Embed Size (px)
Citation preview
Megaloblastic Anemia
קורס להמטולוגיה
' שנה ד–מבוא לרפואה פנימית
ו"תשס
גולדפרבר עדה "ד
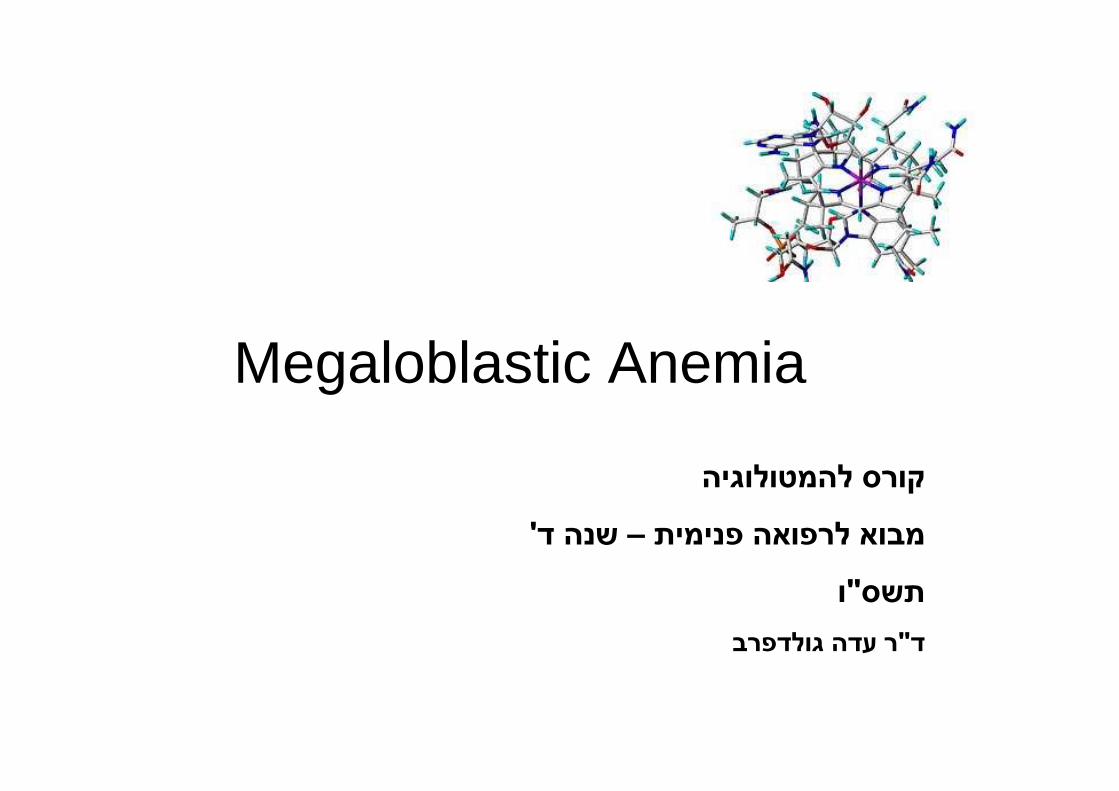
Diagnostic approach based on RBC’sindices
MCV < 80 fl 80 fl < MCV < 98 fl MCV > 98 fl
Microcyticanemia
Normocyticanemia
Macrocyticanemia
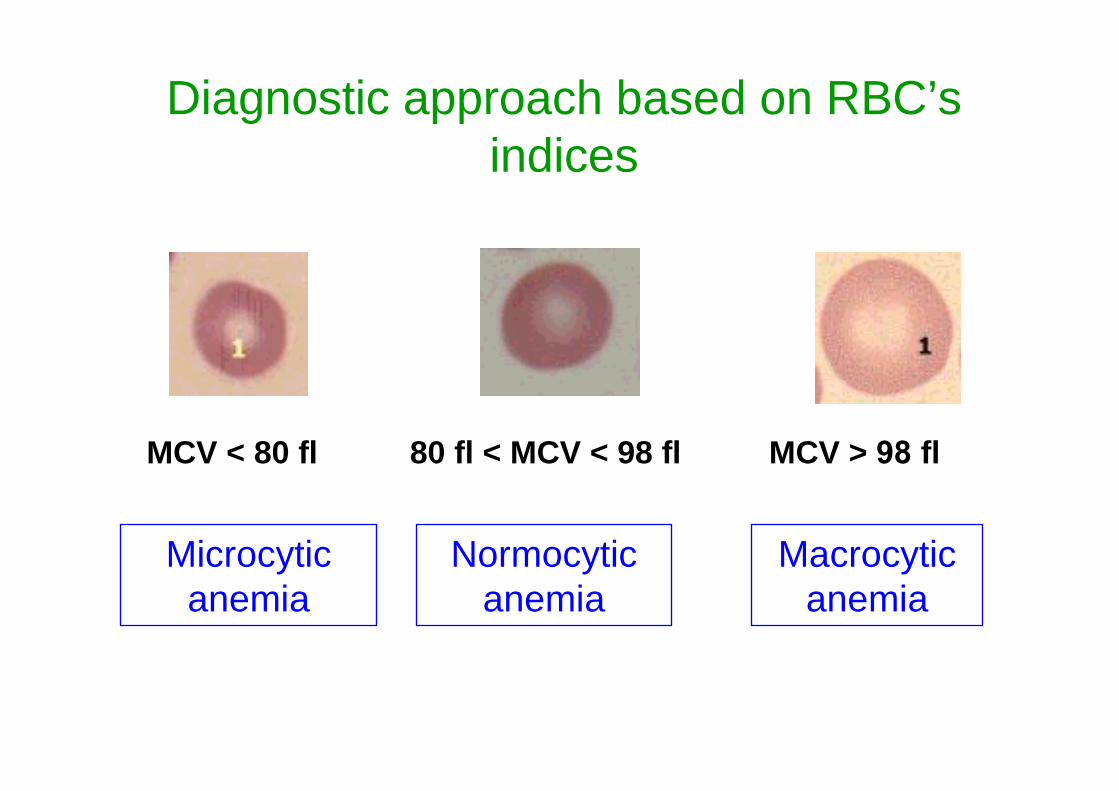
Macrocytic Anemia (MCV>100)
MorphologyPeripheral blood & Bone Marrow
Megaloblastic
Vit B12, Folatedeficiency
Non-Megaloblastic
Reticulocyte count
Increased
Hemorrhage
Hemolysis
Cold agglutinins
Decreased/Normal
Alcoholism
Liver Disease
Hypothyroidism
BM failure:
MDS, Aplastic Anemia
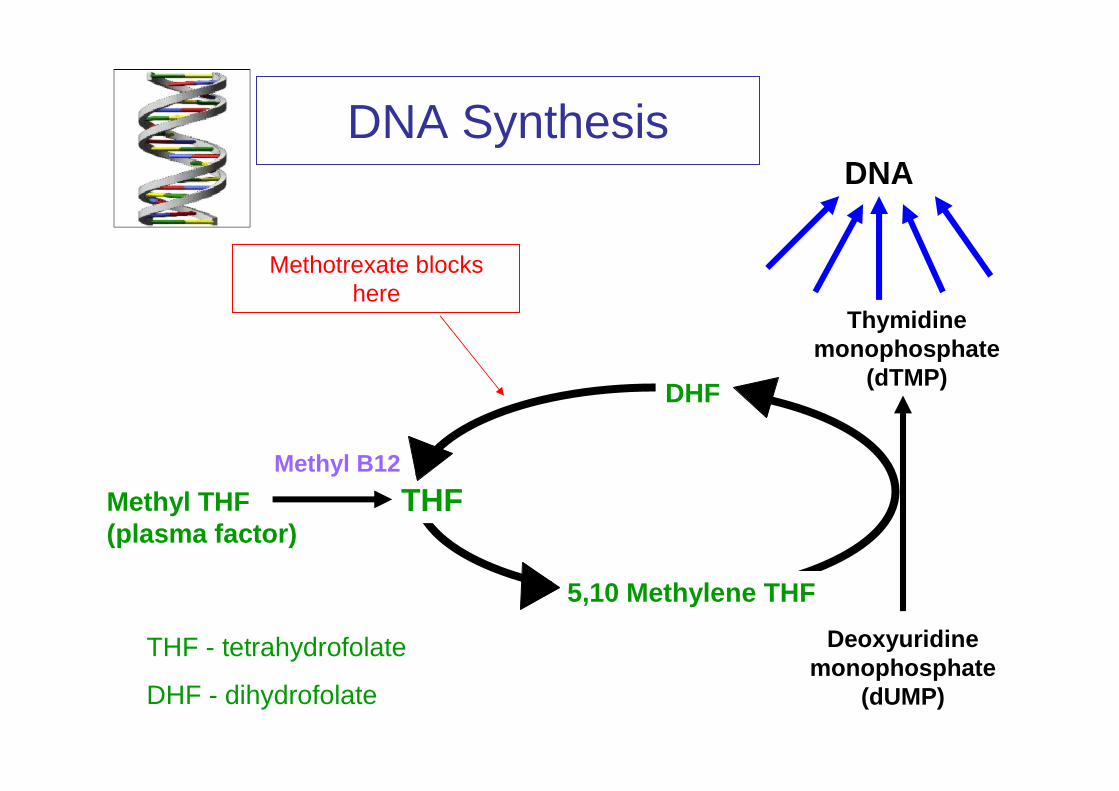
DNA SynthesisDNA
THF
5,10 Methylene THF
DHF
Deoxyuridinemonophosphate
(dUMP)
Thymidinemonophosphate
(dTMP)
Methyl B12
Methyl THF (plasma factor)
THF - tetrahydrofolate
DHF - dihydrofolate
Methotrexate blocks here
B12/Folate deficiency affects all dividing cells
1. Ineffective HematopoiesisIneffective Erythropoiesis Anemia
Ineffective Leukopoiesis Leukopenia
Ineffective Thrombopoiesis Thrombocytopenia
2. RBC survival ↓↓↓↓
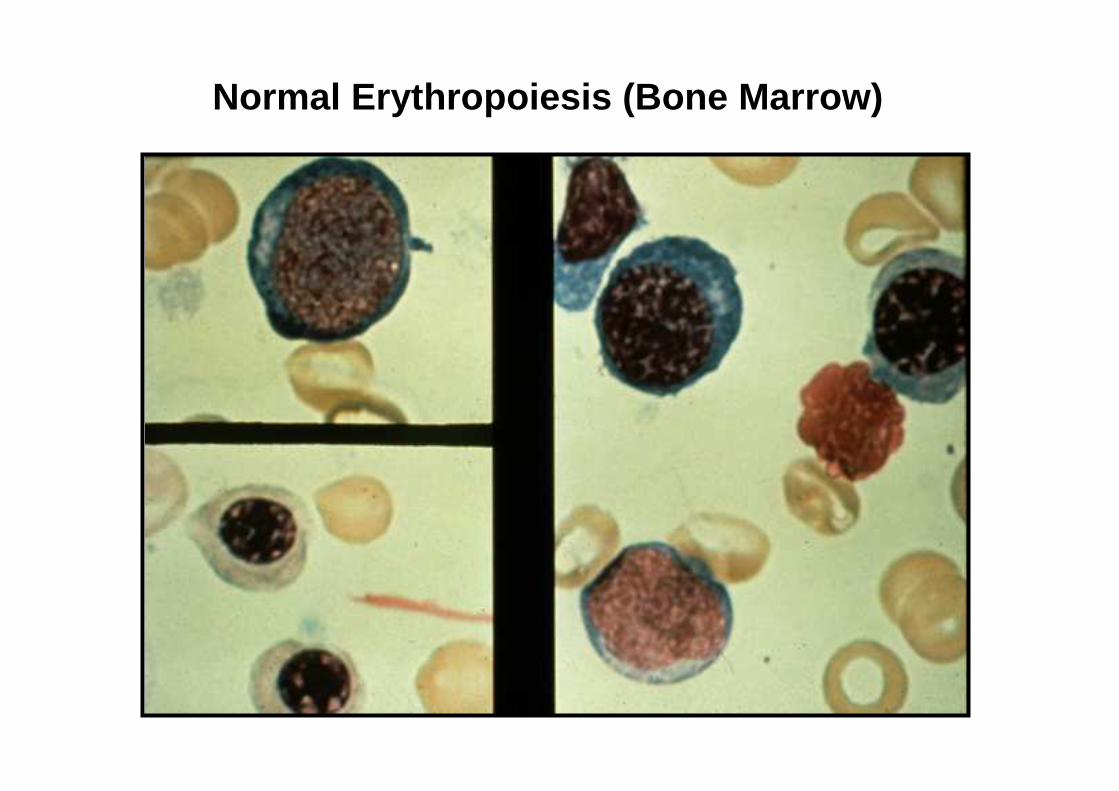
Normal Erythropoiesis (Bone Marrow)
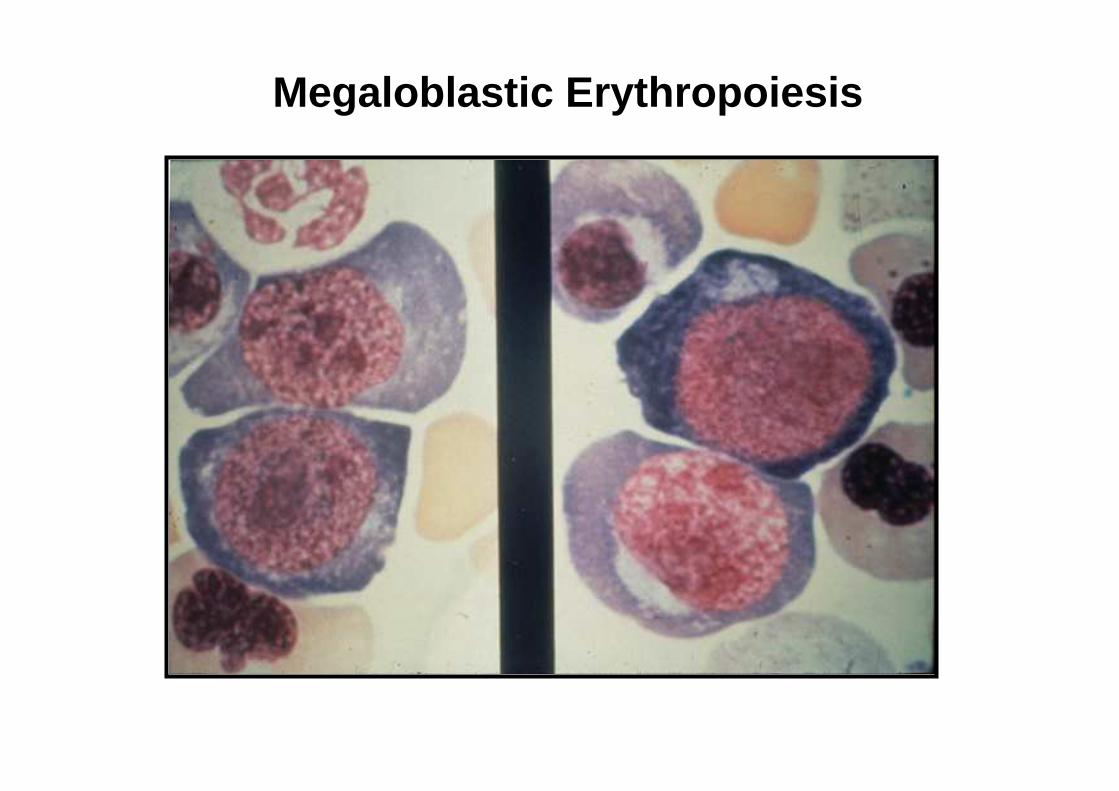
Megaloblastic Erythropoiesis
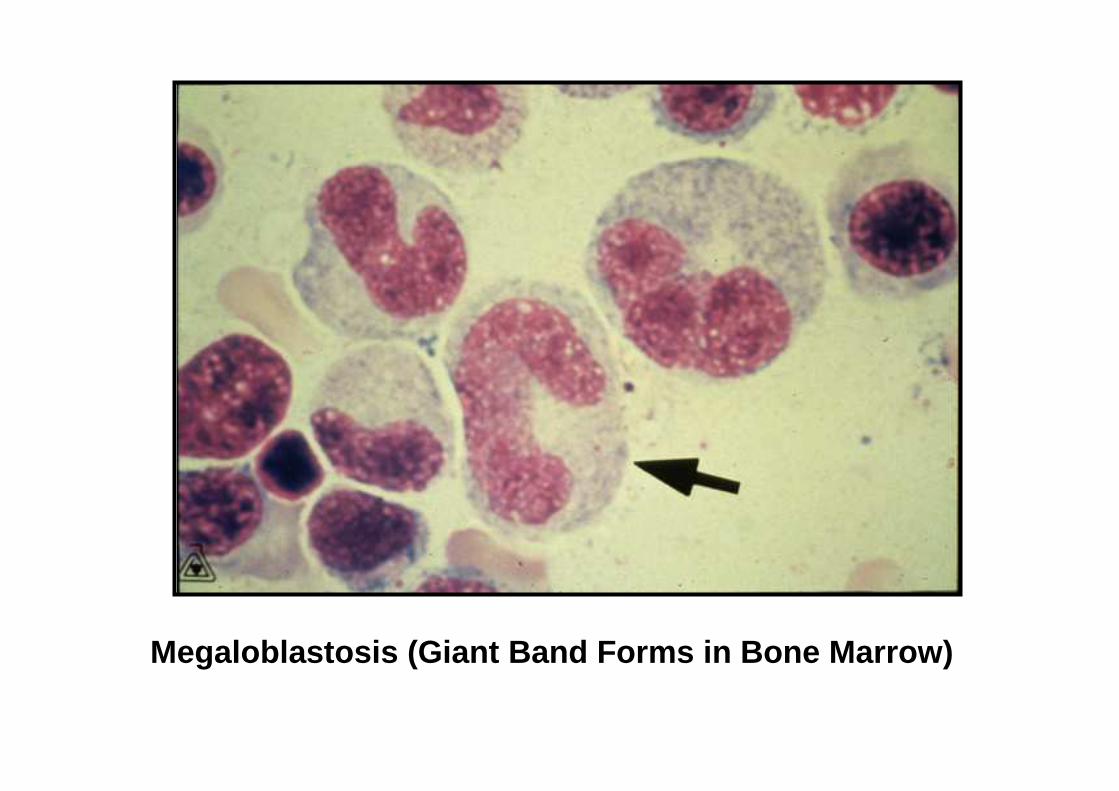
Megaloblastosis (Giant Band Forms in Bone Marrow)
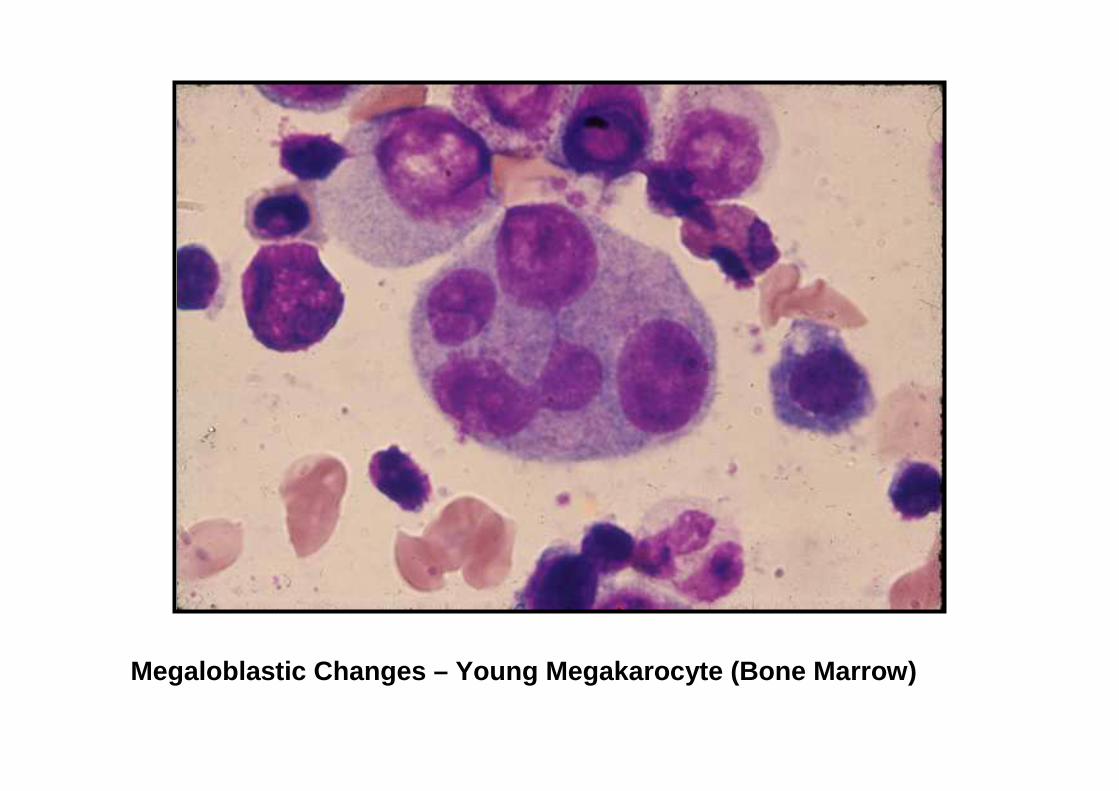
Megaloblastic Changes – Young Megakarocyte (Bone Marrow)
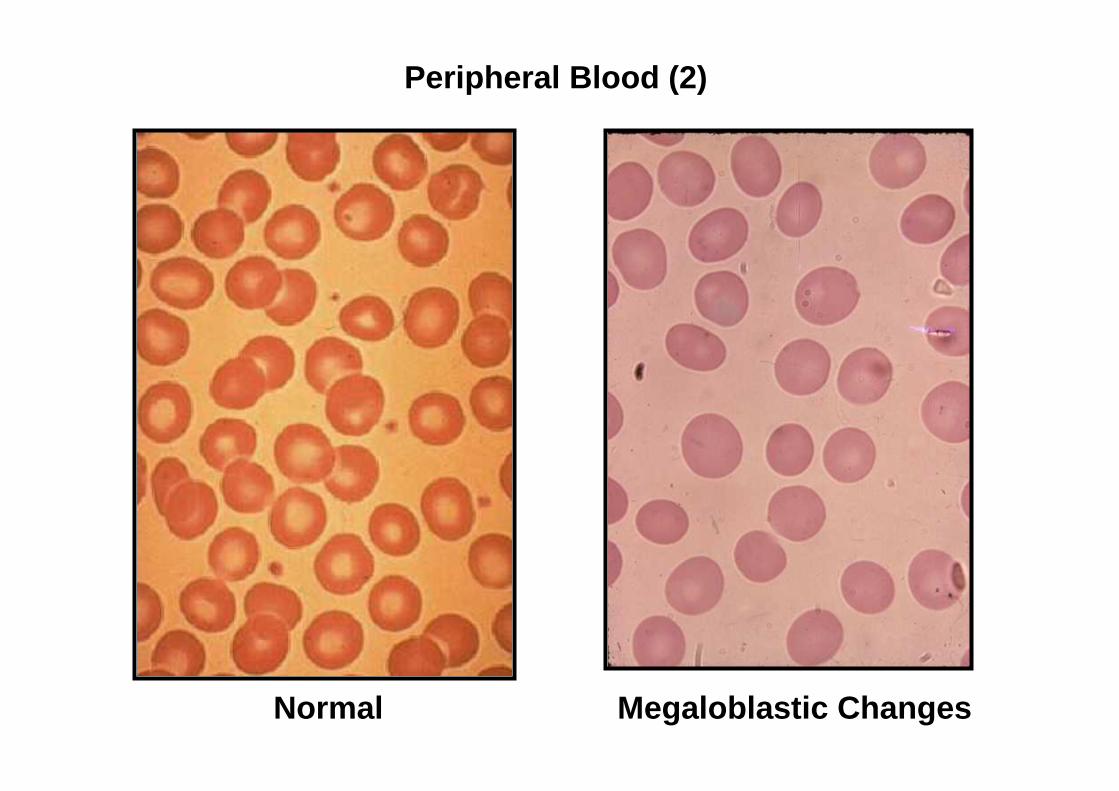
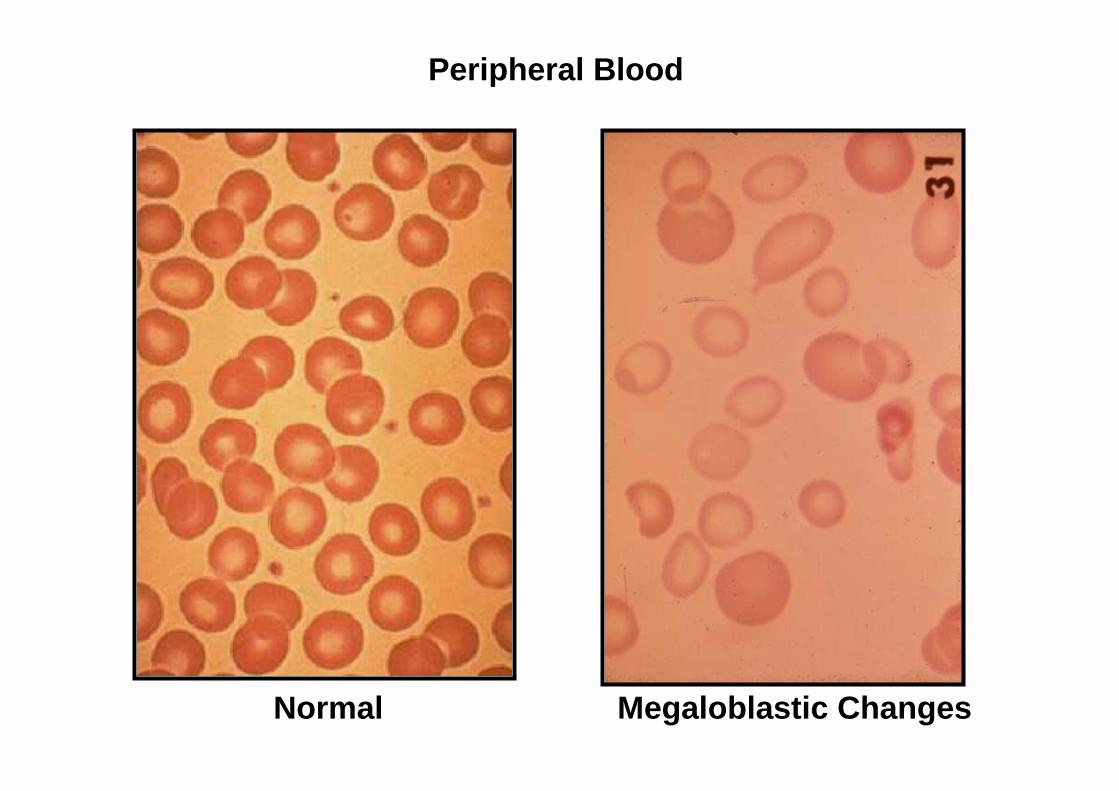
Normal Megaloblastic Changes
Peripheral Blood (2)
Normal Megaloblastic Changes
Peripheral Blood
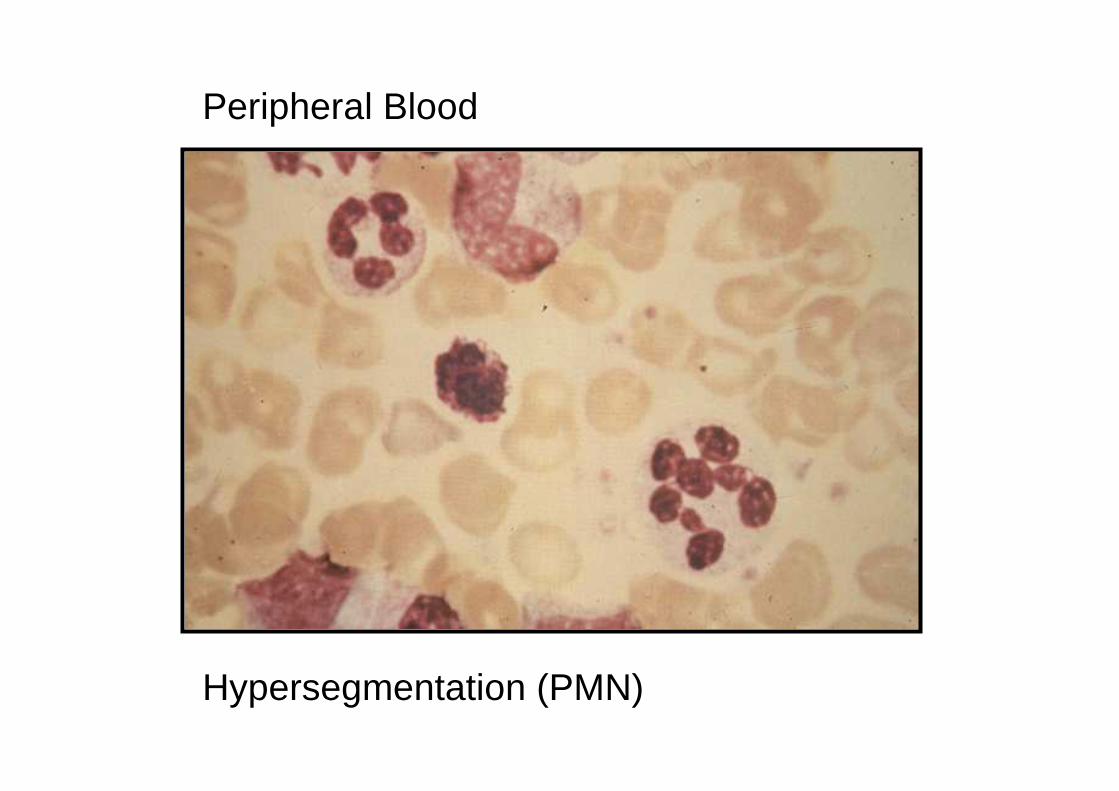
Peripheral Blood
Hypersegmentation (PMN)
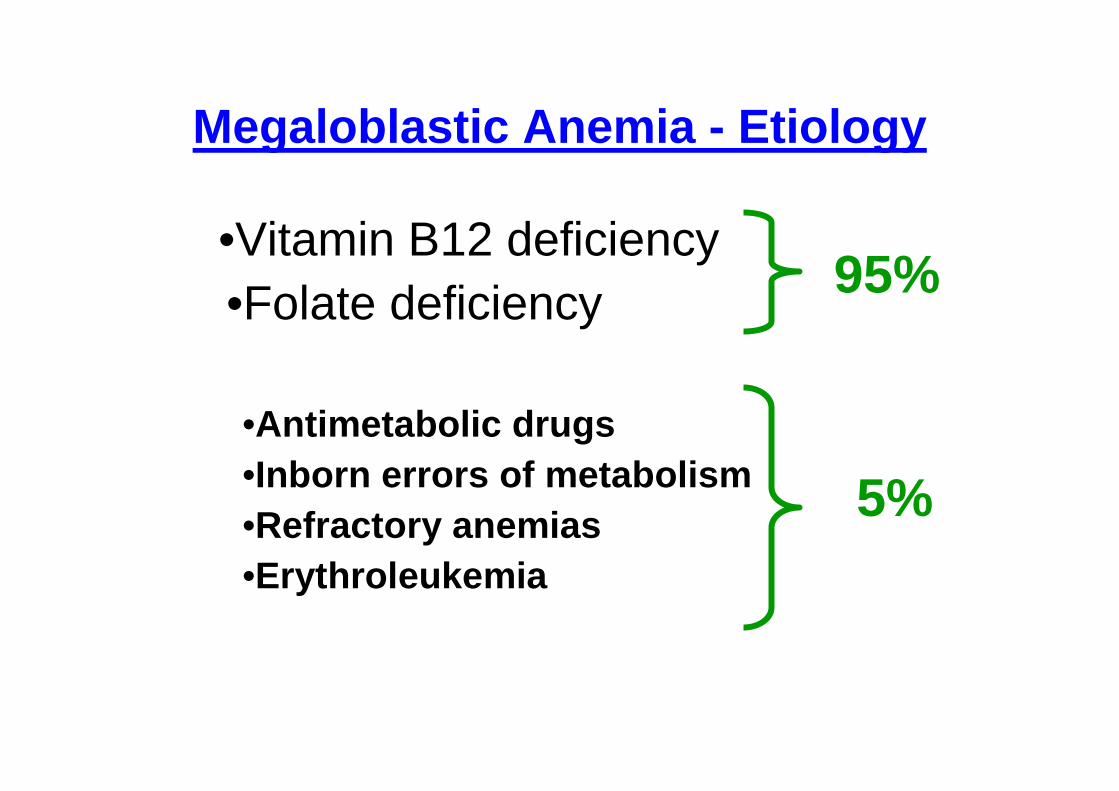
Megaloblastic Anemia - Etiology
•Vitamin B12 deficiency •Folate deficiency
•Antimetabolic drugs•Inborn errors of metabolism•Refractory anemias•Erythroleukemia
95%
5%
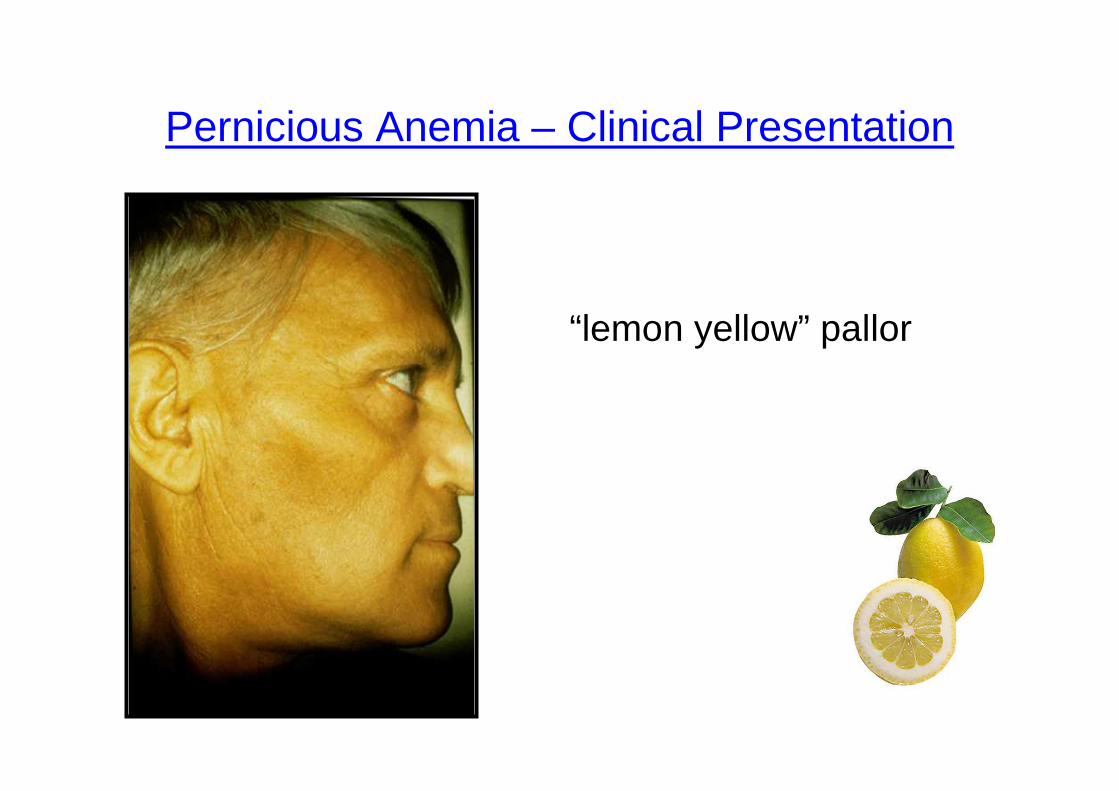
Pernicious Anemia – Clinical Presentation
“lemon yellow” pallor
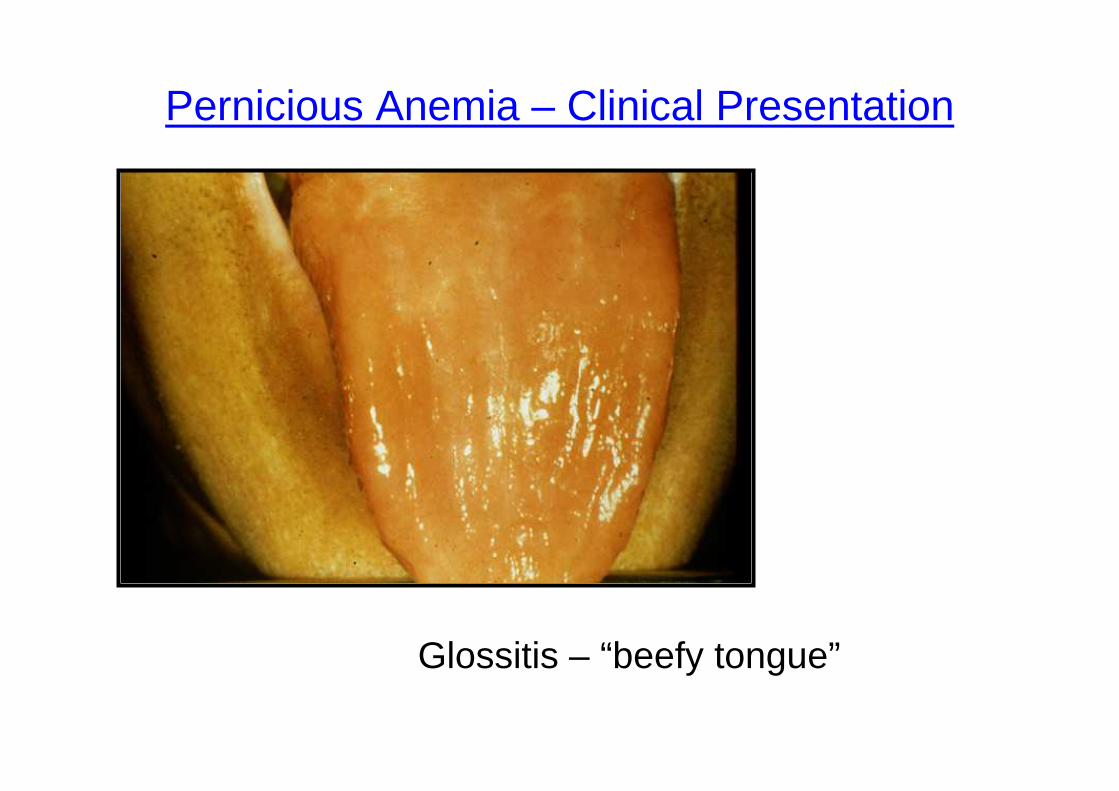
Pernicious Anemia – Clinical Presentation
Glossitis – “beefy tongue”
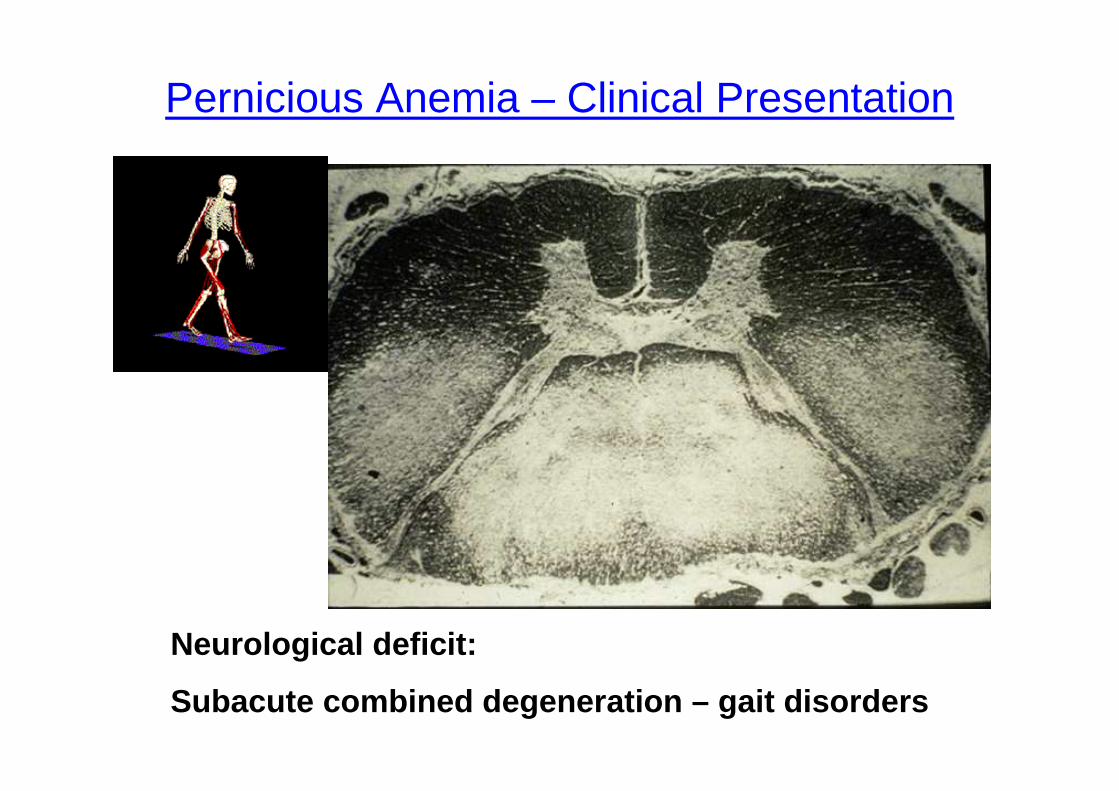
Pernicious Anemia – Clinical Presentation
Neurological deficit:
Subacute combined degeneration – gait disorders
Pernicious Anemia – Clinical Presentation
Neurological deficit:
Depression, dementia, behavioral changes (“megaloblastic madness”)
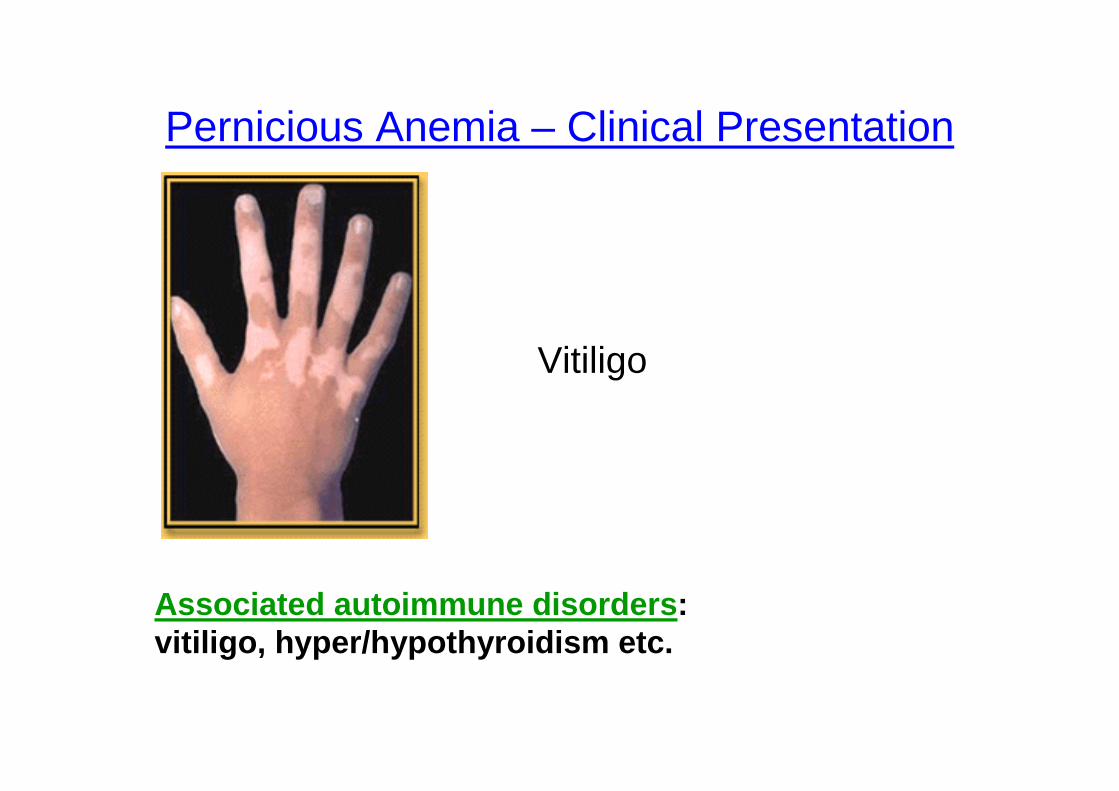
Pernicious Anemia – Clinical Presentation
Vitiligo
Associated autoimmune disorders : vitiligo, hyper/hypothyroidism etc.
Megaloblastic Anemias: Signs & Symptoms (1)
Subjective:
• Fatigue, weight loss,gastrointestinal
complaints, sore tongue or mouth
• Neurological complaints (may be
irreversible !) : Paresthesias, difficulty
walking(?)
Megaloblastic Anemias: Signs & Symptoms (2)
Objective:
• Pallor & jaundice (“lemon yellow”)• Loss of papillae of tongue (“beefy red”)
• Neurological deficit (Only with B12 def)
• (↓ position / ↓ vibration sense + romberg / spastic paraparesis)
• Can also cause dementia & depression• Signs of associated conditions: vitiligo, thyroid
disease etc.
Megaloblastic Anemia – Lab Results
CBC:
• ↓ Hb/Hct, ↑ MCV, ↓ retics, ↑ RDW, ↓ WBC, ↓Plts• CAUTION: mixed deficiency or concurrent states (iron
deficiency or thal+ megaloblastic anemia) MASKED SIGNS!
Biochemistry : • ↑ Bilirubin, ↑ ↑ LDH, ↓ Vit B12
Autoantibodies : • anti-parietal cell, anti-thyroid etc.• Other associated: glucose, thyroid function etc.
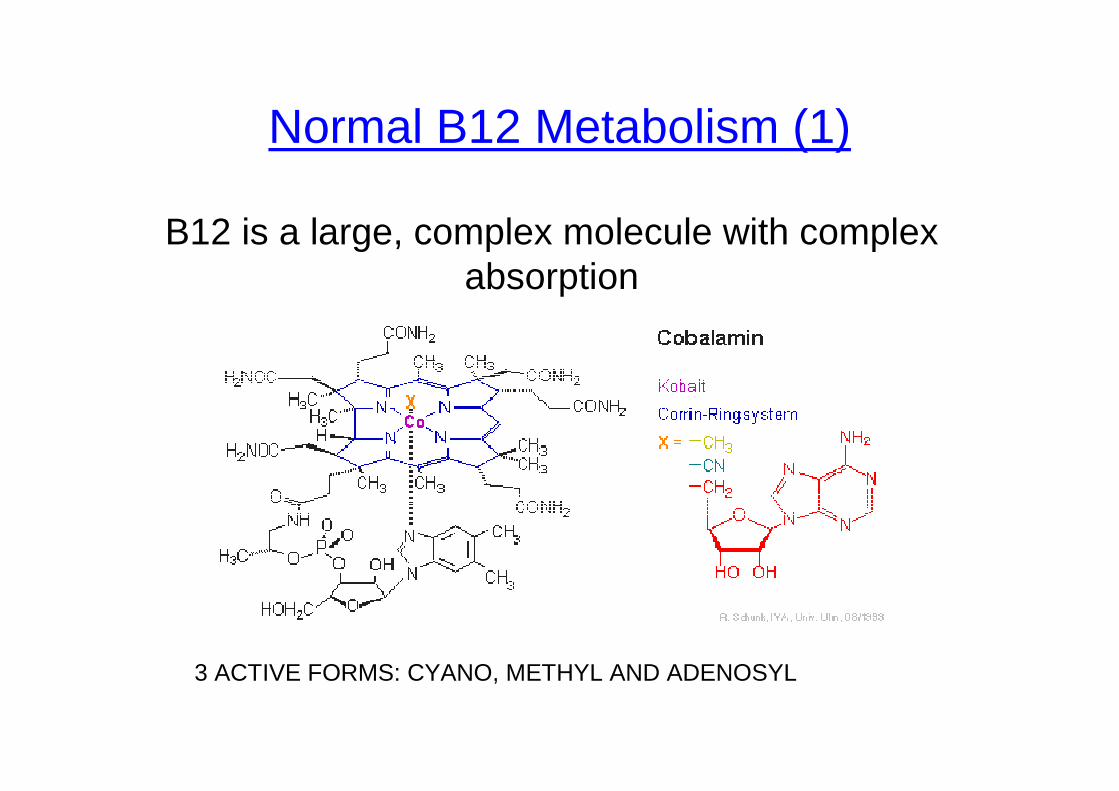
B12 is a large, complex molecule with complex absorption
3 ACTIVE FORMS: CYANO, METHYL AND ADENOSYL
Normal B12 Metabolism (1)
Normal B12 Metabolism (2)
• B12 is present in foods of animal origin
• Not in vegetables or plants!!!
• Minimum daily requirement is only 2µg/day• Body stores total: 3-4000 µg (mainly
hepatic)
• Dietary deficiency: rare, in long term strict vegans
Normal B12 Metabolism (3)
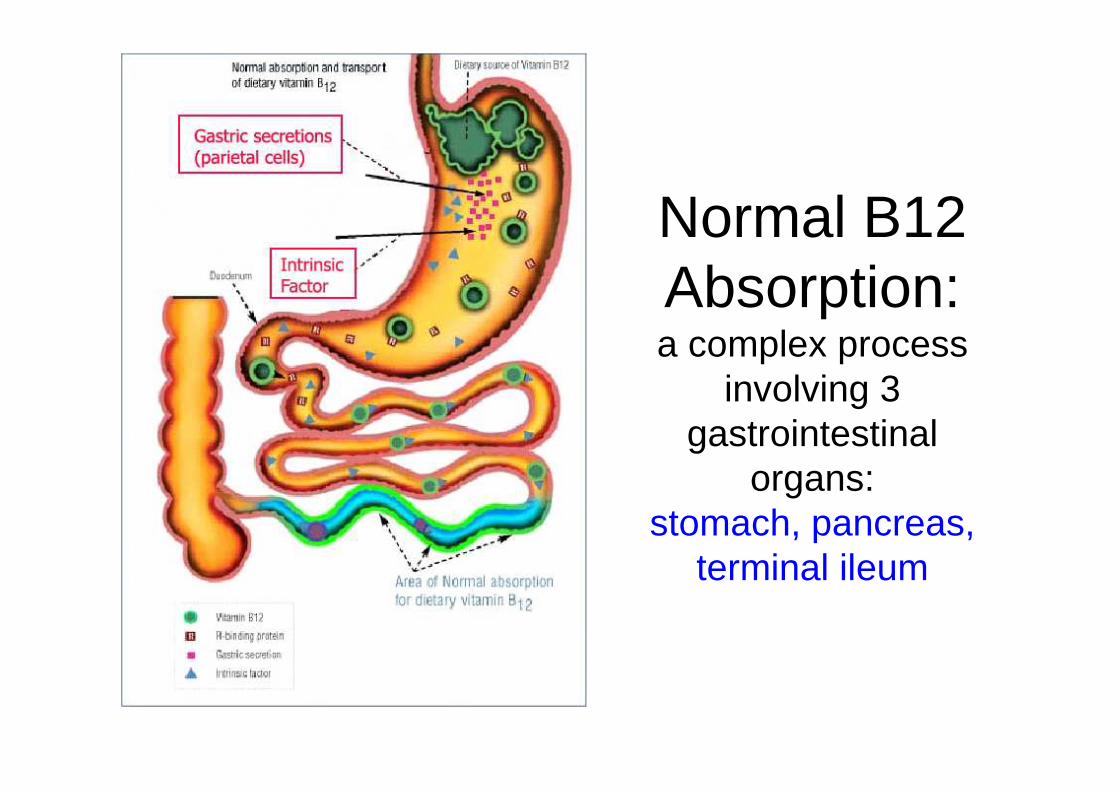
Normal B12 Absorption: a complex process
involving 3 gastrointestinal
organs: stomach, pancreas,
terminal ileum
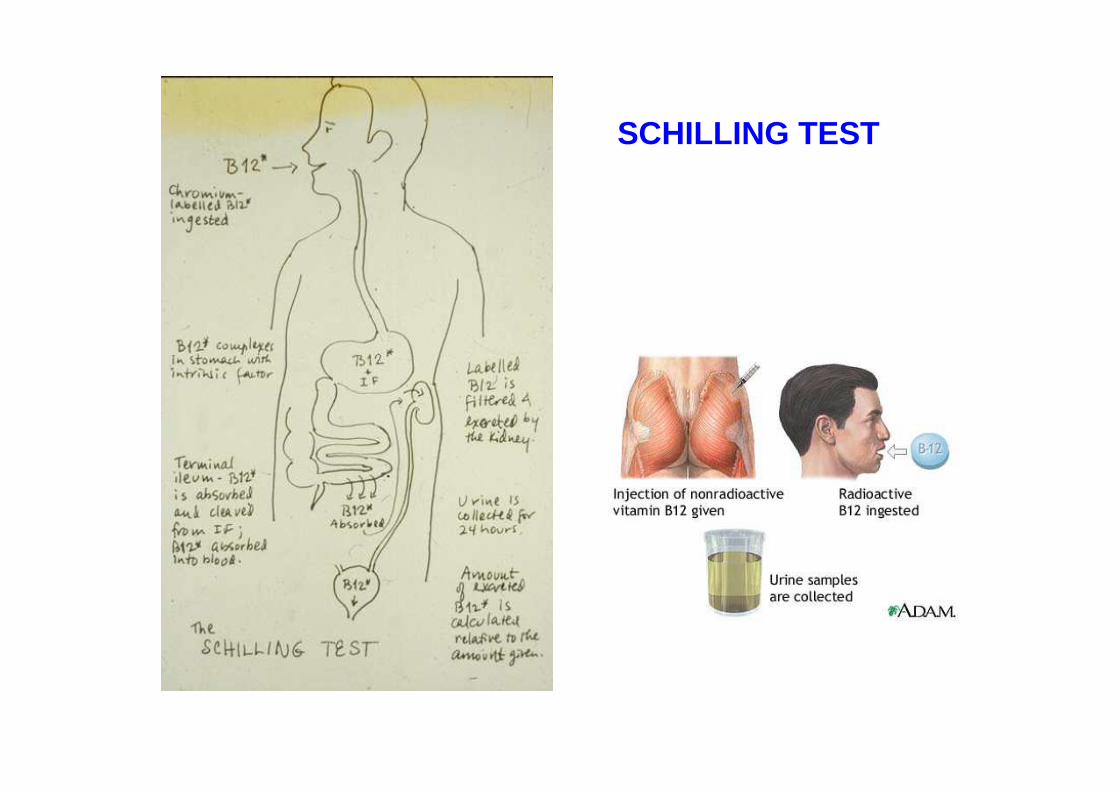
SCHILLING TEST
Common Etiologies of B12 def.
• Lack of intrinsic factor– Pernicious anemia– Post-gastrectomy (partial / total / bypass)– Congenital
• Biological competitiona. Small-bowel bacterial overgrowth
– Jejunal diverticuli– Blind loops– Scleroderma, diabetesb. Fish tapewarm
stasis
Common Etiologies of B12 def.(cont)
• Diseases of the ileumA. Surgical resectionsB. Crohn’s disease
These are differentiated using the Schilling test !!!
B12 def - Treatment
• Oral therapy – only if definitive dietary deficiency (rare)
• Parenteral – injection of B12, 10 injections as a loading dose and then once a month for life
• New!!! Sublingual/
Nasal Vit B12 therapy
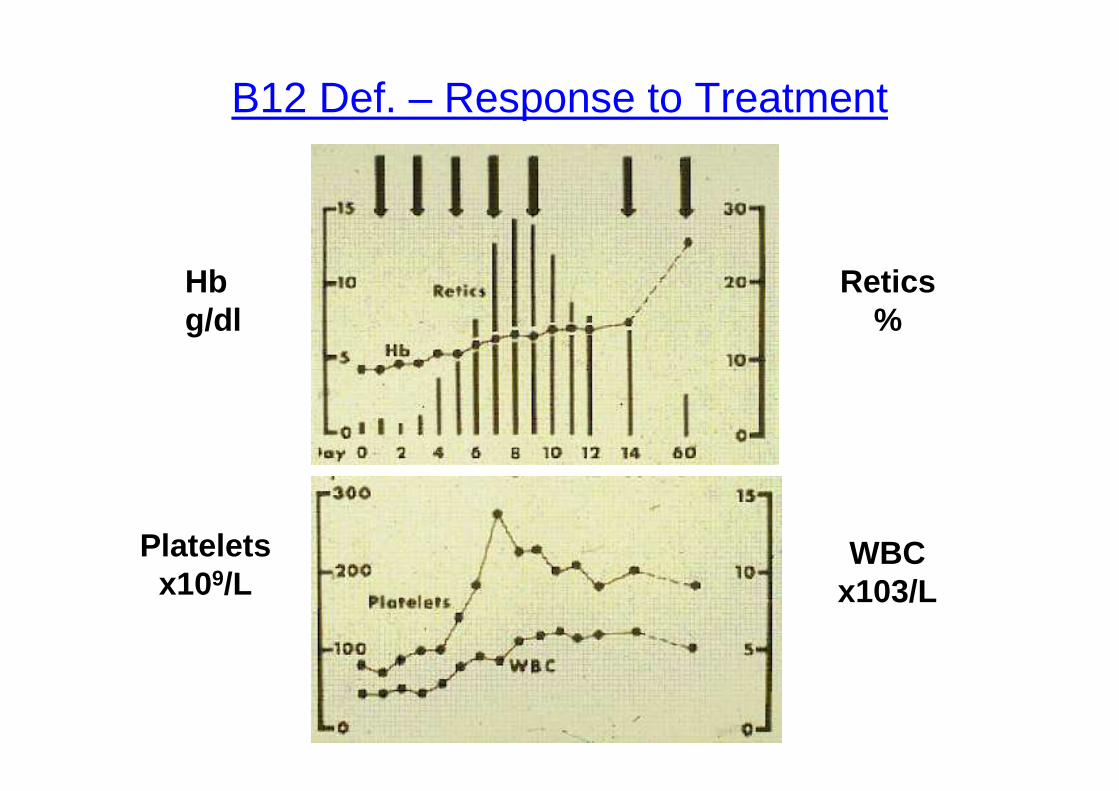
Retics%
Hbg/dl
Platelets x109/L
WBC x103/L
B12 Def. – Response to Treatment
Low B12 level is common
• Since the introduction of commercial kits, the finding of a low B12 level is an all-too common finding in the workup of patients with anemia or other syndromes.
• Even can be found in patients with LOW MCV
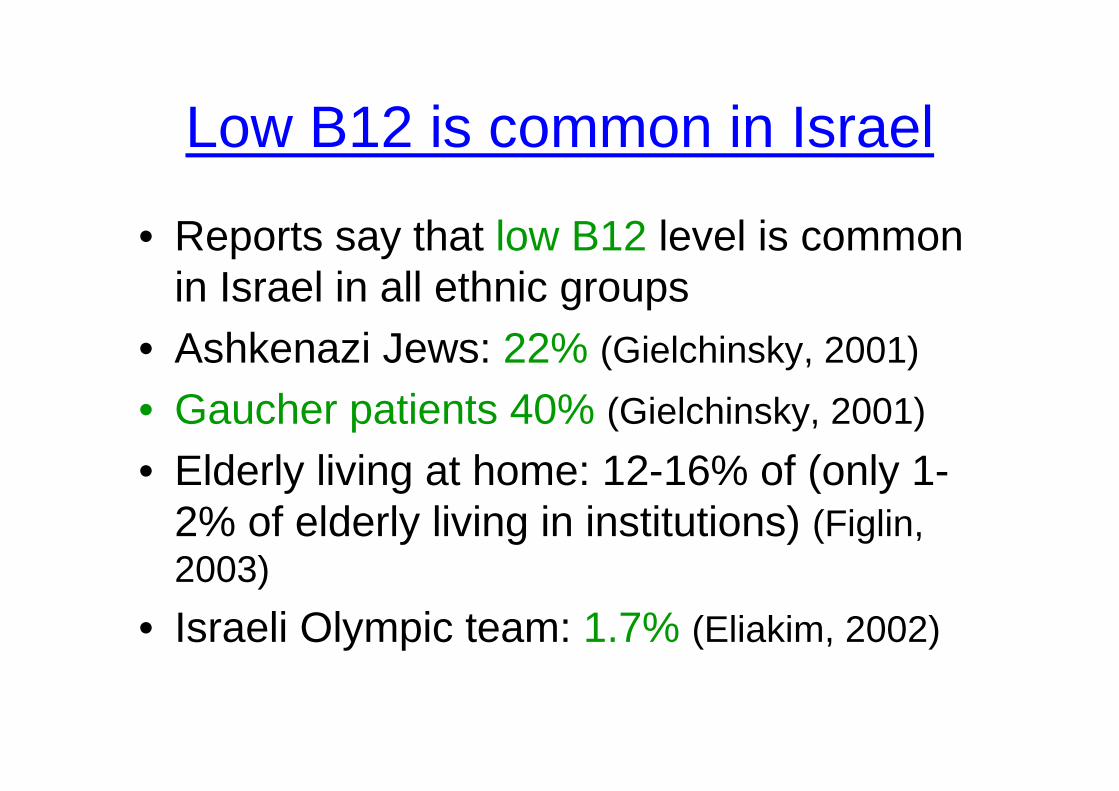
Low B12 is common in Israel
• Reports say that low B12 level is common in Israel in all ethnic groups
• Ashkenazi Jews: 22% (Gielchinsky, 2001)
• Gaucher patients 40% (Gielchinsky, 2001)
• Elderly living at home: 12-16% of (only 1-2% of elderly living in institutions) (Figlin, 2003)
• Israeli Olympic team: 1.7% (Eliakim, 2002)
Confirmation that low B12 level represents true deficiency
HOW TO CONFIRM?
Metabolic tests:
• Methylmalonic acid (MMA) level
• Homocysteine (HC) level
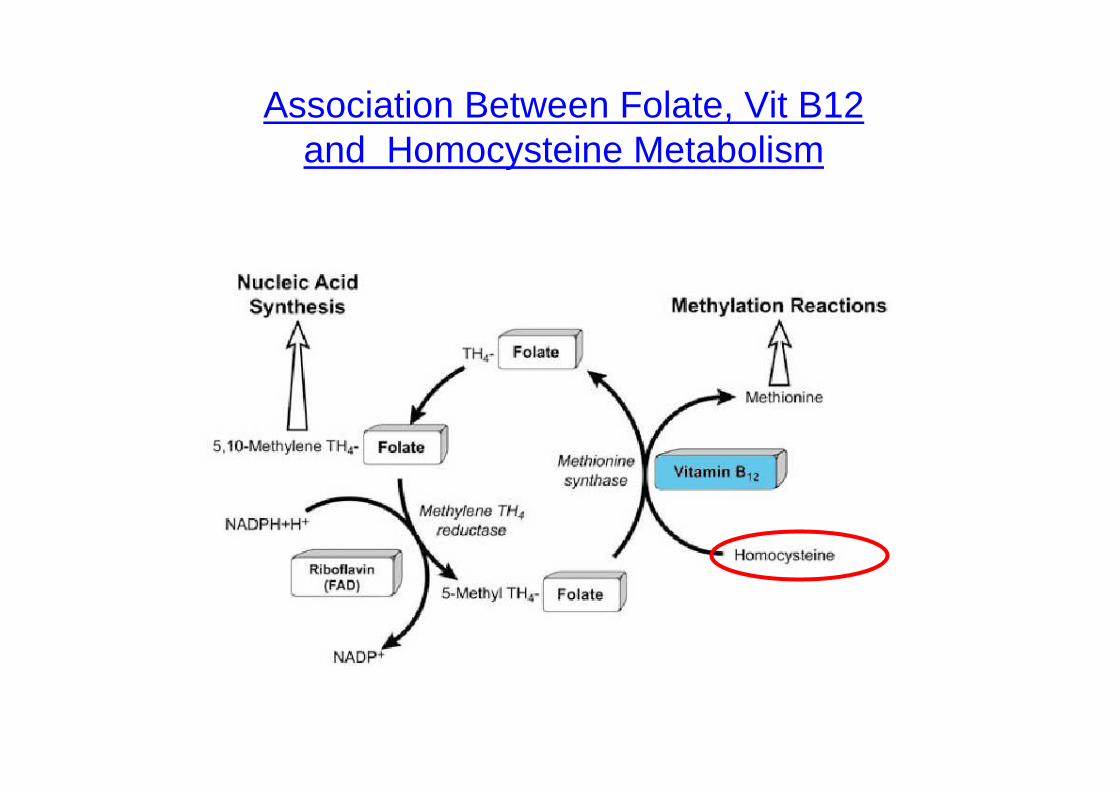
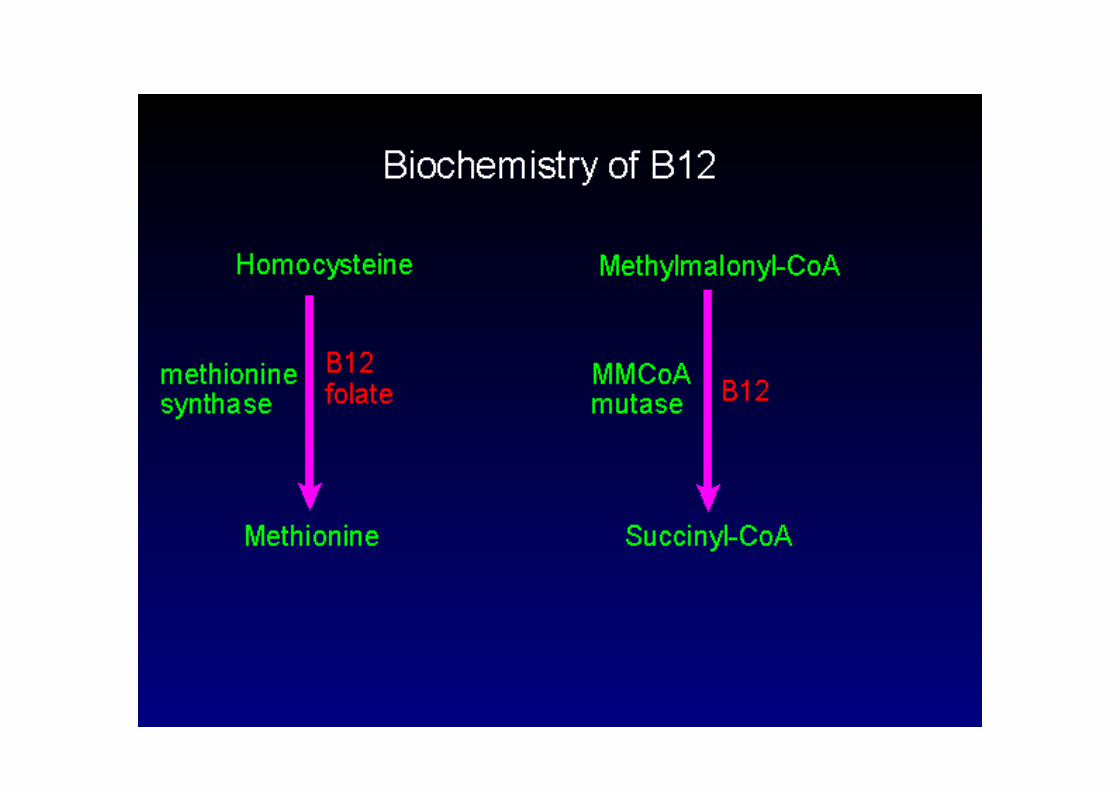
Biochemistry of B12Association Between Folate, Vit B12 and Homocysteine Metabolism
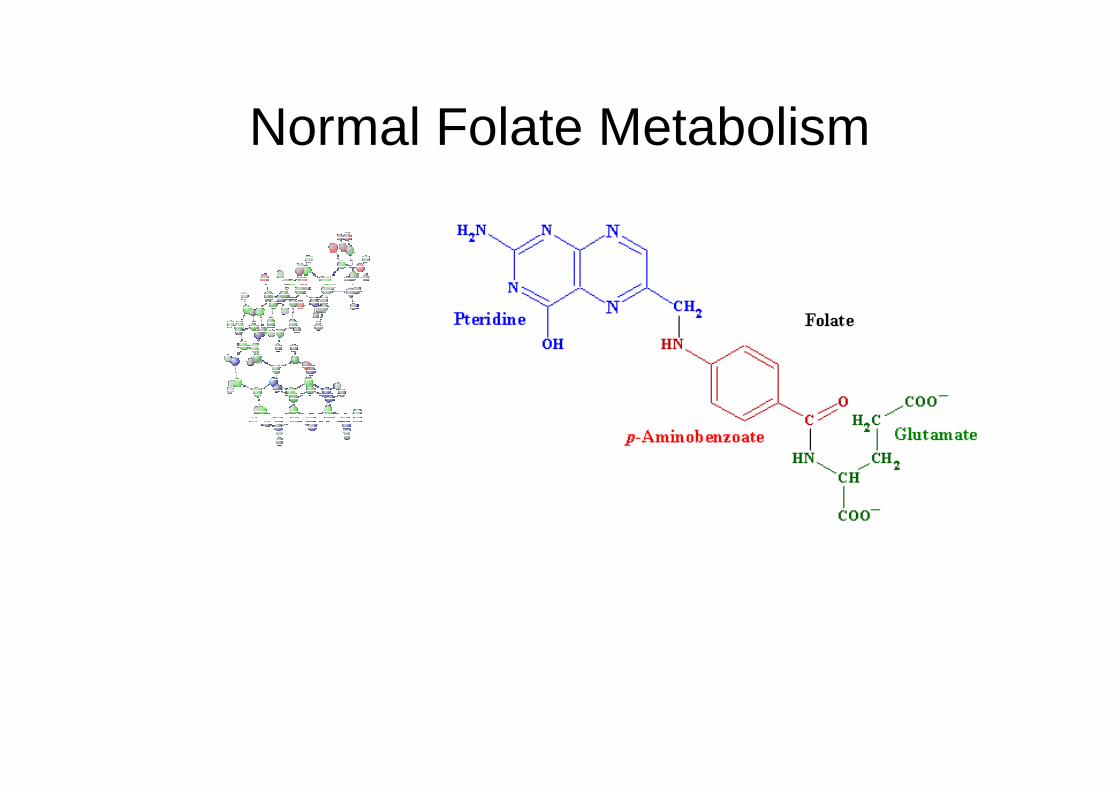
Normal Folate Metabolism
Normal Folate Metabolism (2)
• Folate is present in fruits, vegetables, human milk
• Daily requirement: 50µg/day• Well absorbed throughout the
jejunum,ileum• Total body stores: 5 mg, only for several
months
Etiologies of Folate Deficiency
• Increased requirements (pregnancy, breastfeeding, hemolysis, exfoliativedermatitis)
• Poor diet (longstanding)• Alcoholism, Parenteral feeding etc.• Poor absorption (diffuse intestinal
diseases)
Folate Deficiency - Treatment
• Oral folate (pills) for duration of state leading to deficiency
• Folate supplementation during pregnancy reduces significantly the risk for neural tube defects
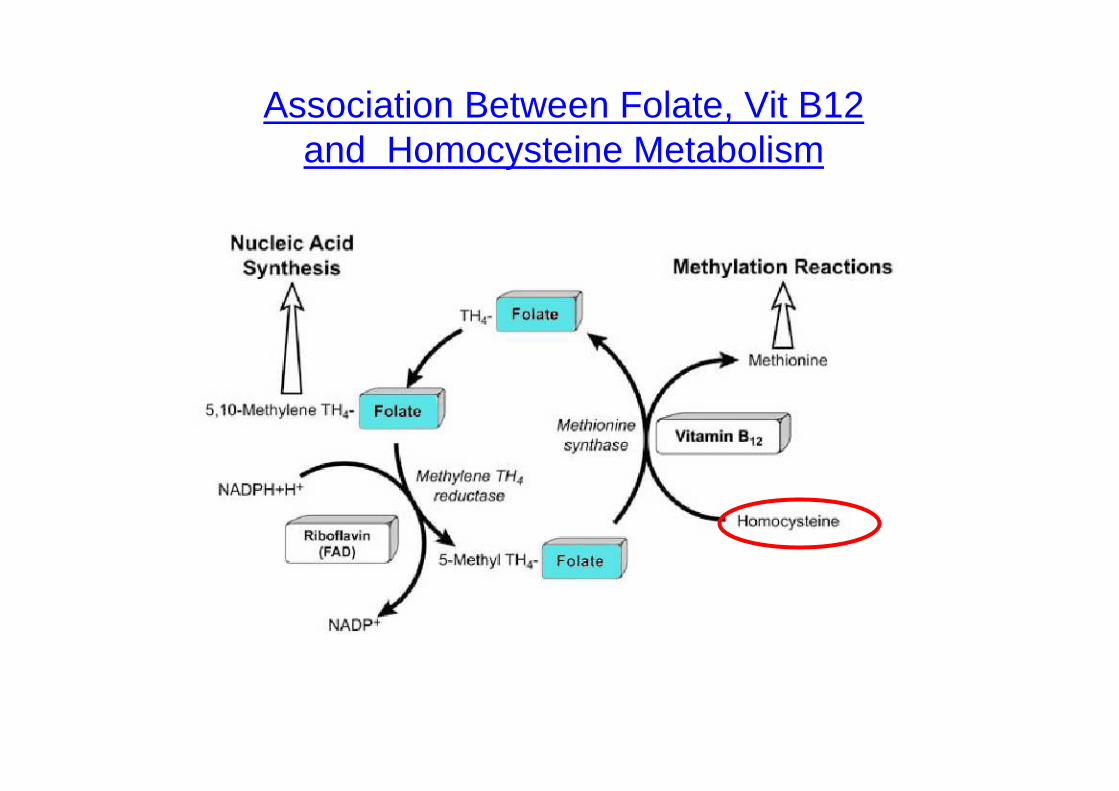
Association Between Folate, Vit B12 and Homocysteine Metabolism