Embed Size (px)
Citation preview
1
Ovarian Cancer: Implications for the Pharmacist
Megan May, Pharm.D., BCOP
Objectives
Describe the etiology and pathophysiology of o arian cancerovarian cancer
Outline the efficacy and safety of treatment options for ovarian cancer
Explain the mechanism of action of poly ADP ribose polymerase inhibitors (PARP inhibitors) available for ovarian cancer
Explain how to evaluate the appropriate selection of therapy for specific ovarian cancer patients
2
Epidemiology
5th most frequent cause of death in women
Incidence in 2018 New cases: 22,240
Deaths: 14,070
Primarily post-menopausal disease Median age at diagnosis: 65-69 years old Median age at diagnosis: 65 69 years old
Caucasians > African American
National Cancer Institute. 2018.
Etiology/Pathogenesis
Sporadic ovarian cancer etiology unknownM (85 90%) Most common type (85-90%)
Familial and hereditary syndromes Less common type (10-15%)
“Incessant ovulation” theory Risk of developing ovarian cancer is related to number
of ovulatory cycles
Tumor suppressor genes BRCA1, BRCA2, p53
National Cancer Institute. 2018.
3
Pathology
Epithelial adenocarcinomaS Serous
Mucinous
Endometroid
Clear-cell
Germ-cell tumor
Sex-cord stromal
Metastatic from other malignancies
Risk Factors
Early menarche, late menopause and nulliparity
Increased age
Prolonged use of ovulatory‐stimulating drugs
Environmental and dietary factors
Residence in North American or Northern Europe
C i Caucasian race
Genetic factors
Hormone replacement therapy

4
Hereditary Risk
F il Hi t f O i C Lif ti Ri kFamily History of Ovarian Cancer Lifetime Risk
None 1.4 – 1.8%
1 first degree relative 3 – 5%
2 first-degree relatives 7 – 9%
Lynch Syndrome 6 – 10%
K BRCA 1 d/ BRCA 2 10 80%Known BRCA 1 and/or BRCA 2 germline mutation
10 – 80%
Ovarian Cancer Research Fund Alliance: Risk Factors. https://ocrfa.org/patients/about-ovarian-cancer/risk-factors/
Favorable Factors
Multiple pregnancies
f Breastfeeding
Use of prolonged oral contraceptives
Tubal ligation
Prophylactic oophorectomy
5
Screening
No effective screening test for ovarian cancer
/ f Low/standard risk (not familial or hereditary) Annual physical and pelvic examination
High risk (hereditary ovarian cancer, BRCA‐1 or BRCA‐2 positive) Pelvic examination, transvaginal ultrasound and
CA‐125 every 6‐12 months starting at age 25‐35
Gynecol Oncol 2007; 104:S14. Abstract 10
Prevention
Oral contraceptives Use for five or more years decreases risk of ovarian
cancer by 50% or more
Longer the use, greater the protection Protection can continue for up to 30 years after stopping use
Prophylactic oophorectomy Decreases risk of ovarian cancer in high‐risk patients
6
Signs and Symptoms
Bloating Pel ic or abdominal pain Pelvic or abdominal pain Eating satiety Urinary symptoms (frequency or urgency) GI symptoms Pulmonary symptoms Unilateral or bilateral, solid, cystic and/or complex
pelvic or adnexal masses CA-125 highly elevated
Staging
International Federation of Gynecologic Oncologists (FIGO) and AJCC staging s stems (stages I IV)(FIGO) and AJCC staging systems (stages I-IV)
Grade 1: well differentiated
2: moderately differentiated
3: poorly differentiated
AJCC Cancer Staging Manual, Sixth Edition (2002)
7
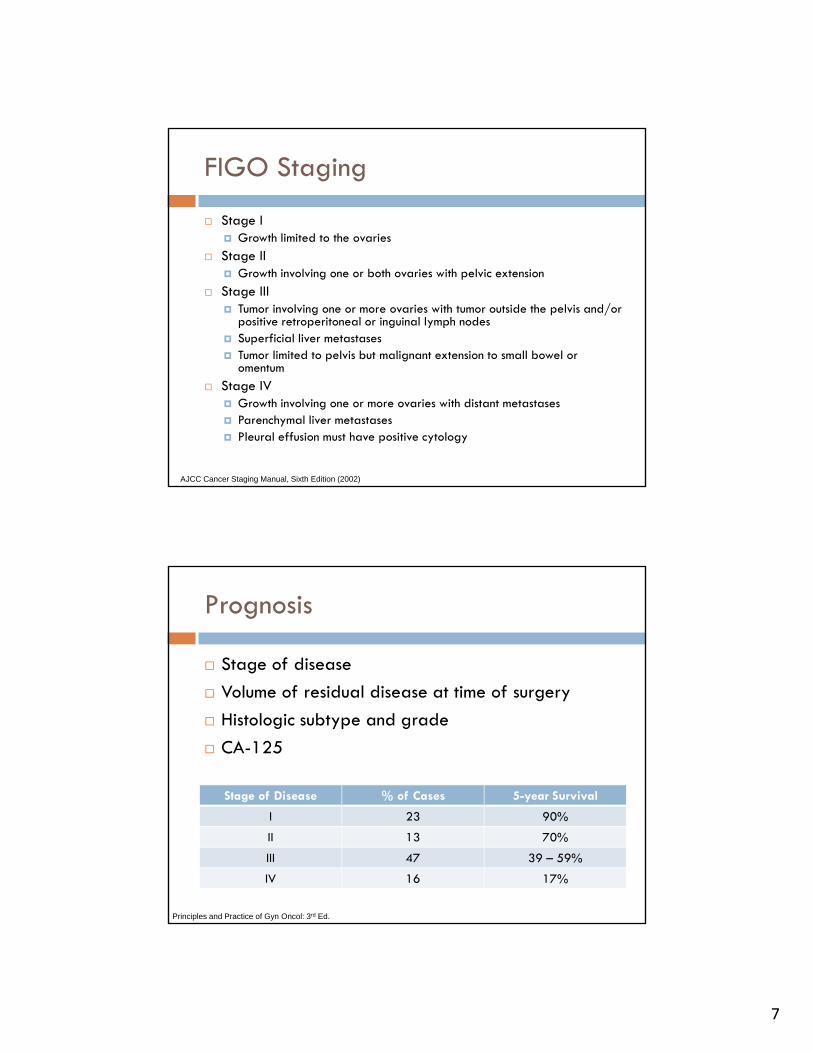
FIGO Staging
Stage I Growth limited to the ovaries
Stage II Growth involving one or both ovaries with pelvic extension
Stage III Tumor involving one or more ovaries with tumor outside the pelvis and/or
positive retroperitoneal or inguinal lymph nodes Superficial liver metastases Tumor limited to pelvis but malignant extension to small bowel or
omentumomentum
Stage IV Growth involving one or more ovaries with distant metastases Parenchymal liver metastases Pleural effusion must have positive cytology
AJCC Cancer Staging Manual, Sixth Edition (2002)
Prognosis
Stage of disease
f f
Stage of Disease % of Cases 5-year Survival
Volume of residual disease at time of surgery
Histologic subtype and grade
CA-125
I 23 90%
II 13 70%
III 47 39 – 59%
IV 16 17%
Principles and Practice of Gyn Oncol: 3rd Ed.
8
Primary Treatment (Stages I-II)
Comprehensive surgical stagingO i l < 1 id l di Optimal: < 1 cm residual disease
Suboptimal: > 1 cm residual disease
Adjuvant combination chemotherapy Taxane + platinum
Number of cycles (3 or 6) varies by stage
Observation in stage 1A or 1B
PDQ® Adult Treatment Editorial Board. PDQ Ovarian Epithelial, Fallopian Tube, and Primary Peritoneal Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated 07/19/2018. Available at: https://www.cancer.gov/types/ovarian/patient/ovarian-epithelial-treatment-pdq. Accessed 09/04/2018.
GOG-157
Early stage ovarian cancer, high-risk features (n = 457)(n = 457)
Randomized following surgery to 3 vs. 6 cycles of paclitaxel + carboplatin
Recurrence rate 33% lower in patients treated with 6 cycles (HR: 0.627, not statistically significant)
Grade 2 neurotoxicity in 2% vs. 11% patients
Bell J, et al. Gynceol Oncol. 2006;102(3):432-439.
9
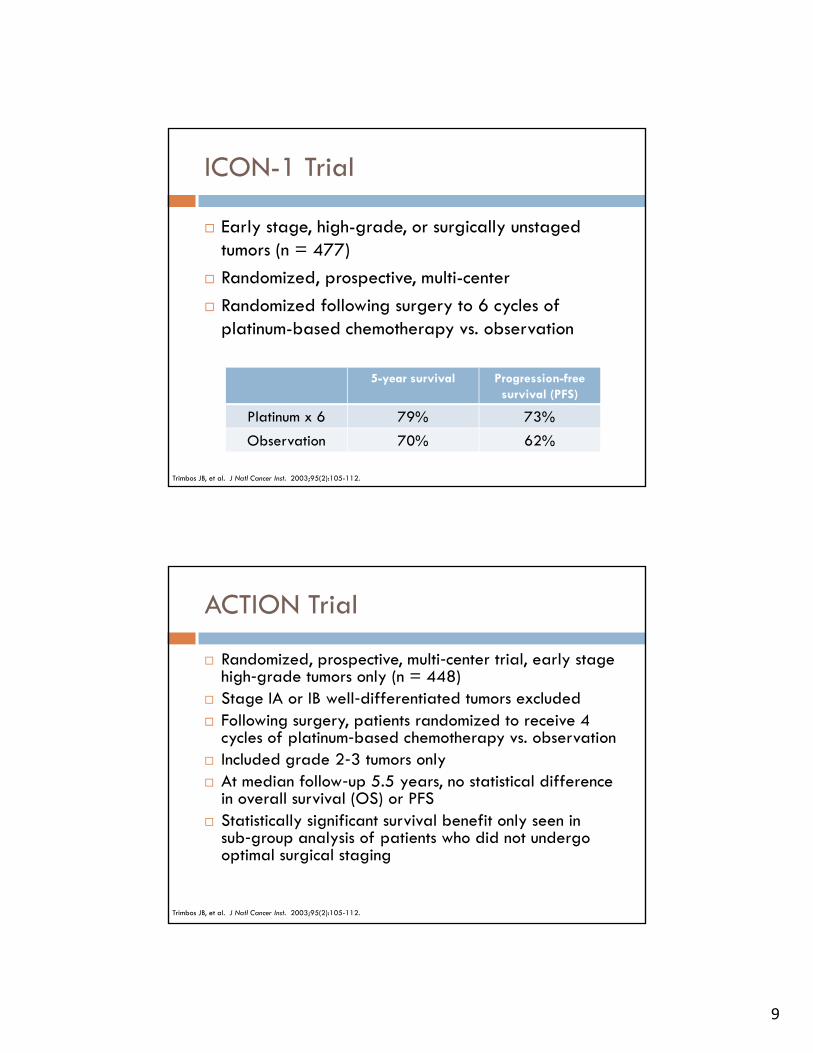
ICON-1 Trial
Early stage, high-grade, or surgically unstagedt mors (n = 477)tumors (n = 477)
Randomized, prospective, multi-center
Randomized following surgery to 6 cycles of platinum-based chemotherapy vs. observation
5-year survival Progression-free survival (PFS)
Platinum x 6 79% 73%
Observation 70% 62%
Trimbos JB, et al. J Natl Cancer Inst. 2003;95(2):105-112.
ACTION Trial
Randomized, prospective, multi‐center trial, early stage high‐grade tumors only (n = 448)g g y ( )
Stage IA or IB well‐differentiated tumors excluded Following surgery, patients randomized to receive 4
cycles of platinum‐based chemotherapy vs. observation Included grade 2‐3 tumors only At median follow‐up 5.5 years, no statistical difference
in overall survival (OS) or PFS( ) Statistically significant survival benefit only seen in
sub‐group analysis of patients who did not undergo optimal surgical staging
Trimbos JB, et al. J Natl Cancer Inst. 2003;95(2):105-112.
10
Advance Stage (Stages III-IV)
Comprehensive surgical staging
f Six cycles of adjuvant combination chemotherapy with taxane + platinum or liposomal doxorubicin + carboplatin Intraperitoneal chemotherapy may be an option in
stage II or III
O ll d h h Occasionally, neoadjuvant chemotherapy
PDQ® Adult Treatment Editorial Board. PDQ Ovarian Epithelial, Fallopian Tube, and Primary Peritoneal Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated 07/19/2018. Available at: https://www.cancer.gov/types/ovarian/patient/ovarian-epithelial-treatment-pdq. Accessed 09/04/2018.
Adjuvant Chemotherapy
GOG-111 Paclitaxel + cisplatin improves median survival Paclitaxel + cisplatin improves median survival
compared to cyclophosphamide + cisplatin
GOG-158 Paclitaxel + carboplatin preferred over paclitaxel +
cisplatin due to equal efficacy and reduced toxicity
SCOTROC trial Docetaxel is equally efficacious and less neurotoxic
than paclitaxel when given in combination with carboplatin
Muggia F, et al. JCO. 2000;18(1):106-115.Bookman MA, et al. Int J Gynecol Cancer. 2003;13(6):735-740.Vasey PA, et al. J Natl Cancer Inst. 2004;96:1682-1691.
11
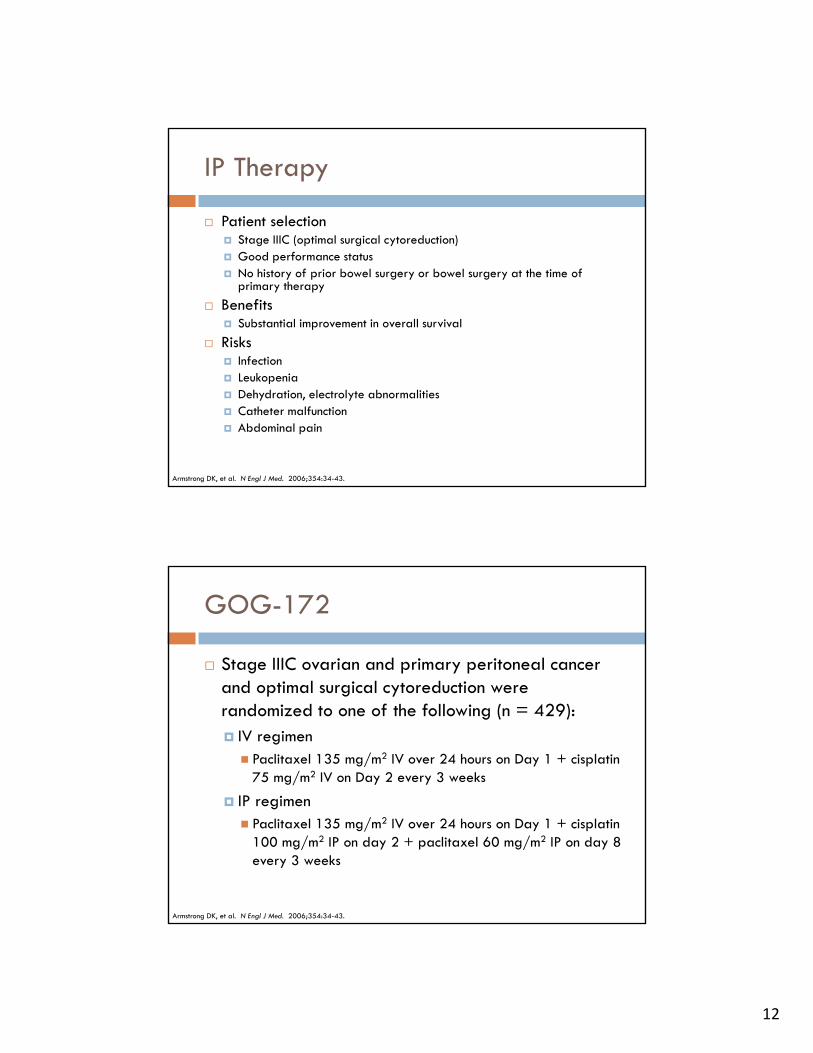
Cisplatin versus Carboplatin
Neurotoxicity Nephrotoxicity N/V
In patients with optimally resected stage III ovarian cancer
Cisplatin +++*paclitaxel 24h infusion
+++ +++
Carboplatin +*paclitaxel 3h infusion
+ ++
Ozols RF JCO 2003;21:3194-3200; GOG 158
Complete remission and overall survival not different between cisplatin/paclitaxel and carboplatin/paclitaxel
Carboplatin regimen easier to administer
Paclitaxel versus Docetaxel
NeurotoxicityG d 2 & 3 h i h li l Greater grade 2 & 3 neuropathy with paclitaxel
Neutropenia Greater grade 4 neutropenia with docetaxel
Edema Greater with docetaxel
12
IP Therapy
Patient selection Stage IIIC (optimal surgical cytoreduction) Good performance status No history of prior bowel surgery or bowel surgery at the time of
primary therapy
Benefits Substantial improvement in overall survival
Risks Infection Leukopenia Dehydration, electrolyte abnormalities Catheter malfunction Abdominal pain
Armstrong DK, et al. N Engl J Med. 2006;354:34-43.
GOG-172
Stage IIIC ovarian and primary peritoneal cancer and optimal s rgical c tored ction were and optimal surgical cytoreduction were randomized to one of the following (n = 429): IV regimen Paclitaxel 135 mg/m2 IV over 24 hours on Day 1 + cisplatin
75 mg/m2 IV on Day 2 every 3 weeks
IP regimen IP regimen Paclitaxel 135 mg/m2 IV over 24 hours on Day 1 + cisplatin
100 mg/m2 IP on day 2 + paclitaxel 60 mg/m2 IP on day 8 every 3 weeks
Armstrong DK, et al. N Engl J Med. 2006;354:34-43.
13
GOG-172
Median PFS and OS at five years significantly improved for patients on IP treatment arm (18.3 vs. 23.8 months and 49.7
6 6 h l )vs 65.6 months, respectively) Grade 3 and 4 toxicities were significantly worse in patients
treated with IP therapy Only 42% of patients randomized to IP therapy completed six
cycles of treatment (median=3)
Patients unable to tolerate IP therapy were switched to the IV treatment arm
QOL was significantly worse for patients in the IP arm while on treatment At 12 months, there was no difference in QOL between the two
groups
Armstrong DK, et al. N Engl J Med. 2006;354:34-43.
Bevacizumab
FDA-approved in combination with liposomal doxorubicin paclitaxel or topotecandoxorubicin, paclitaxel, or topotecan OCEANS Trial AURELIA Trial
Bevacizumab in combination with paclitaxel + carboplatin GOG-0213
Bevacizumab monotherapy GOG-0170D CCC-PHII-45
PDQ® Adult Treatment Editorial Board. PDQ Ovarian Epithelial, Fallopian Tube, and Primary Peritoneal Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated 07/19/2018. Available at: https://www.cancer.gov/types/ovarian/patient/ovarian-epithelial-treatment-pdq. Accessed 09/04/2018.
14
GOG-218
Phase III randomized, double‐blind trial Patients with stage III or IV, any gross residual disease Patients with stage III or IV, any gross residual disease
(n = 1873) Following surgery, patients were randomized standard
chemotherapy (paclitaxel + carboplatin) cycles 1‐6 and either Placebo (cycle 2‐5) followed by placebo every 3 weeks for
15 months B b 15 /k ( l 2 5) f ll d b l b Bevacizumab 15 mg/kg (cycle 2‐5) followed by placebo every 3 weeks for 15 months
Bevacizumab 15 mg/kg (cycle 2‐5) followed by bevacizumab 15 mg/kg every 3 weeks for 15 months
Burger RA, et al. J Clin Oncol. 2010;28:18S
GOG-218
Statistically significant increase in PFS for patients treated on the chemotherapy + bevacizumab + treated on the chemotherapy + bevacizumab + bevacizumab maintenance (14.1 months) vs. chemotherapy + bevacizumab + placebo maintenance (11.2 months) vs. chemotherapy alone (10.3 months) (HR=0.72)
Preliminary OS data shows no difference between groups
No difference in QOL detected between any of the three groups
Burger RA, et al. J Clin Oncol. 2010;28:18S
15
ICON-7
Phase III, randomized, open label
Patients with stage I‐IV, optimal or suboptimal disease (n=1528)
Following surgery, patients were randomized Standard chemotherapy
Chemotherapy + bevacizumab 7.5 mg/kg every 3 weeks followed by bevacizumab 7.5 mg/kg maintenance every 3 weeks for 12 cycle (total one year of bevacizumab)
Perren TJ, et al. N Engl J Med. 2011;365:2484-2496.
ICON-7
At 42 months, the median PFS was modestly improved in the treatment arm vs the control arm improved in the treatment arm vs. the control arm (24.1 months vs. 22.4 months, HR=0.81)
Effect of bevacizumab was greater in patients at high risk for progression (PFS 18 months vs. 14.5 months)
Median OS was improved in the high risk patient p g ppopulation (36 months vs. 28 months)
Toxicity was greater in the bevacizumab treated patients
Perren TJ, et al. N Engl J Med. 2011;365:2484-2496.
16
Recurrent, Refractory, and Resistant Ovarian Cancer
60‐80% of ovarian cancer patients
f Length of subsequent remissions is shorter than the initial remission
Goal of treatment Improve/eliminate symptoms
Achieve an objective response
Improve quality of life
Delay time to symptomatic disease
Prolong survival if possible
PDQ® Adult Treatment Editorial Board. PDQ Ovarian Epithelial, Fallopian Tube, and Primary Peritoneal Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated 07/19/2018. Available at: https://www.cancer.gov/types/ovarian/patient/ovarian-epithelial-treatment-pdq. Accessed 09/04/2018.
Definitions
Platinum‐sensitive disease Initial response to platinum Duration of initial remission > 6 months Longer the initial remission, the greater the likelihood of responding to
second and third‐line agents Probability of response to chemotherapy is 30% or more
Platinum‐resistant disease Initial response to platinum Duration of initial remission < 6 months P b bilit f t dditi l t t t i 10 15% Probability of response to additional treatment is 10‐15%
Primary progressive (platinum‐refractory) disease No response and/or progression of disease during primary therapy with
platinum Worst prognosis Probability of response to additional chemotherapy <10%
PDQ® Adult Treatment Editorial Board. PDQ Ovarian Epithelial, Fallopian Tube, and Primary Peritoneal Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated 07/19/2018. Available at: https://www.cancer.gov/types/ovarian/patient/ovarian-epithelial-treatment-pdq. Accessed 09/04/2018.
17
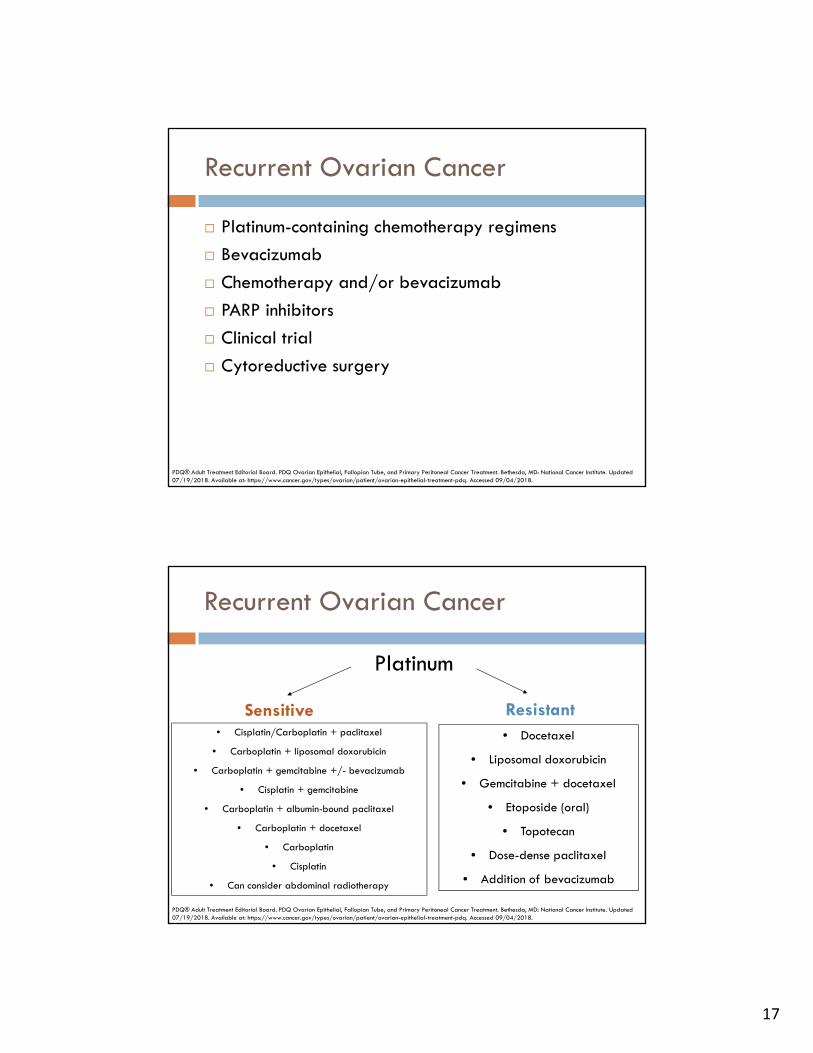
Recurrent Ovarian Cancer
Platinum-containing chemotherapy regimens
Bevacizumab
Chemotherapy and/or bevacizumab
PARP inhibitors
Clinical trial
Cytoreductive surgery Cytoreductive surgery
PDQ® Adult Treatment Editorial Board. PDQ Ovarian Epithelial, Fallopian Tube, and Primary Peritoneal Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated 07/19/2018. Available at: https://www.cancer.gov/types/ovarian/patient/ovarian-epithelial-treatment-pdq. Accessed 09/04/2018.
Platinum
Recurrent Ovarian Cancer
Sensitive Resistant• Cisplatin/Carboplatin + paclitaxel
• Carboplatin + liposomal doxorubicin
• Carboplatin + gemcitabine +/- bevacizumab
• Cisplatin + gemcitabine
• Docetaxel
• Liposomal doxorubicin
• Gemcitabine + docetaxel
Et id ( l)• Carboplatin + albumin-bound paclitaxel
• Carboplatin + docetaxel
• Carboplatin
• Cisplatin
• Can consider abdominal radiotherapy
• Etoposide (oral)
• Topotecan
• Dose-dense paclitaxel
• Addition of bevacizumab
PDQ® Adult Treatment Editorial Board. PDQ Ovarian Epithelial, Fallopian Tube, and Primary Peritoneal Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated 07/19/2018. Available at: https://www.cancer.gov/types/ovarian/patient/ovarian-epithelial-treatment-pdq. Accessed 09/04/2018.
18
PARP Inhibitors
Poly ADP-ribose polymerase inhibitorDNA i h i DNA repair mechanism
BRCA mutated cells more dependent on this mechanism
Directly inhibits PARP 1, 2, 3 and increases formation of PARP-DNA complexes, preventing DNA repair cell death
FDA approved PARP inhibitors FDA- approved PARP inhibitors Rucaparib (Rubraca®)
Olaparib (Lynparza®)
Niraparib (Zejula®)
PDQ® Adult Treatment Editorial Board. PDQ Ovarian Epithelial, Fallopian Tube, and Primary Peritoneal Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated 07/19/2018. Available at: https://www.cancer.gov/types/ovarian/patient/ovarian-epithelial-treatment-pdq. Accessed 09/04/2018.
FDA-Approved Ovarian Cancer Indications
Rucaparib Treatment of advanced ovarian cancer with gBRCA or sBRCA ≥2 prior lines of chemotherapy Maintenance treatment of recurrent ovarian cancer in complete or
partial response to platinum-based chemotherapy
Olaparib Treatment of advanced ovarian cancer with gBRCA ≥3 prior lines of chemotherapy Maintenance treatment of recurrent ovarian cancer in complete or Maintenance treatment of recurrent ovarian cancer in complete or
partial response to platinum-based chemotherapy
Niraparib Maintenance treatment of recurrent ovarian cancer in complete or
partial response to platinum-based chemotherapy
Rubraca [prescribing information]. Clovis Oncology. 2017.Lynparza [prescribing information]. AstraZenca. 2018.Zejula [prescribing information]. Tesaro. 2018.
19
FDA-Approved Dosing
Rucaparib 600 mg by mouth twice daily 600 mg by mouth twice daily Tablet available: 200 mg, 250 mg, 300 mg
Olaparib 400 mg capsule by mouth twice daily Capsule available: 50 mg
300 mg tablet by mouth twice daily Tablet available 100 mg and 150 mg Tablet available: 100 mg and 150 mg
Niraparib 300 mg by mouth once daily Capsule available: 100 mg
Rubraca [prescribing information]. Clovis Oncology. 2017.Lynparza [prescribing information]. AstraZenca. 2018.Zejula [prescribing information]. Tesaro. 2018.
TreatmentA i i i l d i h i k h
Treatment versus Maintenance Therapy
An initial treatment used in attempt to shrink the current tumor
Maintenance therapy Continuing to treat after completion of standard round
of chemotherapy U d t id l th ’ t Used to avoid or slow the cancer’s return
Slow the growth of advanced cancer after the initial treatment
20
Benefits
Risk/Benefits of Maintenance Therapy
May help keep cancer from coming back
May slow down cancer growth
Disadvantages Side effects
Treatment cost Treatment cost
More doctor visits
Limited information on long term side effects and benefits for each individual
All have a similar side effects, but some are more common and/or more se ere in one ers s another
PARP Inhibitor Side Effects
common and/or more severe in one versus another
Acute myeloid leukemia/myelodysplastic syndrome has been reported in 0.5%-2% of patients
Thompson LA. Oncology Nurse Advisor. 2017.
21
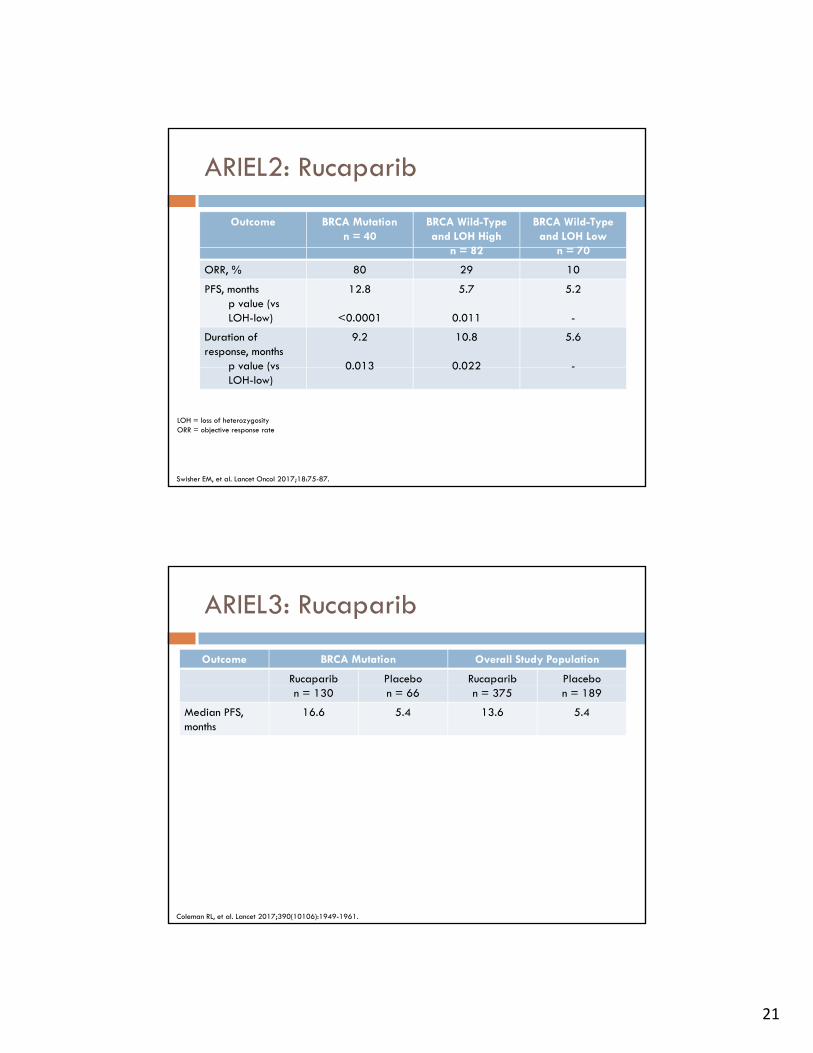
ARIEL2: Rucaparib
Outcome BRCA Mutationn = 40
BRCA Wild-Type and LOH High
82
BRCA Wild-Type and LOH Low
70n = 82 n = 70
ORR, % 80 29 10
PFS, monthsp value (vs LOH-low)
12.8
<0.0001
5.7
0.011
5.2
-
Duration of response, months
p value (vs
9.2
0 013
10.8
0 022
5.6
-p value (vs LOH-low)
0.013 0.022 -
Swisher EM, et al. Lancet Oncol 2017;18:75-87.
LOH = loss of heterozygosityORR = objective response rate
ARIEL3: Rucaparib
Outcome BRCA Mutation Overall Study Population
Rucaparib Placebo Rucaparib Placebon = 130 n = 66 n = 375 n = 189
Median PFS, months
16.6 5.4 13.6 5.4
Coleman RL, et al. Lancet 2017;390(10106):1949-1961.
22
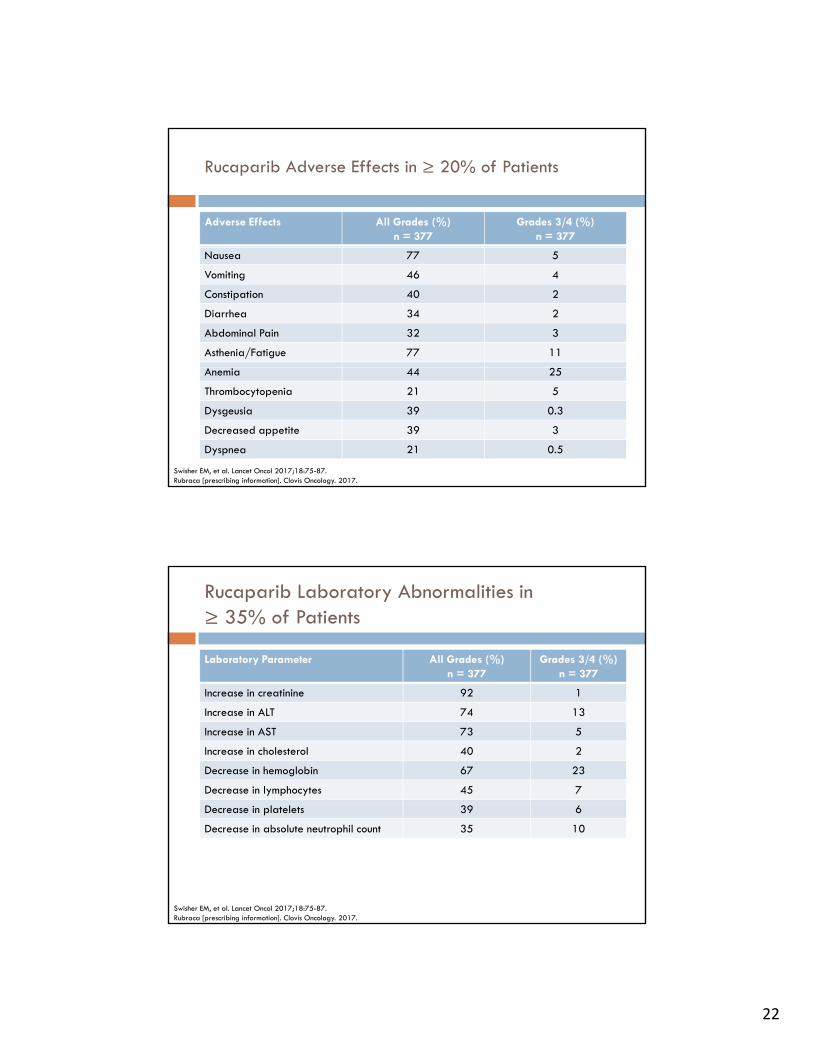
Rucaparib Adverse Effects in ≥ 20% of Patients
Adverse Effects All Grades (%)n = 377
Grades 3/4 (%)n = 377
Nausea 77 5
Vomiting 46 4
Constipation 40 2
Diarrhea 34 2
Abdominal Pain 32 3
Asthenia/Fatigue 77 11
Anemia 44 25
Thrombocytopenia 21 5
Dysgeusia 39 0.3
Decreased appetite 39 3
Dyspnea 21 0.5
Swisher EM, et al. Lancet Oncol 2017;18:75-87.Rubraca [prescribing information]. Clovis Oncology. 2017.
Rucaparib Laboratory Abnormalities in ≥ 35% of Patients
Laboratory Parameter All Grades (%)n = 377
Grades 3/4 (%)n = 377
Increase in creatinine 92 1
Increase in ALT 74 13
Increase in AST 73 5
Increase in cholesterol 40 2
Decrease in hemoglobin 67 23
Decrease in lymphocytes 45 7
Decrease in platelets 39 6
Decrease in absolute neutrophil count 35 10
Swisher EM, et al. Lancet Oncol 2017;18:75-87.Rubraca [prescribing information]. Clovis Oncology. 2017.
23
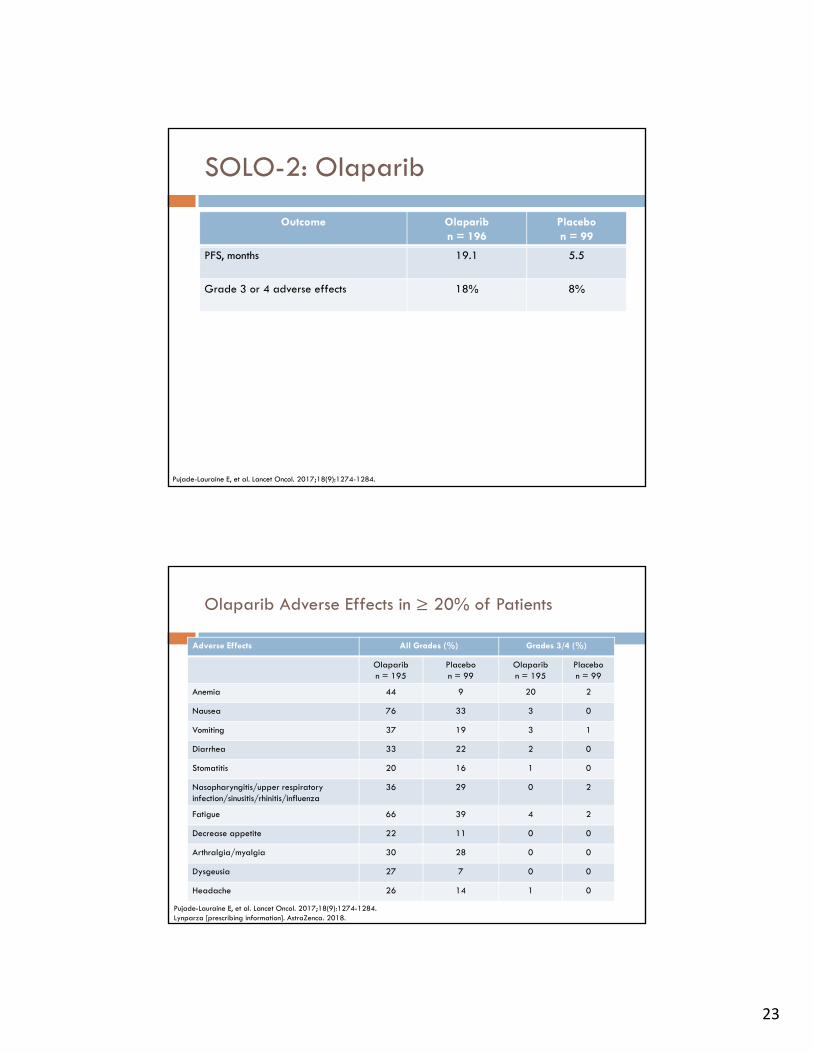
SOLO-2: Olaparib
Outcome Olaparibn = 196
Placebon = 99
PFS, months 19.1 5.5
Grade 3 or 4 adverse effects 18% 8%
Pujade-Lauraine E, et al. Lancet Oncol. 2017;18(9):1274-1284.
Olaparib Adverse Effects in ≥ 20% of Patients
Adverse Effects All Grades (%) Grades 3/4 (%)
Olaparibn = 195
Placebon = 99
Olaparibn = 195
Placebon = 99
Anemia 44 9 20 2
Nausea 76 33 3 0
Vomiting 37 19 3 1
Diarrhea 33 22 2 0
Stomatitis 20 16 1 0
Nasopharyngitis/upper respiratory infection/sinusitis/rhinitis/influenza
36 29 0 2
Fatigue 66 39 4 2
Decrease appetite 22 11 0 0
Arthralgia/myalgia 30 28 0 0
Dysgeusia 27 7 0 0
Headache 26 14 1 0
Pujade-Lauraine E, et al. Lancet Oncol. 2017;18(9):1274-1284.Lynparza [prescribing information]. AstraZenca. 2018.
24
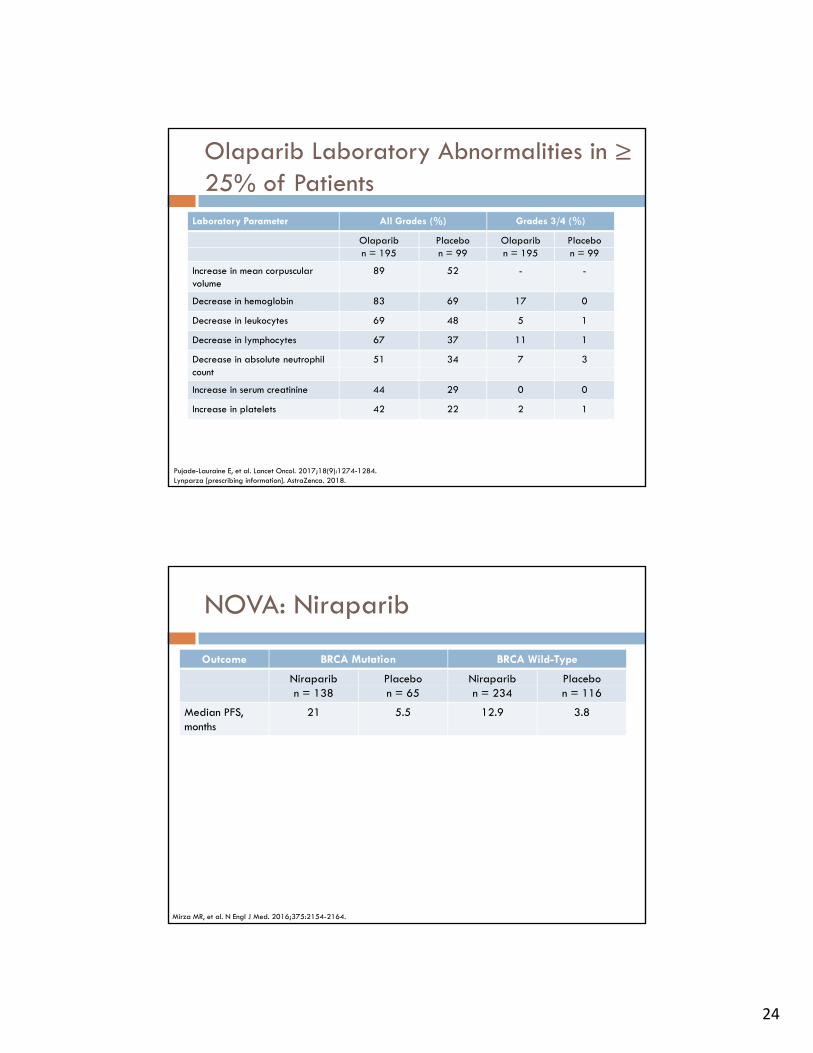
Olaparib Laboratory Abnormalities in ≥ 25% of Patients
Laboratory Parameter All Grades (%) Grades 3/4 (%)
Olaparib Placebo Olaparib Placebon = 195 n = 99 n = 195 n = 99
Increase in mean corpuscular volume
89 52 - -
Decrease in hemoglobin 83 69 17 0
Decrease in leukocytes 69 48 5 1
Decrease in lymphocytes 67 37 11 1
Decrease in absolute neutrophil 51 34 7 3count
Increase in serum creatinine 44 29 0 0
Increase in platelets 42 22 2 1
Pujade-Lauraine E, et al. Lancet Oncol. 2017;18(9):1274-1284.Lynparza [prescribing information]. AstraZenca. 2018.
NOVA: Niraparib
Outcome BRCA Mutation BRCA Wild-Type
Niraparib Placebo Niraparib Placebon = 138 n = 65 n = 234 n = 116
Median PFS, months
21 5.5 12.9 3.8
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.
25
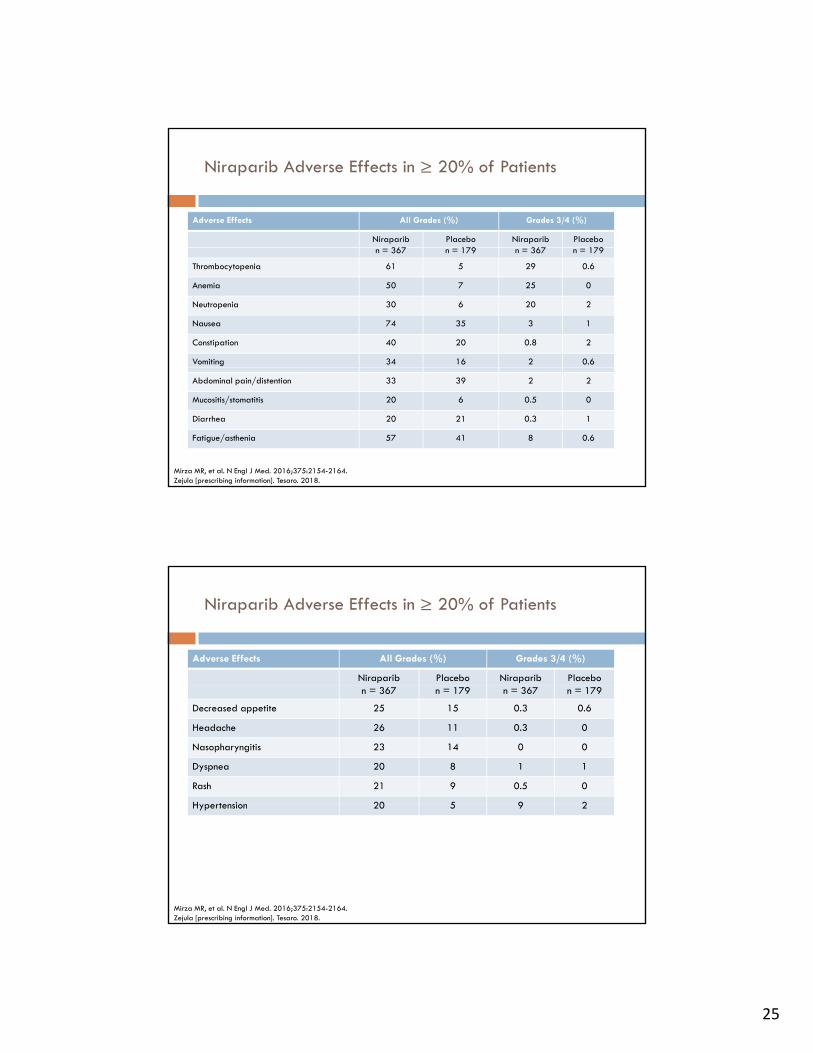
Niraparib Adverse Effects in ≥ 20% of Patients
Adverse Effects All Grades (%) Grades 3/4 (%)
Niraparib 367
Placebo 179
Niraparib 367
Placebo 179n = 367 n = 179 n = 367 n = 179
Thrombocytopenia 61 5 29 0.6
Anemia 50 7 25 0
Neutropenia 30 6 20 2
Nausea 74 35 3 1
Constipation 40 20 0.8 2
Vomiting 34 16 2 0.6
Abdominal pain/distention 33 39 2 2
Mucositis/stomatitis 20 6 0.5 0
Diarrhea 20 21 0.3 1
Fatigue/asthenia 57 41 8 0.6
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.Zejula [prescribing information]. Tesaro. 2018.
Niraparib Adverse Effects in ≥ 20% of Patients
Adverse Effects All Grades (%) Grades 3/4 (%)
Niraparib Placebo Niraparib Placebon = 367 n = 179 n = 367 n = 179
Decreased appetite 25 15 0.3 0.6
Headache 26 11 0.3 0
Nasopharyngitis 23 14 0 0
Dyspnea 20 8 1 1
Rash 21 9 0.5 0
Hypertension 20 5 9 2Hypertension 20 5 9 2
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.Zejula [prescribing information]. Tesaro. 2018.
26
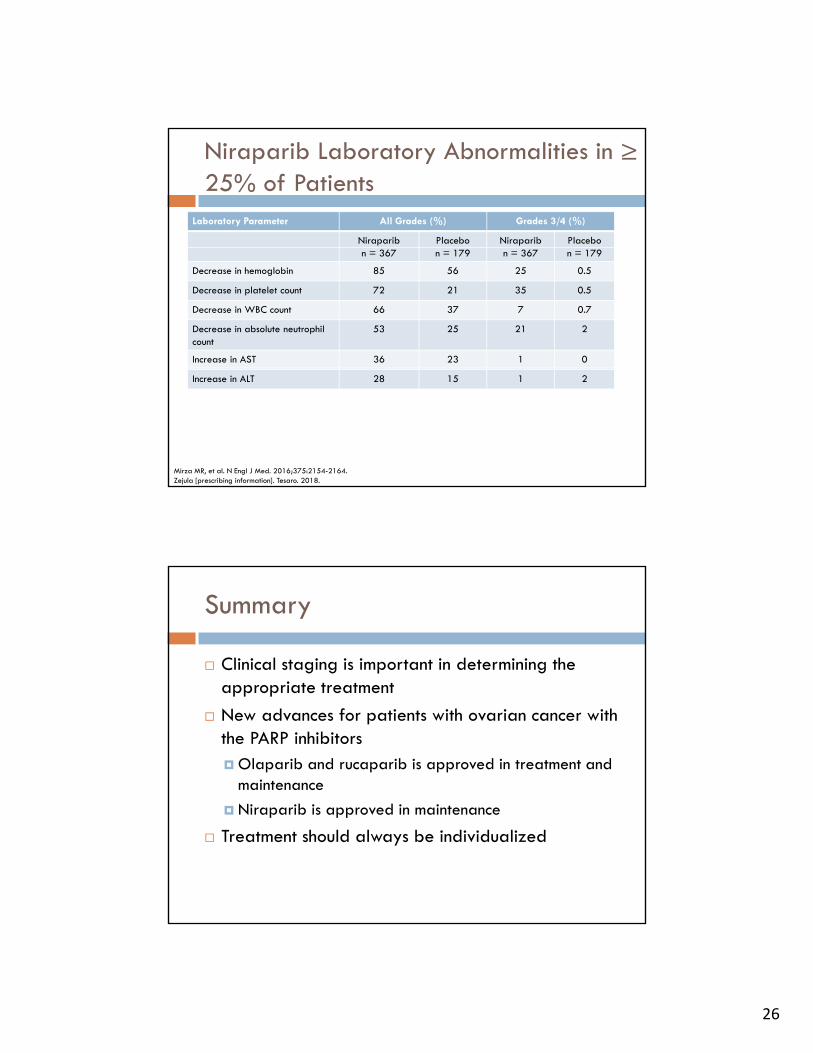
Niraparib Laboratory Abnormalities in ≥ 25% of Patients
Laboratory Parameter All Grades (%) Grades 3/4 (%)
Niraparib Placebo Niraparib Placebon = 367 n = 179 n = 367 n = 179
Decrease in hemoglobin 85 56 25 0.5
Decrease in platelet count 72 21 35 0.5
Decrease in WBC count 66 37 7 0.7
Decrease in absolute neutrophil count
53 25 21 2
Increase in AST 36 23 1 0
Increase in ALT 28 15 1 2
Mirza MR, et al. N Engl J Med. 2016;375:2154-2164.Zejula [prescribing information]. Tesaro. 2018.
Summary
Clinical staging is important in determining the appropriate treatmentappropriate treatment
New advances for patients with ovarian cancer with the PARP inhibitors Olaparib and rucaparib is approved in treatment and
maintenance
Ni ib i d i i Niraparib is approved in maintenance
Treatment should always be individualized
27
Ovarian Cancer: Implications for the Pharmacist
Megan May, Pharm.D., BCOP





























