Embed Size (px)
Citation preview

J Med Genet 1993; 30: 713-727
REVIEW ARTICLE
Mendelian cytogenetics. Chromosomerearrangements associated with mendeliandisorders
Niels Tommerup
The first successful mapping of a mendeliandisorder by chromosome rearrangements wasthat of the Duchenne muscular dystrophylocus to Xp21.1-5 Since then, chromosome ab-errations which delete, truncate, or otherwiserearrange and mutate specific genes have notonly helped in the mapping of other diseaseloci,6 but have turned out to be key elementsfor the rapid isolation of disease genes bypositional cloning strategies.7 Accordingly, alisting of the clinical disorders in which associ-ated chromosome rearrangements have beendescribed forms a part of the Human GeneMapping Workshops.6 Although the early suc-cess led to a proposal for systematic cytogene-tic analysis of subjects with mendelian dis-orders,8 this has rarely been done. A commonfeeling is that, as mutations, these rearrange-ments are rare exceptions. The aim of thepresent review is to document that they may berare, but are not exceptions, and to focus onfactors which may influence their occurrenceand facilitate their detection.
The Danish Centre forHuman GenomeResearch, The John FKennedy Institute, GILandevej 7, DK-2600Glostrup, Denmark,and Department ofMedical Genetics,Ullevaal UniversityHospital, Oslo,Norway.N Tommerup
Contiguous gene syndromes in relationto mendelian geneticsGenetic disorders are usually classified intomendelian, chromosomal, and multifactorialcategories. Mendelism involves transmissionpatterns of traits which traditionally are
thought to be determined by single genes. Themere fact that a chromosome rearrangementmay lead to the development of a mendeliandisorder suggests that this distinction betweenmendelian and chromosome disorders may bearbitrary.9 This is illustrated by Miller-Diekersyndrome (MDCR), lissencephaly with a char-acteristic facial appearance, that was originallylisted as an autosomal recessive conditionowing to the presence of familial cases withtwo or more affected sibs.9 All familial cases
analysed have so far been shown to be associ-ated with unbalanced segregation of familialtranslocations or inversions, leading to seg-
mental aneuploidy (deletion) of a distal seg-
ment of 17p.1''2 Thus, MDCR not associatedwith a chromosome abnormality is probablybest explained as an autosomal dominant con-
dition where all mutations are de novo.
MDCR also illustrates a mutationalmechanism that may eventually explain a sub-
stantial part of the heterogeneity and overlapin syndromology: contiguous gene syndromeswhere microscopic or submicroscopic dele-tions (or duplications) involve an array ofclosely positioned genes.'314 A purpose of themolecular characterisation of contiguous genesyndromes is to identify individual genesresponsible for specific components of thephenotypic complex. This is probably bestillustrated by the molecular studies ofdeletions and translocations involving llp13associated with various combinations ofWilms's tumour, aniridia, genitourinary mal-formations, and mental retardation (WAGRcomplex).'5 The resulting isolation of candi-date genes for Wilms's tumour (WT1)'6 7 andaniridia (AN2, PAX6)'8 '9 now provides ameans for molecular studies and delineation ofmonogenic conditions within 1 lpl3.2"24 Simi-larly, the dissection of the phenotype inMDCR has begun with the demonstration ofsubmicroscopic deletions in cases with isolatedlissencephaly.2526Any visible chromosome imbalance almost
invariably represents a contiguous gene dis-order, but few chromosomal syndromes in-clude features of sufficient specificity to permita correlation with a recognised mendelian dis-order. This includes many of the classicalchromosome disorders,27 as well as newlyrecognised ones.28 Although these chromo-some aberrations may not have immediate im-plications for known mendelian traits, futuremolecular dissection of these disorders maychange this.
Chromosome rearrangements inrelation to autosomal dominant,autosomal recessive, and X linkeddiseaseSpecific chromosome rearrangements havepredominantly been described in autosomaldominant (AD) and in X linked conditions. Ofthe 625 chromosomally mapped loci associatedwith genetic disorders, 54 (8-6%) are Xlinked.29 However, more than one third of theapproximately 70 mendelian disorders associ-ated with a specific chromosome rearrange-ment are X linked6 (figure). This excess can beexplained by almost routine application ofcytogenetic analysis in two particular groups of
713
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Tommerup
.Al
vws -
wsij
HPE2
9
6
I|1 BWSt)DGCR2
AN28
II
III
IIII
10
IBWS
GR
11
t)
12
7
Al
12
MBS MBS
RBI RB1
HSCR
13 14 15 16 17
AIC*
DMD/BMDNDPIP1
EDA
FGDYHPE4 ~~~~~~~MNK*
~~AG ~~TCD
gHP4 g i DGCR SOCRL
IIDS~~~~~~~~~~TKC
18 19 20 21 22 X
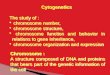
Deletion Duplication 0 Locus specific rearrangement (translocation, inversion)
*Fragile site g Regions where viable deletions have been described.
g Regions with only 1-3 reports of viable deletions.
Translocation breakpoints detected in a non-biased way in prenatal diagnosis79
Localisation of mendelian disorders where chromosome rearrangements have been described. For explanation of symbols, see Appendix.
patients: females affected with X linked dis-eases, suggesting X;autosome translocations,and males suffering from two or more X linkeddisorders, suggesting a contiguous gene syn-drome. Since there are no a priori reasons tobelieve that chromosome rearrangementsshould be less frequent in AD than in X linkeddisorders, the underrepresentation in AD dis-orders is probably because of ascertainmentbias.The cytogenetic data in autosomal recessive
(AR) disorders are so scanty that reliable state-ments regarding their frequency cannot bemade. In only one AR disorder (Zellwegersyndrome) has more than one chromosomerearrangement been described, a de novo dele-tion and a de novo inversion.303' A specific
chromosome mutation will only show an ARlocus if the other allele happens to be mutated(unmasking of heterozygosity),32 and this willbe a rare occurrence as the gene frequencies foreven the most common AR disorders do notexceed 1/25 to 1/50. Owing to the number ofrecessive traits, and the relatively high fre-quency of familial translocations and inver-sions in man,33 some of these breakpoints mayaffect recessive loci. Thus, several murinebalanced translocations are lethal in thehomozygous state.34 The risk of unmasking ofheterozygosity by a transmissible chromosomerearrangement will increase with the numberof individuals that receive the rearrangement.In addition, familial translocations maypredispose to the formation of uniparental
S!S/CDPX1 /MRX2/iSrS/KAL1I/OA1GFDH/AICAIEDAHC/GK/DMD/XK/CYBB/RP3
TCD/IDFN3SRY
ILYP AZF AZF
IFRAXA
y
I
714
VI
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Mendelian cytogenetics. Chromosome rearrangements associated with mendelian disorders
Table I Chromosome rearrangements in deletion viable regions.Disorder Chromosomal Type of rearrangement(locus symbol) localisation
Deletions (No) Locus specific type
Multiple'78b 179aMultiple72 180aMultiple70 181ai 180aMultiplemat)6568a8d 122a 183a
Multiple52a7d 54d
3187a 188a 186c?
5189a 191a 190b 183dMult' le'93-196a4199a 172d
Multiple70Multiple207 208aMultiple72 209 210a,bMultiple37 211Multiple213-2l7a,d7214a,d 8a
Muit ile77 72a,b3163a I 4a
Multiple7' 72a,b
488a,d4233aMultiple234 236 237a,dMulti le234 238a,d3239-24IalMultiple70aMultiple'27 244 245 248a,d
173b1249aMultiple"o- 2 25 26a,dMultiple70
Multiple?703257 259 260a
Multiple(pat)41851,,d
Multiple3844a,b,c?,d7264 2698
Multiple7Oa 267 268aMultiple798Multiple701Multiple37 174b 271a,b
5276-280a,cMultiple282 283a,d1 285a
Multiple52a,b,d130a
t(X;3)(p22;ql2)182.
inv(l5)(pl qI3)mat6'696t(4;I 1)(q22;p13)60bt( 1 ;22)(p I 3;q 12.2)?8t(5;1 1)(qI3.1;p13)26t(5;12l)(pl 1;p13)'6'6t(8; 1 2)(pi I 1 p 1 3) 184b
t(3;8)(p21;pl 1)185bt(5;10)(q22;?)'
t(3;1 1)(q21;q23) 90bt(3;4)(q23;p15.2)20at(3;8)(q23;p2 1.1)17
t(2;22)(q14.1;ql 1.1)212bMultiple2""at(3;7)(p21 .Ip13)960bt(6;7)(q27;p 13) 61bt(6;7)(qI2;pl 3)162
t(4;5)(q2 1;p 15 *3)2t(4;6)(q2 1;p24)2 2b
t(7;9)(q36;q34)235b
t(2;8)(q33;q24. 1)127t(4;8)(pl5.3;q24. 1)127t(8;1 1)(q24.1 1;p15.5)246inv(8)(ql 1.23q21 .1 )247b
t(1;13)(p34;ql 3)250b
t(4;22)(q12;q I 2.2)25bt(4;15)(ql2q21;ql 1)25111 X;A translocation (see ref 61)85 autosomal translocations61binv(15)(pl3ql 3)pat64Multiple4't(5;7;9)(qI 1 .2q34;q21 .2q31 .3;q22. 1)21,t(7;9)(ql 1.21;p12)263b
t(X;7)(q2 1.2;p 14)2711t(X;1 3)(q21 .2;p 1 2)274,t(X;3)(q28;q21 )275at(X;10)(q28;ql 1.2)275,dir ins(8)(q24. 1 ql 3.3q21.13)281b
inv(2)(q35q37.3)217ainv(7)(pl2ql 1.23)31a
See Appendix for explanation of locus symbols. a=de novo aberration. b=familial transmission. c=evidence of germlinemosaicism. d= unbalanced familial reciprocal translocation/inversion. e= Meera-Khan, personal communication. x = visiblyunbalanced translocation.
disomy, whereby AR mutations can bereduced to homozygosity.35 The occasionaloccurrence of an inherited balanced transloca-tion or inversion would therefore not be unex-pected in AR disorders.36
The effect of chromosome localisationon types and frequencies ofchromosome rearrangementsExact determination of frequencies of chromo-some rearrangements in mendelian disorderscan only be made by systematic studies ofspecific mendelian disorders. This has onlybeen done in a few disorders, retinoblastoma(RB1) being the classical one. The results fromRB1 may not necessarily be valid for other
disorders, and one factor that will influence thefrequency of chromosome rearrangements in a
specific disorder is the chromosomal localisa-tion of the corresponding gene.
Visible deletions among liveborns are absentor extremely rare for several regions of thehuman genome (figure),27 probably becausethey are incompatible with fetal survival.37Whereas deletions are the most frequent typeof rearrangement in those disorders whichmap to the 'deletion viable' regions (table 1,figure), visible deletions do not occur in live-borns affected with mendelian disordersmapping to the 'deletion non-viable' regions(table 2). The division of the genome into adeletion viable and non-viable part may haveconsequences not only for the type and fre-
AGSAHCAICAIEDANCRAN2/PAX6
ANKI
APCAZFBPES
CDPX1CRS1CYBBDFN3DGCR1DGCR2DMD/BMDGCPS
GKHLD
HMRDHPE2HPE3HPE4HSCRKALILGCR
LYPMBSMDCRMRX2NF2OAIPBTPWCR
RB1SHFD1
SRYSSSTSTCD
TKC
TRP1VCFSvwSwS1WTIzws
20pl 1.23-12.1Xp2lXp22.3Xp2l15ql 1-12lpl3
8plI.1
5q22Yqll3q23
Xp22.37p21Xp2lXq2l22ql1lOpl3Xp2l7p13
Xp2l4q12
16p13.32p2l7q3518p13q33.1Xp22.38q24.11
Xq2513ql2.217pl3Xp22.322q 12.2?Xp22.34ql2-1315ql 1-12
13q147ql 1.2-21.3
Ypl2Xp22.3Xp22.3Xq2l
Xq28
8q24.1 122ql 1.2lq32-412q35llpl37ql 1.23
715
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Tommerup
Table 2 Chromosome rearrangements in deletion non-viable* regions.
Disorder Chromosomal Type of rearrangement(locus symbol) localisation
Miscellaneous Locus specific type
BWS 1 p15.4-15.5 del(I 1)(p 1 1 p I 3)203't t(9;1 l)(p 1l.1 lpl5.5)mato' +del( 1 )(pl 1 1p3)205,t t(4;-11)(pl 5.2;pl 5.4)mat 03bmultiple dup(l lp)pat103 202d t(I1 ;22)(pI 5.5;qI 2)mat204b
t(l 1;16)(pI5.5;qI2)mat053bt(I 1;12)(pI5.5;q13.1)mat'03binv(l1)(pl 1.2pI5)mat' 26b
inv(l l)(p15.4q22.3)mat053bCMPD1 17q24.3-25.1 46,XX,t( 1;1 7)(q42. 1 ;q25< 95'
46,XX,inv(17)(ql2q25)96aCMPD1/ 17q24.3-25.1 46XY,t(2; 1 7)(q35;q23-24)97aSRA1 46,XY,t(7; 1 7)(q34;q25)95"
46,XY,t(l13;17)(q331;25 /95EDA Xq13.1 t(X;9)(q13.1;p24)225 228a
t(X;1 2)(q 13.1 ;q24.2)227at(X1l)(q13. ;p36.33)224a
F9 Xq27 t(X; 1)(q27;q23)229aFGDY Xql3 t(X;8)(q13;p21 .2)18bIDS Xq28 t(X;5)(q27;q31)243aIPI Xpll t(X; 15)(p ll;ql 1) or (q ll ;p li)42a
t(X;9)(p 1;q34)'43at(X; I 7)(p I 1 ;p I 1.2) 15at(X;9)(p I 1 ;q33.2) 15at(X;13)(pl 1.21;q12.3)'44at(X; I 0)(p l ;q22)'46at(X;4)(q2 1 ;q28)9t(X;5)(p 1 I.2;q35.2) 147a45,X/46,Xr(X)41'a
MNK Xql3.3 t(X;2)(ql3.3;q32.2)"7at(X;1)(ql 3.3;q21 )§'ins(X)(p 11 .4ql 3.3q2 1 .2)mat06
NDP Xpl I t(X;10)(p 1 ;p1 4)253ainv(X)(p 11 .4q22)254b
NFI 17ql 1.2 t(l;l7)(p34.3;ql 1 2)92bt(17;22)(ql 1.2;ql 1.2)93b
+ ?r(l7)(cen-ql2), del(17)(cen-ql2)91OCRL Xq26.1? t(X;3)(q25;q27)256'
t(X;20)(q26. 1 ;ql 1 .2)257RSTS 16pl13.3 t(2;16)(p 13.3;p 13.3?84,
t(7; 16)(q34;pl13. 3)8 ~at(I6;22)(p13.3;?)inv(l1 6)(p 1 3.3;q I 3)-6inv(16)(p 13.3q 13)1
See Appendix for explanation of locus symbols. * Including regions with only 1-3 reports of viable deletions. t Breakpoints not atestablished p1p5.4-.5 loci. + Personal observation. § J Beck, personal communication. Cited in ref 87.
quency of rearrangements in mendelian dis-orders, but also for selection of strategies fortheir detection.
DISORDERS MAPPING TO REGIONS WHERE
DELETIONS ARE VIABLERetinoblastoma, Wilms's tumour, and aniridiaThe early detection of cases with deletion of aD group (No 13) chromosome in associationwith retinoblastoma (RB1 )38-40 led to extensivecytogenetic screening of large series ofpatients.4''4 Consequently visible deletionshave been found in 2 to 4% of all patients withRB1 when examined by metaphase technique,and in 4 to 8% of patients when examined byhigh resolution techniques. Reciprocal trans-locations have been detected in approximately1% of patients in several independent surveysusing both metaphase and prometaphase reso-lution, corresponding to 10% of the detectedrearrangements. Thus, between 5 and 10% ofall cases with RB1 have a visible chromosomemutation.
Larger systematic cytogenetic studies havenot been reported in association with Wilms'stumour (WT1)/aniridia, so a direct compari-son with the individual traits included in theWilms's tumour/aniridia/genitourinary mal-formation/mental retardation (WAGR) com-plex cannot be made. However, in three largeseries of Wilms's tumour patients, altogethercomprising 1335 cases,45-47 aniridia was
observed in 23 cases (1 7%). Furthermore, 1/3of aniridia cases are sporadic and, of these, 1/3develop Wilms's tumour.48 A visible deletionof lipl3 was seen in all 18 cases with com-bined WT1/aniridia in three high resolutioncytogenetic surveys,474950 supporting the factthat most subjects with this combination havea visible deletion. All evidence supports asingle map position for aniridia at llpl3'.5 Ifso, 1/3 x 1/3 (10%) of independent cases withaniridia may have a visible deletion. Since bothtraits are easily recognised, this is in line withthe large number of cases with the WAGRcomplex and deletions of l 11p3 that have beenreported.52 As expected for contiguous genesyndromes, visible deletions and more com-plex rearrangements within 1lp13 may notaffect both loci.50 53 54 The limited distancebetween WT 1 and the candidate aniridialoci (700 to 100kb)'855 explains why a fewpersons with Wilms's tumour and aniridiahave deletions below the limit of microscopicresolution.5556 Balanced chromosome re-arrangements involving lip13 have not beenreported in association with Wilms's tumour,but one translocation with a breakpoint withinthe region has been seen in association withPotter syndrome,57 and three reciprocal trans-locations have been reported in familial aniri-dia.5 0 Taken together, the data are com-patible with a frequency of chromosomerearrangements in all independent cases withWT1, aniridia, and WT1/aniridia in the same
716
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Mendelian cytogenetics. Chromosome rearrangements associated with mendelian disorders
range as observed in RB1 (2 to 10%), withdeletions being by far the most frequent typeof mutation.
Disorders associated with imprinting:Prader-Willi and Angelman syndromesRepeated observations of rearrangementsinvolving chromosome 15 in patients withPrader-Willi syndrome (PWCR) led to numer-ous systematic studies.61-6 As a result, 60% ofpatients have been found to carry detectablechromosome 15 rearrangements, mostly dele-tions within 15qi 1-13 (table 1). The cytogene-tic spectrum of 300 PWCR subjects with achromosome 15 abnormality included 182interstitial deletions, 34 unbalanced reciprocaltranslocations, 14 Robertsonian transloca-tions, 16 small marker chromosomes, and fourduplications,61-3 plus six balanced transloca-tions and one pericentric inversion.6' Theinversion was inherited from an unaffectedfather.64 Assuming that 60% of PWCR caseshave a cytogenetic defect, the frequency ofapparently balanced rearrangements thus ap-pears to be close to that of RB1 (7 * 60/300) = 14%. However, it should be empha-sised that balanced rearrangements were notreported among 358 PWCR patients studied inlarger chromosome surveys in the period 1981to 1991.6-63
Cytogenetic deletion of 15ql 1-13 is alsoobserved in 50 to 60% of subjects with Angel-man syndrome (ANCR).65 68 Among the fewerthan 100 cases with ANCR that have beenstudied so far, one apparently balanced re-arrangement has been reported, a maternallyinherited inversion with a breakpoint within15q13,68 which was associated with a de novosubmicroscopic deletion in the affected child.69The frequency of visible deletions in RB1,
PWCR, and ANCR thus varies considerably(- 5 to 60%), whereas the frequency of appar-ently balanced cytogenetic rearrangementsmay be within the same order of magnitude(_ 1%).
X linked disordersOn the X chromosome, the male deletionviable regions involve Xp22.3, Xp2l, Xq21,and Xq25 (figure).'7 7 Owing to the excellentmorbid anatomy of the X chromosome,29 thesedeletions are associated with recognisablemendelian traits, either as single gene dis-orders73 or as part of contiguous gene syn-dromes.'77>72 In a survey of five males withDMD and additional clinical signs suggestinga contiguous gene disorder, visible deletionswere detected in all five cases.7' Bivariate flowkaryotyping of 10 visible deletions withinXp2 1 associated with contiguous gene syn-dromes has provided a size estimate of thesedeletions int athe a 4 to 14 Mb.72The frequency of visible deletions in
patients with single gene disorders mapping toXp21 appears to be lower than observed inmany autosomal disorders. In a systematicsurvey of 165 males with Duchenne or Beckermuscular dystrophy only, no chromosome re-
arrangements were observed.75 This may besomewhat surprising since submicroscopic de-letions are extremely common in DMD, andsince intragenic deletions in the 2-4 Mb DMDlocus might potentially reach the lower limit ofmicroscopic resolution.
Disease associated deletions involving thedistal part of Xp22.3 are seen in both malesand females, in males associated with recessivetraits and in females with dominant traits.70Most other X chromosome deletions are pre-ferentially inactivated in female carriers, eitherwithout phenotypic effects or associated withTurner symptoms, including gonadal dys-genesis or secondary amenorrhoea/prematuremenopause.76 However, deletion of the regionXq27 may result in preferential activity of thedeleted X chromosome,77 and it has been sug-gested that this might be because of deletion ofa locus which is involved in the normal Xinactivation process.78 If so, visible or submic-roscopic deletions of Xq27 should be con-sidered, along with X;autosome translocations,in females affected with disorders mapping tothis region.
DISORDERS MAPPING TO REGIONS WHEREDELETIONS ARE NON-VIABLEIn contrast to deletions, breakpoints associatedwith constitutional autosome translocationsdetected in an unbiased way in large series ofprenatal diagnoses79 (figure), as well as inreported X;autosome translocations,80 81 aredistributed all over the genome. Hence, thepresence of disease specific translocationswould not be expected to be influenced by thechromosomal localisation of a disorder to thesame extent as deletions. One modification ofthis is that the G-C rich chromosomal reverse(R) bands contain many more genes than theA-T rich G bands.8283 Therefore, disease spe-cific breakpoints in translocations and inver-sions should predominantly be located in Rbands, which is indeed the case (figure).
If RB 1 is the prototype of a clearly recog-nised disease localised within a chromosomalregion where gross deletion is compatible withfetal survival, Rubinstein-Taybi syndrome(RSTS), von Recklinghausen neurofibromato-sis (NF1), and, to some extent, campomelicdysplasia (CMPD 1) exemplify disorders map-ping to regions where deletions do not or onlyrarely occur.
Rubinstein- Taybi syndrome, vonRecklinghausen neurofibromatosis, andcampomelic dysplasiaA locus for RSTS has been assigned to16p 13.3 after the identification of several inde-pendent chromosome rearrangements withbreakpoints within this region.8>87 Apart fromsmall distal deletions associated with the hae-moglobin H/mental retardation syndrome,88viable visible deletions of l6pl3 have not beendescribed at all.278587 This, together with thedetection of submicroscopic deletions in 25%of RSTS subjects with normal karyotypes,87indicates that it is not deletions as such that do
717
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Tommerup
not occur or that are not compatible with theRSTS phenotype, but rather the size of thedeletions.Both RB1 and WT1 are tumour suppressor
loci.89 However, it is unlikely that this featurein itself is associated with the high frequencyof visible deletions seen in these disorders.Neurofibromatosis type 1 (NFl) also involvesa tumour suppressor gene that maps to17q1 1.2.6 The largest deletion which has so farbeen described in a patient with NFI was380 kb in size,90 well below the limit of micro-scopic resolution. This is in line with thegeneral absence of reported constitutive dele-tions of this part of chromosome 17 (figure).27In the only published case with a visible dele-tion of the proximal part of 17q, the deletedsegment was still present in most of the cells asa small ring chromosome.9' In contrast, and byanalogy with the findings in RSTS, reciprocaltranslocations have been described in NF1(table 2).9293
In campomelic dysplasia (CMPD1), chro-mosome analysis has been performed in anumber of cases because of the frequent asso-ciation with 46,XY sex reversal (SRA1).94Four de novo reciprocal translocations and oneinversion, all involving 17q24-25, providecompelling evidence for the localisation ofboth CMPD1 and SRA1 to this region.9997Only a few viable deletions involving the distalpart of 1 7q have been reported.98'00 Thus,CMPD 1 may illustrate a disorder mapping to aregion where viable deletions do occur, butonly rarely. Although CMPD1/SRA1 has beensuggested to be a contiguous gene syn-drome,95 101 visible deletions have not beenreported in patients with CMPD 1/SRA 1.Thus, the observed pattern of chromosomerearrangements in CMPD 1 resembles the pat-tern in disorders mapping to regions wheredeletions do not occur at all.
Disorders associated with imprinting:Beckwith-Wiedemann syndromeGenetic imprinting of one or more loci withinlip15 has been implicated in the aetiology ofBeckwith-Wiedemann syndrome.'02 103 As inPrader-Willi syndrome,61104 several differenttypes of chromosome rearrangements havebeen encountered in BWS, including balancedrearrangements with breakpoints in the criticalregion of lip15, exclusively of maternal ori-gin, and duplications of the distal part ofIp 1 5, exclusively of paternal origin (table 2).It has been suggested that the duplicationslead to excess expression of a paternallyimprinted growth promoting gene within theregion, such as insulin growth factor 2 (IGF2),whereas the balanced translocations might af-fect a maternally imprinted regulator withinthe region.'03 Viable deletions involving thedistal part of l 1p5 have not been described,27so it is not likely that such deletions will beseen in association with BWS either.
X linked disordersMenkes disease illustrates an X linked disorderwhich maps to an R band region (Xql3.3)
where visible deletions have not been de-scribed in males.051'06 In a continuing cyto-genetic survey of more than 200 unrelatedmales with Menkes disease, not a single casewith a visible deletion has been detected.'07Although the proven X linked contiguous
gene syndromes map to those regions wherecytogenetic deletions are viable, X linked con-tiguous gene syndromes located within most Rband regions would be expected to be morenumerous, considering the high gene densityof R bands. However, these disorders willprobably be associated with either submicro-scopic rearrangements'08 or with 'balanced'rearrangements which will lead to limited lossof material. The same argument applies toautosomal contiguous gene syndromes map-ping to deletion non-viable regions.
So far, few mendelian disorders have beenassociated with visible duplications.'03 109 Ingeneral, duplications are better tolerated thandeletions,27 so a smaller part of the genome willbe duplication non-viable. However, it is rea-sonable to assume that for disorders associatedwith duplication of genetic material, the chro-mosomal localisation may also influence theoccurrence of visible chromosome mutations.
The effect of the parental origin of denovo chromosome rearrangementsDe novo chromosome rearrangements are pre-dominantly of paternal origin, including allX;autosome translocations examined sofar.95 110(116 This skewed parental origin hasseveral implications for the detection of struc-tural rearrangements in mendelian disorders.
DE NOVO REARRANGEMENTS OF THE XCHROMOSOMEAs most chromosome rearrangements arepaternal in origin, those involving the X mustoccur predominantly in females, where thephenotypic effect will be influenced by the Xinactivation pattern. In balanced X;autosometranslocations, where the translocation X is asa rule the active one,808' truncation of a diseasegene will lead to affected status in the femalecarrier. This mechanism is a main contributorto the disproportionately large number of Xlinked disorders where structural rearrange-ments have been described (figure). Since af-fected females with normal chromosomes areless likely to be reported, the actual frequencyof X;autosome translocations in affectedfemales is unknown. The best estimate maycome from Menkes disease (MNK), wherediagnosis, including that of females, has beencentralised to a few centres in the world. Sofar, two of six known MNK females are trans-location carriers (J Beck, personal communica-tion).'07117Males will only inherit an X;autosome
translocation if the translocation does not leadto gonadal dysgenesis, a frequent finding infemales with breakpoints on the X chromo-some.76 In addition, an associated mendeliandisorder in the mother will have to be suffi-
718
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Mendelian cytogenetics. Chromosome rearrangements associated with mendelian disorders
ciently mild to allow reproduction. As a conse-quence, X;autosome translocations are ingeneral rare in males.801'8 This, together withthe presumed male non-viability of deletionsinvolving the major part of the X chromosome(figure), led to the suggestion that intrachro-mosomal rearrangements, such as inversionsand shifts, will be likely types of cytogeneticrearrangements in males affected with most Xlinked disorders.'07 These rearrangements are
probably very rare.1"921
DISORDERS WHERE GENOMIC IMPRINTING ISINVOLVEDAs discussed previously, deletions involvingalmost the same region of 15qll-13 are fre-quently observed in both PWCR and ANCR.However, the deletion is always of paternalorigin in PWCR61'3 and always of maternalorigin in ANCR. 122 Although the proportion ofaffected subjects carrying a cytogeneticallyvisible deletion is the same in the two dis-orders, two significant aetiological factors sup-port a higher frequency of PWCR thanANCR: (1) the large excess of maternal non-
disjunction'23 that may predispose to subse-quent uniparental maternal disomy, as
observed in PWCR,'24 125 and (2) the presumedhigher frequency of de novo rearrangements(deletions) of paternal origin which will alsolead to PWCR.
In Beckwith-Wiedemann syndrome, allbalanced rearrangements involving the distalpart of lip 15 have been found to be inheritedfrom the mother, similar to a preponderance ofmaternal transmission of BWS in non-cyto-genetic familial cases.'03'26 Together with thepredominantly paternal origin of de novo re-
arrangements, this implies that few if any denovo balanced rearrangements will beobserved in subjects affected with BWS. Incontrast, the mother may frequently carry thebalanced rearrangement as a de novo re-
arrangement of paternal origin, or may haveinherited the rearrangement from her father.A similar sex dependent transmission pat-
tern might be possible in balanced rearrange-ments associated with ANCR69 and PWCR,6'l 64where the phenotypic effect of truncation or
deletion69 will be influenced by the parentalorigin of the inherited rearrangement.68 Thus,apparently balanced rearrangements in PWCRshould be of paternal origin,6' and of maternalorigin in ANCR.69
It has now become an almost routine pro-
cedure to search for the parental origin ofchromosome rearrangements. Owing to theexcess of de novo rearrangements of paternalorigin, demonstration of a maternal origin ofde novo rearrangements in a specific disorderwill be much more significant with respect to apossible involvement of genomic imprinting'22than demonstration of a paternal origin.95
Mutational aspects with relevance forpositional cloningARE BREAKPOINTS IN BALANCEDREARRANGEMENTS LOCUS SPECIFIC?Although the majority of reciprocal transloca-tions and inversions included in tables 1 and 2are balanced at the cytogenetic level, a few ofthese have been shown to be associated withlarge submicroscopic deletions. 127128 If thiswere a general feature, the assumption thatthese rearrangements involve single breakswithin the target locus would be erroneous.93However, of 23 apparently balanced re-arrangements studied at the gene level,129'38 22had breakpoints within the candidate genelocus (table 3). The assumed locus specificityof breakpoints in cytogenetically balanced re-arrangements in mendelian disorders thereforeseems justified, even though these rearrange-ments may not be truly conserved at the se-
quence level, since small deletions from a fewbp to < 30 kb have been noted (table 3).
LOCALISATION OF BREAKPOINTS OUTSIDE THESPECIFIC TARGET
Six unrelated reciprocal translocations havebeen reported in retinoblastoma patients,4'along with 14 specific reciprocal and eightinsertional translocations. The odds thereforeseem to favour a rearrangement as being dis-ease specific. However, they also illustrate thatthe coincidental occurrence of a rearrangementis not uncommon. Further studies of thefamily, linkage studies in other families, searchfor similar published reports, and comparisonwith the clinical features associated with dele-tions or duplications of the regions involvedare needed when considering the significanceof a detected rearrangement.Even if a structural chromosome mutation
turns out to be the aetiological factor, somemutational mechanisms have been documentedor suggested which may limit the utility ofboth balanced and unbalanced rearrangementsfor positional cloning, or at least provide
Table 3 Molecular details of assumed locus specific rearrangements.
Disorder No of studied No which truncate No with sequenced/ Size of(locus symbol) rearrangements the specific locus estimated deletion deletion
DMD 11 iis29132 2 71/72 bp1295 kb'132
GCPS 3 2166MNK 2 2138251252NFI 1 135RB1 4 4133 134 1 < 30 kb'34TCD 1 i136wS1 1 i 137
Total 23 22
719
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Tommerup
conflicting data as to the disease or locusspecificity.
Spreading of X inactivation in X;autosometranslocationsAlthough the majority of X;autosome translo-cations associated with mendelian disordershave involved the X linked locus, it would belogical to assume that the autosomal break-point would occasionally represent the target.Most of the documented cases have been X; 13translocations associated with RB1.41 139 At thecytogenetic level, 13q14 harbouring the RB1locus seemed to be intact in all cases. Thesuggested mechanism for the development ofRB1 in these cases is spreading of X inactiva-tion into the autosomal segment including theRB1 locus.'39 Inactivation of a putative locus at9q32-34 by spreading of X inactivation hasalso been suggested in two X;autosome trans-location carrying girls with incontinentia pig-menti or hypomelanosis of Ito.'"
The paradox of incontinentia pigmenti (IP1and IP2)At least seven, possibly eight,9 X chromosomerearrangements have been detected in sporadiccases of IP, with most of the breakpointswithin Xpl 1.141-147 IP is considered an X linkeddominant disorder, which is lethal in males,and which only occurs in females as a result ofthe functional mosaicism associated with ran-dom lyonisation. The paradoxes of IP are asfollows. (1) The locus for familial IP has beenassigned to Xq28 by linkage analysis and not toXp 11.148149 Therefore, two loci associated withIP (IP1 and IP2) have been invoked. (2) It hasbeen suggested that two, maybe three, of thetranslocation carriers'43 145 did not have IP buthypomelanosis of Ito (HI).'40150 HI has beenconsidered the 'negative' of IP because theabnormal hypopigmented skin areas are distri-buted in the same pattern. The disorder maybe a clinical manifestation of mosaicism orchimerism, as evidenced by the frequent asso-ciation with chromosomal mosaicism involv-ing a variety of different chromosomes. 50151 (3)Several different X chromosome breakpointshave been detected in the chromosomal re-arrangements associated with IP.'52-'54 Thedistance between two distinct regions of break-points within Xp 1, one close to the centro-mere and one more distal, is at least 2 5 Mb,'54suggesting that if IPI exists, the locus must beextremely large, or several loci within Xp 11may be involved. (4) Of two of the transloca-tions stated to be associated with HI, one mapsto the distal region and one to the proximalregion in Xpl l .'54
Considering the similar distribution of skindefects in IP and HI, the defect in thesesporadic cases with IP may also involve soma-tic mosaicism, perhaps associated with X inac-tivation. One of the rearrangements involved ar(X),'' so dynamic mosaicism associated withring chromosome instability might even beinvolved,'55 in which case the gene(s) respon-sible for the pigmentary abnormalities might
be situated anywhere on the X chromosome(for example, IP2 in Xq28). One implication ofthis would be that positional cloning of aputative IPl locus defined by X chromosomebreakpoints154 may be impossible.
Unmasking of mutations by rearrangementinduced non-random X inactivationIf the normal X chromosome contains amutated locus, non-random X inactivation of astructurally abnormal X chromosome may in-cidentally lead to clinically affected status of afemale.'56 The erroneous conclusion that thedisease locus is regionally defined by thebreakpoints of the rearrangement may beavoided by careful X inactivation studies. Thepossibility exists that this mechanism may beinvolved in IPL. It is uncertain whether asimilar mechanism might be involved in twoX;autosome translocations with differentbreakpoints on Xp in Rett syndrome,'57 158 adisorder in which X linkage has been sug-gested by almost exclusive involvement ofgirls, but where linkage analysis seems to haveexcluded the X chromosome.'59
Localisation of breakpoints close to but outsidethe open reading frameThe locus for Greig cephalopolysyndactyly(GCPS) has been pinpointed to 7p13 by threebalanced familial translocations, 6'1'62 by dele-tions,'63164 and by linkage studies.'65 By thecandidate gene approach,7 two of the threefamilial translocations were found to interrupta zinc finger gene GLI3 located within 7p 13.166However, the breakpoint in the third translo-cation occurred about 10 kb downstream of the3' end of GLI3. It was speculated that as aresult a cis acting element was brought into theregion of GLI3, thereby deregulating itsexpression. 166
Dynamic mosaicism associated with ringchromosomesCarriers of ring chromosomes harbouring tu-mour suppressor genes may be at increasedrisk of developing chromosome specific typesof tumours, for example, r(l 3) carriers maydevelop RB 1, r( 11) carriers WT 1, r(22) car-riers meningioma, etc.'55 Conversely, the de-velopment of a specific type of tumour in a ringcarrier may suggest that a tumour suppressorlocus is located somewhere on that chromosome.Apart from the primary deletion associatedwith the formation of the ring, ring chromo-somes are predisposed to secondary somaticrearrangements initiated by sister chromatidexchanges. The result may be fragmentation,gain or loss of ring material, including com-plete monosomy (dynamic mosaicism). Acomparison between the localisation of theprimary breakpoints and the likely tumoursuppressor loci involved suggests that thesecondary instability may be the most import-ant factor predisposing to the development oftumours.'55 Thus, unlike conventional consti-tutional deletions which can be used for the
720
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Mendelian cytogenetics. Chromosome rearrangements associated with mendelian disorders
generation of disease related deletion maps,correlations between the primary ring associ-ated deletions and phenotypic features shouldbe regarded with caution.Dynamic mosaicism may not be limited to
the development of tumours, but should alsobe considered as a possible mechanism inthe development of other disorders in ringcarriers. One possible association is Russell-Silver syndrome which shares many clinicalfeatures with ring chromosome 15 deficien-cies.'67
ConclusionsThe present review has primarily been con-cerned with those rearrangements which canbe expected to be encountered in a majority ofmendelian disorders. Thus, the fragile site atXq27 associated with the most common formof X linked mental retardation has not beendiscussed since it is so far the only fragile siteknown to be associated with a specific clinicalentity.Although deletions occur less frequently
than reciprocal translocations in newbornscreening series,33 any deletion of visible sizewill have a big chance of involving part or all ofa gene. This may explain why viable deletionsare the most frequent type of cytogenetic mu-tation in mendelian disorders. In contrast, asingle breakpoint or a submicroscopic deletionassociated with a translocation or inversion hasto be more precisely located in order to involvea specific locus.The majority of visible deletions associated
with mendelian disorders has been observed insporadic cases (tables 1 and 2). A few excep-tions have been reported, which may beexplained by the presence of mosaicism in aparental carrier, or a less severe phenotypeassociated with small deletions within certainregions, such as 13q14 associated with RB1.4In most other situations, the assumption thatchromosomal deletions are reproductive lethalmutations is probably true. However, familialoccurrence of deletions associated with men-delian disorders can be expected in two con-ditions: deletions involving the male deletionviable regions of the X chromosome, and fami-lial translocations, especially insertional trans-locations.4' 54 168172Apart from insertional translocations, other
rare types of familial and sporadic rearrange-ments have been identified in association withmendelian disorders, in part during chromo-somal surveys.9' 106 As mentioned previously,intrachromosomal rearrangements, includingshifts, may be the expected type of chromo-some mutation in males affected with themajority of X linked diseases.'07 Whether thisapparent accumulation of otherwise rare typesof rearrangement may reflect ascertainmentswhich are different from those usually encoun-tered in cytogenetics (prenatal diagnosis,MCA/MR, spontaneous abortions, etc) is atpresent unknown.Without valid data derived from systematic
cytogenetic surveys in the majority of dis-orders, the best estimate of a basic frequency
of chromosome rearrangements in an auto-somal dominant disorder is approximately 1 %,corresponding to the frequency of balancedtranslocations and inversions observed in RB1(and maybe in PWCR and ANCR). If, inaddition, visible deletions within the specificchromosome region are viable, this figure willbe considerably higher.The data favour that cytogenetic rearrange-
ments will be present in a small, but notinsignificant, fraction of subjects affected withmany mapped and unmapped mendelian dis-orders. The detection of a chromosome muta-tion will have obvious counselling implicationsin the individual family. Considering theimpact even a single specific rearrangementmay have for gene mapping and cloning, amore systematic effort to detect these re-arrangements should be pursued. In terms ofvalue for rapid molecular isolation of the locusof interest, rearrangements involving locusspecific breaks (for example, balanced translo-cations and inversions) will in general be themost valuable ones. Although the presence ofadditional congenital anomalies, other unex-pected diseases, spontaneous abortions, still-births, etc, may suggest the involvement of achromosome mutation in a patient or within afamily, subjects with balanced rearrangementsmay not suffer from additional disorders.'07Furthermore, translocations and inversionsmay be both familial and de novo mutations(tables 1 and 2). Therefore, some of the mostvaluable mutations in terms of positional clon-ing may only be detected by systematic analy-SiS.
If a reciprocal translocation is detected in adisorder that has not been mapped previously,the odds will favour a breakpoint within an Rband being the specific one. In some cases thismay ease subsequent attempts to confirm thespecificity of new translocations, for example,by linkage mapping. Furthermore, for largescale screening programmes, high resolutionchromosome analysis may be too cumbersomeand time consuming. Screening strategies canbe devised which in part will alleviate this. Indisorders with a known chromosomal localisa-tion, complete karyotyping by high resolutiontechnique may not be needed. In disordersmapping to regions where deletions are un-likely to be viable, normal good quality meta-phase technique may be sufficient to detect thesingle break rearrangements that can beexpected. In addition, the deletion map shownin the figure may provide a basis for tentativeexclusion mapping of mainly autosomal dom-inant disorders, where repeated chromosomeanalysis has failed to identify rearrangements.Such disorders might be expected to mapwithin the deletion non-viable or less viablepart of the genome. This was the case with twoof the most recently mapped disorders,R5T58587 and CMPD1 95Linkage mapping will be greatly eased by
the rapidly increasing numbers of highly poly-morphic microsatellites which can be analysedby the PCR technique. 173 In this context acontinuous registration and clinical follow upof subjects with known chromosome re-
721
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Tommerup
arrangements will become increasingly im-
portant. Whenever a disease has been mappedto a specific chromosome region, rapid rein-
vestigation of subjects carrying chromosomerearrangements within that region for keyclinical features may provide essential map-
ping and clinical data. This approach was usedsuccessfully to detectchoroideraemia 174 in a
patient with a previously reported Xq21 dele-tion, 175 and to show reduced nerve conduc-
tance velocity in a patient with a large visibleduplication encompassing the CMTIA locuson 17p.i10The rapid construction of complete YAC
and cosmid contigs176177 Will greatly facilitate
future mapping and isolation of specific dis-ease breakpoints/genes, for example, in com-
bination with in situ hybridisation techniques.The detection of rearrangements associatedwith mendelian diseases will therefore remainan important challenge for the clinical cyto-
geneticist. Many cytogenetic laboratories may
be discouraged from systematic studies by the
rarity of mendelian disorders and by the
expectation of a relatively low frequency ofassociated cytogenetic rearrangements. As hasbeen shown so convincingly in other fields ofhuman genome mapping, concerted actionwould be the logical way to ensure a systematicdetection of these highly valuable mutations inman.
This study was supported by the DanishCancer Society (89-059, 90-021), the Norwe-
gian Cancer Society, the Danish Medical Re-search Council (12-9292, 12-9744, 12-7414,5.17-.4.2.53), The Foundation of 1870, andthe Danish Biotechnology Research and De-velopment Programme 1991-95 (5.18.03).
1 Greenstein RM, Reardon MP, Chan TS. An X-autosometranslocation in a girl with Duchenne muscular dys-
trophy (DMD): evidence for DMD gene location.Pediatr Res 1977;11:457.
2 Verellen C, Markovic V, DeMeyer R, et al. Expression ofan X-linked recessive disease in a female due to non-
random inactivation of the X chromosome. Am HumGenet 1978;30:97A.
3 Canki CT, Dutrillaux B, TivadarI. Dystrophie muscu-
laire de Duchenne chez une petite fille porteuse d'unetranslocation t(X;3)(p2I;ql3) de novo. Ann Genet(Paris) 1979;22:35-9.
4 Lindenbaum RH, Clarke G, Patel C, et al. Musculardystrophy in an X;1 translocation female suggests that
Duchenne locus is on X chromosome short arm. MedGenet 1979;16:389-92.
5 Jacobs PA, Hunt PA, Mayer M, Bart RD. Duchennemuscular dystrophy (DMD) in a female with an X/autosome translocation: further evidence that the DMDlocus is at Xp2l. Am Hum Genet 1981;33:513-18.
6 Frezal J, Schinzel A. Report of the committee on clinicaldisorders and chromosomal deletion syndromes(HGMI 1). Cytogenet Cell Genet 1991;58:986-1052.
7 Collins FS. Positional cloning: let's not call it reverse
anymore. Nature Genet 1992;1:3-6.8 Edwards JH. Chromosomal abnormalities in mendelian
disorders. Lancet 1982;i:322-3.
9 McKusick VA. Mendelian inheritance in man. Catalogs ofautosomal dominant, autosomal recessive, and X-linkedphenotypes. 10th ed. Baltimore: Johns Hopkins Univer-sity Press, 1992.
10 Stratton R, Dobyns WB, Airhart SD, Ledbetter DH. Newchromosomal syndrome: Miller-Dieker syndrome andmonosomy l7pI3. Hum Genet 1984;67:193-200.
11 Greenberg F, Stratton RF, Lockhart LH, et al. FamilialMiller-Dieker syndrome associated with pericentricinversion of chromosome 17. Am Med Genet1 986;23:853-9.
12 Kuwano A, Ledbetter SA, Dobyns WB, Emanuel BS,
Ledbetter DH. Detection of deletions and cryptic trans-
locations in Miller-Dieker syndrome by in situ hybridi-zation. Am 7Hum Genet 1991;49:707-14.
13 Schmickel RD. Contiguous gene syndromes: a componentof recognizable syndromes. Pediatr 1986;109:231-41.
14 Emanuel BS. Molecular cytogenetics: toward dissection ofthe contiguous gene syndromes. Am Hum Genet1988;43:575-8.
15 Rose EA, Glaser T, Jones C, et al. Complete physical mapof the WAGR region oflip13 localizes a candidateWilms' tumor gene. Cell 1990;60:405-8.
16 Call KM, Glaser T, Ito CY, et al. Isolation and characteri-zation of a zinc finger polypeptide gene at the humanchromosome11 Wilms' tumor locus. Cell1990,60:509-20.
17 Gessler M, Poustka A, Cavenee W, et al. Homozygousdeletion in Wilms' tumours of a zinc-finger gene identi-fied by chromosome jumping. Nature 1990;343:774-8.
18 Gessler M, Simola KOJ, Bruns GAP. Cloning of break-points of a chromosome translocation identifies the AN2locus. Science 1989;244:1575-8.
19 Ton CCT, Hirvonen H, Miwa H, et al. Positional cloningand characterization of a paired box- and homeobox-containing gene from the aniridia region. Cell1991;67:1059-74.
20 Haber DA, Buckler AJ, Glaser T, et al. An internaldeletion within anlIp 13 zinc finger gene contributes tothe development of Wilms' tumor. Cell 1990;61:1257-69.
21 Pelletier J, Bruening W, LiFP, et al. WT1 mutationscontribute to abnormal genital system development andhereditary Wilms' tumour. Nature 1991,353:431-4.
22 Pelletier J, Bruening W, Kashtan CE, et al. Germlinemutations in the Wilms' tumor suppressor gene areassociated with abnormal urogenital development inDenys-Drash syndrome. Cell 1991;67:437-47.
23 Bruening W, Bardeesy N, Silverman BL, et al. Germlineintronic and exonic mutations in the Wilms' tumour gene(WT1) affecting urogenital development. Nature Genet1992;1:144-8.
24 Jordan T, Hanson I, Zaletayev D, et al. The human PAX6gene is mutated in two patients with aniridia. NatureGenet 1992,1:328-32.
25 Ledbetter SA, Kuwano A, Dobyns WB, Ledbetter DH.Microdeletions of chromosome l7pl3 as a cause of iso-lated lissencephaly. Am ] Hum Genet 1992;50: 182-9.
26 Dobyns WB, Elias ER, Newlin AC, Pagon RA, LedbetterDH. Causal heterogeneity in isolated lissencephaly.Neurology 1992;42:1375-88.
27 Schinzel A. Catalogue of unbalanced chromosomal aberra-tions in man. Berlin: Walter deGruyter, 1984.
28 Smith ACM, McGavran L, Robinson J, et al. Interstitialdeletion of(1 7)(pl1l.2p 11.2) in nine patients. Am ] MedGenet 1986;24:393-414.
29 McKusick VA, Amberger JS. The morbid anatomy of thehuman genome: chromosomal location of mutationscausing disease. ] Med Genet 1993,30:1-26.
30 Naritomi K, Hyakuna N, Suzuki Y, Orii T, Hirayama K.Zellweger syndrome and a microdeletion of the proximallong arm of chromosome 7. Hum Genet 1988;80:201-2.
31 Naritomi K, Izumikawa Y, OhshiroS, et al. Gene assign-ment of Zellweger syndrome to 7qll.23: report of thesecond case associated with a pericentric inversion ofchromosome 7. Hum Genet 1989,84:79-80.
32 Buhler EM. Unmasking of heterozygosity by inheritedbalanced translocations. Implications for prenatal dia-gnosis and gene mapping. Ann Genet (Paris)1983;26: 133-7.
33 Hook EB, Hamerton JL.The frequency of chromosomeabnormalities detected in consecutive newborn studies-differences between studies-results by sex and by sever-ity of phenotypic involvement. In: Hook EB, Porter IH,eds. Population cytogenetics. New York: Academic Press,1977: 81-97.
34 Searle AG. Chromosomal variants. In: Lyon MF, SearleAG, eds. Genetic variants and strains of the laboratorymouse. 2nd ed. Oxford: Oxford University Press,1989:582-6 16.
35 Pentao L, Lewis RA, Ledbetter DH, Patel PI, Lupski JR.Maternal uniparental isodisomy of chromosome 14: asso-ciation with autosomal recessive rod monochromacy. Am7 Hum Genet 1992;50:690-9.
36 Fannemel M, Riise R, Lofterod B, Tommerup N. High-resolution chromosome analysis in autosomal recessivedisorders. Laurence-Moon-Bardet-Biedt syndrome. ClinGenet 1993;43:111-12.
37 Cremers FPM, van de Pol TJR, Wierenga B, et al.Molecular analysis of male-viable deletions and duplica-tions allows ordering of 52 DNA probes on proximal Xq.Am Hum Genet 1988,43:452-61.
38 Lele KP, Penrose LS, Stallard HB. Chromosome deletionin a case of retinoblastoma. Ann Hum Genet 1963;27:171-4.
39 Wilson MG, Melnyk J, Towner JWJ. Retinoblastoma anddeletion D(14) syndrome. ] Med Genet 1969;6:322-7.
40 Taylor Al. Dq-, Dr and retinoblastoma. Humangenetik1970;10:209-17.
41 Munier F, Pescia G, Jotterand-Bellomo M, et al. Consti-tutional karyotype in retinoblastoma. Case report andreview of literature. Ophthalmic Paediatr Genet1989;10: 129-50.
42 Cowell JK, Hungerford J, Rutland P, Jay M. Genetic andcytogenetic analysis of patients showing reduced ester-ase-D levels and mental retardation from a survey of 500individuals with retinoblastoma. Ophthalmic Paediatr
Genet 1989;10:117-27.43 Bunin GR, Emanuel BS, Meadows AT, et al. Frequency
of 13q abnormalities among 203 patients with retinoblas-toma. ] Natl Cancer Inst 1989;81:370-4.
44 Lemieux N, Richer CL. Chromosome evolution and high-resolution analysis of leucocytes, bone marrow, andtumor cells of retinoblastoma patients. Am 7 Med Genet1 990;36:456-62.
45 Miller RW, Fraumeni JF Jr, Manning MD. Association of
722
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Mendelian cytogenetics. Chromosome rearrangements associated with mendelian disorders
Wilms's tumor with aniridia, hemihypertrophy, andother congenital malformations. N Engl Med1964;270:922-7.
46 Pendergrass TW. Congenital anomalies in children withWilms' tumor. A new survey. Cancer 1976;37:403-9.
47 Shannon RS, Mann JR, Harper E, et al. Wilms's tumourand aniridia: clinical and cytogenetic features. Arch DisChild 1982;57:685-90.
48 Fraumeni JF Jr, Glass AG. Wilms's tumor and congenitalaniridia. JAMA 1968;206:825-8.
49 Nakagome Y, Ise T, Sakurai M, et al. High-resolutionstudies in patients with aniridia-Wilms tumor associ-ation, Wilms tumor or related congenital abnormalities.Hum Genet 1984;67:245-8.
50 Hotta Y, Fujiki K, Ishida N, et al. High resolution G-banding analysis in aniridia. Ophthalmic Paediatr Genet1987;8: 145-50.
51 Lyons LA, Martha A, Mintz-Hittner HA, et al. Resolu-tion of the two loci for autosomal dominant aniridia, AN I
and AN2, to a single locus on chromosome llp13.Genomics 1992;13:925-30.
52 Turleau C, de Grouchy J, Tournade MF, GagnadouxMF, Junien C. Del 1 lp/aniridia complex: report of threepatients and review of 37 observations from the litera-ture. Clin Genet 1984;26:356-62.
53 Turleau C, de Grouchy J, Nihoul-Fekete C, et al.Dell 1pl3/nephroblastoma without aniridia. Hum Genet1984;67:455-6.
54 Niikawa N, Fukushima Y, Taniguchi N, Iizuka S, Kajii T.Chromosome abnormalities involving llpl3 and lowerythrocyte catalase activity. Hum Genet 1982;60:373-5.
55 Fantes JA, Bickmore WA, Fletcher JM, Ballesta F, Han-son M, van Heyningen V. Submicroscopic deletions atthe WAGR locus, revealed by nonradioactive in situhybridization. Am Hum Genet 1992;51:1286-94.
56 Riccardi VM, Hittner HM, Strong LC, et al. Wilms tumorwith aniridia/iris dysplasia and apparently normal chro-mosomes. _J Pediatr 1982;100:574-7.
57 Porteous DJ, Bickmore W, Christie S, et al. HRAS1-selected chromosome transfer generates markers thatcolocalize aniridia- and genitourinary dysplasia-associ-ated translocation breakpoints and the Wilms' tumorgene within llpl3. Proc Natl Acad Sci USA1987;84:5355-9.
58 Moore JW, Hyman S, Antonarakis SE, Mules EH,Thomas GH. Familial isolated aniridia associated with a
translocation involving chromosome 11 and 22[t(I 1;22)(pl 3;q12.2)]. Hum Genet 1986;72:297-302.
59 Pettenati MJ, Weaver RG, Burton BK. Translocationt(5;1 1)(q13.1;p13) associated with familial isolated aniri-dia. Am Med Genet 1989;34:230-2.
60 Simola KOJ, Knuutila S, Kaitila I, Pirkola A, Pohja P.Familial aniridia and translocation t(4;1 1)(q22;pl3)without Wilms' tumor. Hum Genet 1983;63:158-61.
61 Butler MG. Prader-Willi syndrome: current understand-ing of cause and diagnosis. AmJ Med Genet 1990;35:319-32.
62 Robinson WP, Bottani A, Yagang X, et al. Molecular,cytogenetic, and clinical investigations of Prader-Willisyndrome patients. Am Hum Genet 1991;49:1219-34.
63 Hamabe J, Fukushima Y, Harada N, et al. Molecularstudy of the Prader-Willi syndrome: deletion, RFLP,and phenotype analyses in 50 patients. Am _J Med Genet1991;41:54-63.
64 Winsor EJT, Welch JP. Prader-Willi syndrome associatedwith inversion of chromosome 15. Clin Genet1983;24:456-61.
65 Fryns JP, Kleczkowska A, Decock P, Van den Berghe H.Angelman's syndrome and 15qll-13 deletions. J7 MedGenet 1989;26:538-40.
66 Hamabe J, Kuroki Y, Imaizumi K, et al. DNA deletionand its parental origin in Angelman syndrome patients.Am Med Genet 1991;41:64-8.
67 Imaizumi K, Takada F, Kuroki Y, et al. Cytogenetic andmolecular study of Angelman syndrome. Am MedGenet 1990;35:314-18.
68 Pembrey M, Fennell SJ, Van den Berghe J, et al. Theassociation of Angelman's syndrome with deletionswithin 15qll-13. Med Genet 1989;26:73-7.
69 Webb T, Clayton-Smith J, Cheng XJ, et al. Angelmansyndrome with a chromosomal inversion 15 inv(pl 1q13)accompanied by a deletion in 15ql 1q13. Med Genet1992;29:921-4.
70 Ballabio A, Andria G. Deletions and translocations involv-ing the distal short arm of the human X chromosome.Review and hypotheses. Hum Mol Genet 1992;1:221-7.
71 Matsumoto T, Kondoh, Yoshimoto M, et al. Complexglycerol kinase deficiency: molecular-genetic, cytogene-
tic, and clinical studies of five Japanese patients. AmMed Genet 1988;31:603-16.
72 McCabe ERB, Towbin JA, van den Engh G, Trask BJ.Xp2l contiguous gene syndromes: deletion quantitationwith bivariate flow karyotyping allows mapping ofpatient breakpoints. Am Hum Genet 1992;51:1277-85.
73 Wyandt HE, Grierson HL, Sanger WG, et al. Chromo-some deletion of Xq25 in an individual with X-linkedlymphoproliferative disease. Am J Med Genet1989;33:426-30.
74 Yang HM, Lund T, Niebuhr E, et al. Exclusion mappingof 12 X-linked disease loci and 10 DNA probes from thelong arm of the X-chromosome. Clin Genet 1990;38:94-104.
75 Thomas NST, Ray PN, Worton RG, Harper PS. Molecu-lar deletion analysis in Duchenne muscular dystrophy.Med Genet 1986;23:509-15.
76 Therman E, Susman B. The similarity of phenotypiceffects caused by Xp and Xq deletions in the humanfemale: a hypothesis. Hum Genet 1990;85:175-83.
77 Schmidt M, Certoma A, Du Sart D, et al. Unusual Xchromosome inactivation in a mentally retarded girl withan interstitial deletion Xq27: implications for the fragileX syndrome. Hum Genet 1990;84:347-52.
78 Schmidt M. Do sequences in Xq27.3 play a role in Xinactivation? Am J Med Genet 1992;43:487-91.
79 Daniel A, Hook EB, Wulf G. Collaborative USA data onprenatal diagnosis for parental carriers of chromosomerearrangements: risks of unbalanced progeny. In: Thecytogenetics of mammalian autosomal rearrangements. NewYork: Alan R Liss, 1988:73-162.
80 Mattei MG, Mattei JF, Ayme S, Giraud F. X-autosometranslocation: cytogenetic characteristics and their conse-quences. Hum Genet 1982;61:295-309.
81 Schmidt M, Du Sart D. Functional disomies of the Xchromosome influence the cell selection and hence the Xinactivation pattern in females with balanced X-auto-some translocations: a review of 122 cases. Am J MedGenet 1992;42:161-9.
82 Korenberg JR, Rykowski MC. Human genome organiza-tion: Alu, Lines, and the molecular structure of meta-phase chromosome bands. Cell 1988;53:391-400.
83 Holmquist GP. Chromosome bands, their chromatin fla-vors, and their functional features. Am Jf Hum Genet1992;51:17-37.
84 Imaizumi K, Kuroki Y. Rubinstein-Taybi syndrome withde novo reciprocal translocation t(2;l6)(pl3.3;pl3.3).Am Jf Med Genet 1991;38:636-9.
85 Tommerup N, van der Hagen CB, Heiberg A. Tentativeassignment of a locus for Rubinstein-Taybi syndrome to16pl3.3 by a de novo reciprocal translocation,t(7;16)(q34;p13.3). Am J Med Genet 1992;44:237-41.
86 Lacombe D, Saura R, Taine L, Battin J. Confirmation ofassignment of a locus for Rubinstein-Taybi syndrome to16pl3.3. AmJMed Genet 1992;44:126-8.
87 Breuning MH, Dauwerse HG, Fugazza G, et al. Rubin-stein-Taybi syndrome caused by submicroscopic dele-tions within 16p13.3. Am J Hum Genet 1993;52:249-54.
88 Wilkie AO, Buckle VJ, Harris PC, et al. Clinical featuresand molecular analysis of the alpha thalassemia/mentalretardation syndromes. I. Cases due to deletions involv-ing chromosome band 16p13.3. Am J Hum Genet1990;46:1 112-26.
89 Weinberg RA. Tumor suppressor genes. Science1991;254:1 138-46.
90 Kayes LM, Riccardi VM, Burke W, Bennett RL,Stephens K. Large de novo deletion in a patient withsporadic neurofibromatosis 1, mental retardation, anddysmorphism. J Med Genet 1992;29:686-90.
91 Andersen LB, Tommerup N, Koch J. Formation of amini-chromosome by excision of the proximal region of17q in a patient with von Recklinghausen neurofibroma-tosis. Cytogenet Cell Genet 1990;53:206-10.
92 Schmidt MA, Michels VV, Deward W. Cases of neuro-fibromatosis with rearrangements of chromosome 17involving band 17ql 1.2. Amj Med Genet 1987;28:771-7.
93 Ledbetter DH, Rich DC, O'Connell P, Leppert M, CareyJC. Precise localisation of NFl to 17qll.2 by balancedtranslocation. Am J Hum Genet 1989;44:20-4.
94 Houston CS, Opitz JM, Spranger JW, et al. The campo-melic syndrome: review, report of 17 cases, and follow-up on the currently 17-year-old boy first reported byMaroteaux et al in 1971. Am J Med Genet 1983;15:3-28.
95 Tommerup N, Schempp W, Meinecke P, et al. Assign-ment of an autosomal sex reversal locus (SRA1) andcampomelic dysplasia (CMPD1) to 17q24.3-q25.1.Nature Genet 1993;4:170-4.
96 Maraia R, Saal HM, Wangsa D. A chromosome 17q denovo paracentric inversion in a patient with campomelicdysplasia; case report and etiologic hypothesis. ClinGenet 1991;39:401-8.
97 Young ID, Zuccollo JM, Maltby EL, Broderick NJ.Campomelic dysplasia associated with a de novo 2q;17qreciprocal translocation. J Med Genet 1992;29:251-2.
98 Bridge J, Sanger W, Mosher G, et al. Partial deletion ofdistal 17q. Am J Med Genet 1985;21:225-9.
99 Giannotti A, Alessandri A, Reale A, Digilio MC, ValoraniMG. Partial deletion of the long arm of chromosome 17.Clinical case. Minerva Pediatr 1992;44:51-4.
100 Luke S, Bennett HS, Pitter JH, Verma RS. A new case ofmonosomy for 17q25-qter due to a maternal transloca-tion [t(3;17)(pl2;q24)]. Ann Genet (Paris) 1992;35:48-50.
101 Ebensperger C, Jager RJ, Lattermann U, et al. No evid-ence of mutations in four candidate genes for male sexdetermination/differentiation in sex-reversed XY femaleswith campomelic dysplasia. Ann Genet (Paris)1991;34:233-8.
102 Henry I, Bonaiti-Pellie C, Junien C. Uniparental paternaldisomy in a genetic cancer-predisposing syndrome.Nature 1991;351:665-7. _
103 Mannens M, Hoovers JMN, Redeker B, et al. Parentalimprinting of human chromosome region llpl5.3-pterinvolved in the Beckwith-Wiedemann syndrome andvarious human neoplasia. Eur J Hum Genet (submitted).
104 Nicholls RD, Knoll JHM, Butler MG, Karam S, LalandeM. Genetic imprinting suggested by maternal heterodis-omy in non-deletion Prader-Willi syndrome. Nature1989;342:281-5.
105 Verga V, Hall BK, Wang S, et al. Localization of thetranslocation breakpoint in a female with Menkes syn-
723
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Tommerup
drome to Xql3.2-q13.3 proximal to PGK-1. AmJHumGenet 1991;48:1133-8.
106 Tumer Z, Tommerup N, T0nnesen T, et al. Mapping ofthe Menkes locus to Xql3.3 distal to the X-inactivationcenter by an intrachromosomal insertion of the segmentXql3.3-q21.2. Hum Genet 1992;88:668-72.
107 Tommerup N, Tumer Z, Tonnesen T, Horn N. A cyto-genetic survey in Menkes disease. Implications for thedetection of chromosomal rearrangements in X linkeddisorders. Med Genet 1993;30:314-15.
108 Collins FA, Murphy DL, Reiss AL, et al. Clinical, bio-chemical, and neuropsychiatric evaluation of a patientwith a contiguous gene syndrome due to a microdeletionXpll.3 including the Norrie disease locus and mono-amine oxidase (MAOA and MAOB) genes. Am MedGenet 1992;42:127-34.
109 Lupski JR, Wise CA, Kuwano A, et al. Gene dosage is a
mechanism for Charcot-Marie-Tooth disease type IA.Nature Genet 1992;1:29-33.
110 Chamberlin J, Magenis RE. Parental origin of de novochromosome rearrangements. Hum Genet 1980;53:343-7.
111 Chandley AC. On the parental origin of de novo mutationin man. Med Genet 1991;28:217-23.
112 Ejima Y, Sasaki MS, Kaneko A, Tanooka H. Types, rates,origin and expressivity of chromosome mutations involv-ing 13q14 in retinoblastoma patients. Hum Genet1988;79:1 18-23.
113 Kean VM, MacLeod HL, Thompson MW, et al. Paternalinheritance of translocation chromosomes in a t(X;21)patient with X linked muscular dystrophy. Med Genet1986;23:491-3.
114 Bodrug SE, Roberson JR, Weiss L, et al. Prenatal identifi-cation of a girl with a t(X;4)(p21;q35) translocation:molecular characterisation, paternal origin, and associ-ation with muscular dystrophy. Med Genet1 990;27:426-32.
115 Robinson D, Boyd Y, Collinson M, Jacobs P. Determi-nation of the parental origin of X;autosome transloca-tions by M27f3 methylation analysis. Med Genet1991;28:63-4.
116 Robinson DO, Boyd Y, Cockburn D, et al. The parentalorigin of de novo X-autosome translocations in femaleswith Duchenne muscular dystrophy revealed by M27fmethylation analysis. Genet Res Camb 1990;56:135-40.
117 Kapur S, Higgins JV, Delp K, Rogers B. Menkes syn-drome in a girl with X-autosome translocation. AmMed Genet 1987;26:503-10.
118 Bawle E, Tyrkus M, Lipman S, Bozimowski D. Aarskogsyndrome: full male and female expression associatedwith an X-autosome translocation. Am Med Genet1984;17:595-602.
119 Kaffe S, Hsu LYF. Chromosome inversions in a series of25.000 prenatal diagnoses: frequency and pregnancy out-come. Am Hum Genet 1990;47:A278(1097).
120 Groupe de Cytogeneticiens Francais. Pericentric inver-sions in man. A French collaborative study. Ann Genet(Paris) 1986;29: 129-68.
121 Groupe de Cytogeneticiens Francais. Paracentric inver-sions in man. A French collaborative study. Ann Genet(Paris) 1986;29:169-76.
122 Clayton-Smith J, Webb T, Pembrey ME, Nichols M,Malcolm S. Maternal origin of deletion 15qll-13 in25/25 cases of Angelman syndrome. Hum Genet1992;88:376-8.
123 Petersen MB, Frantzen M, Antonarakis SE, et al. Com-parative study of microsatellite and cytogenetic markersfor detecting the origin of the nondisjoined chromosome21 in Down syndrome. AmJrHum Genet 1992;51:516-25.
124 Purvis-Smith SG, Saville T, Manass S, et al. Uniparentaldisomy 15 resulting from correction of an initial trisomy15. Am 7 Hum Genet 1992;50:348-50.
125 Cassidy SB, Lai LW, Erickson RP, et al. Trisomy 15 withloss of paternal 15 as a cause of Prader-Willi syndromedue to maternal disomy. Am7Hum Genet 1992;51:701-8.
126 Norman AM, Read AP, Clayton-Smith J, Andrews T,Donnai D. Recurrent Wiedemann-Beckwith syndromewith inversion of chromosome (l1)(pll.2p15.5). AmMed Genet 1992;42:638-41.
127 Ludecke HJ, Johnson C, Wagner MJ, et al. Moleculardefinition of the shortest region of deletion overlap in theLanger-Giedion syndrome. Am Hum Genet1991;49:1 197-206.
128 Davis LM, Stallard R, Thomas GH, et al. Two anony-mous DNA segments distinguish the Wilms' tumor andaniridia locus. Science 1988;241:840-2.
129 Bodrug SE, Ray PN, Gonzalez IL, et al. Molecularanalysis of a constitutional X-autosome translocation in a
female with muscular dystrophy. Science 1987;237:1620-4.
130 Bodrug SE, Burghes AH, Ray PN, Worton RG. Mappingof four translocation breakpoints within the Duchennemuscular dystrophy gene. Genomics 1989;4:101-4.
131 Meitinger T, Boyd Y, Anand R, Craig I. Mapping ofXp2ltranslocation breakpoints in and around the DMD geneby pulsed field gel electrophoresis. Genomics 1988;3:315-22.
132 Giacalone JP, Francke U. Common sequence motifs at the
rearrangement sites of a constitutional X/autosome trans-
location and associated deletion. Am Hum Genet
1992;5O:725-41.133 Higgins MJ, Hansen MF, Cavenee WK, Lalande M.
Molecular detection of chromosomal translocations that
disrupts the putative retinoblastoma susceptibility locus.
Mol Cell Biol 1989;9:1-5.134 Mitchell CD, Cowell JK. Predisposition to retinoblastoma
due to a translocation within the 4.7R locus. Oncogene1989;4:253-7.
135 Viskochil D, Buchberg AM, Xu G, et al. Deletions and atranslocation interrupt a cloned gene at the neurofibro-matosis type 1 locus. Cell 1990;62:187-92.
136 Cremers FPM, van de pol DJR, van Kerkhoff LPM,Wieringa B, Ropers HH. Cloning of a gene that isrearranged in patients with choroideraemia. Nature1990;347:674-7.
137 Tsukamoto K, Tohma T, Ohta T, et al. Cloning andcharacterization of the inversion breakpoint at chromo-some 2q35 in a patient with Waardenburg syndrome typeI. Hum Mol Genet 1992;1:315-17.
138 Chelly J, Turmer Z, Tonnesen T, et al. Isolation of acandidate gene for Menkes disease that encodes for a
potential heavy metal binding protein. Nature Genet1993;3:14-19.
139 Stambolian D, Selleinger B, Derrington D, et al. Cytoge-netic and molecular investigation of a balanced Xql3qtranslocation in a patient with retinoblastoma. Am MedGenet 1992;42:771-6.
140 Happle R. Tentative assignment of hypomelanosis of Itoto 9q33-qter. Hum Genet 1987;75:98-9.
141 de Grouchy J, Turleau C, Doussau de Bazignan M,Maroteaux P, Thibaud D. Incontinentia pigmenti (IP)and r(X). Tentative mapping of the IP locus to the Xjuxtacentromeric region. Ann Genet (Paris) 1985;28:86-9.
142 Bernstein R, Dawson B, Kohl R, Jenkins T. X,15 translo-cation in a retarded girl: X inactivation pattern andattempt to localise the hexosaminidase A and other loci.Med Genet 1979;16:254-62.
143 Gilgenkrantz S, Tridon P, Pinel-Briquel N, Beurey J,Weber M. Translocation (X;9)(pl l;q34) in a girl withincontinentia pigmenti (IP): implications for the regionalassignment of the IP locus to Xpl 1? Ann Genet (Paris)1985;28:90-2.
144 Kajii T, Tsukahara M, Fukushima Y, et al. Translocation(X;13)(pl1.21;q12.3) in a girl with incontinentia pig-menti and bilateral retinoblastoma. Ann Genet (Paris)1985;28:219-23.
145 Hodgson SV, Neville B, Jones RWA, Fear C, Bobrow M.Two cases of X/autosome translocation in females withincontinentia pigmenti. Hum Genet 1985;71:231-4.
146 Cannizzaro LA, Hecht F. The gene for incontinentiapigmenti maps to band Xpll with an (X;10)(pl1;q22)translocation. Clin Genet 1987;32:66-9.
147 Bitoun P, Philippe C, Cherif M, Mulcahy MT, Gilgen-krantz S. Incontinentia pigmenti (type 1) and X;5-trans-location. Ann Genet (Paris) 1992;35:51-4.
148 Sefiani A, Abel L, Heuertz S, et al. The gene for inconti-nentia pigmenti is assigned to Xq28. Genomics1989;4:427-9.
149 Harris A, Lankester S, Haan E, et al. The gene forincontinentia pigmenti: failure of linkage studies usingDNA probes to confirm cytogenetic localization. ClinGenet 1988;34:1-6.
150 Moss C, Burn J. Genetic counselling in hypomelanosis ofIto: case report and review. Clin Genet 1988;34:109-15.
151 Flannery DB. Pigmentary dysplasias, hypomelanosis ofIto, and genetic mosaicism. Am Med Genet 1990;35:18-21.
152 Sefiani A, Heuertz S, Turleau C, et al. Incontinentiapigmenti: Xp breakpoint is not the same in a case of r(X)and in X/autosome translocations. Ann Genet (Paris)1989;32: 149-5 1.
153 Crolla JA, Gilgenkranz S, de Grouchy J, Kajii T, BobrowM. Incontinentia pigmenti and X-autosome transloca-tions. Non-isotopic in situ hybridization with an X-centromere specific probe (pSV2X5) reveals a possibleX-centromeric breakpoint in one of five published cases.Hum Genet 1989;81:269-72.
154 Gorski JL, Burright EN, Reyner EL, et al. Isolation ofDNA markers from a region between incontinentia pig-menti 1 (IPI) X-chromosomal translocation breakpointsby a comparative PCR analysis of a radiation hybridsubclone mapping panel. Genomics 1992;14:649-56.
155 Tommerup N, Lothe RA. Constitutional ring chromo-somes and tumour suppressor genes. Med Genet1992;29:879-82.
156 Nisen P, Stamberg J, Ehrenpreis R, et al. The molecularbasis of severe hemophilia B in a girl. N Engl Med
1986;315:1 139-42.157 Journel H, Melki J, Turleau C, Munnich A, de Grouchy J.
Rett phenotype with X/autosome translocation: possiblemapping to the short arm of chromosome X. Am MedGenet 1990;35:142-7.
158 Zoghbi HY, Ledbetter DH, Schultz R, Percy AK, GlazeDG. A de novo X;3 translocation in Rett syndrome. AmMed Genet 1990;35:148-51.
159 Ellison KA, Fill CP, Terwilliger J, et al. Examination of Xchromosome markers in Rett syndrome: exclusion map-ping with a novel variation on multilocus linkage analy-sis. Am Hum Genet 1992;50:278-87.
160 Tommerup N, Nielsen F. A familial reciprocal transloca-tion t(3;7)(p21.1;p13) associated with the Greig polysyn-dactyly-craniofacial dysmorphism syndrome. Am MedGenet 1983;16:313-21.
161 Kruger G, Gotz J, Kvist U, et al. Greig syndrome in a
large kindred due to reciprocal chromosome transloca-
tion t(6;7)(q27;pl3). Am Med Genet 1989;32:411-16.162 Vortkamp A, Thias U, Gessler M, et al. A somatic cell
hybrid panel and DNA probes for physical mapping of
human chromosome 7p. Genomics 1991;11:737-43.
163 Wagner K, Kroisel PM, Rosenkranz W. Molecular and
cytogenetic analysis in two patients with microdeletions
724
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Mendelian cytogenetics. Chromosome rearrangements associated with mendelian disorders
of 7p and Greig syndrome: hemizygosity for PGAM-2and TCRG genes. Genomics 1990;8:487-91.
164 Pettigrew AL, Greenberg F, Caskey CT, Ledbetter DH.Greig syndrome associated with an interstitial deletion of7p: confirmation of the localization of Greig syndrome to7pl3. Hum Genet 1991;87:452-6.
165 Brueton L, Huson SM, Winter RM, et al. Chromosomallocalization of a developmental gene in man: direct DNAanalysis demonstrates that Greig cephalopolysyndactylymaps to 7p13. Am J Med Genet 1988;31:799-804.
166 Vortkamp A, Gessler M, Grzeschik KH. GLI3 zinc-fingergene interrupted by translocations in Greig syndromefamilies. Nature 1991;352:539-40.
167 Wilson GN, Sauder SE, Bush M, Beitins IZ. Phenotypicdelineation of ring chromosome 15 and Russell-Silversyndromes. J Med Genet 1985;22:237-40.
168 Yunis JJ, Ramsay NKC. Familial occurrence of the aniri-dia-Wilms' tumor syndrome with deletion 1 lp13-14. 1. JPediatr 1980;96:1027-30.
169 Kousseff BG, Agatucci A. Aniridia-Wilms tumor associ-ation. J Pediatr 1981;98:676-7.
170 Nakagome Y, Nagahara N. High-resolution studies inpatients with aniridia-Wilms tumor association. HumGenet 1985;70:289.
171 Cross I, Delhanty J, Chapman P, et al. An intrachromoso-mal insertion causing 5q22 deletion and familial adeno-matous polyposis coli in two generations. J Med Genet1992;29:175-9.
172 Williamson RA, Donlan MA, Dolan CR, et al. Familialinsertional translocation of a portion of 3q into llqresulting in duplication and deletion of region 3q22. 1-q24in different offspring. Am J Med Genet 1981;9:105-1 1.
173 Weissenbach J, Gyapay G, Dib C, et al. A second genera-tion linkage map of the human genome. Nature1992;359:794-801.
174 Schwartz M, Rosenberg T, Niebuhr E, et al. Choroidere-mia: further evidence for assignment of the locus toXql3-Xq2l. Hum Genet 1986;74:449-52.
175 Tabor A, Andersen 0, Lundsteen C, Niebuhr E, Sarde-mann H. Interstitial deletion in the 'critical region' of thelong arm of the X chromosome in a mentally retardedboy and his normal mother. Hum Genet 1983;64:196-9.
176 Chumakov I, Rigault P, Guillou S, et al. Continuum ofoverlapping clones spanning the entire human chromo-some 21q. Nature 1992;359:380-7.
177 Foote S, Vollrath D, Hilton A, Page DC. The human Ychromosome: overlapping DNA clones spanning theeuchromatic region. Science 1992;258:60-6.
Appendix This appendix contains references not men-tioned in the text, listed alphabetically according to locus,including references to rearrangements included in tables 1and 2, and some selected key references. Locus specificcross references to the text are included.
AGS Alagille syndrome178 Anad F, Burn J, Matthews D, et al. Alagille syndrome and
deletion of 20p. J Med Genet 1990;27:729-37.9 Teebi AS, Krishna Murthy DS, Ismail EAR, Redha AA.
Alagille syndrome with de novo del(20)(pl.1.2). Am JMed Genet 1992;42:35-8.
AHC Adrenal hypoplasia, congenital72'80 Pillers DAM, Weleber RG, Powell BR, et al. Aland Island
eye disease (Forsius-Eriksson ocular albinism) and anXp2l deletion in a patient with Duchenne musculardystrophy, glycerol kinase deficiency, and congenitaladrenal hypoplasia. Am J Med Genet 1990;36:23-8.
AIC Aicardi syndrome70181 Naritomi K, Izumikawa Y, Nagataki S, et al. Combined
Goltz and Aicardi syndromes in a terminal Xp deletion:are they a contiguous gene syndrome? Am J Med Genet1992;43:839-43.
182 Ropers HH, Zuffardi 0, Bianchi E, Tiepolo L. Agenesis ofcorpus callosum, ocular, and skeletal anomalies (X-linked dominant Aicardi's syndrome) in a girl withbalanced X/3 translocation. Hum Genet 1982;61:364-8.
AIED Aland island eye disease'80ANCR Angelman syndrome (happy puppet)65"-22183 Williams CA, Zori RT, Stone JW, et al. Maternal origin of
15qll-13 deletions in Angelman syndrome suggests arole for genomic imprinting. Am J Med Genet1990;35:350-3.
AN2 Aniridia 2'5 182445- 60128 16870ANK1 Spherocytosis type II (ankyrin defect)'84 Kimberling WJ, Fulbeck T, Dixon L, Lubs HA. Localiza-
tion of spherocytosis to chromosome 8 or 12 and report ofa family with spherocytosis and a reciprocal transloca-tion. AmJ Hum Genet 1975;27:586-94.
185 Bass EB, Smith SW Jr, Stevenson RE, Rosse WF. Furtherevidence for location of the spherocytosis gene on chro-mosome 8. Ann Intern Med 1983;99:192-3.
Chilcote RR, le Beau MM, Dampier C, et al. Association ofred cell spherocytosis with deletion of the short arm ofchromosome 8. Blood 1987;69:156-9.
187 Kitatani M, Chiyo M, Oxaki M, Shike S, Miwa S. Localiza-tion of the spherocytosis gene to chromosome segment8plI.22-8p21. Hum Genet 1988;78:94-5.
'8 Lux SE, Tse WT, Menninger JC, et al. Hereditary sphero-cytosis associated with deletion of human erythrocyteankyrin gene on chromosome 8. Nature 1990;345:736-9.
APC Adenomatous polyposis coli, incl Gardner syn-drome'7'
189 Herrera L, Kakati S, Gibas L, Pietrzak E, Sandberg AA.Gardner syndrome in a man with an interstitial deletionof 5q. Am J Med Genet 1986;25:473-6.
'9 Hockey KA, Mulcahy MT, Montgomery P, Levitt S.Deletion of chromosome 5q and familial adenomatouspolyposis. J Med Genet 1989;26:61-2.
191 Kobayashi T, Narahara K, Yokoyama Y, et al. Gardnersyndrome in a boy with interstitial deletion of the longarm of chromosome 5. Am Jf Med Genet 1991;41:460-3.
192 Lindgren V, Bryke CR, Ozcelik T, Yang-Feng TL,Francke U. Phenotypic, cytogenetic, and molecular stud-ies of three patients with constitutional deletions ofchromosome 5 in the region of the gene for familialadenomatous polyposis. Am 7 Hum Genet 1992;50:988-97.
AZF Azoospermia193 Anderson M, Page DC, Pettay D, et al. Y;autosome translo-
cations and mosaicism in the aetiology of 45,X maleness:assignment of fertility factor to distal Yql 1. Hum Genet1988;79:2-7.
9 Bardoni B, Zuffardi 0, Guioli S, et al. A deletion map of thehuman Yql 1 region: implications for the evolution of theY chromosome and tentative mapping of a locus involvedin spermatogenesis. Genomics 1991;1 1:443-51.
95 Ma K, Sharkey A, Kirsch S, et al. Towards the molecularlocalisation of the AZF locus: mapping of microdeletionsin azoospermic men within 14 subintervals of interval 6of the human Y chromosome. Hum Mol Genet 1992;1:29-33.
198 Diaz-Castanos LR, Rivera H, Gonzales-Montes RM, DiazM. Translocation (Y;19)(ql2;ql3) and azoospermia. AnnGenet (Paris) 1991;34:27-9.
BPES Blepharophimosis, ptosis, epicanthus inversussyndrome'
197 De Almeida JCC, Llerena JC Jr, Neto JBG. Anotherexample favouring the location of BPES at 3q2. 7 MedGenet 1993;30:86.
198 De Die-Smulders CEM, Engelen JJM, Donk JM, FrynsJP. Further evidence for the location of the BPES gene at3q2. J Med Genet 1991;28:725.
99 Fujita H, Meng J, Kawamura M, et al. Boy with a chromo-some del(3)(ql2q23) and blepharophimosis syndrome.Am J Med Genet 1992;44:434-6.
2 Fukushima Y, Wakui K, Nishida T, Ueoka Y. Blepharo-phimosis syndrome and a de novo balanced autosomaltranslocation [46,XY,t(3;4)(q23;p 15.2)]. Possible locationof blepharophimosis syndrome to 3q23. AmJ Hum Genet1990;47:A29.
201 Jewett T, Rao PN, Weaver RG, et al. Blepharophimosissyndrome (BPES) associated with del 3q22: gene assign-ment to the interphase of band 3q22-q23. Am Jf HumGenet 1992;51(suppl):A81.
BWS Beckwith-Wiedemann syndrome'02103128202 Brown KW, Gardner A, Williarns JC, et al. Paternal origin
of Ii pi5 duplications in the Beckwith-Wiedemann syn-drome. Cancer Genet Cytogenet 1992;58:55-70.
203 Haas OA, Zoubek A, Grumayer ER, Gadner H. Constitutionalinterstitial deletion of 1 Ipi 1 and pericentric inversion ofchromosome 9 in a patient with Wiedemann-Beckwithsyndrome and hepatoblastoma. Cancer Genet Cytogenet1986;23:95-104.
204 Pueschel SM, Padre-Mendoza T. Chromosome 11 andBeckwith-Wiedemann syndrome. J Pediatr 1984;104:484-5.
m Schmutz SM. Deletion of chromosome ll(pl 1p13) in apatient with Beckwith-Wiedemann syndrome. ClinGenet 1986;30:154-6.
CDPX1 Chondrodysplasia punctata 170208 Ballabio A, Carrozzo R, Gil A, et al. Molecular characteri-
zation of human X/Y translocations suggests their aetio-logy through aberrant exchange between homologoussequences on Xq and Yq. Ann Hum Genet 1989;53:9-14.
CMPD1/SRAl Campomelic dysplasia/sex reversal,autosomal 194 97101
CMT1A Charcot-Marie-Tooth neuropathy 1109CRS1 Craniosynostosis, syndromic 1207 Motegi T, Ohuchi M, Ohtaki C, et al. A craniosynostosis in
a boy with a del(7) (p15.3p21.3): assignment by deletionmapping of the critical segment for craniosynostosis tothe mid-portion of 7p21. Hum Genet 1985;71:160-2.
208 Speleman F, Craen M, Leroy J. De novo terminal deletion7p22.l1 -pter in a child without craniosynostosis. Jf MedGenet 1989;26:528-32.
CYBB Chronic granulomatous disease209 Royer-Pokora B, Kunkel LM, Monaco AP, et al. Cloning of
the gene for an inherited human disorder-chronic gra-nulomatous disease-on the basis of its chromosomallocation. Nature 1986;322:32-8.
210 de Saint-Basile G, Bohler MC, Fischer A, et al. Xp2l DNAmicrodeletion in a patient with chronic granulomatousdisease, retinitis pigmentosa, and McLeod phenotype.Hum Genet 1988;80:85-9.
DFN3 Deafness, conductive, with fixed stapes"'211 Reardon W, Roberts S, Phelps PD, et al. Phenotypicevidence for a common pathogenesis in X-linked deaf-ness pedigrees and in Xql3-q21 deletion related deaf-ness. Am J Med Genet 1992;44:513-17.
DGCR1 DiGeorge syndrome 1212 Augusseau S, Jouk S, Jalbert P, Prieur M. DiGeorge
syndrome and 22ql 1 rearrangements. Hum Genet1986;74:206.
213 Carey AH, Roach S, Williamson R, etal. Localization of 27DNA markers to the region of human chromosome22ql1 -pter deleted in patients with the DiGeorge syn-drome and duplicated in the der22 syndrome. Genomics1990;7:299-306.
725
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

726
214 Greenberg F, Elder FFB, Haffner P, Northrup H, Ledbet-ter DH. Cytogenetic findings in a prospective series ofpatients with DiGeorge anomaly. Am J Hum Genet1988;43:605-1 1.
215 Driscoll DA, Budarf ML, Emanuel BS. A genetic etiologyfor DiGeorge syndrome: consistent deletions and micro-deletions of 22ql 1. AmJ Hum Genet 1992;5O:924-33.
216 Scambler PJ, Carey AH, Wyse RKH, et al. Microdeletionswithin 22ql 1 associated with sporadic and familialDiGeorge syndrome. Genomics 1991;1O:201-6.
217 Wilson DI, Cross IE, Goodship JA, et al. A prospectivecytogenetic study of 36 cases of DiGeorge syndrome. AmJ Hum Genet 1992;51:957-63.
DGCR2 DiGeorge syndrome 2214218 Monaco G, Ciccimarra F, Pignata C, Garofalo S. T cell
immunodeficiency in a patient with 10p deletion syn-drome. J Pediatr 1989;115:330.
DMD/BMD Duchenne and Becker muscular dys-trophy'-571 7275 113-116129-132
219 Boyd Y, Buckle V, Holt S, et al. Muscular dystrophy in girlswith X;autosome translocations. J Med Genet 1986;23:484-90.
220 Boyd Y, Buckle VJ. Cytogenetic heterogeneity of transloca-tions associated with Duchenne muscular dystrophy.Clin Genet 1986;29:108-15.
221 Boyd Y, Cockburn D, Holt S, et al. Mapping of 12translocation breakpoints in the Xp21 region with re-spect to the locus for Duchenne muscular dystrophy.Cytogenet Cell Genet 1988;48:28-34.
222 Monaco AP, Neve RL, Coletti-Feener C, et al. Isolation ofcandidate cDNA for portions of the Duchenne musculardystrophy gene. Nature 1986;323:646-50.
223 Ray PN, Belfall B, Duff C, et al. Cloning of the breakpointof an X;21 translocation associated with Duchenne mus-cular dystrophy. Nature 1985;318:672-5.
EDA Ectodermal dysplasia, anhidrotic (hypohidrotic)224 Limon J, Filipiuk J, Nedoszytko B, et al. X-linked anhidro-
tic ectodermal dysplasia and de novo t(X;1) in a female.Hum Genet 1991;87:338-40.
225 MacDermot KD, Hulten M. Female with hypohidroticectodermal dysplasia and de novo (X;9) translocation.Clinical documentation of the AnLy cell line case. HumGenet 1990;84:577-9.
226 Plougastel B, Couillin P, Blanquet V, et al. Mapping aroundthe Xql3.1 breakpoints of two X/A translocations inhypohidrotic ectodermal dysplasia (EDA) femalepatients. Genomics 1992;14:523-5.
227 Turleau C, Niaudet P, Cabanis MO, et al. X-linked hypo-hidrotic ectodermal dysplasia and t(X;12) in a female.Clin Genet 1989;35:462-6.
228 Zonana J, Roberts SH, Thomas NS, Harper PS. Recogni-tion and reanalysis of a cell line from a manifesting femalewith X linked hypohidrotic ectodermal dysplasia and anX;autosome balanced translocation. J Med Genet1988;25:383-6.
F9 Haemophilia B (coagulation factor IX deficiency)229 Vianna-Morgante AM, Batista DAS, Levisky RB, Zatz M.
X;autosomal translocations in females with X-linkedrecessive diseases. 7th Int Congr Hum Genet (Berlin)1 987;I:97.
FGDY Aarskog syndrome"8GCPS Greig cephalopolysyndactyly'6"166GFDH Goltz focal dermal hypoplasia70GK Glycerol kinase deficiency7'72230 Walker AP, Muscatelli F, Monaco AP. Isolation of the
human glycerol kinase gene by positional cloning. HumMol Genet 1993;2:107-14.
HLD Huntington-like disease231 Froster-Iskenius UG, Hayden MR, Wang HS, et al. A
family with Huntington disease and reciprocal transloca-tion 4;5. Am ] Hum Genet 1986;38:759-67.
232 Steele MW, Wenger SL, Chorazy A, et al. Chromosomesite 4q21 and Huntington like disease (HLD). Am]I HumGenet 1987;41:A85.
HMRD Haemoglobin H disease/mental retardation(deletion type)88
HPE2 Holoprosencephaly 2233 Hecht BKM, Hecht F, Munke M. Forebrain cleavage gene
causing holoprosencephaly: deletion mapping to chro-mosome band 2p21. Am ] Med Genet 1991;40:130.
HPE3 Holoprosencephaly 323 Munke M. Clinical, cytogenetic, and molecular approaches
to the genetic heterogeneity of holoprosencephaly. Am ]Med Genet 1989;34:237-45.
235 Hatziioannou A, Krauss CM, Lewis MB, Halazonetis 'ID.Familial holoprosencephaly associated with a transloca-tion breakpoint at chromosomal position 7q36. Am ]Med Genet 1991;40:201-5.
236 Lurie IW, Ilyina HG, Podleschuk LV, Gorelik LB, Zaleta-jev DV. Chromosome 7 abnormalities in parents ofchildren with holoprosencephaly and hydronephrosis.Am ] Med Genet 1990;35:286-8.
237 Gurrieri F, Trask BJ, van den Engh G, et al. Physicalmapping of the holoprosencephaly critical region in7q36. Nature Genet 1993;3:247-51.
HPE4 Holoprosencephaly 4238 Cohen MM. Perspectives on holoprosencephaly. Part III.
Spectra, continuities, and discontinuities. Am 7 MedGenet 1989;35:271-88.
HSCR Hirschsprung disease239 Bottani A, Xie Y, Binkert F, Schinzel A. A case of
Hirschsprung disease with a chromosome 13 microdele-tion, del(13)(q32.3q33.2): potential mapping of one dis-ease locus. Hum Genet 1991;87:748-50.
240 Lamont MA, Fitchett M, Dennis NR. Interstitial deletion
Tommerup
of distal 13q associated with Hirschsprung's disease. ]Med Genet 1989;26:100-4.
241 Kiss P, Osztovics M. Association of 13q deletion andHirschsprung's disease. ] Med Genet 1989;26:793-6.
IDS Hunter disease (iduronate-2-sulphatase defi-ciency)
242 le Guern E, Couillin P, Oberle I, Ravise N, Boue J. Moreprecise localization of the gene for Hunter syndrome.Genomics 1990,7:358-62.
243 Mossman J, Blunt S, Stephen R, Jones EE, Pembrey M.Hunter's disease in a girl: association with X;5 chromo-somal translocation disrupting the Hunter gene. Arch DisChild 1986;58:911-15.
IPI Incontinentia pigmenti 114'>'54KALI Kallmann syndrome 17°LGCR Langer-Giedion syndrome'272" Buhler EM, Buhler UK, Beutler C, Fessler R. A final word
on the tricho-rhino-phalangeal syndromes. Cli't Genet1987,31 :273-5.
245 Gorlin RJ, Cervenka J, Bloom BA, Langer LO Jr. Nochromosome deletion found on prometaphase banding intwo cases of Langer-Giedion syndrome. Am] Med Genet1982;13:345-7.
246 Ogle RF, Dalzell P, Turner G, Wass D, Yip MY. Multipleexostoses in a patient with t(8;1 1)(q24.1 l;p l5.5). ] MedGenet 1991;28:881-3.
247 Shabtai F, Sandowski U, Nissimow R, Klar D, Halbrecht I.Familial syndrome with some features of the Langer-Giedion syndrome, and paracentric inversion of chromo-some 8, inv 8 (qll.23-q21.1). Clin Genet 1985;27:600-5.
248 Turleau C, Chavin-Colin F, de Grouchy J, et al. Langer-Giedion syndrome with and without del 8q: assignmentof critical segment to 8q23. Hum Genet 1982;62:183-7.
LYP Lymphoproliferative syndrome, X linked73MBS Moebius syndrome249 Slee JJ, Smart RD, Viljoen DL. Deletion of chromosome 13
in Moebius syndrome. ] Med Genet 1991;28:413-14.250 Ziter FA, Wiser WC, Robinson A. Three generation pedi-
gree of a Moebius syndrome variant with chromosometranslocation. Arch Neurol 1977;34:437-42.
MDCR Miller-Dieker syndrome22125 26MNK Menkes disease'05-107211 Mercer JFB, Livingstone J, Hall B, et al. Isolation of a
partial candidate gene for Menkes disease by positionalcloning. Nature Genet 1993;3:20-5.
252 Vulpe C, Levinson B, Whitney S, Packman S, Gitschier J.Isolation of a candidate gene for Menkes disease andevidence that it encodes a copper-transporting ATPase.Nature Genet 1993;3:7-13.
MRX2 Mental retardation, X linked70NDP Norrie disease'08253 Ohba N, Yamashita T. Primary vitreoretinal dysplasia
resembling Norrie's disease in a female: association withX autosome chromosomal translocation. Br]I Ophthalmol1986;70:64-71.
254 Pettenati MJ, Rao PN, Weaver RG Jr, Thomas IT, McMa-han MR. Inversion (X)(p 11 .4q22) associated with Norricdisease in a four generation family. Am
_Med Genet
1993;45:577-80.NFl Neurofibromatosis 1 (von Recklinghausen)9"""'13SNF2 Neurofibromatosis 2 (central, bilateral acoustic
neurinoma)255 Arai E, Ikeuchi T, Karasawa S, et al. Constitutional translo-
cation t(4;22)(ql2;ql2.2) associated with neurofibroma-tosis type 2. Am ] Med Genet 1992;44:163-7.
OAI Ocular albinism 1 (Nettleship-Falls type)"'OCRL Oculocerebrorenal syndrome of Lowe256 Hodgson SV, Heckmatt JZ, Hughes E, Crolla JA, Dubo-
witz V, Bobrow M. A balanced de novo X autosometranslocation in a girl with manifestations of Lowe syn-drome. Am Med Genet 1986;23:837-47.
257 Mueller OT, Hartsfield JK Jr, Gallardo LA, et al. Loweoculocerebrorenal syndrome in a female with a balancedX;20 translocation: mapping of the X chromosomebreakpoint. Am ] Hum Genet 1991;49:804-10.
PAX6 Paired box gene 6 associated with aniridia'924PBT Piebald trait258 Yamamoto Y, Nishimoto H, Ikemoto S. Interstitial deletion
of the proximal long arm of chromosome 4 associatedwith father-child incompatibility within the Gc-system.Probable reduced gene dosage effect and partial piebaldtrait. Am 7 Med Genet 1989;32:520-3.
259 Funderburk SJ, Crandall BF. Dominant piebald trait in aretarded child with a reciprocal translocation and smallintercalary deletion. Am7 Hum Genet 1974;26:715-22.
260 Hoo JJ, Haslam RHA, van Orman C. Tentative assignmentof piebald trait gene to chromosome band 4ql2. HumGenet 1986;73:230-1.
261' Lacassie Y, Thurmon TF, Tracy MC, Pelias MZ. Piebaldtrait in a retarded child with interstitial deletion ofchromosome 4. Am 7 Hum Genet 1977;29:641-2.
PWCR Prader-Willi syndrome64 104124125RB1 Retinoblastoma susceptibility394" 112 133 134 139RP3 Retinitis pigmentosa 3262 McDowell C, Burghes AH, Anson-Cartwright S, et al. X-
linked retinitis pigmentosa (XLRP): mapping of the geneto Xp2l, pulsed field gel electrophoresis (PFGE) of theregion and cloning strategies. Am ] Hum Genet1990;47:A256(1009).
RSTS Rubinstein-Taybi syndrome 187SHFD1 Split hand and foot deformity 1263 Hasegawa T, Hasegawa Y, Assamura S, et al. EEC syn-
drome (ectrodactyly, ectodermal dysplasia and cleft lip/palate) with a balanced reciprocal translocation between
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from

Mendelian cytogenetics. Chromosome rearrangements associated with mendelian disorders
7q11.21 and 9pl2 (or 7pl1.2 and 9q12). Clin Genet1991;40:202-6.
264 Qumsiyeh MB. EEC syndrome (ectrodactyly, ectodermaldysplasia and cleft lip/palate) is on 7p1l.2-q21.3. ClinGenet 1992;42:101
265 Rivera H, Sanchez-Corona J, Burgos-Fuentes VR, Melen-dez-Ruiz MJ. Deletion of 7q22 and ectrodactyly. GenetCounsel 1992;2:27-3 1.
266 Sharland M, Patton MA, Hill L. Ectrodactyly of hands andfeet in a child with a complex translocation including7q21.2. Am7Med Genet 1991;39:413-14.
SRY Testis-determining factor70267 Disteche CM, Casanova M, Saal H, et al. Small deletions of
the short arm of the Y chromosome in 46,XY females.Proc Natl Acad Sci USA 1986;83:7841-4.
268 Ferguson-Smith MA, Cooke A, Affara NA, Boyd E, TolmieJL. Genotype-phenotype correlations in XX males andtheir bearing on current theories of sex determination.Hum Genet 1990;84:198-202.
269 Sinclair AH, Berta P, Palmer MS, et al. A gene from thehuman sex-determining region encodes a protein withhomology to a conserved DNA-binding motif. Nature1990;346:240-4.
SS Short stature, X linked70270 Ogata T, Matsuo N, Shimuzu N. A ring X chromosome,
46,Y,r(X)(p22.33q28), as a cause of extreme short staturein a male. Am J Med Genet 1990;35:241-4.
STS X linked ichthyosis70TCD Choroideraemia37136 174175271 Cremers FP, Van den Pol DJR, Diergaarde PJ, et al.
Physical fine mapping of the choroideremia locus usingXq21 deletions associated with complex syndromes.Genomics 1989;4:41-6.
272 Kaplan J, Gilgenkrantz S, Dufier JL, Frezal J. Choroidere-mia and ovarian dysgenesis associated with an X;7 denovo balanced translocation (HGM1O). Cytogenet CellGenet 1989;51:1022.
273 Merry DE, Janne PA, Landers JE, Lewis RA, NussbaumRL. Isolation of a candidate gene for choroideraemia.Proc Natl Acad Sci USA 1992;89:2135-9.
274 Siu VM, Gonder JR, Jung JH, Sergovich FR, Flintoff WF.Choroideremia associated with an X-autosomal translo-cation. Hum Genet 1990;84:459-64.
TKC Torticollis, keloids, cryptorchidism, and renaldysplasia
275 Zuffardi 0, Fraccaro M. Gene mapping and serendipity.The locus for torticollis, keloids, cryptorchidism andrenal dysplasia (31430, McKusick) is at Xq28, distal tothe G6PD locus. Hum Genet 1982;62:280-1.
TRP1 Trichorhinophalangeal syndrome 1276 Fryns JP, Van den Berghe H. 8q24. 12 interstitial deletion in
trichorhinophalangeal syndrome type I. Hum Genet1986;74: 188-9.
277 Goldblatt J, Smart RD. Tricho-rhino-phalangeal syndromewithout exostoses, with an interstitial deletion of 8q23.Clin Genet 1986;29:434-8.
278 Hamers A, Jongbloet P, Peeters G, Fryns JP, Geraedts J.Severe mental retardation in a patient with tricho-rhino-phalangeal syndrome type I and 8q deletion. Eur JPediatr 1990;149:618-20.
279 Naritomi K, Hirayama K. Partial trisomy of distal 8qderived from mother with mosaic 8q23.3-24.13 deletion,and relatively mild expression of tricho-rhinophalangealsyndrome I. Hum Genet 1989;82:199-201.
260 Yamamoto Y, Oguro N, Miyao M, Yanagisawa M. Tricho-rhino-phalangeal syndrome type I with severe mentalretardation due to interstitial deletion of 8q23.3-24.13.Am J Med Genet 1989;32:133-5.
28 Haan EA, Hull YJ, White S, et al. Tricho-rhino-phalangealand branchio-oto syndromes in a family with an inheritedrearrangement of chromosome 8q. Am J Med Genet1989;32:490-4.
VCFS Velo-cardio-facial syndrome282 Driscoll DA, Spinner NB, Budarf ML, et al. Deletions and
microdeletions of 22ql 1.2 in velo-cardio-facial syn-drome. Am J Med Genet 1992;44:261-8.
283 Scambler PJ, Kelly D, Lindsay E, et al. Velo-cardio-facialsyndrome associated with chromosome 22 deletionsencompassing the DiGeorge locus. Lancet 1992;339:1138-9.
284 Kelly D, Goldberg R, Wilson D, et al. Confirmation thatthe velo-cardio-facial syndrome is associated with haplo-insufficiency of genes at chromosome 22ql 1. Am J MedGenet 1993;45:308-12.
VWS Van der Woude syndrome 1285 Bocian M, Walker AP. Lip pits and deletion lq32-q41. Am
J Med Genet 1987;26:437-43.WAGR see also AN2, WT1'5286 Puissant H, Azoulay M, Serre JL, Piet LL, Junien C.
Molecular analysis of a reciprocal translocationt(5;I 1)(qI 1;p1 3) in a WAGR patient. Hum Genet1988;79:280-2.
WS1 Wardenburg syndrome 113727 Ishikiriyama S, Tonoki H, Shibuya Y, et al. Wardenburg
syndrome type I in a child with a de novo inversion(2)(q35q37.3). Am J Med Genet 1989;33:505-7.
WT1 Wilms's tumour susceptibility'11720-2345-4952-57 128 168-170 286
XK Kell blood group precursor (McLeod phenotype)288 Ho MF, Monaco AP, Blonden LAJ, et al. Fine mapping of
the McLeod locus (XK) to a 150-380-kb region in Xp21.Am J Hum Genet 1992;50:317-30.
ZWS Zellweger syndrome30 31
727
on February 25, 2022 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.30.9.713 on 1 Septem
ber 1993. Dow
nloaded from