Embed Size (px)
Citation preview
Men United v Prostate Cancer:Five inequalities, five solutions.
2
3
ForewordAt the start of 2014, Prostate Cancer UK launched Men United v Prostate Cancer, a campaign to encourage everyone to stand together and create a movement for change in men’s health. Within three months, over 100,000 people had signed for Men United to help us get men’s health back on the agenda in the UK.
At the heart of this campaign is the issue of inequalities faced by men with, and at risk of, prostate cancer. These inequalities exist across the country, across the population and at different stages of a man’s prostate cancer experience. This report doesn’t outline a single issue, but rather summarises each inequality in its own chapter, providing the evidence around the current situation and our recommendations for the future.
We aim to highlight and eradicate inequalities around awareness, age, ethnicity, address and access to treatments, to ensure that all men diagnosed with prostate cancer in the UK receive the best possible information, treatment and care.
ContentForeword 3
Recommendations 4
Diagnosis, awareness, information and support 6
Inequalities faced by Black men with prostate cancer 10
Quality Care Everywhere? Prostate cancer and variation across the UK 14
Age 18
Access to treatments 24
4
RecommendationsDiagnosis, awareness, information and supportInequality: Despite prostate cancer being the most common cancer in men, public health programmes have not included awareness raising work on the risk factors for this disease. Nor are men getting the right help and support for side effects following treatment.
Our call: Public Health England, the Scottish Government, Public Health Wales and the Public Health Agency in Northern Ireland should design awareness programmes such as ‘Be Clear on Cancer’ and ‘Detect Cancer Early’ around risk factors rather than symptoms alone. Health departments in all countries of the UK must urgently review and update the current prescribing guidance for erectile dysfunction. The Prostate Cancer Risk Management Programme (PCRMP) should be better communicated and used in primary care across the UK.
Inequalities faced by Black men with prostate cancerInequality: Black men have double the average risk of being diagnosed with prostate cancer in their lifetime. However, awareness of prostate cancer is low in Black communities; and Black men with cancer are reporting poorer experiences of NHS care. Black men are more likely to die from prostate cancer compared to other ethnicities, and a lack of comprehensive data on cancer outcomes and experiences by ethnicity makes it difficult to assess what lies behind these inequalities.
Our call: Public Health England, the Scottish Government, Public Health Wales and the Public Health Agency in Northern Ireland should target future awareness programmes on prostate cancer towards Black communities, and encourage more comprehensive collection and reporting of ethnicity data for all aspects of prostate cancer care.
Quality Care Everywhere? Prostate cancer and variation across the UKInequality: There are inconsistencies in the quality of care and support that men receive across the UK.
Our call: NHS England must ensure that measurable aspects of patient experience in low performing trusts are brought into line with the best in England – for example, all men should have a detailed written care plan, an assigned Clinical Nurse Specialist, and the necessary information and support following a prostate cancer diagnosis. The Scottish Government must introduce a National Cancer Patient Experience Survey to identify and find solutions to issues faced by men with prostate and other cancers. In Wales, the Welsh Government should act on the recent Cancer Patient Experience Survey to address the often poor levels of support offered to men with prostate cancer. The Department of Health, Social Services and Public Safety (DHSSPS) in Northern Ireland will also need to listen to its own Cancer Patient Experience Survey when it is released in the coming months to ensure that prostate cancer patients’ needs are addressed.
5
AgeInequality: Older men diagnosed with prostate cancer are far less likely to be told about side effects of treatment, and at times have fewer treatment options offered to them, than younger men. It is not clear that treatment pathways are based on a person’s fitness and preferences rather than their age alone.
Our call: NHS England, NHS Wales, the Scottish Government and Health and Social Care (HSC) in Northern Ireland should ensure that older men are not denied treatments on the basis of their age, and that they are given information about possible treatment side effects.
Access to treatmentsInequality: Not all men in the UK have access to the information they need to make an informed choice about the PSA test, or about the best treatments or aftercare support for prostate cancer, especially for side effects such as erectile dysfunction.
Our call: Commissioning and regulatory authorities should take urgent steps to ensure that the best treatments and diagnostics are available across the UK. For example, the National Institute for Health and Care Excellence (NICE) must ensure that clear guidance is provided to allow men to access treatments for advanced cancer; the Scottish Medicines Consortium (SMC) must ensure greater patient participation and transparency in their decision making; health departments in all countries of the UK must urgently review and update the current prescribing guidance for erectile dysfunction; and the Prostate Cancer Risk Management Programme should be better communicated and used in primary care across the UK.
6
Diagnosis, awareness, information and supportImproving risk assessment for prostate cancerOne of the major challenges facing men in the UK today is that there is no reliable, widely applicable, easy way to assess their individual risk of developing prostate cancer. A PSA (prostate specific antigen) test alone cannot provide men and their doctors with all the information they need to make life-changing decisions about treatment and monitoring. Although some risk calculators (nomograms) have been developed for use in other countries, we need a tool that is applicable to the UK population and acceptable to men in the UK, their doctors and the NHS when delivered through primary care.
This is why we plan to provide up to £1.5m to support research that will develop and test a more effective tool that combines a suite of known risk factors to give a more useful indication of a man’s risk of prostate cancer. Our vision is that this research will deliver a tool backed by appropriate evidence that is ready for wide scale clinical implementation through NHS primary care within a 5 year timescale. Ultimately, the aim of a new risk assessment tool should be to reduce unnecessary biopsies and treatment and increase the number of men whose aggressive prostate cancer is detected and treated early.
Making an informed choice about the PSA testUntil a risk assessment tool is developed and widely used, determining their PSA level is the first step towards a diagnosis for most men with prostate cancer. Men aged 50 and over have the right to make an informed choice about whether to have a PSA test under the Prostate Cancer Risk Management Programme (PCRMP) (1). In order to make this choice, men need to:• know their risks (age, family history and ethnicity); and• know their rights (to a PSA test free of charge on the NHS if they are aged 50 and over
provided they have had a discussion about the pros and cons with a GP (1)).
We know from a recent survey that GPs think that men over 50 should have access to the PSA test if they want one; that balanced information should be provided; and that GPs should be responsible for delivering this information (2). However, the GPs themselves are not initiating conversations about prostate health proactively. We also know that 53% of UK men over 50 have never heard of the PSA test (3). So at the moment men are not in a position to make an informed choice.
Despite being the most common cancer in men in the UK (4), prostate cancer is often omitted from awareness programmes such as Be Clear on Cancer and Detect Cancer Early because early stage prostate cancer does not always present with symptoms. We believe that there is a need for such programmes to be redesigned so that prostate cancer can be incorporated and men can make an informed choice about testing.
Information and supportProstate Cancer UK’s Quality Checklist outlines the care and support men should expect to receive whether in England, Wales, Northern Ireland or Scotland (5). The standards in the Checklist are based on research with over 700 people affected by prostate cancer and healthcare professionals (6,7).
7
Men aren’t getting the right help and support for side effectsA 2012 survey of 866 prostate cancer survivors in England (8,9) showed that on average, 58% of prostate cancer patients were unable to have an erection 1-5 years after treatment, with a further 11% having significant difficulty in having or maintaining an erection, 13% having difficulty controlling their bowels and 39% having some degree of urinary leakage. The presence of urinary leakage was significantly associated with poorer quality of life. Prostate Cancer UK’s 2012 survey of 610 men’s views of quality care found an overwhelming majority of men reported experiences of treatment side effects (7) – over 4 out of 5 (85%) told us that they had experienced side effects as a result of their treatment. Our survey found that of the men who reported experiencing side effects as a result of treatment, 79% rated erectile dysfunction as ‘bad’ or ‘very bad’, 72% rated loss of libido as ‘bad’ or ‘very bad’, 60% rated anxiety as ‘bad’ or ‘very bad’, 59% rated fatigue as ‘bad’ or ‘very bad’ and 54% rated urinary incontinence as ‘bad’ or ‘very bad’ (7).
Prostate Cancer UK has commissioned a 3-year UK-wide survey of prostate cancer survivors with the active involvement of NHS partners. This will give us an unparalleled insight into men’s quality of life following a diagnosis of prostate cancer, including what patients feel they need from treatment and care, and will identify current gaps in treatment and care according to men and families affected by prostate cancer.
Not all men with prostate cancer are receiving information, care and support for the life changing side effects that result from their treatment. The 2013 National Cancer Patient Experience Survey (NCPES) in England (10) found that:• 36% of prostate cancer patients were not told about treatment side effects that could affect
them in the future• 26% of prostate cancer patients did not have possible side effects explained in an
understandable way• 17% of prostate cancer patients were not given written information about side effects.
Prostate Cancer UK’s 2012 survey found that 1 in 5 men (19%) described the care and support they received for the side effects they experienced as ‘bad’ or ‘very bad’. After completing treatment, 1in 3 men (31%) said that they received ‘too little’ aftercare for the treatment of side effects.
Erectile dysfunction and prostate cancerA Prostate Cancer UK survey undertaken in 2012 showed that 76% of men who experienced treatment side effects suffered from erectile dysfunction (ED) (7). Of the men who experienced ED, 79% said they found it very difficult or difficult to deal with. The Department of Health’s 2012 survey of prostate cancer survivors found that only 35% of respondents reported having no difficulty with sexual matters (8). In the same survey, 58% reported that they were unable to have an erection at all with a further 11% reporting difficulty having or maintaining an erection.
The US Prostate Cancer Outcomes Study (PCOS) questioned how big a problem sexual function was at two years post-surgery. They found that 14% of men said it was no problem, 23% said it was a small problem, and 42% said it was a moderate to big problem (13,14). This research also highlights that the effect of ED on patients’ quality of life is both variable and highly individualised; some patients with significant sexual dysfunction experience little bother while others may experience minimal dysfunction but significant bother (15). These findings are reflected in qualitative, interview-based research commissioned by Prostate Cancer UK into the
8
differential support needs of men with prostate cancer at different life stages (11). This research found that for many men, ED is the most distressing impact of their prostate cancer. Before treatment, men often underestimated the impact that this side effect might have on their self-identity. Although ED had more of an impact on younger men, older respondents were often surprised at how much they were emotionally affected by it. There are currently no NICE guidelines on the management of ED. Other professional organisations, including the British Society for Sexual Medicine, have produced a number of guidelines (12), but none of these have the same weight and influence as guidelines produced by NICE or the equivalents in the devolved nations. To address this, Prostate Cancer UK has supported the development of a new guideline (13), and quick guide to complement it, for the treatment of ED post-surgery for prostate cancer. This guidance reflects best practice, including the recognition that the earlier an ED management strategy is in place, the better the outcome is likely to be. This includes having a strategy in place before treatment starts, as well as having access to a combination of drugs and devices to treat ED. In addition, the prescribing guidance has not been comprehensively updated since 1999, despite significant developments in the field, and urgently needs to be reviewed and updated. Without this, men will continue to receive inadequate support for ED.
In summaryInequality: Despite prostate cancer being the most common cancer in men, public health programmes have not included awareness raising work on the risk factors for this disease. Nor are men getting the right help and support for side effects following treatment.
Our call: Public Health England, the Scottish Government, Public Health Wales and the Public Health Agency in Northern Ireland should design awareness programmes such as ‘Be Clear on Cancer’ and ‘Detect Cancer Early’ around risk factors rather than symptoms alone.Health departments in all countries of the UK must urgently review and update the current prescribing guidance for erectile dysfunction. The Prostate Cancer Risk Management Programme should be better communicated and used in primary care across the UK.
9
References1. Burford D, Kirby M, Austoker J. Prostate Cancer Risk Management Programme information for primary
care; PSA testing in asymptomatic men. Evidence document. NHS Cancer Screening Programmes [Internet]. 2010. Available from: http://www.cancerscreening.nhs.uk/prostate/pcrmp-guide-2.html
2. Kantar Health. Figures from a survey of 500 GPs in the UK conducted by Kantar Health on behalf of Prostate Cancer UK in January 2014. 2014.
3. YouGov. Figures from YouGov Plc. Total sample size was 2864 adults. Fieldwork was undertaken between 13th January to 4th February 2014. The survey was carried out online. The figures have been weighted and are representative of all UK adults (aged 18+). 2014.
4. Cancer Research UK. Cancer incidence for common cancers: Ten most common cancers in males (2011) [Internet]. 2014. Available from: http://www.cancerresearchuk.org/cancer-info/cancerstats/incidence/commoncancers/#Ten
5. Prostate Cancer UK. A quality checklist: Your standards of care [Internet]. 2013 [cited 2013 May 10]. Available from: http://prostatecanceruk.org/media/1604548/a_quality_checklist_-_your_standards_of_care.pdf
6. Prostate Cancer UK. It’s time for quality care. Everywhere. [Internet]. 2013 [cited 2013 May 10]. Available from: http://prostatecanceruk.org/media/2105544/2298-its-time-for-quality-care-everywhere_full-2-.pdf
7. Prostate Cancer UK. Men’s views on quality care in prostate cancer: What does good quality care mean for men with prostate cancer? [Internet]. 2012. Available from: http://prostatecanceruk.org/media/1559431/prostate_cancer_uk_quality_care_survey_report_june_2012.pdf
8. Glaser AW, Fraser LK, Corner J, Feltbower R, Morris EJA, Hartwell G, et al. Patient-reported outcomes of cancer survivors in England 1–5 years after diagnosis: a cross-sectional survey. BMJ Open [Internet]. 2013 Jan 1 [cited 2013 Apr 16];3(4). Available from: http://bmjopen.bmj.com/content/3/4/e002317
9. Quality of Life of Cancer Survivors in England - Report on a pilot survey using Patient Reported Outcome Measures (PROMS) [Internet]. Department of Health; 2012. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/267042/9284-TSO-2900701-PROMS-1.pdf
10. Quality Health. Cancer Patient Experience Survey 2012-13 National Report [Internet]. 2013. Available from: http://www.quality-health.co.uk/resources/surveys/national-cancer-experience-survey/2013-national-cancer-patient-experience-survey-reports/301-2013-national-cancer-patient-experience-survey-progr-amme-national-report/file
11. BritainThinks. Findings from qualitative research carried out by BritainThinks. The total sample size was 53 adults affected by prostate cancer across the UK (including 8 partners of men with prostate cancer). The fieldwork was undertaken between 5th February and 13th March 2014, comprising telephone interviews, focus groups and online qualitative research. 2014.
12. British Society for Sexual Medicine. Guidelines on the management of erectile dysfunction [Internet]. 2013. Available from: http://www.bssm.org.uk/downloads/BSSM_ED_Management_Guidelines_2013.pdf
13. Kirby MG, White ID, Butcher J, Challacombe B, Coe J, Grover L, et al. Development of UK recommendations on treatment for post-surgical erectile dysfunction. Int J Clin Pract. 2013;n/a–n/a.
10
Inequalities faced by Black men with prostate cancerBlack men are more likely to develop prostate cancer than men of other ethnic backgrounds. In the UK, 1 in 4 Black men will be diagnosed with prostate cancer in their lifetime, putting them at double the risk of UK men as a whole (1). Black men may also be more likely to be diagnosed with prostate cancer at an average of 3-5 years younger than White men (2–4). The prostate cancer mortality rate is 30% higher for Black men than White men in the UK (5).
Awareness and diagnosisCancer awareness is generally low in Black and Minority Ethnic (BME) groups (6). This is a worrying trend given the crucial role that awareness and detection play in catching cancer early, when it is most treatable (7). Furthermore, prostate cancer survival rates correspond to stage at diagnosis, with survival rates far worse for men with advanced disease than for those with prostate cancer that is caught in the early stages (8). Men’s awareness of prostate cancer is key; yet awareness amongst men is low and, despite an increased risk of being diagnosed with the disease, awareness is lowest amongst Black men (9).
Within BME communities, cancer is sometimes perceived as a disease affecting the White population only (10). This view may be contributing to a lower engagement amongst Black communities with national cancer awareness campaigns, which deliver vital information about risk factors and how to access screening services.
Prostate cancer is the most common cancer in men (11). In a survey of 1377 men, 91% of White men had heard of prostate cancer, decreasing to 81% amongst Black men (9). We call on the Department of Health, NHS England and Public Health England (PHE) to deliver a national awareness campaign for prostate cancer as part of Be Clear on Cancer (BCOC). As most early prostate cancer does not cause any symptoms, an awareness campaign for prostate cancer would need to focus on associated risk factors and how and when men should access diagnostic services. It will be vital to include risk by ethnicity in all information material so that Black men know their increased risk and are empowered to access services.
Another contributing factor to poorer health outcomes and the health inequalities gap is deprivation. Deprivation-based health inequalities are inextricably linked with ethnicity. The unemployment rate of all Black men of working age in 2009-11 was 18% (12), representing the highest rate of unemployment of all ethnicities. With cancer outcomes poorest for men classified as ‘most deprived’, it is clear that the wider, socioeconomic inequalities faced by Black men are impacting on their health. Prostate cancer stage at diagnosis data was only available for 26% of newly diagnosed prostate cancers in 2008-2010. Of these cases, 24% had ‘unknown’ ethnicity (13). We recommend that PHE ensures stage at diagnosis data is systematically collected and recorded by ethnicity. We believe that improved data collection will contribute to our understanding of the barriers Black men face in accessing services, which will in turn inform both national and local strategies about closing the inequalities gap.
11
Treatment and care PHE already collects important data on the treatment routes of men diagnosed with prostate cancer (14). These data are broken down by ethnicity, enabling us to draw demographic comparisons and monitor equality of access.
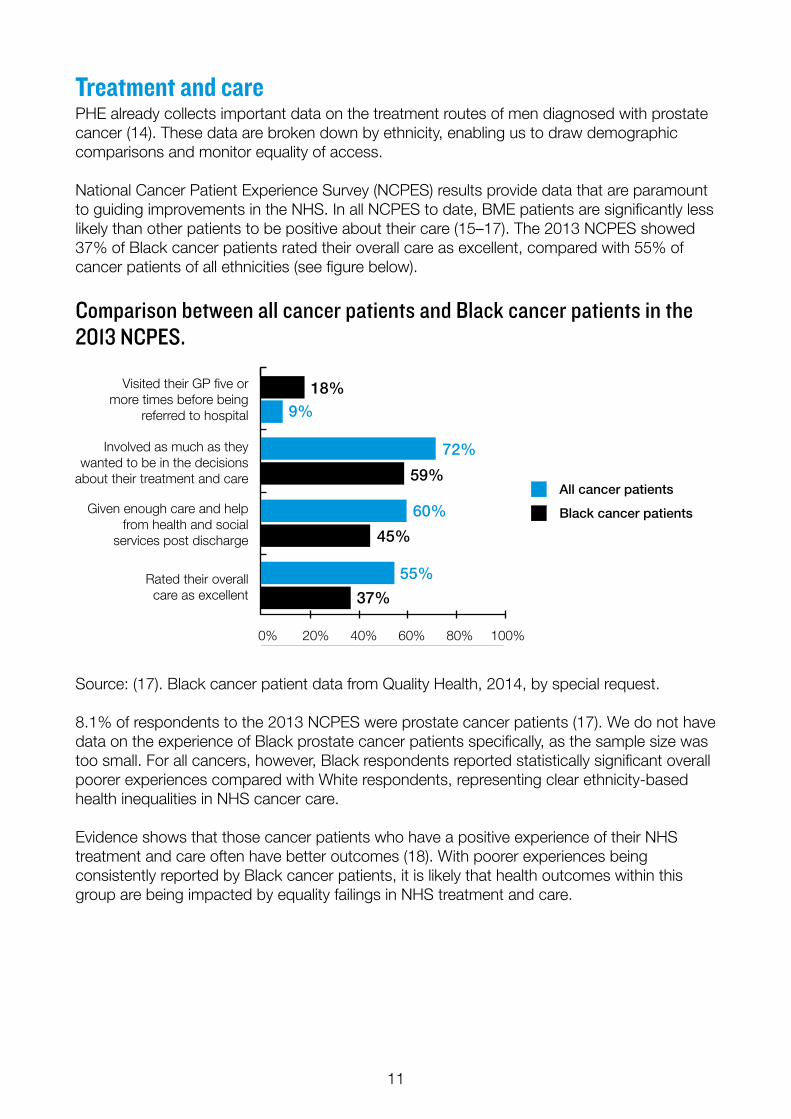
National Cancer Patient Experience Survey (NCPES) results provide data that are paramount to guiding improvements in the NHS. In all NCPES to date, BME patients are significantly less likely than other patients to be positive about their care (15–17). The 2013 NCPES showed 37% of Black cancer patients rated their overall care as excellent, compared with 55% of cancer patients of all ethnicities (see figure below).
Comparison between all cancer patients and Black cancer patients in the 2013 NCPES.
Source: (17). Black cancer patient data from Quality Health, 2014, by special request.
8.1% of respondents to the 2013 NCPES were prostate cancer patients (17). We do not have data on the experience of Black prostate cancer patients specifically, as the sample size was too small. For all cancers, however, Black respondents reported statistically significant overall poorer experiences compared with White respondents, representing clear ethnicity-based health inequalities in NHS cancer care.
Evidence shows that those cancer patients who have a positive experience of their NHS treatment and care often have better outcomes (18). With poorer experiences being consistently reported by Black cancer patients, it is likely that health outcomes within this group are being impacted by equality failings in NHS treatment and care.
0 20 40 60 80
100
9%
Visited their GP five ormore times before being
referred to hospital
Involved as much as theywanted to be in the decisions
about their treatment and care
Given enough care and helpfrom health and social
services post discharge
Rated their overallcare as excellent
0% 20% 40% 60% 80% 100%
All cancer patients
Black cancer patients
18%
72%
59%
60%
45%
55%
37%
12
Of the 68,737 cancer patients that responded to the 2013 NCPES, only 1.4% identified themselves as Black (17). Given that this figure only represents 0.05% of England’s Black population (1,846,614) (19), we do not believe that the views of Black cancer patients have been adequately represented. The proportion of White people represented is significantly higher. (0.15% of England’s 45,281,142 White population). We recommend that PHE set a demographic response rate target for the NCPES which is representative of Black men with cancer.
Living with and beyond prostate cancerThere are 255,000 men living with and beyond prostate cancer in the UK (20). Due to the lack of data on patient ethnicity, we do not know how many of these are Black men; however, using data collected from the NCPES, we do know that Black cancer patients are reporting lower levels of help and care from health and social services following hospital discharge, compared with the level reported by White patients. Whilst these patient experience data inform us of an inequalities gap that needs closing, without adequate regional profiling data, interventions cannot be targeted and prioritised appropriately under localised commissioning structures. Getting healthcare access right in the community setting is important in prostate cancer given that a large proportion of treatment takes place at the primary care level.
The Department of Health found that conclusions on ethnicity-based variations reported in the National Cancer Survivorship Initiative’s (NCSI) first pilot survey of cancer survivors could not be drawn due to the absence of available data (21). By a rise in cancer survey response rates amongst Black participants, health outcomes for this demographic can be improved.
The National Cancer Data Repository (NCDR) recorded 102,252 new cases of prostate cancer in 2008-10 in England. Of these, 26% had no ethnicity recorded (13). Proportionally, prostate cancer incidence is significantly higher in Black men than in White men. Without adequate data, the NHS will not be in a position to prioritise improvements towards meeting the needs of Black men who have returned from hospital care into the community and are living with or beyond prostate cancer with associated morbidities.
In summaryInequality: Black men have double the average risk of being diagnosed with prostate cancer in their lifetime. However, awareness of prostate cancer is low in Black communities; and Black men with cancer are reporting poorer experiences of NHS care. Black men are more likely to die from prostate cancer compared to other ethnicities, and a lack of comprehensive data on cancer outcomes and experiences by ethnicity makes it difficult to assess what lies behind these inequalities.
Our call: Public Health England, the Scottish Government, Public Health Wales and the Public Health Agency in Northern Ireland should target future awareness programmes on prostate cancer towards Black communities, and encourage more comprehensive collection and reporting of ethnicity data for all aspects of prostate cancer care.
13
References1. Prostate Cancer UK. Working out the risk of prostate cancer in Black men [Internet]. 2013
[cited 2013 Oct 30]. Available from: http://prostatecanceruk.org/we-can-help/african-caribbean-communities/1-in-4-stat-explained
2. Ben-Shlomo Y, Evans S, Ibrahim F, Patel B, Anson K, Chinegwundoh F, et al. The risk of prostate cancer amongst black men in the United Kingdom: the PROCESS cohort study. Eur Urol. 2008 Jan;53(1):99–105.
3. Karami S, Young HA, Henson DE. Earlier age at diagnosis: another dimension in cancer disparity? Cancer Detect Prev. 2007;31(1):29–34.
4. Metcalfe C, Evans S, Ibrahim F, Patel B, Anson K, Chinegwundoh F, et al. Pathways to diagnosis for Black men and White men found to have prostate cancer: the PROCESS cohort study. Br J Cancer. 2008 Oct 7;99(7):1040–5.
5. National Cancer Intelligence Network. Mortality from Prostate Cancer: Urological Cancers SSCRG [Internet]. 2012. Available from: http://www.ncin.org.uk/view?rid=1701
6. National Cancer Intelligence Network. Evidence to March 2010 on cancer inequalities in England [Internet]. 2010. Available from: http://www.ncin.org.uk/view?rid=169
7. Richards MA. The size of the prize for earlier diagnosis of cancer in England. Br J Cancer. 2009 Dec 3;101 Suppl 2:S125–129.
8. National Cancer Intelligence Network. Prostate Cancer Survival (1999-2002) - NCIN Data Briefing [Internet]. 2010. Available from: http://www.ncin.org.uk/view?rid=47
9. YouGov. Figures from YouGov Plc. Total sample size was 1723 men. Fieldwork was undertaken between 13th January to 4th February 2014. The survey was carried out online. The figures have been weighted and are representative of all UK adults (aged 18+). 2014.
10. BME Cancer Communities. Hear Me Now - The uncomfortable reality of prostate cancer in black African-Caribbean men [Internet]. 2013. Available from: http://www.bmecancer.com/index.php/cancers/prostate-cancer/82-hearmenow
11. Cancer Research UK. Cancer incidence for common cancers: Ten most common cancers in males (2011) [Internet]. 2014. Available from: http://www.cancerresearchuk.org/cancer-info/cancerstats/incidence/commoncancers/#Ten
12. ethnicity.ac.uk. Unemployment by gender and ethnicity, 2009-2011 [Internet]. [cited 2014 May 15]. Available from: http://www.ethnicity.ac.uk/employment/unemployment.html
13. Public Health England. Prostate cancer and ethnicity [Internet]. 2013. Available from: http://www.ncin.org.uk/view?rid=2635
14. National Cancer Intelligence Network. Treatment Routes in Prostate Cancer Urological Cancers SSCRG [Internet]. 2012. Available from: http://www.ncin.org.uk/view?rid=1260
15. National Cancer Patient Experience Survey Programme: 2010 National Survey Report. Department of Health [Internet]. 2010. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/216682/dh_122520.pdf
16. Department of Health. National Cancer Patient Experience Survey 2011/12 - National Report [Internet]. 2012. Available from: https://www.wp.dh.gov.uk/publications/files/2012/08/Cancer-Patient-Experience-Survey-National-Report-2011-12.pdf
17. Quality Health. Cancer Patient Experience Survey 2012-13 National Report [Internet]. 2013. Available from: http://www.quality-health.co.uk/resources/surveys/national-cancer-experience-survey/2013-national-cancer-patient-experience-survey-reports/301-2013-national-cancer-patient-experience-survey-progr-amme-national-report/file
18. NHS Confederation. Feeling better? Improving patient experience in hospital [Internet]. 2010. Available from: http://www.nhsconfed.org/~/media/Confederation/Files/Publications/Documents/Feeling_better_Improving_patient_experience_in_hospital_Report.pdf?dl=1
19. Office for National Statistics. KS201EW - Ethnic group [Internet]. 2011 [cited 2014 May 2]. Available from: http://www.nomisweb.co.uk/census/2011/KS201EW/view/2092957699?cols=measures
20. Maddams J, Utley M, Møller H. Projections of cancer prevalence in the United Kingdom, 2010-2040. Br J Cancer. 2012 Sep 25;107(7):1195–202.
21. Department of Health. The Quality of Life of Cancer Survivors in England [Internet]. 2012. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213192/9284-TSO-2900701-PROMS.pdf
14
Quality Care Everywhere? Prostate cancer and variation across the UKMen diagnosed with prostate cancer should not be disadvantaged just because of where they live. However there are inconsistencies in the quality of care and support men receive across the UK.
Using the findings from the 2013 National Cancer Patient Experience Survey (NCPES) in England (1), the Welsh Cancer Patient Experience Survey (CPES) (2) and a Prostate Cancer UK commissioned survey of the experiences of men with prostate cancer in Scotland (2013) (3), we have highlighted examples of variation across the UK. In Northern Ireland a Cancer Patient Experience Survey is in progress, however at the time of publication of this document the results were not available. A NCPES for Scotland is urgently needed to drive quality improvements at a local level and allow for comparisons to help improve sharing of best practice between health boards.
All men and their families deserve equal access to information on financial matters.Following a diagnosis of prostate cancer, having access to high quality information and support can help men and their friends and family manage the disease more effectively. This includes support and information on finances.
Shockingly, results from the most recent NCPES showed significant variations in the proportion of prostate cancer patients in England saying they had been given information about how to get financial help or benefits. Gloucestershire Hospitals NHS Foundation Trust performed the worst with only 4% of respondents with prostate cancer stating that they received enough information from hospital staff about financial help or benefits, compared to 85% at South Tees Hospitals NHS Foundation Trust. Data from Scotland reveals that just 30% of men with prostate cancer reported that hospital staff gave them enough information on any financial help that may be available (3). A similar result from the 2013 Welsh CPES highlighted an average of only 32% of men saying they had been given information about how to get financial help or benefits (2).
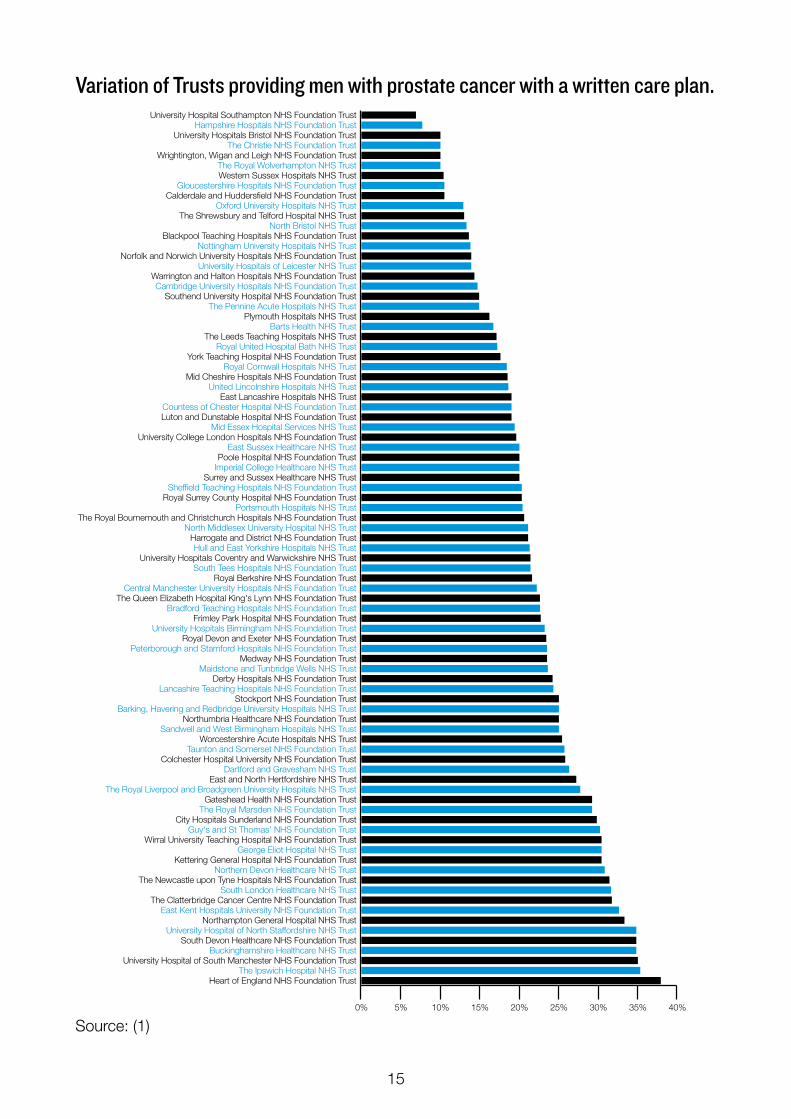
All men should have a written care planNot all men are being offered a written care plan (see figure opposite). Many men experience life-changing side effects from prostate cancer treatment and require support from healthcare professionals for some time after treatment has finished. During treatment, the type of support required varies and a man may see many different healthcare professionals including GPs, urologists, oncologists and specialist nurses. It is therefore essential that men are given a detailed care plan that sets out the follow-up tests and care they should expect to receive from these healthcare professionals.
Despite this, many men still don’t get a written care plan. Just 7% of men with prostate cancer treated at University Hospital Southampton NHS Foundation Trust reported that they were offered one, compared with 38% of men with prostate cancer from the Heart of England NHS Foundation Trust (1). The results from the devolved nations highlight the variation too with an average of 8% of men in Scotland reporting that they received a care plan (3) and 19% of men in Wales (2).
15
Variation of Trusts providing men with prostate cancer with a written care plan.
Source: (1)
0% 5% 10% 15% 20% 25% 30% 35% 40%
Heart of England NHS Foundation TrustThe Ipswich Hospital NHS Trust
University Hospital of South Manchester NHS Foundation TrustBuckinghamshire Healthcare NHS Trust
South Devon Healthcare NHS Foundation TrustUniversity Hospital of North Staffordshire NHS Trust
Northampton General Hospital NHS TrustEast Kent Hospitals University NHS Foundation Trust
The Clatterbridge Cancer Centre NHS Foundation TrustSouth London Healthcare NHS Trust
The Newcastle upon Tyne Hospitals NHS Foundation TrustNorthern Devon Healthcare NHS Trust
Kettering General Hospital NHS Foundation TrustGeorge Eliot Hospital NHS Trust
Wirral University Teaching Hospital NHS Foundation TrustGuy's and St Thomas' NHS Foundation Trust
City Hospitals Sunderland NHS Foundation TrustThe Royal Marsden NHS Foundation Trust
Gateshead Health NHS Foundation TrustThe Royal Liverpool and Broadgreen University Hospitals NHS Trust
East and North Hertfordshire NHS TrustDartford and Gravesham NHS Trust
Colchester Hospital University NHS Foundation TrustTaunton and Somerset NHS Foundation Trust
Worcestershire Acute Hospitals NHS TrustSandwell and West Birmingham Hospitals NHS Trust
Northumbria Healthcare NHS Foundation TrustBarking, Havering and Redbridge University Hospitals NHS Trust
Stockport NHS Foundation TrustLancashire Teaching Hospitals NHS Foundation Trust
Derby Hospitals NHS Foundation TrustMaidstone and Tunbridge Wells NHS Trust
Medway NHS Foundation TrustPeterborough and Stamford Hospitals NHS Foundation Trust
Royal Devon and Exeter NHS Foundation TrustUniversity Hospitals Birmingham NHS Foundation Trust
Frimley Park Hospital NHS Foundation TrustBradford Teaching Hospitals NHS Foundation Trust
The Queen Elizabeth Hospital King's Lynn NHS Foundation TrustCentral Manchester University Hospitals NHS Foundation Trust
Royal Berkshire NHS Foundation TrustSouth Tees Hospitals NHS Foundation Trust
University Hospitals Coventry and Warwickshire NHS TrustHull and East Yorkshire Hospitals NHS Trust
Harrogate and District NHS Foundation TrustNorth Middlesex University Hospital NHS Trust
The Royal Bournemouth and Christchurch Hospitals NHS Foundation TrustPortsmouth Hospitals NHS Trust
Royal Surrey County Hospital NHS Foundation TrustSheffield Teaching Hospitals NHS Foundation Trust
Surrey and Sussex Healthcare NHS TrustImperial College Healthcare NHS TrustPoole Hospital NHS Foundation Trust
East Sussex Healthcare NHS TrustUniversity College London Hospitals NHS Foundation Trust
Mid Essex Hospital Services NHS TrustLuton and Dunstable Hospital NHS Foundation TrustCountess of Chester Hospital NHS Foundation Trust
East Lancashire Hospitals NHS TrustUnited Lincolnshire Hospitals NHS Trust
Mid Cheshire Hospitals NHS Foundation TrustRoyal Cornwall Hospitals NHS Trust
York Teaching Hospital NHS Foundation TrustRoyal United Hospital Bath NHS Trust
The Leeds Teaching Hospitals NHS TrustBarts Health NHS Trust
Plymouth Hospitals NHS TrustThe Pennine Acute Hospitals NHS Trust
Southend University Hospital NHS Foundation TrustCambridge University Hospitals NHS Foundation Trust
Warrington and Halton Hospitals NHS Foundation TrustUniversity Hospitals of Leicester NHS Trust
Norfolk and Norwich University Hospitals NHS Foundation TrustNottingham University Hospitals NHS Trust
Blackpool Teaching Hospitals NHS Foundation TrustNorth Bristol NHS Trust
The Shrewsbury and Telford Hospital NHS TrustOxford University Hospitals NHS Trust
Calderdale and Huddersfield NHS Foundation TrustGloucestershire Hospitals NHS Foundation Trust
Western Sussex Hospitals NHS TrustThe Royal Wolverhampton NHS Trust
Wrightington, Wigan and Leigh NHS Foundation TrustThe Christie NHS Foundation Trust
University Hospitals Bristol NHS Foundation TrustHampshire Hospitals NHS Foundation Trust
University Hospital Southampton NHS Foundation Trust
16
All men should have access to a specialist nurseMen really value access to a specialist nurse (also referred to as a Clinical Nurse Specialist (CNS)) who can help to support them and co-ordinate care through their prostate cancer journey. However, variation exists in men having access to a CNS and being able to contact them. On average, 88% of men with prostate cancer in England reported that they were given the name of the CNS in charge of their care, with the poorest scoring Trust being Calderdale and Huddersfield NHS Foundation Trust, where only 64% of men with prostate cancer were given the name of their CNS (1). Only in 5 Trusts across England reported were 100% of men with prostate cancer were given the name of a CNS (1).
In 2011, a census of the CNS workforce in England (4) found that there are 357 Urology (majority of cases will be prostate) CNS Macmillan support posts compared to 554 Breast CNS Macmillan support posts in cancer practice. Of these, one Working Time Equivalent (WTE) Urology CNS will have a median of 176 new cases per year, compared to a Breast CNS WTE median of 79 new cases. This clearly shows the need for more CNS provision. The next CNS census is currently taking place and will be published later this year.
The Welsh CPES stated that cancer patients, of all tumour groups, who had access to a CNS were significantly more likely to be positive about their experience than those who did not have access to a CNS (2).
Being able to contact their CNS is also a key part of the support that men need. Indeed over three quarters of men in our 2012 ‘Men’s views of Quality Care’ survey stated that being given the name and contact details of a CNS was very important to them (5). There is a wide variation in prostate cancer patients’ experience of contacting their CNS across England. The poorest performing Trust was the Leeds Teaching Hospitals NHS Trust where only the 47% felt they were able to contact their CNS, whilst the best performing Trust was Buckinghamshire Healthcare NHS Trust (96%) (1). The average for prostate cancer patients in England was just under three quarters at 73% (1), compared to 83% in Scotland (3) and just below 80% for all cancer patients in Wales (2). So although the average figures are seemingly high, variation is still prevalent and needs to be addressed.
All men should receive seamless integrated care It is essential to men with prostate cancer that interactions between health and social care are seamless in order to ensure that they receive the best possible care. However, findings from the NCPES show that in the Royal Surrey County Hospital NHS Foundation Trust just 30% of men with prostate cancer were definitely given enough care and help from health/social services, compared to Poole Hospital NHS Foundation Trust where 100% of men with prostate cancer reported that they were (1). The average for prostate cancer patients in England was just 57%, and Wales even lower at 42% (2).
17
In summaryInequality: There are inconsistencies in the quality of care and support that men receive across the UK.
Our call: NHS England must ensure that measurable aspects of patient experience in low performing Trusts are brought into line with the best in England – for example, all men should have a detailed written care plan, an assigned Clinical Nurse Specialist, and the necessary information and support following a prostate cancer diagnosis. The Scottish Government must introduce a National Cancer Patient Experience Survey to identify and find solutions to issues faced by men with prostate and other cancers. In Wales, the Welsh Government should act on the recent Cancer Patient Experience Survey to address the often poor levels of support offered to men with prostate cancer. The Department of Health, Social Services and Public Safety (DHSSPS) in Northern Ireland will also need to listen to its own Cancer Patient Experience Survey when it is released to ensure that prostate cancer patients’ needs are addressed.
References1. Quality Health. Cancer Patient Experience Survey 2012-13 National Report [Internet]. 2013. Available from:
http://www.quality-health.co.uk/resources/surveys/national-cancer-experience-survey/2013-national-cancer-patient-experience-survey-reports/301-2013-national-cancer-patient-experience-survey-progr-amme-national-report/file
2. Wales Cancer Patient Experience Survey: National Report. Quality Health [Internet]. 2014. Available from: http://www.quality-health.co.uk/resources/surveys/welsh-cancer-experience-survey/2013-welsh-cancer-eperience-survey/wales-cancer-patient-experience-reports-english-language-versions/527-wales-cancer-patient-experience-survey-national-report-2013/file
3. Quality Health. Prostate Cancer UK Survey: The Views of Prostate Cancer Patients in Scotland. 2013. 4. Clinical Nurse Specialists in Cancer Care; Provision, Proportion and Performance. A census of the cancer
specialist nurse workforce in England 2011. National Cancer Action Team [Internet]. 2012. Available from: http://webarchive.nationalarchives.gov.uk/20130513211237/http:/ncat.nhs.uk/sites/default/files/NCAT%20Census%20of%20the%20Cancer%20Specialist%20Nurse%20Workforce%202011.pdf
5. Prostate Cancer UK. Men’s views on quality care in prostate cancer: What does good quality care mean for men with prostate cancer? [Internet]. 2012. Available from: http://prostatecanceruk.org/media/1559431/prostate_cancer_uk_quality_care_survey_report_june_2012.pdf
18
AgeAge is a risk factor for prostate cancerProstate cancer incidence is strongly related to age, with 9 out of 10 prostate cancer cases diagnosed in men aged 60 and over, and incidence rates at their highest for men between 70 and 74 years of age (1). Prostate cancer mortality rates are also higher in older men, with 73% of prostate cancer deaths in men aged 75 and over (2). In England, 5 year relative survival rates for prostate cancer ranged from 92% in 60-69 year olds to 60% in 80-99 year olds. The reason for the higher survival rates for men in their 50s and 60s is likely to be due to higher rates of PSA testing in this age group (3).
Age is just a numberAlthough across a population physical fitness may decrease with age, age is far from the only determinant of health. Men of the same age may have different co-morbidities, have been exposed to different environmental conditions affecting health, exhibit different levels of activity and have different lifestyles – all of which will affect their health. That’s why we believe that at every stage of a man’s prostate cancer journey, his personal circumstances, not just his age, must be taken into account.
DiagnosisThis is why decisions about whether to undergo PSA testing are framed in terms of life expectancy rather than age. The information provided to GPs on PSA testing as part of the Prostate Cancer Risk Management Programme states that, ‘PSA testing is not usually recommended for asymptomatic men with less than 10 years’ life expectancy’ (4). However, it is not clear what information GPs may take into account when estimating life expectancy.
We are concerned that average life expectancy might be used in decision making, rather than making an estimate based on an individual’s circumstances. Furthermore, we advocate for a system of informed choice where men can make a decision that is right for them, whatever their age, provided they have an opportunity to discuss the pros and cons of testing with their GP.
Treatment decisionsFor all men to be able to make a shared decision, they must have access to the information they need about their treatment options, and possible side effects. NICE Clinical Guideline 175 Prostate cancer: diagnosis and treatment (5) states that clinicians should:
‘Adequately inform men with prostate cancer and their partners or carers about the effects of prostate cancer and the treatment options on their sexual function, physical appearance, continence and other aspects of masculinity. Support men and their partners or carers in making treatment decisions, taking into account the effects on quality of life as well as survival.’
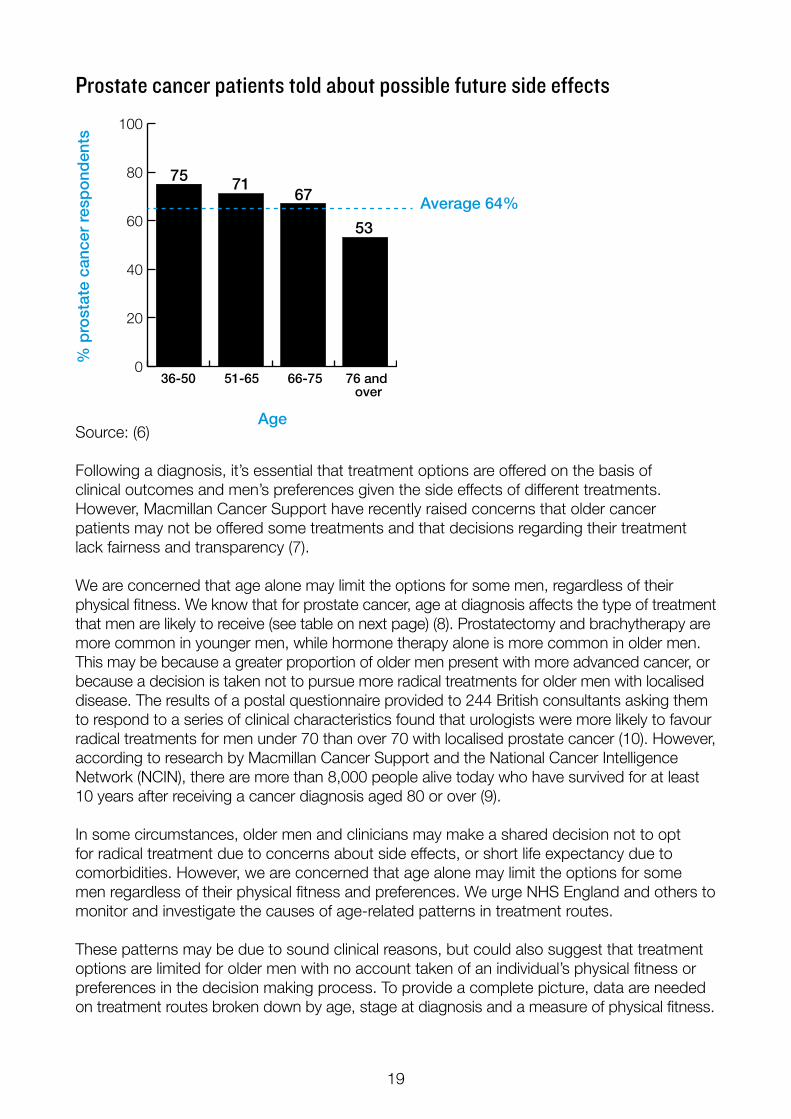
Despite this, the 2013 NCPES found that the extent to which prostate cancer patients are told about side effects of treatment varies according to age (6). Only 53% of prostate cancer patients aged 76 and over were told about side effects that could affect them in the future, compared with 71% of prostate cancer patients aged 51-65 (see figure opposite).
19
Prostate cancer patients told about possible future side effects
Source: (6)
Following a diagnosis, it’s essential that treatment options are offered on the basis of clinical outcomes and men’s preferences given the side effects of different treatments. However, Macmillan Cancer Support have recently raised concerns that older cancer patients may not be offered some treatments and that decisions regarding their treatment lack fairness and transparency (7).
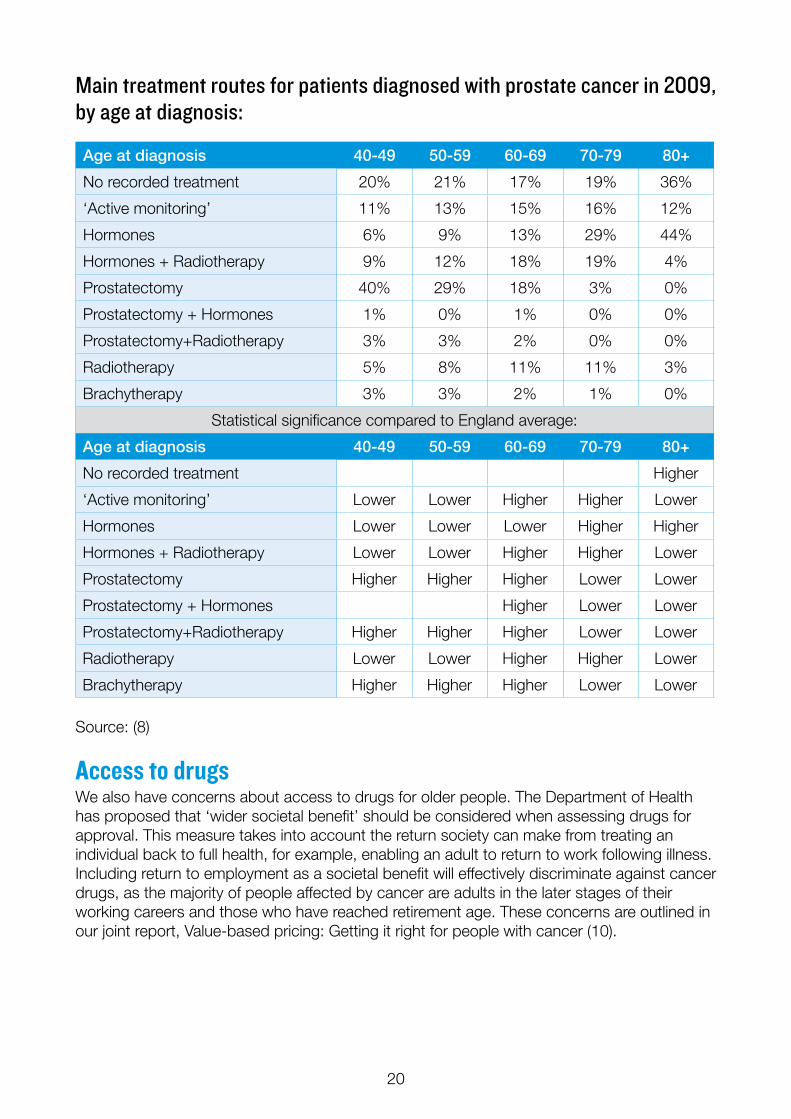
We are concerned that age alone may limit the options for some men, regardless of their physical fitness. We know that for prostate cancer, age at diagnosis affects the type of treatment that men are likely to receive (see table on next page) (8). Prostatectomy and brachytherapy are more common in younger men, while hormone therapy alone is more common in older men. This may be because a greater proportion of older men present with more advanced cancer, or because a decision is taken not to pursue more radical treatments for older men with localised disease. The results of a postal questionnaire provided to 244 British consultants asking them to respond to a series of clinical characteristics found that urologists were more likely to favour radical treatments for men under 70 than over 70 with localised prostate cancer (10). However, according to research by Macmillan Cancer Support and the National Cancer Intelligence Network (NCIN), there are more than 8,000 people alive today who have survived for at least 10 years after receiving a cancer diagnosis aged 80 or over (9).
In some circumstances, older men and clinicians may make a shared decision not to opt for radical treatment due to concerns about side effects, or short life expectancy due to comorbidities. However, we are concerned that age alone may limit the options for some men regardless of their physical fitness and preferences. We urge NHS England and others to monitor and investigate the causes of age-related patterns in treatment routes.
These patterns may be due to sound clinical reasons, but could also suggest that treatment options are limited for older men with no account taken of an individual’s physical fitness or preferences in the decision making process. To provide a complete picture, data are needed on treatment routes broken down by age, stage at diagnosis and a measure of physical fitness.
0
20
40
60
80
100
Average 64%
36-50 51-65 66-75 76 and over
Age
% p
rost
ate
canc
er r
esp
ond
ents
75 7167
53
20
Main treatment routes for patients diagnosed with prostate cancer in 2009, by age at diagnosis:
Source: (8)
Access to drugsWe also have concerns about access to drugs for older people. The Department of Health has proposed that ‘wider societal benefit’ should be considered when assessing drugs for approval. This measure takes into account the return society can make from treating an individual back to full health, for example, enabling an adult to return to work following illness. Including return to employment as a societal benefit will effectively discriminate against cancer drugs, as the majority of people affected by cancer are adults in the later stages of their working careers and those who have reached retirement age. These concerns are outlined in our joint report, Value-based pricing: Getting it right for people with cancer (10).
Age at diagnosis 40-49 50-59 60-69 70-79 80+
No recorded treatment 20% 21% 17% 19% 36%
‘Active monitoring’ 11% 13% 15% 16% 12%
Hormones 6% 9% 13% 29% 44%
Hormones + Radiotherapy 9% 12% 18% 19% 4%
Prostatectomy 40% 29% 18% 3% 0%
Prostatectomy + Hormones 1% 0% 1% 0% 0%
Prostatectomy+Radiotherapy 3% 3% 2% 0% 0%
Radiotherapy 5% 8% 11% 11% 3%
Brachytherapy 3% 3% 2% 1% 0%
Statistical significance compared to England average:
Age at diagnosis 40-49 50-59 60-69 70-79 80+
No recorded treatment Higher
‘Active monitoring’ Lower Lower Higher Higher Lower
Hormones Lower Lower Lower Higher Higher
Hormones + Radiotherapy Lower Lower Higher Higher Lower
Prostatectomy Higher Higher Higher Lower Lower
Prostatectomy + Hormones Higher Lower Lower
Prostatectomy+Radiotherapy Higher Higher Higher Lower Lower
Radiotherapy Lower Lower Higher Higher Lower
Brachytherapy Higher Higher Higher Lower Lower
21
Age-appropriate support needs Prostate Cancer UK recently commissioned research into the differential needs of men with prostate cancer at different life stages, and this work found that age influences the needs, priorities and preferences of men with prostate cancer (11).
Younger men were more likely to perceive diagnosis and treatment as having a larger impact on their lives than older men. In particular, they saw ED, and subsequent effect on sex life, as having a more significant effect on their lives. Younger men were also more likely to be concerned about the impact of the condition and its treatment on their careers. They tended to be less deferential toward doctors, and more likely to go online to research treatment options.
Older men tended to see urinary incontinence as having a more significant impact on their lives than ED. As they were more often retired, they were less concerned about the effect of prostate cancer on their careers. Older men tended to be more reluctant to express their need for support, often only talking about these needs after prompting. Their preference tended to be to access information through leaflets and books, rather than online.
This shows that although men of all ages should have access to the same standards of information and care, health professionals and service providers should be mindful of the fact that men at different stages of their lives may require tailored support.
Older people deserve quality careThe aim of the English national cancer strategy, Improving Outcomes: a strategy for cancer (12) was to help the NHS deliver cancer services that are amongst the best in the world. The number of men diagnosed with prostate cancer is predicted to increase by almost 70% between 2007 and 2030 (13), and many of these will be older men. Therefore, if the Government’s ambition is to be realised, it is essential that older men with prostate cancer are given access to high quality treatment and care. This is acknowledged in the Department of Health report: The impact of patient age on clinical decision making (14), which states that, ‘If we are to improve cancer outcomes, it is therefore important that we do all that we can to ensure that older people are able to benefit from the most appropriate treatment, care and support’.
Men must not be denied quality care on the basis of their age.
In summaryInequality: Older men diagnosed with prostate cancer are far less likely to be told about side effects of treatment, and at times have fewer treatment options offered to them, than younger men. It is not clear that treatment pathways are based on a person’s fitness and preferences rather than their age alone.
Our call: NHS England, NHS Wales, the Scottish Government and Health and Social Care (HSC) in Northern Ireland should ensure that older men are not denied treatments on the basis of their age, and that they are given information about possible treatment side effects.
22
References1. Cancer Research UK. Prostate cancer incidence statistics: By Age (2009-2011) [Internet]. 2014.
Available from: http://www.cancerresearchuk.org/cancer-info/cancerstats/types/prostate/incidence/#age2. Cancer Research UK. Prostate cancer mortality statistics: By Age (2009-2011) [Internet]. 2013.
Available from: http://www.cancerresearchuk.org/cancer-info/cancerstats/types/prostate/mortality/#By3. Cancer Research UK. Prostate cancer survival statistics: By Age (2005-2009) [Internet]. 2012.
Available from: http://www.cancerresearchuk.org/cancer-info/cancerstats/types/prostate/survival/#By4. Burford D, Kirby M, Austoker J. Advising men about the PSA test for prostate cancer [Internet]. 2009.
Available from: http://www.cancerscreening.nhs.uk/prostate/prostate-summary-sheet.pdf5. National Institute for Health and Care Excellence. Prostate cancer: Diagnosis and treatment. NICE clinical
guideline 175 [Internet]. 2014 [cited 2013 Apr 25]. Available from: http://www.nice.org.uk/guidance/CG1756. Quality Health. Cancer Patient Experience Survey 2012-13 National Report [Internet]. 2013. Available from:
http://www.quality-health.co.uk/resources/surveys/national-cancer-experience-survey/2013-national-cancer-patient-experience-survey-reports/301-2013-national-cancer-patient-experience-survey-progr-amme-national-report/file
7. brap for Macmillan Cancer Support. ‘Walking into the unknown’ - Survivors and carers speak out on discrimination and inequality in cancer care services [Internet]. 2011. Available from: http://www.macmillan.org.uk/Documents/AboutUs/Health_professionals/OlderPeoplesProject/Walkingintotheunknown.pdf
8. National Cancer Intelligence Network. Treatment Routes in Prostate Cancer Urological Cancers SSCRG [Internet]. 2012. Available from: http://www.ncin.org.uk/view?rid=1260
9. Macmillan Cancer Support and the NCIN. 130,000 people diagnosed at 65 or over survive cancer for at least a decade [Internet]. 2014 [cited 2014 May 13]. Available from: http://www.macmillan.org.uk/Aboutus/News/Latest_News/130,000peoplediagnosedat65oroversurvivecancerforatleastadecade.aspx#.
10. Prostate Cancer UK. Value-based pricing: Getting it right for people with cancer [Internet]. 2012 [cited 2013 May 10]. Available from: http://prostatecanceruk.org/media/1633387/1513_value-based_pricing_report_for_print.pdf
11. BritainThinks. Findings from qualitative research carried out by BritainThinks. The total sample size was 53 adults affected by prostate cancer across the UK (including 8 partners of men with prostate cancer). The fieldwork was undertaken between 5th February and 13th March 2014, comprising telephone interviews, focus groups and online qualitative research. 2014.
12. Department of Health. Improving Outcomes: A Strategy for Cancer [Internet]. 2011. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213785/dh_123394.pdf
13. Mistry M, Parkin DM, Ahmad AS, Sasieni P. Cancer incidence in the United Kingdom: projections to the year 2030. Br J Cancer. 2011 Nov 22;105(11):1795–803.
14. Department of Health. The impact of patient age on clinical decision-making in oncology [Internet]. 2012. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/215155/dh_133095.pdf

23
24
Access to treatmentsMen with prostate cancer should have access to the best available treatments. The current system needs to be reformed to ensure they receive this. Treatment options for men with prostate cancer are limited due to historical underfunding of prostate cancer research and the time taken for new treatments to be approved. In 2012, abiraterone for use after chemotherapy was the first drug to have been approved for advanced prostate cancer in 12 years. As health budgets are ever more squeezed across the UK, new treatments for prostate cancer face added hurdles to being approved. Access to the best treatments ultimately leads to improvements in overall survival, which is important in helping to realise the Westminster Government’s ambition to deliver cancer services that are amongst the best in the world. Since few treatments currently exist for prostate cancer, it is essential that new innovations are made available to men if they are proven to be effective.
In the UK, the National Institute for Health and Care Excellence (NICE) and the Scottish Medicines Consortium (SMC) decide whether new treatments for prostate cancer can be made available to men. In 2012, Prostate Cancer UK led a successful and award-winning campaign for the use of abiraterone on the NHS – despite its initial rejection. Following this, new treatments have come forward which could offer more choice and hope – particularly to those men who are approaching the end of their lives.
It is important that decisions about making treatments available to men who are running out of options are made in a fair and transparent manner, but we are worried that this is not happening. For example, the SMC has made decisions on whether to approve or reject new treatments with limited opportunity for input from patients and patient organisations as their meetings have been held in private. At the time of writing, several drugs for advanced prostate cancer, offering men the prospect of precious extra months to spend with loved ones, had been considered by NICE and the SMC.
In the case of enzalutamide, a hormone therapy treatment, NICE first announced that the drug should only be made available for those men who had not previously received the drug abiraterone, before finally deciding that this was outside the scope of the review. The SMC recommended that the drug was made available in Scotland without restriction. We are concerned that imposing restrictions based on previous treatments that men have received sets a dangerous precedent and could deny men approaching the end of their lives another option when all else has failed.
We have also seen other treatments rejected by NICE, such as cabazitaxel and radium-223, on the basis of cost and lack of data in comparison with other treatments – this shows that pharmaceutical companies also have a responsibility to provide the evidence necessary to NICE in order that they can make a full evidence-based assessment. There must also be an acceptance that drugs should be reasonably priced in order to stand a better chance of being approved.
The Cancer Drugs Fund (CDF) in England has been established as an interim solution to the cost barrier associated with new cancer treatments. While the CDF is in effect, it remains the only hope for many patients wishing to access innovative drugs that cannot be afforded by the NHS in England. However, we do not feel that a temporary measure, such as the CDF, addresses long-term gaps in provision for cancer drugs. Additionally, it is not fair that only men in England should have access to certain cancer drugs while men in other parts of the UK
25
cannot access them. We want all men with prostate cancer to be able to access the drugs and treatments that their doctor believes will be beneficial to them, no matter where they live.Some of the examples above highlight that, despite advances in treatments for prostate cancer, men are still unable to access all available licensed options. As advances in prostate cancer treatments steadily increase, it would be a travesty if men in the UK were unable to access them on the NHS.
A system fit for purpose – taking account of what matters most to patientsWe do not believe the current system for making cancer drugs available on the NHS is fit for purpose. What is required is a system that takes better account of the current lack of approved treatments for prostate cancer.
Since the Government first floated the idea of Value Based Pricing (VBP) in 2010, there has been much debate about the question of value, and little consultation with patients and patient organisations. In 2012, Prostate Cancer UK led a piece of work looking at VBP and what people affected by cancer believe value should mean to them. Our report highlights what people affected by cancer see as their priorities when assessing the value of new drugs (1). In addition to placing a high value on drugs which offer clear clinical benefits, our research shows that people value drugs which provide quality of life improvements such as reducing pain and fatigue. People affected by cancer have also expressed their belief that drugs which give people nearing the end of their lives precious extra time should be given a high value. The report also identifies the increasing worry about focusing on the value of the societal benefits of drugs.
Prostate Cancer UK is concerned that, if implemented, the measures put forward by the Department of Health in their terms of reference to NICE (2) will mean older people will lose out due to wider societal benefit favouring those of working age – with no recognition of the contribution older people have made over their own working lives. The proposals would disadvantage many people with cancer who may have already retired, are too unwell to ever re-enter the workforce, or are children or young people still in education or training.
In March 2014 NICE launched a public consultation seeking views on two new areas they are proposing to add to their technology process guidance – burden of illness (looking at the loss in quality and length of life) and wider societal impact (looking at the loss of a person’s capacity to engage in society as a result of living with a disease or condition). NICE has proposed incorporating end of life criteria within the burden of illness measures. We are concerned that removal of end of life measures as direct criteria may lead to new prostate cancer treatments not being approved in the future.
Communication of the Prostate Cancer Risk Management ProgrammeAs identified earlier, men aged 50 and over have the right to make an informed choice about whether to have a PSA test under the Prostate Cancer Risk Management Programme (PCRMP) (3). Currently, this is not effectively communicated and used in primary care so that men can make this choice and know their risks.
26
Erectile dysfunction guidelinesAgain as we highlighted earlier, there are no national guidelines on the management of ED. A number of guidelines have been produced by professional organisations, including the British Society for Sexual Medicine (4), but none of these has the same weight and influence as guidelines produced by NICE or the equivalents in the devolved nations. Therefore, there is an urgent need for a review and update of the current guidance for ED given that this is a major side effect following treatment for prostate cancer.
Emerging best practiceIt is important that men are able to access the best standards of treatment as soon as there is good evidence of efficacy. For example, there is an emerging body of evidence about the diagnostic benefits of using multiparametric MRI (magnetic resonance imaging) for ruling some men out of needing unnecessary biopsies (5). A clinical trial is underway that will explore this further (6), but in the meantime there is variation in clinical practice (7). Where robust clinical trial data is published between reviews of clinical guidance, it is important that the necessary steps are taken to ensure that men everywhere can benefit. This may require consideration of training, infrastructure and equipment.
In summaryInequality: Not all men in the UK have access to the information they need to make an informed choice about the PSA test, or about the best treatments or aftercare support for prostate cancer, especially for side effects such as ED.
Our call: Commissioning and regulatory authorities should take urgent steps to ensure that the best treatments and diagnostics are available across the UK. For example, NICE must ensure that clear guidance is provided to allow men to access treatments for advanced cancer; SMC must ensure greater patient participation and transparency in their decision making; Health Departments in all countries of the UK must urgently review and update the current prescribing guidance for erectile dysfunction; and the Prostate Cancer Risk Management Programme should be better communicated and used in primary care across the UK.
References1. Prostate Cancer UK. Value-based pricing: Getting it right for people with cancer [Internet]. 2012 [cited 2013
May 10]. Available from: http://prostatecanceruk.org/media/1633387/1513_value-based_pricing_report_for_print.pdf
2. Department of Health. Value-Based Pricing terms of reference [Internet]. 2013. Available from: http://www.nice.org.uk/proxy/?sourceUrl=http%3A%2F%2Fwww.nice.org.uk%2Faboutnice%2Fhowwework%2Fdevnicetech%2FDevelopmentWorkForValueBasedPricing.jsp%3Fdomedia%3D1%26mid%3D9A46903F-A8A3-2090-57684CA0D69C6E1D
3. Burford D, Kirby M, Austoker J. Prostate Cancer Risk Management Programme information for primary care; PSA testing in asymptomatic men. Evidence document. NHS Cancer Screening Programmes [Internet]. 2010. Available from: http://www.cancerscreening.nhs.uk/prostate/pcrmp-guide-2.html
4. British Society for Sexual Medicine. Guidelines on the management of erectile dysfunction [Internet]. 2013. Available from: http://www.bssm.org.uk/downloads/BSSM_ED_Management_Guidelines_2013.pdf
5. Moore CM, Robertson NL, Arsanious N, Middleton T, Villers A, Klotz L, et al. Image-guided prostate biopsy using magnetic resonance imaging-derived targets: a systematic review. Eur Urol. 2013 Jan;63(1):125–40.
6. MRC Clinical Trials Unit. PROMIS - Prostate MRI Imaging Study: Evaluation of Multi-Parametric Magnetic Imaging in the Diagnosis and Characterisation of Prostate Cancer [Internet]. [cited 2014 May 22]. Available from: http://icon8trial.org/research_areas/study_details.aspx?s=126
7. National Institute for Health and Care Excellence. Prostate cancer: Diagnosis and treatment. NICE clinical guideline 175 [Internet]. 2014 [cited 2013 Apr 25]. Available from: http://www.nice.org.uk/guidance/CG175
27
28
2640
Prostate Cancer UK is a registered charity in England and Wales (1005541) and in Scotland (SC039332). Registered company 2653887.