canal. The rectum stores
the feceswaste material that consists largely of undigested food,
digestive juices, bacteria, and mucusuntil elimination. Then,
muscle contractions in the walls of the rectum push the feces
toward the anus. When sphincters between the rectum and anus relax,
the feces pass out of the body.
IV REGULATION OF THE DIGESTIVE PROCESS
The body coordinates the various steps of digestion so that the
process proceeds smoothly and cells obtain a steady supply of
nutrients and energy. The central nervous system and various glands
control activities that regulate the digestive process, such as the
secretion of enzymes and fluids. For example, the presence of food
in the esophagus, stomach, or intestines triggers peristalsis. Food
entering the stomach also stimulates the central nervous system to
initiate the release of gastric juice. And as hydrochloric acid
passes from the stomach, the small intestine produces secretin, a
substance that simulates secretion of pancreatic juice.
Nervous SystemNervous System
is the master controlling and communicating system of the
body
its functions are:
a. it uses its million of sensory receptors to monitor changes
(stimuli) occurring both inside and outside the body ( sensory
input)
b. it processes and interprets the sensory input and makes
decisions about what should be done at each moment (
integration)
c. it then effects a response by activating muscles or glands (
motor output)
Meninges
- connective tissue layers which covers and protects the CNS
structures
Three (3) Meninges of the Brain
a. Dura mater
- outer layer is tough white fibrous connective tissue
b. Arachnoid
- middle layer of meninges, which resembles a cobweb in
appearance, is a thin
layer with numerous threadlike strands that attach it to the
innermost layer
c. Pia mater
the innermost layer of meninges
thin, delicate membrane that is tightly bound to the surface of
the brain and spinal cord and cannot be dissected away without
damaging the surface
Motor Neurons
A. Upper motor Neurons nerve cells in the cerebral cortex that
help make up the following nerve tracts:
a. Corticospinal Tract
The Corticospinal Tract is the largest descending pathway in
man. It originates in part from the pyramidal cells in the cortex
of each cerebral hemisphere and courses through the internal
capsule, then through the medullary pyramids. At this point some
80% of the fibres from each hemisphere, decussate in the pyramidal
decussation, and continue to descend in the lateral white column of
the opposite side. The remaining 20% continue down ipsilaterally,
in the ventro-medial white column, to innervate bilaterally, the
more medially located motor neurones of the axial and proximal
muscles.
The crossed fibres in the lateral white columns comprise both
sensory axons (from post-central gyrus and parietal association
areas), and motor axons (from precentral gyrus and prefrontal
areas). The sensory axons project into the dorsal horn of the grey
matter, to effect feedback regulation of the input pathways. The
motor axons terminate on motor neurons of the distal muscles,
either directly or indirectly via interneurons.
There is some controversy as to the exact contribution of
different areas of cerebral cortex to the corticospinal tracts. Two
proposed schemes are illustrated below, but authorities vary
widely.
b. Corticobulbar Tract
The corticobulbar (or corticonuclear) tract is a white matter
pathway connecting the cerebral cortex to the brainstem (the term
"bulbar" referring to the brainstem).
The 'bulb' is an archaic term for the medulla oblongata. In
clinical usage, it includes the pons as well.
The muscles of the face, head and neck are controlled by the
corticobulbar system, which terminates on motor neurons within
brainstem motor nuclei. This is in contrast to the corticospinal
tract, which connects the cerebral cortex to spinal motor neurons,
and controls movement of the torso, upper and lower limbs.B. Lower
Motor Neurons
Lower motor neurons (LMNs) are the motor neurons connecting the
brainstem and spinal cord to muscle fibers, bringing the nerve
impulses from the upper motor neurons out to the muscles.
Anatomy and Physiology of Cerebrospinal Fluid
The CSF is clear colorless fluid which has minimal content of
protein. It is contained in the ventricular system as well as the
subarachnoid spaces surrounding the brain and the spinal cord. The
CSF is in hydrostatic equilibrium with the interstitial tissue of
the brain and can permeate across the brain tissue in both
directions. It is expected that the brain tissue and the CSF would
have the same hydrostatic pressure in any part of the brain. As
much as the brain tissue is protected by a blood brain barrier from
changes outside the central nervous system, the CSF has the same
protection and does not change biochemically as a result of changes
in the systemic circulation. These barriers are at the level of the
endothelium of brain capillaries, at the level of the epithelium of
the choroid plexuses and the outer layers of arachnoid matter.
These barriers protect the brain and the subarachnoid spaces from
damaging influences outside the brain.
Cerebrospinal Fluid Volume and Distribution
The cerebrospinal fluid fills the cavity of the ventricles and
the subarachnoid spaces. The subarachnoid spaces are wide in
certain areas and these are called cisterns. At the
cerebellomedullary area the cistern is called cisterna magna. We
have also the pre-pontine cistern surrounding the basilar artery
and the interpeduncular cistern surrounding the circle of Willis.
The subarachnoid space extends caudally around the spinal cord and
ends in lumbar -sacral dural sac where it surrounds the cauda
equina.
The average volume of intracranial cerebrospinal fluid is 125
mls with 89 mls in the subarachnoid space. The volume of CSF in the
lumbar sac is about 30 mls.Cerebrospinal Fluids Formation
The majority of CSF is produced by the choroid plexuses, there
are assumptions that some CSF is formed outside the choroid
plexuses, from the brain substance. This is estimated to be about
10 to 15% of the whole volume of CSF.
It is believed that CSF is formed at a rate of .5 ml per minute.
It is believed that there is a persistent and steady production of
CSF irrespective of systemic changes. It is independent of the mean
arterial blood pressure until this is reduced below 60 mmHg.
However it is believed that the perfusion pressure influenced the
production of CSF i.e. CSF production is reduced at a higher
threshold of systemic blood pressure when the CSF pressure is
raised. Reduction of perfusion pressure might act by diminishing
choroid plexus blood flow and the supply of necessary material for
CSF secretion.
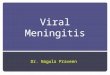
CSF Circulation and Drainage
From the lateral ventricles CSF passes through the foramen of
Munro to the 3rd ventricle(fig 1). From there it passes through the
aqueduct of the Sylvius to the 4th ventricle. With the CSF formed
by the choroid plexus in the 4th ventricle it exits through the
roof of the 4th ventricle. From there it passes along the outer
surface of the cerebellum and through the basal cisterns. It passes
through the hiatus of the tent to the Sylvian fissures and from
there to the para-sagittal area. It is excreted by the arachnoid
villi into the venous sinus, mainly the sagittal sinus. It is
believed that CSF takes one to two hours to reach the basal
cisterns, 3 to 4 hours to reach the sylvian fissure and 10 to 12
hours to spread over the cerebral subarachnoid space. By 24 hours
it started to be cleared into the superior sagittal sinus. The
mechanism by which the CSF is secreted through the arachnoid villi
is still not clear.
Normal CSF Pressure
In children and babies CSF pressure is low. In infants it is
estimated to be 40 to 50 mms of water and in children from 40 - 100
mms of water. In older age group it remains constant of about 150
mms of water or 15 mm of Mercury. Pressures above 200 mms mms of
water or 20 mms of Mercury are considered abnormal.
The cerebral spinal fluid pressure is dependent on intracranial
venous pressure; it is usually about 40 to 50 mms of water above
the intracranial venous pressure. The difference in pressure is
related to the continuous production of CSF and resistance to its
secretion.
There are fluctuations in the CSF pressure, these are influenced
by ventilation and cardiac contraction .CSF pressure falls with
inspiration and rises during expiration, a variation of about 40
mms of water.
VI. LABORATORY
BLOOD CHEMISTRY
TEST09/25/0610/06/06NORMAL VALUES
Creatinine0.2mg/dL0.4 1.5mg/dL
AST402U/L51U/L16-35U/L
Glucose(RBS)247mg/dL