Embed Size (px)
Citation preview

Meeting Update Jennifer Kiser, PharmD University of Colorado
14th International Workshop on Clinical Pharmacology of HIV Therapy April 24, 2013

Impressive Pipeline
Protease Inhibitors: Boceprevir Telaprevir Faldaprevir (BI 201335) Simeprevir (TMC435) ABT-450 ACH-1625 BMS-650032 (asunaprevir) GS-9451 GS-9256 MK-5172 RG7227 (danoprevir) ACH-2684
Kiser JJ, Flexner C. Annual Reviews in Pharmacology and Toxicology [In press]
NS5A Inhibitors: BMS-790052 (daclatasvir) ABT-267 GS-5885 GSK2336805 ACH-2928 IDX719 PPI-461 PPI-668
Nucleos(t)ide Inhibitors: Sofosbuvir (GS-7977) RG7128 (mericitabine) ALS-2158 ALS-2200 Non-Nucleoside Inhibitors: RG7790 (setrobuvir) BI 207127 Filibuvir GS 9190 (tegobuvir) VX-222 ABT-333 BMS-791325 GS-9669
BUT…. Persons with advanced liver disease are under-represented in clinical trials

Ongoing INF-free Trials Allowing or Exclusively Studying Persons with Advanced Liver Disease
DAA Combination Patient Population N NCT# Status
Daclatasvir + simeprevir ± RBV
Allows 1/3 F3 or F4 without decompensation
180 01628692 Ongoing, not recruiting
Sofosbuvir + simeprevir ± RBV
Allows half with F3 or F4 no decompensation
168 01466790 Ongoing, not recruiting
Sofosbuvir + RBV Pre-transplant CP ≤ 7 50 10559844 Enrollment complete
ABT450/r + ABT333 + ABT267 + RBV (TURQUOISE-II)
All cirrhotics CP ≤ 6 300 01704755 Recruiting
Sofosbuvir + RBV All cirrhotics including decompensation CP < 10, HVPG > 6
50 01687257 Recruiting
Sofosbuvir + RBV Post-transplant recurrence, 6 mo-12 yr post-transplant, excludes decompensation
40 01687270 Recruiting
www.clinicaltrials.gov

Major Themes Pre-Transplant
• P/R insufficient – 13-22% SVR • Lots of serious adverse events
with P/R + BOC or TVR – Anemia, infections, death
• Discussion about who the candidates are and how to manage them before and during treatment – Too risky, wait for new agents? – Complete an entire course of
treatment vs. treat for a certain period of time then transplant
• Interferon-free DAA combinations are needed
Post-Transplant • P/R insufficient – 1/3 SVR • Discussion about who the
candidates are and how to manage them before and during treatment
• Awaiting P/R + BOC or TVR SVR rates – forecast 50% SVR – EASL – Management of DDI with
immunosuppressants a challenge
• DAA combinations without interaction potential are needed

Pharmacology Topics
• Pre-Transplant – Effects of advanced liver disease on DAA
pharmacokinetics • Evaluate results of some hepatic impairment studies with
DAA in the context of these pathophysiologic features • Post-Transplant
– Managing immunosuppressant doses and dosing frequency with BOC and TVR
• Coilly A, EASL Late Breaker • Same considerations we tackled with HIV protease inhibitors

Features of Advanced Liver Disease which may Alter DAA PK
1. Hepatic enzyme expression and/or function 2. Membrane transporter expression and/or
function 3. Protein Binding 4. Portal-Systemic Shunting 5. Phosphorylation enzyme expression and/or
function 6. Renal Impairment 7. Reduced gastointestinal absorption

CYP Enzyme Expression and Function with Progressive Hepatic Impairment
Modified from figure by Branch RA, CPT 1998;64:462
CYP3A

ABT450/r Concentrations Increased with Moderate and Severe Hepatic Impairment
ABT450 is a CYP3A substrate reduced CYP3A expression may contribute to increased concentrations of ABT450
Khatri A, et al. AASLD 2012

Bile
NTCP
OATP1B1 OATP1B3* OATP2B1
Systemic Circulation Systemic Circulation
2. Transporter Expression in Liver Disease
OCT1 P-gp
MRP2 MRP3
MRP4
BCRP ABCG5/G8
BSEP
MDR3
Figure adapted from Oswald S. et al. Xenobiotica 2007;37(10-11):1171, 1Nakai K, et al. Drug Metab & Dispos 2008;36(9):1786,2Ogasawara K, et al. Drug Metabol PK 2010;25(2):190, 3Bonin S, et al. Mol Med 2002;8(6):318.
Sinusoidal Membrane Canalicular Membrane
?

Asunaprevir Increased with Moderate and Severe Hepatic Impairment
• Metabolized by CYP3A, substrate for OATP1B1 and OATP2B1
• AUC ↑ 9.8-fold and 32-fold in moderate and severe impairment
Eley T et al. AASLD 2012, #1873

3. Protein Binding
• Impaired production of plasma proteins results in decreased plasma binding of several drugs. – May also be a contribution of competition for binding
sites with endogenous substances and perhaps a reduction in the quality of protein
• For highly protein bound drugs (>90%), even
small changes in binding can have large effects on drug PK.
Verbeeck RK. Eur J Clin Pharmcol 2008;64:1147-1161
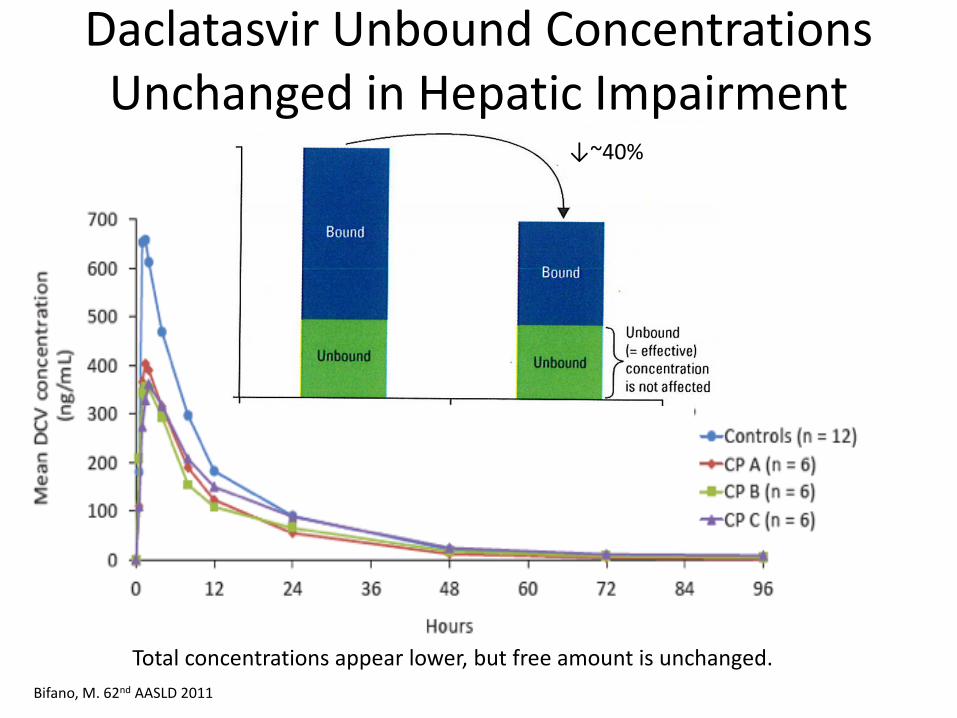
Daclatasvir Unbound Concentrations Unchanged in Hepatic Impairment
Bifano, M. 62nd AASLD 2011
~40%
Total concentrations appear lower, but free amount is unchanged.
↓~40%

4. Portal-Systemic Shunting DAA
Portal vein
Gut wall To feces
Metabolism Metabolism
Absorption
Bioavailability:
Liver
CYP
P-gp efflux
CYP CYP
CYP
CYP
CYP CYP CYP CYP
Portal vein Systemic circulation
Fraction extracted and metabolized (EH)
(Fraction escaping extraction): F = 1-EH
Summary
• Tremendous need for antiviral clinical pharmacology research in this patient population
• This meeting will continue to grow as new DAA reach the market – Workshop is a good place to review the data and
identify research needs in this special patient population



![Kiser Family Genealogy - · PDF fileKiser Family Genealogy Descendants of Mary Magdalena Kiser [#7] & John Shuler & Abraham Step Generations 1-5 Mark B. Arslan 407 Highlands Lake Drive](https://img.pdfslide.us/doc/110x75/5aa41d337f8b9afa758b75aa/kiser-family-genealogy-family-genealogy-descendants-of-mary-magdalena-kiser-7.jpg)