Embed Size (px)
Citation preview
RESEARCH PROPOSAL
By
NSANZIMANA Justin
And
KANSIIME Oliver
Submitted in Partial Fulfillment of the Requirements for the Advanced Diploma in
DEPARTMENT OF DENTISTRY
FACULTY OF ALLIED HEALTH SCIENCES
KIGALI HEALTH INSTITUTE
Supervisor: Dr MUMENA Chrispinus
Kigali August 2009
ASSESSMENT OF PERIODONTAL STATUS OF
PREGNANT WOMEN ATTENDING ANTENATAL
CLINIC AT MUHIMA HOSPITAL
Declaration
We do hereby declare that this Research Proposal submitted in partial fulfillment for the
Advanced Diploma, in Department of DENTISTRY, at KIGALI HEALTH INSTITUTE, is
our original work and has not previously been submitted elsewhere. Also, we do declare that
a complete list of references is provided indicating all the sources of information quoted or
cited.
NSANZIMANA Justin KANSIIME Oliver
Signature Signature
August, 2009
DEDICATION
KANSIIME Oliver
I dedicate this piece of work to the Almighty God, Secondly my family, relatives, my boy
friend and Mr. Joseph Kapkha of ILC consultancy as well as Mr. JEAN Baptist of UN.
DEDICATION
NSANZIMANA Justin
I dedicate this piece of work to the Almighty God, my parents and to my brothers as well as sisters and my relatives.
ACKNOWLEDGEMENT
First of all, the researchers would like to express their special appreciation and gratitude to
their Supervisor Dr MUMENA Chrispinus for his immeasurable assistance, and guidance
during the preparation of this research proposal.
Researchers also exceeding grateful to the staff and all lecturers of Dental Department
including Dr Muhumuza Ibra Head of the department for their piece of advices and
contributions where it seems to be tough.
Finally, the researcher would like to extend their sincere appreciation to Orphans of Rwanda
Inc for both material and financial support during this study. Finally, the researcher cannot
forget to thank all KHI administration in granting the permission to carry out this study in the
sphere of their administration
Almighty GOD blesses you all.
SUMMARY OF THE STUDY
Introduction
Periodontal diseases refer to a group of conditions that cause inflammation and destruction
to the supporting structures of the teeth that is gingival, alveolar bone, periodontal ligaments
and cementum. These chronic oral infections are characterized by the presence of a biofilm
matrix that adheres to the periodontal structures and serves as a reservoir for bacteria.
Periodontal diseases affect the majority of the population either as gingivitis or periodontitis.
Many recent studies have reported that maternal periodontal disease may be an independent
contributor to abnormal pregnancy outcomes such as low birth weight, preterm babies, and
risk for preeclampsia, mortality, as well as growth restriction.
Rationale:
The study will provide the baseline data on periodontal status of pregnant women, and this
information is important for planning and execution of oral health care to pregnant women at
all levels .The findings of the study may help to improve the health status of newborn babies.
Objectives
The main objective of the study is to assess the periodontal status of pregnant women
attending antenatal clinic at Muhima Hospital. Furthermore, the study will determine the
level of oral hygiene and assess the utilization of oral health services among pregnant women
attending antenatal clinic at Muhima Hospital. Nevertheless this study will determine the
proportion of pregnant women affected with gingivitis, periodontitis and characterize the
type of periodontal disease as well as determine the association between gingivitis,
periodontitis and the period of pregnancy.
Methodology
A descriptive cross sectional prospective study will be done at the antenatal clinic in Muhima
hospital over a period of two months. The sample size of 200 subjects will be selected
randomly from the pregnant women. Data collection tools will be a self administered
structured questionnaire followed by clinical examination for the pregnant women.
Conclusion
This project will cost a total of 3.123.500Rfw
Contents
Table of ContentsTABLES OF CONTENTS Page Declaration…………………………………………………………………ii Dedication…………………………………………………………………..iii Acknowledgement……………………………………………………….....iv Summary……………………………………………………………………v Tables of contents…………………………………………………………..vi Abbreviations and acronyms………………………………………………viii List of tables…………………………………………………………………ix List of figures………………………………………………………………..x
CHAPTER 1.INTRODUCTION…………………………………………… 1.1. Definitions of key terms pertinent to the study…………………………. 1.2. Background to the study ………………………………………………… 1.3 Problem statement……………………………………………………….. 1.4. Main objective………………………………………………………….. 1.5. Specific objectives………………………………………………………. 1.6. Study questions/Hypothesis……………………………………………… 1.7. Significance of the study………………………………………………… 1.8. Subdivision of the Project: Mention the main parts of the proposal
CHAPTER 2.LITERATURE REVIEW
CHAPTER 3.METHODOLOGY
CHAPTER 4.PRESENTATION OF THE RESULTS
LIST OF ABBREVIATIONS
Dr: Doctor Mr: Mister WHO: World health organization KHI : Kigali Health Institute LOA: Loss of attachment CEJ: Cemento-enamel junction HIV: Human Immune Virus AIDS: Acquired Immune Deficiency Syndrome UN: United Nation ILC: International limited Company MM: Millimeters LGE: Linear Gingival Erythema CPTIN: Community periodontal Index of Treatment Need %: Percentages
1:0 INTRODUCTION
1.1 DEFINITIONS OF THE KEY TERMS/CONCEPTS
Antenatal clinics:
These are clinics that take care for the health of pregnant women by and their new born
babies.
Plaque:
This refers to the soft; sticky accumulation that occurs on the teeth and various other intra-
oral surfaces around the tooth .it is the host to a complex micro-system of micro-organisms
whose pathogenicity and virulence cause inflammatory diseases of the gingival and other
periodontal tissues and also can be removed by direct brushing or polishing from tooth
surfaces.
Pocket probing depth;
Refers to the distance from the gingival margin to the base of the pocket. Pocket depth refers
to the abnormal space developing between the tooth and the gum.
Gingiva recession
A condition when edge of the gum moves apically along the root surface of the tooth
resulting in exposure of the roots.
Gingivitis;
This is a superficial inflammation of gum tissue (gingival). The clinical feature of gingivitis
varies as they reflect the type and extend of inflammation present which may be either acute
or chronic.
Any or all of the following signs may be noted:
Discolouration of the gingival tissue from pink to bluish red.
Swelling of the gums and loss of stippling.
Retraction of the gingiva.
Bleeding: this is the most common symptom of the inflammation of the gum tissues.
Calculus;
refers to the calcified deposits on the teeth ;formed by the continuous mineralization of
presence of dental plaque ,and also its surface provides an ideal medium for the further
plaque formation and threatening the health of the gingiva.
Root planning;
This refers to the procedure used to treat periodontal condition by scaling the roots of the
teeth to establish a smooth area and send calculus free from teeth surface and usually requires
local anesthesia to prevent pain during procedure and to avoid trauma to the client.
Gingiva (Gum):
This is a portion of the soft tissue that lines the oral cavity, covering and attaching to the
alveolar bone and cervical regional of the teeth. Normally it is salmon pink, stippled and
generally terminates coronally in a knife-edge relationship with the tooth surface. Apiccaly it
extends to the mucogingival line of the vestibular fornix and floor of the mouth. It is firmly
and well attached to the tooth. That part of the gum which forms a point between the teeth is
called the gingiva papilla.
Collagen fibres:
The major portion of the connective tissue of the free and attached gingiva consists of dense
net working of collagen fibres which interdependently fulfil numerous functions and provide
firmness to the gingiva and to the attachement of the gingiva to the underlying cementum and
alveolar bone.
The collagen fibres go in various directions and intimately blended
They are classified into groups based on their functions, location and insertion.
The periodontal ligament:
These connect the tooth with surrounding alveolar bone and it is consequently situated in the
narrow space normally between 0.1mm to 0.25mm in width and it is visual through
radiograph as radioluscent line surrounds the root. The width depends on the age and the
functioning of the tooth,mobility may occur if the width is increase ligaments are partially
lost
The cementum:
This covers the surface of the root; fibers of the periodontal ligaments are attached to this
layer. The thickness of the cementum at the cemento-enamo junction is about 5mm in the age
group and its deposition continues periodically throughout the life
Alveolar bone;
Alveolar processes are the parts of the maxilla and mandible providing the housing for the
roots of the teeth, they develop in accordance with tooth formation and eruption and they are
subjected to atrophy if the teeth are lost
Periodontitis;
Refers to both inflammation and destruction of the supportive tissues around the teeth
(periodontium)
Periodontium;
refers to periodontal tissues and it includes:gingiva(gums),periodontal ligaments,cementum
and alveolar bone.
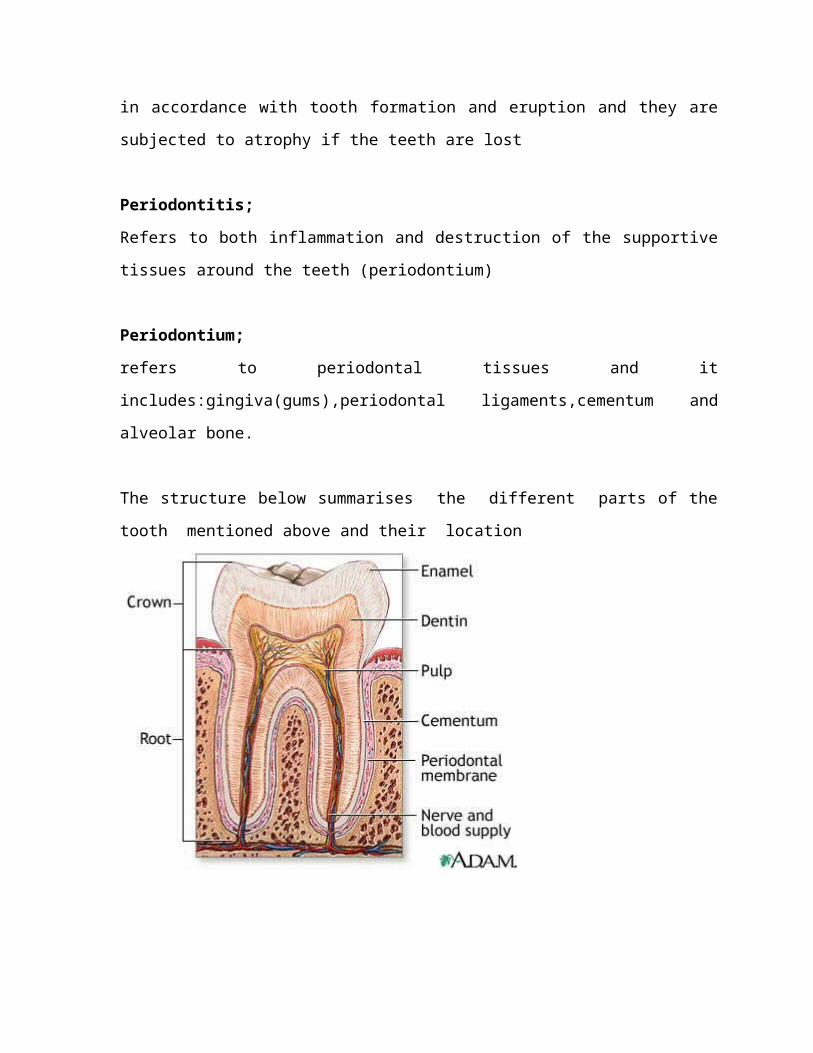
The structure below summarises the different parts of the tooth mentioned above and
their location
1:2: Background of the study
Periodontal diseases refer to a group of conditions that cause inflammation and destruction
to the pe r iodon t ium/ supporting structures of the teeth that is gingival, alveolar bone,
periodontal ligaments and cementum. These chronic oral infections are characterized by the
presence of a biofilm matrix that adheres to the periodontal structures and serves as a
reservoir for bacteria. Periodontal diseases affect the majority of the population either as
gingivitis or periodontitis. Recently there have been many studies that link or seek to find a
relationship between periodontal disease and other systemic dis- eases including,
cardiovascular disease, diabetes, stroke, and adverse pregnancy outcomes (compend contin
Educ Dent Suppl 2000)). The disease affects all ages and sexes without ratio or sex
predilection (ref).
Many recent studies have reported that maternal periodontal disease may be an independent
contributor to abnormal pregnancy outcomes including preterm birth, low birth weight,
risk for preeclampsia, mortality, and growth restriction. However, the causality of how
periodontitis influences pregnancy outcomes has not been established.(Bogges et al. 2006,
Lopez et al. 2002, Dosanayake et al. 1996, Offenbacher et al. 2001, Offenbacher et al. 1996)
Preterm birth has been identified as one of the most important perinatal health problems in
both un developed and developing countries (ref). The rate of preterm birth has not changed
despite improvement in health delivery systems in many countries (ref). Preterm birth is the
leading cause of mortality in neonates (ref). There is about 56.2% of infant mortality
reported
1.3 PROBLEM STATEMENT
The association of periodontal diseases in pregnant women with the bad health status of
newborn has been observed and reported worldwide (Bogges et al. 2006, Lopez et al. 2002,
Dosanayake et al. 1996, Offenbacher et al. 2001, Offenbacher et al. 1996). There is available
literature from developed countries that documents the high prevalence of periodontal
diseases in pregnant women (Bogges et al. 2006, Lopez et al. 2002, Dosanayake et al. 1996,
Offenbacher et al. 2001, Offenbacher et al. 1996). This has increased the emphasis of
integrating the oral health care in antenatal clinics so as to prevent the complications of
periodontal diseases in the newborn babies. The periodontal status of pregnant women in
Rwanda remains unknown, whether oral health care should be integrated in antenatal clinics
or not has never been considered. Nevertheless, a high proportion of pregnant women with
dental problems including periodontitis were observed during the period of clinical
placement at Muhima Hospital in 2008.
There is no available literature documenting magnitude of periodontal diseases of pregnant
women in Rwanda.
1.4 STUDY OBJECTIVES
I. MAIN OBJECTIVE
To assess the periodontal status of pregnant women attending antenatal clinic at
Muhima Hospital.
II. SPECIFIC OBJECTIVES
To determine the level of oral hygiene among pregnant women attending
antenatal clinic at Muhima Hospital.
To assess the utilization of oral health services among pregnant women
attending Muhima Hospital.
To determine the proportion of pregnant women affected with gingivitis
To determine the proportion of pregnant women affected with periodontitis
at Muhima Hospital
To characterize the type of periodontal disease affecting the pregnant
women Muhima hospital
To determine the association between gingivitis and the period of
pregnancy
To determine the relationship between periodontitis and the period of
pregnancy
1:5: STUDY QUESTIONS/HYPOTHESIS
I. Alternative hypothesis
There is a high proportion of pregnant women affected with periodontal disease in Rwanda.
II. Null hypothesis of the study
Periodontal disease in pregnant women is not a serious problem in Rwanda
1.6 SIGNIFICANCE/RATIONALE OF A STUDY
This study will provide the baseline information about the periodontal status among pregnant
women attending at Muhima Hospital. This information is important for planning and
execution of oral health care to pregnant women at all levels. The findings of the study may
help the policy makers on how better to improve the health status of newborn babies.
CHAP 2. LITERATURE REVIEW:
Clinical presentation of periodontal diseases:
Two major categories of periodontal diseases (Gingivitis and periodontitis) have been
described (American Dental Association 1986 )and more than that within each category
there are specific types of diseases that have been identified. The severity, the predisposing
factors and the clinical presentation of these forms differ widely.
Gingivitis is the earliest form of the disease usually present in a variety of forms depending
the causes and the associated predisposing conditions. Five forms have been documented as
commonly occurring and may all present in pregnant women depending on the accompanied
systemic condition (ref).
Plaque-Associated Gingivitis: This is the commonly and simplest form of the disease
caused by poor oral hygiene, but it can be modified by a number of factors therefore
enhancing speed and severity. Normally this form clinically will appear with bleeding of the
gums on probing without loss attachment.
Necrotizing Ulcerative Gingivitis: This is a special type of periodontal disease also known
as “trench mouth” or “Vincent’s infection”. It may be mild or severe, acute or chronic. It is
seen in people of all ages; young people of 15-30 years seem to develop the disease most
easily. It has been found that when emotional tension increases, the infection gets worse. If
the destruction extends into the soft tissues, then it is called Noma or Cancrum Oris. This
condition has been described mostly in tropical African countries where the disease has been
associated with predisposing systemic diseases such as meascles, small pox, malaria and
secondary anemia. These observations strongly suggest that while the initiating factors are
bacterial in origin, the resultant severity and extent of the disease is markedly affected by the
resistance of the host. Patients diagnosed with Necrotizing Ulcerative Gingivitis may present
with the following clinical findings: Papillary necrosis, bleeding, pain and fetor oris (odor).
No any study reported this in pregnant women.
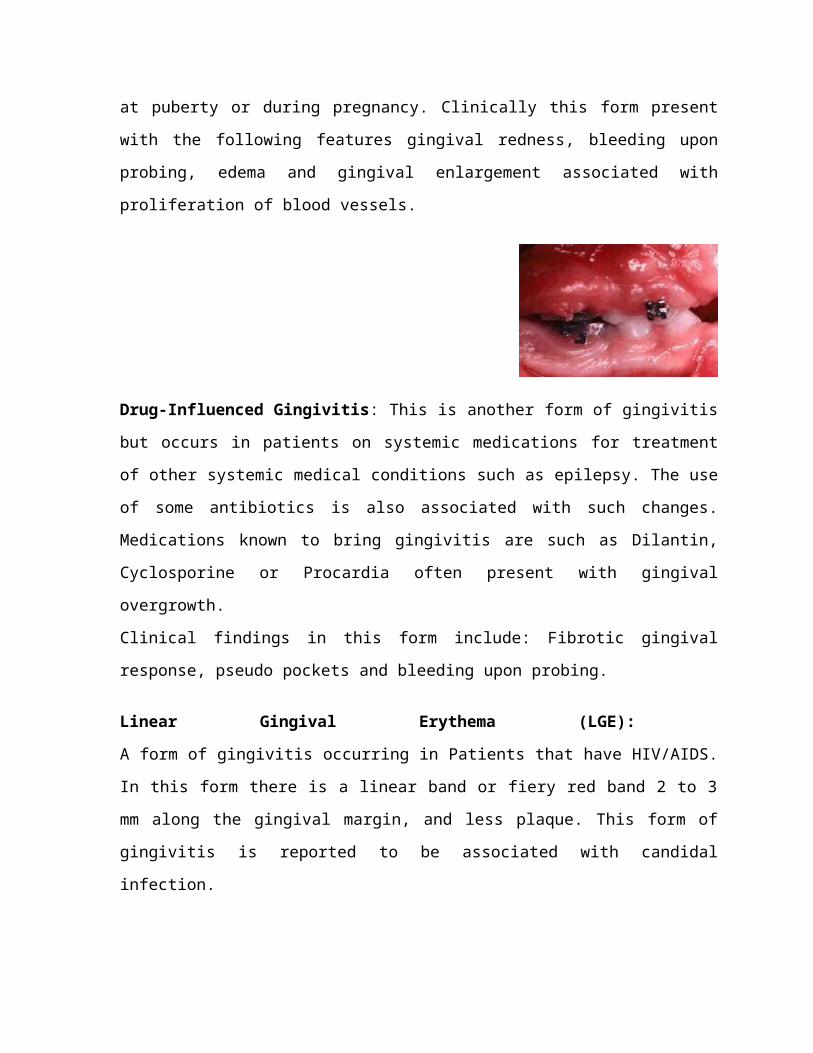
Hormone-Induced Gingival Inflammation (pregnancy gingivitis or epulis):
This form occurs commonly due to changes in the circulating level of hormones such as
estrogen and progesterone. Such hormonal changes induce gingival hyperplasia, this can
occur at puberty or during pregnancy. Clinically this form present with the following features
gingival redness, bleeding upon probing, edema and gingival enlargement associated with
proliferation of blood vessels.
Drug-Influenced Gingivitis: This is another form of gingivitis but occurs in patients on
systemic medications for treatment of other systemic medical conditions such as epilepsy.
The use of some antibiotics is also associated with such changes. Medications known to
bring gingivitis are such as Dilantin, Cyclosporine or Procardia often present with gingival
overgrowth.
Clinical findings in this form include: Fibrotic gingival response, pseudo pockets and
bleeding upon probing.
Linear Gingival Erythema (LGE):
A form of gingivitis occurring in Patients that have HIV/AIDS. In this form there is a linear
band or fiery red band 2 to 3 mm along the gingival margin, and less plaque. This form of
gingivitis is reported to be associated with candidal infection.
Periodontitis is the progression of gingivitis that has not been adequately treated or not
completely treated. This involves the chronic inflammation and destruction of the supporting
bone and parts of the periodontal membrane. As the fibres of the periodontal membrane are
destroyed and the margin of the gums detaches from the tooth, pockets are formed. Pockets
are spaces between the teeth and the surrounding tissues where formerly the attachment was
situated. From pockets pus sometimes can be discharged. As the pockets get deeper, the teeth
get looser. Teeth frequently become abscessed and eventually can even fall out. The clinical
picture of periodontitis therefore in addition to the above mentioned signs of gingivitis,
include pocketing and loosening of teeth. Several forms of periodontits are well known
depending on the aetiological factors, the age of the affected invidividual and the severity.
Aggressive periodontitis : This is a form of the periodontitis that occurs in the patients who
are clinically healthy and common features include rapid attachment loss ,bone destruction
and facial aggression
Chronic periodontitis: This is a form of the periodontal disease resulting in inflammation
with in the supporting tissues of the teeth, progressive attachment loss and bone loss and also
it is characterized by pocket formation, recession of the gingiva. .It is recognized as the most
frequently occurring form of periodontitis which is prevalent in adults but can occur in any
age.
Necrotizing periodontal diseases: an infection characterized by necrosis of gingival tissues,
periodontal ligaments and alveolar bone. These lesions most commonly observed in
individual with systemic conditions including but not limited to HIV infection, malnutrition
and immunosuppressant
Juvenile periodontitis: A common form with onset in adolescence and puberty and
relatively well defined clinical features.
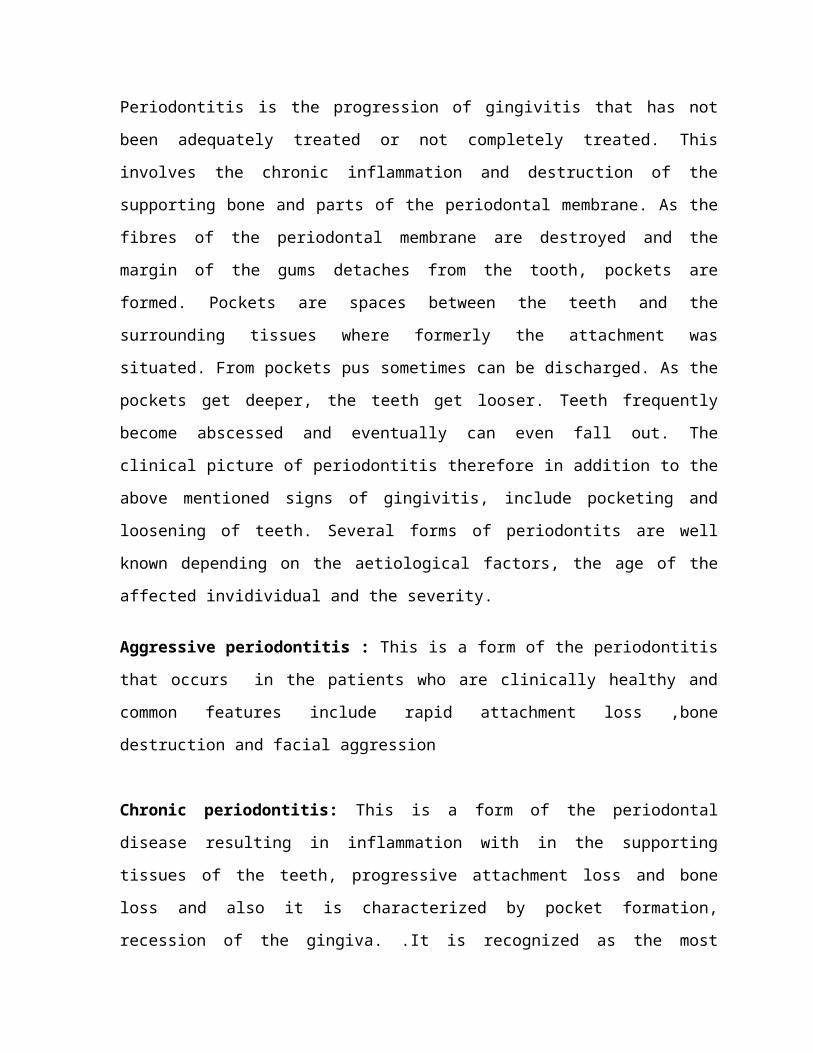
Adult Periodontitis: This is the most common chronic form of periodontitis. The presence
of local factors such as plaque is usually comparable with the disease progression. Usually it
is the progression of simple plaque induced gingivitis.
Picture of Plaque-Associated adult Periodontitis (slowly progressing periodontitis)
Measurement of periodontal disease:
Pathognomic feature of periodontal disease is the destruction of the collagen fibres of the
periodontal ligaments that may result in a loss of bone support of the tooth. Clinically the
condition is defined as measurable loss of attachement (LOA) in relation to cementoenamel
junction (CEJ). This is associated with the presence of an inflammatory reaction which
clinically is recognized as bleeding, erythema, edema, and occasionally suppuration out of
the marginal periodontal tissues. Other commonly identified signs include periodontal pocket
formation, recession of the gingival margin and eventually radiographic bone loss
Prevalence
Epidemiological studies from many countries document that 5 to 20% of the adult population
suffers from severe forms of periodontal disease (periodontitis), depending on the measure of
disease applied (Pilot and Miyazaki 1991, Hugoson et al. 1998, Brown and Loe 1998). In
developing countries such as Thailand the prevalence and severity has been reported to be
generally high. The above findings were obtained by using the WHO community periodontal
index of treatment needs (CPITN), that demonstrated that periodontitis was found in 1.1,
37.2 and 61.6% of subjects aged 15, 35-44 and 60-74 years respectively. Data for child
bearing age was not available therefore not reported.
Causes of periodontal diseases
For many years, it was believed that specific pathogenic bacteria found within dental
plaque biofilm were solely responsible for periodontal diseases. While it is known that
pathogenic bacteria are one facet of the disease process and are consistently present, it is
not the only cause of periodontitis. The host response to the bacterial insult modulates
the severity of the disease by activating the immune system to mediate the disease
process. How well the host responds to the pathogenic bacteria modulates how the
disease is initiated and progresses. This is evidenced by the fact that gingivitis does not
always progress into periodontitis.
Over the years, several risk factors for periodontitis have been identified. For example, stress,
poor dietary habits with high sugar intake, smoking and tobacco use, obesity, age, and poor
dental hygiene all contribute to the development of periodontal disease. Other major risk
factors include clinching or grinding teeth, genetic factors, other family factors, other medical
diseases such as diabetes, cancer, or AIDS, defective dental restorations medication use, and
conditions that change estrogen levels such as puberty, pregnancy, menopause
(http://www.perio.org/consumer/2a.html, http://www.nidcr.nih.gov/nidcr.nih.gov) Eighty
percent of individuals with periodontal disease have at least one risk factor that increases
their susceptibility to the infectious process and subsequent tissue damage. Often multiple
factors are present (http://www.perio.org/consumer/2a.html,
http://www.nidcr.nih.gov/nidcr.nih.gov).
Periodontal Disease and Other Systemic Conditions
There is convincing evidence that link between oral and systemic health. Current evidence
suggests that periodontal disease is associated with an increased risk for cardiovascular dis-
ease (Spahr et al. 2006, Holmlund et al. 2006), diabetes (Jansson et al. 2006, Al-
Shammari et al. 2006), community and hospital acquired respiratory infections
(Azarpazhooh and Leake 2006), and adverse pregnancy outcomes (Beck et al. 2005, Bogges
et al. 2006, Lopez et al. 2002). Individuals with periodontal disease have approximately a 1.5 –
1.9 increased odds for developing cardiovascular disease (Spahr et al. 2006, Dosanayake et al.
2003). There appears to be a bidirectional relationship between periodontal disease and
diabetes with a 2- to 3-fold increased risk for diabetes among individuals with tooth loss.
Teeth and periodontium may serve as a reservoir and may contribute to respiratory infections.
Individuals with poor oral hygiene such as dental decay have 2- to 9-fold increase odds for
pneumonia (Azarpazhooh and Leak 2006).
Periodontal disease and preterm birth
Recent research suggests that the presence of maternal periodontitis has been associated
with adverse pregnancy outcomes, such as preterm birth, (Offenbacher et al. 1996,
Offenbacher et al. 2001, Jeffcoat et al. 2001) preeclampsia (Bogges et al. 2003), gestational
diabetes (Xiong et al. 2006), delivery of a small for gestational age infant (Bogges et al.
2006), and fetal loss (Moore et al. 2004). The strength of these associations ranges from
a 2-fold to 7-fold increase in risk. The increased risks suggest that periodontitis may be an
independent risk factor for adverse pregnancy outcomes.
1. The remote sites infection contribution to preterm birth has been supported by a number
of studies (Collin et al. 1994). The non disseminating low level challenge with
porphyromonas gingivalis which an important periodontal pathogen has been found to
elicit significant fetal weight reduction. Immunonization before experimental induction
were reported not to provide protection from a challenge during pregnancy, rather
potentiated the effects. This suppressive effect on the fetal weight was accompanied by a
proportional rise in TNFα and PGE2 (Ann Periodontol. 1998.).
Study by Offenbacher and collegues (1998) to determine relationship of current periodontal
status to current pregnancy outcome revealed that gingival crevicular fluid (GCF)-PGE2
levels were significantly higher in spontaneous preterm birth(SPB) mothers compared with
normal term delivery controls. Furthermore it was revelaed that there were significant inverse
association between birthweight (gestational age) and the GCF-PGE2 for current births
among mothers. This suggests dose response relationship for increasing GCF-PGE2 as a
marker of current periodontal disease activity and decreasing birthweight.
Jeffcoat et al. (2001) through their prospective study revealed that patients with periodontal
status were at increased risk of preterm birth despite the other risk factors such as smocking,
parity, race and marternal age. The risk of preterm birth increases from 3 to 7 fold in patients
with the most severe periodontitis, demonstrating dose relationship as revealed by other
studies.
Offenbacher et al. (1997) observed that mothers with periodontal disease are seven times
more likely to give birth to premature and low weight babies. Jeffcoat et al. (2001) found
similar results and stated that the risk of premature and low weight births increases four- to
sevenfold according to the severity of periodontal disease. Data from Louro et al.(2001)
support the results found so far, demonstrating that mothers with severe periodontal disease
are seven times more likely to have preterm low birth weight. Glesse, Saba-Chujfi(2003)
demonstrated a 12-fold increase in the chances of a woman with severe gingival
inflammation, associated to generalized periodontitis or not, delivering a premature, low
weight baby. Konopka et al. (2003) stated that women with severe/generalized periodontitis
are three times more likely to deliver a premature, low weight baby. According to Mokeem et
al. (2004), the risk of delivering a premature, low weight baby increases fourfold with an
increase of periodontal disease prevalence, regardless of the control of other risk factors such
as age, smoking, and social extraction. Cruz et al.(2005) found a positive association
between periodontal disease and low birth weight especially among the mothers with
schooling of less than or equal to four years. López et al. (2005) underlie such association,
their data showing that periodontal disease increases the chances of delivering premature,
low weight babies fourfold. Romero and collogues (2002) have documented the risk of
preterm delivery and low birth in pregnant women with current periodontal disease in their
study to establish relationship between periodontal disease in pregnant women and the
condition of their newborns.
Periodontal disease status during pregnancy:
It is well accepted that periodontal tissues can be affected by pregnancy. Pregnancy related
changes are the most frequent and marked in the superficial part of periodontal tissues which
is the gingival. Pregnancy does not cause gingivitis but may aggravate preexisting disease.
The most marked changes are seen in gingival vasculature. Characteristics of pregnancy
gingivitis are that the gingival is dark red, swollen, smooth and bleeds easily (Laine 2002).
Women with pregnancy gingivitis may sometimes develop localized gingival enlargements
known as gingival epulis.
During pregnancy gingival inflammation increases significantly from the first trimester (Loe
and Silness 1963, Cohen et al. 1969) with a maximum increases in the second trimester
(Samant et al. 1976) and a decrease at the end of third trimester (Loe and Silness 1963,
Cohen et al. 1969). Periodontal disease presentation has been shown to be significantly in a
group of pregnant women compared to with non pregnant controls, despite the fact that the
oral hygiene of the 2 groups was comparable (Miyazaki et al. 1976).
CHAP 3 METHODOLOGY OF THE STUDY
STUDY AREA:
This study will be carried out in antenatal clinic at Muhima hospital for a period of 2 month from
June to August 2009.
The hospital is located in Muhima sector in Nyarugenge District, found in Kigali city in the
peripherals of Kigali few metres from Nyabugogo high way below the Kinamba and Yamaha road.
The hospital was constructed by the PSP and the world Bank and officially opened on 13 June
2001.This hospital is one among the districts referral hospitals and it is special for pregnant women
in Kigali city. .
STUDY DESIGN;
A descriptive cross –sectional prospective study.
STUDY POPULATION
All pregnant women attending antenatal clinic at Muhima hospital will be eligible for study. Only
pregnant women who fulfill the inclusion criteria will be studied.
STUDY SAMPLE
The sample size of 200 subjects will be selected randomly from the pregnant women attending the
antenantal clinic at Muhima hospital.
INCLUSION CRITERIA:
Pregnant women from first month to eighth month of conception and who does not have pregnancy
hypertension, or any other medical condition that will make her be uncomfortable for clinical
examination.
EXCLUSION CRITERIA:
Pregnant women who are in the last month of pregnancy, with pregnancy hypertension or any other
medical condition that prohibits her to sit for a long time (30 minutes) for clinical examination.
SAMPLING TECHNIQUE:
Random sampling technique will be used to gather the 200 subjects for study.
DATA COLLECTION TOOLS
QUESTIONNAIREs
A self administered structured questionnaire containing close and open ended questions will be used
to collect information on biodata, knowledge on periodontal diseases and oral health behavior.
Thereafter clinical examination will be performed, in data collection the questionnaire formulation
will be based on the literature review and specific objectives. The questionnaire will be distributed to
participants and there after the researchers will immediately collect them.
The following tools will be used for questionnaire construction:
Pen, pencil, papers, desk top computer and ----
CLINICAL EXAMINATION FORM:
Clinical examination form will be used to collect clinical examination findings.
CLINICAL EXAMINATION INSTRUMENTS:
Periodontal probe
Mouth mirror
Pair of twizzer
Air blower
Gauzes
LIMITATIONS AND THE PROBLEM OF THE STUDY.
Financial position of the participants may be the limiting factor during the study because some of the
pregnant women may not be able to come to the hospital due to insufficient amount of money and it
can lead to the missing of some important information regarding the study.
Cultural beliefs of using traditional healers, particularly traditional birth attendants may cause lack of
certain information in pregnant women regarding to this study.
An Introvert behavior in some people may cause lack of certain information during data collection
therefore affecting the study.
DATA ANALYSIS
The data will be analyzed by using a statistical package microsoft excel software.
ETHICAL CONSIDERATION
Ethical clearance will be sought form the ethical clearance committee. A covering letter
recommending the researcher for the permission to carry out this study will be first obtained from
Kigali Health Institute (KHI) administration and later on it will be presented to the administration of
Muhima Hospital which granted the researcher permission for carrying out the study.
QUESTIONNAIRE FOR ASSESSMENT OF PERIODONTALDISEASES IN PREGNANT
WOMEN ATTENDING AT ANTENATAL CLINIC AT MUHIMA HOSPITAL
1: 0 BIODATA/
1:1 ID
1:2 AGE:
1.3: OCCUPATION (tick the appropriate)
I. Employed
II. Business woman
III. Un employed
1.4: MARITAL STATUS
I. Single
II. Married
III. Divorced
IV. Widower
V. Separated
1.5: EDUCATIONAL LEVEL
I. Primary
II. Secondary
III. Institute
IV. None
1.6: REGION
I. Nyarugenge
II. Gasabo
III. Kicukiro
IV. Other ________________________________________
1.7: Period of pregnancy
I. First trimester (1-3 months)
II. Second trimester ( 4-6months)
III. Third trimester (7-9 months)
2.0.Main theme
2:1 Do you clean your teeth? (tick the appropriate)
1= Yes
2= No (if no go to question No 2.2)
2.1:1 What do you use to clean your teeth?
I. Modern tooth brushing
II. Wooden tooth brush
III. None
IV. If others, mention………………………
2.1.2. How many times do you clean your teeth?
I. Once per a day
II. Twice a day,
III. Thrice a day
IV. None
2.2 Have you ever visited a dentist or any dental practitioner?
1= Yes
2= No (If no go to question No 2.3)
2:2:1 If yes, why did you go to the dentist?
I. Because of dental pain
II. Was referred
III. For dental check up
IV. Others, mention_______________________________________
2.2:2 When was your last dental visit?
2:3 Do you see or spit blood during and after tooth brushing?
1= Yes
2= No
2:4 Are your gums swollen in this moment of pregnancy?
1= Yes
2= No
2:5 Are your gums painful in thus period of pregnancy?
1= Yes
2= No
2.6. Do you have any bad smell from your mouth?
1= Yes
2= No
2.7 Has anyone of your side in the family had gum problems or treated with similar problem?
1= Yes
2= No
2:8 Do you smoke?
1= Yes
2= No
2:9 Do you take alcohol or have you ever taken any alcohol in this moment of pregnancy?
1= Yes
2= No
2:10 Do have any medical condition/illness/diseases like
I. HIV/AIDS
II. Heart problems
III. Diabetes mellitus
IV. Respiratory diseases
V. Epilepsy
VI. Others mention__________________________________________
2:11 Are you on any medication for any of the problem you ticked above?
1= Yes
2= No
2:11:1 If yes mention__________________________________________
UBUSHAKASHATSI KU BUZIMA BWO MU KANWA KU BADAMU BATWITE BAFITE
HAGATI Y’UKWEZI KUMWE KUGEZA KU MEZI ICYEDA BABARIZWA KU BITARO BYA
MUHIMA.
1: 0 IRANGAMIMERERE1:1 UMWIRONDORO
1:2 IMYAKA:
1.3: ICYO UKORA (hitamo igisubizo nyakuri)
I. Ufite akaziII. Umucurizikazi
III. Nta kazi ufite 1.4: IBYEREKERANYE N’URUSHAKO
I. IngaraguII. Warashatse
III. Watanye n’uwo mwashakanyeIV. UmuphakaziV. Ntimubana
1.5: AMASHURI WIZE
I. Amashuri abanzaII. Amashuri yisumbuye
III. KaminuzaIV. Ntiwize 1.6: AHO UBARIZWA
I. Nyarugenge II. Gasabo
III. Kicukiro IV. Ahandi
-1.7: Igihe umaze utwite
I. Kuva ku mezi (1-3 ) II. Kuva ku mezi ( 4-6 )
III. Kuva ku mezi (7-9 )
2.0.Ingingo nyamukuru
2:1 Ese ujya usukura amenyo yawe? (hitamo igisubizo nyakuri) 1= Yego
2= Oya (Niba ari oya, jya ku kibazo cya No 2.2)
2.1:1 Ni iki ukuresha mu gusukura amenyo yawe? I. Uburoso bw’amenyo
II. Agati cyangwa umutozoIII. Nta na kimweIV. Niba hari ikindi, kivuge………………………
2.1.2. Ese ni kangahe usukura amenyo yawe nibura ku munsi?
I. Rimwe ku munsiII. Kabiri ku munsi
III. Gatatu ku munsi cyangwa birenzehoIV. Nta na rimwe
2.2 Ese hari ubwo waba warigeze kujya kwa muganga w’amenyo cyangwa uwita ku menyo? 1= Yego 2= Oya (Niba ari oya, jya ku kibazo cya No 2.3) 2:2:1 Niba ari yego, ni iyihe mpamvu yatumye ujyayo?
I. Kubera ububabare bw’amenyoII. Bamunyoherejeho
III. Kwisuzumisha amenyo IV. Ibindi, bivuge_______________________________________ 2.2:2 Ese ni ryari uheruka kwisuzumisha amenyo? 2:3 Ese ujya ubona cyangwa ugacira amaraso igihe usukura mu kanwa?
1= Yego
2= Oya
2:4 Ese ishinya yawe yaba ifite ikibazo cyo kubyimba muri iki gihe utwite? 1= Yego 2= Oya
2:5 Ese ishinya yawe yaba ikubaba muri iki gihe utwite? 1= Yego 2= Oya
2.6. Ese hari ubwo waba ugira ikibazo cy’impumuro idasanzwe mu kanwa muri iki gihe utwite?
1= Yego 2= Oya
2.7 Ese haba hari undi muntu wo mu muryango wanyu waba waragize ikibazo cy’ishinya cyangwa wivujije ikibazo nk’icyo?
1= Yego 2= Oya
2:8 Ese waba unywa itabi muri iki gihe utwite?
1= Yego 2= Oya
2:9 Ese waba unywa inzoga cyangwa warayinyweye muri iki gihe utwite?
1= Yego 2= Oya
2:10 Ese haba hari bumwe muri ubu burwayi waba ufite?
I. HIV/ SIDAII. Indwara z’umutima
III. Indwara ziterwa n’isukaliIV. Indwara z’ubuhumekero V. Igicuri
VI. Izindi, zivuge__________________________________________ 2:11 Ese haba hari imiti ya zimwe mu ndwara zavuzwe haruguru ufata? 1= Yego
2= Oya
2:11:1 Niba ari yego, yivuge__________________________________________
NSANZIMANA Justin and
KANSIIME Oliver
Dental department
P.O.Box 3286 Kigali
E-mali:[email protected]
Mobile phone :(+250)0788578553
(+250)0788754519
August, 2009
Administration of MUHIMA Hospital.
RE: Request to carry out a study.
We are NSANZIMANA Justin and KANSIIME Oliver, third year students of Dental department in
Kigali Health Institute.
We would like to conduct a study on ‘Assessment of periodontal status of pregnant women attending
antenatal clinic at Muhima hospital:
We humbly wish to request the authorization to carry out this research among MUHIMA Hospital as
a part of our sample population.
Your response will be highly appreciated.
Yours faithfully,
NSANZIMANA Justin
And
KANSIIME Olive
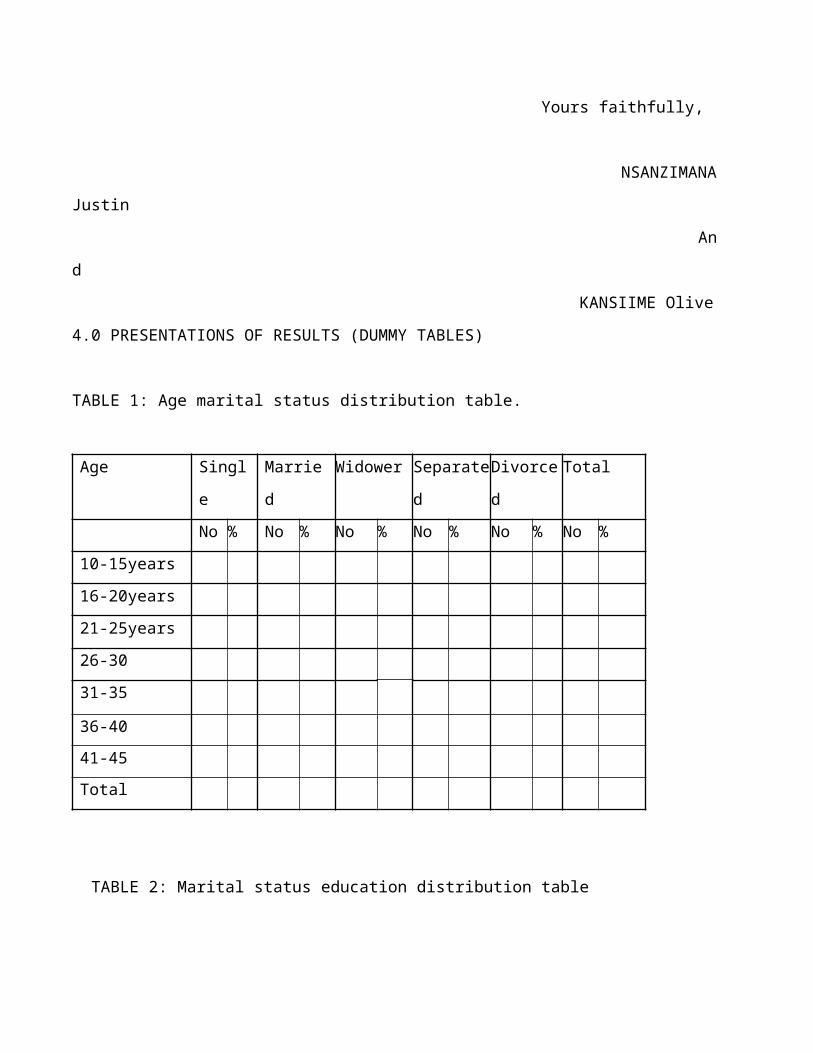
4.0 PRESENTATIONS OF RESULTS (DUMMY TABLES)
TABLE 1: Age marital status distribution table.
Age Single Married Widower Separated Divorced Total
No % No % No % No % No % No %
10-15years
16-20years
21-25years
26-30
31-35
36-40
41-45
Total
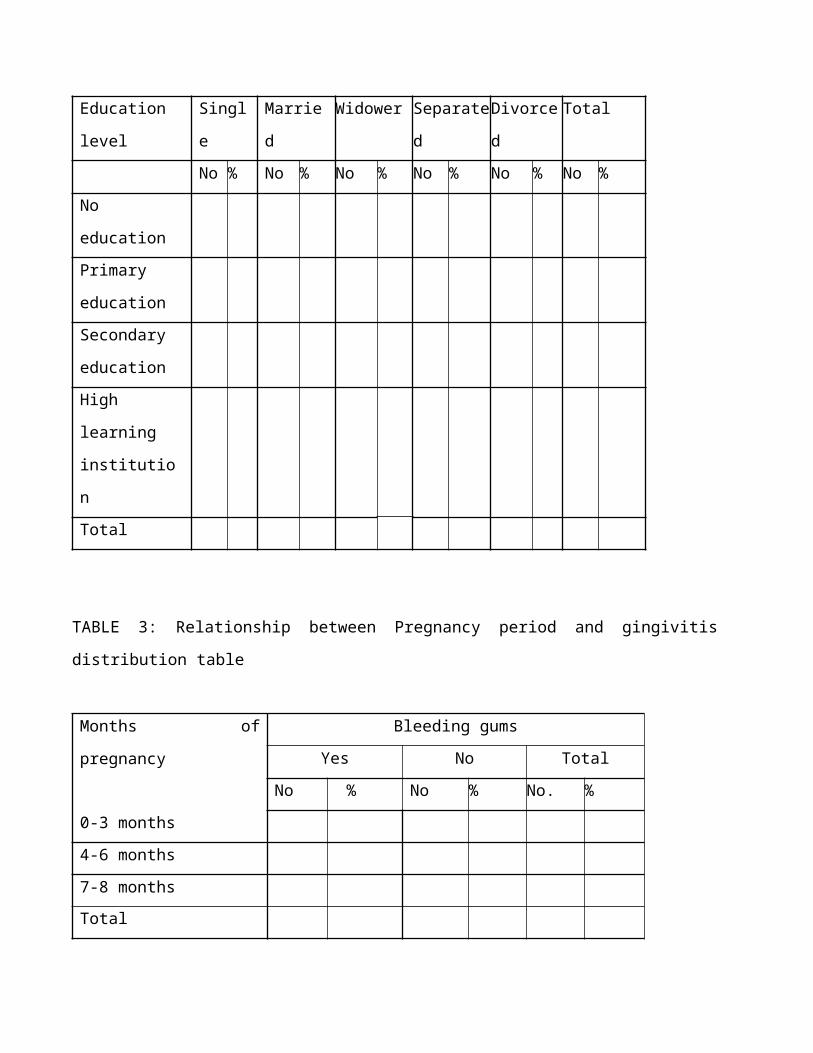
TABLE 2: Marital status education distribution table
Education level Single Married Widower Separated Divorced Total
No % No % No % No % No % No %
No education
Primary
education
Secondary
education
High learning
institution
Total
TABLE 3: Relationship between Pregnancy period and gingivitis distribution table
Months of pregnancy Bleeding gums
Yes No Total
No % No % No. %
0-3 months
4-6 months
7-8 months
Total
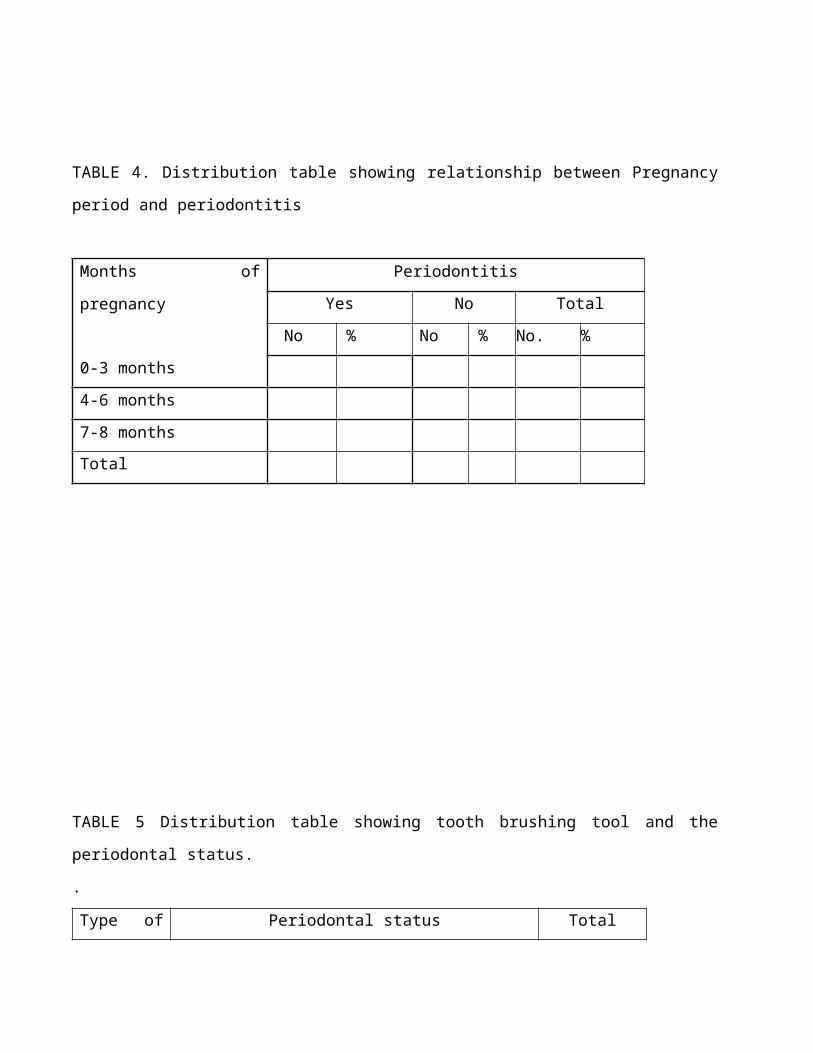
TABLE 4. Distribution table showing relationship between Pregnancy period and periodontitis
Months of pregnancy Periodontitis
Yes No Total
No % No % No. %
0-3 months
4-6 months
7-8 months
Total
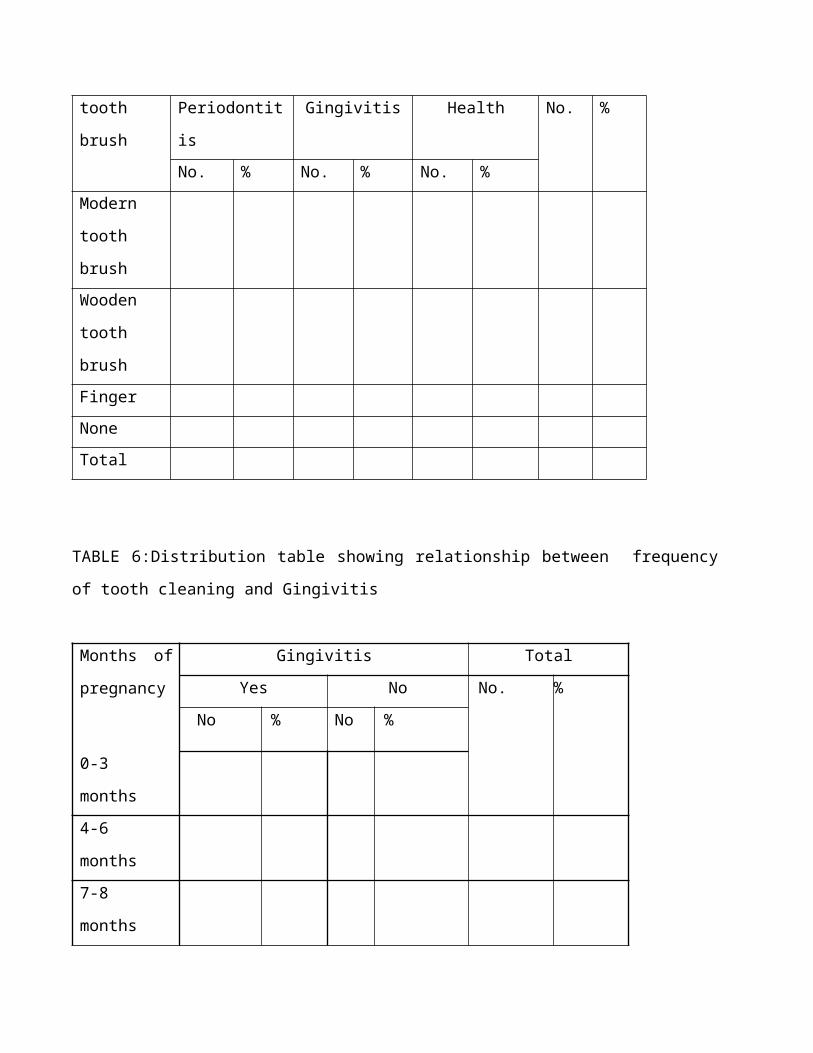
TABLE 5 Distribution table showing tooth brushing tool and the periodontal status.
.
Type of
tooth brush
Periodontal status Total
Periodontitis Gingivitis Health No. %
No. % No. % No. %
Modern
tooth brush
Wooden
tooth brush
Finger
None
Total
TABLE 6:Distribution table showing relationship between frequency of tooth cleaning and
Gingivitis
Months of
pregnancy
Gingivitis Total
Yes No No. %
No % No %
0-3 months
4-6 months
7-8 months
Total
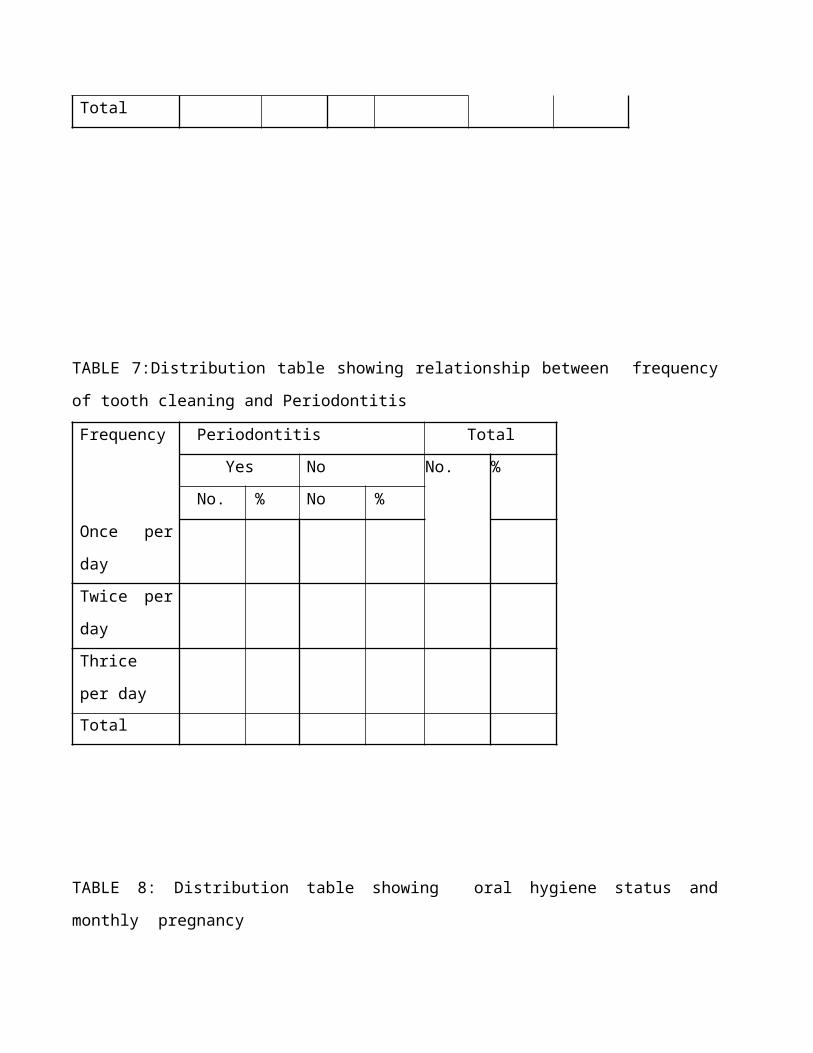
TABLE 7:Distribution table showing relationship between frequency of tooth cleaning and
Periodontitis
Frequency Periodontitis Total
Yes No No. %
No. % No %
Once per day
Twice per day
Thrice per day
Total
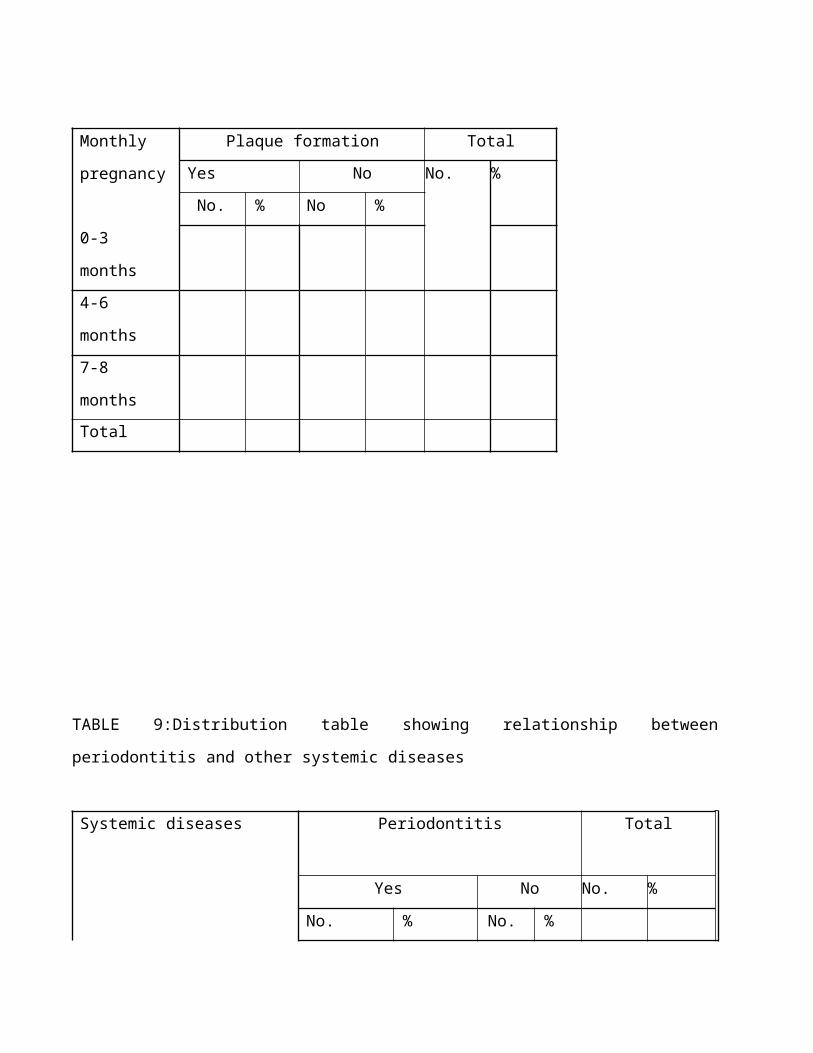
TABLE 8: Distribution table showing oral hygiene status and monthly pregnancy
Monthly
pregnancy
Plaque formation Total
Yes No No. %
No. % No %
0-3 months
4-6 months
7-8 months
Total
TABLE 9:Distribution table showing relationship between periodontitis and other systemic diseases
Systemic diseases Periodontitis Total
Yes No No. %
No. % No. %
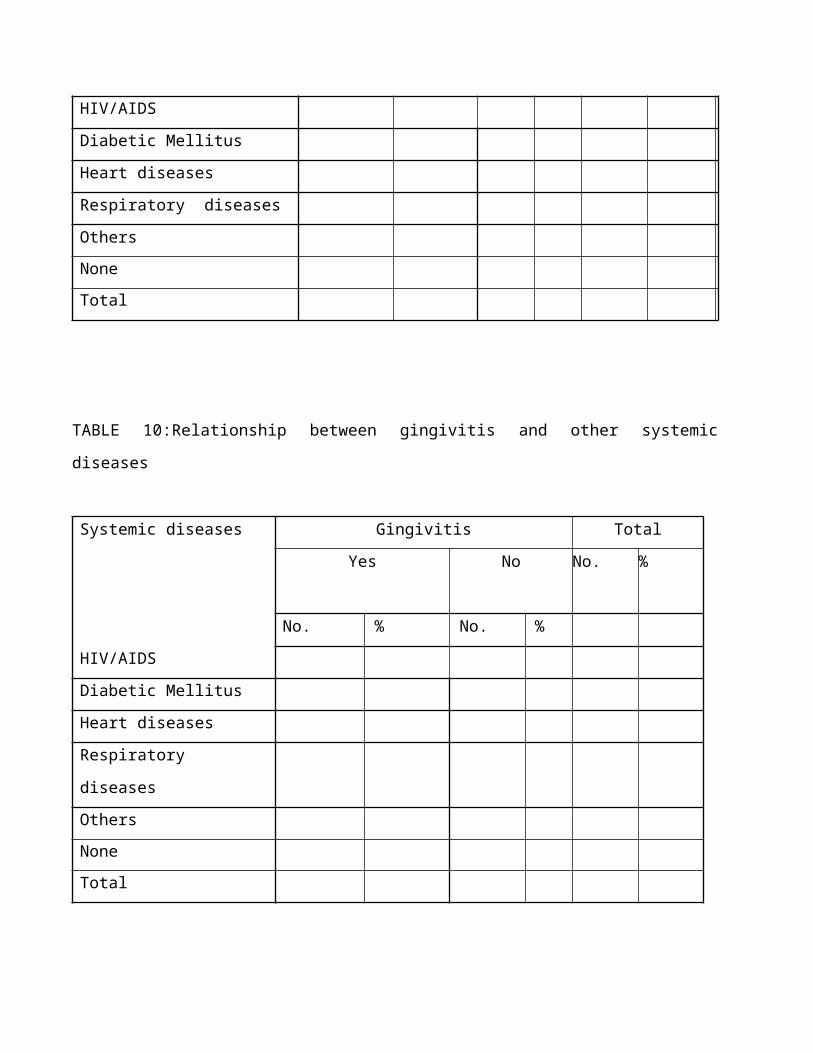
HIV/AIDS
Diabetic Mellitus
Heart diseases
Respiratory diseases
Others
None
Total
TABLE 10:Relationship between gingivitis and other systemic diseases
Systemic diseases Gingivitis Total
Yes No No. %
No. % No. %
HIV/AIDS
Diabetic Mellitus
Heart diseases
Respiratory diseases
Others
None
Total
PROFILE OF KIGALI HEALTH INSTITUTE
Kigali Health Institute (KHI) is an institution of higher education established in 1996 by the Ministry
of Health in collaboration with Ministry of Education .The institute was created to solve the
problems of inadequate health personnel both in quality and quantity
VISION OF KIGALI HEALTH INSTITUTE
“To be center of Excellency in training and development of human professionals”
MISION OF KIGALI HEALTH INSTITUTE
:To train and improve the capacity of the health workers”
Kigali Health Institute has two campuses:
a. The main campus in Kigali city
b. Environmental health sciences at Nyamishaba campus in Karongi District
MANAGEMENT OF KIGALI HEALTH INSTITUTE
The academic team structured as follows:
A.Kigali Health institute composed of faculties and departments
1. Faculty of Allied Health Sciences
-Department of Dentistry
-Department of Aneasthesia
-Department of Medical Laboratory
-Department of Physiotherapy
-Department of Medical Imaging Sciences
-Department of Ophthalmology
2. Faculty of Nursing sciences
-Department of Genaral Nursing
-Department of Midwifery
-Department of Mental Health
3.. Faculty of Health Development
-Department of Environmental Health sciences
B. ADMINISTRATION OF THE INSTITUTE
Rector :Doctor Major NDUSHABANDI Desire
Vice Rector in charge of the academic Affairs and Research : Doctor
KABAGABO Chantal
Vice Rector in charge of Administration and Finance:Mr KAZIGE Eugene
REFERENCES:
2. Albandar 1999
3. Al-Shammari KF, Al-Ansari JM, Moussa NM, Ben-Nakhi A, Al-Arouj M, Wang HL.
Association of periodontal disease severity with diabetes duration and diabetic
complications in patients with type 1 diabetes mellitus. J Int Acad Peri- odontol.
2006;8(4):109-14
4. American Dental Association: Risk Management Series, Diagnosing and managing the
Periodontal Patient, 1986 Periodontal Diseases. Chicago, Ill. American Academy of
Periodontology logy. http://www.perio.org/consumer/2a.html.
5. Azarpazhooh A, Leake JL. Systematic review of the asso- ciation between respiratory
diseases and oral health. J Peri- odontol. 2006;77(9):1465-82.
6. Beck JD, Eke PI, Heiss G, et al. Periodontal disease and coronary heart disease: a
reappraisal of the exposure. Cir- culation. 2005(1); 112:19-24.
7. Bernard 1993A.Collins JG, Smith MA, Arnod RR, Offenbacher S. effect of Escheria coli
and Porphyromonas gingivalis lipopolysaccharide on pregnant outcome in the harmsters.
Infect Immun 1994;62: 4652-5
8. Boggess KA, Beck JD, Murtha AP, et al. Maternal peri- odontal disease in early
pregnancy and risk for a small-for- gestational-age infant. Am J Obstet Gynecol.
2006;194(5): 1316–22.
9. Boggess KA, Lieff S, Murtha AP, Moss K, Beck J, Offen- bacher S. Maternal
periodontal disease is associated with an increased risk for preeclampsia. Obstet
Gynecol. 2003;101(2):227–31
10. Brown LJ, Loe H. Prevalence, extent, severity and progression of periodontal disease.
Periodontol 2000, 1993; 2:57-71
11. Cohen DW, Friedman L, Shapinro J, Kyle GC. A longitunal investigation of the
periodontal changes during pregnancy. J Periodontol 1969; 40:563-70
12. Collins JG, Windley HW III, Arnod RR, Offenbacher S. effect of Porphyromonas
gingivalis infection on inflammatory mediator response and pregnancy outcomein
harmsters. Infect Immun 1994; 62:4356-61
13. Cruz SS, Costa MCN, Gomes Filho IS, Vianna MIP, Santos CT. Maternal periodontal
disease as a factor associated with low birth weight. Rev Saúde Pública. 2005; 39(5):782-
7.
14. Dasanayake AP, Russell S, Boyd D, et al. Preterm low birth weight and periodontal
disease among African Americans. Dent Clin North Am. 2003;47(1):115-25, x-xi
15. ePR on April 1, 2009 - 2:11pm. Dental/Health
16. Genco RJ, Jeffcoat M, Colon J, Papapama P, Armitage, Grossi et al. Consensus report on
periodontal disease: Epidemiology and diagnosis. Am Periodontol 1996 ; 1 :216-22
17. Glesse S, Saba-Chujfi E. An influência da doença periodontal no trabalho de parto pré-
termo [abstract]. Pesqui Odontol Bras. 2003;(17 Suppl 2):155
18. Holmlund A, Holm G, Lind L. Severity of periodontal disease and number of remaining
teeth are related to the prevalence of myocardial infarction and hypertension in a study
based on 4,254 subjects. J Periodontol. 2006; 77(7):1173-8.
19. Hugoson A, Nordeyad O, Slotte C, Thorstensson H. Distribution of periodontal disease in
a Swedish adult 1973, 1983, and 1993. J Clin Periodontol 1998; 25:542-8
20. Jansson H, Lindholm E, Lindh C, Groop L, Bratthall G. Type 2 diabetes and risk for
periodontal disease: a role for den- tal health awareness. J Clin Periodontol.
2006;33(6):408-14.
21. Jared, Heather, Boggess, Kim A, Journal of Dental Hygiene, Number 3, Summer
Supplement, 1 July 2008 , pp. 24-24(1)
22. Jeffcoat MK, Geurs NC, Reddy MS, Cliver SP, Goldenberg R and Hauth JC.
Periodontal infection and preterm birth:Results of a prospective study. J Am Dent
Assoc. 2001; 132(7); 875-880.
23. Jeffcoat MK, Geurs NC, Reddy MS, Cliver SP, Goldenberg RL, Hault JC. Periodontal
infection and preterm birth;results of a prospective study. J Am Dent Assoc 2001;
132:875-80
24. Jeffcoat MK, Geurs NC, Reddy MS, Goldenberg RL, Haulth JC. Periodontal infection
and preterm birth: results of a prospective study. J Am Dent Assoc. 2001; 137(7):875-80.
25. Konopka T, Rutkowska M, Hirnle L, Kopec W, Karolewska E, Rutkowska M et
al.The secretion of prostaglandin E2 and interleukin 1-beta in women with periodontal
diseases and preterm low-birth-weight. Bull Group Int Rech Sci Stomatol Odontol. 2003;
45(1):18-28.
26. Laine MA. Effect of pregnancy on periodontal and dental health. Acta Odontol Scand
2002; 60:257-64
27. Loe H et al . periodontal changes in pregnancy .J periodontal 1965;35;37-44
(www.sciencedaily.com) April issue of the Journal of Clinical Microbiology. Dimensions Dental
Hygiene May 2006
28. Loe H, Silness J. Periodontal disease in pregnancy: Prevalence and severity. Acta
Odontol Scand 1963; 21:533-51
29. López NJ, Da Silva I, Ipinza J, Gutiérrez J. Periodontal therapy reduces the rate of
preterm low birth weight in women with pregnancy-associated gingivitis. J Periodontol.
2005;76(Suppl 11):2144-53.
30. Lopez NJ, Smith PC, Gutierrez J. Higher risk of preterm birth and low birth weight in
women with periodontal dis- ease. J Dent Res. 2002;81(1):58-63.
31. Louro PM, Fiori HH, Louro Filho P, Steibel J, Fiori RM. Doença periodontal na gravidez
e baixo peso ao nascer. J Pediatr. 2001; 77(1):23-8.
32. Miyazaki H, Yamashita Y, Shirahama R, Goto-Kimura K, Shimada N, Sogne A et al.
Periodontal condition of pregnant women assessed by CPITN. J Clin Periodontol 1991;
18:751-4
33. Mokeem SA, Molla GN, Al-Jewair TS. The prevalence and relationship between
periodontal disease and pre-term low birth weight infants at King Khalid University
Hospital in Riyadh, Saudi Arabia. J Contemp Dent Pract. 2004; 5(2):40-56.
34. Moore S, Ide M, Coward PY, et al. A prospective study to investigate the relationship
between periodontal disease and adverse pregnancy outcome. Br Dent J. 2004;
197(10):251-8; discussion 247.
35. Offenbacher S, Jared HI, O’Reilly PG, Wells SR, Salvi GE, Lawrence HP et al. Potential
pathogenic mechanisms of periodontitis associated pregnancy complications. Ann
Periodontol 1998; 3:233-50
36. Offenbacher S, Katz V, Fertik G, Collins J, Boyd D, Maunor G et al. Periodontal
infection as a possible risk factor for preterm low birth weight. J Periodontol. 1997;
67(10):1103-13.
37. Offenbacher S, Katz V, Fertik G, et al. Periodontal infection as a possible risk
factor for preterm low birth weight. J Peri- odontol. 1996;67(10 suppl):1103-13.
(http;www.Cdnp.org/down loads /publication /policy /PTLBW .pdf)
38. Offenbacher S, Lieff S, Boggess KA, et al. Maternal peri- odontitis and prematurity. Part
I: Obstetric outcome of pre- maturity and growth restriction. Ann Periodontol. 2001;6(1):
164-74.
39. Periodontal (Gum) Disease: Causes, Symptoms, and Treat- ments. Bethesda, Md.
National Institute of Dental and Craniofacial Research.
http://www.nidcr.nih.gov/nidcr.nih.gov.
40. Pester, B. J., S. K. Boches, J. L. Galvin, R. E. Ericson, C. N. Lau, V. A. Levanos, A.
Sahasrabudhe, and F. E. Dewhirst. 2001. Bacterial diversity in human subgingival
plaque. J. Bacteriol. 183:3770-3783. [PubMed]).
41. Pihlstrom ,B Michalowicz ,N Johnson ,Lancet ,2005;Elsevier Periodontal diseases 9499
(page 1809_1820)
42. Pilot T, Miyazaki H. Periodontal conditions in Europe. J. Periodontol 1991; 18:353-7
43. Review strength of evidence linking oral conditions and systemic diseases .compend contin
Educ Dent Suppl 2000; (30):12.23 quiz .65(http/ww.mcbi,nlm,gov)
44. Romero BC, Chiquito CS, Elejalde LE, Bemadoni CB. Relationship between periodontal
disease in pregnant women and the nutritional condition of their newboens. J. periodontal
2002; 73(10):1177-83
45. Samant A, Malik CP, Cabra SK, Devi PK. Gingivitis and periodontal disease in
pregnancy. J. Periodontol 1976; 47:415-8
46. Spahr A, Klein E, Khuseyinova N, et al. Periodontal infec- tions and coronary heart
disease: role of periodontal bac- teria and importance of total pathogen burden in the
Coro- nary Event and Periodontal Disease (CORODONT) study. Arch Intern Med.
2006;166(5):554-9.
47. Xiong X, Buekens P, Vastardis S, Pridjian G. Periodontal dis- ease and gestational
diabetes mellitus. Am J Obstet Gynecol. 2006;195(4):1086-9
48. Ann Periodontol. 1998 Jul;3(1):40-50.
APPENDIX I
WORK PLAN
TASK TO BE
PERFORMED
PLANNED
PERIOD
PERSONNEL
ASSIGNED TO
TASK
PERSON-DAYS
REQUIRED
1.Reseach proposal
preparation
7 weeks
01/06-09/07/2010
Researchers (2) 2 persons x35days
=70
2.Finalising the
research proposal and
its submission
8-9weeks
12/07-23/07/2010
Researchers(2)
Supervisor (1)
3personsx10days
=30
3.Ethical clearance and
permission to carry out
the study
10-11weeks
26/07-06/08/2010
Researchers (2) 2persons x10 days
=20
4.Contacting the
administration of
Muhima Hospital and
community contact to
orient to the project
12-13weeks
09/08-20/08/2010
Researchers (2)
Supervisor (1)
3persons x 10 days
=30
5.Data collection 14-17weeks
23/08-10/09/2010
Researchers (2) 2persons x 10 days
=20
6.Data coding, and
entry into computer
18 week
13-17/09/2010
Researchers (2) 2persons x 5 days
=10
7.Data analysis 19week
20-24/09/2010
Researchers (2)
Statistician (1)
3persons x 5 days
=15
8.Report writing(first
draft)
20week
27/09-01/10/2010
Researchers (2) 2persons x 5 days
=10
9.Report presentation 21week Researchers (2) 3persons x 5days
04-08/10/2010 Supervisor
=15
10. Report writing(final
draft)
22week
11-15/10/2010
Researchers (2) 2persons x 5 days
=10
11.Submission of final
report
23week
18-22/10/2010
Researchers (2) 2persons x 5 days
=10
12.Feedback to the
Director of Muhima
hospital
24week
25-29/10/2010
Researchers (2) 2persons x5 days
=10
Appendix II
GANTT CHART
TASKS TO
BE
PERFORMED
Year 2010
June July August September October
1. Research
proposal
preparation
XXXX
*** **
X
2. Finalizing
the research
proposal and
its submission
XX
3. Ethical
clearance and
permission to
carry out the
study
X X
4. Contacting
the
administration
of Muhima
Hospital and
community
contact to
orient to the
project
XX
5. Data
collection
X
** ***X
6. Data coding,
and entry into
computer
X
7. Data
analysis
X
8. Report
writing(first
draft)
**** *
9. Report
presentation
X
10. Report
writing(final
draft)
X
11. Submission
of final report X
12. Feedback
to the Director
of Muhima
hospital
X
Key items :
X : 1week=5days
*: 1day
Appendix III
PROJECT ORGANISATION
The fallowing persons have been involved in different tasks in the project organization.
RESEARCHER: Perceived the idea of doing the study, and carry out all activities of the
project
SUPERVISOR: Will assist the academic quality of project and give orientation to it
STATISTICIAN: Organization of statistical soft ware, put information on a spread sheet and
data analysis
LECTURER: Lecturer who has most knowledge and information about the topic will be
always consulted
KHI: Will provide an introductory letter for the researcher to MUHIMA Hospital, requesting
for permission to carry out the study and also funds for the study
APPENDIX IV
BUDGET FOR THE PROJECT
.
1.Preparation of the research proposal
No Items Number
of persons
Number
of days
Number
of
persons-
days
Unit
price(Rwf)
Total(Rwf)
1. Research
proposal
preparation
2 35 70 5000 350.000
2. Finalizing the
research
proposal and
its submission
3 15 30 5000 150.000
3. Ethical
clearance and
permission to
carry out the
study
2 10 20 5000 100.000
4. Contacting the
administration
of Muhima
Hospital, the
community to
orient
members to
the project
3 10 30 5000 150.000
Sub-total 1 800.000
2. Research activities
Activities Number
of
persons
Number
of days
Number of
persons/days
Unit
price(Rwf)
Total(Rwf)
1. Contacting the
administration of Muhima
Hospital, the community
to orient members to the
project
3 10 3x10=30 2000 60.000
2.Data collection 2 15 2x15=30 2000 60.000
3.Transport 3 130 3x130=390 1500 585.000
4.Restauration 3 130 3x130=390 1500 585.000
Sub-total 1.290.000
3. Statitionay and materials
No Items Quantity of
items
Unit price(Rwf Total(Rwf
1. Flash disk 1 15000 15000
2. Ream of papers 2 3000 6000
3. Pencils 1 dozen 2500 2500
4. Pens 1 dozen 1500 1500
5. Folder 2 3000 6000
6. Printing 410 copies 100 41000
7. Mineral water 50 bottles 300 15000
8. Dental mirrors 215 500 107500
9. Periodontal
probes
215 500 107500
10. Gloves for
examination
3 boxes 3000 9000
11. Gauzes 1box 3500 3500
12. Trays 215 2000 450000
13. Antiseptic
solution(alcohol)
2 tubes 4000 8000
Sub-total 764.500
4. Production of the report
No Items Quantity
of items
Number of
days
Number of
persons-
days
Unit
price(Rwf)
Total
(Rwf)
1. Crosscheck
and
verification
of data
1 3 3 8000 24000
2. Entering
data into
computer
2 5 10 3000 30.000
3. Data
analysis
3 3 9 5000 45.000
4. Report
writing(firs
t draft)
2 5 10 1500 15000
Sub-total 114.000
5. Report presentation/Validation
No Items Quantity
of items
Number of
days
Number of
persons-
days
Unit
price(Rwf)
Total
(Rwf)
1. Projector 1 1 - 70.000 70.000
2. Computer 1 1 - 50.000 50.000
3. Feedback
to the
Direction
of
Muhima
Hospital
3 1 3 5000 15.000
4. Room for
rent
1 1 - 20.000 20.000
Sub-total 155.000
6. BUDGET SUMMARY
No DESCRIPTION TOTAL
1. Preparation for research
proposal
800.000
2. Research activities 1.290.000
3. Stationary and materials 764.500
4. Production of the report 114.000
5. Report
presentation/Validation
155.000
GENERAL TOTAL 3.123.500
BUDGET JUSTIFICATION
The budget of the study is 3.123.500 Rfw which will be sufficient amount for finishing the all
activities planned during the study from the preparation of the research proposal up to the
report presentation/Validation
The financial support to accomplish the research will be KHI and other sponsors who will be
interested by the Project.
CURCULUM VITAE OF THE APPLICANT
No.1
I. IDENTIFICATION
Fist name: NSANZIMANA
Surname: Justin
Father’s name: GWIZA Faustin
Mother’s name: NYIRABAMBARI Aurélie
Marital status: Single
Current address: Kigali Health Institute
Cell: Cyabusheshe
Sector: Gitoki
District: Gatsibo
Province: Eastern
Country: Rwanda
Nationality: Rwandese
Mobile phone :( +250)0788578553
E-mail:[email protected]
II.SCHOOL ATTENDED
Name Level Year
Cyanika Primary school 1993-1999
Ndera Minor Seminary O-Level 1999-2002
Rwankuba Secondary School A-Level 2003-2005
(With the Option of BIO-CHEMISTRY)
Kigali Health Institute Institution 2007-2009
Other educational profile
Knowledge of Computer Microsoft word, Microsoft Excel,
Microsoft Power Point, Internet.
III. LANGUAGES
KINYARWANDA: Excellent
ENGLISH: Good
FRENCH: Good
KANSIIME OLIVER
Mobile phone: (+250)0788754519
Email: [email protected]
EDUCATION:
KIGALI HEALTH INSTITUTE(KHI) 2007-2010
Candidate for Bachelor of Science in Dentistry Kigali,
Rwanda
FAWE GIRLS’ SCHOOL 2003-
2006
Advanced Level Certificate in Biochemistry Kigali,
Rwanda
OTHER RELEVANT EXPERIENCE:
Muhima Hospital October
2007
Intern Kigali,
Rwanda
Assisted medical staff in care of patients in the department of radiology, volunteer care
treatment of HIV patients and maternity services
Living Positive Organization Nov 2008-January 2009
Intern Nairobi, Kenya
Worked as a nurse distributing medication for HIV patients and assisted with the counseling program.
LEADERSHIP EXPERIENCE
Orphans of Rwanda, Inc. 2007-2009
Group House Leader
Counseled and advised members of the group house on residence life issues.
Served as liaison between students and Orphans of Rwanda’s administration.
Kigali Health Institute May
2008
Participant in Oral Health Promotion Training
Attended week long training on oral health pathology related to trauma and prevention
methods.
Developed and implemented a treatment plan for five hundred primary and secondary school
students
Kigali Health Institute Jan 2007-
Dec 2007
Language Coordinator for EPLM
Coordinated the work of all class leaders and organized all language activities for the entire
campus.
Served as link between class leaders and Kigali Health Institute administration.
Secretary General in Dental student Association(KHIDSU) Present
2009
Awards and Honors
Orphans of Rwanda,Inc
Jan2007-Present
Scholar
Recipient of competitive scholarship that covers full university tuition and provides comprehensive
support services including tutoring, mentoring ,career development and life skills training
SKILLS
Microsoft Word, Microsoft Excel, and Internet-Proficient
LANGUAGES:
Kinyarwanda: Fluent, oral and written; English: Fluent, oral and written, French:
Intermediate, oral and written, Swahili: Basic, oral
REFERENCES:
RWAGATARE Joseph, Former FAWE Director, Tel: 0788517145
RUKESHANSHURO Charles Orphans or Rwanda, Tel: 0788486421
NTAKIRUTIMANA Jean Baptiste Former country Director ORI O788301303