Embed Size (px)
Citation preview

M elan o m a - An A id e M em o ire to Assist D iag n o sis
The aim of early detection of melanoma is to improve the cure rate of people who present w ith a melanoma.The general practitioner as doctor of first contact is the key to early diagnosis. To help diagnose melanomaearly the general practitioner needs to have appropriate observational and diagnostic skills and an aw arenessof the risk factors for melanoma. Melanoma may be found opportunistically during clinical examination forother indications. In the absence of any substantial evidence as to its effectiveness in reducing mortality frommelanoma, population-based skin screening cannot be recommended.
Patients w ho note disturbing skin lesions are frequently in a better position to observe changes andsymptoms of skin lesions than their doctors. If a patient expresses concern about a particular lesion,reassurance should be given only when there is no doubt about the nature of the lesion. If there is anydoubt, repeat observation after one to three months is essential.
Surgical excision biopsy with a 2 mm margin is the of choice if any signs suggestive of earlymelanoma are present. Partial biopsies i.e. shave or punch biopsies are nnoott appropriate except when excisionbiopsy is not possible. Locally advanced melanoma when recognised, is best referred for specialist carew ithout biopsy.
PRACTICE POINTS
• The history of a skin lesion is very important. A history of change in size, shape or colour is animportant clue to the diagnosis of melanoma. Intermittent itch is sometimes a symptom. Pain and/orbleeding are rare and indicate an advanced melanoma.
• Physical examination should assess the skin surface with high-quality illumination to detect lesions ofwhich the patient is unaw are. Melanoma seldom resembles other pigmented skin lesions - it is an“ ugly duckling” .
• Not all melanomas are black - variation in colour and multiple colours e.g. brown, tan, pink and areasof depigmentation are often indicators of malignancy; they are frequently present in melanoma andare useful in clinical diagnosis.
• For suspicious lesions, depending on the skill level of the GP, biopsy or referral should be considered.
• A period of observation (preferably for one to two months, but for a maximum of three months) maybe appropriate for clinically doubtful pigmented skin lesions. When waiting for the longer period,photography of the lesion is recommended to be used as a baseline to observe/compare any changesover the three months – warning patients not to wait, but to seek review if there are obvious changesbefore the three months. Another approach is to use a dermoscopy image capture device to detectchange over this time.
• Locally advanced melanoma should be referred to a specialist surgeon or where possible, to aspecialist melanoma clinic, w ithout biopsy.
CLINICAL DIAGNOSIS
General practitioners should be aware of the appearance and clinical types of melanoma. In most cases thediagnosis of melanoma is based on the ABCDE method of clinical diagnosis:A- asymmetryB- border irregularityC- colour variation NB - black is not essential and may not be present in some melanomas, eg. amelanotic or some
nodular melanomasD- diameter greater than 6 mm. However melanoma can be diagnosed when less than this diameterE- evolution and/or elevation eg. lesions may enlarge and a flat lesion may become raised in a matter of a few
weeks.
The bottom line is that general practitioners should strongly consider excision of lesions that are unusual, new,changing or difficult to diagnose.
Many melanomas will be diagnosed by the patient in the general observation of their own body. All patients andespecially those at high risk should be encouraged to undertake regular self examination using a mirror orinvolving a partner or carer in the process and be advised to be suspicious of new or changing lesions on the skin.
This aide-memoire has been developed to ass ist the diagnostic process and help improvethe outcome of clinical management of melanoma.
procedure
This aide-memoire has been developed to assist the diagnostic processand help improve the outcome of clinical management of melanoma.
M elan o m a - An A id e M em o ire to Assist D iag n o sis
The aim of early detection of melanoma is to improve the cure rate of people who present w ith a melanoma.The general practitioner as doctor of first contact is the key to early diagnosis. To help diagnose melanomaearly the general practitioner needs to have appropriate observational and diagnostic skills and an aw arenessof the risk factors for melanoma. Melanoma may be found opportunistically during clinical examination forother indications. In the absence of any substantial evidence as to its effectiveness in reducing mortality frommelanoma, population-based skin screening cannot be recommended.
Patients w ho note disturbing skin lesions are frequently in a better position to observe changes andsymptoms of skin lesions than their doctors. If a patient expresses concern about a particular lesion,reassurance should be given only when there is no doubt about the nature of the lesion. If there is anydoubt, repeat observation after one to three months is essential.
Surgical excision biopsy with a 2 mm margin is the of choice if any signs suggestive of earlymelanoma are present. Partial biopsies i.e. shave or punch biopsies are nnoott appropriate except when excisionbiopsy is not possible. Locally advanced melanoma when recognised, is best referred for specialist carew ithout biopsy.
PRACTICE POINTS
• The history of a skin lesion is very important. A history of change in size, shape or colour is animportant clue to the diagnosis of melanoma. Intermittent itch is sometimes a symptom. Pain and/orbleeding are rare and indicate an advanced melanoma.
• Physical examination should assess the skin surface with high-quality illumination to detect lesions ofwhich the patient is unaw are. Melanoma seldom resembles other pigmented skin lesions - it is an“ ugly duckling” .
• Not all melanomas are black - variation in colour and multiple colours e.g. brown, tan, pink and areasof depigmentation are often indicators of malignancy; they are frequently present in melanoma andare useful in clinical diagnosis.
• For suspicious lesions, depending on the skill level of the GP, biopsy or referral should be considered.
• A period of observation (preferably for one to two months, but for a maximum of three months) maybe appropriate for clinically doubtful pigmented skin lesions. When waiting for the longer period,photography of the lesion is recommended to be used as a baseline to observe/compare any changesover the three months – warning patients not to wait, but to seek review if there are obvious changesbefore the three months. Another approach is to use a dermoscopy image capture device to detectchange over this time.
• Locally advanced melanoma should be referred to a specialist surgeon or where possible, to aspecialist melanoma clinic, w ithout biopsy.
CLINICAL DIAGNOSIS
General practitioners should be aware of the appearance and clinical types of melanoma. In most cases thediagnosis of melanoma is based on the ABCDE method of clinical diagnosis:A- asymmetryB- border irregularityC- colour variation NB - black is not essential and may not be present in some melanomas, eg. amelanotic or some
nodular melanomasD- diameter greater than 6 mm. However melanoma can be diagnosed when less than this diameterE- evolution and/or elevation eg. lesions may enlarge and a flat lesion may become raised in a matter of a few
weeks.
The bottom line is that general practitioners should strongly consider excision of lesions that are unusual, new,changing or difficult to diagnose.
Many melanomas will be diagnosed by the patient in the general observation of their own body. All patients andespecially those at high risk should be encouraged to undertake regular self examination using a mirror orinvolving a partner or carer in the process and be advised to be suspicious of new or changing lesions on the skin.
This aide-memoire has been developed to ass ist the diagnostic process and help improvethe outcome of clinical management of melanoma.
procedure
Melanoma - An Aide Memoire to Assist Diagnosis The aim of early detection of melanoma is to improve the cure rate of people who present with a melanoma. The general practitioner as doctor of first contact is the key to early diagnosis. In the absence of any substantial evidence as to its effectiveness in reducing mortality from melanoma, population-based skin screening cannot be recommended. To help diagnose melanoma early the general practitioner needs to have appropriate observational and diagnostic skills and an awareness of the risk factors for melanoma. Melanoma may be found opportunistically during clinical examination for other indications.
Patients who note disturbing skin lesions are frequently in a better position to observe changes and symptoms of skin lesions than their doctors. If the patient expresses concern about a particular lesion, reassurance should be given only when there is no doubt about the nature of the lesion. If there is any doubt, repeat observation after one to three months is essential. Surgical excision biopsy with a 2 mm margin is the treatment of choice if any signs suggestive of early melanoma are present. Partial biopsies i.e. shave or punch biopsies are not appropriate except when excision biopsy is not possible. Locally advanced melanoma when recognised is best referred for specialist care without biopsy.
PRACTICE POINTS
The history of a skin lesion is very important. A history of change in size, shape or colour is an important clue to the diagnosis of melanoma. Intermittent itch is sometimes a symptom. Pain and/or bleeding are rare and indicate an advanced melanoma.
Physical examination should assess the skin surface with high-quality illumination to detect lesions of which the patient is unaware. Melanoma seldom resembles other pigmented skin lesions - it is an “ugly duckling”.
Not all melanomas are black - variation in colour and multiple colours e.g. brown, tan, pink and areas of depigmentation are useful indicators of malignancy; they are frequently present and are clinically useful.
For suspicious lesions, depending on the skill level of the GP, biopsy or referral should be considered.
A period of observation (preferably for one to two months but for a maximum of three months) may be appropriate for clinically doubtful pigmented skin lesions. When waiting for the longer period photography of the lesion is recommended to be used as a baseline to observe/compare any changes over the three months – warning patients not to wait, but to seek review if there are changes before the three months. Another approach is to use a dermoscopy image capture device to detect change over this time.
Locally advanced melanoma should be referred to a specialist surgeon or where possible, to a specialist melanoma clinic, without biopsy.
CLINICAL DIAGNOSIS
General practitioners should be aware of the appearance and clinical types of melanoma. In most cases the diagnosis of melanoma is based on the ABCDE method of clinical diagnosis: A- asymmetry B- border irregularity C- colour variation NB - black is not essential and may not be present in some melanomas, ie. nodular or amelanotic melanoma D- diameter greater than 6 mm. However melanoma can be diagnosed when less than this diameter E- evolution and /or elevation e.g. lesions may enlarge and a flat lesion may become raised in a matter of a few weeks.
The bottom line is that general practitioners should strongly consider excision for lesions that are unusual, new, changing or difficult to diagnose.
Many melanomas will be diagnosed by the patient in the general observation of their own body. All patients and especially those at high risk should be encouraged to undertake regular self examination using a mirror or involving a partner or carer in the process and be advised to be suspicious of new or changing lesions on the skin.
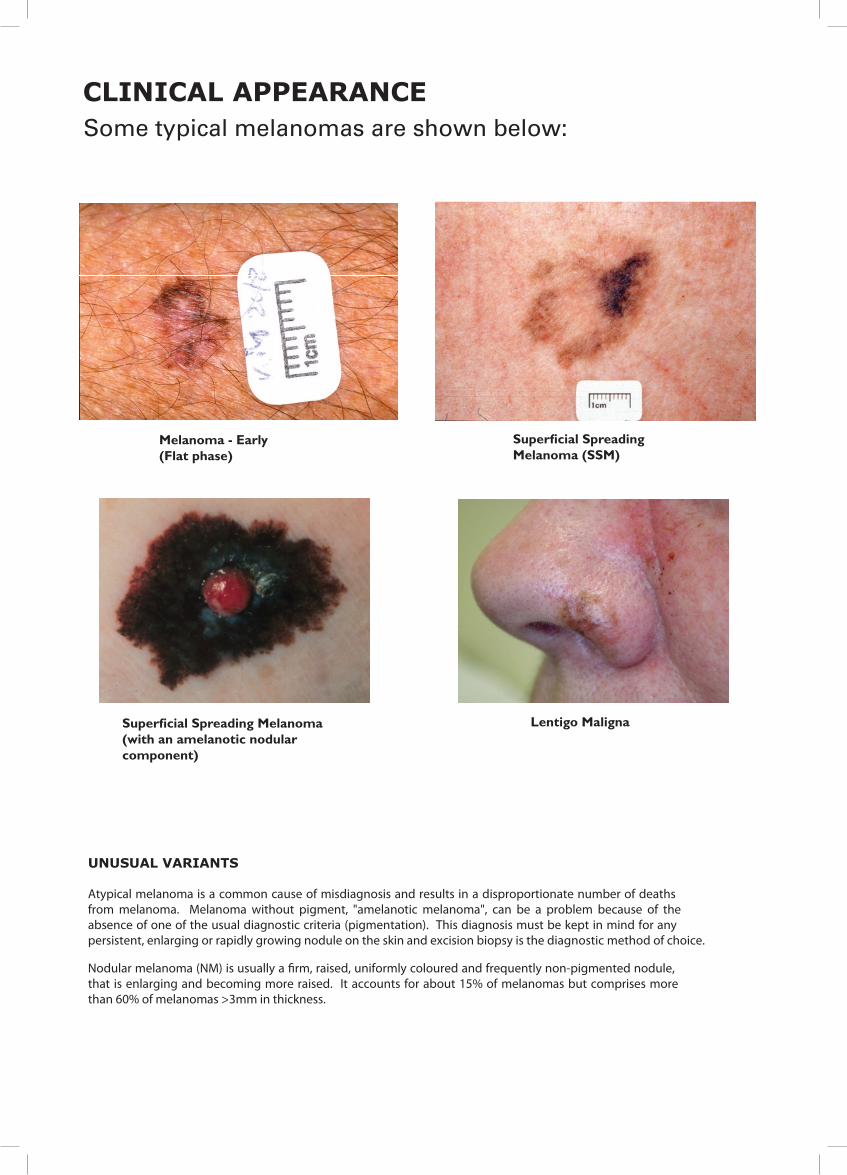
CLINICAL APPEARANCE
UNUSUAL VARIANTS
Atypical melanoma is a common cause of misdiagnosis and results in a disproportionate number of deaths from melanoma. Melanoma without pigment, "amelanotic melanoma", can be a problem because of the absence of one of the usual diagnostic criteria (pigmentation). This diagnosis must be kept in mind for any persistent, enlarging or rapidly growing nodule on the skin and excision biopsy is the treatment of choice.
Nodular melanoma (NM) is usually a firm, raised, uniformly coloured and frequently non-pigmented nodule, that is enlarging and becoming more raised. It accounts for about 15% of melanomas but comprises more than 60% of melanomas >3mm in thickness.
Some typical melanomas are shown below:
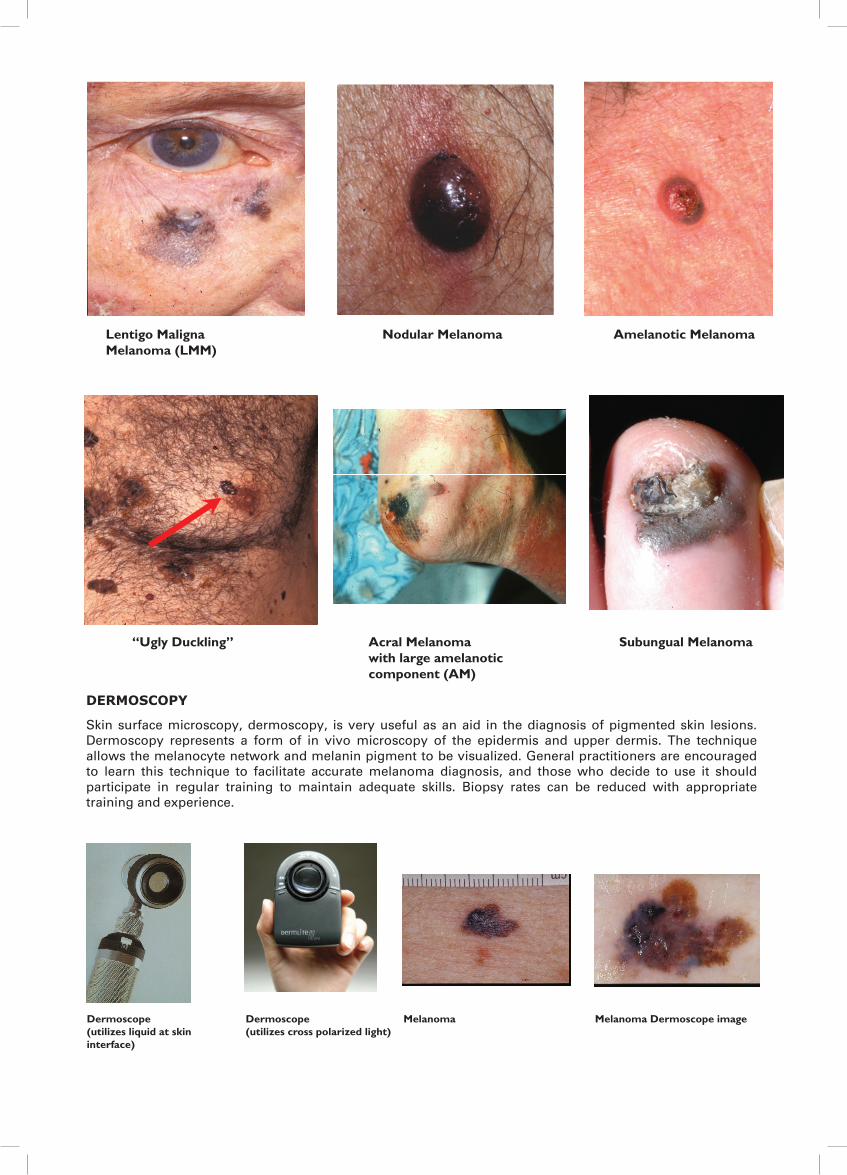
Acral Melanomawith large amelanoticcomponent (AM)
“Ugly Duckling” Nodular Melanoma Amelanotic melanoma
SubungualMelanoma
Lentigo MalignaMelanoma (LMM)
CLINICAL APPEARANCE
Some typical melanomas are shown below:
M elanom a - E arly S uperficia l S preading S uperficia l S preading(Flat phas e) M elanom a (S S M ) M elanom a (w ith an L entigo M aligna (L M )
am elanotic nodular com ponent)
L entigo M aligna A cral M ela nom a S ubungual “ U gly Duckling” N odular M elanom aM elanom a (LM M ) w ith large am elanotic M elanom a
com ponent (A M )
A m elanotic m elanom a
UNUSUAL VARIANTS
Atypical melanoma is a common cause of misdiagnosis and results in a disproportionate number of deathsfrom melanoma. Melanoma without pigment, "amelanotic melanoma", can be a problem because of theabsence of one of the usual diagnostic criteria (pigmentation). This diagnosis must be kept in mind for anypersistent, enlarging or rapidly growing nodule on the skin and excision biopsy is the diagnostic method of choice.
Nodular melanoma (NM) is usually a �rm, raised, uniformly coloured and frequently non-pigmented nodule,that is enlarging and becoming more raised. It accounts for about 15% of melanomas but comprises morethan 60% of melanomas >3mm in thickness.
DERMOSCOPY
Skin surface microscopy, dermoscopy, is very useful as an aid in the diagnosis of pigmented skin lesions.Dermoscopy represents a form of in vivo microscopy of the epidermis and upper dermis. The techniqueallows the melanocyte network and melanin pigment to be visualized. General practitioners are encouragedto learn this technique to facilitate accurate melanoma diagnosis, and those who decide to use it shouldparticipate in regular training to maintain adequate skills. Biopsy rates can be reduced with appropriatetraining and experience.
DERMOSCOPY
Skin surface microscopy, dermoscopy, is very useful as an aid in the diagnosis of pigmented skin lesions. Dermoscopy represents a form of in vivo microscopy of the epidermis and upper dermis. The technique allows the melanocyte network and melanin pigment to be visualized. General practitioners are encouraged to learn this technique to facilitate accurate melanoma diagnosis, and those who decide to use it should participate in regular training to maintain adequate skills. Biopsy rates can be reduced with appropriate training and experience.
Dermoscope Dermoscope Melanoma Melanoma: Dermoscopyimage(utilizes liquid at skin interface) (utilizes cross polarized light)
Superficial SpreadingMelanoma - Early
Superficial Spreading
Melanoma - Early(Flat phase)
Lentigo Maligna (LM)
Superficial SpreadingMelanoma (SSM)
Superficial SpreadingMelanoma (with an
Superficial SpreadingMelanoma (with anamelanotic nodular c
Melanoma (with anamelanotic nodular component)
Melanoma - Early(Flat phase)
Superficial Spreading Melanoma (SSM)
Superficial Spreading Melanoma (with an amelanotic nodularcomponent)
Lentigo Maligna
DERMOSCOPY
Skin surface microscopy, dermoscopy, is very useful as an aid in the diagnosis of pigmented skin lesions. Dermoscopy represents a form of in vivo microscopy of the epidermis and upper dermis. The technique allows the melanocyte network and melanin pigment to be visualized. General practitioners are encouraged to learn this technique to facilitate accurate melanoma diagnosis, and those who decide to use it should participate in regular training to maintain adequate skills. Biopsy rates can be reduced with appropriate training and experience.
Dermoscope Dermoscope Melanoma Melanoma: Dermoscopyimage(utilizes liquid at skin interface) (utilizes cross polarized light)
Superficial SpreadingMelanoma - Early
Superficial Spreading
Melanoma - Early(Flat phase)
Lentigo Maligna (LM)
Superficial SpreadingMelanoma (SSM)
Superficial SpreadingMelanoma (with an
Superficial SpreadingMelanoma (with anamelanotic nodular c
Melanoma (with anamelanotic nodular component)
CLINICAL APPEARANCE
UNUSUAL VARIANTS
Atypical melanoma is a common cause of misdiagnosis and results in a disproportionate number of deaths from melanoma. Melanoma without pigment, "amelanotic melanoma", can be a problem because of the absence of one of the usual diagnostic criteria (pigmentation). This diagnosis must be kept in mind for any persistent, enlarging or rapidly growing nodule on the skin and excision biopsy is the treatment of choice.
Nodular melanoma (NM) is usually a firm, raised, uniformly coloured and frequently non-pigmented nodule, that is enlarging and becoming more raised. It accounts for about 15% of melanomas but comprises more than 60% of melanomas >3mm in thickness.
Some typical melanomas are shown below:
Acral Melanomawith large amelanoticcomponent (AM)
“Ugly Duckling” Nodular Melanoma Amelanotic melanoma
SubungualMelanoma
Lentigo MalignaMelanoma (LMM)
CLIN
ICA
L A
PP
EA
RA
NC
E
UN
US
UA
L V
AR
IAN
TS
Aty
pic
al m
elan
om
a is
a c
om
mo
n c
ause
of
mis
dia
gn
osi
s an
d r
esu
lts
in a
dis
pro
po
rtio
nat
e n
um
ber
of
dea
ths
fro
m m
elan
om
a.
Mel
ano
ma
wit
ho
ut
pig
men
t, "
amel
ano
tic
mel
ano
ma"
, ca
n b
e a
pro
ble
m b
ecau
se o
f th
e ab
sen
ce o
f o
ne
of
the
usu
al d
iag
no
stic
cri
teri
a (p
igm
enta
tio
n).
T
his
dia
gn
osi
s m
ust
be
kep
t in
min
d f
or
any
per
sist
ent,
en
larg
ing
or
rap
idly
gro
win
g n
od
ule
on
th
e sk
in a
nd
exc
isio
n b
iop
sy is
th
e tr
eatm
ent
of
cho
ice.
No
du
lar
mel
ano
ma
(NM
) is
usu
ally
a f
irm
, rai
sed
, u
nif
orm
ly c
olo
ure
d a
nd
fre
qu
entl
y n
on
-pig
men
ted
no
du
le,
that
is
enla
rgin
g a
nd
bec
om
ing
mo
re r
aise
d.
It
acco
un
ts f
or
abo
ut
15%
of
mel
ano
mas
bu
t co
mp
rise
s m
ore
th
an 6
0% o
f m
elan
om
as >
3mm
in t
hic
knes
s.
So
me
typ
ical
mel
ano
mas
are
sh
ow
n b
elo
w:
Acr
alM
elan
om
aw
ith
larg
eam
elan
oti
cc o
mp
on
ent
(AM
)
“Ug
lyD
uck
lin
g”
No
du
lar
Mel
ano
ma
Am
elan
oti
cm
elan
om
a
Su
bu
ng
ual
Mel
ano
ma
Len
tig
oM
alig
na
Mel
ano
ma
(LM
M)
CLINICAL APPEARANCE
UNUSUAL VARIANTS
Atypical melanoma is a common cause of misdiagnosis and results in a disproportionate number of deaths from melanoma. Melanoma without pigment, "amelanotic melanoma", can be a problem because of the absence of one of the usual diagnostic criteria (pigmentation). This diagnosis must be kept in mind for any persistent, enlarging or rapidly growing nodule on the skin and excision biopsy is the treatment of choice.
Nodular melanoma (NM) is usually a firm, raised, uniformly coloured and frequently non-pigmented nodule, that is enlarging and becoming more raised. It accounts for about 15% of melanomas but comprises more than 60% of melanomas >3mm in thickness.
Some typical melanomas are shown below:
Acral Melanomawith large amelanoticcomponent (AM)
“Ugly Duckling” Nodular Melanoma Amelanotic melanoma
SubungualMelanoma
Lentigo MalignaMelanoma (LMM)
CLINICAL APPEARANCE
UNUSUAL VARIANTS
Atypical melanoma is a common cause of misdiagnosis and results in a disproportionate number of deaths from melanoma. Melanoma without pigment, "amelanotic melanoma", can be a problem because of the absence of one of the usual diagnostic criteria (pigmentation). This diagnosis must be kept in mind for any persistent, enlarging or rapidly growing nodule on the skin and excision biopsy is the treatment of choice.
Nodular melanoma (NM) is usually a firm, raised, uniformly coloured and frequently non-pigmented nodule, that is enlarging and becoming more raised. It accounts for about 15% of melanomas but comprises more than 60% of melanomas >3mm in thickness.
Some typical melanomas are shown below:
Acral Melanomawith large amelanoticcomponent (AM)
“Ugly Duckling” Nodular Melanoma Amelanotic melanoma
SubungualMelanoma
Lentigo MalignaMelanoma (LMM)
CLINICAL APPEARANCE
UNUSUAL VARIANTS
Atypical melanoma is a common cause of misdiagnosis and results in a disproportionate number of deaths from melanoma. Melanoma without pigment, "amelanotic melanoma", can be a problem because of the absence of one of the usual diagnostic criteria (pigmentation). This diagnosis must be kept in mind for any persistent, enlarging or rapidly growing nodule on the skin and excision biopsy is the treatment of choice.
Nodular melanoma (NM) is usually a firm, raised, uniformly coloured and frequently non-pigmented nodule, that is enlarging and becoming more raised. It accounts for about 15% of melanomas but comprises more than 60% of melanomas >3mm in thickness.
Some typical melanomas are shown below:
Acral Melanomawith large amelanoticcomponent (AM)
“Ugly Duckling” Nodular Melanoma Amelanotic melanoma
SubungualMelanoma
Lentigo MalignaMelanoma (LMM)
CLINICAL APPEARANCE
UNUSUAL VARIANTS
Atypical melanoma is a common cause of misdiagnosis and results in a disproportionate number of deaths from melanoma. Melanoma without pigment, "amelanotic melanoma", can be a problem because of the absence of one of the usual diagnostic criteria (pigmentation). This diagnosis must be kept in mind for any persistent, enlarging or rapidly growing nodule on the skin and excision biopsy is the treatment of choice.
Nodular melanoma (NM) is usually a firm, raised, uniformly coloured and frequently non-pigmented nodule, that is enlarging and becoming more raised. It accounts for about 15% of melanomas but comprises more than 60% of melanomas >3mm in thickness.
Some typical melanomas are shown below:
Acral Melanomawith large amelanoticcomponent (AM)
“Ugly Duckling” Nodular Melanoma Amelanotic melanoma
SubungualMelanoma
Lentigo MalignaMelanoma (LMM)Lentigo Maligna
Melanoma (LMM)Nodular Melanoma Amelanotic Melanoma
“Ugly Duckling” Acral Melanomawith large amelanoticcomponent (AM)
Subungual Melanoma
Dermoscope(utilizes liquid at skin interface)
Dermoscope(utilizes cross polarized light)
Melanoma Melanoma Dermoscope image
RISK FACTORS
The main risk factors for melanoma are:
• having a history of previous melanoma• the presence of many moles (50+) particularly atypical "dysplastic” naevi• a family history of melanoma (one or more)• a history of many sunburns• sun sensitive skin / fair complexion• patient age and sex (increasing age increases the risk of melanoma and males are at greater risk)
Any patient with a history of a previous melanoma has at least a �vefold increased risk of developing a subsequentmelanoma compared with the average population. Whilst the early follow up strategy (during the �rst fewyears following diagnosis and de�nitive treatment) will be particularly directed to monitoring for recurrenceof that tumour locally, in the regional node �elds and at distant sites, the hazard of a further new primarymelanoma needs to be recognized and these patients supervised appropriately, especially in the longer term.
At the present time, genetic testing has no speci�c value in the clinical management of patients who are atrisk for melanoma. Although some genes associated with melanoma have been detected in familialmelanoma patients, the prevalence of these gene changes is, as yet, too low to be clinically useful. Genetictesting is, however, of value to those clinicians and patients interested in clinical research studies – socontributing to �nding new facts and a basis for new treatments. Referral of high-risk patients to adermatologist or melanoma clinic for surveillance is appropriate.
PROGNOSIS
The thickness of a melanoma is the strongest predictor of outcome. In general, the thinner the lesion thebetter the prognosis.
Other features that have been shown to in�uence prognosis are:
• ulceration• mitotic rate• sex• age• site
POINTS TO REVIEW
• Achievement of a high level of survival of melanoma patients largely depends on early diagnosis by theprimary care clinician.
• Whilst current detection rates for melanoma with conventional diagnostic features are good they can beimproved further by increased awareness of the atypical forms of melanoma, especially the amelanoticand sparsely pigmented variants. Dermoscopy can prove a useful adjunct to diagnosis.
• Early diagnosis necessitates careful observation by the general practitioner of the body skin surface,examination of suspicious lesions with good illumination, with dermoscopy if possible, and awareness ofthe clinical appearance and risk factors for melanoma.
• High risk patients and their partners should be educated to recognise lesions suspicious of melanoma.Regular surveillance is necessary and should be supported by dermoscopy and total body photographyas required.
• High risk patients should be managed in consultation with appropriate specialists.
Based on Clinical Practice Guidelines for the Management of Melanoma in Australia and New Zealand (2008) pre-publicationhttp://www.cancer.org.au/Healthprofession als/clinicalguidelines/skincancer.htm (NHMRC approved 7 November 2008)
ACN wishes to thank the many volunteers who have helped in the development and re�nement of this aide-memoire.This aide-memoire was developed with funding received from the Australian Government.
November 2008
TOTAL BODY PHOTOGRAPHY (TBP)
TBP may be used in the follow-up of high risk patients, particularly those with large numbers of melanocytic ordysplastic naevi. Its role in management is still being determined





























