Embed Size (px)
Citation preview

Memory functioning in patients with unilateral temporal lobe epilepsy: Neuroimaging indicators of functional
integrity in the hippocampus and beyond.
by
Alexander Barnett
A thesis submitted in conformity with the requirements for the degree of Master of Arts
Department of Psychology University of Toronto
© Copyright by Alexander Barnett 2012

ii
Memory functioning in patients with unilateral temporal lobe
epilepsy: Neuroimaging indicators of functional integrity in the
hippocampus and beyond.
Alexander Barnett
Master of Arts
Department of Psychology
University of Toronto
2012
Abstract
Temporal lobe epilepsy (TLE) is a common form of intractable epilepsy that can be treated with
surgical resection of the epileptogenic medial temporal lobe tissue, specifically the hippocampus.
This resection can lead to a variable degree of memory deficit and considerable research has
been directed at identifying predictors of these deficits. This thesis explores the relationship
between structural predictors and functional predictors in TLE. I looked at fMRI activation
asymmetry produced by a scene encoding task as well as volume asymmetry ratios within the
hippocampus and the relationship of these predictors to memory performance in patients with
TLE. Mediation analysis was performed according to Baron and Kenny (1986) and showed that
fMRI activation asymmetry mediated the relationship between volume asymmetry and memory
asymmetry in patients with TLE. This suggests that activation asymmetry may be a preferred
variable for assessing functional adequacy in the medial temporal region.

iii
Acknowledgments
First and foremost I would like to acknowledge Dr. Mary Pat McAndrews for all of her
mentorship and guidance throughout this thesis. I would also like to acknowledge Dr. Andy Lee
for his helpful comments and training that helped me better understand MTL anatomy. Finally, I
would like to acknowledge my lab mates Melanie Cohn, Irene Giannoylis, Conny McCormick,
Areeba Adnan, Marie St-Laurent and Massih Moayedi for their assistance in scanning patients
and with assistance performing analysis.

iv
Table of Contents
Chapter 1: Introduction 1
1 Predictors of Decline 3
1.1 Neuropsychological Testing 3
1.2 Neuroimaging 4
1.3 Multimodal 6
Chapter 2: Methods 10
1 Participants 10
2 Neuropsychological Testing 12
3 fMRI Data Acquisition 12
4 fMRI Task 13
5 Functional Data Processing 13
6 Data Analysis 14
7 Structural Data Analysis 16
8 Group Comparison 16
9 Neuroimaging Measures and Behaviour 17
Chapter 3: Results 19
1 Demographics 19
2 Task Activation 19
3 Asymmetry Ratios 22
4 Neuroimaging Measures and Behaviour 22
Chapter 4: Discussion 26

v
List of Tables Table 1 11
Table 2 24

vi
List of Figures Figure 1 15
Figure 2 18
Figure 3 20
Figure 4 21
Figure 5 23
Figure 6 25
Figure 7 27

Chapter 1 Introduction
Epilepsy is a prevalent neurological disorder. In 2001 the World Health Organization estimated
that approximately 50 million people worldwide were affected by epilepsy (Levav & Rutz,
2002). Temporal lobe epilepsy (TLE) specifically is one of the most common presentations of
this disorder (Bell, Lin, Seidenberg, & Hermann, 2011). Epilepsy is characterized by recurrent
seizures, but also involves a profile of cognitive deficits, the most apparent being memory.
Medication is prescribed to reduce the frequency of seizures, but within this population can
sometimes be ineffective (Kwan & Brodie, 2000). Surgical interventions have been able to
successfully eliminate or greatly reduce the occurrence of seizures in patients with TLE (Engel,
1993; Engel et al., 2003). This surgery involves the resection of the varying amounts of anterior
portion of the hippocampus and the amygdala. Despite the overwhelming success of these
surgical procedures, post-surgical memory declines are very common (Gleissner, Helmstaedter,
Schramm, & Elger, 2004; Hermann, Seidenberg, Haltiner, & Wyler, 1995; Martin et al., 1998).
The canonical example of this effect is the case of Henry Molaison, who was unable to form any
new long term memory following bilateral resection of the anterior hippocampus (Scoville &
Milner, 1957). Since surgical treatment involves the resection of critical memory structures,
particularly the hippocampus, post-surgical memory decline is highly prevalent and variable
(Bell & Davies, 1998; Chelune, 1995). The case of Henry Molaison launched an extensive body
of research investigating the relationship between the hippocampus and memory as well the
investigation of predictors of post-surgical memory change.
As part of standard procedure in epilepsy surgery centres, all patients undergo an
extensive battery of neuropsychological testing pre- and post-surgically which allows clinicians
to understand the specific deficits of this patient population. This battery of testing also provides

2
insight to determining laterality of functional deficits as these tests have been shown to correlate
with areas of brain dysfunction and seizure focus (Hermann, Wyler, Somes, Berry, & Dohan,
1992; Jones-Gotman et al., 2010; McAndrews & Cohn, 2012; Saling et al., 1993). Patients with
left unilateral TLE (LTLE) tend to have poor verbal memory performance presurgically
compared to healthy controls whereas patients with right unilateral TLE (RTLE) tend to show
poor visual memory compared to healthy controls (Jones-Gotman et al., 2010; McAndrews &
Cohn, 2012). Similar trends were initially observed in post-surgical neuropsychological testing,
revealing that surgical resection of the left anterior hippocampus and amygdala lead to verbal
memory decline, while resection of the right is more related to visual memory decline, though
the evidence is less robust for RTLE (Bell & Davies, 1998; R C Martin et al., 1998; Milner,
1974; Morris, Abrahams, & Polkey, 1995). This led to the material specificity theory, which
states that the left hippocampus (in individuals with left-language dominance, which is the
majority of the population) is responsible for verbal memory while the right hippocampus is
responsible for visual memory (Milner, 1968). This theory is considered to be one of the
foundations of this field of research and has been looked at in terms of behavioural
neuropsychology measures and neuroimaging (Delaney, Rosen, Mattson, & Novelly, 1980; U
Gleissner, Helmstaedter, & Elger, 1998; Golby et al., 2001; Hermann, Wyler, Richey, & Rea,
1987; R C Martin et al., 2001).
Anatomical pathology has also been characterized within this population by examining
excised and post-mortem hippocampi taken from patients with TLE. Patients with TLE are very
likely to show signs of hippocampal sclerosis (HS), which is characterized by cell loss and
synaptic reorganization in the hippocampus and is the most common lesion in patients with TLE
(Blümcke, Thom, & Wiestler, 2002; Shamim et al., 2004). This lesion has been shown to be
related to memory deficits, with HS associated with poorer memory scores (Hermann et al.,

3
1992; Kneebone, Lee, Wade, & Loring, 2007; Marques et al., 2007; Saling et al., 1993; Trenerry
et al., 1993) and, with the advent of MRI, HS is typically diagnosed pre-operatively (Berkovic et
al., 1991). Of importance, structural neuroimaging studies using MRI for region of interest (ROI)
volumetry and voxel-based morphometry have shown atrophy not only in the hippocampus, but
also in a broader extent of medial temporal lobe including parahippocampal gyrus, fornix,
amygdala and entorhinal cortex (Bernasconi, 2003; Bernasconi et al., 1999, 2001; Kuzniecky et
al., 1999). The literature focuses heavily upon hippocampal changes in patients with TLE, but
there are clearly structural differences that occur in the MTL.
1 Predictors of Memory Decline
1.1 Neuropsychological Testing
Since the variability of memory decline is so high, researchers and clinicians have focused on
identifying factors that affect or predict the degree of memory decline due to surgery (Bell et al.,
2011). One of the first trends noted was that there is an inverse relationship between preoperative
memory functioning and postoperative memory change, with higher pre-operative scores
associated with greater post-operative declines (Chelune, Naugle, Lüders, & Awad, 1991;
Elshorst et al., 2009; Helmstaedter & Elger, 1996; Hermann et al., 1995). Chelune, (1995)
looked at a sample of 181 patients with TLE and observed that higher verbal memory
presurgically on the Wechsler Memory Scale Revised (Wechsler, 1987) resulted in greater
postsurgical decline of verbal memory in patients LTLE. They also found that that higher visual
memory presurgically resulted in greater postsurgical decline of visual memory in patients with
RTLE. Chelune (1995) explains this by reasoning that if a patient has high presurgical
functioning they may have a greater amount of functioning to lose after surgical resection.

4
1.2 Neuroimaging
Neuroimaging advances provide additional opportunities for predictive markers of post-surgical
memory decline. Structural MRI has allowed us to examine hippocampal atrophy. As discussed
earlier, hippocampal sclerosis has been shown to relate to cognitive deficits (Hermann et al.,
1992; Marques et al., 2007; Saling et al., 1993) and thus MRI measures of presurgical structural
integrity of the hippocampus may relate to the post-surgical outcome of memory. Several studies
have linked hippocampal volume in patients with TLE to post-surgical memory change
(Kneebone et al., 2007; Martin et al., 2001; Martin et al., 2002; Mechanic-Hamilton et al., 2009).
The results indicate that larger ipsilateral volumes, indicating a higher degree of intact tissue, are
related to greater declines in memory post-surgery. These results are often best seen using
asymmetry ratios (AR) [contralateral volume – ipsilateral volume] / [contralateral volume +
ipsilateral volume] since ARs tend to provide a greater spread separating patients with LTLE and
RTLE (Mechanic-Hamilton et al., 2009). The understanding here is that if the epileptogenic
hippocampus has little atrophy then it is more likely to support memory processes as it does in
the healthy brain. Therefore, removal of a more intact and useful hippocampal piece will result in
greater decline.
Functional MRI (fMRI) has allowed researchers to examine the functional integrity of the
to-be-resected tissue. Studies have attempted to use memory tasks during fMRI to allow for
quantification of hippocampal activity. Analysis of this activity, which is taken as a measure of
functional integrity, has been linked with memory changes following surgery (Bonelli et al.,
2010; Mechanic-Hamilton et al., 2009; Rabin et al., 2004; Richardson et al., 2004; Richardson,
Strange, Duncan, & Dolan, 2006). Rabin et al. (2004) examined 35 unilateral TLE patients (20
RTLE, 15 LTLE) and 30 healthy controls. This group used a scene encoding task (Stern et al.,
1996) to elicit medial temporal lobe activation in participants. All subjects were shown a series

5
of novel visual scenes in block design with a control scene that was degraded and retiled.
Contrasts between novel scenes and the control block were created for each individual and
activation was extracted from the hippocampus in the left and right hemispheres. Activation was
used to make an asymmetry ratio using the formula [(Lactivity- Ractivity)/(Lactivity+Ractivity)]. This
method was also used for a larger ROI encompassing the hippocampus, parahippocampus and
fusiform (HPF ROI). The ARs created from the larger HPF ROI were shown to significantly
correlate with post-surgical change in visual memory in patients with RTLE such that patients
having more right activation compared to left activation showed greater post-surgical decline.
The authors did not find significant correlations in their LTLE patients however and attribute this
to the scene encoding potentially being more sensitive to right hemisphere dysfunction.
Richardson et al. (2004) examined 10 LTLE patients presurgically on a verbal encoding
task in which patients were presented with a list of words and asked to make “living” or
“nonliving” judgments on the words, though not asked to memorize the words in the scanner.
Following the scan patients were given a surprise memory test on the words and asked to make
recognition judgments on the words. This judgment involved subjects giving a recollection
response (R), a familiarity response (K), or a new response (N) as described by Tulving (1985).
Recognition responses that are associated with recollection responses specifically activate the
hippocampus compared to recognition responses associated with familiarity (Eldridge,
Knowlton, Furmanski, Bookheimer, & Engel, 2000). They then contrasted the words for each
subject labeled correctly as R against the words labeled correctly as K. Activation from this
contrast was then used to create “encoding asymmetry” indices for each subject by subtracting
left activation from right activation using a small volume correction on the hippocampus. The
researchers then were able to find that this presurgical encoding asymmetry was able to
significantly predict post-surgical memory decline. They found that the greater the activation in

6
the left compared to the right hippocampus was linked with larger declines in memory following
surgical resection of the anterior portion of the left hippocampus in these patients.
Much of the data relating presurgical measures to predicting memory outcome support a
model called the functional adequacy theory. This theory posits that the amount of memory
decline seen in patients with TLE postsurgery is dependent upon the presurgical integrity of the
to-be-resected tissue. If the tissue is intact, and functionally involved in memory processes, then
removal of this tissue will presumably cause a larger reduction in memory functioning than if the
tissue was atrophied and not functionally involved in memory (Chelune, 1995).
1.3 Multimodal
Several studies have attempted to use multimodal methods for predicting post-surgical memory
change in patients with TLE. Elshorst et al.(2009) looked at presurgical neuropsychological
memory scores, MRI grading of hippocampal integrity and WADA memory performance as
predictors for post-surgical memory change in 59 patients with LTLE. They used the California
Verbal Learning Test (CVLT) and the Rey Auditory Verbal Learning Test (RAVLT) as
determinants of memory change and as predictors. They also used a ranking for MTS which was
based on a combination of anatomical scans to identify size (T1-weighted) and MR signal
increase (T2-weighted scans) which are indicators of neural atrophy. Finally, patients underwent
an intracarotid amytal procedure (IAP) in which one hemisphere of the brain is anesthetized
while the other hemisphere is given a memory task. This is used to identify the ability of one
hemisphere without the assistance of the anesthetized hemisphere. Each patient was shown a
series of 18 objects to remember on a subsequent recognition test that took place after clearance
of the drug that include the original 18 objects with 36 lures. Scores for each hemisphere were
determined in a pass/fail manner whereby the patient had to recognize at least 60% of the items
encoded at optimal anesthetization. Elshorst et al. (2009) found that presurgical

7
neuropsychological memory best predicted post-surgical memory outcome along with MRI
classification of hippocampal atrophy to explain around 45% of the variance in memory change.
In contrast, memory as assessed via the IAP did no add any predictive power to explaining post-
surgical memory outcome.
Mechanic-Hamilton et al. (2009) looked at the relationship between neuropsychological
functioning and WADA with fMRI as well as examining (in a separate analysis) the predictive
power of hippocampal volume and fMRI activation with memory outcome following surgery.
The study examined 49 patients with TLE (21 LTLE, 24 RTLE, 4 bilateral) and 25 controls.
Participants performed a visual scene encoding task while in the MRI scanner. Scenes were
presented in a block design fashion, alternating a series of novel scenes in the encoding blocks
with a single randomly retiled scene in the control blocks. Participants performed a self-paced
forced choice recognition test following the scan. After surgery, the majority of patients returned
to perform an alternative version of the visual scene encoding task outside the scanner and a pre-
to post- recognition change score was calculated. Activation was calculated by contrasting novel
blocks against the control block. ROI analysis yielded voxel counts for the hippocampus and a
mask that included the hippocampus, parahippocampus cortex and fusiform gyrus (HPF). The
resultant voxel counts were used to create ARs using the formula (voxelcountContra –
voxelcountIpsi) / (voxelcountContra + voxelcountIpsi). These ARs were used as predictors for
changes in clinical neuropsychological measures from pre- to post- surgery. Mechanic-Hamilton
et al. (2009) also used signal change within the ROIs as predictors of changes in clinical
neuropsychological measures.
Hippocampal volumes were calculated by manual tracing using published guidelines
(Watson et al., 1992). Volumes were also used to create ARs. In addition to examining changes
on the scene task, the study included pre- and post-operative measures from clinical memory

8
tests. For verbal memory, tasks included the CVLT and the Logical Memory subtest of the
WMS-III as measures of verbal memory. To measure visuospatial memory, they used the Faces
and visual reproduction subtests of the WMS-III. They calculated change scores for each subtest
by subtracting presurgical scores from postsurgical scores.
This study demonstrated a correlation between fMRI activation in the hippocampus in the
left hemisphere of LTLE patients and memory change determined by scene recognition.
Activation ARs did not however relate to changes in neuropsychological measures of memory
following surgery in either patients with LTLE or those with RTLE. Volume ARs were able to
correlate with several of the neuropsychological measures of memory following surgical
resection. Interestingly and in accord with Elshorst et al (2009), the strongest predictor of post-
surgical memory change was pre-surgical clinical memory scores.
Although these results provide important information regarding predictive values of
preoperative functional and structural measures, the authors did not directly explore a
relationship between functional ARs and volumetric ARs. If volumetric ARs are presumed to
provide us with some index of structural integrity we would expect that this would reflect the
functionality of the tissue, whether it be that ipsilateral atrophy results in hypo-activation of the
afflicted tissue or that ipsilateral atrophy results in a hyper-activation of the afflicted tissue for
compensation. Indeed, there are important reasons to expect that there may be a mediating
relationship between functional and structural integrity such that by understanding how much
tissue is available, and how efficiently the tissue is being used, we can better understand the link
between the brain and memory. In the literature on functional neuroimaging in
neurodegenerative conditions, Dickerson et al. (2004) examined the relationship between clinical
impairment and functional activation in individuals with Mild Cognitive Impairment (MCI).
They found that greater impairment (patients with ‘severe’ rather than ‘milder’ symptoms; all of

9
them non-demented by clinical criteria) was linked with increased MTL activation. Furthermore,
those individuals who activated a larger extent of the MTL showed accelerated cognitive decline.
In a later study the investigators reported that older adults with MCI showed greater MTL
activation compared to controls, whereas those with Alzheimer’s Disease showed significantly
less MTL activation (Dickerson et al., 2005). This evidence was taken to demonstrate that
increased activation may be a compensatory mechanism or might reflect a pathophysiological
mechanism leading towards Alzheimer ’s disease (AD). The authors suggested that there may be
a transitional continuum between normal aging and AD in which individuals with early MCI
show increased activation compared to controls, but as damage accrues in the MTL resulting in
more severe deficits, MTL activation also decreases. Such a relationship between volume,
activation and impairment may exist in TLE and is the driving force behind this study. We,
however, are not looking for a transitional continuum between healthy brain function and
epilepsy since our patient population has intractable epilepsy. Rather, we are looking at the
continuum between patients that have milder deficits to severe deficits in memory domains.
In summary, this study intends to build off of past research to better understand how
neuroimaging measures relate to memory in TLE. As discussed earlier, several studies have
shown that patients with TLE tend to have decreased volume in medial temporal lobe regions
beyond the hippocampus, including parahippocampal gyrus, fornix, amygdala and entorhinal
cortex (Bernasconi et al., 2003; Kuzniecky et al., 1999). Therefore, this thesis will attempt to
look at activation and volume, not solely in the hippocampus but also the parahippocampal
gyrus. Not only will this thesis look at an extended view of the MTL, but also it will examine
both volume and functional activation and how they relate to memory in this clinical population.
With this in mind we will employ the use of a scene encoding task which has been shown to
produce robust activation in the hippocampus and parahippocampal gyrus (Stern et al., 1996)

10
within the MRI scanner to allow for visualization of MTL functionality. We hypothesize that the
functional integrity, as measured by weighted voxel count in our ROIs, will correlate
significantly with presurgical neuropsychological measures of memory. We also hypothesize
that volume measures for the hippocampus and parahippocampal gyrus will correlate with
presurgical neuropsychological measures of memory. Finally, this thesis proposes that measures
of MTL activation mediate the relationship between volume and memory. In the current study
we are using presurgical memory performance so that we may examine the relationship between
volume and activation with memory when the MTL is intact. The implications of understanding
the relationship between functional activation and volume extend beyond TLE and may help
explain phenomenon that occur other disease populations with altered hippocampal functioning
such as MCI, AD, or depression.
Chapter 2 Methods
1 Participants Twenty three patients with pharmacologically intractable unilateral TLE were recruited from the
Neuropsychology and Epilepsy Surgery program at Toronto Western Hospital. Thirteen
presented with RTLE (5 men, 7 women; mean age = 35.5 years, range = 22-58 years) and 11
presented with LTLE (4 men, 7 women; mean age = 36 years, range = 19-53 years). Seizure
focus was determined using scalp EEG, and (if necessary) intracranial EEG. Twelve controls
were also recruited (8 men, 4 women; mean age = 29.4 years, range = 23-38). Exclusion criteria
included any history of neurological disorders or severe head trauma. Consent was obtained from
all participants. A list of demographics can be found in Table 1.

11
Table 1 Group Demographics, range in brackets
Controls RTLE LTLE
Age (years) 29.4 (23-38) 35.5 (22-58) 36 (19-53)
Years of education 17.9 (10-26) 14.4 (8-20) 14.6 (10-20)
Gender
Female
Male
4
8
7
5
7
4
Seizure Duration -- 16.2 (4-39) 18.4 (3-32)

12
2 Neuropsychological Testing Patients were administered a standard neuropsychological battery as part of the clinic’s standard
pre-operative investigation which included several tests assessing learning/memory. These
include verbal and visual long term memory tests. Two verbal tests were available and included
the Rey Auditory Verbal Learning Test (RAVLT) and Warrington Recognition Memory Test for
words. The visual long term memory tests included the Rey Visual Design Learning Test
(RVDLT) and Warrington Recognition Memory Test for faces. These measures were used to
create behavioural ARs according to the formula [(Verbal memory – Visual memory)/(Verbal
memory + Visual memory)]. One behavioural AR was calculated using scores from the RAVLT
and the RVDLT (REY-AR) and one was calculated using scores from the Warrington memory
test for words and the Warrington memory test for faces (WARR-AR). These tests were used to
examine the relationship of recall (via REY-AR) and recognition (via WARR-AR) on other
neuroimaging measurements. Both are clinically relevant, but there is no consensus on which
may be superior for characterizing hippocampal function (McAndrews & Cohn, 2012).
3 fMRI Data Acquisition Data was collected on a 3-T Signa MR system (GE Medical Systems, Milwaukee WI). A high-
resolution 3D anatomic scan was collected first for visualization, normalization of fMRI data to a
common anatomic template and volumetric analysis (T1-weighted sequence, FOV 220mm, 146
slices, flip angle=12degree, TE=3ms, TR=8ms, 256 x 256 matrix, resulting in voxel size of
.85939 x .85939 x 1.0). Echo-Planar Imaging sequences (TE=20 ms, TR=2000 msec, 32 5mm
oblique slices angled to be orthogonal to the long axis of the hippocampus to maximize signal
and minimize partial volume effects in the MTL) were run during the 6 ½ min functional scan.

13
4 fMRI Task Participants performed a commonly used scene encoding task during an fMRI scan. While in the
scanner they passively viewed a series of 60 complex visual scenes for 3500ms each. Two of
these visual scenes were exposed repeatedly immediately prior to the fMRI run and were
presented 15 times each during the critical run to serve as ‘baseline’ trials while the other 30
were novel. Presentation order of scenes was randomized for each subject. Previous literature
suggests that hippocampal activation will be seen for the novel>repeated contrast (Stern et al.,
1996).
5 Functional Data Preprocessing Preprocessing was done using SPM8 (Statistical Parameter Mapping 8; Wellcome Department of
Imaging, London) run through Matlab 7.9 (Mathworks, Inc). The first three images of the
functional scan were dropped to remove acquisition artifact. Preprocessing first included
realignment of anatomical and functional scans to the anterior commissure and then co-
registration of the functional scans to the anatomical scan. The functional scans were then
realigned and unwarped to correct to scanner motion artifact and subject movement. The
anatomical scan was segmented into gray matter, white matter and cerebral spinal fluid. The
resulting parameter files of this segmentation were then used to normalize functional and
anatomical scans into MNI space using affine registration. Finally, the functional images were
smoothed using a full-width at half maximum Gaussian kernel to 8 x 8 x 8 mm resolution. Data
went through a high-pass filter to account for low-frequency drift. Each stimulus event was then
modeled by SPM8’s canonical haemodynamic response function.

14
6 Data Analysis Novel encoding scenes were contrasted against repeated events using a general linear model
(GLM) in SPM8 for each subject. The resulting contrast images were used for group level
analyses to compare LTLE vs. controls, RTLE vs. controls and LTLE vs. RTLE. Healthy
individuals were used as a positive control to ensure implementation of the scene encoding
paradigm was successful. Group differences between healthy controls and our patient groups
were performed to see global changes between healthy and disease state.
ROI masks derived from MARINA (Walter et al., 2003) were applied to each patient’s
contrast to find voxel counts and t-values at a threshold of p<0.15, uncorrected. This liberal
threshold was chosen to allow for an inclusive representation of activated voxels, while
excluding those that are very likely to be due to chance. The application of low thresholding for
this purpose has been applied in the past (Branco et al., 2006; Mechanic-Hamilton et al., 2009).
Individual masks were made for left and right hippocampus and left and right parahippocampus,
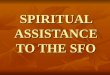
as shown in Figure 1. Voxel counts were weighted by their t-scores using these masks. Weighted
voxel counts have been shown to provide a better measure than voxel count alone (Chlebus et al.,
2007). These weighted voxel counts (WVC) were used to create activation ARs using the
formula [(Left WVC-Right WVC) / (Left WVC + Right WVC)]. Larger activation ARs indicate
greater activity in the left ROIs compared to right ROIs. An AR of zero indicates equal activity
bilaterally in the ROIs and negative ARs indicate greater activity in the right ROIs. This resulted
in two activation ARs for each patient (one for the hippocampus and one for the
parahippocampus). If there was no activation above threshold in either the left or right ROI, then
that data point was discarded for that patient. At the p<0.15 threshold there was 5 discarded (1
RTLE, 4 LTLE) for the hippocampal analysis.

15
Figure 1. These coronal MRI images depict the masks used for small volume correction in each patient to produce
activation asymmetry ratios (ARs). Right hippocampus in blue, left hippocampus in red, right parahippocampal
gyrus in purple, left hippocampal gyrus in green.

16
7 Structural Data Analysis FreeSurfer [Martino Center for biomedical Imaging, Harvard-MIT, Boston USA;
http://surfer.nmr.mgh.harvard.edu] was used to find volumetric values for the hippocampi, and
cortical thickness for the parahippocampal gyrus. Cortical thickness rather than volume is used
for the parahippocampal gyrus because the methods used by FreeSurfer tend to underestimate
cortical volume due to its surface based measurement procedures. FreeSurfer has been
previously described in detail (Fischl et al., 2004) and has been assessed in terms of validity and
accuracy (Dickerson et al., 2008; Han et al., 2006; Lee et al., 2006; Morey et al., 2010; Pardoe,
Pell, Abbott, & Jackson, 2009). Preprocessing included intensity normalization, removal of non-
brain tissue, Talaraich transformation and segmentation of tissue into grey matter, white matter
and cerebral spinal fluid. Subcortical structures are then segmented. For cortical thickness, the
white and grey matter boundaries are identified and the distance between the two surfaces are
calculated. The cortex is then automatically parcellated. Thickness is then calculated for a
structure based on this cortical parcellation. Structural ARs were calculated for the hippocampus
according to the formula [(left volume – right volume) / (left volume + right volume)] while ARs
for the parahippocampal gyrus used the formula [(leftthickness-
rightthickness)/(leftthickness+rightthickness)].
8 Group Comparison Independent samples t-tests were used to look at group differences between left and right TLE
patients on neuropsychological memory test ARs, activation ARs, and structural ARs using
SYSTAT 13 (Systat Software Inc. Chicago IL).

17
9 Neuroimaging Measures and Behaviour Mediation analysis was performed following the methods outlined in Baron and Kenny (1986)
using linear regression in SYSTAT 13 (Systat Software Inc. Chicago IL). The hippocampal
activation AR (acting as the predicted mediator) was regressed onto the hippocampal volume AR
(acting as the independent variable). Each behavioural AR (the dependent variables) was then
regressed onto the hippocampal volume ARs, separately. Finally, each behavioural AR was
regressed onto both the hippocampal activation ARs and the hippocampal volume ARs. A
mediation relationship could exist if there is a significant decrease in structural volume ARs
ability to predict memory once activation ARs are added into the regression model. A model of
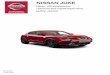
this is shown in Figure 2. In Figure 2, if c’ is significantly smaller than c, then this suggests a
mediation interaction is present. This significance can be assessed by testing the indirect effect as
outlined by Sobel (1982) which is as follows:
Where b is the slope of the mediator for predicting the dependent, in this case structural
AR predicting memory scores, sb is the standard error of the slope represented by b, a represents
the slope of the independent variable on the mediator, in this case structural AR on activation AR
and sa is the standard error of the slope represented by a. This test produces a z-score which can
be used to test for significance. Additionally, behavioural ARs scores were regressed onto the
parahippocampal activation AR and parahippocampal thickness ARs (separately) for each
subject to test the contribution of the parahippocampus to understanding memory presurgically.

18
A.
B.
Figure 2. A model of the interaction between structural volume, fMRI activation and memory. A. The influence of
volume on memory is shown as path c. B. Shows the model of influence provided a mediation relationship exists.
Volume now indirectly influences memory through activation and the direct path (c’) should be significantly smaller
than the previous direct path (c).
c
c’
a b

19
Chapter 3 Results
1 Demographics There was no difference in age between the RTLE, the LTLE group, and the control group,
F(32,2) = 1.63, p = 0.21. There was a significant group level difference in years of education
between patients with RTLE, patients with LTLE and healthy controls, F(32,2) = 3.5 , p = .042.
Post-hoc tests revealed no difference in years of education between patients with RTLE and
those with LTLE, t(21) = .16, p = .87, no difference in years of education between patients with
RTLE and healthy controls, t(22) = 2.2, p = .12 and no difference between patients with LTLE
and healthy controls, t(21) = 2.15, p = .13. There was no difference in seizure duration between
patients with RTLE and those with LTLE, t(21) = .384, p = .7. These demographic variables are
summarized in Table 1.
2 Task Activation As shown in Figure 3, all groups showed bilateral activation in occipital, fusiform gyrus,
parahippocampal gyrus and hippocampus (p<0.005, uncorrected). Group level analysis, shown in
Figure 4, controls activated bilateral parahippocampal to a greater extent than patients with
LTLE (p<0.005, uncorrected). There were no voxels in the MTL that activated greater in patients
with LTLE compared to healthy controls subjects. Controls had greater activation in the left
parahippocampal and compared to patients with RTLE (p<0.005, uncorrected). There were no
voxels in the MTL that activated more strongly in patients with RTLE compared to healthy
control subjects. Patients with RTLE had greater left parahippocampal and greater left
hippocampal activation compared to patients with LTLE patients (p<0.005, uncorrected). There

20
.
Figure3. Whole brain analysis of functional activation for the contrast novel > repeated scenes for LTLE, RTLE and
control groups at p<0.005, uncorrected, showing activation bilaterally in occipital, fusiform, parahippocampal and
hippocampal regions. Colour bars display t-values.
L
y=-28 z=-8 x=-28
LTLE novel>repeat
Control novel>repeat
L
y=-20 x=-28 z=-16
RTLE novel>repeat
L
y=28 x=-20 z=-10

21
Figure 4. Whole brain group analysis of functional activation for the contrast novel> repeated scenes contrasting
LTLE>RTLE, Controls>LTLE and Controls>RTLE at p<0.005, uncorrected. Colour bars display t-values.
RTLE>LTLE for novel>repeat
L
y=-20 x=-20 z=-20
Controls>LTLE for novel>repeat
y=-48 x=-32 z=-14
L
Controls>RTLE for novel>repeat
y=-32 x=-54 z=-8
L

22
were no voxels in the MTL that demonstrated greater activation in patients with LTLE compared
to those with RTLE at this threshold.
3 Asymmetry Ratios There was no significant difference for behavioural ARs between the LTLE and RTLE groups
Rey Test AR t(21) = 1.85, p = .078, Warrington test AR t(21) = 1.62, p = .12). These null results
are likely a function of small sample size as the Cohen’s d value for REY-AR was 0.79, which is
considered a large effect size, while the Cohen’s d value for the WARR-AR was 0.70 which is
considered to be medium-large. Turning to functional activation, patients with RTLE had
significantly more left lateralized activity compared to LTLE in the hippocampal activation ARs,
t(16) = 3.11, p = .007, but this was not observed for the parahippocampal activation ARs, t(16) =
1.56, p = 0.14. Patients with RTLE also had a significantly different hippocampal volume ARs
compared to patients with LTLE, t(21) = 4.97, p <0.001 but there was no significant difference
in parahippocampal thickness ARs, t(21) = 0.42, p = .68 (See Figure 5 and Table 2).
4 Neuroimaging Measures and Behaviour Hippocampal volume ARs were able to explain a significant proportion of variance in
hippocampal activation ARs, R2= .31, F(1,16) = 7.31, p = .016, establishing a link between the
independent variable and the mediator. This regression is shown in Figure 6A. Hippocampal
volume ARs were not able to significantly explain the variance in WARR-AR, R2 = .061,
F(1,21) = 1.37, p = .26, nor was it able to significantly explain the variance in REY-AR, R2=
.004, F(1,21) = .094, p = .762. This failed to produce a link between the independent variable
and the dependent variable. Hippocampal activation ARs were able to explain a significant
proportion of variance in the WARR-ARs (Figure 6B), R2 = .28, F(1,16) = 6.26, p = .024, but not
REY-ARs, R2 = .003, F(1,16) = .046, p = .833. This established the link between the mediator

23
RTLE LTLE-0.8
-0.4
0.0
0.4
0.8
Rey T
est
AR
RTLE LTLE-0.250
-0.125
0.000
0.125
0.250
Warr
ingto
n T
est
AR
RTLE LTLE-1.0
-0.5
0.0
0.5
1.0
Hip
po A
ctivation A
R
RTLE LTLE-1.0
-0.5
0.0
0.5
1.0
Para
Activation A
R
RTLE LTLE-0.50
-0.25
0.00
0.25
0.50
Hip
po V
olu
me A
R
RTLE LTLE-0.2
-0.1
0.0
0.1
0.2
Para
Thic
kness A
R
Figure 5. Behavioural ARs, activation ARs, hippocampal volume ARs and parahippocampal cortical thickness ARs
using “box-and-whisker” plots between patients with RTLE and LTLE. The centre horizontal line represents the
group median, while the edges of the box represent the 25th
and 75th
percentiles. The ends of the whiskers represent
the 1.5 interquartile range (IQR) of the distribution. Asterisks represent values that fall beyond the 1.5 (IQR).
denotes significant group differences (p < .05) in ARs after correcting for multiple comparisons.

24
Table 2. A summary of the means and standard deviations of the asymmetry ratios (ARs)
produced for the LTLE and RTLE groups.
RTLE LTLE
M SD M SD
REY-AR .22 .22 .054 .2
WARR-AR .073 .051 .037 .054
Hippo activation AR -.050 .24 -.458 .32
Hippo volume AR .11 .11 -.13 .12
Para activation AR .29 .21 .112 .282
Para thickness AR -.011 .031 -.019 .053

25
A
B
Figure 6. Regression models for the mediation analysis. A. hippocampal volume ARs shown as a predictor for
hippocampal activation ARs. B. Hippocampal activation ARs shown as a predictor for WARR-ARs. Patients who
did not show activation in both hemispheres were excluded.

26
and one of the behavioural ARs. When both hippocampal volume ARs and hippocampal
activation ARs were included as predictors of WARR-ARs the overall model failed to explain a
significant amount of variance in WARR-ARs, R2 = .29, F(1,16) = 3.04, p = .078. Activations
ARs were still significant predictors, β = .586, t(16) = 2.23, p = .042, and Volume ARs were not,
β = -.099, t(16) = -.378, p = .711.
Despite the failure to establish a link between volume ARs and a behavioural AR, we
proceeded to test the indirect effect of a mediation relationship using Sobel’s Test (1982), since
the link between volume ARs and behaviour has been reported previously in the literature
(Mechanic-Hamilton et al., 2009). According the Sobel’s Test (1982) there is a significantly
large indirect effect of this mediation model, z = 1.74, p = 0.041, which indicates that the effect
of volume on memory flows through activation. The model is summarized in Figure 7.
Parahippocampal activation ARs and Parahippocampal thickness ARs did not correlate
significantly with any behavioural asymmetry ratios.
Chapter 4 Discussion
This thesis examined the relationship between volume, functional activation during
encoding, and behavioural measures of memory. During the novel scene encoding task all
patients and healthy controls activated bilateral MTL regions including the hippocampus and the
parahippocampal gyrus. This was in support of previous work (Rabin et al., 2004; Stern et al.,
1996). Healthy controls showed greater parahippocampal activation bilaterally compared to
patients with LTLE. This could be due to the widespread structural changes in the MTL that are
seen in TLE (Bell et al., 2011; Bernasconi et al., 2003). The opposite contrast did not reveal

27
Hippo Volume AR
Hippo Activation AR
WARR-AR
r=.56*
controlling for Volume AR
r=.499*
Path c: r=.247
controlling for Activation AR Path c’ r=.054
Figure 7. A depiction of the proposed mediation model accompanied by path correlations showing a
significant correlation between volume ARs and activation ARs for path a, a significant correlations
between activation ARs and WARR-ARs when controlling for volume ARs in path b and a significant
reduction in path c to path c’.

28
any significant regions in the MTL that were activated in LTLE compared to controls.
Interestingly, healthy controls also had greater left parahippocampal activation compared to
patients with RTLE. Patients with RTLE did not activate any MTL regions to a greater degree
than healthy controls. Patients with RTLE activated the left hippocampus and parahippocampus
greater than patients with LTLE during novel scene encoding. This could be due to the fact that
patients with LTLE have damaged left hippocampi leading to weaker activation. There were no
regions in the MTL that were significantly more active in patients with LTLE compared to those
in RTLE, even at very liberal thresholds.
This study was unable to find a significant difference between neuropsychological
asymmetry ratios between patients with LTLE and RTLE though there was a trend shown in
which RTLE patients tended to perform better on verbal memory compared to visual memory
and LTLE patients tended to perform better on visual memory tests than verbal memory tests.
We would expect that an increase in sample size would produce a significant difference that is
shown in the literature in line with material specificity (Marques et al., 2007; McAndrews &
Cohn, 2012; Milner, 1968). The effect sizes between groups for both the Rey memory tests and
the Warrington memory tests were substantial suggesting that a larger sample would yield results
more consistent with the literature.
Functional activation asymmetry within the hippocampus during a novel scene encoding
task differed significantly between our RTLE and LTLE group. As predicted, patients with
LTLE displayed a greater proportion of right hippocampal activation compared to left
hippocampal activation, while patients with RTLE displayed a greater amount of left
hippocampal activation compared to right hippocampal activation. This is in support of previous
findings (Detre et al., 1998; Mechanic-Hamilton et al., 2009). However, there was not a
significant difference in parahippocampal activation asymmetry between patients with LTLE and

29
those with RTLE. Rather, there was a non-significant trend that showed patients with LTLE
preferentially activating the right parahippocampus compared to the left and patients with RTLE
preferentially activating the left parahippocampus compared to the right. Several studies have
included the parahippocampus in ROI analysis, but as a part of a large ROI including the
hippocampus and the fusiform (Mechanic-Hamilton et al., 2009; Rabin et al., 2004) but none
have included a separate mask for the parahippocampal gyri specifically. We expect that a larger
sample would reveal that a significant difference between these two patient groups does in fact
exist.
This study also saw a significant difference in hippocampal volume asymmetry between
patients with LTLE and those with RTLE. This is in line with past studies (Bernasconi et al.,
2003; Mechanic-Hamilton et al., 2009) and showed that patients with LTLE had smaller left
hippocampi compared to their right hippocampus and those with RTLE had smaller right
hippocampi compared to their left hippocampus. There was not a significant asymmetry in
parahippocampal thickness between patients with RTLE and those with LTLE. This could be due
to the extensive boundaries considered for parahippocampal cortex in thickness analysis. It has
been previously shown that parahippocampal atrophy may be more restricted to anterior portion,
specifically the entorhinal and to a lesser degree the perirhinal cortices whereas the posterior
portion of the parahippocampal cortex does not show much atrophy when comparing patients
with TLE to healthy controls (Bernasconi et al., 1999, 2003). Our boundaries for measuring
cortical thickness included entorhinal, perirhinal and posterior parahippocampal cortices together
as one measurement. This may have diluted any differences that may exist in this patient group.
Future studies would therefore be encouraged to use a finer method of examining
parahippocampal cortical measurements that differentiate entorhinal, perirhinal and posterior
parahippocampal cortices.

30
The results of this study also demonstrated that the link between hippocampal volume
and memory is mediated by hippocampal activation. The link between volume and memory was
not found to be significant in this study, but has been previously shown (Mechanic-Hamilton et
al., 2009; Reminger et al., 2004). Despite not finding a significant link between volume and
memory, the influence of hippocampal volume on memory was found to decrease significantly
following the introduction of hippocampal activation asymmetry. Hippocampal volume
asymmetry was correlated with hippocampal activation asymmetry, which in turn was correlated
with memory asymmetry in Warrington words and faces. This relationship leaves hippocampal
activation as the middle link between volume and memory. This finding represents a link that has
not previously been explored in the literature and suggests that the relationship between
hippocampal volume and memory is partially explained through the activation (extent and
magnitude in this case) that tissue is able to generate during encoding. This may suggest that
hippocampal activation asymmetry may be a better marker of hippocampal adequacy than
hippocampal volume is. Two individuals with TLE may both have significant ipsilateral
hippocampal damage, but if one of those individuals has activation biased to their ipsilateral side
and shows relatively unimpaired presurgical memory, that individual may be at greater risk of
post-surgical memory loss than their counterpart who may have activation biased more towards
the contralateral side. The first individual has a decrease in hippocampal volume, yet is still
using their ipsilateral hippocampus to its best ability, whereas the second individual has a
decrease in hippocampal volume, and is relying on their contralateral hippocampus, suggesting
that ipsilateral removal would not cause as much of a disruption.
There was very little overlap between volume asymmetry scores for patients with LTLE
and those with RTLE. This lack of variance however may restrict the ability of volume
asymmetry to correlate with memory. It may have better clinical utility therefore in serving to aid

31
in the assessment of seizure laterality. Conversely, activation asymmetry has a larger variance
that correlates strongly with memory asymmetry. This would allow activation asymmetry to
better assess presurgical functional adequacy of the to-be-removed hippocampus. According to
the functional adequacy theory (Chelune, 1995), individuals who demonstrate a higher degree of
hippocampal adequacy presurgically are at greater risk of post-surgical memory decline.
The relationship between MRI measures of structural and functional integrity is one that
has not been investigated extensively but has more recently become explored (Poppenk &
Moscovitch, 2011; Voets et al., 2012). Poppenk & Moscovitch (2011) looked at healthy controls
across multiple studies to find a relationship between posterior-anterior hippocampal volume
ratios and recollective memory. They went on to find that this relationship between hippocampal
volume and recollective memory was mediated by post-encoding resting-state connectivity of the
posterior hippocampus to precuneus, inferior parietal and lateral frontal cortex. Voets et al. 2012
used resting-state connectivity, voxel-based morphometry and diffusion tensor imaging (DTI) to
look at patients with TLE to identify voxel-wise associations between resting state connectivity
and white matter coherence (determined by fractional anisotropy from DTI). They found the
functional connectivity between parahippocampal cortex, frontal and temporal neocortex was
associated with white matter coherence in the pathways connecting these regions. Their overall
findings suggest that cortical atrophy and white matter coherence are associated with functional
connectivity. Now that neuroimaging has developed tools to look at structural integrity measures
via DTI, volumetry, voxel based morphometry and at functional integrity via activation
contrasts, functional connectivity and multivoxel pattern analysis, we are better prepared to
identify and exploit connections between structure integrity, activation and connectivity. Within
the hippocampus, we have shown a link between volume asymmetry and activation asymmetry

32
and this may generalize to other disorders that may have MTL disruption such as AD,
schizophrenia and depression.
This study attempted to find a link between activation asymmetry and thickness
asymmetry in the parahippocampal gyrus, but was unsuccessful. This may be explained through
having a somewhat small sample size, and having overly inclusive boundaries that would have
been better restricted to certain regions of parahippocampal gyrus such as entorhinal cortex.
Despite the failure of finding significant correlations or differences in parahippocampal regions,
I maintain that exploring parahippocampal parameters as potential predictors post-surgical
memory change may still be of interest, since parahippocampal cortex is also removed during
temporal lobectomy procedures. There have been changes in volume seen in regions of the
parahippocampal cortex (Bernasconi et al., 1999, 2001, 2003) some of which are independent of
hippocampal volume changes, specifically the entorhinal cortex. The entorhinal cortex is thought
to be a gate to the hippocampus and an independent change in the entorhinal cortex could
therefore affect memory performance. This study therefore suggests a more precise look at
entorhinal cortex structure and function measures as potential predictors of post-surgical memory
in future studies following this thesis.
Several limitations to this study exist. Firstly, all patients were using anticonvulsive
medication during all stages of the study. It is unclear as to how this medication may have
affected the memory performance or functional activation during fMRI scanning. For example,
we do not know how these medications may affect vasodilation which would ultimately alter the
BOLD signal. This limitation exists in most studies of this nature. The use of ARs may temper
part of this limitation because it measures a ratio of activation between the hemispheres. Also,
the control group used was not age matched with the patient sample. The control group however
was used to ensure proper task implementation, while the true results of this thesis focusses

33
specifically on differences between LTLE and RTLE groups and on correlations between the
neuroimaging measures with patient memory performance.
Future work should follow up on the reported patients following surgery, to correlate
post-surgical memory change with presurgical activation and volume asymmetries in both the
hippocampus and parahippocampal cortices.
The main goal of this thesis was to explore the relationship between volume, activation
and memory in patients with TLE as well as exploring any influence the parahippocampus may
have on memory. We discovered that activation asymmetry mediates the relationship between
volume asymmetry and memory asymmetry in patients with TLE. This is in line with recent
research that has shown that underlying brain processes mediate the relationship between volume
and memory (Poppenk & Moscovitch, 2011) and suggests the need for more structure-activation
based analyses, such as DTI and resting-state connectivity. Based on our findings we conclude
that hippocampal activation asymmetry is indeed a good predictor of hippocampal adequacy,
perhaps even more so than volume asymmetry. Despite our concerns about the independent
value of activation measures (given the patterns seen in MCI and AD), current results make us
more confident in interpreting regional activation as a viable ‘biomarker’.

34
References
Baron, R. M., & Kenny, D. a. (1986). The moderator-mediator variable distinction in social
psychological research: conceptual, strategic, and statistical considerations. Journal of
personality and social psychology, 51(6), 1173-82. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/3806354
Bell, B., & Davies, K. G. (1998). Anterior temporal lobectomy, hippocampal sclerosis, and
memory: recent neuropsychological findings. Neuropsychology review, 8(1), 25-41.
Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9585921
Bell, B., Lin, J. J., Seidenberg, M., & Hermann, B. (2011). The neurobiology of cognitive
disorders in temporal lobe epilepsy. Nature reviews. Neurology, 7(3), 154-64. Nature
Publishing Group. doi:10.1038/nrneurol.2011.3
Berkovic, S. F., Andermann, F., Olivier, A., Ethier, R., Melanson, D., Robitaille, Y., Kuzniecky,
R., et al. (1991). Hippocampal sclerosis in temporal lobe epilepsy demonstrated by
magnetic resonance imaging. Annals of neurology, 29(2), 175-82.
doi:10.1002/ana.410290210
Bernasconi, N., Bernasconi, A., Andermann, F., Dubeau, F., Feindel, W., & Reutens, D. C.
(1999). Entorhinal cortex in temporal lobe epilepsy: a quantitative MRI study. Neurology,
52(9), 1870-6. AAN Enterprises. Retrieved from
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation
&list_uids=10371536
Bernasconi, N., Bernasconi, A., Caramanos, Z., Antel, S. B., Andermann, F., & Arnold, D. L.
(2003). Mesial temporal damage in temporal lobe epilepsy: a volumetric MRI study of the
hippocampus, amygdala and parahippocampal region. Brain : a journal of neurology,
126(Pt 2), 462-9. doi:10.1093/brain/awg034
Bernasconi, N., Bernasconi, A., Caramanos, Z., Dubeau, F., Richardson, J., Andermann, F., &
Arnold, D. L. (2001). Entorhinal cortex atrophy in epilepsy patients exhibiting normal
hippocampal volumes. Neurology, 56(10), 1335-9. Retrieved from
http://www.neurology.org/content/56/10/1335.1.short
Blümcke, I., Thom, M., & Wiestler, O. D. (2002). Ammon’s horn sclerosis: a maldevelopmental
disorder associated with temporal lobe epilepsy. Brain pathology (Zurich, Switzerland),
12(2), 199-211. doi:10.1111/j.1750-3639.2002.tb00436.x
Bonelli, S. B., Powell, R. H. W., Yogarajah, M., Samson, R. S., Symms, M. R., Thompson, P. J.,
Koepp, M. J., et al. (2010). Imaging memory in temporal lobe epilepsy: predicting the
effects of temporal lobe resection. Brain : a journal of neurology, 133(Pt 4), 1186-99.
doi:10.1093/brain/awq006
Branco, D. M., Suarez, R. O., Whalen, S., O’Shea, J. P., Nelson, A. P., da Costa, J. C., & Golby,
A. J. (2006). Functional MRI of memory in the hippocampus: Laterality indices may be

35
more meaningful if calculated from whole voxel distributions. NeuroImage, 32(2), 592-602.
doi:10.1016/j.neuroimage.2006.04.201
Chelune, G. J. (1995). Hippocampal adequacy versus functional reserve: predicting memory
functions following temporal lobectomy. Archives of clinical neuropsychology : the official
journal of the National Academy of Neuropsychologists, 10(5), 413-32. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/14588901
Chelune, G. J., Naugle, R. I., Lüders, H., & Awad, I. A. (1991). Prediction of cognitive change
as a function of preoperative ability status among temporal lobectomy patients seen at 6-
month follow-up. Neurology, 41(3), 399-404. Retrieved from
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation
&list_uids=2006008
Chlebus, P., Mikl, M., Brázdil, M., Pazourková, M., Krupa, P., & Rektor, I. (2007). fMRI
evaluation of hemispheric language dominance using various methods of laterality index
calculation. Experimental brain research. Experimentelle Hirnforschung. Expérimentation
cérébrale, 179(3), 365-74. doi:10.1007/s00221-006-0794-y
Delaney, R. C., Rosen, A. J., Mattson, R. H., & Novelly, R. A. (1980). Memory function in focal
epilepsy: a comparison of non-surgical, unilateral temporal lobe and frontal lobe samples.
Cortex, 16(1), 103-117. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/6769639
Detre, J. A., Maccotta, L., King, D., Alsop, D. C., Glosser, G., D’Esposito, M., Zarahn, E., et al.
(1998). Functional MRI lateralization of memory in temporal lobe epilepsy. Neurology,
50(4), 926-32. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9566374
Dickerson, B. C., Fenstermacher, E., Salat, D. H., Wolk, D. a, Maguire, R. P., Desikan, R.,
Pacheco, J., et al. (2008). Detection of cortical thickness correlates of cognitive
performance: Reliability across MRI scan sessions, scanners, and field strengths.
NeuroImage, 39(1), 10-8. doi:10.1016/j.neuroimage.2007.08.042
Dickerson, B. C., Salat, D. H., Bates, J. F., Atiya, M., Killiany, R. J., Greve, D. N., Dale, A. M.,
et al. (2004). Medial temporal lobe function and structure in mild cognitive impairment.
Annals of neurology, 56(1), 27-35. doi:10.1002/ana.20163
Dickerson, B. C., Salat, D. H., Greve, D. N., Chua, E. F., Rand-Giovannetti, E., Rentz, D. M.,
Bertram, L., et al. (2005). Increased hippocampal activation in mild cognitive impairment
compared to normal aging and AD. Neurology, 65(3), 404-11.
doi:10.1212/01.wnl.0000171450.97464.49
Eldridge, L. L., Knowlton, B. J., Furmanski, C. S., Bookheimer, S. Y., & Engel, S. a. (2000).
Remembering episodes: a selective role for the hippocampus during retrieval. Nature
neuroscience, 3(11), 1149-52. doi:10.1038/80671
Elshorst, N., Pohlmann-Eden, B., Horstmann, S., Schulz, R., Woermann, F., & McAndrews, M.
P. (2009). Postoperative memory prediction in left temporal lobe epilepsy: the Wada test is

36
of no added value to preoperative neuropsychological assessment and MRI. Epilepsy &
behavior : E&B, 16(2), 335-40. Elsevier Inc. doi:10.1016/j.yebeh.2009.08.003
Engel, J. (1993). Update on surgical treatment of the epilepsies. Summary of the Second
International Palm Desert Conference on the Surgical Treatment of the Epilepsies (1992).
Neurology, 43(8), 1612-7. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/8102482
Engel, J., Wiebe, S., French, J., Sperling, M., Williamson, P., Spencer, D., Gumnit, R., et al.
(2003). Practice parameter: temporal lobe and localized neocortical resections for epilepsy:
report of the Quality Standards Subcommittee of the American Academy of Neurology, in
association with the American Epilepsy Society and the American Association of Neuro.
Neurology, 60(4), 538-47. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/12601090
Fischl, B., van der Kouwe, A., Destrieux, C., Halgren, E., Ségonne, F., Salat, D. H., Busa, E., et
al. (2004). Automatically parcellating the human cerebral cortex. Cerebral cortex (New
York, N.Y. : 1991), 14(1), 11-22. doi:10.1093/cercor/bhg087
Gleissner, U, Helmstaedter, C., & Elger, C. E. (1998). Right hippocampal contribution to visual
memory: a presurgical and postsurgical study in patients with temporal lobe epilepsy.
Journal of neurology, neurosurgery, and psychiatry, 65(5), 665-9. Retrieved from
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2170342&tool=pmcentrez&ren
dertype=abstract
Gleissner, Ulrike, Helmstaedter, C., Schramm, J., & Elger, C. E. (2004). Memory outcome after
selective amygdalohippocampectomy in patients with temporal lobe epilepsy: one-year
follow-up. Epilepsia, 45(8), 960-2. doi:10.1111/j.0013-9580.2004.42203.x
Golby, a J., Poldrack, R. a, Brewer, J. B., Spencer, D., Desmond, J. E., Aron, a P., & Gabrieli, J.
D. (2001). Material-specific lateralization in the medial temporal lobe and prefrontal cortex
during memory encoding. Brain : a journal of neurology, 124(Pt 9), 1841-54. Retrieved
from http://www.ncbi.nlm.nih.gov/pubmed/11522586
Han, X., Jovicich, J., Salat, D., van der Kouwe, A., Quinn, B., Czanner, S., Busa, E., et al.
(2006). Reliability of MRI-derived measurements of human cerebral cortical thickness: the
effects of field strength, scanner upgrade and manufacturer. NeuroImage, 32(1), 180-94.
doi:10.1016/j.neuroimage.2006.02.051
Helmstaedter, C., & Elger, C. E. (1996). Cognitive consequences of two-thirds anterior temporal
lobectomy on verbal memory in 144 patients: a three-month follow-up study. Epilepsia,
37(2), 171-80. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/8635428
Hermann, B. P., Seidenberg, M., Haltiner, a, & Wyler, a R. (1995). Relationship of age at onset,
chronologic age, and adequacy of preoperative performance to verbal memory change after
anterior temporal lobectomy. Epilepsia, 36(2), 137-45. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/7821270

37
Hermann, B. P., Wyler, a R., Richey, E. T., & Rea, J. M. (1987). Memory function and verbal
learning ability in patients with complex partial seizures of temporal lobe origin. Epilepsia,
28(5), 547-54. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/3653060
Hermann, B. P., Wyler, A. R., Somes, G., Berry, A. D., & Dohan, F. C. (1992). Pathological
status of the mesial temporal lobe predicts memory outcome from left anterior temporal
lobectomy. Neurosurgery, 31(4), 652-656; discussion 656-657. Retrieved from
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=med3
&AN=1407450
Jones-Gotman, M., Smith, M. L., Risse, G. L., Westerveld, M., Swanson, S. J., Giovagnoli, A.
R., Lee, T., et al. (2010). The contribution of neuropsychology to diagnostic assessment in
epilepsy. Epilepsy & behavior : E&B, 18(1-2), 3-12. Elsevier Inc.
doi:10.1016/j.yebeh.2010.02.019
Kneebone, A. C., Lee, G. P., Wade, L. T., & Loring, D. W. (2007). Rey Complex Figure: figural
and spatial memory before and after temporal lobectomy for intractable epilepsy. Journal of
the International Neuropsychological Society : JINS, 13(4), 664-71.
doi:10.1017/S1355617707070828
Kuzniecky, R., Bilir, E., Gilliam, F., Faught, E., Martin, R., & Hugg, J. (1999). Quantitative MRI
in temporal lobe epilepsy: evidence for fornix atrophy. Neurology, 53(3), 496-501.
Retrieved from http://www.neurology.org/cgi/content/abstract/53/3/496
Kwan, P., & Brodie, M. J. (2000). Early identification of refractory epilepsy. The New England
journal of medicine, 342(5), 314-9. doi:10.1056/NEJM200002033420503
Lee, J. K., Lee, J.-M., Kim, J. S., Kim, I. Y., Evans, A. C., & Kim, S. I. (2006). A novel
quantitative cross-validation of different cortical surface reconstruction algorithms using
MRI phantom. NeuroImage, 31(2), 572-84. doi:10.1016/j.neuroimage.2005.12.044
Levav, I., & Rutz, W. (2002). The WHO World Health Report 2001 new understanding--new
hope. (World Health Organization, Ed.)The Israel journal of psychiatry and related
sciences, 39(1), 50-6. World Health Organization. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/12013710
Marques, C. M., Caboclo, L. O. S. F., da Silva, T. I., Noffs, M. H. D. S., Carrete, H., Lin, K.,
Lin, J., et al. (2007). Cognitive decline in temporal lobe epilepsy due to unilateral
hippocampal sclerosis. Epilepsy & behavior : E&B, 10(3), 477-85.
doi:10.1016/j.yebeh.2007.02.002
Martin, R C, Sawrie, S. M., Knowlton, R. C., Bilir, E., Gilliam, F. G., Faught, E., Morawetz, R.
B., et al. (2001). Bilateral hippocampal atrophy: consequences to verbal memory following
temporal lobectomy. Neurology, 57(4), 597-604. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/11524466
Martin, R C, Sawrie, S. M., Roth, D. L., Gilliam, F. G., Faught, E., Morawetz, R. B., &
Kuzniecky, R. (1998). Individual memory change after anterior temporal lobectomy: a base

38
rate analysis using regression-based outcome methodology. Epilepsia, 39(10), 1075-82.
Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9776328
Martin, Roy C, Kretzmer, T., Palmer, C., Sawrie, S., Knowlton, R., Faught, E., Morawetz, R., et
al. (2002). Risk to verbal memory following anterior temporal lobectomy in patients with
severe left-sided hippocampal sclerosis. Archives of neurology, 59(12), 1895-901. Retrieved
from http://www.ncbi.nlm.nih.gov/pubmed/12470177
McAndrews, M. P., & Cohn, M. (2012). Neuropsychology in Temporal Lobe Epilepsy:
Influences from Cognitive Neuroscience and Functional Neuroimaging. Epilepsy Research
and Treatment, 2012, 1-13. doi:10.1155/2012/925238
Mechanic-Hamilton, D., Korczykowski, M., Yushkevich, P. A., Lawler, K., Pluta, J., Glynn, S.,
Tracy, J. I., et al. (2009). Hippocampal volumetry and functional MRI of memory in
temporal lobe epilepsy. Epilepsy & behavior : E&B, 16(1), 128-38.
doi:10.1016/j.yebeh.2009.07.012
Milner, B. (1968). Disorder of memory after brain lesions in man. Preface: material-specific and
generalized memory loss. Neuropsychologia, 6, 175-179.
Milner, B. (1974). Hemispheric specialization: scope and limits. In F. Schmitt & W. FG (Eds.),
The neurosciences: third study program (pp. 75–89). Massachusetts: MIT Press.
Morey, R. A., Selgrade, E. S., Wagner, H. R., Huettel, S. A., Wang, L., & McCarthy, G. (2010).
Scan-rescan reliability of subcortical brain volumes derived from automated segmentation.
Human brain mapping, 31(11), 1751-62. doi:10.1002/hbm.20973
Morris, R. G., Abrahams, S., & Polkey, C. E. (1995). Recognition memory for words and faces
following unilateral temporal lobectomy. The British journal of clinical psychology the
British Psychological Society, 34 ( Pt 4)(Pt 4), 571-576. Retrieved from
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=med3
&AN=8563663
Pardoe, H. R., Pell, G. S., Abbott, D. F., & Jackson, G. D. (2009). Hippocampal volume
assessment in temporal lobe epilepsy: How good is automated segmentation? Epilepsia,
50(12), 2586-92. doi:10.1111/j.1528-1167.2009.02243.x
Poppenk, J., & Moscovitch, M. (2011). A hippocampal marker of recollection memory ability
among healthy young adults: contributions of posterior and anterior segments. Neuron,
72(6), 931-7. Elsevier Inc. doi:10.1016/j.neuron.2011.10.014
Rabin, M. L., Narayan, V. M., Kimberg, D. Y., Casasanto, D. J., Glosser, G., Tracy, J. I., French,
J. a, et al. (2004). Functional MRI predicts post-surgical memory following temporal
lobectomy. Brain : a journal of neurology, 127(Pt 10), 2286-98. doi:10.1093/brain/awh281
Reminger, S. L., Kaszniak, A. W., Labiner, D. M., Littrell, L. D., David, B. T., Ryan, L.,
Herring, A. M., et al. (2004). Bilateral hippocampal volume predicts verbal memory

39
function in temporal lobe epilepsy. Epilepsy & behavior : E&B, 5(5), 687-95.
doi:10.1016/j.yebeh.2004.06.006
Richardson, M. P., Strange, B. A., Duncan, J. S., & Dolan, R. J. (2006). Memory fMRI in left
hippocampal sclerosis: optimizing the approach to predicting postsurgical memory.
Neurology, 66(5), 699-705. doi:10.1212/01.wnl.0000201186.07716.98
Richardson, M. P., Strange, B. a, Thompson, P. J., Baxendale, S. a, Duncan, J. S., & Dolan, R. J.
(2004). Pre-operative verbal memory fMRI predicts post-operative memory decline after
left temporal lobe resection. Brain : a journal of neurology, 127(Pt 11), 2419-26.
doi:10.1093/brain/awh293
Saling, M. M., Berkovic, S. F., O’Shea, M. F., Kalnins, R. M., Darby, D. G., & Bladin, P. F.
(1993). Lateralization of verbal memory and unilateral hippocampal sclerosis: evidence of
task-specific effects. Journal of clinical and experimental neuropsychology, 15(4), 608-18.
doi:10.1080/01688639308402582
Scoville, W. B., & Milner, B. (1957). Loss of recent memories after bilateral hippocampal
lesions. Journal of Neurology Neurosurgery and Psychiatry, 20, 11-21.
Shamim, S., Hasler, G., Liew, C., Sato, S., Theodore, W. H., & Wieser, H.-G. (2004). ILAE
Commission Report. Mesial temporal lobe epilepsy with hippocampal sclerosis. Epilepsia,
45(6), 695-714. Blackwell Publishing Inc. doi:10.1111/j.0013-9580.2004.09004.x
Sobel, M. E. (1982). Asymptotic confidence intervals for indirect effects in structural equation
models. (S. Leinhardt, Ed.)Sociological Methodology, 13(1982), 290-312. American
Sociological Association. doi:10.2307/270723
Stern, C. E., Corkin, S., González, R. G., Guimaraes, a R., Baker, J. R., Jennings, P. J., Carr, C.
a, et al. (1996). The hippocampal formation participates in novel picture encoding: evidence
from functional magnetic resonance imaging. Proceedings of the National Academy of
Sciences of the United States of America, 93(16), 8660-5. Retrieved from
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=38729&tool=pmcentrez&render
type=abstract
Trenerry, M. R., Jack, C. R., Ivnik, R. J., Sharbrough, F. W., Cascino, G. D., Hirschorn, K. A.,
Marsh, W. R., et al. (1993). MRI hippocampal volumes and memory function before and
after temporal lobectomy. Neurology, 43(9), 1800-1805. AAN Enterprises. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/8414035
Tulving, E. (1985). Memory and consciousness. (E. Tulving & F. I. M. Craik, Eds.)Canadian
Psychology, 26(1), 1-12. Canadian Psychological Association. doi:10.1037/h0080017
Voets, N. L., Beckmann, C. F., Cole, D. M., Hong, S., Bernasconi, A., & Bernasconi, N. (2012).
Structural substrates for resting network disruption in temporal lobe epilepsy. Brain : a
journal of neurology, 2350-2357. doi:10.1093/brain/aws137

40
Walter, B., Blecker, C., Kirsch, P., Sammer, G., Schienle, A., Stark, R., & Vaitl, D. (2003).
MARINA: An easy to use tool for the creation of MAsks for Region of INterest Analyses.
NeuroImage, 19(2), CD-Rom. Retrieved from
http://scholar.google.com/scholar?q=MARINA:+An+easy+to+use+tool+for+the+creation+
of+MAsks+for+Region+of+INterest+Analyses&um=1&ie=UTF-
8&sa=N&hl=en&tab=ws#0
Watson, C., Andermann, F., Gloor, P., Jones-Gotman, M., Peters, T., Evans, a, Olivier, a, et al.
(1992). Anatomic basis of amygdaloid and hippocampal volume measurement by magnetic
resonance imaging. Neurology, 42(9), 1743-50. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/1513464